Embed Size (px)
Citation preview

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Chronic Lymphocytic Leukemia (CLL):
Diagnosis, Treatment, and Side Effects Management
• Describe the various types and subtypes of chronic lymphocytic
leukemia (CLL)
• Identify tests used to diagnose disease and monitor treatment of CLL
• Explain the overarching goals of treatment for the types of CLL
• Explain approved and emerging treatment options for CLL, including stem
cell transplantation, and the role of clinical trials.
• Describe strategies to manage treatment side effects as well as potential
long-term and late effects of treatments for CLL
• Describe the roles of the pharmacist, the nurse and the social worker in
treating patients with CLL
LEARNING OBJECTIVES
1
2

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
FACULTY
William G. Wierda, MD, PhDProfessor of Medicine
Section Head – CLL
Department of Leukemia
The University of Texas MD Anderson Cancer Center
Houston, TX
Deborah McCue, PharmD, BCOPClinical Pharmacy Manager
Division of Pharmacy
The University of Texas MD Anderson Cancer Center
Houston, TX
Jackie Broadway-Duren, DNP, APRN, FNP-BCFamily Nurse Practitioner
Department of Leukemia
The University of Texas MD Anderson Cancer Center
Houston, TX
Chronic Lymphocytic Leukemia
3
4

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
CLL/SLL: Background
▪ More than 20,000 estimated new cases in 2019 in the United States alone[1]
‒ Most common type of leukemia in adults (37%)
▪ Median age at diagnosis: 70 yrs[2]
▪ SLL and CLL considered the same B-cell malignancy[3]
‒ CLL: > 5000 clonal lymphocytes in peripheral blood
‒ SLL: presence of lymphadenopathy and/or splenomegaly and < 5000 clonal lymphocytes in peripheral blood
▪ Historical 5-yr survival: 66% (range: few mos to normal life span)[4]
‒ Current (2009-2015) 5-yr survival: 85%[2]
SLL, small lymphocytic lymphoma1. Siegel. CA Cancer J Clin. 2019;69:7. 2. SEER Cancer Stat Facts. Chronic lymphocytic leukemia.3. American Cancer Society. Chronic lymphocytic leukemia. 4. Nabhan. JAMA. 2014;312:2265.
CLL: Prognostic Value of FISHFISH Abnormalities Present in 268/325 Patients (82%)
Lesion % Median OS, Mos
del(13q) 55 133
del(11q) 18 79
Trisomy 12 16 114
del(17p) 7 32
del(6q) 6 N/A
Normal 18 111
Dohner. NEJM. 2000;343:1910. Dohner. Leukemia. 1997;11(suppl 2):S19. Oscier. Haematologica. 1999;84(suppl EHA-4):88. Jarosova. Onkologie. 2001;24:60. Dewald. Br J Haematol. 2003;121:287. Sindelárová. Cancer Genet Cytogenet. 2005;160:27.
Probability of OS From Diagnosis, by Genetic Aberration
100
80
60
40
20
0
Pat
ien
ts S
urv
ivin
g (%
)
Mos
17p deletion11q deletion12q trisomyNormal13q deletion as sole abnormality
FISH Lesion
Patients With Abnormality (%)
Dohner et al 1997
Oscier et al 1999
Jarosova et al 2001
Dewald et al 2003
Sindelarava et al 2005
del(13q) 45 36 18 47 54
Trisomy 12 15 15 13 25 16
del(17p) 10 8 11 8 16
del(11q) 20 17 11 15 12
FISH, fluorescence in situ hybridization; OS, overall survival
5
6

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
▪ OS effect of TP53 wild type:
‒ vs TP53 mut only: P = .013
‒ vs TP53 del only: P = .006
‒ vs TP53 mut + del: P < .001
▪ Analysis based on cases referred to the Munich Leukemia Laboratory between August 2005 and May 2013
CLL: Impact of TP53 Mutations and TP53 Deletion on OS (N = 1148)
Stengel. Leukemia. 2017;31:705.
9
8
7
6
5
4
3
2
1
0
Freq
uen
cy o
f TP
53
Alt
erat
ion
s in
Rel
atio
n t
o
Tota
l Siz
e o
f Ea
ch C
oh
ort
(%
)
CLL
TP53 mut onlyTP53 del onlyTP53 mut + del
Yrs
100
OS
(%)
80
60
40
20
0
TP53 wt
TP53alteration
P < .001
100 1 2 3 4 5 6 7 8 9Yrs
100
OS
(%)
80
60
40
20
0
TP53 wt
TP53 mut only
100 1 2 3 4 5 6 7 8 9
TP53 del only
TP53 mut + del
Survival in CLL According to IGHV Mutational Status
Surv
ivin
g (%
)
Su
rviv
ing
(%
)
P = .0008
All Patients (n = 84) Binet Stage* A Patients (n = 62)
P = .001
Mutated
UnmutatedUnmutated
Mutated
Mos0 50 100 150 200 250 300
0
20
40
60
80
100
Mos0 50 100 150 200 250 300
0
20
40
60
80
100
IGHV, immunoglobulin heavy chain variable regionHamblin. Blood. 1999;94:1848.
*See Staging Systems slide in Appendix
7
8

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Hallek et al Blood 2008;111:5446-5456
IWCLL-NCI: Indications to
Initiate Treatment for CLL• Constitutional symptoms referable to CLL
• Progressive marrow failure
• Autoimmune anemia +/- thrombocytopenia poorly responsive to steroids or other
• Massive (>6 cm) or progressive splenomegaly
• Massive (>10 cm) or progressive lymphadenopathy
• Progressive lymphocytosis, >50% increase over 2 months or LDT < 6 months
• NO EARLY TREATMENT, EVEN FOR HIGH-RISK
IWCLL-NCI, International Workshop on Chronic Lymphocytic Leukemia- National Cancer Institute; LDT, lymphocyte doubling time
Treatment Goals for CLL
• Potentially curative treatments: FCR for m-IGHV and allo-HCT
• Majority requiring treatment are older (>70 yo) with
comorbidities and more treatment-associated toxicities
• Goals for first-line:
Best opportunity for most effective treatment, most
eventually relapse and need retreatment:
– Deeper remission and treatment-free interval, later retreat
– Maintain disease control on continuous (IBR) treatment
Allo-HCT, allogeneic hematopoietic stem cell transplant; FCR, fludarabine, cyclophosphamide, and rituximab; IBR, ibrutinib
9
10

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Essential Tests for Selecting First-Line Treatment in CLL
1. FISH: del(17p) status – can change
– Know % of cells with deletion
2. TP53 mutation status – can change
3. IGHV mutation status – does not change
FISH, fluorescence in situ hybridization
Therapeutic Agents for CLL
Chemotherapy
CD20
Antibody BTK-inhibitor
PI3 kinase-
inhibitor
BCL2-
inhibitor Others
Chlorambucil
(Leukeran)
Rituximab
(Rituxan)
Ibrutinib
(Imbruvica)
Idelalisib
(Zydelig)
Venetoclax
(Venclexta)
Lenalidomide
(Revlimid)
Fludarabine
(Fludara)
Ofatumumab
(Arzerra)
Acalabrutinib
(Calquence)
Duvelisib
(Copiktra)CAR T cells
Cyclophosphamide
(Cytoxan)
Obinutuzumab
(Gazyva™)
Zanubrutinib
(Brukinsa™)Umbralisib
Bendamustine
(Treanda)Vecabrutinib
ARQ 531
LOXO-305
CG-806
(Aptose)
11
12

