-
8/3/2019 CHMI Report 112711 High Links
1/32
HIGHLIGHTS: 201
-
8/3/2019 CHMI Report 112711 High Links
2/32
ABOUT THE CENTER FOR HEALTH MARKET INNOVATIONS:
The Center or Health Market Innovations (CHMI) accelerates
innovative health initiatives by inorming and connecting
program managers, unders, researchers, and policy makers who
strive to create better health markets or the poor. CHMI is
the worlds largest reely accessible web platorm on programs
improving the access, quality, and aordability o privately
delivered health care or the poor. Funded by the Bill &
Melinda Gates Foundation and the Rockeeller Foundation, CHMI is
a global network o partners coordinated by the Results or
Development Institute.
ABOUT THIS REPORT:
This report was compiled by the Center or Health Market
Innovations team at the Results or Development Institute with
contributions rom CHMI partners (below). Maria Belenky, Donika
Dimovska, Gina Lagomarsino, Trevor Lewis, and Rose
Reis contributed content. The observations highlighted in this
report are valid as o September 2011. For more up-to-date
gures, please visit www.HealthMarketInnovations.org.
UCSFs Global Health Group
Results for Development
Institute
BroadReachh e a l t h c a r e
I ns t i t u t e o f Heal t h Pol icy , Management &
Research
http://healthmarketinnovations.org/content/chmi-partnershttp://healthmarketinnovations.org/http://healthmarketinnovations.org/http://healthmarketinnovations.org/content/chmi-partners
-
8/3/2019 CHMI Report 112711 High Links
3/32
Dear Colleagues,
In July 2010, we launched the Center or Health Market
Innovations (CHMI; www.healthmarketinnovations.org). Today,
with more than 75,000 visitors rom 190 countries, CHMI is the
worlds largest reely accessible web platorm on programs
improving the access, quality, and aordability o privately
delivered health care or the poor.
This report highlights key observations about innovative,
market-based health programs based on CHMIs initial phase o
operation. We hope you will nd this inormation useul in
advancing your work.
Our recent progress includes:
Or1000romiinHlhMrkInnoionidnidinmorhn100conri. CHMIs partners in
16
countries identiy programs that are aggregated on our website in
an interactive, downloadable Programs Database.
RordRliniiilnchdodicorwhworkin.CHMI is beginning to create an
evidence base
to identiy eective programs through our new Reported Results
initiative. Programs now report their results in such
areas as quality, cost, and eciency.
Nwinihohlhmrk. Weve identied promising practices and new program
models spreading
around the world. CHMI also commissions research about market
challenges like drug quality in India and inormal
providerspracticing in Bangladesh, India, and Nigeria.
Nworkokykholdrcrd. More than 300 program managers, unders,
researchers, and policy makers
have attended CHMI events in Indonesia, Brazil, Pakistan, the
Philippines, and Kenyato discuss innovations in their
countries.
CHMI will continue to identiy and analyze market-based
innovations and connect people to acilitate the scale up o
whats working. We invite you to:
Lrnmor onwmrk-drorm. Search our Programs Database to locate
health initiatives by
Program Type, Health Focus, Target Population, or Legal
Status.Knowoninnoirorm?Adda new program
prole, update a listing, or write about it on the CHMI Blog.
Lknowwhwork.Report results or programs that you manage, und, or
study.
Conncwihinnoor. Join CHMI to directly contact people running
programs listed in CHMIs database. Have
conversations with the Health Market Innovations community on
CHMIs Blog.
Downlodord. The CHMI database is reely available or the public.
Use CHMI lters to browse the Programs
Database or a slice o interest, or download the entire
databasetoconduct analysis.
We welcome your suggestions and eedback and look orward to
sharing uture updates on topics relevant to health
markets in developing countries.
Sincerely,
Gina Lagomarsino
Results or Development Institute (R4D)
On behal o the CHMI Network
http://www.healthmarketinnovations.org/http://healthmarketinnovations.org/about/chmi-partners/analytic-partnershttp://healthmarketinnovations.org/http://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_reported_results-2386http://healthmarketinnovations.org/emerging-health-market-innovationshttp://healthmarketinnovations.org/health-market-studies#drugretailhttp://healthmarketinnovations.org/health-market-studies#informalprovidershttp://healthmarketinnovations.org/health-market-studies#informalprovidershttp://healthmarketinnovations.org/blog/2011/aug/24/dispatch-indonesiahttp://healthmarketinnovations.org/blog/2011/jun/16/what-innovators-brazil-can-learn-flexible-dynamic-indian-subcontinenthttp://healthmarketinnovations.org/blog/2011/may/23/asia-foundation-roundtable-islamabadhttp://healthmarketinnovations.org/blog/2011/jul/14/philippines-institute-development-studies-works-identify-key-health-market-innovatihttp://healthmarketinnovations.org/blog/2011/feb/28/just-back-kenyahttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/node/add/program-summary-formhttp://healthmarketinnovations.org/node/add/program-summary-formhttp://healthmarketinnovations.org/node/add/program-change-requesthttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/user/registerhttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/user/registerhttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/node/add/program-change-requesthttp://healthmarketinnovations.org/node/add/program-summary-formhttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/blog/2011/feb/28/just-back-kenyahttp://healthmarketinnovations.org/blog/2011/jul/14/philippines-institute-development-studies-works-identify-key-health-market-innovatihttp://healthmarketinnovations.org/blog/2011/may/23/asia-foundation-roundtable-islamabadhttp://healthmarketinnovations.org/blog/2011/jun/16/what-innovators-brazil-can-learn-flexible-dynamic-indian-subcontinenthttp://healthmarketinnovations.org/blog/2011/aug/24/dispatch-indonesiahttp://healthmarketinnovations.org/health-market-studies#informalprovidershttp://healthmarketinnovations.org/health-market-studies#informalprovidershttp://healthmarketinnovations.org/health-market-studies#drugretailhttp://healthmarketinnovations.org/emerging-health-market-innovationshttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_reported_results-2386http://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/http://healthmarketinnovations.org/about/chmi-partners/analytic-partnershttp://www.healthmarketinnovations.org/
-
8/3/2019 CHMI Report 112711 High Links
4/32
TABLE OF CONTENTS
5MappINgHeaLtHMaRKetINNOvatIONs
7 OveRvIewOfHeaLtHMaRKetINNOvatIONs
10 ObseRvatIONsabOutHeaLtHMaRKets10 Organizing private providers
to deliver priority health interventions
12 Giving purchasing power to the poor
14 Using technology to improve access, quality, and eciency o
care
18 Funding or innovative programs
20 fIveINNOvatIveMODeLsappeaRINgaROuNDtHewORLD
24buILDINgtHeevIDeNCebaseabOutwHatwORKs
26 CReatINgagLObaLNetwORK26 Personal connections
26 Virtual connections
28 useCHMItOsuppORtYOuRwORK
-
8/3/2019 CHMI Report 112711 High Links
5/32CENTER FOR HEALTH MARKET INNOVATIONS5
Mapping HealtH MarketInnovatIons
The Center or Health Market Innovations (CHMI) was established
in 2010 to accelerate innovative
health initiatives around the world by inorming and connecting
program managers, unders,
researchers, and policy makers who strive to create better
health markets or the poor. CHMIs long-
term aspiration is to improve the access, quality, and
aordability o privately delivered health care
or the poor.
CHMI works through a network o in-country partners1 to identiy,
document, and promote
the diusion oHlhMrk Innoion. These are promising programs and
policies
implemented by governments, non-governmental organizations
(NGOs), social entrepreneurs,
or private companiesthat have the potential to improve the way
health markets operate or
the poor.
Hlhmrkri. In many countries, most health care expenditures occur
through private transactions
even when governments oer ree care at public acilities. In at
least 17 countries in Asia and 16 countries in A-
rica, more than halo all health spending is made up o
out-o-pocket payments rom consumers.2
thooronrlyonhlhmrk. In most developing countries, the poor rely
on private health care provid-
ers or a large portion o their care. In Sub-Saharan Arica and
South Asia, they use the private sector just as much as
the rich.
