Embed Size (px)
Citation preview

Chronic Viral Hepatitis B Chronic Viral Hepatitis B and C in Pediatricsand C in Pediatrics
Phyllis Losikoff, MDPhyllis Losikoff, MDEzequiel Neimark, MDEzequiel Neimark, MD
Hasbro Children’s HospitalHasbro Children’s HospitalBrown University Medical SchoolBrown University Medical School
Divisions of Infectious Diseases and Pediatric Divisions of Infectious Diseases and Pediatric Gastroenterology, Hepatology and NutritionGastroenterology, Hepatology and Nutrition

Speakers: Speakers: Phyllis Losikoff and Phyllis Losikoff and Ezequiel Neimark Ezequiel Neimark
Drs. Losikoff and Neimark have documented that Drs. Losikoff and Neimark have documented that he has nothing to disclose.he has nothing to disclose.
Disclosure StatementDisclosure Statement

Phyllis Losikoff and Ezequiel Neimark have Phyllis Losikoff and Ezequiel Neimark have documented that their presentation will not documented that their presentation will not involve discussion of unapproved or off-label, involve discussion of unapproved or off-label, experimental or investigational use.experimental or investigational use.
Off Label Use DisclosureOff Label Use Disclosure

NeimarkNeimark EpidemiologyEpidemiology TransmissionTransmission Natural HistoryNatural History TreatmentTreatment
LosikoffLosikoff PreventionPrevention RI screening and RI screening and
preventionprevention Perinatal Hepatitis Perinatal Hepatitis
ProgramProgram
Chronic Viral Hepatitis B Chronic Viral Hepatitis B and C in Pediatricsand C in Pediatrics

Hepatitis B Virus (HBV)Hepatitis B Virus (HBV)

Epidemiology of Hepatitis B in Epidemiology of Hepatitis B in PediatricsPediatrics
Prevalent in Asia, Africa, Southern Prevalent in Asia, Africa, Southern Europe and South America (2-20%)Europe and South America (2-20%)
Children adopted from AsiaChildren adopted from Asia
Age of infection is important in Age of infection is important in determining the outcome of the determining the outcome of the disease.disease.

Chronic Hepatitis B Chronic Hepatitis B InfectionInfection

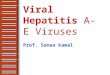
Risk Factors for Hepatitis BRisk Factors for Hepatitis B
40
14
31
15
1 3 30
5
10
15
20
25
30
35
40
1998
Heterosexual
IV Drug
High RiskbehaviorHomosexual
Health CareWorkerHousehold
Unknown

Diagnostic Interpretations of Diagnostic Interpretations of Hepatitis B markersHepatitis B markers
HBsAgHBsAg Non infectious component of viral coat
Indicator of disease. If > 6 months: chronic HBV
Anti-HBsAnti-HBs Antibody response to HBsAg
Indicates recovery and/or immunity
HBeAgHBeAg Antigen that correlates with replication and infectivity
High level of infectivity and replication
Anti-HBeAnti-HBe Antibody response to HBeAg
Decreasing level of replicationRemission/resolution
Anti-HBc Anti-HBc IgMIgM
Non protective antibody to the HBcAg
Recent HBV infection
Anti-HBc IgGAnti-HBc IgG As above Acute or remote exposure to HBV
HBV DNAHBV DNA Replictative genetic material of HBV; infectious agent
Viral replication and continues infection

Diagnostic Interpretations of Diagnostic Interpretations of Hepatitis B markersHepatitis B markers
HBsAgHBsAg Non infectious component of viral coat
Indicator of disease. If > 6 months: chronic HBV
Anti-HBsAnti-HBs Antibody response to HBsAg
Indicates recovery and/or immunity
HBeAgHBeAg Antigen that correlates with replication and infectivity
High level of infectivity and replication
Anti-HBeAnti-HBe Antibody response to HBeAg
Decreasing level of replicationRemission/resolution
Anti-HBc Anti-HBc IgMIgM
Non protective antibody to the HBcAg
Recent HBV infection
Anti-HBc IgGAnti-HBc IgG As above Acute or remote exposure to HBV
HBV DNAHBV DNA Replictative genetic material of HBV; infectious agent
Viral replication and continues infection

