Embed Size (px)
Citation preview
6/1/2015
1
Heart Failure Certification
Review CoursePart 3
Ashley Moore-Gibbs, MSN, AGPCNP-BC, CHFN
Objectives
♥ Review the hemodynamic patient profiles of acute decompensated
heart failure (ADHF)
♥ Discuss the current ACCF/AHA Heart Failure Guidelines for management of ADHF
♥ Define advanced HF and outline treatment recommendations
Case Study 1• WD is a 48 year old African American male being evaluated in the ED for
complaints of DOE, worsening lower extremity edema, abdominal distention
• PMH: NICM (Dx 2004) , S/P ICD (2005), NSVT, DM Type 2, Obesity, Gout,
Obstructive Sleep Apnea (OSA). Last admission for HF 3 months ago; 3
admits total in last 9 months
• PSH: none
• Dx Tests:
• Echocardiogram 6 months ago showing LVEF < 20%
• No recent labs
• ICD no interrogations in 9 months

6/1/2015
2
Case Study 1: WD• Social hx:
– Lives with father
– 3 children with youngest living with him
– Disabled since diagnosis of CMP (2004)
– Assists with coaching basketball at a local Boys & Girls Club
– No prior/current history of tobacco, ETOH, or illicit drug use
• Review of Systems
– Significant for 3 pillow orthopnea, decrease in exercise tolerance,
decrease in appetite, nonproductive cough, lower extremity &
abdominal edema
Case Study 1: WD• Medications
– Aspirin 325 mg PO daily
– Amiodarone 200 mg PO daily
– Lasix 80 mg PO daily
– Aldactone 25mg PO daily
– Colchicine 0.6mg BID prn
– Coreg 12.5mg PO BID
– Glyburide 10mg PO daily
• Allergies:
– PCN: hives
Case Study 1: WD• Physical Exam
– VS: BP 92/54 mm/Hg, HR 110, RR 24, Temp 98.4 degrees, pulse ox 95%
on O2 2LNC, Ht: 5’ 10”, Wt: 295 lbs, BMI 42.3
– HEENT: unremarkable
– Neck: significant JVD (> 10 cm H2O)
– Lungs: clear bilaterally, respirations even; mildly labored during
conversation
– CV: RRR, + S3, - S4, systolic murmur II/VI. PMI displaced laterally; 6th ICS
– Abd: morbidly obese, soft, distended, mild tenderness RUQ. Bowel
sounds x 4 quad
– Ext: 3 + pitting edema mid-thigh down bilaterally.
• Pulses 2 + throughout, capillary refill < 2 sec
– Skin: Intact, cool warm upper/lower extremities bilaterally.

6/1/2015
3
Cardiac Remodeling
• Damage/insult occurs to the muscle followed by inflammation
• Neurohormonal (NH) activation occurs increasing ventricular pressure, volume, and peripheral vasoconstriction
• Heart changes in structure (dimensions, mass, shape) and function
• NH activity continues causing further structural & functional changes
Case Study 1 : WD
• BMP: Na 130, K 4.0, BUN 20, Cr 1.6
• CBC: WBC 5.0, Hgb 11.5, Hct 32.3, plt 232
• Cardiac BNP: 1160
• Cardiac biomarkers (CK-MB, trop): normal
• 12 lead ECG: Sinus tachycardia, vent rate: 110 bpm, normal axis
• CXR: cardiomegaly
Why did we draw a BNP on WD?