Hlhmrkcncrmnychlln.Patients do not always seek the kind o care
that will make them
healthier, and providers do not always act in patients best
interests.4 Appropriate care is oten expensive and pushes
people urther into poverty. According to the World Health
Organization, each year, 150 million people globally
ace severe nancial hardship, 100 million are orced into poverty,
and many orgo or delay care because they lack
nancial resources.3
Hlhmrkcnhrndoimrohlhorhoor.When well-monitored and regulated,
health
markets can be a source o creative new approaches with the
potential to achieve greater eciencies, improved
quality, and increased access to care or underserved
populations.
WHy ocus on IMprovIng HealtH Markets?
http://users/Home/Dropbox/CHMI-FirstYearReport/CHMI-report-112711%20Folder/sh%20HD/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/MacOS/Users/R4D/AppData/Local/Adobe/InDesign/Version%207.5/en_GB/Caches/InDesign%20ClipboardScrap1.pdfhttp://healthmarketinnovations.org/sites/healthmarketinnovations.org/files/Table_OPP.pnghttp://healthmarketinnovations.org/sites/healthmarketinnovations.org/files/Table_privatebyquintile_2.pnghttp://healthmarketinnovations.org/sites/healthmarketinnovations.org/files/Table_privatebyquintile_2.pnghttp://healthmarketinnovations.org/sites/healthmarketinnovations.org/files/Table_OPP.pnghttp://users/Home/Dropbox/CHMI-FirstYearReport/CHMI-report-112711%20Folder/sh%20HD/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/Applications/Adobe%20InDesign%20CS5/Adobe%20InDesign%20CS5.app/Contents/MacOS/Users/R4D/AppData/Local/Adobe/InDesign/Version%207.5/en_GB/Caches/InDesign%20ClipboardScrap1.pdf
-
8/3/2019 CHMI Report 112711 High Links
6/32
-
8/3/2019 CHMI Report 112711 High Links
7/32CENTER FOR HEALTH MARKET INNOVATIONS7
Overview of HealtH MarketInnovatIons
The CHMI database contains online proles o more than 1000
programs and policies with the
potential to improve the quality and aordability o privately
delivered health care or the poor
in low- and middle-income countries (Figure 2). Each prole
provides inormation about the
programs operational design, including health ocus areas,
targeted populations, unding sources,
and where available, results to date.
Inhr,CHMIrormrolyildmcro-ll
inormiono innoionin hlhmrklolly. With the collection o data
over
time, CHMI will continue to identiy, analyze, and report on
Health Market Innovations and provide
insights into patterns observed.
prormty:CHMIs rst year o scanning has yielded more than 1000
programs in 107
countries. Most programs organize delivery, change consumer and
provider behavior,
or enhance operational processes (Figure 3); some multi-aceted
programs do all three.
Programs that leverage inormation technology or health represent
more than a quarter o
all documented programs.
Fu 2: cHMI Db oiw (smb 2011)
nmb pfd pm 1015
nmb ci d 107
*Some programs are categorized into more than one program
type.
Fu 3: nmb cHMI pm b m *
-
8/3/2019 CHMI Report 112711 High Links
8/32CENTER FOR HEALTH MARKET INNOVATIONS8
Hlhfoc:Health Market Innovations cover a wide array o health
areas. Programs ocusing
on general primary care are prevalent among those proled by CHMI
in its rst year. Programstargeting HIV/AIDS, amily planning and
reproductive health, and maternal and child health
make up about hal o the database. CHMI identied ewer
market-based programs ocusing
on inectious diseases such as malaria and tuberculosis, though
some large and infuential
initiatives, such as the Aordable Medicines Facility or Malaria
(AMFM) have recently launched.7
Chronic disease care, emergency care, eye care, nutrition,
dental care, rehabilitative care, and
mental health were also identied as areas o market-based
activity in health (Figure 4).
Lls:A little over hal o CHMI-proled programs are operated by
private, not-or-prot
organizations, and one out o ve operates as a public-private
partnership. Pro-poor, or-prot
health care models represent 10% o the database. Programs in
this category are largely service
delivery organizations (e.g., hospital chains and retail
pharmacies) and technology-enabled
programs (e.g., telemedicine networks and health hotlines).
Government-led initiatives such
as health nancing programs and accreditation policies make up 7%
o all proled innovations(Figure 5).
ConryoOrion: CHMI has identied innovation in all regions,
particularly in South
Asia and East Arica, with many programs in India and Kenya,
refecting high private-sector
activity as well as the presence o CHMI partners.However, a
variety o innovative models can
be ound across all countries scanned by CHMI: rom Vietnam to
Uganda, rom Pakistan to
Peru, and rom Indonesia to Brazil (Figure 6). An interactive map
o all CHMI programs is online
at tinyurl.com/CHMImap.
Fu 4: nmb cHMI-fd m b hh
General Primary Care
HIV/AIDS
Family Planning & Reproductive Health
Maternal & Child Health
General Secondary/Tertiary Care
Tuberculosis
Malaria
Chronic Diseases
Emergency Care
Eye Care
Nutrition
Rehabilitative Care
Mental Health
Dentistry
Other/Not Applicable
264
256
190
181
120
60
59
46
42
37
32
19
15
7
81
http://healthmarketinnovations.org/program/affordable-medicines-facility-malaria-amfmhttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-169&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?display=default&sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-177http://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-276&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?display=default&sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-269&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-229&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-226&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-166&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-114&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?search=&display=views-mode-maphttp://healthmarketinnovations.org/programs/browse?search=&display=views-mode-maphttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-114&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-166&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-226&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-229&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?display=default&sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-269&display=defaulthttp://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-276&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/programs/browse?display=default&sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-177http://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_country_ies_of_operation-169&display=views-mode-map&display=defaulthttp://healthmarketinnovations.org/program/affordable-medicines-facility-malaria-amfm
-
8/3/2019 CHMI Report 112711 High Links
9/32CENTER FOR HEALTH MARKET INNOVATIONS9
Fu 6: ghi diibi m*
* Numbers and sizes o dots indicate number o programs by
country. An interactive version o the map can be ound online at
www.healthmarketinnovations.org.
57%
22%
10%
7%
3%
2%
Private (not- for-profit)
Public-private partnership
Private (for-profit)
State/government
Private (unspecified)
Corporate program
Fu 5: p cHMI-fd m b
http://www.healthmarketinnovations.org/http://www.healthmarketinnovations.org/
-
8/3/2019 CHMI Report 112711 High Links
10/32
-
8/3/2019 CHMI Report 112711 High Links
11/32CENTER FOR HEALTH MARKET INNOVATIONS1
socilrnchi.CHMI documents over 60 social ranchises operating in
over 30 countries
around the world. Franchising has gained popularity in recent
years as an eective mechanism
to organize independent private providers to oer a range o
quality health services. Family
planning and reproductive health services are key areas o ocus
or most documented
ranchises, but many programs are beginning to expand beyond
these two areas, leveraging
their platorms to deliver TB, HIV/AIDS, and malaria
interventions. Franchises are also emerging
as a potential service delivery mechanism or the screening and
treatment o chronic diseases.
In Myanmar, Sun Quality Health is beginning to oer low-cost
cervical cancer screenings and
cryotherapy (the use o cold temperatures to destroy abnormal
tissue) through its network oranchised clinics. Similar initiatives
are underway in Kenya and Uganda.8
aordlroidrchin.Over 150 programs documented by CHMI are service
delivery
chains managing multiple sites that rely on standardized
operational processes. The majority
o these programs provide general primary care at rates aordable
to the poorAkhuwat
Clinics in Pakistan and Kriti Arogyam Kendram in India are two
recently launched examples
o this model. Other chains choose to ocus on low-cost
specialized services. Jacaranda Health
in Kenya and LieSpring in India provide sae delivery services.
Eye-Q Hospitals in India and
ASEMBIS in Costa Rica oer eye care services while
SorridentsandDentista do Bemprovide
dental care in Brazil.
pro-oorhoilndclinic.Close to 90 programs in the CHMI database
are standalonehospitals and clinics that aspire to serve the poor.