Hepatitis B e Antigen Hepatitis B e Antigen (HBeAg)(HBeAg)
•Spontaneous clearance occurs Spontaneous clearance occurs gradually as children agesgradually as children ages
•Low before 3 years of ageLow before 3 years of age
•Increases 5%/year after 3 years of Increases 5%/year after 3 years of ageage
•Most common between 15-30 years Most common between 15-30 years oldold

Natural History of Chronic Natural History of Chronic Hepatitis BHepatitis B
H ep a to ce llu la r ca rcin om a
C irrh os is
D e a th
L ive r Fa i lu re
C h ro n ic H e p ati t is
C h ro n ic H B V in fe ction
A sym pto m atic ca rr ie r

Chronic Hepatitis B Chronic Hepatitis B Infection in PediatricsInfection in Pediatrics
•Mostly asymptomaticMostly asymptomatic
•Normal growthNormal growth
•Liver damage mild during childhoodLiver damage mild during childhood
•Cirrhosis, hepatocellular carcinoma at any age Cirrhosis, hepatocellular carcinoma at any age (rare)(rare)

Zacharakis G. J Pediat Gastr Nutr; 44:84-91.2006
Natural History of Chronic HBV Natural History of Chronic HBV (Pediatrics)(Pediatrics)
•HBeAb seroconversion rate 55% HBeAb seroconversion rate 55% in 12 yearsin 12 years
•Lower seroconversion in vertical Lower seroconversion in vertical transmitted (38.5%) Vs. horizontal transmitted (38.5%) Vs. horizontal (74%)(74%)
•Loss of HBsAg seen in 5%Loss of HBsAg seen in 5%

Courtesy of Jerrold R. Turner, M.D., Ph.D.
Hepatitis B Liver BiopsyHepatitis B Liver Biopsy

Courtesy of Jerrold R. Turner, M.D., Ph.D.
Hepatitis B Liver BiopsyHepatitis B Liver Biopsy

Courtesy of Jerrold R. Turner, M.D., Ph.D.
Hepatitis B Liver BiopsyHepatitis B Liver Biopsy

Courtesy of Jerrold R. Turner, M.D., Ph.D.
Hepatitis B Liver BiopsyHepatitis B Liver Biopsy

Who to treat?Who to treat?
High ALTHigh ALT Inflammation in biopsyInflammation in biopsy Low HBV DNALow HBV DNA Late acquisition of Late acquisition of
infectioninfection
Better Better Response Response
to to treatmentreatmen
tt
Better Better Response Response
to to treatmentreatmen
tt
Mei-Hwei Chang. Pediatric Gastroint Dis. 2004
Children with chronic HBV (HBsAg > 6 months)Children with chronic HBV (HBsAg > 6 months)

Goals of treatment in Pediatric Goals of treatment in Pediatric populationpopulation
Reducing the risk of HBV related Reducing the risk of HBV related cirrhosis and HCCcirrhosis and HCC
Elimination of HBeAg may Elimination of HBeAg may
considerable improve prognosisconsiderable improve prognosis

How to treat?How to treat?
PediatricsPediatrics
IFN-IFN-αα LamivudinLamivudinee

How to treat?How to treat?
PediatricsPediatrics
IFN-IFN-αα LamivudinLamivudinee
AdefovirAdefovirEntecavirEntecavir

INF-INF-αα
Approx 58% of patient responseApprox 58% of patient response Pros:Pros:
More durable responseMore durable response Fixed duration of treatmentFixed duration of treatment Lack of resistant mutantsLack of resistant mutants
Cons:Cons: Weekly SC administrationWeekly SC administration Very expensiveVery expensive Adverse reactions:Adverse reactions: Flu-like symptoms, Flu-like symptoms,
depression, anorexia, bone marrow suppressiondepression, anorexia, bone marrow suppression