6/1/2015
4
Treatment Goals for ADHF
Primary Treatment Goals
• Improve/decrease symptoms
• Identify precipitating factors
• Optimize volume status
Other Goals during Hospitalization
• Optimize chronic oral therapy
• Increase exercise tolerance
• Improve heart function
• Identify patients who may benefit
from revascularization
• Educate patients on Self-Care
activities
Heart Failure Updated Guidelines
Chronic versus Acute Decompensated HF
• Chronic HF:
– more stable condition
– organ function remains
adequate
• ADHF:
– unstable condition
– immediate treatment is warranted to prevent injury
to systemic organs

6/1/2015
5
Treatment Options for ADHF
• Fluid & sodium restriction
• Diuretics (loop and thiazide)
• Intravenous vasodilators (nitropusside, nitroglycerin, nesiritide)
• Inotropes (milrinone, dobutamine)
• Ultrafiltration (in selected patients)
• Mechanical Circulatory Support
• Orthotopic Heart Transplant
Basic Hemodynamic Parameters
1. Presence or absence of elevated filling pressures
– Wet or Dry
2. Perfusion status: Sufficient or Diminished
– Warm or Cold
Evidence of Congestion
• Orthopnea
• Paroxysmal nocturnal
dyspnea
• Jugular venous distention
• Adventitious breath sounds
• Third heart sound (S3)
• Ascites
• Peripheral edema
6/1/2015
6
Signs of Poor Perfusion
• Mental status changes
• Narrow pulse pressure
• Sinus tachycardia
• Poor urine output
• Hypotension
• Cool extremities above
hands/feet
Monitoring Patients Hospitalized with ADHF
Parameter Frequency Specifics to consider
Weight At least daily � Obtain after patient voids
� Obtain prior to breakfast
Fluid intake & output At least daily
Vital signs More than daily � Include orthostatic blood
pressure
Physical exam At least daily � Edema
� Ascites/hepatojugular reflux
� Hepatomegaly/ Liver tenderness
� Pulmonary rales
�Increased JVP
Symptoms At least daily � Orthopnea/PND
� Nocturnal cough/dyspnea
� Fatigue
Laboratory data At least daily � Serum potassium, sodium,
creatinine, & BUN
HFSA 2010 Comprehensive Heart Failure Practice Guideline
Hemodynamic Profile AssessmentCongestion at Rest
Low
Perfusion
at Rest
No
No Yes
Yes
Warm & Dry Warm & Wet
Cold & WetCold & Dry
Signs/symptoms of congestion:
• Orthopnea/PND
• JVD
• Ascites
• Edema
• Rales (rare in HF)
Possible evidence of low perfusion• Narrow pulse pressure• Sleepy/obtunded• Low serum sodium
• Cool extremities• Hypotension • Renal dysfunction
Stevenson LW. Eur J Heart Fail. 1999;1:251
6/1/2015
7
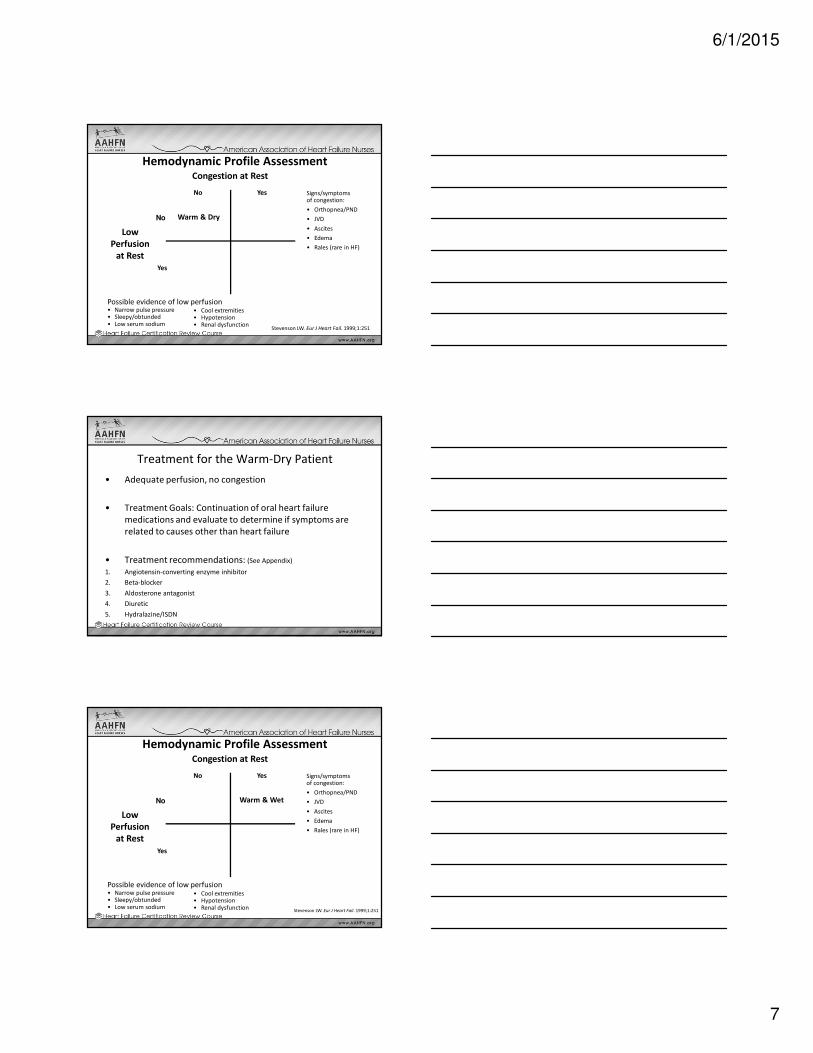
Hemodynamic Profile AssessmentCongestion at Rest