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
First-Line Phase III Randomized Trials
• RESONATE-2
– IBR vs.
– CHLOR
• iLLUMINATE (PCYC-1130) (>65 yo or ≤65 yo with comorbidities)
– IBR + OBIN vs.
– CHLOR + OBIN
• Alliance (A041202) (>65 yo)
– IBR vs.
– IBR + RIT vs.
– BR
• ECOG E1912 [<70 yo; non-del(17p)]
– IBR + RIT vs.
– FCR
• CLL14 (CIRS >6; CrCl <70 mL/min)
– VEN + OBIN vs.
– CHLOR + OBIN
IBR, ibrutinib (Imbruvica); CHLOR, chlorambucil (Leukeran); OBIN, obinutuzumab (Gazyva™); RIT, rituximab (Rituxan) ; BR, bendamustine (Treanda) and rituximab (Rituxan); FCR, fludarabine (Fludara), cyclophosphamide (Cytoxan), and rituximab (Rituxan); VEN, venetoclax (Venclexta)
iLLUMINATE (PCYC-1130) Study Design
Primary end point• PFS by IRC assessment
Secondary end points include• PFS by IRC in high-risk population• Rate of undetectable MRD• ORR
• OS• Infusion-related reactions• Safety
Patients (N=229)• Previously untreated CLL/SLL • Requiring treatment per
iwCLL criteria • Age ≥65 years or <65 years
old with ≥1 coexisting condition:▪ CIRS >6▪ CrCl <70 mL/min▪ del(17p) or TP53
mutation
aPatients in the chlorambucil-obinutuzumab arm could receive next-line single-agent ibrutinib in crossover following IRC-confirmed PD.
R
A
N
D
O
M
I
Z
E
1:1
Ibrutinib – obinutuzumabIbrutinib 420 mg once daily until PD or unacceptable
toxicity + obinutuzumab1000 mg split on days 1-2, and on day 8 and 15 (cycle 1)
then day 1 (total 6 cycles)
Chlorambucil–obinutuzumabChlorambucil 0.5 mg/kg on days 1 and 15
(6 cycles) + obinutuzumab 1000 mg split on days 1-2 and on day 8 and 15 (cycle 1) then
day 1 (total 6 cycles)
After IRC-confirmed PD, patients were allowed to receive
single-agent ibrutiniba
Stratification: del(17p) vs. del(11q) vs. neither del(17p) or del(11q); ECOG 2 vs 0-1
Moreno et al. ASH 2018. Abstract 691.
Ibrutinib, (Imbruvica); obinutuzumab, (Gazyva™)CIRS, Cumulative Illness Rating Scale; IRC, independent review committee; iwCLL, International Working Group on CLL; MRD, minimal residual disease; ORR, overall response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival
13
14

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Superior Progression-Free Survival With Ibrutinib (Imbruvica) -Obinutuzumab (Gazvya™)
Ibrutinib, (Imbruvica); Obinutuzumab, (Gazyva™); Chlorambucil, (Leukeran)INV, investigator; NR, not reached
Independent Review Assessment Investigator Assessment
▪ Median follow-up, 31.3 months (range, 0.2–36.9)▪ Estimated PFS at 30 months: 79% with ibrutinib-obinutuzumab vs. 31% with chlorambucil-obinutuzumab▪ Even after excluding patients with del(17p): 74% reduction in risk of progression or death with ibrutinib-obinutuzumab
Moreno et al. ASH 2018. Abstract 691.
Alliance (A041202) Schema
Stratify*
Documented progression
RANDOMIZE
Bendamustine (Treanda) 90 mg/m2 days 1 and 2 of each 28-day cycle +Rituximab (Rituxan) 375 mg/m2 day 0 cycle 1,then 500 mg/m2 day 1 cycles 2-6
Ibrutinib (Imbruvica)420 mg daily until disease progression
Stratification• High risk vs intermediate risk Rai stage*• Presence vs absence of del(11q22.3) or del(17p13.1) on FISH performed locally• <20% vs ≥20% Zap-70 methylation of CpG 3 performed centrally
P
R
E
-
R
E
G
I
S
T
E
R
Ibrutinib (Imbruvica) 420 mg daily until disease progression +Rituximab (Rituxan) 375 mg/m2 weekly for 4 weeks starting cycle 2 day 1, then day 1 of cycles 3-6
Untreated patients age ≥65 who meet IWCLL criteria for CLL treatment
Woyach et al. ASH 2018. Abstract 6.
*See Staging Systems slide in Appendix
15
16

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Primary Endpoint: Progression-Free SurvivalEligible Patient Population
Arm C (IR)Arm B (I)
Arm A (BR)
% A
live a
nd
Pro
gre
ssio
n-F
ree
0 6 12 18 24 30 36 42 48 52
Time (Months)
0
10
20
30
40
50
60
70
80
90
100
0 6 12 18 24 30 36 42 48 52
Time (Months)
0
10
20
30
40
50
60
70
80
90
100
Censor
32/170Arm C (IR)
34/178Arm B (I)
68/176Arm A (BR)
Events/TotalArm
Patients-at-Risk176 140 129 122 103 88 57 26 11 0178 165 154 147 136 120 78 45 22 0170 159 145 138 132 115 74 40 20 0
Pairwise Comparisons
I vs BR:Hazard Ratio 0.39 95% CI: 0.26-0.58
(1-sided P-value <0.001)
IR vs BR: Hazard Ratio 0.38 95% CI: 0.25-0.59
(1-sided P-value <0.001)
IR vs I: Hazard Ratio 1.00 95% CI: 0.62-1.62
(1-sided P-value 0.49)
Arm N 24-Month Estimate
BR 176 74% (95% CI: 66-80%)
I 178 87% (95% CI: 81-92%)
IR 170 88% (95% CI: 81-92%)
I , ibrutinib (Imbruvica); BR, bendamustine (Treanda) and rituximab (Rituxan); IR, ibrutinib (Imbruvica)
Woyach et al. ASH 2018. Abstract 6.
E1912: Study DesignArm A – Ibrutinib + RituximabCycles 1: Ibrutinib 420 mg PO daily, days 1-28
Cycle 2:Ibrutinib 420 mg PO daily, days 1-28 Rituximab 50 mg/m2 IV, day 1Rituximab 325 mg/m2 IV, day 2
Cycles 3-7: Ibrutinib 420 mg PO daily, days 1-28 Rituximab 500 mg/m2 IV, day 1
Arm B - FCRCycles 1-6:Fludarabine 25 mg/m2 IV, days 1-3Cyclophosphamide 250 mg/m2 IV, days 1-3
Cycle 1:Rituximab 50 mg/m2 IV, day 1, cycle 1Rituximab 325 mg/m2 IV, day 2, cycle 1
Cycle 2-6:Rituximab 500 mg/m2 IV, day 1, cycles 2-6
Cycle 8 until progression: Ibrutinib 420 mg PO daily, days 1-28
Planned Accrual: 519
E1912Eligibility:-Previously untreated CLL -Requires treatment (IWCLL 2008)-Age ≤70-ECOG 0-2-CrCL >40 -Able to tolerate FCR-No deletion 17p by FISH
Ran
do
miz
atio
n
Dis
ease
Pro
gres
sio
n
Shanafelt et al. ASH 2018. Abstract LBA-4.Fludarabine, (Fludara); Ibrutinib (Imbruvica); Rituximab (Rituxan)
17
18

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Progression-Free SurvivalIntent to Treat Eligible
HR = 0.35 (95% CI 0.22-0.5)One sided p<0.00001
HR = 0.32 (95% CI 0.20-0.51)One sided p<0.00001
Shanafelt et al. ASH 2018. Abstract LBA-4.
Overall Survival
Intent to Treat Eligible
0 1 2 3 4
0.0
0.2
0.4
0.6
0.8
1.0
Years
Pro
ba
bili
ty
IR (4 events/ 354 cases)
FCR (10 events/ 175 cases)
Number at risk
354 347 318 166 18
175 155 130 58 1
HR = 0.17 (95% CI 0.05−0.54)
One−sided p = 3.22 ´ 10-4
0 1 2 3 4
0.0
0.2
0.4
0.6
0.8
1.0
Years
Pro
ba
bili
ty
IR (3 events/ 332 cases)
FCR (10 events/ 166 cases)
Number at risk
332 327 298 154 18
166 149 125 54 1
HR = 0.13 (95% CI 0.03−0.46)
One−sided p = 9.86 ´ 10-5
HR = 0.17 (95% CI 0.05-0.54)One sided p<0.0003
HR = 0.13 (95% CI 0.03-0.46)One sided p<0.0001
Shanafelt et al. ASH 2018. Abstract LBA-4.
19
20