LamivudineLamivudine
Virologic response in children, 23% Virologic response in children, 23% compared to 13% in placebocompared to 13% in placebo
Pros:Pros: OralOral Well toleratedWell tolerated CheapCheap
Cons:Cons: Less durability of responseLess durability of response Increased risk of drug resistant , 70% by 5 yearsIncreased risk of drug resistant , 70% by 5 years

Courtesy of the C. Everett Koop Institute at Dartmouth
Hepatitis C Virus Hepatitis C Virus (HCV)(HCV)

El-Kamary SS. J Pediatr. 143:54-9, 2003.
Jonas MM. J Pediatr. 131:314-6, 1997.
Yeung LT. Hepatology. 34:223-9, 2001.
Aletr MJ. N Engl J Med. 341; 556-62. 1999
Prevalence of Hepatitis Prevalence of Hepatitis CC
•1.8% prevalence in US (NHANES III)1.8% prevalence in US (NHANES III)
•150,000-200,000 US children with 150,000-200,000 US children with HCVHCV
•10,000-60,000 newborn will be 10,000-60,000 newborn will be infected worldwide yearlyinfected worldwide yearly

Prevalence of Hepatitis Prevalence of Hepatitis CC

Genotype Distribution Genotype Distribution of Hepatitis Cof Hepatitis C

Mode of Mode of Transmission of Transmission of
Hepatitis CHepatitis C•Transfusion of blood or contaminated Transfusion of blood or contaminated products (prior to 1992)products (prior to 1992)
•Use of intravenous drugsUse of intravenous drugs
•SexualSexual
•Vertical (most important among Vertical (most important among children)children)

Mast EE. J Infect Dis. 192:1880-1889, 2005
Perinatal Perinatal Transmission of Transmission of
Hepatitis CHepatitis C•3.7% of the infants acquired HCV.3.7% of the infants acquired HCV.
•Infection rate in HIV positive mothers, Infection rate in HIV positive mothers, 25%25%
•Multivariate analysis for infected Multivariate analysis for infected mothers, membrane rupture for >6 h and mothers, membrane rupture for >6 h and internal fetal monitoring were associated internal fetal monitoring were associated with maternal transmission of HCVwith maternal transmission of HCV

Breast feeding and Breast feeding and transmission of Hepatitis transmission of Hepatitis
CC• HCV detected in breast milk and colostrumHCV detected in breast milk and colostrum
• Rate of transmission identical to bottle-fed Rate of transmission identical to bottle-fed infantsinfants
• Safety based on the absence of traumatized, Safety based on the absence of traumatized, cracked or bleeding nipplescracked or bleeding nipples
Yeung LT. Hepatology.34:223-9, 2001.

Risk Factors for Vertical Risk Factors for Vertical Transmission of Hepatitis CTransmission of Hepatitis C
Does not increaseDoes not increase vertical vertical transmission:transmission:
Breast feedingBreast feeding Vaginal deliveryVaginal delivery
Mast EE. J Infect Dis. 192:1880-1889, 2005

Risk Factors for Vertical Risk Factors for Vertical Transmission of Hepatitis CTransmission of Hepatitis C
Does increaseDoes increase vertical transmission: vertical transmission: Use of internal fetal monitoring Use of internal fetal monitoring
devicesdevices High viral loadsHigh viral loads Prolonged rupture of membranes Prolonged rupture of membranes
(>6 h)(>6 h) HIV co-infectionHIV co-infection
Mast EE. J Infect Dis. 192:1880-1889, 2005

Natural History of Natural History of Hepatitis CHepatitis C
ExposureExposure
No No infectioninfection
AcuteAcuteChronicChronic
SpontaneoSpontaneous us
clearance clearance (early)(early)
•CirrhosiCirrhosis s (20-40%)(20-40%)
•HCC HCC (1-4%/year)(1-4%/year)
<75%<75%
>20%>20%



