Embed Size (px)
DESCRIPTION
egdyhjuhkiu
Citation preview

Choroidal Findings in Dome-Shaped Macula in HighlyMyopic Eyes: A Longitudinal Study
FRANCESCO VIOLA, LAURA DELL’ARTI, ELEONORA BENATTI, ALESSANDRO INVERNIZZI, CHIARA MAPELLI,FABIO FERRARI, ROBERTO RATIGLIA, GIOVANNI STAURENGHI, AND GIULIO BARTESELLI
� PURPOSE: To describe choroidal findings in dome-shaped macula associated with high myopia using fluores-cein angiography (FA), indocyanine green angiography(ICGA), and spectral-domain optical coherence tomogra-phy (SD OCT), and to elucidate the mechanism and nat-ural course of serous retinal detachment (RD) associatedwith dome-shaped macula.� DESIGN: Retrospective, observational case series.� METHODS: We reviewed longitudinal imaging results of52 highly myopic eyes with dome-shaped macula.Changes on FA and ICGA were assessed. Retinal,choroidal, and scleral thicknesses and bulge height weremeasured on SD OCT.� RESULTS: Serous RD was the most common abnormal-ity associated with dome-shaped macula, detected by SDOCT in 44% of the cases with no associated choroidalneovascularization. Significant differences in the propor-tion of eyes with pinpoint leakage on FA (P < .001),punctate hypercyanescence on ICGA (P < .001),and pigment epithelium detachment on SD OCT(P < .001) were noted inside the inward bulge of thestaphyloma between eyes with and without serous RD.Serous RD was not associated with hyperpermeabilityareas on ICGA. Eyes with serous RD had thicker choroid(P[ .004) and tended to have thicker sclera (P[ .067)and greater bulge height (P [ .079). Choroidal thick-ness, scleral thickness, and bulge height were positivelycorrelated (P < .01). All eyes presented a fluctuatingcourse of serous RD during follow-up. Worsening ofserous RD was associated with appearance of new punc-tate hypercyanescent spots on ICGA and leaking pointson FA (P < .001 and P [ .016, respectively).� CONCLUSION: Serous RD in dome-shaped macula waslikely caused by choroidal vascular changes, similar to cen-tral serous chorioretinopathy, but specifically confined inthe inward bulge of the staphyloma and secondary to exces-sive scleral thickening. Serous retinal detachment showed
Accepted for publication Sept 16, 2014.From the Ophthalmological Unit, Ca’ Granda Foundation-Ospedale
Maggiore Policlinico, University of Milan, Department of ClinicalSciences and Community Health (F.V., L.D.A., E.B., A.I., C.M., F.F.,R.R., G.B.), and Eye Clinic, Department of Biomedical and ClinicalSciences ‘‘Luigi Sacco,’’ Luigi Sacco Hospital, University of Milan (A.I.,G.S.), Milan, Italy.
Inquiries to Francesco Viola, University of Milan, OphthalmologicalUnit, Ca’ Granda Foundation-Ospedale Maggiore Policlinico, ViaFrancesco Sforza 35, 20122 Milan, Italy; e-mail: [email protected]
44 � 2015 BY ELSEVIER INC.
fluctuating changes over time, with alternating active andinactive stages. Angiographic findings in dome-shapedmacula suggest the choroid as a target for possible treat-ment strategies. (Am J Ophthalmol 2015;159:44–52.� 2015 by Elsevier Inc. All rights reserved.)
DOME-SHAPED MACULA WAS FIRST DESCRIBED BY
Gaucher and associates in 2008 by the use oftime-domain optical coherence tomography
(OCT) as an inward convexity or bulge of the maculathat occurred in approximately 10% of highly myopiceyes within the concavity of the posterior staphyloma.1
Subsequently, enhanced depth imaging optical coherencetomography (EDI OCT) showed that dome-shaped maculais the result of a localized variation in scleral thickness inthe macular area.2 By using swept source OCT, whichallowed deeper tissue penetration into the choroid andeven sclera, Ellabban and associates reported the precisetopography of the posterior pole in eyes with dome-shaped macula, describing a horizontal ridge formed withinthe posterior staphyloma by uneven thinning of the sclera.3
More recently, Caillaux and associates described 3morpho-logic dome-shaped macula patterns according to spectral-domain OCT (SD OCT) features: round domes (withoutpredominant axis), horizontally oriented oval-shapeddomes, and vertically oriented oval-shaped domes.4
Vision-threating macular complications typicallydescribed in highly myopic patients, including choroidalneovascularization (CNV), retinal pigment epithelial(RPE) changes, macular holes, and foveoschisis, havebeen reported to be associated with dome-shaped maculaas well.3,5 Serous retinal detachment (RD) without CNVis a well-established complication responsible for visionloss in dome-shaped macula, but is rarely reported in highlymyopic eyes without the presence of dome-shaped mac-ula.1–5 To date, however, limited information is availableon the role played by choroid dynamics based onfluorescein (FA) and indocyanine green (ICGA)angiography in the pathogenesis of serous RD associatedwith dome-shaped macula. Interestingly, this complicationpresents similar ophthalmoscopic and angiographic find-ings to central serous chorioretinopathy (CSC),6 as wellas tilted disc syndrome.7–9
In the study described herein, we aimed to analyze mac-ular changes in highly myopic eyes with dome-shaped mac-ula imaged by FA and ICGA angiography combined with
0002-9394/$36.00http://dx.doi.org/10.1016/j.ajo.2014.09.026
ALL RIGHTS RESERVED.

