Embed Size (px)
Citation preview

1
Chronic Stroke Review Tool and
Intervention Guide
(Chronic Stroke Rev-TIG)
Victorian Stroke Clinical Network – Enhancing Stroke Care Program
Acknowledgement: This project was supported by a grant from the
Victorian Stroke Clinical Network (VSCN).
18th May, 2015
2
Introduction
In Australia, stroke is a leading cause of long-term, permanent disability. In 2003, more than 140,000 Australians were living with a disability as a result of their stroke [1]. Most stroke survivors live at home, with half of these individuals requiring assistance to complete some aspects of their daily life, such as household chores, home maintenance and transport [1]. Informal carers provide most of the assistance required for these, and many other activities. Given the incidence of stroke is increasing due to an ageing population, and that close to 20 per cent of all strokes occur to people under 55 years old, the need to optimise the recovery of people with stroke is clear [2]. As the Victorian Stroke Care Strategy outlines, stroke survivors and their carers often experience an intense and difficult lifestyle adjustment as they attempt to resume their former way of living [3]. After the initial intensive rehabilitation period (both inpatient and ambulatory), there may be a lack of access to community-based services and programs that can provide support for the adjustment, potential lifestyle change and loss of independence, and to facilitate community reintegration and return to a healthy and active lifestyle, in the context of disability. Individuals who have had a stroke should have a review by a healthcare clinician with stroke care expertise at least three, six, and twelve months after discharge from hospital (with at least one review being conducted by specialist medical practitioner) [4, 5]. The Australian Clinical Guidelines for Stroke Management (National Stroke Foundation, 2010) recommend annual reviews for those people who have ongoing impairments in order to determine current status and the merits for further intervention [4]. In addition, the person who has had a stroke and their family/carer should have access to the details of a relevant contact person within the community setting [4]. Whilst the Clinical guidelines of the National Stroke Foundation (NSF) for stroke rehabilitation and recovery present evidence-based recommendations, these guidelines are not specific to the community setting [4]. The Chronic Stroke Review Tool and Intervention Guide (Chronic Stroke Rev-TIG) has been designed specifically to enhance the recovery process and minimise functional decline of individuals who have had a stroke and are in the chronic phase of recovery (that is, at least six months post the stroke event). The Chronic Stroke Rev-TIG does not address the initial community based rehabilitation phase following acute stroke. These services are well established in Victoria’s community rehabilitation sector. Purpose The purpose of the Chronic Stroke Rev-TIG is to provide guidelines on current evidence-based practice for the multidisciplinary assessment, treatment and overall management of chronic stroke survivors within the community setting. The development of this resource and assessment tool will support high quality care for stroke survivors within the community setting. It will ensure greater access to evidence-based information for clinicians, have potential to improve patient outcomes through timely and effective patient management, and will also result in greater consistency in the assessment and treatment of this patient population across Victoria. Aims
To provide a literature review of current evidence-based practice in the management of chronic stroke survivors
To provide a comprehensive, multidisciplinary assessment form based on current evidence-based practice with flags for treatment interventions
To provide intervention guidelines to direct appropriate treatment, and enhance referrals to other health services as required
To assist community organizations providing stroke care to meet the recommendations of the Stroke Care Strategy for Victoria
Intended Audience The Rev-TIG has been designed as a resource for Clinicians working with chronic stroke survivors who have completed their post stroke rehabilitation, and who are seeking ongoing assistance and management. This toolkit is preferably for use by a multidisciplinary team in the community setting.

3
Contents of the Chronic Stroke Rev-TIG The Rev-TIG contains guidelines for assessment and management under specific domains:
1. Participation 2. Functional limitations and decline 3. Minimising risk of falls 4. Communication 5. Cognition 6. Mood Status / Depression 7. Health-related quality of life 8. Secondary stroke prevention and risk factor management 9. Carer support 10. Goal setting
The Chronic Stroke Rev-TIG also contains a screening assessment summary. This two-page assessment summary is designed to be filed in the individual’s medical record, given to the stroke survivor and their carer, and sent as a summary to the individual’s general practitioner. Note that not all domains that are outlined in the Rev-TIG will be of relevance to all individuals. It is recommended that community based clinicians be discerning with the use of this kit, and use the screening assessments to identify ‘Flags’ that require further investigation as to their impact on the post-stroke recovery process. The domains that are covered in the Rev-TIG are not exhaustive with regards to the problems and issues that may be encountered by an individual post-stroke. Some aspects are not covered in detail (for example, vocational training, sexuality issues), and community based clinicians should explore further resources pertaining to the issues that arise during individual consultations. It is important to adopt a person-centred approach to the management of chronic stroke sequelae, using strategies such as implementing appropriate collaborative goal setting and healthcare management plans. The person who has had a stroke should be considered as an equal partner in the healthcare relationship, with respect and dignity. Considerable focus in this Kit is placed on the concepts of goal identification and participation, as these areas require a person-centred practice. Table of Contents for Rev-TIG
Component Information for the following domains: 1. Participation (p. 3) 2. Functional limitations and decline (p. 7) 3. Minimising risk of falls (p. 11) 4. Communication (p. 14) 5. Cognition (p. 16) 6. Mood Status / Depression (p. 20) 7. Health-related quality of life (p. 24) 8. Secondary stroke prevention and risk factor management (p. 26) 9. Carer support (p. 29) 10. Goal setting (p. 33)
Chronic Stroke Rev-TIG Screening Assessment (p. 40)
Chronic Stroke Rev-TIG Screening Assessment Summary and Care Plan (p46) References 1. Senes, S. How we manage stroke in Australia. 2006, Australia: Australian Institute of Health
and Welfare. 2. Australian Institute of Health and Welfare. Australian Facts: Heart, stroke and vascular
diseases. 2004, Australia: Australian Institute of Health and Welfare. 3. Victorian Government Department of Human Services, Stroke Care Strategy for Victoria.
2007, Melbourne, Australia. 4. National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne 5. Lindsay, P., et al., Canadian best practice recommendations for stroke care.
Canadian Medical Association Journal, 2008. 179(12): p. S1-S25.

4
Domain 1: Participation
Background Efforts to enhance activity status and minimise limitations to participation for patients post-stroke remain key aims of the rehabilitation process. Participation is described as an ‘involvement in a life situation’, with the participation restrictions being therefore defined as ‘problems an individual may experience in involvement in life experiences’ [1, p12]. The notion of participation has been constructed into a framework involving six dimensions: physical independence, orientation, mobility, social integration, occupation and financial self-sufficiency [2]. Of particular importance to the Rev-TIG is the facet of the participation concept that encompasses aspects of personal and social community re-integration, and a return to valued and meaningful activities. Valued activities are an individual phenomenon, and may relate to life aspects such as: domestic, family, and social roles; employment; hobbies, socialising; and sporting pursuits [3]. The event of a stroke has been shown to have an adverse effect on participation levels, with a deterioration in engagement in social, leisure, and vocational activities being common post-stroke [4, 5, 6]. In particular, deficits in ability to mobilise and the presence of depressive symptoms are predictive of lower participation status [7]. An individual’s participation in vocational and leisure activities has been associated with their perception of life satisfaction and level of social integration [5, 8]. Reduction in social activity status also has implications in the development of depressed mood post-stroke. Monitoring of social activities and the reduction, or withdrawal, from social events and valued activities is an important aspect of post-stroke management [9]. Rehabilitation services have been identified as having a long-term role in the identification and management of aspects that lead to the resumption of valued activities post-stroke [3]. Interventions targeting participation and leisure pursuits may result in improved participation status and health related quality of life [4,10].
Participation Screening Assessment Identification of valued activities Questions to explore with the patient / carer:
What activities did you enjoy doing prior to the event of your stroke?
What activities do you enjoy or value now? Document current participation status in relation to the identified activities (devise a daily/weekly activity profile). Determine whether the activity has been ceased, continuing, or is a new activity since the stroke event. Highlight those activities in the profile that the patient particularly values.
What stops you from engaging in activities that you enjoy or value? (Determine any barriers contributing to a reduced participation status)
Who do you see regularly? (Determine level of social interaction)
Valued activities prior to stroke Level of participation (e.g. daily, weekly etc)
Current activity status Level of participation (e.g. daily, weekly etc)

5
Main barriers to participation in above activities (consider community access, transportation, social support network):
Level of social support / Status of family role / Adaptation and adjustment to altered status: Who do you see regularly?
Level of social interaction: Increased since stroke Reduced since stroke
Similar to pre-stroke Severely reduced since stroke
Concerns with family role / Adjustment to altered roles:
Specific ‘Flags’:
- Altered participation status. Failure to resume, or reduced participation in, valued activities - Reduced community access / transportation issues - Reduced social support network - Identified problems with family role / Adjustment concerns
Interventions Interventions that have shown to affect social activity and participation status [4, 8] include:
Targeted rehabilitation services
Leisure therapy
Active case management
Day service programs
Those patients who have been identified by the screening process as having limitations to their participation status should be assisted with:
Identification and documentation of specific valued activities and goals (Refer also to ‘Goal Setting’ component)
Treatment care plan and strategies that aim to facilitate re-engagement in desired social, vocational, and leisure/recreational activities. Address barriers to participation status.
Facilitate community access (Consider: Outdoor physical mobility status, Public transport ability, Social network support, Community transport options, Driving status, Scooter/Wheelchair options)
Education and exploration about adapted or new activities (especially with regard to desired activities that are difficult to accomplish due to severity of the sequelae post-stroke). Supporting adaptation and adjustment to alterations in abilities.
Monitoring of participation status and level of goal attainment
Strategies to promote and enhance social support
Strategies to address identified family role issues
Additional Referral options: Consider providing guidance regarding linkages to:
Community support resources (appropriate social and activity groups)
Local stroke support group
Transportation resources (such as community and council services, taxi vouchers)
Referral to an occupational therapist who may address the following: o Evaluation for return to work o Evaluation for driving ability and community access alternatives
Education and counselling services for support with family role / relationship aspects
Social Work services
Psychology services

6
NSF sessions
References 1. World Health Organisation, International Classification of Functioning, Disability and Health:
ICF. 2001, Geneva: World Health Organisation. 2. World Health Organisation, International Classification of impairments, disabilities and
handicaps. 1980, WHO: Geneva. 3. Robison, J., et al., Resuming previously valued activities post-stroke: who or what helps?
Disability and Rehabilitation, 2009. 31(19): p. 1555-1566. 4. Salter, K., et al. The evidence-based review of stroke rehabilitation (EBRSR): Community
reintegration. 2008 [cited August 2010]; Available from: www.ebrsr.com. 5. Black-Schaffer, R.M. and L. Lemieux, Vocational outcome after stroke. Topics in Stroke
Rehabilitation, 1994. 1(1): p. 74-86. 6. O’Sullivan, C. and Chard, G. An exploration of participation in leisure activities post stroke
Australian Journal of Occupational Therapy, 2010. 57: p. 159-166 7. Desrosiers, J., et al., Short-term changes in and predictors of participation of older adults after
stroke following acute care or rehabilitation. Neurorehabilitation and Neural Repair, 2008. 22: p. 288-297.
8. Parker, C.J., J.R.F. Gladman, and A.E.R. Drummond, The role of leisure in stroke rehabilitation. Disability and Rehabilitation, 1997. 19(1): p. 1-5.
9. Lindsay, P., et al., Canadian best practice recommendations for stroke care. Canadian Medical Association Journal, 2008. 179(12): p. S1-S25.
10. Graven, C., et al., Are rehabilitation and/or care-co-ordination interventions delivered in the community effective in reducing depression, facilitating participation and improving quality of life after stroke? Disability and Rehabilitation, 2011: p. 1-20.

7
Domain 2: Functional limitations and decline
Background Functional limitations and decline Residual activity limitations in bathing, dressing, feeding, and stair climbing skills are common in stroke survivors greater than one year post-stroke [1]. Whilst these activity limitations may exist, often these individuals are no longer linked into formal rehabilitation services [2]. Ongoing physiotherapy, occupational therapy and speech therapy rehabilitation may further improve an individual’s functional abilities in the chronic phase of recovery, that is greater than six months post-stroke [2,3]. Whilst activity limitations may exist, clinicians also need to be aware that long-term functional decline is common following stroke [4-6]. While reduced functional abilities may occur as the result of recurrent strokes and other disabling co-morbidities, functional decline may also occur independently of these factors [4,5]. Decline of function in stroke survivors has been demonstrated over a five-year period, with individuals gradually becoming more dependent over this time [4]. Several factors have been associated with long-term functional decline in stroke survivors. These include age, diabetes mellitus, marital status/social support, stroke severity, side of stroke (commonly right), and urinary continence [4]. Deterioration of walking ability following stroke may occur over time, with approximately one-fifth of chronic stroke survivors experiencing mobility decline within three years of their stroke [7]. Decline in walking ability post-stroke has been linked with poor levels of activity, depression, cognitive factors and fatigue [7,8]. Reduced walking ability may not only contribute to dependence in personal activities of daily living but also lead to social isolation [7]. Like functional limitations, functional decline and deterioration of walking ability normally occurs when individuals following stroke are no longer linked into formal rehabilitation services [4-8]. Given chronic stroke survivors are at risk of functional decline, deterioration in these abilities should be routinely screened for by community based allied health clinicians [5]. If functional decline is identified as part of the assessment process, and realistic and meaningful goals to the individual can be set, then interventions that address these goals should be considered. Fatigue Fatigue is also common following stroke. Forty to seventy percent of stroke survivors may experience fatigue for more than one year post event [5]. Post-stroke or ‘’pathologic’ fatigue is characterised by weariness unrelated to previous exertion levels and is generally not improved by rest [9]. This is in contrast to ‘normal’ fatigue that results from overexertion and may be improved with rest. The aetiology of fatigue after stroke is uncertain [10].
Functional limitations and decline screening assessment Functional Status:
How has your mobility / walking / stairs been recently?
Improved Same Declined
What precipitated this change?
How far can you walk before you are tired?
Comments:
Are you able to use your arm? Yes No
Has this changed recently? Improved Same Declined
Comments:
Are you able to perform self care tasks without help? eg. Showering, dressing, grooming
Yes No
Has this changed recently? Improved Same Declined
Comments:

8
Fatigue:
Over the past month, have you felt fatigued, had a lack of energy, or have had to rest every day for a period of two weeks? [11]
Yes No
Has this fatigue led to difficulty completing tasks that you normally do as part of your daily life?
Yes No
Continence:
Do concerns about continence limit your ability to get out and about?
Yes No
Comments:
Specific ‘Flags’:
- Deterioration in mobility / level of function over time - Specific mobility/functional goals that may be achievable with a burst of therapist input - Fatigue limiting ability to perform activities of daily living
Interventions Functional decline is often a multifaceted issue, and as with depression, should be managed in such a way that addresses the nature of the presentation. Depending on the area of functional decline and possible causes, the following referral options should be considered:
Physiotherapy
Occupational Therapy
Speech Therapy
General Medical Practitioner
Continence Services
Community resources (PCA, MOW, HH etc.) Referral to physiotherapy and occupational therapy may assist in reducing functional decline and improving functional abilities by addressing the following:
Cardiovascular exercise
Strength training
Gait retraining
Constraint-induced movement therapy
Botulinum toxin A
Ankle-foot orthoses Practical management strategies should also be provided by community based clinicians if fatigue is identified as an issue as part of the screening process. Cardiovascular Training Reduced cardiorespiratory fitness is common in chronic stroke survivors [12]. Cardiovascular training in individuals with chronic stroke has been shown to improve cardiovascular fitness, walking speed and walking endurance in those who have a relatively low risk of cardiac complications with exercise [13,14]. Strength Training Weakness following stroke is a major contributor to limitation of physical activity [15]. Strength training in people following chronic stroke has been found to increase strength, gait speed and functional outcomes and improve quality of life [15,16]. Gait retraining Task specific practice of walking in chronic stroke survivors has been shown to have beneficial effects for improving gait speed and endurance [17]. The effect of walking practice on walking function is less clear [17].

