Embed Size (px)
Citation preview
CHF/Pulmonary Edema & CPAP
McHenry Western Lake County EMS System Education
CHF
Common & potentially fatal condition Occurs when the left ventricle fails Pressure builds up in the ventricle This causes an overload of fluid in body When this fluid occurs in lungs it’s called
pulmonary edema CHF is on the rise in the US
CHF/Pulmonary Edema
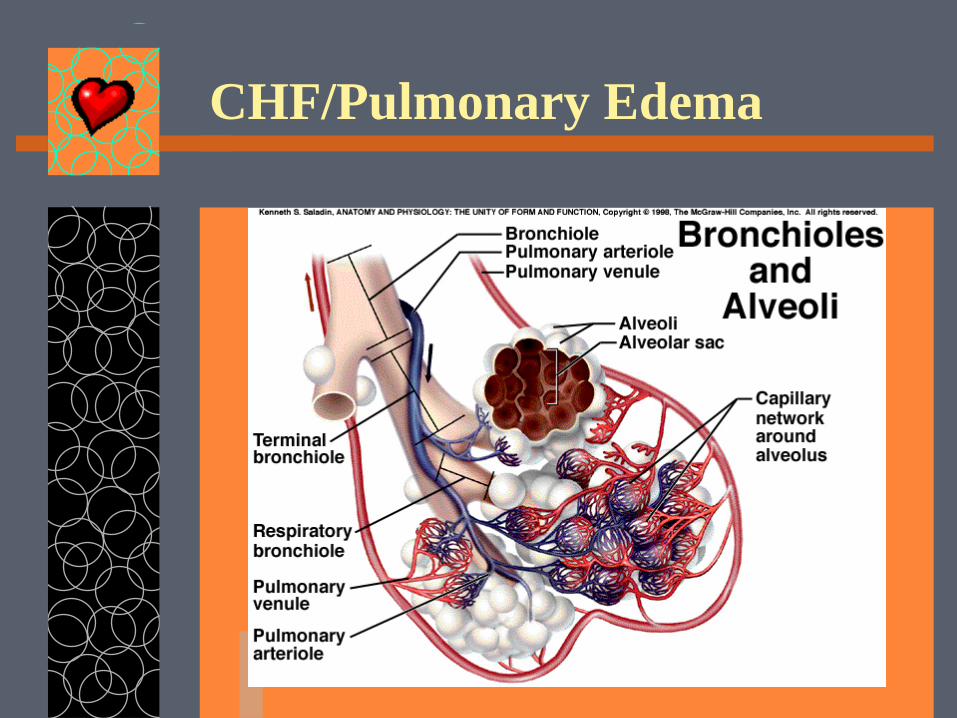
CHF/Pulmonary Edema
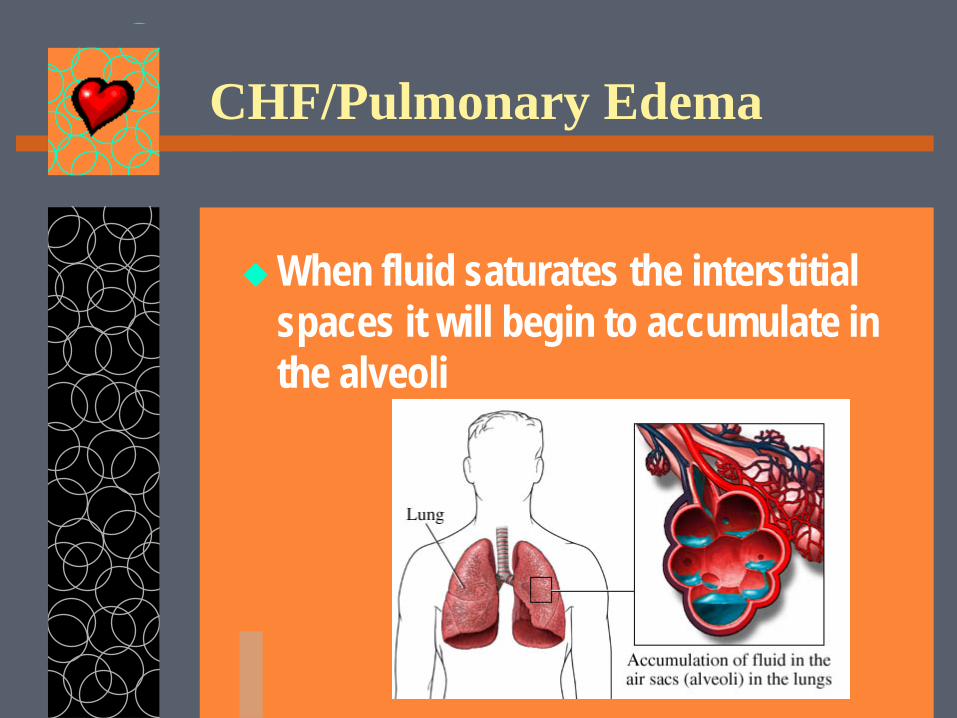
When fluid saturates the interstitial spaces it will begin to accumulate in the alveoli
CHF/Pulmonary Edema
Alveoli collapse with each exhalation Fluid washes out the surfactant Alveoli can not re-expand Pink frothy sputum Acute respiratory distress Rapid deterioration
CHF/Pulmonary Edema
Signs & Symptoms – Dyspnea of varying degrees – Orthopnea – Anxiety / Restlessness – Tachypnea / tachycardia – Pink Frothy Sputum – SpO2 ≤ 94 %
CHF/Pulmonary Edema
Signs & Symptoms – Pale/Cool/Diaphoretic – Labored respirations – Severe apprehension or confusion – BP usually elevated
(Low would be ominous) – Pt not able speak normally – Lung Sounds-crackles & / or wheezes
CHF/Pulmonary Edema
Rapid Aggressive Treatment is required All that wheezes is not asthma and
should not be treated with albuterol!
Treatment for CHF
Position the patient in a sitting upright at 90* and dangle legs if possible.
If the patient is in severe distress you may have to consider DAI.
Treatment for CHF
CPAP if immediately available – Do not use C-PAP in AMI

Treatment for CHF
Monitor-from the time of pt contact
IV-tko
Pulse Ox
Treatment for CHF
ASA 324mg – (unless contraindicated)
NTG – EVERY 3-5 MIN as long as SBP remains >90. No limit

Treatment for CHF