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Causes of Death
Cause of DeathIR
n=354FCR
n=175CLL 1 6
Unexplained/unwitnessed 1 2
Other: acute/chronic respiratory failure; hx lung adenocarcinoma
1 0
Acute respiratory failure 1 0
Metastatic colon cancer 0 1
Drug overdose 0 1
TOTAL 4 10
Death during active treatment +30 days: IR (n=3); FCR (n=1)
Shanafelt et al. ASH 2018. Abstract LBA-4.
T-MDS/AML AFTER FCR
N Treatment T-MDS/AML %
MDACC 2004-2012234
131
FCR-based
FCR only
5.1
0.7
MDACC 1999-2003 300 FCR 4.6
German CLL8 408 FCR 1.5
MDACC, MD Anderson Cancer Center; T-MDS, therapy-related myelodysplastic syndrome; T-AML: therapy related acute myeloid leukemiaJohn Benjamini. Leuk Lymphoma. 2015; Thompson. Blood. 2016; Fischer. Blood. 2016.
21
22

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Fischer, ASCO 2019 (Abstract 7502)
Safety Run-in Phase*
Venetoclax (Venclexta) –
Obinutuzumab
(Gazyva™)
Previously untreated
patients with CLL and
coexisting medical
conditions
CIRS >6 and/or
CrCl <70 mL/min
*Fischer K et al. Blood. 2017;129:2702-2705.
Chlorambucil
(Cytoxan) –
Obinutuzumab
(Gazyva™)
6 cycles
Venetoclax (Venclexta)
– Obinutuzumab
(Gazyva™)
6 cycles
Venetoclax
(Venclexta)
6 cycles
Obinutuzumab
(Gazyva™)
6 cycles
Follow-up Phase
Primary endpoint:
Progression-free survival
Key secondary endpoints:
Response, Minimal
Residual Disease, Overall
Survival
1:1
randomization
CLL14: TRIAL DESIGN
Fischer, ASCO 2019 (Abstract 7502)
100
Patients
with r
esponse (
%)
Chlorambucil-
Obinutuzumab
Venetoclax-
Obinutuzumab
50%
35%
23%
48%
Overall response
P = 0.0007
Complete response
P<0.0001
Partial response
CLL14: RESPONSE TO TREATMENT
0
10
20
30
40
50
60
70
80
90
(Venclexta-
Gazyva™)
(Leukeran-
Gazyva™)
23
24

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Fischer, ASCO 2019 (Abstract 7502)
0
Investigato
r-assesse
d
Pro
gre
ssio
n-f
ree s
urv
ival (%
)10
0
80
60
40
20
00
Time on study in months
Hazard ratio 0.35 (95% CI 0.23‒0.53), P<0.0001
29-months median follow-up
6 12 18 24 30 36
Venetoclax–
Obinutuzumab
Chlorambucil–
Obinutuzumab
CLL14: PROGRESSION-FREE SURVIVAL
(Venclexta-
Gazyva™)
(Leukeran-
Gazyva™)
FCR300: PFS by IGHV Mutation Status (IGHV-MS)
Thompson PA, et al. Blood 2016; 127:303–309.
P<0.0001Perc
en
tag
e P
rog
ressio
n-f
ree
Time (Years)
0
25
50
75
100
0 1 2 3 4 8 9 105 6 7 11 12 13 14 15 16
N Prog-free
IGHV mutated 88 49
IGHV unmutated 126 12
25
26

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
CLL10 Study: FCR vs BR in Front-LineProgression-free survival by IGHV-MS
MS, mutation status.Eichhorst et al. Lancet Oncol. 2016;17:928-942.
IGHV-M
FCR
IGHV-M
BR
FCR First-Line: 6-Month Landmark PFS by MRD at EoT and IGHV-MS
0 6 1 2 1 8 2 4 3 0 3 6 4 2 4 8 5 4 6 0 6 6 7 2 7 8 8 4 9 00
2 5
5 0
7 5
1 0 0
T im e (M o n th s )
Pe
rc
en
t p
ro
gre
ss
ion
-fre
e
IG H V -U M , M R D -p o s
IG H V -U M , M R D -n e g
IG H V -M , M R D -p o s
IG H V -M , M R D -n e g
N P ro g - fre e
4 5 4 1
2 9 2 0
6 4 2 3
4 3 3 1
p = 0 .0 2
Thompson PA et al. Leukemia. 2018;32:2388-2398.
IGHV-M
61% uMRD
EoT, end of treatment U-MRD, undetectable minimal residual disease
27
28

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Fischer, ASCO 2019 (Abstract 7502)
0
Inve
stig
ato
r-a
ssesse
d
Pro
gre
ssio
n-f
ree s
urv
ival (
%)
100
80
60
40
20
00
Time on study in months
6 12 18 24 30 36
CLL14: PFS BY IGHV MUTATIONAL STATUS
Venetoclax–Obinutuzumab
IGHV unmutated
Chlorambucil–Obinutuzumab
IGHV unmutated
Venetoclax–
Obinutuzumab
IGHV mutated
Chlorambucil–Obinutuzumab
IGHV mutated
Chlorambucil, (Leukeran); Obinutuzuman, (Gazyva™); Venetolclax, Venclexta
Fischer et al , N Engl J Med 2019; 380:2225-2236- Supplemental Appendix
CR, complete remission; ASO-PCR, allele-specific oligonucleotide polymerase chain reaction; Clb, chlorambucil; G, obinutuzumab; MRD, minimal residual disease negative; Ven, venetoclax.Data cutoff: August 17, 2018.
Deeper response rates (MRD negativity and CR) were significantly higher with VenG vs GClb in patients with mutated IGHV.
SubgroupsTotal
NVenG GClb Odds
Ratio 95% CIn MRD– (%) n MRD– (%)
All patients 432 216 75.5 216 35.2 5.67 3.74–8.60
Mutated IGHV 159 76 73.7 83 43.4 3.66 1.87–7.15
Subgroup Analysis for Undetectable PB MRD Rate (ASO-PCR)1
SubgroupsTotal
NVenG GClb Odds
Ratio 95% CIn CR (%) n CR (%)
All patients 432 216 49.5 216 23.1 3.26 2.15–4.93Mutated IGHV 159 76 51.3 83 34.9 1.96 1.04–3.71
Subgroup Analysis for Complete Response Rate2
CLL14: Subgroup Analysis for Mutated IGHVby MRD Negativity and by CR Rates
1. Fischer K et al. N Engl J Med. 2019;380:2225-2236. 2. Data on File.
29
30

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
First-Line Treatment for CLL
TP53 Status [del(17p)/TP53]
Age/Fitness IGHV-MS First-Line Treatment
Deleted and/or Mutated
All IrrelevantBTKi ±Obinutuzumab(Gazyva™)
Intact
Young/FitMutated
BCL2i + Obinutuzumab(Gazyva™)
Unmutated
Older/Unfit
Mutated
UnmutatedBTKi ±Obinutuzumab(Gazyva™)
BTKi, Bruton’s tyrosine kinase inhibitor; BCL2i, BCL-2 inhibitor
• Investigator-initiated phase II trial
• Ibrutinib (Imbruvica) monotherapy – 3 months
• Ibrutinib (Imbruvica) + venetoclax (Venclexta) – 24 months
• Option to continue ibrutinib (Imbruvica) if <CR or MRD+
• Tx-naive with at least 1 high-risk feature:
• Del(17p) or mutated TP53
• Del(11q)
• Unmutated IGHV
• Age ≥65 yrs
Ibrutinib (Imbruvica) + Venetoclax (Venclexta)
IBR + VEN in TN CLL. ASH 2018. Abstract 186.
31
32

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Responses Improve With Ongoing Therapy
n=75 n=72 n=70 n=60 n=33 n=26
96
43
2717
124
1
57
7383 88
96
017
4052
6169
0
10
20
30
40
50
60
70
80
90
100
PR% CR/CRi % BM U-MRD4 %3 mo IBR 3 mo VEN+IBR 6 mo VEN+IBR 9 mo VEN+IBR 12 mo VEN + IBR 18 mo VEN + IBR
IBR + VEN in TN CLL. ASH 2018. Abstract 186.
Cri, complete response with incomplete blood count recovery; PR: partial response
Wierda et al. ASCO 2018;Abstract 7502.
Phase 2 CAPTIVATE Study Design (NCT02910583)
Patients (N=164)Key eligibility:• Treatment-naïve CLL/SLL• Active disease requiring
treatment per iwCLL criteria• Age <70 years• ECOG PS 0‒1
Randomizationb
Confirmed undetectable MRDc
Double-blind 1:1 randomization,
placebo:ibrutinib (Imbruvica)
Undetectable MRD not confirmed1:1 randomization,
ibrutinib: I+V(Imbruvica)
Study Populations:▪ MRD cohort (N=164): exposure and safety analysis
– Safety Run-in: first 14 patients completed C15 treatment (12 cycles of I+V); no dose-limiting toxicities (DLT) or clinical TLS during first 6 weeks of I+V combination
– First 30 patients completed C9 treatment (6 cycles of I+V) for MRD evaluation
▪ Fixed duration cohort (N=159): separate cohort; analysis not shown
a1 cycle = 28 days.bStratified by IGHV mutation status. cConfirmed undetectable MRD for randomization defined as undetectable MRD serially over at least 3 cycles in peripheral blood (PB), and undetectable MRD in both PB and BM.
Ibrutinib (Imbruvica) lead-In:ibrutinib (Imbruvica)420 mg
once daily for 3 cyclesa
Followed by I+V:Add venetoclax (Venclexta)
ramp-up to400 mg once daily for
12 cycles
33
34