9
Constraint-induced movement therapy Constraint-induced movement therapy involves forced use and the massed practice of the affected arm by restraining the unaffected arm [18]. It may be considered with those stroke survivors who have a minimum of ten degrees active finger/wrist extension, but tend not to use the arm in functional tasks [18,19]. Constraint-induced movement therapy has been found to benefit arm function and improve a patient’s ability to manage activities of daily living [18,19]. Botulinum toxin A The use of Botulinum toxin A to reduce focal spasticity should only be considered when the level of spasticity present interferes with the stroke survivor’s capacity to participate in functional tasks, or the ability to provide care to the individual [5]. Specific injecting of Botulinum toxin A by an appropriately certified medical practitioner has been found to decrease spasticity and facilitate the achievement of patient specific goals based on the goal attainment scale [20]. Ankle-foot orthoses Marked foot drop, equino-varus deformity and medio-lateral instability of the foot may be present in chronic stroke survivors. If these individuals are ambulant and the deformities are not addressed appropriately, then pain may develop and walking ability may deteriorate over the long term. In these cases, it may be appropriate for an ankle-foot orthosis to be prescribed [21]. Ankle foot orthoses have been shown to improve walking speed, efficiency and gait pattern in individuals following stroke [21]. Ground reaction ankle-foot orthoses, which accentuate knee extension in mid-stance, may be appropriate to consider if the individual’s knee normally remains flexed throughout the stance phase of gait. Management Strategies for Fatigue Community based clinicians should recognise stroke survivors with excess levels of fatigue and provide information and practical strategies to these individuals and their families/carers. Potential management strategies include energy management techniques, exercise, establishing good sleep patterns, and avoidance of sedating drugs and excessive alcohol [5]. Continence Continence is frequently affected post-stroke, with alteration to mobility status presenting as a significant predictive factor of incontinence [22]. Health professionals need to be aware of medications and substances that can affect a person’s continence status such as: diuretics, sedatives, alcohol, and caffeine. If the person who has had a stroke has already had specialised continence assessment, they may require assistance and encouragement to follow the management plan. Strategies often include: re-training program, exercise program (targeting pelvic floor muscles), timed toileting, and prompted toileting, and alterations to medications. Additional Resources
National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia. Website www.strokefoundation.com.au/clinical-guidelines
National Stroke Foundation ‘Bladder control after stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au
National Stroke Foundation ‘Fatigue after stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au
National Stroke Foundation ‘Movement and exercise after stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au
Continence Foundation of Australia: Helpline 1800 330 066 Website:
www.continence.org.au Brochures / Booklets / Charts / AV resources
Relevant factsheets available, such as:
- Stroke and bladder and bowel health
- Caring for people with incontinence
- Depression and incontinence
- Bladder control and Bladder habits
- Pelvic floor muscle training
- Continence products

10
References 1. Anderson, C.S., J. Linto, and E.G. Stewart-Wynne, A population based assessment of the impact
and burden of caregiving for long-term stroke survivors. Stroke, 1995. 26: p. 843-849. 2. Werner, R.A. and S. Kessler, Effectiveness of an intensive outpatient rehabilitation program for
postacute stroke patients. American Journal of Physical Medicine and Rehabilitation, 1996. 75(2): p. 114-120.
3. Lindsay, P., et al., Canadian best practice recommendations for stroke care. Canadian Medical Association Journal, 2008. 179(12): p. S1-S25.
4. Dhamoon, M.S., et al., Long-term functional recovery after first ischaemic stroke: the Northern Manhattan study. Stroke, 2009. 40: 2805-2811.
5. National Stroke Foundation. Clinical Guidelines for Stroke Management 2010. http://www.strokefoundation.com.au/news/latest/clinical-guidelines-for-acute-stroke-management-2010
6. Pettersen R., Dahl, T., and Wyller, T.B., Prediction of long-term functional outcome after stroke rehabilitation. Clinical Rehabilitation, 2002. 16: p. 149-159.
7. van de Port, I.G.L., et al., Susceptibility to deterioration of mobility long-term after stroke: a prospective cohort study. Stroke, 2006. 37: p. 167-171.
8. Wijk, I., et al., Change in mobility activity in the second year afters stroke in a rehabilitation population: Who is at Risk for Decline? Archives of Physical Medicine and Rehabilitation, 2006. 87: 45-50.
9. de Groot M, Phillips S, Eskes G. Fatigue associated with stroke and other neurologic conditions: implications for stroke rehabilitation. Arch Phys Med Rehabil. 2003. 84(11): p. 1714–20.
10. McGeough E, Pollock A, Smith LN, Dennis M, Sharpe M, Lewis S, et al. Interventions for post-stroke fatigue. Cochrane Database Syst Rev. 2009, Issue 3. CD007030.
11. Lynch J, Mead G, Greig C, Young A, Lewis S, Sharpe M. Fatigue after stroke: the development and evaluation of a case definition. J Psychosom Res. 2007. 63: p. 539–544.
12. Macko, R.F., et al., Treadmill aerobic exercise training reduces the energy expenditure and cardiovascular demands of hemiparetic gait in chronic stroke patients. A preliminary report. Stroke, 1997. 28(2): 326-30.
13. Pang, M.Y.C., et al., The use of aerobic exercise training in improving aerobic capacity in individuals with stroke: a meta-analysis. Clinical Rehabilitation, 2006. 20(2): p. 97–111.
14. Saunders, D.H., et al. Physical fitness training for stroke patients. Cochrane Database of Systematic Reviews, 2009. Issue 4. Art. No.: CD003316. DOI: 10.1002/14651858.CD003316.pub3.
15. Ada, L., Dorsch, S., and Canning, C., Strengthening interventions increase strength and improve activity after stroke: a systematic review. Journal of Physiotherapy, 2006. 52(4): p. 241–8.
16. Pak, S., Patten, C., Strengthening to promote functional recovery poststroke: an evidence-based review. Topics in Stroke Rehabiltation, 2008. 15(3): p. 177–99.
17. States, R.A., Pappas, E, and Salem, Y. Overground physical therapy gait training for chronic stroke patients with mobility deficits. Cochrane Database of Systematic Reviews, 2009, Issue 3. CD006075.
18. Sirtori, V., et al. Constraint-induced movement therapy for upper extremities in stroke patients. Cochrane Database of Systematic Reviews, 2009, Issue 4. CD004433.
19. Langhorne, P., Coupar, F., and Pollock, A. Motor recovery after stroke: a systematic review. Lancet Neurology. 2009. 8(8): p. 741–54.
20. Rosales, R.L., and Chua-Yap, A.S. Evidence-based systematic review on the efficacy and safety of botulinum toxin-A therapy in post-stroke spasticity. Journal of Neural Transmission, 2008. 115(4): p. 617–23.
21. Leung, J. and Moseley, A. Impact of Ankle-foot orthoses on gait and leg muscle activity in adults with hemiplegia. Physiotherapy, 2002. 89(1): p. 39-55.
22. Deakin University / Eastern Health, A continence resource guide for acute and subactue care settings. 2008: Melbourne Victoria
11
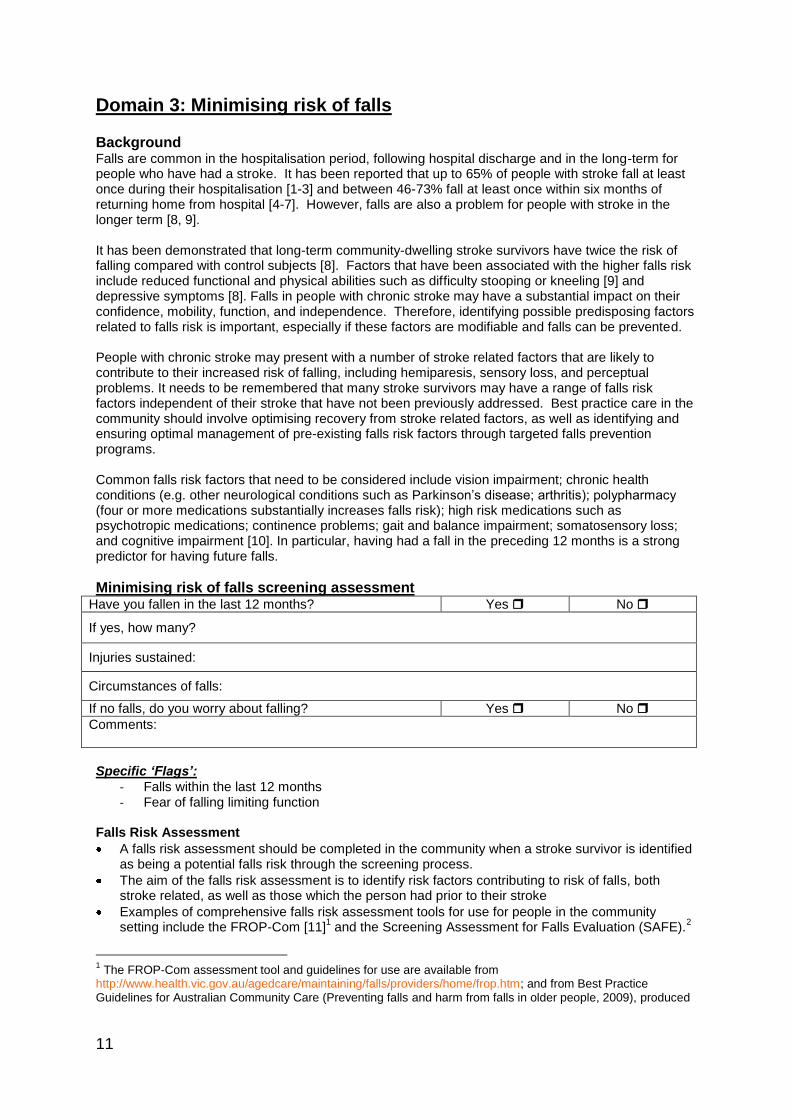
Domain 3: Minimising risk of falls Background Falls are common in the hospitalisation period, following hospital discharge and in the long-term for people who have had a stroke. It has been reported that up to 65% of people with stroke fall at least once during their hospitalisation [1-3] and between 46-73% fall at least once within six months of returning home from hospital [4-7]. However, falls are also a problem for people with stroke in the longer term [8, 9]. It has been demonstrated that long-term community-dwelling stroke survivors have twice the risk of falling compared with control subjects [8]. Factors that have been associated with the higher falls risk include reduced functional and physical abilities such as difficulty stooping or kneeling [9] and depressive symptoms [8]. Falls in people with chronic stroke may have a substantial impact on their confidence, mobility, function, and independence. Therefore, identifying possible predisposing factors related to falls risk is important, especially if these factors are modifiable and falls can be prevented. People with chronic stroke may present with a number of stroke related factors that are likely to contribute to their increased risk of falling, including hemiparesis, sensory loss, and perceptual problems. It needs to be remembered that many stroke survivors may have a range of falls risk factors independent of their stroke that have not been previously addressed. Best practice care in the community should involve optimising recovery from stroke related factors, as well as identifying and ensuring optimal management of pre-existing falls risk factors through targeted falls prevention programs. Common falls risk factors that need to be considered include vision impairment; chronic health conditions (e.g. other neurological conditions such as Parkinson’s disease; arthritis); polypharmacy (four or more medications substantially increases falls risk); high risk medications such as psychotropic medications; continence problems; gait and balance impairment; somatosensory loss; and cognitive impairment [10]. In particular, having had a fall in the preceding 12 months is a strong predictor for having future falls.
Minimising risk of falls screening assessment Have you fallen in the last 12 months? Yes No
If yes, how many?
Injuries sustained:
Circumstances of falls:
If no falls, do you worry about falling? Yes No
Comments:
Specific ‘Flags’:
- Falls within the last 12 months - Fear of falling limiting function
Falls Risk Assessment
A falls risk assessment should be completed in the community when a stroke survivor is identified as being a potential falls risk through the screening process.
The aim of the falls risk assessment is to identify risk factors contributing to risk of falls, both stroke related, as well as those which the person had prior to their stroke
Examples of comprehensive falls risk assessment tools for use for people in the community setting include the FROP-Com [11]
1 and the Screening Assessment for Falls Evaluation (SAFE).
2
1 The FROP-Com assessment tool and guidelines for use are available from
http://www.health.vic.gov.au/agedcare/maintaining/falls/providers/home/frop.htm; and from Best Practice Guidelines for Australian Community Care (Preventing falls and harm from falls in older people, 2009), produced
12
Interventions Research evidence shows that a range of single and multi-factorial interventions can be effective in reducing falls among older people, including those with high levels of falls risk [12]. Few randomised controlled trials have investigated the effectiveness of these interventions specifically in the chronic stroke population [13]. Successful interventions in older people in the community have included:
Exercise (group exercise, home exercise, or tai chi). Importantly, programs need to include individually tailored exercises that challenge balance and are of an intensive nature [14]. A recent systematic review found that the minimally effective dose for balance training was 50 hours, and therefore utilising supervised group exercise and/or home exercise programs may be beneficial [14]. Walking programs should only be included as part of the exercise program if it occurs in addition to the specific balance training outlined [14];
Management of identified visual impairment- eg. Referral for Cataract surgery and Vitamin D supplementation for people with vitamin D insufficiency;
Home modifications, particularly for people at increased falls risk; adequate follow-up to ensure uptake of falls prevention related recommendations;
Multifactorial approaches, utilising two or more interventions, often based on falls risk assessment;
In addition, to minimise the risk of falls in people with chronic stroke, the following actions should be considered:
Aim to address any identified pre-stroke falls risk factors (e.g. poor vision, polypharmacy, incontinence) as well as any stroke-related falls risk factors (e.g. inattention or neglect, visual field deficits);
Referral to occupational therapy and physiotherapy who may address the following: o Ensure a safe home environment, and that the client understands the rationale for
recommended home modifications to minimise hazards, promote independence and maximise update of recommended strategies;
o Discuss safer options for the person to undertake desired activities; o Provide follow-up to maximise uptake of recommended falls prevention strategies; o Prescribe individually tailored exercises that challenge balance and are of an
appropriate dosage. References 1. Davenport R, Dennis M, Wellwood I, CP. W: Complications after acute stroke. Stroke, 1996.
27(3): p. 415-420. 2. Nyberg L, Gustafson Y: Patient falls in stroke rehabilitation. A challenge to rehabilitation
strategies. Stroke, 1995. 26(5): p. 838-842. 3. Teasell R, McRae M, Foley N, Bhardwaj A: The incidence and consequences of falls in stroke
patients during inpatient rehabilitation: factors associated with high risk. Arch Phys Med Rehabil, 2002. 83(3): p. 329-333.
4. Forster A, Young J: Incidence and consequences of falls due to stroke: A systematic inquiry. British Medical Journal, 1995. 311: p. 83-86.
5. Kerse N, Parag V, Feigin V, McNaughton H, Hackett M, Bennett D, Anderson C, Auckland Regional Community Stroke (ARCOS) Study Group: Falls after stroke: results from the Auckland Regional Community Stroke (ARCOS) Study, 2002 to 2003. Stroke, 2008. 39(6): p. 1890-1893.
6. Mackintosh S, Hill K, Dodd K, Goldie P, Culham E: Balance score and a history of falls in hospital predict recurrent falls in the six months following stroke rehabilitation. Archives of Physical Medicine and Rehabilitation, 2006. 87: p. 1583-1589.
7. Mackintosh S, Hill K, Dodd K, Goldie P, Culham E: Falls and injury prevention should be part of every stroke rehabilitation plan. Clinical Rehabilitation, 2005. 19: p. 441-451.
by the Australian Commission on Safety and Quality in health care - http://www.health.gov.au/internet/safety/publishing.nsf/content/com-pubs_FallsGuidelines/$File/30456-Guidelines-COMM.PDF (p 135). 2 The SAFE tool is available from the Victorian Government Department of Health website:
http://www.health.vic.gov.au/agedcare/maintaining/falls/providers/home/safe.htm

