Embed Size (px)
Citation preview

1
Supplement to the Journal of Invasive Cardiology, June 2012
Percutaneous Intervention of Chronic Total Occlusion in Critical Limb Ischemia
Kiran Y. Saraff, MD
CLINICAL CASE UPDATE
Chronic critical limbischemia (CLI) representsthe extreme spectrum ofperipheral arterial disease(PAD), accounting forabout 1% to 3% of allPAD patients.1 CLI mani-fests as ischemic rest pain,gangrene and/or ulcera-tion. CLI is consideredchronic when symptomspersist for more than 2weeks. It occurs when skinperfusion pressure at theaffected site is reduced to adegree such that tissues’resting metabolic needsare not met. Generally,ischemic rest pain occurswhen systolic pressures atthe ankle and toe arelower than 50 mm Hg and 30 mm Hg, respectively.Particularly in non-diabetic patients, the loss of per-fusion pressure is due to multi-level occlusionsbetween the aorta and pedal vessels.1
Some ulcers are caused solely by ischemia; othersare caused by a combination of factors such asischemia, neuropathy, trauma and venous insuffi-ciency. Regardless of the etiology of the ulcer, ifischemia is present, it must be corrected to achievewound healing.
The majority of the foot ulcers present below theankle are typically due to arterial insufficiency.Wound healing is an inflammatory response and,therefore, requires greater blood flow than is neededto simply sustain tissues. Perfusion pressure needs tobe about 70 mm Hg at the ankle and 50 mm Hg atthe toe to achieve wound healing. Collateral flow
generally lacks enough pressure-head to achievewound healing. To heal wounds in chronic CLI,therefore, it becomes necessary to establish straight-line pulsatile flow from the aorta to the vessel sup-plying the affected area.
Like ischemic ulcers, ischemic gangrene resultsfrom spontaneous necrosis of the skin due to severeischemia, usually precipitated by some local trauma.While the underlying cause of gangrene is ischemia,the treatment often is primary amputation of theaffected part. A study that involved a large Medicaredatabase found the rate of primary amputation forgangrene to be 67%.2 The same study reported sur-gical revascularization before amputation at 23%and percutaneous revascularization at 10%.2 Thestudy also reported underutilization of vascular stud-ies, such as ABI and angiography, to diagnoseischemia before amputation.
Failing to correct underlying ischemia before pri-mary amputation often results in amputation revi-sion to higher levels, until the plane of adequate vas-culature is reached. Major amputations such as
LLC
, ™
From Saint Joseph Hospital, Lexington, KY. Address for correspon-dence: Kiran Y. Saraff, MD; 1401 Harrodsburg Road, Suite B-395;Lexington, KY 40513. Email: [email protected]. Disclosure: Theauthor has received an honorarium from Bard Peripheral Vascular.
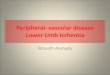
Femoral CTO — pre-intervention
Proximal occlusion cap
Distal reconstitutionin the Hunter'scanal
Profunda femoris artery
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 1
BardCCU_1-6.indd 1 5/10/12 4:46 PM

2
below-the-knee or above-the-knee carry 6.3% to13.3% mortality rates in the perioperative periodand 43% and 61% mortality rates within 3 years.3
Only about 70% of stumps heal by primary inten-tion with a 15% conversion rate to above-the-knee amputation.4 Furthermore, the contralaterallimb is also at risk in an amputee, as about 30%to 53% of amputees undergo contralateral majoramputation within 5 years.5 The goal should be toachieve enough revascularization to establish astraight-line pulsatile flow to the pedal arch, witha view to minimizing the amputation level (so thatthe patient remains ambulatory) or healing with-out amputation.6
Tibial vessels are involved in the majority of CLIcases. Tibial occlusions are often long-segment occlu-sions. Revascularization can be achieved with surgicalbypass or via percutaneous endovascular means.Surgical revascularization of tibial vessels has goodlong-term patency when venous conduits are used.1
However, many CLI patients have had coronarybypass surgery, making venous conduits unavailable.Further, surgical revascularization is associated withprolonged recovery, potential saphenous vein loss,chronic lower-extremity edema, and worsened symp-toms if a graft fails. Infrainguinal bypass complicationsinclude death (up to 6%), myocardial infarction (up to3.4%), wound infection and complication (up to 40%),and vein infection (1.4%).7,8
