Embed Size (px)
Citation preview

Chronic obstructive pulmonary disease (COPD)
Professor Bill MacNee

Definition of COPD
COPD, a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases.
Exacerbations and comorbidities contribute to the overall severity in individual patients.
© 2014 Global Initiative for Chronic Obstructive Lung Disease

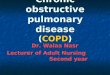
Emphysema
BronchiolitisSmall airways disease
ChronicBronchitis
Normal COPD
COUGH and SPUTUM
AIRWAYS OBSTRUCTION
BREATHLESSNESS

COPD:Quality Issues
• Diagnosis and assessment
• Therapy
• Reduction exacerbations

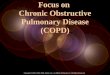
SYMPTOMScoughcough
sputumsputumshortness of breathshortness of breath
EXPOSURE TO RISKFACTORS
tobaccotobaccooccupationoccupation
indoor/outdoor pollutionindoor/outdoor pollution
SPIROMETRYSPIROMETRY
Diagnosis of COPD Diagnosis of COPD
èè èè èè
The diagnosis requires spirometry;
a post-bronchodilator FEV1/(FVC) <0.7
confirms the presence of airflow limitation
that is not fully reversible.
Fixed ratio FEV1/FVC <0.7 may over
diagnose COPD in elderly

Assessment of COPD
Assess symptoms
Assess degree of airflow limitation using spirometry
Assess risk of exacerbations
Assess comorbidities

Medical Research Council (MRC) Breathlessness Scale
Grade 1 2 3 4 5
Degree of breathless-ness related to activities
Not troubled by breathlessness except on strenuous exercise.
Short of breath when hurrying or walking up a slight hill.
Walks slower than contemporaries on level ground because of breathlessness or has to stop for breath when walking at own pace.
Stops for breath after walking about 100m or after a few minutes on level ground.
Too breathless to leave the house, or breathless when dressing or undressing.

• Patients read the two statements for each item, and decide where on the scale they fit
• Scores for each of the 8 items are summed to give single, final score (minimum 0, maximum 40)
• This is a measure of the overall impact of a patient’s condition on their life
1 Jones P et al. Eur Respir J 2009; 34: 648-654
COPD Assessment Test (CAT)

In patients with FEV1/FVC < 0.70:
Mild FEV1 > 80% predicted
Moderate 50% < FEV1 < 80% predicted
Severe 30% < FEV1 < 50% predicted
Very Severe FEV1 < 30% predicted
*Based on Post-Bronchodilator FEV1
Severity of Airflow LimitationSeverity of Airflow LimitationSeverity of COPDSeverity of COPD

Assess Risk of Exacerbations
To assess risk of exacerbations use history of exacerbations and spirometry:
Two or more exacerbations within the last year or an FEV1 < 50 % of predicted value are indicators of high risk.
One or more hospitalizations for COPD exacerbation should be considered high risk.
© 2014 Global Initiative for Chronic Obstructive Lung Disease

Assess COPD Comorbidities
COPD patients are at increased risk for:
• Cardiovascular diseases• Osteoporosis• Respiratory infections• Anxiety and Depression• Diabetes• Lung cancer• BronchiectasisThese comorbid conditions may influence
mortality and hospitalizations and should be looked for routinely, and treated appropriately.
© 2014 Global Initiative for Chronic Obstructive Lung Disease

Relieve symptoms Improve exercise tolerance Improve health status
Prevent disease progression Prevent and treat exacerbations Reduce mortality
Reducesymptoms
Reducerisk
Manage Stable COPD: Goals of Therapy
© 2014 Global Initiative for Chronic Obstructive Lung Disease

Therapeutic Options: COPD MedicationsBeta2-agonists
Short-acting beta2-agonists
Long-acting beta2-agonists
Anticholinergics
Short-acting anticholinergics
Long-acting anticholinergics
Combination short-acting beta2-agonists + anticholinergic in one inhaler
Combination long-acting beta2-agonists + anticholinergic in one inhalerMethylxanthines
Inhaled corticosteroids
Combination long-acting beta2-agonists + corticosteroids in one inhaler
Systemic corticosteroids
Phosphodiesterase-4 inhibitors© 2014 Global Initiative for Chronic Obstructive Lung Disease

Long-acting inhaled bronchodilators are convenient and more effective for symptom relief than short-acting bronchodilators.
Long-acting inhaled bronchodilators reduce exacerbations and related hospitalizations and
improve symptoms and health status.
Combining bronchodilators of different pharmacological classes may improve efficacy and decrease the risk of side effects compared to increasing the dose of a single bronchodilator.
Therapeutic Options: Bronchodilators

An inhaled corticosteroid combined with a long-acting beta2-agonist is more effective than the individual components in improving lung function and health status and reducing exacerbations in moderate to very severe COPD.
Inhaled corticosteroids are associated with an increased risk of pneumonia.
Addition of a long-acting beta2-agonist/inhaled glucorticosteroid combination to an anticholinergic (tiotropium) provides additional benefits.
Therapeutic Options: Combination Therapy

Chronic treatment with systemic corticosteroids should be avoided because of an unfavorable benefit-to-risk ratio.
Therapeutic Options: Systemic corticosteroids

Therapeutic Options: Theophylline
Theophylline is less effective and less well tolerated than inhaled long-acting bronchodilators.
There is evidence for a modest bronchodilator effect and some symptomatic benefit compared with placebo in stable COPD. Addition of theophylline to salmeterol produces a greater increase in FEV1 and breathlessness than salmeterol alone.
Low dose theophylline reduces exacerbations but does not improve post-bronchodilator lung function.