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Bruton Tyrosine Kinase (BTK) Inhibitors
BTK Inhibitors – Dosing
Ibrutinib(Imbruvica)
Acalabrutinib*
(Calquence)
FDA Approval Date November 2013 October 2017 for mantle cell lymphoma (MCL)
Usual Starting Dose 420 mg PO once dailyTake with a glass of water with or without food
100 mg PO BIDTake with water with or without food
Dose in Hepatic Dysfunction Child-Pugh A: 140 mg PO dailyChild-Pugh B: 70 mg PO dailyChild-Pugh C: Avoid use
Child-Pugh A & B: No recommended dose reductionsChild-Pugh C: Not studied
Availability Capsules: 70 mg, 140 mgTablets: 140 mg, 280 mg, 420 mg, 560 mg (MCL)
Capsules: 100 mg
1. Imbruvica [ibrutinib (prescribing information)]. Sunnyvale, CA: Pharmacyclics LLC; 2019. 2. Calquence [acalabrutinib (prescribing information)]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2017.
*Acalabrutinib approved for CLL/SLL in sNDA on 11-22-19
35
36

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
BTK Inhibitors – Drug InteractionsIbrutinib(Imbruvica)
Acalabrutinib(Calquence)
Substrate of CYP3A CYP3A, P-gp, BCRP
Effects on enzymes/transporters
Not a clinically significant inhibitor or inducer Not a clinically significant inhibitor or inducerMay inhibit BCRP transporter
Dosing Recommendations with Restricted Concomitant Medications
Moderate CYP3A inh. – 280 mg dailyStrong CYP3A Inhibitors:Voriconazole (Vfend )/Posaconazole(Noxafil) susp. ≤400 mg/day – 140 mg dailyPosaconazole (Noxafil) tabs or IV (any dose) or susp. >400 mg/day – 70 mg daily
Moderate CYP3A inh. – 100 mg dailyStrong CYP3A inh. – avoid use or interrupt acalabrutinib (Calquence) if short duration Strong CYP3A inducer – avoid use. If cannot avoid, increase to 200 mg BIDH2-blockers – take acalabrutinib (Calquence) dose 2 hours prior to H2-blocker Short-acting antacids – separate doses by at least 2 hours
Avoid concomitant use with: Any other strong CYP3A inhibitorsStrong CYP3A inducersGrapefruit and Seville oranges
Proton pump inhibitorsGrapefruit and Seville oranges
CYP, cytochrome p450; P-gp, P glycoprotein; BCRP:, breast cancer resistance protein.1. Imbruvica [ibrutinib (prescribing information)]. Sunnyvale, CA: Pharmacyclics LLC; 2019. 2. Calquence [acalabrutinib (prescribing information)]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2017.
BTK Inhibitors – Warnings Ibrutinib(Imbruvica)
Acalabrutinib(Calquence)
Cardiac Arrhythmias Atrial fibrillation: 4%Rare ventricular arrhythmiasCaution in patients with cardiac historyObtain an EKG in symptomatic patients
Atrial fibrillation: 3%Obtain an EKG in symptomatic patients
Cytopenias Grade 3 and 4 events can occurMonitor blood counts monthly
Grade 3 and 4 events can occurMonitor blood counts monthly
Hemorrhage Major bleeding: 4%; all grades: 39%Concomitant anticoagulants increase riskConsider holding ibrutinib at least 3-7 days prior to and postsurgical procedures depending on risks of surgery, bleeding, and ibrutinib interruption
Major bleeding: 2%; all grades: 50%Concomitant anticoagulants increases riskConsider holding acalabrutinib at least 3-7 days prior to and postsurgical procedures depending on surgery and bleeding risks
EKG, electrocardiogram.1. Imbruvica [ibrutinib (prescribing information)]. Sunnyvale, CA: Pharmacyclics LLC; 2019. 2. Calquence [acalabrutinib (prescribing information)]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2017. 3. NCCN Clinical Practice Guidelines in Oncology for CLL/SLL V 1.2020.
37
38

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
BTK Inhibitors – Warnings* Ibrutinib(Imbruvica)
Acalabrutinib(Calquence)
Infections Grade 3 or greater: 24% Cases of progressive multifocal leukoencephalopathy (PML), hepatitis B reactivation, invasive fungal infections & Pneumocystis jirovecii pneumonia (PJP)
Grade 3 or greater: 18%Cases of PML, hepatitis B reactivation, and invasive fungal infections have been reported
SecondaryMalignancies
10% occurrence rateMost common – non-melanoma skin cancers
11% occurrence rateMost common – non-melanoma skin cancers
Hypertension Any grade: 12%Grade 3 or greater: 5%Monitor blood pressure periodically
Not listed as a warning
Tumor lysis syndrome
Rarely occurs Not listed as a warning
1. Imbruvica [ibrutinib (prescribing information)]. Sunnyvale, CA: Pharmacyclics LLC; 2019. 2. Calquence [acalabrutinib] (prescribing information)]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2017. 3. NCCN Clinical Practice Guidelines in Oncology for CLL/SLL V 1.2020.
*Embryo-Fetal Toxicity: Based on findings in animals, BTK Inhibitors can cause fetal harm when administered to a pregnant woman. Advise women to avoid becoming pregnant and to use contraception. See Full PI for each drug for more specifics
BTK Inhibitors – Other Common Side EffectsNon-lab events occurring in ≥20% of patients in Ibrutinib (Imbruvica) clinical trials
• Rash
• Musculoskeletal pain
• Fatigue
• Pyrexia
• Cough
• Diarrhea
• Nausea
Non-lab events occurring in ≥20% of patients in Acalabrutinib (Calquence) clinical trials
• Headache• Occurs early and typically resolves with
continued therapy
• Fatigue
• Myalgia
• Diarrhea
• Bruising
1. Imbruvica [Ibrutinib (prescribing information)]. Sunnyvale, CA: Pharmacyclics LLC; 2019. 2. Calquence [acalabrutinib (prescribing information)]. Wilmington, DE: AstraZeneca Pharmaceuticals LP; 2017.
• Advise patients about the possibility of lymphocytosis after initiating treatment• Occurs within the first month of therapy and can persist for several weeks. Not progression!
39
40

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Venetoclax(Venclexta)
Venetoclax (Venclexta) Dosing
• Inhibits the B-cell lymphoma 2 (BCL2) protein, which is overexpressed in CLL leading to prolonged cell survival
• Inhibition of BCL2 by venetoclax (Venclexta) restores apoptosis
• CLL dosing (requires a ramp-up at initiation):• Each dose should be taken with a meal and water• Week 1: 20 mg PO daily x 7 days• Week 2: 50 mg PO daily x 7 days• Week 3: 100 mg PO daily x 7 days• Week 4: 200 mg PO daily x 7 days• Week 5 and thereafter: 400 mg PO daily, continuously
• Dosing in hepatic impairment:• Child-Pugh C: Decrease dose by 50%
• See prescribing information for modifications for toxicity
• Availability:• Tablets: 10 mg, 50 mg, 100 mg
Venclexta [venetoclax (prescribing information)]. North Chicago, IL: AbbVie Inc; 2019.
41
42