Low
Perfusion
at Rest
No
No Yes
Yes
Warm & Dry
Signs/symptoms of congestion:
• Orthopnea/PND
• JVD
• Ascites
• Edema
• Rales (rare in HF)
Possible evidence of low perfusion• Narrow pulse pressure• Sleepy/obtunded• Low serum sodium
• Cool extremities• Hypotension • Renal dysfunction
Stevenson LW. Eur J Heart Fail. 1999;1:251
Treatment for the Warm-Dry Patient
• Adequate perfusion, no congestion
• Treatment Goals: Continuation of oral heart failure
medications and evaluate to determine if symptoms are
related to causes other than heart failure
• Treatment recommendations: (See Appendix)
1. Angiotensin-converting enzyme inhibitor
2. Beta-blocker
3. Aldosterone antagonist
4. Diuretic
5. Hydralazine/ISDN
Hemodynamic Profile AssessmentCongestion at Rest
Low
Perfusion
at Rest
No
No Yes
Yes
Warm & Wet
Signs/symptoms of congestion:
• Orthopnea/PND
• JVD
• Ascites
• Edema
• Rales (rare in HF)
Possible evidence of low perfusion• Narrow pulse pressure• Sleepy/obtunded• Low serum sodium
• Cool extremities• Hypotension • Renal dysfunction
Stevenson LW. Eur J Heart Fail. 1999;1:251

6/1/2015
8
Treatment for the Warm-Wet Patient
• Most common type of ADHF
• Treatment Goals: Reduce ventricular filling pressures &
relieve symptoms
• Limitations in medical therapies in ADHF
• Treatment recommendations:
- Ideally treated with intravenous diuretics
- Vasodilator therapy in combination with IV diuretics in patients with diuretic
resistance or Chronic Kidney Disease
Medical Therapy During Hospitalization
• Patients with HFrEF (HF with reduced Ejection Fraction)
experiencing HF exacerbation should have guideline-driven
medical therapy continued in the absence of hemodynamic
instability contraindications
– Oral therapy should be continued, or even uptitrated, during hospitalization
• Initiation of beta blocker (BB) therapy is recommended after
optimization of volume status and successful discontinuation of
IV diuretics, vasodilators, and inotropic agents
– BB should be initiated at low dose only in stable patients
– Caution should be used in patients when initiating BB that have required
inotropes during their hospital course
2013 ACCF/AHA Guideline for the Management of Heart Failure
Recommendation for Diuretics
• Dose should produce a rate of
diuresis sufficient to achieve
optimal volume status with
relief in symptoms of
congestion without inducing
excessive, rapid reduction in:
– Intravascular volume
– Serum electrolytes
6/1/2015
9
Diuretics in HF
• Indicated in HF patients with fluid retention.