SD OCT in order to elucidate the mechanism of serous RDdevelopment. We also aimed to study the long-term clin-ical course of dome-shaped macula by analyzing morpho-logic and angiographic changes over time.
METHODS
� PATIENTS: We retrospectively reviewed charts andimaging studies of highly myopic patients diagnosed withdome-shaped macula between October 2009 andSeptember 2013 at the Ophthalmological Unit, Ca’Granda Foundation-Ospedale Maggiore Policlinico, or atthe Eye Clinic, ‘‘Luigi Sacco’’ Hospital, 2 tertiary care cen-ters specialized in the diagnosis and treatment of retinal dis-eases in Milan, Italy. Patients had been referred to us fordiagnosis of visual complains or imaging of suspectedfundus anomalies diagnosed in an examination performedroutinely. To be included in the chart and imaging review,eyes must have had: (1) refractive error of 6.0 diopters ormore, axial length of 26.5 mm or more, or both; (2) unilat-eral or bilateral dome-shaped macula configuration onOCT according to the description of Gaucher and associ-ates1; and (3) posterior staphyloma resembling Curtintype I or II.10 We excluded eyes with inferior staphyloma(type V10) alone or associated with tilted disc syndromein which the macula lays on the edge or slope of the inferiorstaphyloma; eyes with poor image quality owing to mediaopacities; and eyes with history of CSC, retinal vasculardiseases, or major retinal surgery. Patients with a historyor receiving medications potentially at risk of serous RD(eg, corticosteroids) were excluded from the study aswell. The study and data accumulation were in conformitywith Italian laws. The study was in adherence to the tenetsof the Declaration of Helsinki.
� IMAGING PROTOCOL AND ANALYSIS: All patients werescanned with a confocal scanning laser ophthalmoscope(cSLO) after measurement of the best-corrected visual acu-ity (BCVA) using standard Early Treatment Diabetic Reti-nopathy Study (ETDRS) charts. Patients underwentmultimodal imaging including late-phase FA, late-phaseICGA, and SD OCT scans carried out with the HeidelbergSpectralis (Heidelberg Engineering, Heidelberg,Germany), which allows simultaneous co-localization ofposterior structures on bidimensional cSLO images andcross-sectional SD OCT scans with high accuracy.11 TheSD OCT scanning protocol included 9-mm horizontaland vertical scans centered on the fovea in EDI modeand a 3D raster scan centered on the fovea; the baselinescans were set as reference for the subsequent scans thatwere taken usually every 3 months. Scans were performedbetween 8 AM and 11 AM for logistical reasons.
Two trained physicians (F.V., L.D.A.) performed imag-ing analysis to identify fundus abnormalities on multimodal
VOL. 159, NO. 1 CHOROIDAL FINDINGS IN MYOP
imaging. On late-phase FA, the physicians evaluated pres-ence of leaking points. On late-phase ICGA, they evalu-ated presence of punctate hypercyanescent spots, areas ofhyperpermeability of the choriocapillaris, and subfovealhypocyanescent oval area. In case of disagreement, a thirdphysician (G.B.) was consulted to achieve an acceptableresult. On SD OCT scans, the physicians evaluated pres-ence of macular anomalies or complications (eg, macularholes, foveoschisis, foveal serous RD, fibrovascular RPEdetachment suggesting a CNV), subfoveal retinal thick-ness, choroidal thickness in the fovea and at 1500 mm su-periorly and inferiorly to the fovea, subfoveal scleralthickness, and macular bulge height and orientation.To measure the choroidal thickness, the line correspond-
ing to the internal limiting membrane automatically placedby the built-in automated segmentation software of the SDOCT device was manually moved to the outer part of thehyperreflective line corresponding to the base of the RPE.The line corresponding to the basement membrane wasmoved to the posterior edge of the choroid, as demarcatedby the hyperreflective margin line corresponding to thechorioscleral interface. This method allowed automaticmeasurement of the choroidal thickness along the 9-mmline scans using the built-in retinal thickness software,with high reproducibility as previously shown.12 A similarapproachwas used tomeasure the subfoveal scleral thicknessas well. The macular bulge height was measured on horizon-tal andvertical SDOCTscans by using the caliper tool of thedevice between the outer border of the RPE at the fovea andthe line tangent to the outer border of theRPE at the bottomof the staphyloma, using a previously described method.4
� STATISTICAL ANALYSIS: The statistical analyses,including the Fisher exact test, Mann-Whitney U test,and Spearman rank correlation coefficient test, wereperformed using SPSS statistical software version 20(SPSS Inc, Chicago, Illinois, USA). The alpha level(type I error) was set at 0.05.