13
8. Jørgensen L, Engstad T, Jacobsen B: Higher incidence of falls in long-term stroke survivors than in population controls: depressive symptoms predict falls after stroke. Stroke, 2002. 33(2): p. 542-547.
9. Mackintosh S, Goldie P, Hill K: Falls incidence and factors associated with falling in older, community-dwelling, chronic stroke survivors (> 1 year after stroke) and matched controls. Ageing: Clinical and Experimental Research, 2005. 17: p. 74-81.
10. Lord S, Sherrington C, Menz H, Close J: Falls in Older People: Risk Factors and Strategies for Prevention, 2nd edn: Cambridge University Press, United Kingdom; 2007.
11. Russell M, Hill K, Blackberry I, Gurrin L, Dharmage S, Day L: Development of the falls risk for older people in the community (FROP-Com) screening tool. Age and Ageing, 2009. 38(1): p. 40-46.
12. Gillespie L, Robertson M, Gillespie W, Lamb S, Gates S, Cumming R, Rowe B: Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews. Issue 2. Art. No.: CD007146. DOI: 10.1002/14651858.CD007146.pub2. 2009.
13. Batchelor F, Hill K, Mackintosh S, Said C: What works in falls prevention after stroke? A systematic review and meta-analysis. Stroke, 2010. 41: p. 1715-1722.
14. Sherrington C, Whitney J, Lord S, Herbert R, Cumming R, Close J: Effective exercise for the prevention of falls: a systematic review and meta-analysis. J Am Geriatr Soc, 2008. 56(12): p. 2234-2243.

14
Domain 4: Communication Background Communication allows people to engage in social relationships, express personal attitudes and maintain identity, and thus the ability to communicate and participate in conversation contributes to psychological wellbeing [1]. Communication and cognitive ability exerts a direct influence on depression and positive affect and the presence of aphasia increases the risk of major depression in stroke patients [2]. The loss of autonomy and a lack of communicative access in the community can impact on emotional health and quality of life for people with aphasia [3]. As a result, people with aphasia and other acquired communication disorders are at risk of increased social isolation and reduced participation. Studies have reported that people with chronic aphasia have significantly fewer social contacts and social activities than their peers [4], that aphasia can restrict the number of everyday activities undertaken, the number of communication partners engaged with and the number of social situations experienced [5], and that aphasia is a barrier to full participation in life [6]. There has been an emphasis on social approaches to the management of aphasia, particularly targeting functional communication and addressing life participation [7] . Relationships with family and friends and leisure activities are important for positive wellbeing and therefore, rehabilitation should consider conversation partner training programs to maintain relationships and encouraging and supporting people with communication difficulties in leisure activities of their choice [4] . Communication groups [6] and conversation partner training [1] should be considered for people with post stroke communication difficulties, as well as access to and training to use both high and low tech communication aids.
Communication screening assessment Do you have difficulty communicating with other people? (understanding what is said to you; speaking to others) Does your communication difficulty affect your ability to do the things you want to do?
Yes Yes
No No
Does the patient have difficulty with communication? If yes, type:
Yes No
Has this difficulty with communication changed since your discharge from hospital? (ie improved/ the same/ worse) If improved – consider speech referral to consolidate gains If worse – consider speech referral to investigate deterioration
Yes No
Is your communication ability impacting on your ability to participate in activities? Yes No
Are you able to communicate with? Examples of Other: Shop owner / a stranger / on the telephone / order a meal, etc.
Your partner/carer
Family
Friends
Other ______________
Do you use any communication strategies / aids? If yes, discuss type of strategy / aid and compliance:
Yes No
Guidelines for interpreting screening assessments These questions aim to gain some information about whether the patient has an acquired communication impairment and whether this is impacting on their ability to participate. Pre-existing communication difficulties (e.g. low literacy, impaired vision, hearing loss) have also been included as presence of pre-existing communication difficulties or impairments needs to be considered when making referrals.
Interventions If the patient has an acquired communication impairment (e.g. dysphasia, dysarthria, dyspraxia) and it is impacting on their ability to participate in their community, consider-

15
Referral to a communication/aphasia/stroke support group
Referral to a leisure/social group e.g. art program, exercise group
Referral to a speech pathologist who may address the following o Conversation partner training for carer, family, friends and other relevant people o Development of augmentative and alternative communication aids/strategies o Education regarding communication impairment and counselling o Return to previous activities or developing new interests in the context of their
communication impairment
Referral to a social worker for counselling/support (patient, carer or both)
These interventions aim to address participation and re-engagement in the context of a communication impairment. Additional Resources
National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia. Website www.strokefoundation.com.au/clinical-guidelines
National Stroke Foundation ‘Communication after stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au
Recommended reading Kagan, A. (1998). Supported conversation for adults with aphasia: methods and resources for training conversation partners. Aphasiology, 12(9), 816-830 LPAA Project Group (2001). Life Participation Approach to Aphasia. In R. Chapey (Ed.). Language Intervention Strategies in Aphasia and related Neurogenic Communication Disorders. Philadelphia: Lippincott, Williams & Wilkins Shadden, B. & Agan, J. (2004). Renegotiation of Identity: The Social Context of Aphasia Support Groups. Topics in Language Disorders, 24(3), 174-186 Threats, T. (2007). Access for persons with neurogenic communication disorders: Influences of Personal and Environmental Factors of the ICF. Aphasiology, 21(1), 67-80 References 1. Kagan, A. and G. Gailey, Functional is not enough: training conversation partners for aphasic
adults, in Aphasia treatment: World Perspectives, A. Holland and M. Forbes, Editors. 1993, Singular Publishing Group: San Diego, CA.
2. Kauhanen, M., et al., Poststroke depression correlates with cognitive impairment and neurological deficits. Stroke, 1999. 30: p. 1875-1880.
3. Cruice, M., et al., Finding a focus for quality of life with aphasia: social and emotional health and psychological well-being. Aphasiology, 2003. 17(333-354).
4. Cruice, M., L. Worrall, and L. Hickson, Quantifying aphasic people’s social lives in the context of non-aphasic peers. Aphasiology, 2006. 20: p. 1210-1225.
5. Davidson, B., L. Worrall, and L. Hickson, Identifying the communication activities of older people with aphasia: evidence from naturalistic observation. Aphasiology, 2003. 17: p. 243-264.
6. Ross, A., et al., Evaluation of communication, life participation and psychological well-being in chronic aphasia: the influence of group intervention. Aphasiology, 2006. 20: p. 427-448.
7. LPAA Project Group, Life Participation Approach to Aphasia, in Language intervention strategies in aphasia and related neurogenic communication disorders, R. Chapey, Editor. 2001, Lippincott, Williams & Wilkins: Philadelphia.

16
Domain 5: Cognition
Background Problems with cognitive function are common post-stroke and occur in approximately a third of the people who have had a stroke [1]. Continued management of post-stroke cognitive issues is advocated into the chronic phase of stroke, as gains may continue to be achieved even years after stroke onset [2, 3].
A top-down approach is preferred with people with cognitive problems following stroke. A top down approach refers to starting with looking at the client as a whole person with their own unique needs, wants, life experiences, roles, values, opinions, and interests prior to identifying and honing in on the impairment [4].
Problems with cognition post-stroke may have a devastating effect on a person’s independence and ability to participate in self-care and household tasks, such as cooking, cleaning, home maintenance and gardening. Cognitive problems may also impact on a person’s ability to catch public transport, shop, drive, manage their own finances, resume work roles, use a computer, attend appointments and organise one’s own schedule. Other people, such as a person’s partner or carer, may have resumed some of the individual’s roles that require complex thinking skills, which may lead to decreased confidence for the stroke survivor.
The main cognitive deficits evident post-stroke include issues with:
Memory - for example, people with memory problems may have difficulty remembering names or remembering tasks that they need to do.
Attention and concentration – for example, problems with attention and concentration may cause difficulty with tasks such as cooking, driving and computer use.
Executive function- for example, financial management, organising an overseas holiday, writing reports and purchasing large household items may be difficult if problems exist with executive function.
Spatial awareness / neglect – for example, locating items in a cupboard, driving, shopping and reading the newspaper are tasks that may be problematic if spatial neglect is present.
Apraxia – for example, tasks that may be difficult for an individual with apraxia include grooming tasks such as cutting one’s own nails and the use of computers or mobile phone devices.
Agnosia – for example, the individual may mistake a teapot for a kettle, a dishwasher for a fridge or different tool items in a shed.
Visual perceptual deficits include:
Acuity (usually as part of aging/changes in blood pressure but need consideration post stroke)
Fields (eg hemianopias, quadrantanopias)
Oculomotor (eg diplopia)
Visual attention/scanning
Pattern recognition/visual memory
Visual deficits may combine with the cognitive and perceptual deficits outlined above and result in disorders of body scheme, body image and spatial relations such as visuo-spatial neglect. Perceptual deficits may exist independently of visual deficits.
Cognitive screening assessment It is important to gather a clear history of the patient’s pre-stroke and current cognitive status via a patient / family / carer interview.
History of cognitive impairment: Obtain information from medical records, the patient, and family / friends / carers regarding the patient’s history of cognitive impairment, including:
Cognitive history prior to stroke, including any evidence of premorbid cognitive decline (such as dementia)
Cognitive status at discharge from inpatient hospital admission (acute and/or rehabilitation)

17
Cognitive status at discharge from sub-acute rehabilitation services and management strategies utilised (such as Community Rehabilitation Centre, Home rehabilitation services)
Education level and any cultural / language implications
Further alterations to cognitive function since stroke
Establish current cognitive status: In chronic stroke, the therapist should ideally initially assess cognition by observing the person’s participation of a familiar task. Standardised cognitive assessments that can be used in task observation include the Assessment of Motor and Process Skills (AMPS) [7] and the Perceive, Recall, Plan and Perform Process (PPRP) [8]. These tests require the therapist to undergo specific formal training to conduct these tests. Tests that do not require formal training are the Structured Observational Test of Function (SOTOF) [9] and the Executive Function Performance Test [10]. Non-functional based cognitive assessments that may supplement an occupational performance based assessment include the Cognistat [11]. The Occupational Therapy Adult Perceptual Screening Test (OT-APST) [12], the Motor-Free Visual Perception Test (MPVT), the Developmental Test of Visual Perception-A (DVPT), and the Test of Visual Perceptual Skills (TVPS) are examples of screening tools that can be used to assess visual perception [13]. Other validated and reliable screening tools are also available [14,15]. It may be necessary to use several screening tools, as there is no universal, test that covers the spectrum of possible cognitive or perceptual deficits. However, it is important to note that many tests of cognition are inappropriate for patients with significant communication disorders [3]. Specific ‘Flags’:
- Patient, family/friend, or carer reports of decline in cognitive function
- Safety concerns arising due to cognitive impairments
- Evidence of specific deficits arising from performance on screening tools
Interventions Cognitive rehabilitation aims to increase the person’s participation in daily tasks that they need or want to do. Strategies (both cognitive and behavioural) and task practice may be used to assist the recovery process, and has been defined as a ‘systematic, functionally oriented service of therapeutic activities that is based on assessment and understanding of the patient’s brain-behavioural deficits’ [16]. The purpose of therapy is to enhance recovery, establish constructive compensatory strategies, and to educate patients and carers about the consequences of cognitive deficits [3]. Overall, there is inconclusive evidence to date regarding the merits of a particular treatment technique for any specific cognitive disorder [3]. However, there is consensus across the research literature which recommends that people who display cognitive deficits post-stroke should continue to be engaged in stroke rehabilitation programs [3, 17, 18]. Interventions usually involve the adoption of retraining and/or compensatory strategies. The Occupational Therapist’s role with people with cognitive difficulties post-stroke is to provide opportunities for participation in the tasks that the person needs and wants to do, promoting resumption of lost roles or encouraging the individual to take on new roles [19]. Providing opportunities to participate in tasks in familiar, real-life environments is very important with people with cognitive problems as the challenges of unfamiliar environments may not give the therapist a true understanding of the patient’s cognitive abilities [20]. Observation of an individual performing hot drink preparation in their own kitchen is preferable for example, than observing this in a community centre’s kitchen. If participation in shopping is a goal it is preferable to go shopping with the person to the shops they would normally go to or would like to go to. Practising catching public transport is best done following the routes that the person will be using. Practice, repetition and opportunities to participate in real world contexts and environments are essential components of a cognitive rehabilitation program post-stroke [21]. Working on increasing the person’s confidence by grading tasks is essential. Management options include:
Medical evaluation (consider Specialist Rehabilitation, Geriatric or Psychiatric assessment), including a medication review
Occupational Therapy and Speech Pathology for Cognitive and Perceptual rehabilitation – with comprehensive assessment and development of specific treatment goals
Neuropsychology for further assessment and recommendations