Many o these programs work in the areas
o chronic disease and secondary and tertiary care, but a large
number also provide general
primary care and maternal and child health services. Specialized
service models such as
Narayana Hrudayalaya Cardiac Hospital in India, the NICE
Foundation Institute o Newborn Care
also in India, and the Lumbini Eye Institutein Nepal use
standardized operational processes to
allow more patients to receive care while keeping costs low.
Some o these institutions pair
the high-volume approach with cross subsidization, directing
revenue rom wealthy patients
to cover the cost o care or the poor.
More inormation about innovative delivery models, including
retail pharmacy chains, telemedicine
models, aordable primary care models, and health hotlines, is
provided on page 20.
pid h id h ih i h nIce di Ii nwb c iHdbd, Idi.
http://healthmarketinnovations.org/program/sun-quality-health-network-myanmarhttp://healthmarketinnovations.org/program/akhuwat-healthhttp://healthmarketinnovations.org/program/akhuwat-healthhttp://healthmarketinnovations.org/program/kriti-arogyam-kendramhttp://healthmarketinnovations.org/program/jacaranda-healthhttp://healthmarketinnovations.org/program/lifespring-hospitals-private-limited-lhplhttp://healthmarketinnovations.org/program/eye-qhttp://healthmarketinnovations.org/program/asembishttp://healthmarketinnovations.org/program/sorridentshttp://healthmarketinnovations.org/program/dentista-do-bem-0http://healthmarketinnovations.org/program/narayana-hrudayalaya-hospital-nhhttp://healthmarketinnovations.org/program/nice-foundationhttp://healthmarketinnovations.org/program/lumbini-eye-institutehttp://healthmarketinnovations.org/program/lumbini-eye-institutehttp://healthmarketinnovations.org/program/nice-foundationhttp://healthmarketinnovations.org/program/narayana-hrudayalaya-hospital-nhhttp://healthmarketinnovations.org/program/dentista-do-bem-0http://healthmarketinnovations.org/program/sorridentshttp://healthmarketinnovations.org/program/asembishttp://healthmarketinnovations.org/program/eye-qhttp://healthmarketinnovations.org/program/lifespring-hospitals-private-limited-lhplhttp://healthmarketinnovations.org/program/jacaranda-healthhttp://healthmarketinnovations.org/program/kriti-arogyam-kendramhttp://healthmarketinnovations.org/program/akhuwat-healthhttp://healthmarketinnovations.org/program/akhuwat-healthhttp://healthmarketinnovations.org/program/sun-quality-health-network-myanmar
-
8/3/2019 CHMI Report 112711 High Links
12/32CENTER FOR HEALTH MARKET INNOVATIONS2
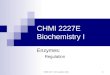
g u o o ooApproximately 200 programs in the CHMI database are
categorized as finncinCr (Figure 8). Demand-
side nancing programs such
asornmnhlhinrnc,riinrnc,microndcommniy
hlh inrnc, and ochr decrease nancial barriers to care by
enabling consumers to access
services rom their choice o provider, who is then reimbursed.
Other nancing tools include conrcin,
a supply-side intervention that channels government unds
directly to selected private providers to expand
their reach, cro-idizion,making care aordable or the poor by
channeling unds rom wealthier
patients, and mHlhinprograms that encourage consumers to save or
uture health care needs,oten through cell phone payment plans.
Figure 8 shows how programs use dierent kinds o nancing tools
to improve access to health services or the poor.
A closer look at ve common types o nancing care programs
documented by CHMI provides more insight
into promising initiatives that help poor amilies to pay or
care:
Fu 8: p m fi b hh
-
8/3/2019 CHMI Report 112711 High Links
13/32CENTER FOR HEALTH MARKET INNOVATIONS3
gornmnhlhinrnc.CHMI proles 27 national insurance schemes that
target the
poor to move toward universal health coverage. While some
schemes, such as Ghanas National
Health Insurance Scheme and Indonesias Jamkesmas, oer
comprehensive benets, others
such as Indias RSBY scheme, the Philippiness PhilHealth,9 and
Kenyas National Hospital
Insurance Fundcover primarily inpatient services, though each o
these schemes is now
working to expand to outpatient benets. (The Joint Learning
Network or Universal Health
Coveragehas produced case studies on national health insurance
reorms being implemented
by low- and middle-income countries.10)
Micro nd commniy hlh inrnc. CHMI documents 53 micro and
community
health insurance programs. They are common throughout parts o
Sub-Saharan Arica, South
Asia, and Latin America. Though they remain small in scale,
schemes such as those oered
by MicroEnsure, which recently expanded into Tanzania, and SKY
Microinsurance, operating
in Cambodia since 2007, oten target specic geographic or
economically linked communities
like armers cooperatives. Micro health insurance programs may
have the potential to
complement or become integrated with national schemes.
Twenty-two programs are ro-
oor, ri inrnc chm, allowing employers, various organized groups,
and
amilies to purchase health insurance at low rates.
Cro-idizion. Forty-two programs use this popular pro-poor
pricing model that
redirects revenue rom wealthy patients to cover those unable to
pay. Specialty eye hospitals,such as Aravind and L. V. Prasad Eye
Institute in India, oer vision screening and treatment
at tiered rates so that better o patients subsidize the care o
lower income patients. Cross-
subsidization is also commonly used to provide access to chronic
diseases and in-patient
health services.
vochr. Twenty-nine programs use vouchers to help the poor access
reproductive health
and maternal and child-care services. O all CHMI-proled programs
nancing reproductive
health services, 75% are vouchers that women can redeem or
services like amily planning. O
all nancing programs improving access to maternal and child
care, 50% are voucher programs.
While they are still small in scale, the number o CHMI-proled
voucher programs launched
ater 2006 is more than double the number o voucher programs
started between 2000 and
2006. The Kenya Output-Based Aid Voucher Program or amily
planning and reproductive
health services is a well-known example o this model.
gornmnconrcin.CHMI proles 73 programs that contract with private
providers.
Contracting is oten used to nance emergency care, particularly
in India where state
governments have contracted companies such as Ziqitzaor groups o
private providers such
as the Janani Express model in Madhya Pradeshto operate
ambulance networks.Contracting
is also oten used to expand the availability o key health
interventions such as basic primary
care and maternal and child health services, health areas
accounting or hal o all contracting
initiatives. In Bangladesh, the government implements theUrban
Primary Health Care Project,
which contracts out primary health care services to
non-governmental organizations working
in low-income urban areas.
http://healthmarketinnovations.org/program/ghana-national-health-insurance-schemehttp://healthmarketinnovations.org/program/ghana-national-health-insurance-schemehttp://healthmarketinnovations.org/program/ghana-national-health-insurance-schemehttp://healthmarketinnovations.org/program/jamkesmas-schemehttp://healthmarketinnovations.org/program/rashtriya-swasthya-bima-yojana-rsbyhttp://healthmarketinnovations.org/program/rashtriya-swasthya-bima-yojana-rsbyhttp://healthmarketinnovations.org/program/philhealthhttp://jointlearningnetwork.org/content/national-hospital-insurance-fundhttp://jointlearningnetwork.org/content/national-hospital-insurance-fundhttp://www.jointlearningnetwork.org/http://www.jointlearningnetwork.org/http://www.jointlearningnetwork.org/http://healthmarketinnovations.org/program/microensure-0http://healthmarketinnovations.org/program/sokapheap-krousat-yeugn-sky-micro-health-insurancehttp://healthmarketinnovations.org/program/aravind-eye-care-system-aecshttp://healthmarketinnovations.org/program/l-v-prasad-eye-institute-lvpeihttp://healthmarketinnovations.org/program/national-hospital-insurance-fund-nhifhttp://healthmarketinnovations.org/program/bangladesh-second-urban-primary-health-care-projecthttp://healthmarketinnovations.org/program/bangladesh-second-urban-primary-health-care-projecthttp://healthmarketinnovations.org/program/bangladesh-second-urban-primary-health-care-projecthttp://healthmarketinnovations.org/program/national-hospital-insurance-fund-nhifhttp://healthmarketinnovations.org/program/l-v-prasad-eye-institute-lvpeihttp://healthmarketinnovations.org/program/aravind-eye-care-system-aecshttp://healthmarketinnovations.org/program/sokapheap-krousat-yeugn-sky-micro-health-insurancehttp://healthmarketinnovations.org/program/microensure-0http://www.jointlearningnetwork.org/http://www.jointlearningnetwork.org/http://jointlearningnetwork.org/content/national-hospital-insurance-fundhttp://jointlearningnetwork.org/content/national-hospital-insurance-fundhttp://healthmarketinnovations.org/program/philhealthhttp://healthmarketinnovations.org/program/rashtriya-swasthya-bima-yojana-rsbyhttp://healthmarketinnovations.org/program/rashtriya-swasthya-bima-yojana-rsbyhttp://healthmarketinnovations.org/program/jamkesmas-schemehttp://healthmarketinnovations.org/program/ghana-national-health-insurance-schemehttp://healthmarketinnovations.org/program/ghana-national-health-insurance-scheme
-
8/3/2019 CHMI Report 112711 High Links
14/32CENTER FOR HEALTH MARKET INNOVATIONS4
U oloy o mo , quly, dfy o eHealth, the use o inormation and
communication technology or health, has become
increasingly common in recent years. CHMI has identied more than
260 technology-enabled
programs, such as a health insurance scheme whose client
interactions are entirely through smart
cards and primary care clinics that use cell phones or patient
ollow-ups. CHMI analyzed these 260
programs to better understand the types o technologies most
commonly used and the reasons
technology was employed. These programs can be ound worldwide
with larger clusters in Southand Southeast Asia and East Arica
(Figure 9).