England K. J Pediatr. 147:227-32, 2005.
Clinical Features of Clinical Features of Hepatitis C in Hepatitis C in
PediatricsPediatrics•Normal growthNormal growth
•Mostly are asymptomaticMostly are asymptomatic
•Hepatomegaly 2-61%Hepatomegaly 2-61%
•Elevated liver enzymes 44-93%Elevated liver enzymes 44-93%

Diagnosis of Diagnosis of Hepatitis CHepatitis C
HCV HCV antibodies antibodies (IgG)(IgG)
HCV RNA PCR HCV RNA PCR (quantitative/qualitativ(quantitative/qualitative)e)
Initial Initial screeningscreeningDiagnosisDiagnosis
Confirmation of DiagnosisConfirmation of Diagnosis (qualitative)(qualitative)
Pretreatment Pretreatment evaluationevaluationPost treatment Post treatment monitormonitor

Kelly DA. Hepatology; 34:680A. 2001
Wirth S. Hepatology; 36:1280-4. 2002
Davis GL. N Engl J Med; 339:1493-9.1998
McHutchinson JG. N Engl J Med; 339:1485-92.1998
Antiviral Therapy for Antiviral Therapy for Hepatitis CHepatitis C
•Combined PEG interferon and Combined PEG interferon and RibavarinRibavarin
•45-62% sustained virological response45-62% sustained virological response
•Better responseBetter response
•Ribavirin Side effectsRibavirin Side effects
•Anemia/ThrombocytopeniaAnemia/Thrombocytopenia
•Fetal malformationsFetal malformations
Genotype 2, Genotype 2, 33Low pretreatment viral Low pretreatment viral loadloadYounger ageYounger age
Absence of cirrhosisAbsence of cirrhosis

Hepatitis B vs. Hepatitis Hepatitis B vs. Hepatitis CC
Hepatitis BHepatitis B Hepatitis CHepatitis C
PrevalencePrevalence DecreasingDecreasing IncreasingIncreasing
TransmissioTransmissionn
Blood, SexualBlood, Sexual Blood, SexualBlood, Sexual
Natural Natural HistoryHistory
Carrier, Carrier, clearance, clearance,
cirrhosis, HCCcirrhosis, HCC
Similar but Similar but unknownunknown
TreatmentTreatment INF, INF, Lamivudine, Lamivudine,
Adefovir, Adefovir, EntecavirEntecavir
INF/RibavirinINF/Ribavirin

Chronic Viral Hepatitis in Chronic Viral Hepatitis in PediatricsPediatrics
PreventionPrevention

The Good News: Hepatitis BThe Good News: Hepatitis B
(HBV)(HBV)VaccineVaccineHBsAg recombinant DNA technology HBsAg recombinant DNA technology
90%-95% efficacy (anti-HBs titers 90%-95% efficacy (anti-HBs titers >> 10mIU/ml) 10mIU/ml)Long-term protection Long-term protection
Post Exposure Prophylaxis(PEP)Post Exposure Prophylaxis(PEP)Hep B Immunoglobulin(HBIG) passively acquired anti-HBs Hep B Immunoglobulin(HBIG) passively acquired anti-HBs
Infants born to HBsAg+ mothers Infants born to HBsAg+ mothers (HBIG & vaccine, efficacy 95% )(HBIG & vaccine, efficacy 95% )

Advisory Committee on Immunization Advisory Committee on Immunization Practices (ACIP) 1991Practices (ACIP) 1991
Comprehensive National Strategy to Eliminate Comprehensive National Strategy to Eliminate Transmission of HBVTransmission of HBV
Prevent perinatal HBV transmissionUniversal infant vaccination Catch-up vaccination of all children and
adolescents <19 years
Vaccination of adults in high risk groups
Well Conceived Public Health Strategy?Well Conceived Public Health Strategy?
In Taiwan rates of HCC among children born after In Taiwan rates of HCC among children born after routine immunization was started have declined >50%. routine immunization was started have declined >50%.