18
Cognitive Dementia and Memory Service (CDAMS) referral
For visual perceptual deficits, consider referral to opticians, orthoptists, opthamologists, Vision Australia
May require a Community Mobility referral if community ambulant (such as the Acquired Brain Injury Mobility Service run by Guide Dogs Victoria)
Consider a Social Work referral for patient/family counselling or referral for support services.
Team based approach for education and support for patient, family, and carers and recommendation of appropriate strategies.
Use of technological devices as deemed appropriate for the individual. For example: o Mobile phones and computers can be used to assist with organisation, prioritisation of
tasks and schedules o Consider use of computer programs accessed on iPhones or laptops which prompt /
cue a person through the steps of a complex task o Environmental control units can be controlled by laptops, iPhones or personal digitial
assistants to operate appliances [22] Additional Resources
National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia. Website www.strokefoundation.com.au/clinical-guidelines
National Stroke Foundation ‘Thinking and Perception after stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au
ComTEC. An information and advisory service with expertise in assistive technology for communication, computer access and environmental control. Free call: 1300 885 886 (Vic only). http://www.yooralla.com.au/comtec.php
Technical Solutions Australia. Electronic devices for people with a disability. Phone: (03) 9737 9000. http://www.tecsol.com.au/
References 1. Doorhein, K. and E. De Haan, Cognitive training for memory deficits in stroke patients.
Neuropsychological Rehabilitation, 1998. 8(4): p. 393-400. 2. Sohlberg, M., et al., Evidence based practice for the use of external aids as a memory
compensation technique. Journal of Medical Speech-Language Pathology, 2007. 15: p. xv. 3. Miller, E., et al., Comprehensive overview of nursing and interdisciplinary rehabilitation care of
the stroke patient. A scientific statement from the American Heart Association, 2010. 41: p. 2402-2448.
4. Duggan, R., Reflection as a means to foster client centred practice. Canadian journal of Occupational Therapy, 2005. 72(2): p. 103.
5. Royall, D., et al., Executive control function: A review of its promise and challenges for clinical research. A report from the committee on research of the American Neuropsychiatric Association. Journal of Neuropsychiatry and Clinical Neurosciences, 2002. 14(377-405).
6. Heilman, K., R. Watson, and E. Valenstein, Neglect and related disorders, in Clinical Neuropsychology, K. Heilman and E. Valenstein, Editors. 1993, Oxford University Press: New York. p. 243-294.
7. Assessment of Motor and Process Skills: http://www.ampsintl.com/AMPS/ 8. Chapparo, C. & Ranka, J., Development of an information processing task analysis to identify
errors in self-maintenance performance of brain injured clients: Final Category B Grants Research Report. 1992. Lidcombe, NSW, Australia: University of Sydney, Faculty of Health Sciences.
9. Laver, A.J., and Powell, G.E., The Structured Observational Test of Function (SOTOF). 1995. NFER-Nelson, Windsor.
10. Baum, C.M., Connor, L.T., Morrison, T., Hahn, M., Dromerick, A.W., and Edwards, D.F., Reliability, validity, and clinical utility of the executive function performace test: a measure of executive function in a sample of people with stroke. The American Journal of Occupational Therapy, 2008. 62(4): p. 446-455.
11. Cognistat Cognitive Assessment: www.cognistat.com 12. Cooke, D., McKenna, K., and Fleming, J., Development of a standardised occupational
therapy screening tool for visual perception in adults. Scand J Occup Ther, 2005. 12: p. 59-71 13. Brown, T., Sutton, E., Burgess, D., Elliott, S., Bourne, R., Wigg, S., Glass, S., and Lalor, A.,
The reliability of three visual perception tests used to assess adults. Perceptual and Motor Skills, 2010. 111(1): p. 45-59.

19
14. Douglas, A., Liu, L., Warren, S., and Hopper, T., Cognitive Assessments for older adults: which ones are used and why. Canadian Journal of Occupational Therapy, 2007. 74(5): p. 370-382.
15. Dunn, W., Measurement issues and practices. In Law, M.C., Baum C.M., & Dunn, W., Measuring Occupational Performance; Supporting best practice in Occupational Therapy, 2005. p. 21-32.Thorofare, NJ: Slack.
16. Cicerone, K., et al., Evidence-based cognitive rehabilitation: Updated review of the literature from 1998 through 2002. Archives of Physical Medicine and Rehabilitation, 2005. 86: p. 1681-1692.
17. Bowen, A. and N. Lincoln, Cognitive rehabilitation for spatial neglect following stroke. Cochrane Database of Systematic Reviews, 2007. Issue 3. Art. No.: CD002293. DOI: 10.1002/14651858.CD002293.pub2.
18. West, C., et al., Interventions for motor apraxia following stroke. Cochrane Database of Systematic Reviews, 2008. Issue 1. Art. No.: CD004132. DOI: 10.1002/14651858.CD004132.pub2.
19. Doig, E., Fleming, J., and Kuipers, P., Achieving optimal outcomes in CBR following ABI: A qualitative investigation of therapist’s perspectives. British Journal of Occupational Therapy, 2008. 71: p. 360-370.
20. Guidetti, S., Asaba, E., and Tham, K., The lived experience of recapturing self care. American Journal of Occupational Therapy, 2007. 61(3): p. 303-310.
21. National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia.
22. das Nair, R. and N. Lincoln, Cognitive rehabilitation for memory deficits following stroke. Cochrane Database of Systematic Reviews 2007. Issue 3. Art. No.: CD002293. DOI: 10.1002/14651858.CD002293.pub.

20
Domain 6: Mood Status / Depression Background Post-stroke depression (PSD) Depressive symptoms are common post-stroke, and will be experienced by approximately one-third of people who have had a stroke [1]. Depression is characterised by persistent low mood (of a duration greater than two weeks) with additional symptoms of: loss of energy; alterations to appetite or weight; suicidal ideation; disturbed sleep; sense of worthlessness; anhedonia (diminished interest or pleasure in usual activities); psychomotor retardation and/or agitation [2]. Effect of PSD on outcomes Post-stroke depression can affect the recovery process, including the person’s ability to participate in rehabilitation, which can potentially limit their long-term outcomes [3,4]. Negative outcomes have been associated with the presence of PSD, such as dependence in activities of daily living [5] and reduced perception of quality of life [6]. PSD has also been associated with an increased risk of mortality [7]. Restrictions in participation have also been associated with PSD [8,9]. Participation, in this context, relates to a person’s ability to engage in life situations [10]. This concept also encompasses aspects of personal and social re-integration, and a return to valued and meaningful activities [11] Factors associated with PSD risk The main factors that have been linked to PSD are physical disability, stroke severity, and cognitive impairment [12]. Several other factors have also been correlated with a raised risk for PSD, such as, female gender, social isolation, presence of dysphasia, past history of depression, and level of activity limitations [1, 13, 14]. Other aspects that may contribute to a person’s emotional health post-stroke are the sense of dependence upon others and the uncertainty about the recovery process [15]. However, overall the body of literature is equivocal about the level of contribution that the above factors play in the presence and development of PSD. PSD is often under-recognised and under-treated, and there is a need to establish a more consistent approach to assessment, diagnosis, and management [3]. It should be considered that all patients who have had a stroke are at risk of developing or exacerbating depressive symptoms, and it is recommended that a validated tool be used to screen and monitor post-stroke patients for signs of depression in the clinical setting [4]. Depressive symptoms can vary in severity (from mild to severe). The greatest risk period for development of depressive symptoms appears to be within the first two years post-stroke, and notably during the transition from structured rehabilitation programs [7, 16]. Nevertheless, the development of PSD may occur at any time, in any setting, and follow a variable course.
Depression screening assessment History of depression:
Do you have a history of depression? Yes No
If yes, the depression was diagnosed by: General Medical Practitioner Psychiatrist Psychologist Other_________________________________ Not formally diagnosed / Patient self-report Date diagnosed:___________________________
Treatment / Management strategies that have been used previously: (e.g. medications, cognitive behaviour therapy, interpersonal therapy or counselling, physical exercise programs)
Contact details of practitioner Mental Health Practitioner:
Date of last review appointment:
21
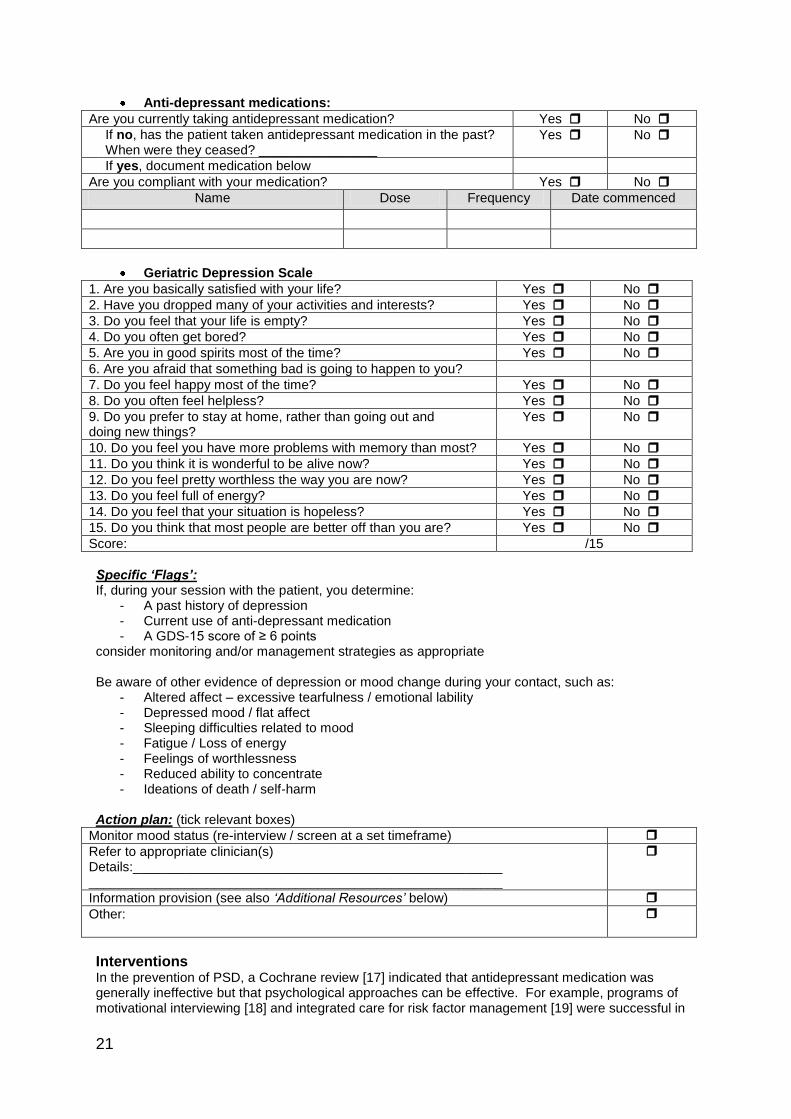
Anti-depressant medications:
Are you currently taking antidepressant medication? Yes No
If no, has the patient taken antidepressant medication in the past? When were they ceased? ________________
Yes No
If yes, document medication below
Are you compliant with your medication? Yes No
Name Dose Frequency Date commenced
Geriatric Depression Scale
1. Are you basically satisfied with your life? Yes No
2. Have you dropped many of your activities and interests? Yes No
3. Do you feel that your life is empty? Yes No
4. Do you often get bored? Yes No
5. Are you in good spirits most of the time? Yes No
6. Are you afraid that something bad is going to happen to you?
7. Do you feel happy most of the time? Yes No
8. Do you often feel helpless? Yes No
9. Do you prefer to stay at home, rather than going out and doing new things?
Yes No
10. Do you feel you have more problems with memory than most? Yes No
11. Do you think it is wonderful to be alive now? Yes No
12. Do you feel pretty worthless the way you are now? Yes No
13. Do you feel full of energy? Yes No
14. Do you feel that your situation is hopeless? Yes No
15. Do you think that most people are better off than you are? Yes No
Score: /15
Specific ‘Flags’: If, during your session with the patient, you determine:
- A past history of depression - Current use of anti-depressant medication - A GDS-15 score of ≥ 6 points
consider monitoring and/or management strategies as appropriate Be aware of other evidence of depression or mood change during your contact, such as:
- Altered affect – excessive tearfulness / emotional lability - Depressed mood / flat affect - Sleeping difficulties related to mood - Fatigue / Loss of energy - Feelings of worthlessness - Reduced ability to concentrate - Ideations of death / self-harm
Action plan: (tick relevant boxes)
Monitor mood status (re-interview / screen at a set timeframe)
Refer to appropriate clinician(s) Details:__________________________________________________ ________________________________________________________
Information provision (see also ‘Additional Resources’ below)
Other:
Interventions In the prevention of PSD, a Cochrane review [17] indicated that antidepressant medication was generally ineffective but that psychological approaches can be effective. For example, programs of motivational interviewing [18] and integrated care for risk factor management [19] were successful in