• Types of Diuretics:
Thiazides (chlorothiazide)
Loop diuretics (furosemide, torsemide, bumetanide)
• Thiazides are useful in hypertensive HF patients with mild
fluid retention.
• Loop diuretics are effective in the presence of renal
impairment.
• HFSA Guidelines 12.10
– Patients with mod to severe renal dysfunction & evidence of fluid
retention should continue to be treated with diuretics
Case Study 1 from Part 1Defining HF, HF symptoms, History & Physical Exam,
Class/Stage of HF, ECHO, HF Medical Therapy
DF is a 72 year old male with a long-standing history of an ischemic
cardiomyopathy. Prior echocardiogram performed in Jan 2012 showed LVEF
40%. He has been added on to the office schedule for cardiac evaluation for
complaints of (C/O) SOB.
Echocardiogram performed the day of the office visit shows a decrease in LVEF
from 40% to 20%.
Current meds:
Lasix 40 mg PO daily
Lisinopril 10mg PO daily
Carvedilol 12.5mg PO BID
Aspirin 81mg PO daily
Atorvastatin 80mg PO QHS
26
Diuretic Therapy
• Increase urine excretion & decrease fluid retention
• Two studies (SOLVD & PRAISE) suggested that there is a risk of ↑ in morbidity & mortality when non-potassium- sparing diuretics are used
• No studies have examined the effects of long-term outcomes
• Potential adverse effects:
- electrolyte imbalance
- hypotension
- decline in renal function
- diuretic resistance
- hearing impairment or tinnitus
6/1/2015
10
Diuretics and HF
Patients may become unresponsive to high doses of diuretic drugs if they:
● Consume large amounts of dietary sodium2
● Take agents that can block effects of diuretics
(eg, NSAIDs, COX-2 inhibitors)1
● Have significant impairment of renal function or
perfusion1
Diuretic resistance can generally be overcome by
● IV administration of diuretics2
● Using 2 or more diuretics in combination2
1Ravnan SL et al. Congest Heart Fail. 2002;8:802Brater DC. Drugs. 1985;30:427
Diuretic Resistance: Considerations for Ultrafiltration
• Known diuretic resistance
• > 10 – 15 pounds of excess fluid
• Volume loaded during surgery and fluctuating blood pressure (once BP stable)
• RV failure/Pul HTN
Hemodynamic Profile AssessmentCongestion at Rest
Low
Perfusion
at Rest
No
No Yes
Yes Cold & Wet
Signs/symptoms of congestion:
• Orthopnea/PND
• JVD
• Ascites
• Edema
• Rales (rare in HF)
Possible evidence of low perfusion• Narrow pulse pressure• Sleepy/obtunded• Low serum sodium
• Cool extremities• Hypotension • Renal dysfunction
Stevenson LW. Eur J Heart Fail. 1999;1:251
6/1/2015
11
Treatment for the Cold-Wet Patient
• More intense therapy may be needed in this patient
population. Therapy adjusted based on systemic vascular
resistance (SVR).
• Treatment Goals: Achieve adequate diuresis and maintain
adequate perfusion; can be adjusted based on levels of SVR
• Treatment recommendations:
- Intravenous loop diuretics + vasodilators or nesiritide in pts with � SVR & �cardiac output
- Short term inotropic treatment may be useful in patients with normal or � SVR
Intravenous Vasodilators
Mechanism of action:
• Directly reduce SVR & filling
pressures which allows for rapid
reversal of decompensation
• Not associated with exacerbations of
ischemia or ventricular dysrhythmias
• Can be utilized with long-term oral
therapy including ACE inhibitors and
diuretics
IV Vasodilators:
• Nitroglycerin- commonly used in ADHF. Primarily through effects on venodilation.