RESULTS
� BASELINE EXAMINATION: The study included 52 eyeswith dome-shaped macula of 32 consecutive white highlymyopic patients, whose characteristics are summarized inTable 1. The dome-shaped macula was bilateral in 20 of32 patients (62.5%). Mean age was 56.7 6 15.4 years(range, 20–82 years). Mean spherical equivalent was �146 5.6 diopter (D) (range,�3 to�25 D). Mean axial lengthwas 29.02 6 1.18 mm (range, 27.59–31.51 mm). MeanBCVA was 0.32 6 0.24 logMAR.Seventeen eyes out of 52 (32.7%) had foveal serous RD
at baseline SD OCT scan with no associated vitreomaculartractions or CNV. Other macular abnormalities or compli-cations detected by SD OCT included CNV (13 eyes),
45IC DOME-SHAPED MACULA

TABLE 1. Characteristics of the 52 Highly Myopic Eyes Witha Dome-Shaped Macula
Eyes/patients (n) 52/32
Sex 23 female/9 male
Age (y), mean 6 SD (range) 56.7 6 15.4 (20–82)
Spherical equivalent (D), mean
6 SD (range)
�14.0 6 5.6 (�3 to �25)
Axial length (mm), mean 6 SD
(range)
29.02 6 1.18 (27.59–31.51)
BCVA (logMAR), mean 6 SD
(range)
0.32 6 0.24 (0–1.0)
Macular abnormalities on SD
OCT
Foveal SRD 17/52 (32.6%)
CNV 13/52 (25.0%)
Extrafoveal schisis 5/52 (9.6%)
Foveoschisis 2/52 (3.8%)
Lamellar MH 1/52 (2.0%)
Dome-shaped macula patterns
Horizontally oriented, oval 39/52 (75.0%)
Vertically oriented, oval 12/52 (23.1%)
Central, round 1/52 (1.9%)
BCVA ¼ best-corrected visual acuity; CNV ¼ choroidal
neovascularization; D ¼ diopters; MH ¼ macular hole; SD
OCT ¼ spectral-domain optical coherence tomography;
SRD ¼ subretinal detachment.
TABLE 2. Analysis of Imaging Characteristics by Presence of Sero
Without Choroidal Ne
Test Finding
FA Pinpoint leakage Yes (n ¼ 1
No (n ¼ 24
RPE atrophic changes Yes (n ¼ 1
No (n ¼ 22
ICGA Punctate hypercyanescent spots Yes (n ¼ 1
No (n ¼ 23
Focal choroidal hyperpermeability Yes (n ¼ 2
No (n ¼ 37
Subfoveal oval hypofluorescent area Yes (n ¼ 6
No (n ¼ 33
SD OCT Small PED Yes (n ¼ 2
No (n ¼ 19
Horizontally oriented, oval dome Yes (n ¼ 3
No (n ¼ 1)
Vertically oriented, oval dome Yes (n ¼ 1
No (n ¼ 27
Central, round dome Yes (n ¼ 1
No (n ¼ 28
FA ¼ fluorescein angiography; ICGA ¼ indocyanine green angiograp
epithelium; SD OCT ¼ spectral-domain optical coherence tomography.
46 AMERICAN JOURNAL OF
extrafoveal schisis (5 eyes), foveoschisis (2 eyes), andlamellar macular hole (1 eye). Three-dimensional OCTimaging of the posterior pole showed 39 eyes (75%) witha horizontally oriented oval-shaped dome (ie, showing aconvex configuration on the vertical scan through thefovea, while the horizontal scan showed an almost flatRPE line4), 12 eyes (23%) with a central round dome,and only 1 eye (2%) with a vertically oriented oval-shaped dome.
� COMPARISON BETWEEN EYES WITH AND WITHOUTSEROUS RETINAL DETACHMENT: Among the 39 eyeswithout a CNV, 17 (44%) showed serous RD at baselineSD OCT examination. No differences in age (P ¼ .586),axial length (P ¼ .358), and BCVA (P ¼ .226) were foundbetween eyes with serous RD and eyes without serous RD.Among eyes with and without serous RD (Table 2) wefound a statistically significant difference in the proportionof eyes with pinpoint leakage on FA (P< .001, Fisher exacttest), punctate choroidal hypercyanescent spots on ICGA(P < .001), and oval hypocyanescent area on ICGA (P ¼.033) (Figure 1). Among the 17 eyes with serous RD, asmall nonfibrovascular pigment epithelium detachment(PED) was detected in 15 eyes (88%) (Figure 1); therewas a statistically significant difference in the proportionof eyes with a PED among eyes with and without serousRD (P < .001). The presence of a PED was significantly
us Retinal Detachment in 39 Eyes With Dome-Shaped Macula
ovascularization
Serous Retinal Detachment
Yes (n ¼ 17) No (n ¼ 22) P Value (Fisher Exact Test)
5) 15 (88%) 0 (0%) <.001
) 2 (12%) 22 (100%)
7) 7 (32%) 10 (59%) .092
) 15 (68%) 7 (41%)
6) 15 (88%) 1 (5%) <.001
) 2 (12%) 21 (95%)
) 2 (12%) 0 (0%) .184
) 15 (88%) 22 (100%)
) 5 (29%) 1 (5%) .033
) 12 (71%) 21 (95%)
0) 15 (88%) 5 (23%) <.001
) 2 (12%) 17 (77%)
8) 16 (94%) 22 (100%) .436
1 (6%) 0 (0%)
2) 8 (47%) 4 (18%) .053
) 9 (53%) 18 (82%)
1) 7 (41%) 4 (18%) .114