22
reducing rates of PSD. In terms of treating PSD, another Cochrane review [20] found that psychological approaches were ineffective but that antidepressant treatment was effective in reducing depressive symptoms (while also carrying greater risk of adverse events). Recent studies have shown that programs based on initiating and monitoring antidepressant use [21] and adding a behavioural intervention to medication use [22] have been successful in mitigating PSD. There is evidence that exercise may have a positive effect on PSD in the sub-acute phase of stroke [23, 24]. Depression is generally a multifaceted issue, and should be managed in such a way that addresses the nature of the presentation. Those patients who have been identified by the above screening process as having evidence of depression should have:
Referral to appropriate clinicians who are able to accurately diagnose depression, determine the extent of the symptoms, and manage the condition. Such clinicians may include: Psychiatrist, Psychologist, General Medical Practitioner, Rehabilitation Medicine Specialist and community mental health teams. Antidepressant treatment should be monitored and should continue for a minimum of 6 months [25]
Identification and management of known risk factors.
Information provision – specific to issues that are causing concern.
A process for ongoing monitoring of mood status
Adequate support given to caregivers Additional Resources
Investigate your local health network mental health resources (create a resource file containing information such as: local medical and allied health professionals who specialise in mental health)
National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia. Website www.strokefoundation.com.au/clinical-guidelines
National Stroke Foundation ‘Depression after Stroke’ Fact Sheet Freecall: 1800 787 653 Website: www.strokefoundation.com.au Also refer to NSF Clinical Guidelines for Stroke Management 2010.
Beyondblue Guides for patients / carers / health professionals. Available is also a search tool for local mental health professionals. Phone: 1300 224 636 Website: www.beyondblue.org.au (downloadable resources. DVD available: http://www.beyondblue.org.au/index.aspx?link_id=59.1292).
Carers Victoria Advice, Information, and workshops Freecall: 1800 242 638 Website: www.carersvic.org.au
Lifeline Counselling, information, and referral. Phone: 13 11 14. [*World Health Organisation: http//www.who.int/mental_health/management/depression/definition/en] References 1. Hackett, M.L., et al., Frequency of depression after stroke. Stroke, 2005. 36: p. 1330-1340. 2. American Psychiatric Association. Diagnosis and statistical manual of mental disorders. 4
th
Edition, text revision. Washington DC. 2000. American Psychiatric Association. 3. Turner-Stokes, L. and N. Hassan, Depression after stroke: a review of the evidence base to
inform the development of an integrated pathway. Part 1: Diagnosis, frequency and impact. Clinical Rehabilitation, 2002. 16: p. 231-247.
4. Lindsay, P., et al., Canadian best practice recommendations for stroke care. Canadian Medical Association Journal, 2008. 179(12): p. S1-S25.
5. Ramasubbu, R., et al., Functional impairment associated with acute poststroke depression: The stroke data bank study. The Journal of Neuropsychiatry and Clinical Neurosciences, 1998. 10: p. 26-33.
6. Sturm, J.W., et al., Quality of life after stroke: the North East Melbourne Stroke Incidence Study (NEMESIS). Stroke, 2004. 35: p. 2340-2345.
7. Hosking, S.G., N.V. Marsh, and P.J. Friedman, Poststroke depression: prevalence, course and associated factors. Neuropsychology Review, 1996. 6(3): p. 107-132.
8. Clarke, P.J., et al., Handicap in stroke survivors. Disability and Rehabilitation, 1999. 21(3): p. 116-123.

23
9. Gall, S.L., et al., Handicap 5 years after stroke in the North East Melbourne Stroke Incidence Study. Cerebrovascular Diseases, 2009. 27: p. 123-130.
10. World Health Organisation, International Classification of Functioning, Disability and Health: ICF. 2001, Geneva: World Health Organisation.
11. Siegert, R.J. and W.J. Taylor, Theoretical aspects of goal-setting and motivation in rehabilitation. Disability and Rehabilitation, 2004. 26(1): p. 1-8.
12. Hackett, M. and C. Anderson, Predictors of depression after stroke. A systematic review of observational studies. Stroke, 2005. 36: p. 2296-2301.
13. Ouimet, M.A., F. Primeau, and M.G. Cole, Psychosocial factors in poststroke depression: A systematic review. Canadian Journal of Psychiatry, 2001. 46: p. 819-828.
14. Astrom, M., R. Adolfsson, and K. Asplund, Major depression in stroke patients: a 3-year longitudinal study. Stroke, 1993. 24(976-982).
15. Flick, C.L., Stroke Rehabilitation. 4. Stroke outcome and psychosocial consequences. Archives of Physical Medicine and Rehabilitation, 1999. 80: p. S21-S26.
16. Parikh, R.M., et al., A two year longitudinal study of poststroke mood disorders: Prognostic factors related to one and two year outcome. International Journal of Psychiatry in Medicine, 1988. 18: p. 45-56.
17. Hackett, M.L., et al., Interventions for preventing depression after stroke. Cochrane Database of Systematic Reviews, 2008. Issue 3. Art. No.: CD003689. DOI: 10.1002/14651858.CD003689.pub3.
18. Watkins, C., et al., Motivational interviewing early after acute stroke. Stroke, 2007. 38: p. 1004-1009.
19. Joubert, J., et al., The positive effect of integrated care on depressive symptoms in stroke survivors. Cerebrovascular Diseases, 2008. 26(2): p. 199-205.
20. Hackett, M.L., et al., Interventions for treating depression after stroke. Cochrane Database of Systematic Reviews, 2008. Issue 4. Art.No.:CD003437.DOI:10.1002/14651858.CD003437.pub3.
21. Williams, L.S., et al., Care management of poststroke depression: A randomised control trial. Stroke, 2007. 38: p. 998-1003.
22. Mitchell, P., et al., Brief psychosocial-behavioural intervention with anti-depressant reduces post-stroke depression significantly more than usual care with antidepressant. Living well with stroke: Randomized controlled trial. Stroke, 2009. 40: p. 3073-3078.
23. Graven, C., et al., Are rehabilitation and/or care-co-ordination interventions delivered in the community effective in reducing depression, facilitating participation and improving quality of life after stroke? Disability and Rehabilitation, 2011: p. 1-20.
24. Lai, S., et al., Therapeutic exercise and depressive symptoms after stroke. Journal of American Geriatrics Society, 2006. 54: p. 240-247.
25. Turner-Stokes L, Macwalter R. Use of antidepressant medication following acquired brain injury: concise guidance. Clin Med 2005. 5: p. 268-274.

24
Domain 7: Health-Related Quality of life
Background Quality of life (QoL) is a complex concept that encompasses many dimensions of an individual’s existence. Although there are many ways to categorise QoL, these dimensions can be generally classified into: social relationships, socio-economic status, global issues, personal characteristics, and health. A widely accepted definition is that ‘QoL is an individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns’ [1 p1405]. In line with this definition, QoL is a perception that can only be reasonably judged by a particular individual [2]. Over the past few decades, there has been an increased use of the measurement of QoL as an outcome for health interventions, and its utility in the clinical setting is now becoming generally accepted [2]. In the healthcare forum, the type of QoL measures that are typically adopted are those that reflect health-related QoL (HRQoL). The concept of HRQoL tries to capture how an individual views the impact of their health status on their QoL, especially in relationship to physical, cognitive, and emotional factors. People who have had a stroke tend to report a reduced HRQoL, however, there is an enormous variation in QoL estimates present in the literature [3-5]. The improvement of QoL is often proposed as a global goal of rehabilitation services, however undue focus on only an individual’s activity limitations may limit the overall achievement of this goal [6]. Presence of depressed mood, low functional activity status, and lack of social support are predictors of HRQoL post-stroke, however, it is important to note that a poor perception of HRQoL can also be evident despite overall good functional recovery [3, 7, 8]. Improvements in HRQoL may be elicited via interventions that address depressed mood and participation status. Resumption of previously valued activities may have an impact on an individual’s sense of life quality [3, 9]. A systematic review, which explored the efficacy of post-stroke community-based interventions (undertaken by nursing or allied health professionals) on perception of QoL, indicated that there was evidence to support some types of rehabilitation interventions that generally targeted patient’s valued activities conducted in the patient’s community context [10]. Measures of HRQoL are now frequently used in relation to the evaluation of healthcare resource allocation.
Health-related quality of life screening assessment To introduce the patient to the concept of quality of life, a global question is often helpful:
How satisfied are you with your life as a whole?
If the patient reports a diminished quality of life, ask further questions that examine the factors that contribute to the patient’s perception of their quality of life. Explore such concepts as [11, 12]:
- Health - Personal relationships / wider sense of feeling part of a community - Psychological wellbeing - Sense of safety - Faith, spirituality, religion - Standard of living - Level of achievement in life - Future concerns / future security

25
Are there goals that you could pursue which would influence your quality of life perception?
Use a Health-related Quality of Life (HRQoL) measurement tool (for example, the Assessment of Quality of Life [12,13], Medical Outcomes Study Short Form-36 [14,15]).
Use a measure of global life satisfaction (for example, the Personal Wellbeing Index [16]). Specific ‘Flags’:
- Specific aspects that an individual may identify as having an impact on their quality or satisfaction with their life.
Interventions Management strategies will depend on which factors have been identified during the interview. Referrals to other health professionals may be appropriate, or referrals to other appropriate services and resources. Certain aspects that an individual has identified as affecting their quality of life may, or may not, be modifiable. References 1. The WHOQOL Group, The World Health Organisation Quality of Life Assessment
(WHOQoL): Position paper from the World Health Organisation. Social Science and Medicine, 1995. 41: p. 1403-1409.
2. Schipper, H., Clinch, J., Powell, V. Definitions and conceptual issues. In: Spiler B. Ed, Quality of Life Assessments in Clinical Trials. New York. Raven Press. 1990.
3. Sturm, J.W., et al., Determinants of handicap after stroke: The North East Melbourne Stroke Incidence Study (NEMESIS). Stroke, 2004. 35: p. 715-720.
4. Kelly-Hayes, M. and C. Paige, Assessment and psychological factors in stroke rehabilitation. Neurology, 1995. 45: p. S29-S32.
5. Tengs, T., M. Yu, and E. Luistro, Health-related quality of life after stroke. A comprehensive review. Stroke, 2001. 32: p. 964-972.
6. Secrest, J. and S. Thomas, Continuity and discontinuity: The Quality of life following stroke. Rehabilitation Nursing, 1999. 24(6): p. 240-246.
7. King, R.B., Quality of life after stroke. Stroke, 1996. 27: p. 1467-1472. 8. Carod-Artal, J., et al., Quality of life among stroke survivors evaluated 1 year after stroke:
Experience of a stroke unit. Stroke, 2000. 31: p. 2995-3000. 9. Robinson, J., et al., Resuming previously valued activities post-stroke: who or what helps?
Disability and Rehabilitation, 2009. 31(19): p. 1555-1566. 10. Graven, C., et al., Are rehabilitation and/or care-co-ordination interventions delivered in the
community effective in reducing depression, facilitating participation and improving quality of life after stroke? Disability and Rehabilitation, 2011: p. 1-20.
11. Phillips, D. Quality of Life and the individual. In: Quality of LIfe: Concept, policy and practice. New York. Taylor and Francis. 2006.
12. Hawthorne G, Richardson J, Osborne R: The Assessment of Quality of Life (AQoL) instrument: A psychometric measure of health-related quality of life. Quality of Life Research
1999, 8(3): p. 209-224.
13. Assessment of Quality of Life: http://www.psychiatry.unimelb.edu.au/centres-units/cpro/aqol/use_aqol.html. Permission must be sought prior to use.
14. Ware, J. E., Jr., Snow, K. K., Kosinski, M., & Gandek, B. (1993). SF-36 health survey. Manual and interpretation guide. Boston: The Health institute, New England Medical Center.
15. Medical Outcomes Study Short Form-36: www.sf-36.org 16. International Wellbeing Group (2006). Personal Wellbeing Index. Melbourne: Australian
Centre on Quality of Life, Deakin University (http://www.deakin.edu.au/research/acqol/instruments/wellbeing_index.htm.)
26
Domain 8: Secondary stroke prevention & risk factor management
Background People who have had an ischaemic stroke have an elevated risk of a recurrent stroke event. There are evidence-based recommendations on the prevention of further ischaemic stroke events, with strategies including: the control of risk factors, the use of antithrombotic and antiplatelet agents, and the use of interventional approaches [1]. People who have the presence of intracranial aneurysms also require ongoing monitoring and management [2]. A broad approach to risk factor modification (that incorporates both elements of pharmacological management and lifestyle modification) has been shown to be effective in the reduction of vascular events post-stroke [3]. Adoption of five key prevention strategies, ie. dietary modification, exercise, aspirin, a statin and an antihypertensive agent, may reduce the risk of a further stroke or myocardial infarct over a five year period by 80% [3]. Health professionals who work with people who have had a stroke should be aware of presence of any risk factors, the type of interventions being employed, and the adequacy of their management. In a study by Bravata et al. (2007), more than half the patient cohort (n=2603, who had been discharged after a hospital admission for an acute stroke event) had deceased or required at least one readmission during the first twelve months post-discharge [4]. The most common reasons for readmission were: pneumonia / respiratory illnesses, recurrent stroke, and acute myocardial infarction [4]. General risk factor management Lifestyle modification [5]
Diet modification including reduction of intake of salt and fats, and increased intake of fruit and vegetables.
.Exercise – participating in regular moderate activity lowers blood pressure and helps with weight control.
Alcohol consumption – limiting alcohol consumption to two standard drinks a day
Cigarette Smoking – advice to quit / behavioural therapy / nicotine products / oral smoking cessation medications / Quitline
Obesity – weight reduction program Medication for specific risk factors [5]
Blood pressure lowering medication
Antiplatelet therapy; eg. aspirin for patients with a history of non cardioembolic ischaemic stroke
Diabetes; Monitoring of glycaemic control – diet / exercise / oral hypoglycaemic agents / insulin. Diabetes education for patient and spouse/care-giver
Anticoagulation therapy eg. warfarin for cardiogenic embolism eg. atrial fibrillation. Regular monitoring of INR is recommended for warfarin
Cholesterol lowering medication eg. statins
Medication review [5]
Secondary stroke prevention medications such as aspirin, warfarin, anti-hypertensive therapy and cholesterol lowering agents are advised lifelong
Interventions to improve adherence,such as education, reminder systems and dose administrative aids should be considered.