For severe anxiety in CHF, Versed in 2mg increments every 30-60 sec IVP (0.2 mg/kg IN) up to 10mg IVP/IN.
May repeat to 20mg if SBP >90. Anxiety worsens the condition
CPAP : What it is
Applies positive pressure to the airways throughout the respiratory cycle
This keeps the alveoli open during expiration
Allows for O2 & CO2 exchange Can rapidly improve pt’s condition Frequently prevents intubation
CPAP
Why wouldn’t we want to intubate? – Mandatory ICU admission – Prolonged hospital stay & recovery – Higher potential for complications – Airway trauma possible – Infection can occur – More invasive & uncomfortable
CPAP : What it isn’t
CPAP does not maintain the airway CPAP does not allow you to assist
your pt with ventilation Pt MUST be able to maintain their
own airway Pt MUST be able to clear their own
airway
CPAP
If your pt requires ventilatory assistance with a BVM he is not a candidate for CPAP
Altered mental status – GCS ≤ 8 requires ventilatory assistance, therefore no CPAP
CPAP – Indications/Inclusions
Pulmonary Edema
Dyspnea Crackles Wheezes
At least 18 yrs old Alert with airway
intact/maintainable SBP > 90 DBP >60 Sp02 < 94%
CPAP - Contraindications
Age less than 18 AMS SBP < 90 Need for immediate airway control Unstable airway Acute MI
CPAP – May exclude
Uncooperative patient Facial hair making it impossible to obtain seal Pregnancy Inability to properly fit mask
CPAP - Procedure
Follow appropriate SOP Prepare equipment
– Connect oxygen to 15 L – Peep will be 3.0-4.0 – Have intubation equipment
available Position pt sitting up Explain procedure to pt &
reassure
CPAP - Procedure
Hold mask gently to face to allow patient to feel what the pressure will be like.