) 10 (59%) 18 (82%)
hy; PED ¼ pigment epithelium detachment; RPE ¼ retinal pigment
JANUARY 2015OPHTHALMOLOGY

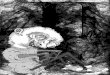
FIGURE 1. Multimodal imaging of a patient affected by bilateral dome-shaped macula. Left to right: fundus color photography (FP),late-phase fluorescein angiography (FA), late-phase indocyanine green angiography (ICGA), and spectral-domain optical coherencetomography (SD OCT). White vertical arrows on late FA images correspond to the area of the retina scanned by SD OCT. (Toprow) Right eye baseline examination. Serous retinal detachment is clearly visible on SD OCT scan (Top right) at the apex of thedome, with also a small detachment of the retinal pigment epithelium (RPE). Leaking points are visible on late FA. Two punctate hyper-fluorescenthypercyanescent spots (white arrowheads) canbe appreciatedon late-phase ICGA.These signs represent anactive stage of thedisease. (Second row)Right eye examination at 1 year. Serous retinal detachment is still present on SDOCT scan, although reduced andmodified in shape and position. The detachment of the RPE is also improved but still present. Fluorescein angiography is almost un-changed. A single punctate hypercyanescent spot is visible on late-phase ICGA (white arrowhead). The disease was still active. (Thirdrow) Left eye baseline examination.No signs of disease activity can be identified through any of the imagingmodality. (Bottom row) Lefteye examination at1year. Serous retinal detachment appears beneath the foveaonSDOCTscanas signofdisease activity.At this timeFAshows a well-identifiable leaking point, whereas a punctate hypercyanescent spot is visible on late-phase ICGA (white arrowhead).
correlated with the presence of pinpoint leakage on FA(P < .001) and punctate choroidal hypercyanescent spotson ICGA (P < .001). Seventeen out of 39 eyes (44%)had RPE atrophic changes at baseline. No differenceswere found in the proportion of eyes showing RPE atrophicchanges on FA (P ¼ .092), or hyperpermeability areas onlate-phase ICGA (P ¼ .184), or a particular orientationof the dome (P > .05) between eyes with and withoutserous RD.
The comparison of the 2 groups of eyes with and withoutserousRDbyMann-WhitneyU test indicated that eyeswith
VOL. 159, NO. 1 CHOROIDAL FINDINGS IN MYOP
serous RD had a thicker choroid in the fovea (P¼ .004) and1500mm inferiorly to the fovea (P¼ .014) compared to eyeswithout serous RD (Table 3). They also tended to have agreater subfoveal scleral thickness (P ¼ .067) and a greatermacular bulge height (P ¼ .079). The subfoveal choroidalthickness was positively correlated with the macular bulgeheight (P < .001, Spearman rank correlation coefficienttest) (Figure 2) and with the scleral thickness (P ¼ .002),but was not associated with BCVA (P ¼ .660). A positivecorrelation was also found between the bulge height andthe subfoveal scleral thickness (P ¼ .004).
47IC DOME-SHAPED MACULA

TABLE 3. Analysis of Thickness Measurements by Presence of Serous Retinal Detachment in 39 Eyes With Dome-Shaped MaculaWithout Choroidal Neovascularization
All Eyes (n ¼ 39)
Serous Retinal Detachment
No (n ¼ 22) Yes (n ¼ 17) P Value (Mann-Whitney U Test)
Choroidal thickness (mm)
Fovea 132.7 6 79.1 100.5 6 61.5 174.3 6 79.8 .004
Superior 1500 135.7 6 88.0 114.3 6 75.4 165.1 6 95.3 .092
Inferior 1500 131.2 6 93.3 93.7 6 57.4 182.8 6 107.4 .014
Foveal scleral thickness (mm) 577.4 6 137.3 547.2 6 147.8 653.1 6 58.1 .067
Macular bulge height (mm) 371.2 6 217.7 322.8 6 228.6 425.2 6 190.7 .079
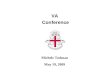
FIGURE 2. Scatterplots of the relationship between subfoveal scleral thickness, subfoveal choroidal thickness, and bulge heightamong the 39 eyes with dome-shaped macula without choroidal neovascularization. (Left) Scleral thickness and choroidal thicknessshowed a significant positive correlation (R2 [ 0.281, P [ .002). (Middle) Scleral thickness and bulge height showed a significantpositive correlation (R2 [ 0.268, P[ .004). (Right) Choroidal thickness and bulge height showed a significant positive correlation(R2 [ 0.316, P < .001).