Even with successful bypass, amputation is need-ed in 5% to 10% of patients.7 In contrast to surgicalrevascularization, the endovascular approach offersseveral advantages. It is minimally invasive with vir-tually no recovery time. Mortality and morbidity aremuch lower. Restenosis that occurs after woundhealing is easily tolerated, as intact skin has muchlower metabolic demands than healing tissue.Revascularization via the endovascular approach canbe achieved in up to 94% of patients, with resulting5-year limb salvage rates up to 91%.9
The BASIL trial supported the percutaneousapproach, showing equivalent patency and limb-salvage rates compared to bypass surgery at 3years and superior cost effectiveness.10 In CLI,revascularization’s goal is to heal tissue and com-plete wound closure. With good wound care andinfection control, wounds typically heal within 6to 12 weeks of achieving straight-line pulsatileflow in the affected area. After wound healing,intact skin can maintain integrity with good footcare, even with occluded vessels. Further, percu-atenous intervention can be repeated as neededuntil wound healing is achieved. While thisapproach may seem expensive compared to pri-mary amputation, economic analysis has shown
that successful revascularization and amputationprevention are more economical from patient andsocietal standpoints.2
Percutaneous revascularization (percutaneoustransluminal angioplasty, or PTA) of tibio-pedalvessels poses many challenges. Calcification andlong-segment total occlusions are some of them.Calcification is especially problematic in chronicrenal failure and dialysis patients. Chronic totalocclusions (CTOs) of tibial vessels are the rule ratherthan the exception in patients with CLI. Ipsilateralfemoral antegrade access, popliteal access, and tibialaccess are essential in many cases.
Tools available to cross these CTOs include0.014-in. and 0.018-in. stiff wires, 0.018-in. glidewires and, more recently, the CROSSER™
Recanalization Catheter (Bard, Inc., Murray Hill,NJ). The CROSSER™ Catheter uses high-frequencymechanical vibration (delivered at 20,000 cps) andcavitation to penetrate through atheroscleroticplaque. The CROSSER™ Catheter is indicated to facili-tate the intraluminal placement of a conventionalguidewire beyond the peripheral artery’s chronictotal occlusion via atherectomy. A multicenter, non-randomized prospective clinical trial of 85 patientswith guidewire refractory CTOs demonstrated 84%success crossing with an average activation time of 2minutes.11 A large, single-center, registry experiencehas shown this device successfully crosses CTOs at arate of about 95% in tibial arteries.12
The following sections examine 3 successful cases.
Femoral CTOA 77-year-old, nonsmoker, nondiabetic African
American female presented with a more than 6-month history of severe calf claudication of theleft leg. She had a prior history of CLI, withthreatened amputation of the left leg, which hadbeen due to an infected, non-healing ulcer of theleft great toe in August 2010. At that time, shewas noted to have a totally occluded left externaliliac artery; severely diffusely diseased commonfemoral, superficial femoral and popliteal arteries;and an occluded left anterior tibial artery. She hadbeen treated with PTA and stenting of the leftexternal iliac artery, orbital atherectomy, and PTAof the left femoro-popliteal and anterior tibialarteries in a staged manner.
At this visit, the angiogram showed patent leftexternal iliac and common femoral arteries. Thesuperficial femoral artery (SFA) was totally occlud-ed just past the ostium, with a favorable anatomy.It reconstituted in the Hunter’s canal, where therewas diffuse stenosis up to the origin of the poplitealartery. Infrapopliteal arteries were patent.
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 2
BardCCU_2-5.indd 2 5/10/12 4:47 PM

3
A contralateral approach was used with a 6 Fr, 45cm Pinnacle sheath. The sheath tip was positioned inthe left common femoral artery. The CROSSER™
Catheter 14P (RX) system was used over aGrandslam wire. Using the roadmap technique, theproximal cap was crossed in 15 seconds. Heavy cal-cification in the middle portion of the occlusionposed some difficulty. The distal cap was crossedluminally. Balloon angioplasty was performed usinga 5.0 x 200 mm VASCUTRAK® PTA DilatationCatheter at 6 atmospheres of pressure for 3 minutes.Due to dissection and residual stenosis in the calci-fied portion of the artery, the SFA was stented using6.0 x 150 mm and 6.0 x 80 mm LIFESTENT® VascularStent Systems. The stents were post-dilated using a5.0 x 200 mm balloon.