Devices That Programs Use
In recent years, mHealth, the use o mobile technologies or
health, has sparked much interest
due to the penetration o cell phones in developing countries. As
Figure 10 shows, the cell phone
is the most commonly used device, but programs also use other
devices. Operation ASHA uses
ngerprint scanners to help monitor compliance with TB treatment.
Comprehensive Medical
Emergency Response Services in Punjab, India, uses GPS to
coordinate its ambulances. Changamka
uses smart cards to help pregnant women save or care.
Fu 9: ghi diibi m i h*
* The size o the dots indicates number programs by country. An
interactive version o the map can be ound online at
www.healthmarketinnovations.org.
http://healthmarketinnovations.org/program/operation-ashahttp://healthmarketinnovations.org/program/comprehensive-medical-emergency-response-services-punjabhttp://healthmarketinnovations.org/program/comprehensive-medical-emergency-response-services-punjabhttp://healthmarketinnovations.org/program/changamka-microhealth-limitedhttp://www.healthmarketinnovations.org/http://www.healthmarketinnovations.org/http://healthmarketinnovations.org/program/changamka-microhealth-limitedhttp://healthmarketinnovations.org/program/comprehensive-medical-emergency-response-services-punjabhttp://healthmarketinnovations.org/program/comprehensive-medical-emergency-response-services-punjabhttp://healthmarketinnovations.org/program/operation-asha
-
8/3/2019 CHMI Report 112711 High Links
15/32
-
8/3/2019 CHMI Report 112711 High Links
16/32CENTER FOR HEALTH MARKET INNOVATIONS6
How technology improves program effectiveness
eHealth has garnered much interest rom the global health
community in recent years, yet there
has not been a systematic eort to examine why health programs
use technology. CHMI identied
six reasons programs choose to use technology (Figure 11).
Increasingly, program managers and
policy makers can use technology to improve program eectiveness
in these areas.
Many programs extend orhicccocrby connecting remote rural
populations
to trained health proessionals in urban areas. OTTET
Telemedicine in India enables doctorvisits via video. Medical help
lines, such as Healthline in Bangladesh and MeraDoctorin India,
provide phone access to health proessionals (more examples can
be ound on p. 23).
Programs such as Cell-PREVEN in Peru, GATHER in Uganda, and
Handhelds or Health in India
imro d collcionndmnmn by replacing paper orms with remote
data
collection devices and sotware.
WelTel in Kenya and other similar programs use text messages to
cili in
commnicion by allowing health proessionals to maintain contact
with patients outside
o traditional oce visits.
D-Tree International and others use clinical decision support
sotware to imrodinoindrmn o minimally trained health workers.
Programs aiming tomiirdndthrough the use o innovative
technologies are
beginning to appear. Initiatives using cell phones to help
detect countereit medications, such
as Unique Identication Mobile Verication, Sproxil, and
mPedigree, have launched recently.
A handul o programs such as Mamakiba in Kenya, which uses text
messaging to help women
save money or health care during pregnancy, rmlinnncilrncion by
enabling
payment or care.
a i h phiii Wi a Hh i d. I i hm hcHIts i d m, whih d d i im.
http://healthmarketinnovations.org/program/ottet-telemedicinehttp://healthmarketinnovations.org/program/healthline-bangladeshhttp://healthmarketinnovations.org/program/meradoctorhttp://healthmarketinnovations.org/program/cell-prevenhttp://healthmarketinnovations.org/program/gatherhttp://healthmarketinnovations.org/program/handhelds-for-healthhttp://healthmarketinnovations.org/program/weltel-technology-providerhttp://healthmarketinnovations.org/program/d-tree-international-0http://healthmarketinnovations.org/program/unique-identification-mobile-verification-uimvhttp://healthmarketinnovations.org/program/sproxilhttp://healthmarketinnovations.org/program/mpedigreehttp://healthmarketinnovations.org/program/mamakibahttp://healthmarketinnovations.org/program/mamakibahttp://healthmarketinnovations.org/program/mpedigreehttp://healthmarketinnovations.org/program/sproxilhttp://healthmarketinnovations.org/program/unique-identification-mobile-verification-uimvhttp://healthmarketinnovations.org/program/d-tree-international-0http://healthmarketinnovations.org/program/weltel-technology-providerhttp://healthmarketinnovations.org/program/handhelds-for-healthhttp://healthmarketinnovations.org/program/gatherhttp://healthmarketinnovations.org/program/cell-prevenhttp://healthmarketinnovations.org/program/meradoctorhttp://healthmarketinnovations.org/program/healthline-bangladeshhttp://healthmarketinnovations.org/program/ottet-telemedicine
-
8/3/2019 CHMI Report 112711 High Links
17/32CENTER FOR HEALTH MARKET INNOVATIONS7
Technology is used to prevent raud and abuse. (e.g., using texts
and pin codes to veriy a drug is not countereit; using
biometricdata to conrm that a health worker has actually visited a
patient). Subcategories in CHMIs database include:
Verication o: medical product, patient identity, nancial
transactions Tracking human resources or operations
Figure 11: six reao health program ue iformatio techology
2. FACILITATING PATIENT COMMUNICATIONS
Technology is used to acilitate communications between health
workers/programs and patients outside o regular visits.Examples
include using technology or general health education, texting
patients to encourage drug compliance and to ollow upater an
appointment. Subcategories in CHMIs database include:
General health education Encouraging patient compliance
Protecting patient privacy
4. IMPROVING DIAGNOSIS AND TREATMENT
Technology is used to allow a health worker to improve clinical
perormance, during training or in real-time in the eld.
Examplesinclude the use o technology to enhance actual training or
connect health workers to a clinical decision-support application
toassist with patient diagnosis.
5. STREAMLINING FINANCIAL TRANSACTIONS
6. MITIGATING FRAUD AND ABUSE
Technology is used to increase the eciency o nancial
transactions, allowing the patient to pay or care more easily and
thedoctor to receive payments more easily. Examples include mobile
insurance premium payments and phone-based vouchers.
1. EXTENDING GEOGRAPHIC ACCESS
Technology is used to overcome distance between doctor and
patient and replaces a traditional visit to the doctor. It includes
what
is oten called telemedicine. Examples include videoconerencing
with patients in rural areas, automated helplines, and
instantmessaging with a health practitioner or medical advice.