After 3-5 min. lift mask & give next NTG Now gently place head straps on patient.
CPAP - Procedure
If needed, flow can be increased to 20 lpm which will provide 6.0 -7.0 of peep
Sp02 of >95% is our goal.
CPAP - Procedure
If no improvement in 3 minutes: – Increase O2 to 25 LPM – PEEP will now be 8.5 – 10.0 – Maintain Sp02 >95%
Continuously monitor pt for S/S requiring intubation
Cardiogenic Shock
SBP < 90 MAP <60 Signs and Symptoms of hypoperfusion Dopamine 400mg/250ml
– Start at 5mcg/kg/min and titrate up to 20 mcg/kg/min until SBP is >90.
– NS 200 ml increments if lungs clear and respirations are not labored!
CPAP – D/C in field
Inability to tolerate mask (Nobody likes CPAP at first)
Need to intubate SBP falls below 90 ECG instability with evidence of
acute ischemia
CPAP
Be sure to document : – Time of initiation – Settings – Pt response-VS, color, work of
breathing, SpO2, EtC02 Continually watch pt for
improvement or deterioration
CPAP
System is dependent on a good seal Pt MUST remain on O2 & cardiac
monitor at ALL times, even when transferring pt care to hospital
Continue to give NTG SL every 3-5 min, just lift mask briefly to administer medication
Documentation
Time initiated O2 settings Patient response
– V/S-resp. rate & depth – SpO2 & mental status – Respiratory distress-WOB, comfort level – Lung sounds – Complications- gastric distention, inability to
tolerate
Additional Indications for CPAP Include
Asthma/COPD patient in severe respiratory distress
Near drowning patient who is congested has increased work of breathing who can maintain their own airwy.
Case Study
You have a 68 y/o male with sudden onset of dyspnea, coughing pink sputum. He is restless and has tachycardia. His BP is 168/94 SpO2 is 94% and pulse is 140. What should your treatment be?
Answer
Prepare equipment – Connect oxygen to 15 L – Have intubation equipment available
Position pt sitting up Explain procedure to pt & reassure
Answer
Hold mask gently to face After 5 min. lift mask & give next NTG Now gently place head straps on and
increase flow as needed.
Case Study
You have given your patient 4 ASA and 2 NTG during your treatment. His pressure remains stable at 154/78 and his pulse is still 140. SpO2 is 96%. Can you give him another NTG?
Answer
Yes…there is no limit to the NTG every 3-5 minutes as long as the patient has a SBP >90
Questions??
Color good
Alert
Good Airway
Sitting Upright
Thanks Guys! I feel much better now!!






![CPAP and BiPAP - UW Health · PDF fileCPAP and BiPAP “A CPAP a day ... CHF/Pulmonary Edema Interstitial fluid interferes with gas ... Microsoft PowerPoint - Ppt0000025.ppt [Read-Only]](https://img.pdfslide.us/doc/110x75/5ab6fddf7f8b9a86428e42ed/cpap-and-bipap-uw-health-and-bipap-a-cpap-a-day-chfpulmonary-edema-interstitial.jpg)



![CPAP Introduction presentation.ppt - Wild Apricot CPAP Introduction. Outline ... Mild epistaxis 1 (4.0%) 6 (11.3%) 2 ... CPAP Introduction presentation.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5ae60d537f8b9a9e5d8d3430/cpap-introduction-wild-apricot-cpap-introduction-outline-mild-epistaxis-1.jpg)


