� FOLLOW-UP EXAMINATION OF EYES WITH SEROUSRETINAL DETACHMENT: Follow-up OCT examination ofat least 12 months was available in 13 out of 39 eyeswithout CNV (33%), with a mean duration of 20 65 months (range, 12–24 months). None of the eyes weretreated when serous RD was present. All 13 eyes presenteda fluctuating course of serous RD among follow-up visits; in3 of them (23.1%) it disappeared completely and thenreappeared at some point (Figure 3), while in the remainingeyes (76.9%) it was reduced or increased without disappear-ing completely. After complete or partial resolution of se-rous RD, punctate hypercyanescent spots on late-phaseICGA disappeared in all cases (Figure 3, Middle line),while leaking points on late-phase FA disappeared in57% of the cases. Worsening of serous RD from the previ-ous OCT examination was significantly associated with theappearance of new punctate hypercyanescent spots on late-phase ICGA and small leaking points on late-phase FA (P< .001 and P¼ .016, respectively) (Figure 3, Bottom line).No correlation was found with the appearance of hyperper-meability areas (P ¼ .098) or oval hypocyanescent areason ICGA (P ¼ .920). Mean amplitude (peak-trough
48 AMERICAN JOURNAL OF
difference) of the variation in subfoveal retinal thicknessduring follow-up was 124 6 65 mm (range, 34–235 mm)and corresponded to a variation in serous RD height of 1206 38 mm. Mean amplitude (peak-trough difference) of thevariation in subfoveal choroidal thickness during follow-upwas 266 12mm (range, 3–43mm). There was no correlationbetween variation in subfoveal retinal thickness and varia-tion in subfoveal choroidal thickness (P ¼ .168).
DISCUSSION
THE PRESENT STUDY CONFIRMED THAT SEVERAL TYPES OF
macular abnormalities or complications might occur inmyopic eyes with dome-shaped macula. Foveal serous RDwas the most common finding, observed in almost one thirdof the eyes with dome-shaped macula and in 44% of theeyes with dome-shaped macula without myopic CNV. Se-rous RD is generally not described in highly myopic eyeswithout CNV or tractional phenomena, except for eyeswith dome-shaped macula or tilted disc syndrome.4,7
JANUARY 2015OPHTHALMOLOGY

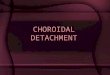
FIGURE 3. Multimodal imaging of a patient affected by relapsing dome-shaped maculopathy in the right eye. Left to right: late-phasefluorescein angiography (FA), late indocyanine green angiography (ICGA), and spectral-domain optical coherence tomography (SDOCT). White vertical arrows on late FA images correspond to the area of the retina scanned by SD OCT (large scans on the right).Black horizontal arrows on ICGA correspond to SD OCT scans through the punctate hypercyanescent spots (small sub-squares).(Top row) Baseline examination showing active disease. Serous retinal detachment is visible beneath the fovea on SD OCT scan.A leaking point is detectable on late FA. Indocyanine green angiography shows a punctate hypercyanescent spot, and SD OCTscan through the spot demonstrates the presence of a corresponding serous retinal detachment (white arrowheads). (Middle row)Three-month follow-up examination showing inactive phase. Spectral-domain optical coherence tomography scan shows no presenceof serous retinal detachment. The leaking point on FA has disappeared, as well as the punctate hypercyanescent spot on late-phaseICGA. (Bottom row) One-year follow-up examination showing disease relapse. A very shallow serous retinal detachment is presenton SD OCT scan through the fovea. Late-phase FA shows a leaking point, and a punctate hypercyanescent spot is visible on ICGA.Spectral-domain optical coherence tomography scan through the spot still demonstrates the presence of a new serous retinal detach-ment (white arrowheads) as a sign of active disease.
Although recent advances in OCT technology helped inevaluating dome-shaped macula, the pathogenesis of serousRD in such pathology remains uncertain. In the presentstudy we provided new data on angiographic findingsrelated to the presence of this vision-threatening complica-tion. Serous retinal detachment was associated withpinpoint leakage on FA, with punctate hypercyanescentspots and oval hypocyanescence on ICGA, and with smallPEDs. We found a high incidence (88%) of pinpointleakage on FA in eyes with serous RD. This was consistentwith the description of FA dynamics in such eyes previouslypresented by Gaucher and associates. These authors re-ported that points with active leakage on late-phase FAoccurred in an area of RPE atrophic changes, and were
VOL. 159, NO. 1 CHOROIDAL FINDINGS IN MYOP
mimicking leaking points typically seen in chronic idio-pathic CSC.1 However, limited information was reportedon choroid dynamics based on ICGA. Indeed, as a newfinding we demonstrated the presence of punctate hyper-cyanescent spots on ICGA in 88% of eyes with serousRD. In addition, serous RD had a fluctuating course amongfollow-up visits, with an average height variation of120 mm, and temporarily disappeared in 31% of the eyeswithout treatment. This variation was independent of thesubfoveal choroidal thickness. Interestingly, in cases ofworsening of serous RD, appearance of punctate hypercya-nescent spots on late-phase ICGA and pinpoint leakage onFA was observed, but without appearance of hyperperme-ability areas or oval hypocyanescent area on ICGA.
49IC DOME-SHAPED MACULA

Moreover, subfoveal choroidal thickness was significantlygreater in eyes with serous RD. All these angiographicand tomographic characteristics are typical findings inCSC.13 The lack of evidence of focal hypercyanescentspots on ICGA in Gaucher’s studies1,4 may be explainedby the fact that these authors focused more on OCTdescription of dome-shaped macula, while ICGA wasperformed mainly to rule out the presence of CNV.