27
Post-stroke complications in the chronic phase [5]
Neurological (recurrent stroke, epileptic seizure)
Infection (urinary tract, chest)
Fatigue
Falls
Osteoporosis / bone density loss (especially on hemiplegic side)
Pain (e.g. shoulder, musculoskeletal, spasticity, headache, central post-stroke pain)
Osteoporosis / bone density loss (especially on hemiplegic side)
Spasticity and contractures
Skin integrity An increase risk of post-stroke complications is associated with advancing age and severity of stroke. There is also an association between the presence of post-stroke complications and poor overall outcomes [6].
Secondary stroke prevention and risk factor management screening assessment Identification of risk factors
Do you have any stroke risk factors? (for example, hypertension, diabetes, altered lipid status, smoking, elevated alcohol consumption).
Risk factor Current management
How often do you attend your General Practitioner or Medical Specialist for a specific review of your risk factors, such as the status of your blood pressure, diabetes, and/or cholesterol levels?
How often do you attend your General Practitioner or Medical Specialist for a thorough review of your medications?
Do you have any post-stroke complications? (for example, recurrent stroke, seizures, recurrent infections, pain, osteoporosis)
Post-stroke complications Current management
Specific ‘Flags’
- Presence of risk factors with evidence of sub-optimal management. - Presence of post-stroke complications. - Review of risk factors and medications occurs less often than annually.
Intervention Those patients who have been identified by the above screening process as having sub-optimal risk factor management. Referral to:
General Practitioner – liaise with GP regarding concerns about risk factor management, medications, or other general issues for consideration. Assist to arrange a GP review appointment for the patient if necessary. Advice and support regarding risk factor management, especially modifiable lifestyle risk factors.
Physician liaison / review if concerned (eg. Rehabilitation physician associated with community rehabilitation service)

28
Pharmacy / Royal District Nursing Services – for consideration of safe medicine dispensing (Pharmacy involvement / home-based Nursing services / carer education)
Additional Resources
National Stroke Foundation “Clinical guidelines for stroke management 2010” http://www.strokefoundation.com.au/clinical-guidelines
National Stroke Foundation “Preventing another stroke” and ‘Medication after stroke’ Fact Sheets Freecall: 1800 787 653 Website: www.strokefoundation.com.au
National Stroke Foundation ‘Clinical Guidelines for stroke and TIA management- a guide for general practice’ 2008
The Royal Australian College of General Practitioners – guidelines and factsheets www.racgp.org.au
References 1. Sacco, R., et al., Guidelines for prevention of stroke in patients with ischemic stroke or
transient ischemic attack. Circulation, 2006. 113: p. e409-449. 2. Bederson, J., et al., Recommendations for the management of patients with unruptured
intracranial aneurysms. Stroke, 2000. 31: p. 2742-2750. 3. Hackam, D. and D. Spence, Combining multiple approaches for the secondary prevention of
vascular events after stroke. A quantitative modeling study. Stroke, 2007. 38(6): p. 1881-1885.
4. Bravata, D., et al., Readmission and death after hospitalisation for acute ischaemic stroke: 5 year follow-up in the Medicare population. Stroke, 2007. 38: p. 1899-1904.
5. National Stroke Foundation “Clinical guidelines for stroke management 2010” http://www.strokefoundation.com.au/clinical-guidelines
6. Langhorne, P., et al., Medical complications after stroke: A multicentre study. Stroke, 2000. 31: p. 1223-1229.

29
Domain 9: Carer Support Background Many people who have had a stroke will return to live in the community and require ongoing support from informal carers such as spouses, family members, and social networks. Carers may provide assistance for the person who has had a stroke throughout all phases of rehabilitation and recovery, and in turn require support themselves in order to be able continue their role [1]. There is a general shift in the delivery of rehabilitation services from the inpatient setting to outpatient and home-based services, with also a common resolve to maintain people in the home environment as long as possible and avoid or delay the need for institutionalisation [2]. These shifts in health care delivery have ongoing impacts on informal carers. The need to provide long-term care for the person who has had a stroke can place carers under considerable emotional, financial, and physical stress [3, 4]. Carers may have minimal time to adjust to their new roles, and undergo significant social changes, alterations to self-perception, and changes in family relationships [4]. Also, since the role of caring often takes place within the family setting, the experiences of carers are likely to be dependent on cultural, social, and ethnic differences [5]. Carers report dissatisfaction with the level of support available after the person who has had a stroke has been discharged from hospital [5]. They describe feeling ill-prepared for their role and the resultant lifestyle changes that emerge [6]. There is a considerable body of research investigating the possible impacts of caring for a person who has a stroke [1, 5, 7]:
Increased psychological morbidity, especially elevated levels of depression and anxiety [8]. The presence of elevated stress and depressed mood in carers may impact on the overall rehabilitation process, and also worsen mood status of the person who has had the stroke [8].
Decline in carer health, and higher mortality risk [9, 10].
Increased risk of experiencing carer burden [11] – which may include a sense of lack of freedom and reduced time for self. It is important to note that ‘objective burden’ (such as hours of caregiving), and the level of burden experienced by carers are two different notions and not necessarily always associated [12].
Perception of reduced quality of life
Reduced sense of autonomy and independence [7]
Financial burden and possible alterations to employment status (for both the carer and the person who has had the stroke). Concerns about the future.
Alterations to roles and responsibilities, such as assisting the person who has had a stroke with self-care activities, taking on new domestic chores, and engaging in community tasks.
Experiences of social isolation, reduced time for social activities, diminished social life, alterations to relationships.
Patient factors that have been identified to be related to carer outcomes:
Level of disability (in ADLs) and resultant dependency status
Presence of patient depression
Personality and behavioural changes
Incontinence
Presence of cognitive deficits
The ability of carers to adopt coping strategies may assist in their ability to lessen the negative impacts of their role. Commonly identified coping strategies are: taking one day at a time, accepting and asking for help, obtaining information, receiving reassurance and understanding, and taking time to look after oneself [5]. Information and education should be provided for people who have had a stroke, their families, and their carers. The information should encompass details about stroke, its sequelae, signs and symptoms, the recovery process, resources available, financial entitlements, risk factors and secondary stroke prevention, local services and support networks [13]. Education on such topics should be provided across the continuum of stroke care, specific to the current recovery phase [14]. Information provision alone has minimal effects on carer outcomes [3].

30
It is recommended that carers receive appropriate and targeted training in how to safely assist and manage the person who has had a stroke, and that this training be conducted by the multidisciplinary team prior to discharge from hospital [15]. Review of carer skills should also be conducted into the chronic phase of stroke recovery, especially with regard to manual handling techniques. It is important to gain an overview of the type of activities that the carer is required to engage in their role To date, many interventions aimed at reducing the negative impacts of caring have shown minimal effect [7, 12]. There is a need for a heightened understanding of the relationships between patient and carer characteristics and overall carer outcomes in order to try to determine the most suitable type and timing of interventions [7]. Ongoing research is required to investigate the other factors that may influence carer outcomes, such as alterations to roles and life expectations [7]. The role of caring has different effects and meaning to different people. Positive aspects of caring can emerge, such as strengthening relationships, and developing a sense of fulfilment, pride, and purpose [5, 16].
Carer assessment Name: Relationship to patient:
Co-resides with patient: Yes No
Describe caring role / usual tasks (e.g. provides manual assistance with transfers, prepares main meals, provides transport, emotional support to patient, availability)
Formal support for carer (e.g. allowances, respite arrangements)
Informal support for carer (e.g. family, friends, religious affiliations, clubs). Describe how they assist:
Previous use of services for carers (such as counselling, education sessions, support groups)
Yes No
If ‘Yes’, give details:
Do you feel that you are currently managing at home? (discuss any issues that may be causing stress to the carer – such as: care recipient impairments resulting in cognitive, communication, and physical deficits that increase the stress and burden of caring. Also, inquire about patient personality changes (such as irritability or emotionalism), and changes to the roles within the family and household (such as inequality with tasks and decisions, financial implications, relationship issues)
Outline needs / concerns from the carer’s perspective:
Does the carer require / request other information?
Depression Screening Tool
Geriatric Depression Scale (15 item) If yes, Score: /15 [17]
Yes No
Carer Burden Screening Tool
Zarit Caregiver Burden Scale (22 item) If yes, Score: / 88 [18]
Yes No

31
Flags: - Verbal or non-verbal evidence of reduced carer coping (derived either from patient or carer)
Consider screening for:
carer depression, such as the Geriatric Depression Scale Ref (score of ≥ 6 points is suggestive of low mood status)
carer burden, such as the Zarit Caregiver Burden Scale Ref (Scoring Key: 0 to 20 = little or no burden; 21 to 40 = mild to moderate burden; 41 to 60 = moderate to severe burden; 61 to 88 = severe burden).
presence and causes of carer stress - Change in carer status (such as, change in personnel, time availability or level of assistance
offered, carer becomes unwell)
Interventions Engagement of the carer in the rehabilitation process – including carer involvement in
decision making and treatment planning, and involvement in negotiating choice and control [1, 3, 19]. Allow time for assessment of needs and concerns from the carer’s perspective.
Referral to social work for review of carer psychosocial and support needs [4]. Including: - A review of coping strategies and promotion of a self-management / problem-solving
approach to arising issues. Offer counselling options as appropriate (educational / family / problem-solving) [20]
- Financial aid options for carers. - Respite options - Information provision – specific to the person they are caring for and to their situation, as
well as general information - written material (pamphlets, booklets, fact-sheets), web-based information. Interactive and written format. [5, 20]
- Inform the carer of the availability of local support groups (both stroke support groups and carer support groups)
Intermittent review of techniques and strategies that are used by the carer to assist the person who has had a stroke, especially with regard to manual handling techniques. Provide education and modifications to techniques as required.
Offer ongoing verbal support and encouragement to the carer in their role.
Explore the availability of relevant community programs
Documentation of carer contacts and education in medical records
Additional Resources
Contact with the carer’s General Medical Practitioner to discuss concerns about carer depression, carer burden, or other arising issues.
Carer benefits / Centrelink / New Carer Card www.centrelink.gov.au
Carers Victoria / Carers Australia Level 1, 37 Albert Street Footscray 3011 Ph: 9396 9500 Fax: 9396 9555 Email: [email protected] www.carersaustralia.com.au
Commonwealth Carer Resource Centre Victoria Victorian Carers Services Network Carer Advisory and Counselling Service Ph: 1800 242 636 http://vcsn.infoxchange.net.au
Commonwealth Respite and Carelink Centre Ph: 1800 052 222 www.commcarelink.health.gov.au
National Stroke Foundation Stroke Connect Ph: 1800 787 653 www.strokefoundation.com.au/strokeconnect/
The Stroke Association of Victoria Inc

32
Ph: 9670 1117 Email: [email protected] www.strokeassociation.com.au
National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia. Website www.strokefoundation.com.au/clinical-guidelines
References 1. Miller, E., et al., Comprehensive overview of nursing and interdisciplinary rehabilitation care of
the stroke patient. A scientific statement from the American Heart Association, 2010. 41: p. 2402-2448.
2, Howe, A.L. (2000). Rearranging the compartments: the financing and delivery of care for Australia’s elderly. Health Affairs, 19(3): p. 57-71
3. Duncan, P., et al., Management of adult stroke rehabilitation care: A clinical practice guideline. Stroke, 2005. 36: p. e100-e143.
4. Murray, J., et al., Developing a primary care-based stroke service: A review of the qualitative literature. British Journal of General Practice, 2003. 53: p. 137-142.
5. Greenwood, N., et al., Informal primary carers of stroke survivors living at home - challenges, satisfactions and coping. Disability and Rehabilitation, 2009. 31(5): p. 337-351.
6. McKevitt, C., et al., Qualitative studies of stroke: A systematic review. Stroke, 2004. 35: p. 1499-1505.
7. Greenwood, N., et al., Informal carers of stroke survivors - factors influencing carers: A systematic review of quantitative studies. Disability and Rehabilitation, 2008. 30(18): p. 1329-1349.
8. Han, B. and W.E. Haley, Family caregiving for patients with stroke. Review and analysis. Stroke, 1999. 30: p. 1478-1485.
9. Tooth, L., et al., Caregiver burden, time spent caring and health status in the first twelve months following stroke. Brain injury, 2005. 19: p. 963-974.
10. Schulz, R. and S. Beach, Caregiving as a risk factor for mortality: The Caregiver Helath Effects Study. JAMA, 1999. 282: p. 2215-2219.
11. Anderson, C.S., J. Linto, and E.G. Stewart-Wynne, A population based assessment of the impact and burden of caregiving for long-term stroke survivors. Stroke, 1995. 26: p. 843-849.
12. Visser-Meily, J.M.A., et al., Measures used to assess burden among caregivers of stroke patients: a review. Clinical Rehabilitation, 2004. 18: p. 601-623.
13. Canadian Stroke Network and the Heart and Stroke Foundation of Canada, Canadian Stroke Strategy: Canadian best practice recommendations for stroke care. 2006, Ottawa.
14. Lindsay, P., et al., Canadian best practice recommendations for stroke care. Canadian Medical Association Journal, 2008. 179(12): p. S1-S25.
15. National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne Australia.
16. Morrison, V., Predictors of carer distress following stroke. Reviews in Clinical Gerontology, 1999. 9: p. 265-271.
17. Sheikh JL, Yesavage JA: Geriatric Depression Scale (GDS): Recent evidence and development of a shorter version. In Clinical Gerontology: A guide to assessment and intervention. New York: The Haworth Press; 1986. p. 165-173.
18. Zarit SH, Reever KE, Bach-Peterson J: Relatives of the impaired elderly: correlates to feelings of burden. The Gerontologist, 1980, 20: p. 649-655.
19. Greenwood, N., et al., Loss of autonomy, control, and independence when caring: A qualitative study of informal carers of stroke survivors in the first three months after discharge. Disability and Rehabilitation, 2010. 32(2): p. 125-133.
20. Low, J., S. Payne, and P. Roderick, The impact of stroke on informal carers: a literature review. Social Science and Medicine, 1999. 49: p. 711-725.