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Venetoclax (Venclexta) Drug Interactions
• Substrate of CYP3A, P-gp; inhibitor of P-gp and BCRP; weak inhibitor of CYP2C9 (may affect warfarin)
• Dosing recommendations for specific concomitant medications:• Concomitant strong or moderate CYP3A inhibitors and P-gp inhibitors are
contraindicated during ramp-up or require a venetoclax (Venclexta) dose reduction
• Concomitant posaconazole – 70 mg PO daily (82.5% reduction)• Other strong CYP3A inhibitor – 100 mg PO daily (75% reduction)• Moderate CYP3A inhibitor or P-gp inhibitor – 200 mg PO daily (50% reduction)• P-gp substrate – administer at least 6 hours before venetoclax (Venclexta) dose
• Advise patient to avoid grapefruit, Seville orange, and starfruit consumption while taking venetoclax (Venclexta)
Venclexta [venetoclax (prescribing information)]. North Chicago, IL: AbbVie Inc.; 2019.
Venetoclax (Venclexta) Warnings
• Tumor lysis syndrome (TLS)• Fatal and serious TLS events have occurred in patients with high tumor burden (rate 2% after ramp-
up schedule/aggressive prophylaxis instituted)• See prescribing information for risk assessment and TLS prophylaxis guidance based on risk
• Neutropenia• Grade 3 or 4 neutropenia occurred in approximately 63% of patients in clinical trials• Monitor counts periodically during therapy
• Infections• Fatal and serious infections have occurred
• Embryo-Fetal Toxicity• May cause embryo-fetal harm when administered to a pregnant woman. Advise females of
reproductive potential to avoid pregnancy during treatment
• Immunization• Do not administer live attenuated vaccines prior to, during, or after treatment until B-cell recovery
occurs. Advise patients that vaccinations may be less effective.
Venclexta [venetoclax (prescribing information)]. North Chicago, IL: AbbVie Inc.; 2019.
43
44

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Venetoclax (Venclexta): Other Common Side Effects
• Events (non-lab) occurring in 20% or greater of patients in clinical trials
• Edema• Upper respiratory tract infections• Musculoskeletal pain• Fatigue• Cough• Diarrhea• Nausea
• Venetoclax (Venclexta): does not cause lymphocytosis compared to some of the other oral agents being discussed
Venclexta [venetoclax (prescribing information)]. North Chicago, IL: AbbVie Inc.; 2019.
Chemoimmunotherapy
45
46

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Anti-CD20 Monoclonal Antibodies• Three anti-CD20 monoclonal antibodies currently on the market:
• Rituximab [Rituxan (IV)] and rituximab (Rituxan)/hyaluronidase (SQ) (chimeric)• Ofatumumab [Arzerra (human)]• Obinutuzumab [Gazyva™ (humanized)]
• Toxicities profiles are fairly similar:• Infusion-related reactions (follow premedication recommendations)• Injection site reactions (SQ)• Tumor lysis syndrome• Mucocutaneous reactions (rituximab)• Cytopenias• Risk of infections (eg, hepatitis B reactivation, PML)
• Add minimal overlapping toxicity when combined with other agents, such as chemotherapy or oral targeted agents
• Based on human data, RITUXAN can cause fetal harm due to B-cell lymphocytopenia in infants exposed to rituximab in-utero. Advise pregnant women of the risk to a fetus. Females of childbearing potential should use effective contraception while receiving RITUXAN and for 12 months following the last dose of RITUXAN
• ARZERRA (ofatumumab) may cause fetal B-cell depletion based on findings from animal studies and the drug’s mechanism of action There are no data on ARZERRA use in pregnant women to inform a drug-associated risk. See full PI.
• GAZYVA™ is likely to cause fetal B-cell depletion based on findings from animal studies and the drug’s mechanism of action There are no data with GAZYVA™ use in pregnant women to inform a drug-associated risk. See full PI.
1. Rituxan [rituximab (prescribing information)]. South San Francisco, CA: Genentech; 2019.2. Rituxan Hycela [(Rituxan)/hyaluronidase (SQ) (chimeric) (prescribing information)]. South San Francisco, CA: Genentech; 2018.3. Arzerra [ofatumumab (prescribing information)]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2016.4. Gazyva™ [obinutuzumab (prescribing information)]. South San Francisco, CA: Genentech; 2017.
Chemoimmunotherapy
• Chemoimmunotherapy = Anti-CD20 monoclonal antibody + alkylating agent +/-purine nucleoside analog
• Alkylating agents – bendamustine (Treanda), cyclophosphamide (Cytoxan), chlorambucil (Leukeran)
• Purine analogs – fludarabine, pentostatin• Anti-CD20 monoclonal antibodies – rituximab (Rituxan), ofatumumab (Azerra), obinutuzumab
(Gazvya)
• Alkylating agents crosslink DNA strands leading to impaired DNA replication and transcription, and ultimately cell death
• Purine analogs inhibit DNA synthesis by inhibiting critical enzymes involved in the process, such as DNA polymerase and adenosine deaminase
• Anti-CD20 monoclonal antibodies attach to the CD20 antigen expressed on CLL cells and activate antibody-dependent cellular and complement-dependent cytotoxicity
• Up to 6 cycles of chemotherapy may be given with cycles repeated every 28 days• Chlorambucil regimens may be given for up to 12 cycles• After completion of cycles, patients are observed until progression
47
48

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Chemoimmunotherapy Side Effects
• Major toxicities associated with chemoimmunotherapy are myelosuppression and infections
• Infection prophylaxis is indicated, and growth factor support may be necessary• FCR > BR > Clb-R
• Chemotherapy-induced nausea and vomiting can be managed per the guidelines
• Ensure patients have a PRN antiemetic for home
• Tumor lysis syndrome is also a risk in patients with high tumor burden• Assess patient’s TLS risk and provide appropriate prophylaxis
• Secondary malignancies are also a long-term risk of chemoimmunotherapy
• Potential risks to fetal health must be weighed against risks of delaying treatment in pregnant women. Pregnancy should be avoided during treatment and after as indicated by prescribing information.
PRN, “as needed”1. Eichhorst B et al. Lancet Oncol. 2016;17:928-42.2. Michallet AS et al. Haematologica. 2018;103(4):698-706.
R/R CLL
49
50

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Phase III RESONATE: Ibrutinib (Imbruvica) vs
Ofatumumab (Arzerra) in R/R CLL/SLL
▪ At time of interim analysis, median time on study was 9.4 mos
Protocol amended for crossover with support of data-monitoring committee and discussion with health authorities.
Enrollment dates:June 2012 - April 2013
Patients with CLL/SLL diagnosis; ≥1 prior therapy; ECOG PS 0/1; measurable
nodal disease (N = 391)
Ibrutinib (Imbruvica)420 mg/day PO until PD or
unacceptable toxicity (n = 195)
Ofatumumab (Arzerra)IV starting dose of 300 mg
followed by 2000 mg x 11 doses for 24 wks
(n = 196)
Crossover to Ibrutinib (Imbruvica)
420 mg/day following PD(n = 122)
Stratified by refractory to purine analogue chemoimmunotherapy (no response or relapsed within 12 mos); presence or absence of 17p13.1 (17p del)
Byrd. NEJM. 2014;371:213.
RESONATE: PFS (Primary Endpoint) and OS
HR for progression or death: 0.22 (95% CI: 0.15-0.32; P<.001 by log-rank test)
Ibrutinib
0
20
40
60
80
100
0 3 6 9 12 15Mos
PFS
(%
)
Patients at Risk, n
IbrutinibOfatumumab
195196
183161
11683
3815
71 0
OfatumumabHR for death: 0.43 (95% CI: 0.24-0.79; P = .005 by log-rank test)
Ibrutinib
0
20
40
60
80
100
0 3 6 9 12 15Mos
OS
(%)
Patients at Risk, nIbrutinib
Ofatumumab195196
191183
184164
11588
3221
53
Ofatumumab
18
Byrd. NEJM. 2014;371:213.
Ibrutinib, (imbruvica ); ofatumumab, (Arzerra)
51
52