Influenza vaccines can reduce serious illness. Pneumococcal polysaccharide vaccine is recommended for COPD patients 65 years and older and for COPD patients younger than age 65 with an FEV1 < 40% predicted.
The use of antibiotics, other than for treating infectious exacerbations of COPD and other bacterial infections, is currently not indicated.
Therapeutic Options: Other Pharmacologic Treatments

NICE 2010-Inhaled therapies in COPD
SABA or SAMA as required*Breathlessness and exercise limitation
Exacerbations or persistent breathlessness
Persistent exacerbations or breathlessness
LABA LAMADiscontinue
SAMA________
Offer LAMA in preference to regular SAMA four times a
day
LABA + ICS in a combination
inhaler________
Consider LABA + LAMA if ICS
declined or not tolerated
LAMADiscontinue
SAMA________
Offer LAMA in preference to
regular SAMA four times a day
FEV1 ≥ 50% FEV1 < 50%
LABA + ICS in a combination
inhaler________
Consider LABA + LAMA if ICS
declined or not tolerated
LAMA + LABA + ICS in a combination
inhaler
Offer Consider* SABAs (as required) may continue at all stages

Combined Assessment of COPD
(C)
(A)
(D)
(B)
2 CAT < 10
2 CAT 10
Breathlessness
1
2
3
4
Ris
k(G
OLD
cla
ssifi
catio
n of
airf
low
lim
itatio
n)
Ris
k(E
xace
rba
tion
/ ye
ar)
mMRC 0 - 1
mMRC 2
Symptoms
≥ 2 or > 1 leading to hospital admission
1 (not leading to hospital admission)
0
© 2014 Global Initiative for Chronic Obstructive Lung Disease
ICS + LABAor
LAMA
ICS + LABAand/or LAMA
SAMA prnor
SABA prn
LABA or
LAMA
Recommended First Choice

InhalersBe sure to:• teach the technique and recheck• be familiar with different types of inhalers• change inhalers if a patient is having trouble coping with a certain type• encourage the use of spacer devices when needed.The correct delivery system is as important as the drug used.
Nebulisers• nebuliser assessments trials should be done by secondary care
respiratory physicians (this gives an added benefit to the patient of having the nebuliser maintained)
• consider a nebuliser if the patient has excessive or distressing shortness of breath despite maximum therapy.
• nebulised therapy should not continue to be prescribed without confirming improvement in one or more of the following:• a reduction in symptoms and/or• an increase in activities of daily living or exercise capacity.

PULMONARY REHABILITATION
Pulmonary rehabilitation benefits all patients with COPD, particularly those with severe to very severe COPD or an MRC breathlessness score of 3 or more.
All patients with repeated exacerbations or who are admitted to hospital with an exacerbation should be fast tracked for pulmonary rehabilitation.
Pulmonary rehabilitation:•improves exercise tolerance•improves the quality of life •reduces symptoms•reduces the number of exacerbations•reduces hospital admissions•available in all CHPs (In Edinburgh, CHP home-based rehabilitation is available).

Oxygen therapySBOT - short-burst oxygen therapyThere is no good evidence to support the use of short burst oxygen therapy.
LTOT - Long-term oxygen therapy
LTOT can prolong life. It is indicated in patients with hypoxaemia (PaO2 < 7.3 kPa) when in a stable condition. Secondary care assessment is required for the provision of long-term oxygen therapy.
Consider long-term oxygen therapy in patients with: • severe airflow obstruction (FEV1 < 40% predicted) • cyanosis • polycythemia• raised JVP or peripheral oedema • pulmonary hypertension • O2 saturation of < 92% while breathing air.
Patients who continue to smoke will rarely be considered for long-termoxygen therapy.
Consider ambulatory oxygen therapy in mobile patients on long-term oxygen therapy.

Impact on symptoms
and lungfunction
Negativeimpact on
quality of life
Consequences of COPD Exacerbations
Increasedeconomic
costs
Acceleratedlung function
decline
IncreasedMortality
EXACERBATIONS
© 2013 Global Initiative for Chronic Obstructive Lung Disease

Short-acting inhaled beta2-agonists with or without short-acting anticholinergics are usually the preferred bronchodilators for treatment of an exacerbation.
Systemic corticosteroids and antibiotics can shorten recovery time, improve lung function (FEV1) and arterial hypoxemia (PaO2), and reduce the risk of early relapse, treatment failure, and length of hospital stay.
A dose of 40 mg prednisone per day for 5 days is recommended .
Manage Exacerbations: Key Points
© 2014 Global Initiative for Chronic Obstructive Lung Disease

Antibiotics should be given to patients with:
Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence.
Two cardinal symptoms if one of which is increased sputum purulence. ventilation.
Manage Exacerbations: Treatment Options
© 2014 Global Initiative for Chronic Obstructive Lung Disease


CRT
SAS
LUCS/GP
respiratory physician
front door
RNS
smoking cessation
IMPACT
pulmonary rehab

Referral for Specialist Opinion
Consider referral if:• diagnosis is unclear• patient has severe COPD (FEV1 < 30% of
predicted)• cor pulmonale (fluid retention or peripheral
oedema)• increasing shortness of breath • rapidly decreasing FEV1• for assessment for O2 therapy if oxygen
saturation (92% or less) while breathing air• chest x-ray shows bullae in the lung• patient is less than 40years old• symptoms are disproportionate to pulmonary
function• patient has frequent infections/exacerbations• for assessment for nebuliser.