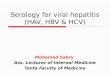
A Well Conceived Public Health StrategyA Well Conceived Public Health StrategyReported Acute HBV Incidence by Age Group: Reported Acute HBV Incidence by Age Group:
US, 1990-2004US, 1990-2004
0
2
4
6
8
10
12
1990 1992 1994 1996 1998 2000 2002 2004
≥20 years
12-19 years
<12 years
71% decline71% decline94% decline94% decline
Year
Case
s per
100
,00
0

HBV: Despite Success Challenges RemainHBV: Despite Success Challenges Remain
Identified &Expected Births to HBsAg + Mothers; 1993-2003Identified &Expected Births to HBsAg + Mothers; 1993-2003
0
20
40
60
80
100
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
Year
Perc
ent
Iden
tifie
d
0
5000
10000
15000
20000
Expe
cted
Num
ber
Expected number
Percent identified
Source: National Immunization Program, CDC
48%
23,827
19,043
41%

HBV: Remaining ChallengesHBV: Remaining ChallengesProportion of Infants Receiving Birth Dose, Proportion of Infants Receiving Birth Dose,
1999-20041999-2004
0102030405060708090
100
1999 2000 2001 2002 2003 2004
Year
Perc
ent
of I
nfan
ts
46.0%53.7%
Source: CDC, National Immunization SurveySource: CDC, National Immunization Survey
Hepatitis B Vaccine 0-2 Days from Birth

HBV: Remaining ChallengesHBV: Remaining ChallengesMedical ErrorsMedical Errors
Baby girl; DOB: 9/99Baby girl; DOB: 9/99Died: 12/99; Cause - fulminant hepatitis B Died: 12/99; Cause - fulminant hepatitis B Mother tested HBsAg-positive during pregnancyMother tested HBsAg-positive during pregnancy
Prenatal care providerPrenatal care providerMade a transcription error and reported mother as Made a transcription error and reported mother as
“hepatitis negative” to the hospital “hepatitis negative” to the hospital Used prenatal record form from 1966Used prenatal record form from 1966Did not report HBsAg-positive test (Michigan law)Did not report HBsAg-positive test (Michigan law)
Hospital staffHospital staffRelied on written record from prenatal providerRelied on written record from prenatal providerDid not have a copy of mother’s laboratory resultDid not have a copy of mother’s laboratory result

HBV: ACIP New RecommendationsHBV: ACIP New Recommendations
December 2005December 2005
Improve prevention of perinatal and Improve prevention of perinatal and early childhood HBV transmission early childhood HBV transmission
Improve hepatitis B vaccine coverage Improve hepatitis B vaccine coverage in children/adolescents not previously in children/adolescents not previously vaccinatedvaccinated

HBV: ACIP 2005 RecommendationsHBV: ACIP 2005 RecommendationsThe Hospital is aThe Hospital is a SAFETY NETSAFETY NET
1.1. Universal verificationUniversal verification of maternal HBsAg status in of maternal HBsAg status in the hospitalthe hospital
2.2. Identification of infants born to HBsAg-positive Identification of infants born to HBsAg-positive and HBsAg-unknown status women, and HBsAg-unknown status women, administration of administration of PEP PEP and initiation ofand initiation of case case management to monitor completion of vaccine management to monitor completion of vaccine series and post vaccination testingseries and post vaccination testing
3.3. Universal birth dose administrationUniversal birth dose administration