3. IMPROVING DATA MANAGEMENT
Technology is used to improve the collection, organization or
analysis o data, resulting in increased speed, enhanced
transmissiono data, and the enabling o remote collection. Examples
include using PDAs to electronically collect inormation about
certaindiseases or or tracking patient records. Subcategories in
CHMIs database include:
Data collection Data organization and analysis
-
8/3/2019 CHMI Report 112711 High Links
18/32CENTER FOR HEALTH MARKET INNOVATIONS8
Fud o o omO the 667 programs that have reported a primary source
o unding (Figure 12), about 50% receive a
inicnorionohirndinromonorohowoorc:ilrldonornci
ndriondion . 34% o all programs are unded primarily by
government contracts or
through out-o-pocket payments by patients. The remaining 16% are
unded through a mix o
debt and equity investments, membership ees, and in-kind
contributions. The large number o
donor-unded programs may indicate their greater visibility,
which has made inormation about
them easier to capture during CHMIs rst year o operation. Going
orward, CHMI will continue to
ocus eorts on identiying non-donor-dependent and lesser known
programs, which may lead
to dierent conclusions about the prevalence o donor unding or
health market innovations.
However, CHMIs initial data suggest that a large proportion o
health market innovations in almost
all 16 countries where its partners are present are
donor-dependent.
Donor are the primary source o unding or 82% o CHMI-proled
HIV/AIDS programs,75% o malaria programs, and 72% o TB programs,
representing donor priorities around
the prevention, diagnosis, and treatment o high-burden
communicable diseases.11 Donor
unding is a less prevalent source o unding or secondary care,
including chronic diseases and
specialized services such as eye care. While grants and
donations are the main source o unding
or a relatively small portion o emergency care programs, donor
unding supports innovative
ambulatory transportation initiatives such as Bike4Care, a
bicycle-based system aimed at helping
patients reach health acilities in rural Kenya, and Riders or
Health, a program that manages and
maintains the vehicles used in the delivery o health care across
Sub-Saharan Arica.
Chronic
Diseases
Family
Planning...
Emergency
Care
HIV/AIDS Malaria Tuberculosis General
Secondary
Care
Eye Care General
Primary
Care
Maternal &
Child Health
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Figure 12: peretge o rogrms by rimry soure o udig, b hh
Funding (primary)
Donor
GovernmentIn-kind of contributions
Membership/Subscription fees
Other 3rd party (e.g. debt, equity)
Out-of-pocket payments
Revenue (e.g., interest on loans
contributions
)
FamilyPlanning
andReproductive
Health
Membership/subscription fees
Other 3rd party (e.g., debt, equity)
http://healthmarketinnovations.org/program/bike4carehttp://healthmarketinnovations.org/program/riders-for-healthhttp://healthmarketinnovations.org/program/riders-for-healthhttp://healthmarketinnovations.org/program/riders-for-healthhttp://healthmarketinnovations.org/program/bike4care
-
8/3/2019 CHMI Report 112711 High Links
19/32CENTER FOR HEALTH MARKET INNOVATIONS9
Figure 13: peretge o rogrms by rimry udig soure, by outry
Vietnam Uganda Tanzania South
Africa
Phil ippines Kenya Indonesia Ghana Cambodia Brazi l Bol iv ia
Bangladesh Peru Ind ia Ecuador Pakistan
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Funding (primary)
Donor
GovernmentIn-kind of contributions
Membership/Subscription fees
Other 3rd party (e.g. debt, equity)
Out-of-pocket payments
Revenue (e.g., interest on loans
)
gornmnare a primary source o unding or many CHMI-proled programs
ocusing on
emergency care (48%), secondary care (43%), and care or chronic
diseases (26%). Although
largely donor-unded, 10% o TB programs receive their primary
unding rom government
sources. Operation ASHA, or example, is channeling unds provided
by the government o
India to establish local TB treatment centers in slum areas.
These subsidies allow patients to
seek care or ree.
O-o-ock ymn are the primary source o revenue or approximately
30% o
programs delivering amily planning and reproductive health
services. They are also the
primary unding source or 15% o maternal and child health
programs and 25% o primary
care programs. Over 50% o specialty eye care programs receive
most o their unding rom
out-o-pocket payments, whereas TB and malaria programs are much
less likely to be nanced
by consumer payments.
Dndqiynncinare generally used by programs ocusing on secondary
and tertiary
services to support investments in growth, capital equipment, or
inormation technology. Capital
nancing is also used in emergency care, general primary care and
maternal and child care.
In nearly all countries where CHMI partner organizations
operate, donorndinihrimry
orconncinorinicnorionororminmocmorhn50% . Yet
the most common sources o primary unding vary slightly rom
country to country (Figure 13).
http://healthmarketinnovations.org/program/operation-ashahttp://healthmarketinnovations.org/program/operation-asha
-
8/3/2019 CHMI Report 112711 High Links
20/32CENTER FOR HEALTH MARKET INNOVATIONS0
Five innOvative MODeLsappearIng arounD tHe WorlD
CHMI identies and tracks the development o innovative
market-based models in health. A new
model is uncovered when CHMI identies multiple programs in
dierent countries with similar
goals, services, organizational structures, and operational
processes. Examples o well-known
models include social marketing, social ranchising, and micro
insurance, which have existed or
some time and have increased their global scale in recent years.
Others, like technology-based
programs oering telemedicine, have more recently begun operating
in low- and middle-income
countries.
Below, we prole ve innovative models that have emerged during
the past decade, with examples
o specic programs and details on their dates o launch, countries
o operation, legal status, and
some indicators o their scale. CHMI will continue to identiy and
track the development o these
and other new health market models. More groupings o noteworthy
program models are online at
www.healthmarketinnovations.org/Analysis.
1. Low-cost retaiL pharmacies
Low-cost pharmacy chains and ranchise networks
improveoperational eciency while keeping prices low. Manyoperate
through a or-prot model, generating revenueby adding on low-cost
clinical and laboratory services andlowering prices by substituting
expensive brands withlow-cost generic drugs.
t Gn p
Launched in 2007 | PhilippinesFor-prot | 1160 outlets
mdpl
Launched in 2006 | IndiaFor-prot | 880 outlets
m F Nnl
Launched in 2003 | MexicoFor-prot | 57 outlets
Generics is a growing pharmacy ranchise providing access to
quality and afordablegeneric drugs throughout the Philippines.
Drugs are provided on consignment andsourced through a network o
domestic manuacturers.
MedPlus is a pharmacy chain operating in ve Indian states.
MedPlus has alsolaunched diagnostic lab services to aid in the
prevention, detection, or managemento a wide range o illnesses and
started clinic services to provide one-stop access tohealth
consultation.
Mi Farmacita Nacional is a pharmacy ranchise providing access to
generic drugs or common conditions. The ranchise
supplements revenue by selling beauty and hygiene products. Some
outlets also ofer medical consultations or $2.
Similar programs: Farmacias Similares in Mexico andBotika ng
Bayan in the Philippines.
http://www.healthmarketinnovations.org/Analysishttp://healthmarketinnovations.org/program/the-generics-pharmacyhttp://healthmarketinnovations.org/program/medplushttp://healthmarketinnovations.org/program/mi-farmacita-nacionalhttp://healthmarketinnovations.org/program/farmacias-similareshttp://healthmarketinnovations.org/program/farmacias-similareshttp://healthmarketinnovations.org/program/botika-ng-bayan-bnbhttp://healthmarketinnovations.org/program/botika-ng-bayan-bnbhttp://healthmarketinnovations.org/program/botika-ng-bayan-bnbhttp://healthmarketinnovations.org/program/farmacias-similareshttp://healthmarketinnovations.org/program/mi-farmacita-nacionalhttp://healthmarketinnovations.org/program/medplushttp://healthmarketinnovations.org/program/the-generics-pharmacyhttp://www.healthmarketinnovations.org/Analysis
-
8/3/2019 CHMI Report 112711 High Links
21/32CENTER FOR HEALTH MARKET INNOVATIONS1
2. aFForDaBLe primary care cLiNicchaiNs
Chains o afordable primary care clinics expand access toquality
care or low-income groups. Many operate in urbanand peri-urban
areas, generating revenue rom higherpatient volumes and targeting
those able to pay a smallsum or services. A number o or-prot
examples o thismodel have launched over the past ew years.
cg Lvwll
Launched in 2008 | KenyaFor-prot | 1 Anchor Clinic, 3 Satellite
Clinics
sd 10
Launched in 2010 | BrazilFor-prot
chl
Launched in 2011 | South AricaFor-prot
LiveWell uses a hub-and-spoke primary care clinic model to serve
densely populated,low-income areas. The anchor clinic is ully
automated to reduce waiting times andprovides consultation,
diagnosis, and treatment or a wide range o illnesses, while
thesatellite clinics are run by qualied clinical ocers and
registered nurses. The satellitesare electronically linked to the
anchor clinic or medical reerrals and advice.