Gaucher and associates found RPE atrophic changes onFA that corresponded to a subfoveal oval-shaped hypo-fluorescent area on ICGA in all eyes with serous RD.1
On the contrary, in our study atrophic changes were pre-sent in only 44% of the eyes and were not significantly asso-ciated with serous RD. This discrepancy may be explainedby the fact that Gaucher and associates observed a symp-tomatic population with severe dome-shaped macula formsresulting in RPE dysfunction and subsequent chronic serousRD. In our series the presence of serous RD was not accom-panied by significant visual loss compared to the group ofeyes with dome-shaped macula without serous RD,confirming that we probably recruited a population withan early stage of the disease. Therefore, in our populationwith less RPE atrophic change, serous RD likely arosefrom punctate choroidal vascular abnormalities attribut-able to the posterior inward bulge as an active/acute stageof the disease, rather than arising from chronic RPEdysfunction.
Interestingly, punctate hypercyanescent spots on ICGAwere also recently reported with a similar incidence (93%of affected eyes and 78% of unaffected fellow eyes) in pa-tients with serous RD associated with acute CSC by Tsuji-kawa and associates,13 but not reported in eyes with serousRD associated with tilted disc syndrome. In our series, thisangiographic finding was not detected in eyes with dome-shaped macula without serous RD or in the fellow eyewithout dome-shaped macula. Therefore, an initialchoroidal abnormality, displayed with tiny punctate hyper-cyanescent spots on ICGA, may cause anatomic changes ofthe RPE that are seen as small PEDs and punctate leakageon FA, with subsequent development of serous RD. In thecurrent series of eyes with dome-shaped macula, punctatehypercyanescent spots on ICGA were not associated withfocal areas of choroidal hyperpermeability; this is notconsistent with CSC, where these changes are observedin more than 90% of the cases including unaffected felloweyes.14 This may be explained by substantially differentamounts and location of choroidal abnormalities betweendome-shaped macula and CSC. Indeed, peculiar choroidalchanges (eg, punctate hypercyanescent spots on late-phaseICGA) are localized only inside the inward bulge withinthe posterior staphyloma of highly myopic eyes withdome-shaped macula. On the contrary, in CSC choroidalvascular abnormalities are seen not only posteriorly butalso outside the vascular arcade, indicating a widespreadinvolvement of the choroid. Other important differencesbetween dome-shaped macula and CSC eyes are the extent
50 AMERICAN JOURNAL OF
of subfoveal choroidal thickness, as well as the pattern ofchanges in retinal and choroidal thickness over time. Aspreviously described by Imamura and associates, eyes withCSC have a much greater subfoveal choroidal thicknessthan highly myopic eyes with dome-shaped macula.2 Inaddition, choroidal thickness in CSC eyes is significantlyreduced after the spontaneous resolution of serous RDand reduction of retinal thickness.15 On the contrary,changes in subfoveal retinal thickness for improvement/resolution of serous RD did not correspond to similarchanges in subfoveal choroidal thickness in our series ofeyes with dome-shaped macula. Because choroidal vascularabnormalities in dome-shaped macula are limited to themacular bulge area, they may not be sufficient to createvisible changes over time in the overall choroidal perme-ability and thickness, as seen in real CSC eyes. This hy-pothesis may also explain limited cases reporting CSC inmyopic eyes without dome-shaped macula.6 For all theabove reasons, we agree with previous investigators that apathophysiologic mechanism similar to CSC is unlikelyin dome-shaped macula; in other words, serous RD indome-shaped macula is not the result of a real CSC.An interesting finding of the present study was the strong
correlation between subfoveal choroidal thickness, scleralthickness, and macular bulge height. Not surprisingly,choroidal and scleral thicknesses were strictly related;this was likely owing to the myopic elongation of theeyeball. Indeed, previous investigators have shown thatwith increasing axial length there was a progressive thin-ning of both choroid and sclera.16–18 More interestingwas the association between scleral thickness and bulgeheight. It has been reported that the mean scleralthickness in cadaver eyes is 0.90 mm19 and in highlymyopic eyes without dome-shaped macula is 0.28 mm.2
In the present study, and consistent with the literature,2,18
the scleral thickness of dome-shaped macula eyes had amean value of 0.57 mm, which is within the range betweennormal eyes and highly myopic eyes. Ohsugi end associateshave recently demonstrated that the difference betweensubfoveal scleral thickness and average thickness of theperifovea was correlated with the mean bulge height.18
Similarly, we found that the greater was the bulge height,the greater was the subfoveal scleral thickness. Therefore,we agree with previous investigators that the dome-shaped macula is likely the result of a relative thickeningof the sclera in the fovea compared with the surroundingareas,18 as a possible adaptive or compensatory responseto the myopic ocular expansion.2 Finally, our data alsoshowed that the greater the scleral thickness or the bulgeheight, the greater the subfoveal choroidal thickness.This finding was also reported by Caillaux and associates.4
As speculated by Imamura and associates,2 scleral thick-ening within the bulge may locally affect the outflow ofchoroidal fluid and eventually lead to a thickened choroid.In summary, our data suggest that the cause of localizedchoroidal abnormalities and thickening in dome-shaped
JANUARY 2015OPHTHALMOLOGY

macula is a combined mechanical and vascular damage tothe choroid by an excessive scleral thickening within thestaphyloma. Consequently, impairment of the RPE occurs,small PEDs develop, and serous RD occurs at the top of theinward bulge from a slow choroidal leakage. However,while choroidal thickening tends to be permanent indome-shaped macula, choroidal vascular abnormalitiesare temporary and lead to changes in serous RD over time.