HBV: ACIP 2005 RecommendationsHBV: ACIP 2005 Recommendations
Birth Dose Birth Dose
““For all medically stable infants weighing ≥2,000 grams For all medically stable infants weighing ≥2,000 grams
at birth and born to HBsAg negative mothers, the first at birth and born to HBsAg negative mothers, the first
dose of vaccine should be administered before hospital dose of vaccine should be administered before hospital
discharge.” discharge.”
Exceptions on a case-by case basis and rareExceptions on a case-by case basis and rare. .
If birth dose delayed, medical record should document: If birth dose delayed, medical record should document:
physician’s order not to administer birth dose physician’s order not to administer birth dose
copy of original laboratory report indicating copy of original laboratory report indicating mother was mother was HBsAg-negative during this HBsAg-negative during this pregnancypregnancy

ACIP 2005ACIP 2005HBV Vaccination of Children and AdolescentsHBV Vaccination of Children and Adolescents
Not Previously Vaccinated Not Previously Vaccinated
Immunization record reviews should be conducted for:Immunization record reviews should be conducted for: all children aged 11-12 yearsall children aged 11-12 years
all children and adolescents <19 years:all children and adolescents <19 years:
born in Asia, the Pacific Islands, Africa, or other countriesborn in Asia, the Pacific Islands, Africa, or other countries w/ HBsAg prevalence >2% w/ HBsAg prevalence >2%
who have at least one parent who was born in these countrieswho have at least one parent who was born in these countries
Children not previously vaccinated or incompletely vaccinated Children not previously vaccinated or incompletely vaccinated should complete the vaccine seriesshould complete the vaccine series

Prevention HBV Rhode IslandPrevention HBV Rhode Island
2004 Birth dose coverage 84% 2004 Birth dose coverage 84%
97% infants born to HBsAg+ women received 97% infants born to HBsAg+ women received PEP w/in 24PEP w/in 24oo
Perinatal Hepatitis Prevention ProgramPerinatal Hepatitis Prevention Program
YearYear HBV exposed infantsHBV exposed infants
20052005 67 67 20062006 46 46

Prevention HBV Rhode IslandPrevention HBV Rhode Island
Vaccinate Before you GraduateVaccinate Before you Graduate
Hepatitis B Vaccination provided to juveniles Hepatitis B Vaccination provided to juveniles at the Rhode Island Training Schoolat the Rhode Island Training School

Prevention Prevention The Less Good News: HepatitisThe Less Good News: Hepatitis CC
There is NO effective vaccineThere is NO effective vaccine
Spontaneous clearance of HCV can occur in Spontaneous clearance of HCV can occur in 20-50% of acute infections20-50% of acute infections
Immunity against persistent HCV can be acquiredImmunity against persistent HCV can be acquired

Prevention HCVPrevention HCVImmune Correlates of Viral ClearanceImmune Correlates of Viral Clearance
Humoral Immunity Humoral Immunity Neutralizing antibodies, in vitro, are not necessary for Neutralizing antibodies, in vitro, are not necessary for
resolution of HCV infection.resolution of HCV infection.
Cellular ImmunityCellular Immunity Vigorous polyclonal CD4+ and CD8+ T-cell responses Vigorous polyclonal CD4+ and CD8+ T-cell responses
Weak and narrowly in chronically infectedWeak and narrowly in chronically infected

HCVHCV Cellular Immune Response in Acute Cellular Immune Response in Acute
InfectionInfection
Bowen and Walker, Nature 2005

Prevention HCV Prevention HCV
Acquired Immunity to HCV InfectionAcquired Immunity to HCV Infection The majority of re-exposed individuals do not develop The majority of re-exposed individuals do not develop
chronic diseasechronic disease
Risk for chronic infection after re-exposure to HCV was 12-Risk for chronic infection after re-exposure to HCV was 12-fold fold lowerlower among persons with prior HCV infection among persons with prior HCV infection
Mehta 2002 LancetMehta 2002 Lancet Resolution of HCV infection results in durable memory cells Resolution of HCV infection results in durable memory cells
Subjects who resolved an infection from a single Subjects who resolved an infection from a single contaminated source had strong HCV-specific T-cell contaminated source had strong HCV-specific T-cell immunity 18 years later immunity 18 years later Takaki 2000 Nature MedTakaki 2000 Nature Med