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Phase III ASCEND Trial of Acalabrutinib (Calquence) vs
Idelalisib (Zydelig) + Rituximab (Rituxan) or BR in R/R CLL
R/R: relapsed/refractory, DoR: duration of responseGhia. EHA 2019. Abstr LB2606. NCT02970318.
▪ International, randomized, open-label phase III trial
▪ Primary endpoints: PFS per IRC
▪ Secondary endpoints: ORR, DoR, PFS per investigator, OS
▪ Interim analysis planned after ≈79 PFS events
Patients with R/R CLL, ≥1 previous systemic therapy for
CLL excluding BCL-2 or B-cell receptor inhibitors, ECOG PS ≤2
(N = 310)
Acalabrutinib (Calquence) 100 mg PO BID
Idelalisib (Zydelig) 150 mg PO BID +Rituximab (Rituxan)
orBendamustine (Treanda) 70 mg/m2 IV on
Days 1, 2 + Rituximab (Rituxan)
del(17p)(yes vs no), ECOG PS (0/1 vs 2), prior lines of therapy (1-3 vs ≥ 4)
PD (crossover from IdR/BR arm to acalabrutinib
allowed)
ASCEND: PFS by IRC Review (Primary Endpoint)
Ghia. EHA 2019. Abstr LB2606.
Acalabrutinib(n = 155)
IdR/BR(n = 155)
Median PFS, mos NR 16.5
HR (95% CI) 0.31 (0.20-0.49; P < .0001)
1-yr PFS rate, % 88 68
100
80
0
60
40
20
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Mos
PFS
(%
)
Patients at Risk, nAcalabrutinib
IdR/BR155155
153150
153150
149146
147144
146142
145136
143130
143129
139112
139105
137101
11882
6144
11677
7356
6039
2110
2518
0218
10
1 1
acalabrutinib , (Calquence); NR, not reached
53
54

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
BTK Inhibitors in Clinical DevelopmentAgent Mechanism Disease
Current
PhaseStatus
Ibrutinib
(Imbruvica)
irBTKi-C481 MCL, CLL Approved
(CLL/MCL)
Being tested in combinations
Acalabrutinib
(Calquence)
irBTKi-C481 MCL, CLL Approved
(MCL); III (CLL)
To be filed for FDA approval in
newly diagnosed and R/R CLL*
Zanubrutinib
(Brukinsa™)
irBTKi-C481 MCL, CLL III (CLL); I/II
(MCL)
Under FDA review for R/R MCL**
Ono-/GS-4059 irBTKi-C481 CLL, NHL I completed No clear plan
Spebrutinib irBTKi-C481 CLL I/Ib No clear plan
M7583 irBTKi-C481 Heme malignancies I/II Early development
Evobrutinib irBTKi-C481 Autoimmune II Autoimmune development
Fenebrutinib rBTKi CLL, NHL I completed Autoimmune development
Vecabrutinib rBTKi CLL Ib/II Early development for CLL
ARQ-531 rBTKi Heme malignancies I Early development
LOXO-305 rBTKi CLL I Early development; plan for CLL
*FDA approved for CLL,November 2019; **FDA approved for MCL November, 2019.
Phase III Trial of Venetoclax (Venclexta) + Rituximab
(Rituxan) vs BR in R/R CLL/SLL (MURANO): Study Design
▪ Multicenter, randomized, open-label phase III trial
Seymour. NEJM. 2018;378:1107. NCT02005471.
Adult patients with R/R CLL, 1-3 prior tx lines (with
≥1 CT-containing regimen), prior bendamustine
(Treanda) permitted if DoR ≥24 mos
(N = 389)
Venetoclax (Venclexta)monotherapy
until PD, unacceptable toxicity, or maximum of
2 yrs from day 1 of cycle 1
Venetoclax (Venclexta) dose ramp-up 20-400 mg PO QD for 5 wks then 400 mg PO QD for cycles 1-6 +
Rituximab (Rituxan) 375 mg/m2 on day 1 of cycle 1, then 500 mg/m2 on day 1 of cycles 2-6
(n = 194)
Bendamustine (Treanda) 70 mg/m2 on Days 1, 2 of cycles 1-6 + Rituximab (Rituxan) 375 mg/m2
on Day 1 of cycle 1, then 500 mg/m2 Day 1 of cycles 2-6(n = 195)
Stratified by del(17p), prior tx response,* geographic region
*High-risk CLL defined as del(17p); no response to first-line CT-containing tx; or relapsed in ≤12 mos after CT or in ≤24 mos after chemoimmunotherapy.
▪ Primary endpoint: investigator-assessed PFS ▪ Secondary endpoints: IRC-assessed PFS and MRD negativity, IRC-assessed CR → ORR → OS (hierarchical testing), safety
28-day cycles
55
56

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
MURANO: Updated PFS and OS
▪ Median follow-up: 36.0 mos
Kater. J Clin Oncol. 2019;37:269.
PFS
(%
)
OS
(%)
Mos Mos
Median: 17 mos
Median: NR
Median: NR
Median: NR
0 3 6 9 12 15180
20
40
60
80
100
21 24 27 30 33 36 39 42 45 48 51
HR: 0.16 (95% CI: 0.12-0.23; P < .001)
VenR (n = 194)BR (n = 195)
194195
VenRBR
185164
179142
176128
174103
17084
16779
16165
15055
13541
9926
6110
212
6 2 1190178
Mos0 3 6 9 12 1518
0
20
40
60
80
100
21 24 27 30 33 36 39 42 45 48 51
HR: 0.50 (95% CI: 0.30-0.85; P = .0093)
194195
VenRBR
185175
183167
182162
179155
178152
176150
173147
168141
163136
128111
8776
3934
139
41
2190181
Patients at Risk, n Patients at Risk, n
MURANO: MRD and Progression Status at EOT
MRD Status at EOT (n = 130)
Missing
High MRD+ ( 10–2)
Low MRD+ (10–4 to < 10–2)
uMRD (< 10–4)
83
10
1423
Status Off Therapy, n (%)
uMRD(n = 83)
Low MRD+
(n = 23)
High MRD+
(n = 14)
Missing (n = 10)
Progression free
81 (97.6) 20 (87.0) 3 (21.4) 10 (100)
Progressive disease
2 (2.4) 3 (13.0) 11 (78.6) 0
EOT, end of treatment; MRD, minimal residual disease; uMRD, undetectable minimal residual diseaseKater. J Clin Oncol. 2019;37:269.
57
58

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
MURANO: Predictors of Disease Progression at EOT
Characteristic, n/N (%) Patients With PD P Value
Blood MRD status at EOT▪ Undetectable▪ Low ▪ High
2/83(2.4 )3/23 (13.0)
11/14 (78.6)< .0001
del(17p) and/or TP53 mutation▪ At least one present▪ Neither present
10/43 (23.3)5/78 (6.4)
.01
del(11q)▪ No▪ Yes
13/80 (16.3)1/38 (2.6)
.03
del(11q) without del(17p)▪ No▪ Yes
7/58 (12.1)1/32 (3.1)
.25
Characteristic, n/N (%) Patients With PD P Value
IGHV mutation▪ No▪ Yes
13/84 (15.5)2/38 (5.3)
.14
No. previous therapies▪ 1▪ ≥2
9/78 (11.5)7/52 (13.5)
.79
Bulky disease (largest lymph node diameter)▪ <5 cm▪ ≥5 cm
9/67 (13.4)7/53 (13.2)
1.0
Nodal status at EOCT▪ <1.5 cm▪ ≥1.5 to <2 cm▪ ≥2 cm
5/64 (7.8)2/23 (8.7)
9/39 (23.1).08
Univariate analysis of clinical and cytogenetic risk factors in VenR pts who completed therapy without progression
EOT, end of treatment; EOCT: end of combination therapyKater. J Clin Oncol. 2019;37:269.
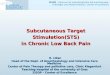
BCL-2 Coding Mutation Detected in 7 Patients With
CLL-Type Progression on Venetoclax (Venclexta)
▪ BCL-2 c.302G>T, p.(Gly101Val) detected in samples from 7 of 15 patients sequenced at CLL-type progression on venetoclax(Venclexta)
Blombery. Cancer Discov. 2019;9:342.
Exon 1
Exon 2 Exon 3
c.302G>Tp.(Gly101Val)
BCL-2 - NM_00063
Pre-VEN
C C G G C G A
Progression
C C G G C G A
59
60