The angiographic findings in our eyes with dome-shapedmacula also resembled typical findings seen in tilted discsyndrome.9 However, in tilted disc syndrome there is anormal curvature of the sclera and a second curvaturethat corresponds to the outward protrusion of the inferiorsclera. In addition, the pathogenesis of dome-shaped mac-ula and tilted disc syndrome seems to be quite different, asalso supported by previously reported angiographic findingsin tilted disc syndrome cases.8,9 Hypercyanescence at theborder of the inferior staphyloma on late-phase ICGAwas observed in only 0% to 38% of the cases, and activefocal leakage on FA was absent as well.8,9 Moreover,these studies reported a foveal choroidal thinning intilted disc syndrome eyes with serous RD, postulating acontribution to a focal disturbance in the choroidalcirculation. Eventually, serous RD in tilted disc syndromerarely shows spontaneous resolution or a fluctuatingcourse.7 Therefore, the mechanism of serous RD develop-ment in tilted disc syndrome seems to be more related tomechanical forces on choroidal layers at the macula causedby anatomic disturbances at the superior border of thestaphyloma.8 As a consequence, RPE atrophy could causea breakdown of the blood-retinal barrier and a subsequentserous RD.
To date, there is no validated therapy for serous RD sec-ondary to dome-shaped macula. However, considering thatpunctate hypercyanescent spots arising from the choroidalvasculature seem to have a role in its pathogenesis, wesuggest targeting the choroid for a possible treatment. Acc-ording to our hypothesis of CSC-like appearance of dome-shaped macula, ICG-guided photodynamic therapy may berecommended as potential treatment in the active stage ofthe disease, as previously suggested.3 In addition, targetingthe choroid is also supported by the fact that the choroidwas significantly thicker in the group of eyes with serousRD than in the group of eyes without serous RD, as alsorecently reported by Errera and associates.20 However,considering that resolution of serous RD is common inthis pathology, we suggest that possible treatments beconsidered only in the few cases of persistent or quicklyrecurrent serous RD with significant impairment of a
VOL. 159, NO. 1 CHOROIDAL FINDINGS IN MYOP
patient’s visual function. Further longitudinal studies aremandatory to verify the usefulness of this treatment hy-pothesis.The current study has a number of limitations. First
among these is its retrospective nature; however, our obser-vational study is the largest series of reported cases of dome-shaped macula in highly myopic eyes, and because patientswere not treated it may be considered a comprehensivedescription of the natural history of the disease. Second,because this is a specialty clinic–based study, it is difficultto assess precisely the prevalence of macular complicationsof dome-shaped macula in the general population. Third,all measurements of choroidal and scleral thicknesseswere carried out manually using a built-in caliper of theSD OCT device; novel choroidal segmentation softwaremay help in future studies about this disease. Finally,because choroidal thickness fluctuates during daytime,measurements may have been influenced by the time ofthe SD OCT examination. However, previous investiga-tors have shown that in thin choroids (ie, with subfovealchoroidal thickness <200 mm) there was no significantfluctuation in thickness in the morning.21 Consideringthat our myopic patients had a mean choroidal thicknessof 133 mm and that they were imaged between 8 AM and11 AM, it is therefore unlikely that diurnal changes inchoroidal thickness substantially confounded the resultsof this study.In summary, foveal serous RD associated with dome-
shaped macula seems to resemble acute CSC in highlymyopic eyes, but the pathophysiologic mechanism is quitedifferent. In dome-shaped macula serous RD is likely causedby choroidal vascular changes secondary to excessive thick-ening of the sclera. Such changes are present only inside theinward bulge within the posterior staphyloma and notwidely spread in the entire choroid like in CSC. Dome-shaped macula in highly myopic eyes may also resembletilted disc syndrome complicated by serous RD; however,angiographic and tomographic findings suggest that these2 diseases have a quite different pathogenesis. Dome-shaped macula presents a fluctuating change in serous RDover time, with alternating active and inactive stages, asdemonstrated by the presence/absence of punctate leakingpoints on FA and hypercyanescent spots and ICGA arisingfrom the choroidal vasculature. Although it appears thatchoroidal changes are associated with dome-shaped mac-ula, the clinical importance of this finding, as well as the po-tential factors influencing the presence or development ofchoroidal changes, remains obscure and should be furtherinvestigated to suggest possible treatments.
THE AUTHORS HAVE COMPLETED AND SUBMITTED THE ICMJE FORM FOR DISCLOSURE OF POTENTIAL CONFLICTS OF INTERESTand none were reported. The authors indicate no funding support. Contributions of authors: design and conduct of the study (F.V., L.D.A., E.B., A.I.);collection and management of the data (F.V., L.D.A., E.B., A.I., C.M., F.F.); analysis and interpretation of the data (G.B., F.V., G.S., R.R.); and prepa-ration of the draft (F.V., G.B., A.I.); review and approval of the manuscript (G.B., F.V., G.S.).