33
Domain 10: Goal Setting Introduction Goal setting provides an ideal opportunity for the person who has had a stroke, their carers, and the involved health professionals to communicate their aims for the future. Goal setting is an essential part of rehabilitation practice, and should be viewed as a dynamic process that can be adjusted according to progress [1]. The event of stroke can result in enduring activity limitations and restrictions to participation for an individual. Many people who have had a stroke perceive the discontinuation of rehabilitation therapies as the cessation of their recovery process. The promotion of goal directed behaviour is recognised as an imperative component for ongoing recovery and the achievement of successful adjustment [2]. Further rehabilitation input for people who have had a stroke requires new goals to be devised and targeted management plans developed. [3] There should be a person-centred approach to the goal setting process, which involves a collaborative process to determine which activities are intrinsically motivating for an individual [4]. Motivation and goals are considered to be inextricably linked. The concept of motivation can be viewed in several different ways – including intrinsic characteristics or personality traits of the individual, and extrinsic environmental influences (such as qualities of the involved health professionals or the status of the person’s social support) [1]. With this concept in mind, it is therefore important for health professionals to get to know the person in order to assist them to set meaningful goals, and to empower and support them to make behavioural changes. It is necessary to gather insight into the person’s perspective about their current situation. During the early post-stroke recovery phase there is generally an initial focus on goals aimed at achieving medical stability, and maximal independence in personal activities of daily living and basic mobility status. As the person transitions into the sub-acute phases post-stroke, goals that encompass social functioning and community reintegration become more important. Goals need to be established that reflect the continuum of the person’s recovery process, and reflect overall functional aims in relation to home, vocational, and community environments [5]. Initially, the person who has had a stroke may want to resume various meaningful activities, however, the severity of their activity limitations may preclude their future involvement. As time progresses post-stroke, the perceived attainability of some valued goals may change as the individual adjusts to their altered ability status [1]. Health professionals should utilise their clinical experience to assist the person who has had a stroke to determine realistic and appropriate goals, and to allow for modification and adaptation of aims as the recovery process evolves. Guidelines for Goal Setting: Rehabilitation services should adopt uniform guidelines and processes for the goal setting practice. Goals are often not well established, therefore making evaluation and measurement of actual goal attainment difficult. Vague or global goals also make it difficult for the health professional and the person who has had a stroke to recognise change in status or improvement [5]. A common acronym used when constructing goals is S.M.A.R.T. There are variations to the make-up of the letters of this acronym, but in general, the typically accepted connotation is: S = Specific Set specific goals in collaboration with the individual and family or carer that will motivate the person. Examples:
Walk ‘Scout’ (the dog) twice around the oval every second day.
Return to weekly aqua-exercise group with an assistant to help with dressing
M = Measurable Be able to measure status or progression towards a achieving a goal. Avoid non specific terms such as ‘improve’, ‘increase’, and ‘more or less often’. Identify possible outcomes (such as behaviours or events) which will reflect change (either improvement or decline). Consider outcomes in terms of: How much? (quantity), How often? (frequency), How long? (duration), and Level of assistance or supervision required? Examples,
Babysit my grandchild (Jeremy) once a fortnight for a three hour session.

34
Bring myself forward in the shower chair independently so that the carer can wash and dry my back (daily)
Tend to the vegetable patch on two occasions per week – weeding and turning soil with my left hand
A = Attainable Set realistic / reachable goals. This may require the setting of smaller goals initially, with a more complex goal being the final outcome. Examples,
Hit 30 golf balls at the driving range in first session. Build up to 50 balls (in one session) at the driving range by three weeks.
Stay out of bed during the day for equivalent of half a day (five hours duration in total)
Attend lunch with girlfriends once a month
R = Relevant The type of goals set should reflect the needs and interests of the individual, and endeavour to give direction and purpose to their chosen way of life. Examples,
Go to the bowls club for a meal at least once a fortnight, even though I am unable to play at this stage.
Catch a tram to the Kew library every week to read the magazines of interest (especially gardening magazines)
T = Timebound A timeframe should be established. Examples,
Be able to consistently read the time on my watch in less than four seconds by the time of my next review (3 months)
Order a cappuccino for my wife at the cafe each Sunday (initiate communication strategies without prompting). Be able to also place the entire breakfast order by six months.
In three weeks, I will have walked to Jake’s house to have afternoon tea and discuss the football draw.
At the end of an agreed timeframe, goals need to re-assessed to determine their effectiveness to produce desired results. Readjustment of different aspects of the S.M.A.R.T. process may be required over time. Future contact with the client may necessitate resetting of goals Example, During her first engagement with the Community Rehabilitation Centre, a collaborative goal was devised with Lilian (45 yr old, 8 months post stroke, living at home with family, walking 50m independently with stick and orthosis): Goal - To leave the house at least once a week for a purpose other than a healthcare appointment On her second engagement with the Community Rehabilitation Centre (8 months later), a new collaborative goal was added that reflected her current wishes and concerns: Goal – To dance with my husband at social events without feeling embarrassed Modification and adaptation of goals over time is an important part of the therapy process, and should be an essential part of the rehabilitation service. Goal domains: When managing the person who has had a stroke, the goals that are set need to reflect the recovery phase. A person who is over six months post-stroke may require an additional focus on goals that encourage participation and community reintegration, but with consideration of body structure/function impairments and activity limitations related to these goals. Example,
As time progresses post-stroke, more attention to may be required to mobility aids that enhance independence and community access if the current mobility aid is limiting function. For example, Charles (69 yr old, 15 months post-stroke, home alone) is reticent to walk the 1.2 km to the newsagent to get the daily paper and stop by the local cafe. Even with a more supportive gait aid that has recently been supplied (he is now trying a 4 wheel walker for longer distances), Charles is still not walking the distance to the shops. He is now tending not to venture out of the house very much, as he

35
is not someone who ‘just goes for a walk without a purpose’. Consideration needs to be given to the importance of Charles continuing to get out into his community. An electric scooter may be a feasible option to explore. Walking ability could be interwoven into another goal that specifically targets mobility if there were concerns about the maintenance of this function. Charles should still strive for the goal to walk to the local shops, but he may require a more specific stepwise plan. Therapy sessions could focus on community mobility, with the goal to walk to and from the shops by the fifth session. Goal setting is difficult for many people with stroke. If the person struggles with collaborative setting on the initial review, consider delaying goal setting until you come to understand the person and the activities that are meaningful to them. Consider appropriate referral to other community or health services to facilitate specific goal achievement.
Goal setting process Determine a list of goals across a spectrum of timeframes and settings. For example, devise suitable goals whilst the patient is engaged in active rehabilitation with health professionals (i.e. for the duration of a sub-acute care rehabilitation episode), and also devise longer terms goals that patient and family can continue to pursue in their home/community setting. Goals should be re-evaluated, with adaptation as necessary. There are validated methods for evaluating goal achievement, such as the use of Goal Attainment Scaling [6]. Clearly document GOALS:
1.
2.
3.
4.
5.
6.
Specific ‘Flags’: Goals not achieved within timeframe – seek to identify the reasons for reduced goal attainment. Consider:
- The individual’s awareness and understanding of the set goals - Motivational factors (such as individual traits, external support networks – both health
professionals and family/friends/carers) - The health status of the individual, or occurrence of interim adverse events - The realistic nature of the goals and timeframes that have been set
References 1. Siegert, R.J. and W.J. Taylor, Theoretical aspects of goal-setting and motivation in
rehabilitation. Disability and Rehabilitation, 2004. 26(1): p. 1-8. 2. Kelly-Hayes, M. and C. Paige, Assessment and psychological factors in stroke rehabilitation.
Neurology, 1995. 45: p. S29-S32. 3. National Stroke Foundation, Clinical guidelines for stroke management. 2010, Melbourne
Australia. 4. Cott, C.A., R. Wiles, and R. Devitt, Continuity, transition and participation: Preparing clients
for life in the community post-stroke. Disability and Rehabilitation, 2007. 29(20-21): p. 1566-1574.
5. Ottenbacher, K.J. and Cusick, A, Goal attainment scaling as a method of clinical service evaluation. American Journal of Occupational Therapy, 1990. 44(6): p. 519-525.

36
6. Kiresuk, T.J. and R.E. Sherman, Goal Attainment Scaling: A general method for evaluating comprehensive community mental health programs. Community Mental Health Journal, 1968. 4(6): p. 443-453.
Case Examples
Case 1
James is a 64 year old gentleman who had stroke 14 months ago – with residual physical deficits of mild (L) hemiparesis (upper limb > lower limb) and moderate dysarthria. He is independent with all transfers and mobility (stick). He tends to tire at about 1km, and occasionally then his left foot will begin to scuff the ground during swing phase of gait. Since his stroke, James’ wife tends to do set-up tasks for him – such as get out his clothes for the day, lay out his grooming items (shaver, comb, toothbrush and paste), and cut up his meals.
Initially James was using his left hand to assist with all functional activities, but over the past 4 months he has tended to increasingly just use the right hand. James is embarrassed about his slurred speech, and now particularly dislikes conversing on the phone.
Prior to his stroke, James enjoyed:
Writing short stories and poetry on the computer – he has resumed this, tending to type with one hand. He used to enter his work into local writing competitions.
Punting on the horses at the local TAB – still enjoys this. Was attending weekly prior to stroke. Now goes once or twice a month.
Supporting Collingwood Football Club – plans to buy a membership again, but doesn’t think that he will go to the matches very often any more - ‘Too much bother’
Breakfast every Thursday at ‘Chico’s Café’ – was walking there with his wife (about 1.8 km away) prior to his stroke.
Reading ‘The Age’ over a morning cuppa – he mentions that this is ‘an important start to the day’
James has been referred for an assessment in the Community Rehabilitation Centre (CRC) after a fall, and his wife also thinks that he should be using his left hand more.
There were many activities that James highlighted as being of interest prior to his stroke. In collaboration with James, it was decided to initially focus on attendance to the football and writing a poem for the next local writing competition. There were also some domains that the therapists wished to address (concerning left hand functional ability, speech clarity, and the fall incident), and in discussion with James, activities that incorporated these aspects were also devised. In addition to re-engaging the CRC’s Occupational therapist, Physiotherapist, and Speech Therapist, a plan was devised to utilise James’ network of friends to assist with the football goal. An important part of the process was to determine the barriers to James’ participation in attending a Collingwood football match – what was creating the impression that it was ‘too much bother’? Goal – attend a Collingwood football match at the MCG with the assistance of friends. Previously James used to catch the train to the football. During discussions, train travel emerged as significant concern for James, as he was worried about losing balance on the train and walking to the football ground in the crowds. His friend is happy to drop him to and from the ground, whilst another friend is happy to accompany him to the matches. Working on balance on a moving train and in crowds could be an ongoing goal for the future, but currently it was determined that the main goal was to actually attend some matches. Plan – James is to attend the Collingwood match next week. During the next CRC session the therapists will review how the outing went and whether any other concerns arose that would prevent James from wanting to attend in the future. Goal - write a poem for the next local writing competition The next writing competition is in seven weeks (run jointly by the library and local Heritage group). James’ task prior to the next CRC session is to ‘brainstorm’ ideas for some poems, and to try to produce at least four lines of written work. The plan is to produce three poems over the next six weeks, then choose which one he would like to submit for the competition.

37
At a review appointment (8 weeks after the CRC episode of engagement), James has been attending all the Collingwood home matches (MCG). He had not ventured to the match via train as yet, as his friends are happy to continue driving him to the ground, and James still thinks that he would not manage the moving train if he was forced to stand. Later in the month Collingwood has a match at Docklands. The goal is now for James to attend a Collingwood football match there.
Case 2
Jessie is a 76 year old woman who sustained a right occipital haemorrhage (13 months ago) – with a resultant left homonymous hemianopia. Her husband died 8 years ago, and she has lived alone ever since. None of her 4 adult children reside in Melbourne.
Jessie was managing all her activities of daily living (ADLs) independently at home prior to her stroke, and was also independent with her gait (using a single point stick when outdoors). She used to ambulate around the retirement village once a day (weather permitting), which was a very social event as she would stop frequently to chat to the other residents.
Since the stroke, Jessie uses a 4-wheel frame when walking outdoors, and a single point stick indoors. Her unit has been modified with the installation of rails in the toilet, shower, and front entrance. She is safe and stable with all her ADLs and mobility.
Jessie tends not to go outdoors for walks anymore. She now has a fear of falling, especially since she tripped over a table leg whilst in hospital – she mentions that she has had several friends who have ‘broken their hips’ over recent years. Jessie walks to her letter box to retrieve her mail, and tends to hover for a while in the hope that a neighbour may pass to converse with.
Other areas of interest:
Gardening, especially her rose bushes – one of her children has now arranged for a gardener to attend to the garden monthly.
Avid reader of fiction novels – now having great trouble reading due to her visual deficits.
Watching TV – especially cooking or gardening shows
Church attendance (weekly) – was on the coffee roster prior to her stroke. A friend drives her to church.
Volunteer at the Op Shop – was volunteering 2 x per week prior to the stroke, but has only been down to the Shop twice since her stroke to ‘catch up with the girls’.
Fortnightly Sewing group – making goods to donate to the Royal Children’s Hospital – not attending – ‘can’t sew anymore’.
Jessie’s General Practitioner has referred her for a review by the Community Rehabilitation Centre (CRC) to ‘improve her outdoor mobility’.
There are many activities that Jessie enjoyed prior to her stroke. In particular, her confidence with walking appears diminished over time, and it is now having an overriding effect on various other activities that she used to enjoy. There are several activities that could be targeted during this CRC engagement, but in discussion with the CRC therapists, Jessie is very keen to resume her outdoor walks around her home. Goal – to walk around the retirement village daily There would be a need to address the factors that are contributing to Jessie’s fear of falling, with a concurrent focus on outdoor mobility. After a thorough review of balance and falls risk, many of Jessie’s therapy sessions were conducted outdoors, with emphasis on particular strategies to maximise compensation for her visual deficits. The final three sessions involved ambulating around her retirement village, initially with supervision. Goal - resume reading fiction novels. However, even with adaptation to font size and other reading strategies from the therapists, Jessie found reading to be laborious task that caused fatigue and headaches. Jessie was then introduced to audio-books, which she thoroughly enjoys. At a review appointment (six weeks after the cessation of the Community Rehabilitation Centre sessions), Jessie is walking daily around parts of the retirement village. Her distance and speed are