Sade 10 is a start-up chain o primary health clinics in Rio de
Janeiro that oferlow-cost, high quality medical services. Clinics
are located in densely populated areasand are easily accessible
through public transportation. Units have our medicaloces designed
to serve up to 200 people per day. Services ofered include
pediatrics,geriatrics, general practice, gynecology and
otorhinolaryngology (ENT).
The ComHealth initiative aims to make high-quality health
services accessible and afordable or the people o SouthAricas
townships. ComHealth will build and operate acilities (beginning in
2011/2012 in Soweto) that ocus onbasic care. The acilities will
include a clinic or primary care, maternity wards, ENT and
ophthalmology specialistservices, and theaters or simple procedures
that can be done on an outpatient basis or that require less than
24hourshospitalization.
a wom reeivig tiets t liveWes hor ii i nirobi.
Similar programs: Kriti Arogyam Kendram andGlocal Health Care,
India,Por Ti, Familia, Peru.
http://healthmarketinnovations.org/program/carego-livewellhttp://healthmarketinnovations.org/program/sa%C3%BAde-10http://healthmarketinnovations.org/program/comhealthhttp://healthmarketinnovations.org/program/kriti-arogyam-kendramhttp://healthmarketinnovations.org/program/glocal-healthcarehttp://healthmarketinnovations.org/program/por-ti-familiahttp://healthmarketinnovations.org/program/por-ti-familiahttp://healthmarketinnovations.org/program/por-ti-familiahttp://healthmarketinnovations.org/program/por-ti-familiahttp://healthmarketinnovations.org/program/glocal-healthcarehttp://healthmarketinnovations.org/program/kriti-arogyam-kendramhttp://healthmarketinnovations.org/program/comhealthhttp://healthmarketinnovations.org/program/sa%C3%BAde-10http://healthmarketinnovations.org/program/carego-livewell
-
8/3/2019 CHMI Report 112711 High Links
22/32CENTER FOR HEALTH MARKET INNOVATIONS2
3. Vouchers For heaLth serVices
4. teLemeDiciNe
Vouchersdistributed or ree or sold or a small eeincrease access
to key health services, such as amilyplanning and reproductive
health, by allowing individualsto purchasea specic package o
services rom a networko clinics. The networks oten include both
public andprivate acilities.
Technology-enabled networks help increase accessto primary care
or the poor by bridging the distancebetween doctors and patients
through Internet and othertelecommunication technologies. Some ofer
patients videoconsultations with distant doctors, others work to
supporthealth proessionals in rural areas through tele-advice,
and yet others ofer chat-based virtual clinic services
withround-the-clock access to health inormation.
s sl cd
Launched in 2009 | PakistanPublic-Private Partnership | Vouchers
are redeemable in over 100 acilities across twodistricts
wld hl pn
Launched in 2008 | IndiaNon-prot | 1300 shops, 120 telemedicine
centers, 9 diagnostic centers, 16
ranchisee clinics
cnjv yjn
Launched in 2005 | IndiaPublic-Private Partnership | 294,635
clients served
e hl pn
Launched in 2009 | IndiaNon-prot | 8 E Health Points
Sehat Sahulat Card, or Health Facilities Card, is a
public-private partnership modelbetween the district governments o
Kasur and Rawalpindi and Contech International. Itis a voucher
scheme that increases accessibility to quality maternal, newborn,
and child
health services or expecting mothers rom disadvantaged
backgrounds. The servicepackage covers antenatal care, delivery,
and postnatal care.
World Health Partners (WHP) uses telemedicine to connect rural
patients with little accessto ormal health care to trained doctors
based remotely. The our-tiered network includessmall village shops,
ranchised telemedicine Skycenters connected to a central
medicalacility in Delhi, diagnostic centers, and ranchised clinics
or reerrals. Initially launchingin Uttar Pradesh, WHP is
replicating the model in Bihar, ocusing on management oinectious
diseases like TB and childhood pneumonia.
Chiranjeevi Yojana was created to signicantly reduce maternal
and inant mortality byworking with the private sector to provide
delivery and emergency obstetric care at nocost to amilies living
below the poverty line. Under the scheme, the government
contractswith private providers that volunteer to render their
services by signing a memorandum ounderstanding with the district
government.
E Health Point is a chain o clinics that provide amilies in
rural villages with cleandrinking water, medicines, comprehensive
diagnostic tools, and advanced tele-medicalservices that bring
doctors and modern health care to their communities.
Tele-medicalconsultations are assisted by local health workers at
the village level. The programconnects patients with licensed
medical doctors in the urban telemedicine centeroperated by
HealthPoint Services India.
rdv hl
oBd ad pg
Launched in 2005 | KenyaGovernment | 145,333 vouchers used
s F
Launched in 2010 | PakistanFor-prot | 3 centers
The Reproductive Health Output-Based Aid Voucher Program is a
perormance-based reproductive healthprogram that incentivizes
access to womens health care. The program is currently in its
second phase(2009-2012) and is being implemented in rural and
peri-urban districts in Kenya, representing a populationo
approximately three million. The program works with both private
and public sector acilities, allowing orgreater competition and
better service coverage.
Sehat First provides access to basic health care and
pharmaceutical services in Sindh province throughsel-nancing
ranchised tele-health centers. The model consists o a health
clinic, pharmacy, multipurposetele-center, and general store, with
80-90% o revenues coming rom the pharmacy and general store.
SehatFirst has plans to expand in 2012.
Similar programs: Bangladesh Demand Side Financing Pilot
Program, Uganda Reproductive Health Voucher Program,Tanzania
National Voucher Scheme.
Similar programs: OncoNETin India,Buddy Works in the
Philippines, Markle Telemedicine Clinic in Cambodia.
http://healthmarketinnovations.org/program/sehat-sahulat-card-sschttp://healthmarketinnovations.org/program/world-health-partners-whphttp://healthmarketinnovations.org/program/chiranjeevi-yojana-cyhttp://healthmarketinnovations.org/program/e-health-point-0http://healthmarketinnovations.org/program/kenya-output-based-aid-voucher-programhttp://healthmarketinnovations.org/program/kenya-output-based-aid-voucher-programhttp://healthmarketinnovations.org/program/sehat-firsthttp://healthmarketinnovations.org/program/bangladesh-demand-side-financing-dsf-pilot-programhttp://healthmarketinnovations.org/program/uganda-reproductive-health-voucher-program-rhvphttp://healthmarketinnovations.org/program/tanzania-national-voucher-schemehttp://healthmarketinnovations.org/program/onconet-india-sanjeevani-mobile-telemedicine-unitshttp://healthmarketinnovations.org/program/onconet-india-sanjeevani-mobile-telemedicine-unitshttp://healthmarketinnovations.org/program/buddyworkshttp://healthmarketinnovations.org/program/buddyworkshttp://healthmarketinnovations.org/program/markle-telemedicine-clinic-a-model-for-remote-health-care-in-cambodiahttp://healthmarketinnovations.org/program/markle-telemedicine-clinic-a-model-for-remote-health-care-in-cambodiahttp://healthmarketinnovations.org/program/buddyworkshttp://healthmarketinnovations.org/program/onconet-india-sanjeevani-mobile-telemedicine-unitshttp://healthmarketinnovations.org/program/tanzania-national-voucher-schemehttp://healthmarketinnovations.org/program/uganda-reproductive-health-voucher-program-rhvphttp://healthmarketinnovations.org/program/bangladesh-demand-side-financing-dsf-pilot-programhttp://healthmarketinnovations.org/program/sehat-firsthttp://healthmarketinnovations.org/program/kenya-output-based-aid-voucher-programhttp://healthmarketinnovations.org/program/kenya-output-based-aid-voucher-programhttp://healthmarketinnovations.org/program/e-health-point-0http://healthmarketinnovations.org/program/chiranjeevi-yojana-cyhttp://healthmarketinnovations.org/program/world-health-partners-whphttp://healthmarketinnovations.org/program/sehat-sahulat-card-ssc
-
8/3/2019 CHMI Report 112711 High Links
23/32
-
8/3/2019 CHMI Report 112711 High Links
24/32CENTER FOR HEALTH MARKET INNOVATIONS4
bUiLDing the eviDence baseaBout WHat Works
For the past year, CHMI has been documenting health market
innovations across the developing
world. The CHMI database currently proles more than 1000
programs rom 107 countries.