National HCV Prevention StrategyNational HCV Prevention StrategyIdentifying and Screening At Risk IndividualsIdentifying and Screening At Risk Individuals
Increased screening and knowledge of HCV status Increased screening and knowledge of HCV status reduces HCV transmissionreduces HCV transmission
Kwiatkowski 2002 AddictionKwiatkowski 2002 AddictionHagan 2001 Am J Pub HealthHagan 2001 Am J Pub Health
Treatment options (early therapy more efficacious)Treatment options (early therapy more efficacious)Test for co-infection (HIV,HBV)Test for co-infection (HIV,HBV)Education alcohol cessation, risk reductionEducation alcohol cessation, risk reductionHepatitis A and B vaccinationHepatitis A and B vaccination
2/3 of people with chronic HCV are not 2/3 of people with chronic HCV are not diagnoseddiagnosed
*No federal funding is available to support HCV counseling and *No federal funding is available to support HCV counseling and testing services.testing services.

HCV Prevention HCV Prevention Risk Based ScreeningRisk Based Screening
Ever injected illegal drugsEver injected illegal drugs
Blood transfusion or organ transplant before July Blood transfusion or organ transplant before July 1992 or clotting factor before 1987 or ever on 1992 or clotting factor before 1987 or ever on long-term dialysislong-term dialysis
Children born to HCV-positive womenChildren born to HCV-positive womenNo routine testing for pregnant womenNo routine testing for pregnant women

HCV Prevention HCV Prevention Risk Based ScreeningRisk Based Screening
Sexual Transmission(2-6%) Sexual Transmission(2-6%) Tahan 2005 Am J GastroTahan 2005 Am J Gastro
Magder 2005 Int J of EpiMagder 2005 Int J of Epi
Intranasal Drug Use *Intranasal Drug Use *Household contacts of HCV positiveHousehold contacts of HCV positiveCosmetic procedures; tatooing, piercing*Cosmetic procedures; tatooing, piercing*
Hand 2005 Am J GastroHand 2005 Am J Gastro **Hwang 2006 Hwang 2006
HepatologyHepatology
10% of people with HCV infection have 10% of people with HCV infection have no recognized source for their infection no recognized source for their infection

Rhode Island HCVRhode Island HCV At Risk Pediatric Populations At Risk Pediatric Populations
Rhode Island Training SchoolRhode Island Training School; Risk based screening; Risk based screening
1% (5/484) HCV positive0.4% prevalence in the general adolescent population
12% reported intravenous or intranasal drug use Losikoff 2004 NCCHC, New Orleans La.
Perinatal HCV Exposure
Estimated 150-200 infants born to HCV + mothers annually Estimated 150-200 infants born to HCV + mothers annually

Perinatal Hepatitis ProgramPerinatal Hepatitis ProgramRhode Island Department of HealthRhode Island Department of Health
2005 Rhode Island expanded the Perinatal Hepatitis 2005 Rhode Island expanded the Perinatal Hepatitis Prevention Program to include services for pregnant Prevention Program to include services for pregnant women with HCV and case management of their women with HCV and case management of their infants infants
YearYear HCV+ mother/infant pairs HCV+ mother/infant pairs 20052005 35 3520062006 26 26
Department of Health: Department of Health: Pat Raymond RN, Susan Ferrara RNPat Raymond RN, Susan Ferrara RN W&I Center for Womens’ GI Disorders: W&I Center for Womens’ GI Disorders: Dr Silvia Degli-Esposti, DirectorDr Silvia Degli-Esposti, DirectorPediatric Viral Hepatitis Clinic Pediatric Viral Hepatitis Clinic

Pediatric Viral Hepatitis ClinicPediatric Viral Hepatitis Clinic
Resource for Providers and Families in Resource for Providers and Families in Rhode Island Rhode Island
444-6191444-6191
Ezequiel NeimarkEzequiel Neimark Phyllis LosikoffPhyllis Losikoff