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Phase III Trial of Idelalisib (Zydelig) + Rituximab (Rituxan) in Relapsed
CLL: Final Results of PFS (Primary Endpoint) and OS
▪ Phase III trial in patients with relapsed CLL after at least 1 prior line of tx
‒ Primary study 116 with idelalisib (Zydelig) /rituximab (Rituxan) followed by extension study 117 with single-agent idelalisib (Zydelig)
Sharman. JCO. 2019;37:1391.
10090
8070605040302010
0
Pro
bab
ility
of
PFS
(%
)
Mos Since Treatment Assignment
240 2 4 6 8 10
12 14 16 18 20 22
IdRPlacebo/R
PFS, median mos (95% CI)
IdR(n = 110)
19.4 (12.3-NR)
Placebo/R(n = 110)
6.5(4.0-7.3)
10090
8070605040302010
0
Pro
bab
ility
of
OS
(%)
Mos Since Treatment Assignment
560 4 8 12 16 20 24 28 32 40 44 52
IdR (to idelalisib in the extension study)Placebo/R (to idelalisib in the extension study)
OS, median mos (95% CI)
IdR(n = 110)
40.6(28.5-57.3)
Placebo/R(n = 110)
34.6(16.0-NR)
60 64 68
Phase III DUO Trial of Duvelisib (Copiktra) vs Ofatumumab
(Arzerra) in R/R CLL
▪ Duvelisib is a dual inhibitor of PI3K delta and PI3K gamma[1]
▪ Administered orally twice daily[1]
▪ Prolonged PFS compared with ofatumumab in the DUO study[2]
▪ FDA approved for patients with R/R CLL/SLL and ≥2 previous therapies in September 2018
1. Flinn. Blood. 2018;131:877. 2. Flinn. Blood. 2018;132:2446.
DUV OFAMedian PFS, mos (95% CI) 13.3 9.9
(12.1-16.8) (9.2-11.3)HR: 0.52; P < .0001
PFS
by
IRC
(%
)
PFS[2]
Mos
0
20
40
60
80
100
0 3 6 9 12 15 18 21 24 27 30
Duvelisib 25 mg BIDOfatumumab
33 36
160159
149126
10895
9577
7843
5815
337
296
133
102
31
21
00
Patients at Risk, nDuvelisib
Ofatumumab
61
62

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Phosphatidylinositol 3-Kinase (PI3K) Inhibitors
PI3K Inhibitors – Dosing
Idelalisib (Zydelig) Duvelisib (Copiktra)
Enzyme isoform(s) inhibited PI3K delta PI3K delta and gamma
FDA Approval Date July 2014 September 2018
Usual Starting Dose 150 mg PO BID continuouslyTake with or without food
25 mg PO BID continuouslyTake with or without food
Dose in Hepatic Dysfunction No dose adjustments are recommended but limited data in patients with baseline AST or ALT > 2.5 x ULN or bilirubin > 1.5 x ULN. Monitor for toxicity.
No specific recommendations as no effect of Child-Pugh A, B, or C hepaticimpairment on duvelisib exposure was seen
Availability Tablets: 100 mg, 150 mg Capsules: 15 mg, 25 mg
AST, aspartate aminotransferase, ALT, alanine aminotransferase, ULN, upper limit of normal1. Zydelig® [idelalisib (prescribing information)]. Foster City, CA: Gilead Sciences, Inc.; 2018. 2. Copiktra® [duvelisib (prescribing information)]. Needham, MA: Verastem, Inc.; 2018.
63
64

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
PI3K Inhibitors – Drug Interactions
Idelalisib (Zydelig®) Duvelisib (Copiktra®)
Substrate of CYP3A, P-gp, BCRP CYP3A, P-gp, BCRP
Effects on enzymes/transporters Strong inhibitor of CYP3A Moderate inhibitor of CYP3A
Dosing Recommendations with Restricted Concomitant Medications
Strong CYP3A inhibitor – avoid use. If not possible, monitor patient more closely for side effectsSensitive CYP3A substrates – avoid use
Strong CYP3A inhibitor – 15 mg BIDSensitive CYP3A substrates – use with caution
Avoid concomitant use with: Strong CYP3A inducers Strong CYP3A inducers
1. Zydelig [idelalisib (prescribing information)]. Foster City, CA: Gilead Sciences, Inc.; 2018. 2. Copiktra [duvelisib (prescribing information)]. Needham, MA: Verastem, Inc.; 2018.
PI3K Inhibitors – WarningsIdelalisib (Zydelig) Duvelisib (Copiktra)
Hepatotoxicity Fatal/serious hepatotoxicity: 18%Avoid concomitant agents that are liver toxicMonitor AST and ALT:• Every 2 weeks for the first 3 months, then• Every 4 weeks for the next 3 months, then• Every 1 to 3 months thereafter
Grade 3 or 4 ALT and AST elevations: 8% and 2%, respectivelyAvoid concomitant agents that are liver toxicMonitor AST and ALT periodically
Diarrhea/Colitis Grade 3 or higher diarrhea or colitis: 14% Responds poorly to antimotility agents; slow to respond to treatment interruption with or without corticosteroids
Fatal/serious diarrhea or colitis: 18%
Pneumonitis Pneumonitis: 4%Onset ranged from within the first month to 15 months into therapyDo not rechallenge
Fatal/serious pneumonitis: 5%
1. Zydelig® [idelalisib (prescribing information)]. Foster City, CA: Gilead Sciences, Inc.; 2018. 2. Copiktra® [duvelisib (prescribing information)]. Needham, MA: Verastem, Inc.; 2018. 3. NCCN Clinical Practice Guidelines in Oncology for CLL/SLL V 1.2020. 4. Cuneo A et al. Hematol Oncol. 2019;37:3-14.
65
66

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
PI3K Inhibitors – WarningsIdelalisib (Zydelig®) Duvelisib (Copiktra®)
Infections Fatal and/or serious infections: 21%Cases of cytomegalovirus (CMV) reactivation and Pneumocystis jirovecii pneumonia have been reported
Serious/fatal infections: 31%Cases of CMV reactivation and Pneumocystis jirovecii pneumonia have been reported
Neutropenia Grade 3 or 4 neutropenia: 25%Monitor blood counts every 2 weeks for the first 6 months, then as clinically indicated. Monitor weekly when ANC is less than 1K
Grade 3 or 4 neutropenia: 42% Monitor blood counts every 2 weeks for the first 2 months, then as clinically indicated. Monitor weekly when ANC is less than 1K
Cutaneousreactions
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) have occurred.Do not rechallenge if SJS or TEN occurs
Serious/fatal cutaneous reactions: 5% Drug reaction with eosinophilia and systemic symptoms (DRESS) and TEN have occurred
Intestinalperforation
Rare occurrence, not always in the setting of diarrhea/colitisDo not rechallenge
Not listed as a warning
Anaphylaxis Rare occurrence Not listed as a warning
Embryo-fetal toxicity
May cause fetal harm. avoid pregnancy while taking; use effective contraception during and at least 1 month after treatment
Can cause fetal harm when administered ; conduct pregnancy testing before initiating treatment. Advise females, and males with female partners of reproductive potential, to use effective contraception during treatment and for at least 1 month after the last dose
ANC, absolute neutrophil count; CMV, cytomegalovirus 1. Zydelig [idelalisib (prescribing information)]. Foster City, CA: Gilead Sciences, Inc.; 2018. 2. Copiktra [duvelisib (prescribing information)]. Needham, MA: Verastem, Inc.; 2018.3. NCCN Clinical Practice Guidelines in Oncology for CLL/SLL V 1.2020.
PI3K Inhibitors – Other Common Side Effects
Non-lab events occurring in ≥20% of patients in idelalisib (Zydelig ®) clinical trials
• Rash
• Pneumonia
• Fatigue
• Pyrexia
• Cough
• Diarrhea
• Nausea
Non-lab events occurring in ≥20% of patients in duvelisib (Copiktra ®) clinical trials
• Fatigue
• Pyrexia
• Upper respiratory tract infection
• Diarrhea
• Nausea
• Rash
• Pneumonia
• Cough
1. Zydelig® [idelalisib (prescribing information)]. Foster City, CA: Gilead Sciences, Inc.; 2018. 2. Copiktra® [duvelisib (prescribing information)]. Needham, MA: Verastem, Inc.; 2018.
• Advise patients about the possibility of lymphocytosis after initiating treatment• Occurs within the first month of therapy and can persist for several weeks. Not progression!
67
68