The completion angiogram showed an excellentresult, with no residual stenosis or gradient. Distalrunoff was normal. Heparin (50 units/kg of body
weight) was used for periproce-dural anticoagulation. The arte-riotomy was closed with thePerclose device.
Infrapopliteal CTOA 70-year-old male smoker
presented with a history ofchronic venous stasis edema anda 6-month history of bilateral,lower-leg/foot ulceration andgangrene of the heels. Anangiogram performed elsewhereshowed stenotic SFA and occlud-ed infrapopliteal vessels. SFAwas treated percutaneously. Anattempt at tibial vessel interven-tion was unsuccessful, resultingin a pseudoaneurysm of the rightanterior tibial artery. The patientwas sent for tibial vessel angio-plasty consideration.
Ipsilateral antegrade femoralaccess was obtained, and a 6 FrPinnacle sheath was used. A prox-imal occlusion cap in the rightanterior tibial artery (ATA) wascrossed with the CROSSER™
Catheter 14P (RX) system over anAsahi Prowater wire within 9 sec-onds. However, the CROSSER™
Catheter was caught in thepseudoaneurysm in the mid-vessel(which was unknown to the oper-ator at the time). Therefore, theCROSSER™ Catheter was with-
drawn, and the wire was exchanged for an AsahiAstato-30 wire, which was maneuvered into thedistal vessel. The wire was then exchanged for aGrand Slam wire, and PTA was performed using a2.0 x 200 mm balloon at 6 atmospheres for 3 min-utes. More proximally, PTA was performed using3.0 x 100 mm balloon at 8 atm for 2 minutes. Theportion of ATA with pseudoaneurysm was stentedusing a 3.0 x 32 mm stent. The distal ATA termi-nated at the ankle.
Next, the occluded posterior tibial artery wascrossed with the CROSSER™ Catheter 14P (RX) sys-tem over the Asahi Prowater wire in 5 seconds.The CROSSER™ Catheter was taken to the pedalarch. The wire was then switched to a Viper wireand orbital atherectomy was performed using a1.25 mm classic crown at 140,000 rpm for 24 sec-onds and 180,000 rpm for 16 seconds.Subsequently, balloon angioplasty was performed
Femoral CTO
CROSSER™
RecanalizationCatheter crossing theproximal cap
CROSSER™
RecanalizationCatheter crossing the distal cap
Superficialfemoral artery
Profundafemoris artery
Superficialfemoral artery
Poplitealartery
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 3
BardCCU_3-4.indd 3 5/10/12 4:47 PM

4
with a 2.0/2.5 x 210 mm balloon at 6 atmospheresfor 3 minutes. The more proximal vessel was treat-ed with a 3.0 x 100 mm balloon at 7 atmospheresof pressure for 1 minute.
Heparin was used for periprocedural anticoagula-tion. The arteriotomy was closed with the Angio-Sealdevice. Intravenous antibiotics were administered andwound care was performed on a long-term basis; 8weeks later, the wounds had completely healed.
Popliteal CTOA 66-year-old white male with history of diabetes,
hypertension and smoking presented with a 6-monthhistory of a non-healing ulcer on the dorsal shin ofthe right leg. He had undergone primary trans-metatarsal amputation of the right leg 3 years prior.PAD had not been diagnosed previously.
The right leg ABI was 0.37, and the left leg ABIwas 0.94. Arterial duplex suggested occlusive dis-
Tibial CTO
Reconstituted peroneal artery
Occluded anterior tibial artery
Occluded peroneal artery
Occluded posterior tibial artery
Dorsalis pedisartery
Anterior tibial artery
Posterior tibial artery
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 4
BardCCU_3-4.indd 4 5/10/12 4:47 PM

ease in the popliteal segment. Angiography showeddiffuse disease in the SFA with focal high-gradestenosis in the distal segment, occlusion of poplitealartery with reconstitution above the popliteal bifur-cation, and severe disease in the distal poplitealartery and the origins of ATA and tibioperoneal(TP) trunk with three-vessel runoff. The SFA wastreated with PTA using contralateral femoral accessat the time of diagnostic angiography.