38
reduced compared to prior to the stroke, and she now tends to walk a particular, familiar route. Jessie is pleased with her achievement, and also considers that she would now like to resume helping at the Op Shop as she is much more confident with standing and walking, especially in familiar environments. A new goal was set in line with what Jessie had voiced – volunteer at the Op Shop once a week, with some simple modifications to the tasks that she was doing prior to her stroke.
Case 3
Harold is a 68 year old male who had a stroke 15 months ago - which resulted in (L) neglect and reduced short-term memory (nil focal muscle weakness evident).
He recently attended a 12 month review appointment with the Rehabilitation Medicine Specialist. At this appointment, his wife expressed great concern about the amount of idle time that Harold seems to have nowadays, which appears to make him bored, frustrated and irritable. It was recommended by the doctor that Harold attend an assessment at the Community Rehabilitation Centre for an overview of his activity profile, with the view to try to structure a weekly routine that would assist him to re-engage in activities. The Rehabilitation Medicine Specialist considered that a trial of anti-depressants was also warranted.
Social history: Harold lives at home with wife. He is a retired photographer, currently receiving aged pension. 3 children / 1 grandchild.
Harold was managing all ADLs independently at home prior to his stroke. As part of his family role he enjoyed preparing breakfast each day for his wife. He would also drive his wife to the shops each week, where they would complete the shopping tasks together (wife does not drive). Harold was also independent with banking (i.e. had set up direct debit for most bills, and paid all others over the internet).
Harold enjoyed photography (he used his high powered digital camera on most days of the week), and would spend much of his day editing photos on the computer. He would also frequently use the internet to ‘surf’ and email friends. Harold and his wife liked to walk around the block daily after dinner. He used to walk, feed, and groom his pet cocker spaniel ‘Ruby’.
Current level of functioning:
Harold is independent with all personal care tasks. He is able to complete light meal preparation tasks independently, however his wife often comments on the amount of mess he now makes when he prepares her breakfast. Harold has commented on being frustrated with the amount of time it takes him to prepare meals and the difficulty he has with locating items in the kitchen, and around the house in general.
Harold needs to be supervised by his wife when accessing the community due to his difficulty with recognising the streets surrounding his local environment. He also needs reminders to check his left hand side when crossing the road (due to his neglect). He reports that he is embarrassed with his wife having to continually tell him to look to his left side, and at times gets irritable with her. He is unable to independently take ‘Ruby’ for a walk, and his wife has tended to take over the other pet care tasks since his stroke.
Harold now requires assistance with using his computer (such as, help to locate icons on the screen and the keys on the keyboard). He finds attempting to use the computer upsetting, and has tended not to try this over the last seven months.
Harold requires assistance with using his own digital camera (he is unable to locate buttons, unable to recall basic operations, and tends to perseverate with turning the camera around & around to locate buttons). He finds this task frustrating and reports that he is no longer finding enjoyment with this activity.
Due to his (L) neglect, Harold is no longer able to drive. Harold and his wife rely on public transport to travel to the shops.
Harold reports being optimistic that things may get easier into the future, but does admit to feeling “low” a lot of the time, especially about how reliant he is on his wife.
Harold is receptive to idea of attending the CRC for some therapy input, as he would like to resume some of his leisure pursuits, but he is somewhat pessimistic as to whether anything will change.

39
The CRC therapists interviewed Harold to develop an activity profile reflecting his usual daily/weekly participation status. There was indeed a lot of idle time during the day when Harold would tend to just sit, or wander about the house without a true purpose.
Goal – to resume taking photographs, and perform basic editing on the computer
Harold owns a very expensive, complex digital camera. He has been unable to negotiate its multiple functions since his stroke. It was decided that a camera with simplified functions would initially be more appropriate. Harold purchased a suitable camera, and therapy sessions involved basic camera use, navigation of commonly used functions, and downloading of the photos onto a computer. The therapists developed a pictorial guide specifically for Harold to prompt his memory and simplify the process. Harold was given certain ‘projects’ that he had to achieve prior to the next CRC session. For example, Project 1 – Harold had to ‘teach’ the therapist how to use the camera and download photos. Project 2 – Harold was asked to take a series of pictures of ‘Ruby’ the dog throughout the week in different settings. Project 3 – Harold had to perform basic editing on the computer using five photos that he had taken of his grandson (this involved zoom / crop / red-eye reduction) etc.
Another goal that was set was concerning the family pet ‘Ruby’. Harold had inadvertently delegated all care of ‘Ruby’ to his wife since his stroke.
Goal – take full responsibility for all pet-care tasks for ‘Ruby’, except for walking.
This includes tasks such as: grooming, feeding, veterinary appointments, council registration, and training. These are all jobs that are within Harold’s capabilities. A daily list was placed on the fridge to prompt Harold with his pet-care tasks.
At a 6 week review appointment, there was a marked reduction in the amount of idle time evident during Harold’s day. The therapists suggested that Harold could continue to set ‘projects’ for himself – perhaps choosing a different topic to photograph, or add a camera or computer skill to learn. A future goal was to trial his complex digital camera with the use of coloured stickers over the function buttons to simplify its use.

40
Chronic Stroke Rev-TIG Screening Assessment
Participation Screening Assessment Identification of valued activities Questions to explore with the patient / carer:
What activities did you enjoy doing prior to the event of your stroke?
What activities do you enjoy or value now? Document current participation status in relation to the identified activities (devise a daily/weekly activity profile). Determine whether the activity has been ceased, continuing, or is a new activity since the stroke event. Highlight those activities in the profile that the patient particularly values.
What stops you from engaging in activities that you enjoy or value? (Determine any barriers contributing to a reduced participation status)
Who do you see regularly? (Determine level of social interaction)
Valued activities prior to stroke Level of participation (e.g. daily, weekly etc)
Current activity status Level of participation (e.g. daily, weekly etc)
Main barriers to participation in above activities (consider community access, transportation, social support network):
Level of social support / Status of family role / Adaptation and adjustment to altered status: Who do you see regularly?
Level of social interaction: Increased since stroke Reduced since stroke
Similar to pre-stroke Severely reduced since stroke
Concerns with family role / Adjustment to altered roles:
Name:_________________________
DOB:_______________________
Strike through any
components not relevant

41
Functional limitations and decline screening assessment Functional Status:
How has your mobility / walking / stairs been recently?
Improved Same Declined
What precipitated this change?
How far can you walk before you are tired?
Comments:
Are you able to use your arm? Yes No
Has this changed recently? Improved Same Declined
Comments:
Are you able to perform self care tasks without help? eg. Showering, dressing, grooming
Yes No
Has this changed recently? Improved Same Declined
Comments:
Fatigue:
Over the past month, have you felt fatigued, had a lack of energy, or have had to rest every day for a period of two weeks? [11]
Yes No
Has this fatigue led to difficulty completing tasks that you normally do as part of your daily life?
Yes No
Continence:
Do concerns about continence limit your ability to get out and about?
Yes No
Comments:
Minimising risk of falls screening assessment Have you fallen in the last 12 months? Yes No
If yes, how many?
Injuries sustained:
Circumstances of falls:
If no falls, do you worry about falling? Yes No
Comments:
Communication screening assessment Do you have difficulty communicating with other people? (understanding what is said to you; speaking to others) Does your communication difficulty affect your ability to do the things you want to do?
Yes Yes
No No
Does the patient have difficulty with communication? If yes, type:
Yes No
Has this difficulty with communication changed since your discharge from hospital? (ie improved/ the same/ worse) If improved – consider speech referral to consolidate gains If worse – consider speech referral to investigate deterioration
Yes No
Is your communication ability impacting on your ability to participate in activities? Yes No

42
Are you able to communicate with? Examples of Other: Shop owner / a stranger / on the telephone / order a meal, etc.
Your partner/carer
Family
Friends
Other ______________
Do you use any communication strategies / aids? If yes, discuss type of strategy / aid and compliance:
Yes No
Cognition screening assessment Functional Status:
Has your memory/thinking abilities changed recently?
Improved Same Declined
What precipitated this change?
Are you able to remember the things you need to remember in everyday life?
Do you use any strategies to help you remember things or organise your day?
Comments:
Depression screening assessment
History of depression:
Do you have a history of depression? Yes No
If yes, the depression was diagnosed by: General Medical Practitioner Psychiatrist Psychologist Other_________________________________ Not formally diagnosed / Patient self-report Date diagnosed:___________________________
Treatment / Management strategies that have been used previously: (e.g. medications, cognitive behaviour therapy, interpersonal therapy or counselling, physical exercise programs)
Contact details of practitioner Mental Health Practitioner:
Date of last review appointment:
Anti-depressant medications:
Are you currently taking antidepressant medication? Yes No
If no, has the patient taken antidepressant medication in the past? When were they ceased? ________________
Yes No
If yes, document medication below
Are you compliant with your medication? Yes No
Name Dose Frequency Date commenced

43
Geriatric Depression Scale
1. Are you basically satisfied with your life? Yes No
2. Have you dropped many of your activities and interests? Yes No
3. Do you feel that your life is empty? Yes No
4. Do you often get bored? Yes No
5. Are you in good spirits most of the time? Yes No
6. Are you afraid that something bad is going to happen to you?
7. Do you feel happy most of the time? Yes No
8. Do you often feel helpless? Yes No
9. Do you prefer to stay at home, rather than going out and doing new things?
Yes No
10. Do you feel you have more problems with memory than most? Yes No
11. Do you think it is wonderful to be alive now? Yes No
12. Do you feel pretty worthless the way you are now? Yes No
13. Do you feel full of energy? Yes No
14. Do you feel that your situation is hopeless? Yes No
15. Do you think that most people are better off than you are? Yes No
Score: /15
Health-related quality of life screening assessment
How satisfied are you with your life as a whole?
If the patient reports a diminished quality of life, ask further questions that examine the factors that contribute to the patient’s perception of their quality of life. Explore such concepts as [11, 12]:
- Health - Personal relationships / wider sense of feeling part of a community - Psychological wellbeing - Sense of safety - Faith, spirituality, religion - Standard of living - Level of achievement in life - Future concerns / future security
Are there goals that you could pursue which would influence your quality of life perception?
Secondary stroke prevention and risk factor management screening assessment Identification of risk factors
Do you have any stroke risk factors? (for example, hypertension, diabetes, altered lipid status, smoking, elevated alcohol consumption).
Risk factor Current management
How often do you attend your General Practitioner or Medical Specialist for a specific review of your risk factors, such as the status of your blood pressure, diabetes, and/or cholesterol levels?
How often do you attend your General Practitioner or Medical Specialist for a thorough review of your medications?

44
Do you have any post-stroke complications? (for example, recurrent stroke, seizures, recurrent infections, pain, osteoporosis)
Post-stroke complications Current management
Carer assessment Name: Relationship to patient:
Co-resides with patient: Yes No
Describe caring role / usual tasks (e.g. provides manual assistance with transfers, prepares main meals, provides transport, emotional support to patient, availability)
Formal support for carer (e.g. allowances, respite arrangements)
Informal support for carer (e.g. family, friends, religious affiliations, clubs). Describe how they assist:
Previous use of services for carers (such as counselling, education sessions, support groups)
Yes No
If ‘Yes’, give details:
Do you feel that you are currently managing at home? (discuss any issues that may be causing stress to the carer – such as: care recipient impairments resulting in cognitive, communication, and physical deficits that increase the stress and burden of caring. Also, inquire about patient personality changes (such as irritability or emotionalism), and changes to the roles within the family and household (such as inequality with tasks and decisions, financial implications, relationship issues)
Outline needs / concerns from the carer’s perspective:
Does the carer require / request other information?
Depression Screening Tool
Geriatric Depression Scale (15 item) If yes, Score: /15 [17]
Yes No

45
Goal setting process Determine a list of goals across a spectrum of timeframes and settings. For example, devise suitable Clearly document GOALS:
1.
2.
3.
4.
5.
6.
Clinician’s Name: ________________ Signature: ___________________ Date:_____________

46
Chronic Stroke Rev-TIG Screening Assessment Summary
Participation status
List of valued and required activities
Current level of involvement
Unable to do
Limited Active
Comments:
Main barriers to participation in above activities:
Functional limitations (including if recent decline in function)
Functional Domain Decline? (circle)
Outline current status & any change in status
Mobility: transfers / gait Yes No
Arm function Yes No
Self care activities Yes No
Fatigue
Fatigue experienced every day for two weeks consecutively Yes No
Fatigue has led to difficulty completing daily tasks and activities Yes No
Continence
Concerns regarding continence Yes No
If ‘Yes’, comment:
Minimising risk of falls
Fallen in the past 12 months Yes No If ‘Yes’, how many falls?
Circumstances of falls:
Injuries sustained:
Worried about falling (even if there are no episodes of falls) Yes No
Communication
Acquired communication impairment Yes No
Difficulty communicating with other people Yes No
This difficulty with communication has changed recently Yes No
If ‘Yes’, comment:
Cognition
History of cognitive impairment Yes No Pre-stroke Post-stroke
Describe:
Decline in cognitive function recently Yes No
If ‘Yes’, comment:
Name:_________________________
DOB:_______________________
Strike through any
components not relevant

47
Mood status – depressive symptoms, anxiety, reduced coping, reduced self-efficacy
Geriatric Depression Scale (15 item) Score: /15
Mood status warrants further discussion Yes No
Comments:
Health-related quality of life
The individual identifies certain factors as affecting their perception of their quality of life:
Secondary stroke prevention and Risk factor management
Risk Factors & Current management:
Recent medication review? Yes No
Carer assessment
The carer feels that they are currently managing at home Yes No
Outline needs / concerns from the carer’s perspective:
Geriatric Depression Scale (15 item) Score: /15
Zarit Caregiver Burdern Scale (22 item) Score: /88
Does the carer request / require further information? Yes No
Comment:
Goals set – collaborative goals with individual / family / carer
1.
2.
3.
4.
5.
Community Rehabilitation Centre Plan
Therapies involved, attendances per week, groups etc:
Next CRC review:
Additional information for GP / Issues that the CRC would like raised in the next GP review:
Clinician’s Name: _________________________ Signature: _________________________ Date:_____________ This summary is designed to be given to the individual and their carer, sent as a summary to the individual’s GP, and filed in the individual’s medical record





