While much rich descriptive inormation has been captured,
iiloimornondrnd
whichrormrcllyworkinimroinhcc, qliy, ndordiliy
orilydlirdhlhcror hoor. These results are important to national
and
global health policy makers, donors, investors, and other
program managers wanting to replicate
proven models. Ideally, each CHMI-proled program would have a
rigorous third-party evaluation,
including baseline data and/or a control group. However, given
the cost o such studies, the reality
is that ew innovative programs are or ever will be evaluated to
academic standards.
But this does not mean that no inormation exists about how well
programs are working. Many
initiatives track perormance through in-house monitoring. While
this type o inormation is
imperect and may be unreliable at times, it is better than no
inormation at all. Frequently, these
data are lost in internal documents and grey literature, thus
becoming a missed opportunity to
promote the growth o successul programs.
Recognizing these realities, in June 2011, CHMI launched an
initiative to collect, record, and publicize
programmatic resultsclear, quantiable, and sel-reported measures
o program perormance
across key dimensions. This initiative will inorm longer term
activities such as the development
o program perormance metrics and the acilitation o ormal program
evaluation. Since June,
more than 80 programs have reported results to CHMI. See Figure
14 or more inormation about
the types o results captured by CHMI and visit the website to
participate in the Reported Results
initiative.
c m oi asHa hd d hwi i h b d tB. th m h dd tB d i m i Dhi.
http://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_reported_results-2386http://healthmarketinnovations.org/programs/browse?sl=environment-chmi_programs%252Cterm_data_tid_features_reported_results-2386
-
8/3/2019 CHMI Report 112711 High Links
25/32CENTER FOR HEALTH MARKET INNOVATIONS5
Fu 14: ci d i cHMI rd r Iiii
AvAilAbility
UtilizAtion
HeAltH oUtpUt
HeAltH oUtcome
QUAlity
User sAtisfAction
cost
pro-poor tArgeting
efficiency
sUstAinAbility
Evidence of increased availability of services in previously
underserved areas.
Evidence of increased use of key health interventions at the
population level (e.g., increase in institutional
deliveries).
Quantitative evidence about services provided, including change
in service provision over time and
modeled estimates of impact based on number of products
sold.
Evidence of impact as demonstrated by improvements in health
indicators.
Evidence of improvements in the quality of services to the
patient, possibly including improved
adherence to established protocols, increased appropriate
diagnoses, and/or decreased issuance of
incorrect prescriptions.
Evidence of good service quality as perceived by the
patient.
Evidence of a decrease in the price of products or services to
the patient.
Quantitative evidence that (1) a large portion of a programs
clients come from lower income brackets
and/or (2) the proportion of poor clients served has increased
over a given time period.
Evidence of a decrease in operational cost or time to providers
of health care services or improvements in
operational processes leading to the provision of better or less
expensive care.
Quantitative evidence of ability to cover costs in the
long-term, including a broad donor base or other
secure revenue streams.
-
8/3/2019 CHMI Report 112711 High Links
26/32CENTER FOR HEALTH MARKET INNOVATIONS6
creating a gLObaL netwOrk
CHMI is creating a global network that connects organizations
and people working to improve
health marketplaces. Below are highlights o CHMIs eorts to oster
greater connections among
program managers, unders, researchers, and policy makers and
encourage virtual interactions
through the CHMI web platorm.
Personal connections
CHMIs partner institutions oten host small, ocused interactions
in their countries o operation to
promote greater awareness, open discussion, and connections
among innovators, policy makers,
and private care providers. In the past year, more than 300
people attended CHMI events around
the world. Highlights include:
eninlicndricoroHlhMrkInnoion.A competition
held in Manila by the Philippine Institute o Development
StudiesCHMIs partner in the
Philippinesbrought together government health ocials, academics,
HMO representatives,
and program managers to present and review twenty programs
considered highly promising
in the Filipino context. Selection criteria included measurable
impact, sustainability, use
o appropriate technology, and a demonstrated ability to target
the poor. PIDS researcherspresented their ndings at several
national and international conerences.
Conncin hoil mnr o imro orionl roc. ACCESS Health
International-India connected doctors, nurses, and quality
managers rom eleven Hyderabad
hospitals seeking to improve service delivery. Managers rom L.V.
Prasad, Care, and LieSpring
were among those who gathered to learn about ways to improve
operations and boost eciency.
exlorin link wn micronnc nd hlh. Ater documenting numerous
micronance institutions providing health services, Freedom rom
Hunger is designing a
community o practice or micronance and health, initially in the
Andean region and later,
globally. The group will publish a report on its ndings and
organize a regional workshop on
the subject in early 2012.
For reports rom other activities in Indonesia, Brazil,
Pakistan,
Kenya, and more, visit the CHMI blog.
Virtual connections
To encourage networking that promotes the growth and
adaptation o promising programs and practices, CHMI allows
web visitors to contact program managers through its
website.
This unction has produced many virtual interactions. See
Figure 15 or a map showing some o the connections made
globally. prormmnr connected with others running
similar programs to exchange inormation about sustainingrevenue,
overcoming technical challenges, and assuring
quality. Inor connected with candidates or unding.
Rrchrconnected with program managers and technical
experts to exchange detailed inormation about input cost and
program design issues.
ri k m, d, dh izi d wih iim m i 2011.
http://healthmarketinnovations.org/blog/2011/jul/14/philippines-institute-development-studies-works-identify-key-health-market-innovatihttp://healthmarketinnovations.org/program/l-v-prasad-eye-institute-lvpeihttp://healthmarketinnovations.org/program/care-hospitalshttp://healthmarketinnovations.org/program/lifespring-hospitals-private-limited-lhplhttp://healthmarketinnovations.org/blog/2011/aug/24/dispatch-indonesiahttp://healthmarketinnovations.org/blog/2011/jun/16/what-innovators-brazil-can-learn-flexible-dynamic-indian-subcontinenthttp://healthmarketinnovations.org/blog/2011/may/23/asia-foundation-roundtable-islamabadhttp://healthmarketinnovations.org/blog/2011/oct/5/kenya-forum-health-innovationshttp://healthmarketinnovations.org/blog/2011/oct/5/kenya-forum-health-innovationshttp://healthmarketinnovations.org/blog/2011/may/23/asia-foundation-roundtable-islamabadhttp://healthmarketinnovations.org/blog/2011/jun/16/what-innovators-brazil-can-learn-flexible-dynamic-indian-subcontinenthttp://healthmarketinnovations.org/blog/2011/aug/24/dispatch-indonesiahttp://healthmarketinnovations.org/program/lifespring-hospitals-private-limited-lhplhttp://healthmarketinnovations.org/program/care-hospitalshttp://healthmarketinnovations.org/program/l-v-prasad-eye-institute-lvpeihttp://healthmarketinnovations.org/blog/2011/jul/14/philippines-institute-development-studies-works-identify-key-health-market-innovati
-
8/3/2019 CHMI Report 112711 High Links
27/32
-
8/3/2019 CHMI Report 112711 High Links
28/32CENTER FOR HEALTH MARKET INNOVATIONS8
Use chMi to support your Work
CHMI can support your work, andyou can contribute to make this
resource even more useul:
sy ono o CHMI nw. Sign up or CHMIs newsletter to receive the
latest updates
rom the CHMI network, including program developments, analyses,
and upcoming events.
Read CHMIs active blog, eaturing commentary rom CHMI partners,
program managers,researchers, and others in the global health
community.
Lrn mor o mrk-d rorm. Search in Programs to locate
innovative
health initiatives in your area o interest (Figure 16). Case
studies, produced by CHMI partner
organizations, oer a deeper look at the structure, activities,
and impact o proled Health
Market Innovations, and explore program successes, challenges,
and lessons learned. Know
about an innovative program? Add a new program prole, update an
existing listing, or write
about it on the CHMI Blog.