For popliteal and below-the-knee intervention,ipsilateral antegrade femoral access was used with a6 Fr system. The CROSSER™ Catheter 14P (RX) sys-tem was used over a Grandslam wire, and the lesioncrossed in 36 seconds. PTA of the anterior tibial-dis-tal popliteal artery was carried out with a 3.0 x 80
5
Popliteal CTO Runoffs
Anterior tibial artery
Peroneal artery
Posterior tibial artery
Anterior tibial artery
Posterior tibial artery
Proximal occlusion point
Distal reconstitution
Tibioperoneal trunk
Anterior tibial artery
Popliteal artery
Anterior tibial artery
Posterior tibial artery
Peroneal artery
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 5
BardCCU_2-5.indd 5 5/10/12 4:47 PM

6
mm VASCUTRAK® PTA Dilatation Catheter at 3atmospheres of pressure for 3 minutes. PTA of thedistal popliteal artery-TP trunk was carried outwith a 4.0 x 80 mm VASCUTRAK® PTA DilatationCatheter at 3 atm pressure for 3 minutes. Proximalpopliteal-distal SFA was treated with a 5.0 X 150mm VASCUTRAK® PTA Dilatation Catheter at 5 atmpressure for 3 minutes. A stent-like result was achievedwith PTA alone with no dissection. Heparin was usedat 70 units/kg bodyweight for periprocedural anticoag-ulation and arteriotomy was closed with the Mynx clo-sure device. Dual antiplatelet therapy with acetyl sali-cylic acid and clopidogrel was prescribed.
References1. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA,
Fowkes FG, et al. Inter-Society Consensus for theManagement of Peripheral Arterial Disease (TASC II). J VascSurg. 2007;45(Suppl S):S5–S67.
2. Allie DE, Hebert CJ, Lirtzman MD, et al. Critical limbischemia: a global epidemic. A critical analysis of currenttreatment unmasks the clinical and economic costs of CLI.EuroIntervention. 2005;1:75–84.
3. Feinglass J, Pearce WH, Martin GJ, et al. Postoperative andlate survival outcomes after major amputation: Findings fromthe Department of Veterans Affairs National Surgical QualityImprovement Program. Surgery. 2001;130:21–29.
4. Dormandy J, Belcher G, Broos P, et al. Prospective study of713 below-knee amputations for ischaemia and ehte effect ofa prostacyclin analogue on healing. Br J Surg. 1994;81:33–37.
5. Izumi Y, Satterfield K, Lee S, Harkless LB. Risk of reamputationin diabetic patients stratified by limb and level of amputation: a10-year observation. Diabetes Care. 2006;29:566–570.
6. Rastogi S, Stavropoulos SW. Infrapopliteal angioplasty. TechVasc Interv Radiol. 2004;7:33–39.
7. Nanjundappa A, Laird Jr. Critical limb ischemia: understand-ing the scope of the problem. Endovasc Today. July 2006.Available at http://bmctoday.net/evtoday/2006/07/article.asp?f=EVT0706_03.htm
8. Treiman GS, Copland S, Yellin AE, et al. Wound infectionsinvolving infrainguinal autogenous vein grafts: a current eval-uation of factors determining successful graft preservation. JVasc Surg. 2001;33:948–954.
9. Dorros G, Jaff MR, Dorros AM, Mathiak LM, He T.Tibioperoneal (outflow lesion) angioplasty can be used as pri-mary treatment in 235 patients with critical limb ischemia:five-year follow-up. Circulation. 2001;104:2057–2062.
10.Adam DJ, Beard JD, Cleveland T, et al.; BASIL trial partici-pants. Bypass versus angioplasty in severe ischaemia of the leg(BASIL): multicentre, randomised controlled trial. Lancet.2005;366:1925–1934.
11.Cannon L, Patel S. Novel high-frequency vibration approachfor recanalization of difficult coronary and peripheral chron-ic total occlusion. Interv Cardiol. 2010;2:281–288.
12.Staniloae CS, Mody KP, Yadav SS, et al. Endoluminal treat-ment of peripheral chronic total occlusion using the Crosser®
recanalization device. J Invasive Cardiol. 2011;23:359–362.
This clinical case update was supported through an unrestricted educational grant from Bard Peripheral Vascular.
© HMP Communications, LLC • 83 General Warren Blvd • Suite 100 • Malvern, PA 19355 • 800-237-7285 www.hmpcommunications.com
BardCCU_0312-6PAGE-MOREBARDCHaNGES:CCU 5/10/12 4:42 PM Page 6
BardCCU_1-6.indd 6 5/10/12 4:46 PM