The authors thank Laura Conner, MS (University Hospitals Case Medical Center, Cleveland, Ohio) for helping with the revision of the manuscript.
51IC DOME-SHAPED MACULA

REFERENCES
1. Gaucher D, Erginay A, Lecleire-Collet A, et al. Dome-shapedmacula in eyes with myopic posterior staphyloma. Am JOphthalmol 2008;145(5):909–914.
2. Imamura Y, Iida T, Maruko I, Zweifel SA, Spaide RF.Enhanced depth imaging optical coherence tomography ofthe sclera in dome-shaped macula. Am J Ophthalmol 2011;151(2):297–302.
3. Ellabban AA, Tsujikawa A, Matsumoto A, et al. Three-dimensional tomographic features of dome-shaped maculaby swept-source optical coherence tomography. Am JOphthalmol 2013;155(2):320–328.e2.
4. Caillaux V, Gaucher D, Gualino V, Massin P, Tadayoni R,Gaudric A. Morphologic characterization of dome-shapedmacula in myopic eyes with serous macular detachment.Am J Ophthalmol 2013;156(5):958–967.e1.
5. Coco RM, Sanabria MR, Alegria J. Pathology associated withoptical coherence tomography macular bending due to eitherdome-shaped macula or inferior staphyloma in myopicpatients. Ophthalmologica 2012;228(1):7–12.
6. Yzer S, Fung AT, Barbazetto I, Yannuzzi LA, Freund KB.Central serous chorioretinopathy in myopic patients. ArchOphthalmol 2012;130(10):1339–1340.
7. Cohen SY, Quentel G, Guiberteau B, Delahaye-Mazza C,Gaudric A. Macular serous retinal detachment caused bysubretinal leakage in tilted disc syndrome. Ophthalmology1998;105(10):1831–1834.
8. Nakanishi H, Tsujikawa A, Gotoh N, et al. Macular compli-cations on the border of an inferior staphyloma associatedwith tilted disc syndrome. Retina 2008;28(10):1493–1501.
9. Maruko I, Iida T, Sugano Y, Oyamada H, Sekiryu T.Morphologic choroidal and scleral changes at the maculain tilted disc syndrome with staphyloma using optical coher-ence tomography. Invest Ophthalmol Vis Sci 2011;52(12):8763–8768.
10. Curtin BJ. The posterior staphyloma of pathologic myopia.Trans Am Ophthalmol Soc 1977;75:67–86.
11. Barteselli G, Bartsch DU, Viola F, et al. Accuracy of the Hei-delberg Spectralis in the alignment between near-infrared
52 AMERICAN JOURNAL OF
image and tomographic scan in a model eye: a multicenterstudy. Am J Ophthalmol 2013;156(3):588–592.
12. Chhablani J, Barteselli G, Wang H, et al. Repeatability andreproducibility of manual choroidal volume measurementsusing enhanced depth imaging optical coherence tomogra-phy. Invest Ophthalmol Vis Sci 2012;53(4):2274–2280.
13. Tsujikawa A, Ojima Y, Yamashiro K, et al. Punctate hyper-fluorescent spots associated with central serous chorioretin-opathy as seen on indocyanine green angiography. Retina2010;30(5):801–809.
14. Iida T, Kishi S, Hagimura N, Shimizu K. Persistent and bilat-eral choroidal vascular abnormalities in central serouschorioretinopathy. Retina 1999;19(6):508–512.
15. Kang NH, Kim YT. Change in subfoveal choroidal thicknessin central serous chorioretinopathy following spontaneousresolution and low-fluence photodynamic therapy. Eye
(Lond) 2013;27(3):387–391.16. Fujiwara T, Imamura Y, Margolis R, Slakter JS, Spaide RF.
Enhanced depth imaging optical coherence tomography ofthe choroid in highly myopic eyes. Am J Ophthalmol 2009;148(3):445–450.
17. Barteselli G, Lee SN, El-Emam S, et al. Macular choroidalvolume variations in highly myopic eyes withmyopic tractionmaculopathy and choroidal neovascularization. Retina 2014;34(5):880–889.
18. Ohsugi H, Ikuno Y, Oshima K, Yamauchi T, Tabuchi H.Morphologic characteristics of macular complications of adome-shaped macula determined by swept-source opticalcoherence tomography. Am J Ophthalmol 2014;158(1):162–170.e1.
19. Olsen TW, Aaberg SY, Geroski DH, Edelhauser HF. Humansclera: thickness and surface area. Am J Ophthalmol 1998;125(2):237–241.
20. Errera MH, Michaelides M, Keane PA, et al. The extendedclinical phenotype of dome-shaped macula. Graefes ArchClin Exp Ophthalmol 2014;252(3):499–508.
21. Lee SW, Yu SY, Seo KH, Kim ES, Kwak HW. Diurnal varia-tion in choroidal thickness in relation to sex, axial length,and baseline choroidal thickness in healthy Korean subjects.Retina 2014;34(2):385–393.
JANUARY 2015OPHTHALMOLOGY