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Additional Patient Support
Infection Monitoring and ProphylaxisNewly Diagnosed CLL Relapsed/Refractory CLL
Ibrutinib (Imbruvica) HSV, HBV* HSV, HBV*
Acalabrutinib (Calquence) --- HSV, HBV*
Venetoclax (Venclexta) HSV HSV
Idelalisib (Zydelig) --- HSV, PJP, HBV*, CMV**
Duvelisib (Copiktra) --- HSV, PJP, HBV*, CMV**
CD20 monoclonal antibodies HBV* HBV*
Chemoimmunotherapy HSV, PJP, HBV*, CMV**#Consider bacterial/fungal during periods of neutropenia
HSV, PJP, HBV*, CMV**#Consider bacterial/fungal during periods of neutropenia
Alemtuzumab --- HSV/VZV, PJP, HBV*, CMV** Considerfungal
CMV, cytomegalovirus; HSV, herpes simplex virus; HBV, hepatitis B virus; PJP, Pneumocystis jirovecii pneumonia ;VZV, varicella zoster virus1. NCCN Clinical Practice Guidelines in Oncology for CLL/SLL V 1.2020. 2. NCCN Clinical Practice Guidelines in Oncology for Prevention and Treatment of Cancer-Related Infections V 1.2019.
*Patients should be screened for hepatitis and those patients HBsAg positive should receive prophylaxis**Monitor for CMV reactivation weekly using quantitative PCR while on therapy and for a period of time after. #Fludarabine-based chemoimmunotherapy.
69
70

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Medication Access• Oral agents present unique challenges with regard to patient access to the
medication• Most patients will not be able to start a new therapy on the day the prescription is written• Challenges in scheduling concomitant IV medication if combination therapy planned
• Prescriptions may require prior authorization, which can delay the start of therapy
• Covered prescriptions may still have high copays that necessitate applications to programs/foundations for financial assistance
• Patients without prescription coverage must rely on manufacturer’s assistance programs to acquire free drug
• Many members of the healthcare team may need to assist the patient in obtaining access to the medication
Medication Adherence
• The transition to oral therapies as the backbone of CLL therapy has highlighted the importance of monitoring patient adherence to therapy
• Therapy is continuous with no defined end point
• Data in other disease states as well as CLL demonstrate the importance of adherence on outcomes
• A retrospective analysis of patients receiving Ibrutinib on the RESONATE study evaluated the effect of dose intensity on CLL outcomes
• Patients that maintained high dose intensity with ibrutinib therapy had improved PFS
• Treatment interruptions of greater than 7 days were associated with increased PFS events
• Members of the healthcare team should assess patient’s adherence to therapy at each visit at a minimum
• More frequent assessments may be necessary at therapy initiation and when managing toxicities
Barr PM et al. Blood. 2017;129(19):2612-5.
71
72

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Oral CLL Therapies – Patient Counseling Points
• When initiating therapy, encourage patients to reach out for any barriers acquiring the medication
• Stress adherence to prescribed dose, taking at the same time(s) each day
• Educate patients on the common or serious side effects
• Remind patients to report any changes to medical problems and concomitant medications to healthcare teams
Nursing Considerations in CLLJACKIE BROADWAY-DUREN, DNP, APRN, FNP-BC
73
74

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Who Are Oncology Nurses?
Registered nurses (RNs) have varied levels of educational preparation
▪Associate degree
▪Bachelor’s degree
▪Doctorate degrees
▪DNP/PhD
▪ Many oncology nurses are oncology certified (OCN)
▪ Have specialized training applicable to area of specialty
Rationale for Nurses in CLL▪ Nurses are vital to oncology patient care
▪ Deliver high-quality clinical services
▪ Contribute to improved patient outcomes
▪ Serve in multifaceted roles in CLL patient care
Oncology Nursing Society. Retrieved from http://www.ons.org
75
76

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Nursing Roles in CLL Patient Care
Patient Care Advocate
EducatorResearch Study
Coordinators
Oncology Nurse Roles
Interprofessional Team MemberAs a member of the interprofessional team, nurses:
▪ Triage patients based on symptoms
▪Assist in patient education for oral therapies
▪Assist in coordinating treatment schedules and patient appointments
▪Administer IV infusions (i.e., antibody therapy)
▪Collaborate with physicians, APPs, pharmacists, social work, and patient
advocates in coordinating patient care
77
78

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Role of the RN in Patient Care▪ Review medications during each clinic visit
▪ Provide initial review of systems with each clinic visit
▪ Administer outpatient injections (vaccine) and monitor patients for side effects
▪ Perform bedside nursing for hospitalized patients (Richter’s)
▪ Work with multidisciplinary teams to ensure patient needs are met
Nurse Educator Role in CLL▪RNs provide pertinent patient education
▪RNs provide written drug side effect information
▪Instruct patients on oral drug adherence and assist in patient follow-up
▪APRNs educate patients with specific disease-related information and mechanism of action of various therapies (e.g., MAB, BTK inhibitors)
79
80

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Patient Advocacy in CLL▪ Transitional care – collaborate with patient’s community providers
▪ Facilitate prior authorizations
▪Collaborate with specialty pharmacies to ensure patient medications are delivered on time
▪Care coordination is an integral component of the oncology nurse’s job
▪Assist with communication among patients, family members, and other disciplines
▪ Prepare patients and caregivers on expectations for clinic and treatments
Research Nurse Role in CLL▪Collaborate with the interprofessional team members to determine best
treatment recommendations
▪Research nurses (RNs) educate patients regarding research protocols, specific drug information, and study requirements
▪Register patients for research protocols
▪Obtain consent for research studies
▪Monitor adverse events of therapy and report to PI, attending physician/APP
▪Collaborate with pharmaceutical and FDA sponsors of research studies and report adverse events using grading scales
81
82

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Advanced Practice Nurses (APRNs) in CLL▪APRNs perform physical examinations, order and interpret laboratory and
radiologic diagnostic tests, and order blood products and growth factors as indicated
▪APRNs consent patients for treatments for off-protocol therapy
▪Collaborate with physicians and pharmacists regarding appropriate treatments
▪APRNs assist in managing adverse drug effects (AEs) by:
▪Monitoring lab data with intervention as indicated (TLS)
▪ Prescribe appropriate medications or needed intervention to manage AEs
Integration of Interprofessional Roles▪New patient presents to clinic with new diagnosis of B CLL
▪ The RN is the first point of contact upon patient entering clinic
▪ The RN does initial review of systems (ROS), reviews and updates medications
▪ The RN hands the patient off to the APRN or PA (APP)
▪ The APRN assesses the patient, including past medical history, past cancer therapies, performs H&P and medication review, and orders appropriate tests
▪ The attending physician is then given a report on the patient, and further evaluation and decisions are made with team input
83
84

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
RESOURCES FOR YOU & YOUR PATIENTS
FROM THE LEUKEMIA & LYMPHOMA SOCIETY (LLS)
WWW.LLS.ORG
LLS RESOURCES FOR HEALTHCARE PROFESSIONALS
Online and in-person CE/CME webinars, symposia & rounds
Free CME & CE www.LLS.org/CE
Podcast series for healthcare professionals Conversations with experts about diagnosing & treating blood
cancers www.LLS.org/HCPpodcast
HCP palm card – User friendly links to resources for you & your patients
www.LLS.org/CE
85
86

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
LLS RESOURCES FOR PATIENTS AND CAREGIVERS
❑ Information Specialists – disease information, emotional support, financial, travel & co-pay assistance, support
through local LLS patient access staff. Also send free materials to patients & HCPs
❑Nutrition Consultations – One-on-one consultations from certified dietitian
Specialists can serve as a resource for your HCP team
M - F, 9 am to 9 pm ET:
❑ Phone: (800) 955-4572
❑ Live chat: www.LLS.org/InformationSpecialists
❑ Email: [email protected]
❑Additional support for patients & caregivers – www.LLS.org/Support
❑Booklets on disease, treatment, & support - www.LLS.org/Booklets
❑Webinars, videos, in-person programs - www.LLS.org/Programs & www.LLS.org/Educationvideos
CLINICAL TRIAL NURSE NAVIGATORS
Help patients find and enroll in
clinical trials based on highly
detailed individualized assessments
www.LLS.org/Navigation
602patients provided with in-depth clinical trial
navigation and support in past year
87
88

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
We have one goal: A world without blood cancers
THANK YOU
Appendix
89
90

© National Comprehensive Cancer Network, Inc. 2019, All Rights Reserved. No part of this
publication may be reproduced or transmitted in any other form or by any means, electronic or
mechanical, without first obtaining written permission from NCCN®.
Rai and Binet Staging Systems and CLL International Prognostic Index
Chronic Lymphocytic Leukemia Booklet, The Leukemia & Lymphoma Society- LLS.org
91