Lknowwhwork.CHMI is collecting Reported Results to create a
preliminary evidence
base about what works and encourage programs to track and share
their perormance. Report
results or programs that you manage, und, or study.
Chckonmrklcdi. CHMI commissions thematic studies to take a
deeper look
at health markets. Two studies o health marketplace challenges
are currently underway: 1) A
study on the dynamics o the inormal provision o care in
Bangladesh, India, and Nigeria and
2) an evaluation o the eect o MedPlus, a new high-quality chain
pharmacy, on drug quality
in the broader health marketplace in Andhra Pradesh, India.
Conncwih innoor. Join CHMI to directly contact people running
programs listed
in CHMIs database. Have conversations with the Health Market
Innovations community on
CHMIs Blog.
Downlodhd.The CHMI database o more than 1000 programs can be
downloaded
or ree. Browse in Programs or a topic o interestlike or-prot
primary care enterprisesor emergency helplines operated under
government contractsor download the entire
Programs database. Data can be combined with additional
variables, adapted or modied,
with citations. See box at right or an example o how researchers
have used CHMI.
Tell us how CHMI can better support your work. CHMI strives to
provide relevant, timely, and
useul inormation to the Health Market Innovation community. We
welcome eedback on the
content o this report, the CHMI website, or the initiative more
broadly. Please send comments to
[email protected].
http://resultsfordevelopment.us1.list-manage.com/subscribe?u=6c3212a6ca42b75aaead60ceb&id=fd7adc5569http://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/program-case-studieshttp://healthmarketinnovations.org/node/add/program-summary-formhttp://healthmarketinnovations.org/node/add/program-change-requesthttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/health-market-studieshttp://healthmarketinnovations.org/user/registerhttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programs/browse/csv?search=http://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/user/registerhttp://healthmarketinnovations.org/health-market-studieshttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/analysis/reported-results-initiativehttp://healthmarketinnovations.org/bloghttp://healthmarketinnovations.org/node/add/program-change-requesthttp://healthmarketinnovations.org/node/add/program-summary-formhttp://healthmarketinnovations.org/program-case-studieshttp://healthmarketinnovations.org/programshttp://healthmarketinnovations.org/bloghttp://resultsfordevelopment.us1.list-manage.com/subscribe?u=6c3212a6ca42b75aaead60ceb&id=fd7adc5569
-
8/3/2019 CHMI Report 112711 High Links
29/32CENTER FOR HEALTH MARKET INNOVATIONS9
Fu 16: cHMI m h i
prorminloliiiliyndoorniioxnd:The CHMI website is one o the
[reasons why]
we are known outside India, said Rajeev Kumar o the health
technology company Neurosynaptic. We have been
receiving inquiries rom hospitals and individuals outside India
to know more about the ReMeDi telemedicine kit,
the Bangalore-based business leader continued. Because o CHMI,
Kumars company was eatured in the BBC Horizon
program on innovations.
fndridniyromiininmncndid:Impact Investment Partners, o Mumbai,
used CHMIs database
to idniyndconcromiinro-oor,or-rohlhrormorininIndi . CHMI helps
educate
everyone on what is happening in the sector and can help
industry participants identiy channel partners, said Amit
Sharma.
Rrchrccrdonmrk-dhlhrorm:Onil Bhattacharyya, a researcher at
theUniversity o Toronto, used CHMIs database to identiy the
percentage orormmrinimcincori
likin,cincy,o,ndocom. In a presentation at the 2011
International Health Economics As-
sociation (iHEA) meeting, Bhattacharyya noted the diculty o
assessing programmatic perormance without strategic
indicators. (See page 24 to learn how CHMI is tracking
results.)
policymkrxchnidohoworwrdhricor:In Islamabad, a roundtable
organized
by CHMIs Pakistan-based partner, the Asia Foundation, provided a
unique opportunity or government and private sector
practitioners to meet and discuss policy issues. The orum served
as a neutral platorm to rankly discuss issues such as ri-
hlhrlionndmrk-ldinnoion , which are being debated by at least
two provincial governments.
HoW people are usIng cHMI
http://healthmarketinnovations.org/program/remedi-%E2%80%93-mdau-multi-parameter-data-acquisition-unithttp://www.horizonsbusiness.com/#playlisthttp://www.horizonsbusiness.com/#playlisthttp://www.horizonsbusiness.com/#playlisthttp://www.horizonsbusiness.com/#playlisthttp://healthmarketinnovations.org/program/remedi-%E2%80%93-mdau-multi-parameter-data-acquisition-unit
-
8/3/2019 CHMI Report 112711 High Links
30/32
-
8/3/2019 CHMI Report 112711 High Links
31/32CENTER FOR HEALTH MARKET INNOVATIONS1
1. CHMI partners operate in the ollowing countries:
Bangladesh, Bolivia, Brazil, Cambodia, Ecuador, India,
Indonesia, Kenya, Pakistan, Peru, the Philippines, Rwanda,
South
Arica, Tanzania, Uganda, and Vietnam. See list at let.
2. WHO National Health Accounts data or 2006.
3. Van Doorslaer E., et al. (2006). Eect o payments or
health
care on poverty estimates in 11 countries in Asia: an analysis
o
household survey data. Lancet, 368:1357-1364.
4. Goodman C, Kachur SP, Abdulla S, Bloland P, Mills A.
(2007).
Drug shop regulation and malaria treatment in Tanzaniawhy
do shops break the rules, and does it matter? Health Policy
Plan,
22:393403.
5. CHMI does not document private practices o individual
providers, instead proling organizations that make health
care delivery less ragmented. For an explanation o the kinds
o programs included in and excluded rom CHMIs Programs
Database, visit www.HealthMarketInnovations.org/about
6. CHMI strives to collect inormation about innovative programs
in
all low- and middle-income countries. In practice, the
database
contains more comprehensive inormation or countries in
which CHMI partners operate. See all at www.tinyurl.com/
CHMIpartners.
7. Currently, CHMI statistics are primarily based on numbers
o programs.This measurement is imperect because some
programs are small and others are large. CHMI aims to
collect
more data on scale in the coming years.
8. More inormation about social ranchising can be ound on
s4health.org.
9. PhilHealth beneciaries have access to a package o
services
that include inpatient care, catastrophic coverage,
ambulatory
surgeries, deliveries, and outpatient treatment or malaria
and
tuberculosis. Those identied as indigent and Overseas
Filipino
Workers are also entitled to outpatient primary care.
10. The Joint Learning Network or Universal Health Coverage
is
a network o low- and middle-income countries in the midst
o demand-side health nancing reorms aimed at achieving
universal health coverage. The JLN is ocused on linking
practitioners and policy makers to help disseminate best
practices
and provide targeted assistance in specic technical areas.
More
inormation is available at jointlearningnetwork.org.
11. Percentages in this section correspond to the number o
programs
reporting a particular source o unding as their primary
source
rather than percentages o overall revenues coming rom that
source.
COVER PHOTO: A young mother at the Nice Foundations Institute
or
Newborn Care, taken by Andr J.P. Fathome or CHMI.
Page 11 and 24: Photos by Andr J.P. Fathome or CHMI.
Page 15 and 16: Photo by Nacho Hernandez or CHMI.
Page 20: Photo by Ida Marie Pantig/PIDS or CHMI.
Page 21 (top let): Advertisment or Sade 10, courtesy o
program.
Page 21 (bottom): Photo by Chris Whiteman or CHMI.
Page 22 (top let), 23 (bottom): Photos by Richard Lord, used
courtesy
o the Population Council.
Page 23: Photo rom MeraDoctor.co.
Page 26: Photo by Alex Kamweru or CHMI.
Page 27: Map design by Gizelle Gutierrez or CHMI.
END NOTES PHOTO CREDITS
-
8/3/2019 CHMI Report 112711 High Links
32/32
http://healthmarketinnovations.org
ConcCHMIR4D:
1100 15th Street, NW, Suite 400
Washington, DC 20005
[email protected]
mailto:[email protected]:[email protected]