Embed Size (px)
Citation preview

CHOICE OF ANTIBIOTICS IN THE VIEW OF DEVELOPING ANTIBIOTIC RESISTANCE
Dr. Jolanta Miciulevičienė
Vilnius City Clinical HospitalNational Public Health Surveillance Laboratory
BARN 3rd Workshop ʺPrevention of Surgical Site InfectionsʺVisby, 2012

In 1928 Sir Alexander Fleming, a Scottish bacteriologist, left a Petri dish with staphylococci uncovered. When he returned, he noticed that there was mold growing on it. Upon further examination, he saw that the area around the mold had no bacteria growing.
Fleming concluded that the mold was releasing a substance that was inhibiting bacterial growth. He grew a pure culture of the mold and discovered that it was a Penicillium, now known to be Penicillium notatum.
Discovery of Penicillin Changes theHistory of Medicine


Antimicrobial resistance
• Soon after the introduction of the penicillin into clinical practice, the fact that the development of antibiotic resistance would be a problem became apparent.
• Resistance to penicillin in some strains of Staphylococcus was recognized almost immediately after introduction of the drugs. Resistance to penicillin today occurs in as many as 90% of all strains of Staphylococcus aureus

Most commonly, this refers to infectious microbes that have acquired the ability to survive exposures to clinically relevant concentrations of antimicrobial drugs that would kill otherwise sensitive organisms of the same strain.
Antimicrobial resistance

• S.aureus (MRSA, GISA),• Enterococcus spp. (VRE),• E.coli (ESBL),• Klebsiella pneumoniae (ESBL, KPC),• Enterobacteriaceae (MDR),• Pseudomonas aeruginosa (MDR),• Acinobacter baumannii (MDR).
Resistant Nosocomial Pathogens

Streptococcus pneumoniae,Staphylococcus aureus,Enterococcus faecalis,Enterococcus faeciumEscherichia coli,Klebsiella pneumoniae,Pseudomonas aeruginosa.
European Antimicrobial Resistance Surveillance Network (EARS – Net)

EARS – Net participants in Lithuania: 10 laboratories of microbiology 37 hospitals

Number of blood-stream infections, Lithuania, 2007 – 2011

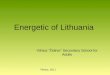
Staphylococcus aureus: trends of invasive isolates resistant to meticillin (MRSA),Lithuania, 2007-2011
2007m. - 241/22, 2008m. - 280/31, 2009m. - 255/29, 2010m. – 257/36, 2011m. – 263/16

Staphylococcus aureus: proportion (%) of invasive isolates resistant to methicillin (MRSA), 2010

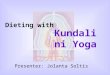
Klebsiella pneumoniae: trends of invasive isolates resistance to third-generation cephalosporins,
fluoroquinolones and aminoglycosides, Lithuania, 2007-2011

Klebsiella pneumoniae: proportion (%) of invasive isolates with resistance to third-generation cephalosporins, 2010

Klebsiella pneumoniae: proportion (%) of invasive isolates with resistance to carbapenems, 2010

Number of K.pneumoniae blood stream infections, Lithuania, 2007-2011.

Risk factors of developing bacterial resistance
• Inappropriate prescribing (overprescribing);
• Inappropriate selection of antimicrobial (broad spectrum cephalosporins, fluoroquinolones, carbapenems, glycopeptides);
• Prolonged administration of antimicrobial.

Evidence Based
• “Evidence-based medicine is the process of systematically finding, appraising, and using research findings as the basis for clinical decisions.”
BMJ 1995;310:1122-1126 (29 April)
William Rosenberg, Anna Donald
Evidence-based Medicine: An Approach to Clinical Problem-solving

Evidence-based medicine
Reference:
Cook PP, Catrou P, Gooch M, Holbert D. Effect of reduction in ciprofloxacin use on prevalence of methicillin-resistant Staphylococcus aureus rates within individual units of a tertiary care hospital. Journal of Hospital Infection. 2006; 64: 348-351
Setting:
731-bed tertiary care teaching hospital, Greenville, NC, USA.

Evidence based medicine
• Intervention
Reduction - Active monitoring of oral and IV ciprofloxacin use. • Impact:
Ciprofloxacin use decreased by 31.2% (p<0.0001). MRSA rates decreased from 59.6% to 54.2% (p=0.112). Correlation between ciprofloxacin use and MRSA rates (r=0.70; 95% CI -0.01-0.94 p=0.053).

Evidence based medicine
• Reference:
Rahal JJ, Urban C, Horn D, Freeman K, Segal-Maurer S, Maurer J, Mariano N, Marks S, Burns JM, Dominick D, Lim M. Class restriction of cephalosporin use to control total cephalosporin resistance in nosocomial Klebsiella. JAMA, 1998;280(14): 1233-1237
• Setting:
500-bed university affiliated community hospital, Queens, NY, USA

Evidence based medicine
• Intervention
Restriction - Hospital adopted antibiotic guidelines restricting routine cephalosporin use.
• Impact:
80.1% reduction in hospital-wide cephalosporin use in 1996 compared to 1995. 44% reduction in incidence of ceftazidime-resistant Klebsiella infection and colonization throughout medical center (p<0.01) and 70.9% reduction in all intensive care units (p<0.001).

Evidence based medicine
• Intervention
Restriction - Hospital adopted antibiotic guidelines restricting routine cephalosporin use.
• Impact:
80.1% reduction in hospital-wide cephalosporin use in 1996 compared to 1995. 44% reduction in incidence of ceftazidime-resistant Klebsiella infection and colonization throughout medical center (p<0.01) and 70.9% reduction in all intensive care units (p<0.001).

Take home message:
Inappropriate selection and prolonged administration of antimicrobials
Fluoroquinolones;Cephalosporins;Carbapenems; Glycopeptides.
S.aureus (MRSA, GISA),Enterococcus spp. (VRE),E.coli (ESBL),Klebsiella pneumoniae (ESBL, KPC),Enterobacteriaceae (MDR),Pseudomonas aeruginosa (MDR),Acinobacter baumannii (MDR).
THANK YOU !