• Nitroprusside- despite favorable impact on hemodynamics not as widely used for ADHF due to it’s pharmacologic effects. (Need PA Cath)
• Nesiritide- VMAC trial established clinical benefit of this agent in ADHF. Meta-analyses have suggested an ↑ in worsening renal function & mortality. Indicated in patients with dyspnea and volume overload
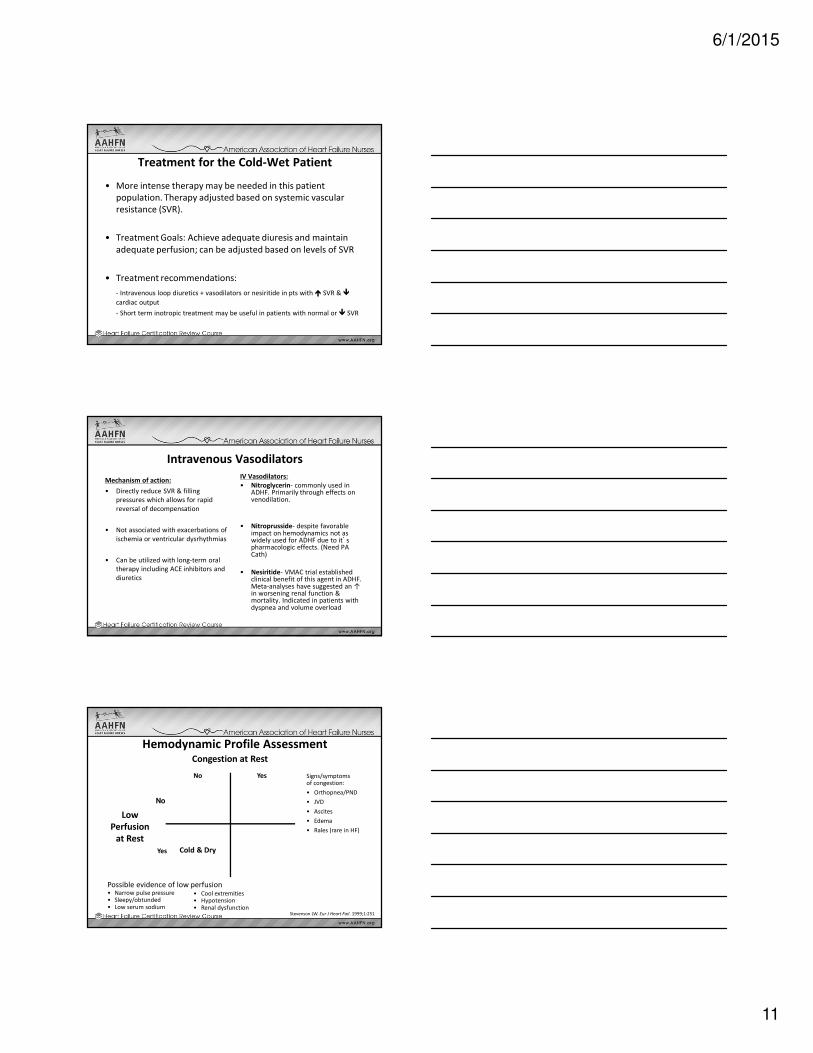
Hemodynamic Profile AssessmentCongestion at Rest
Low
Perfusion
at Rest
No
No Yes
Yes Cold & Dry
Signs/symptoms of congestion:
• Orthopnea/PND
• JVD
• Ascites
• Edema
• Rales (rare in HF)
Possible evidence of low perfusion• Narrow pulse pressure• Sleepy/obtunded• Low serum sodium
• Cool extremities• Hypotension • Renal dysfunction
Stevenson LW. Eur J Heart Fail. 1999;1:251

6/1/2015
12
Treatment for the Cold-Dry Patient
• Most challenging to manage
– Low BP + low CO
– Volume management
• Treatment Goals: Improve cardiac output and blood pressure
• Treatment recommendations:
- Consider inotropic therapy in combination with vasopressors
- Meticulous fluid management required
- Consider decreasing or withdrawing beta-blockers
- Consider intra-aortic balloon pump or ventricular assist device
Inotropes
Mechanism of action:
• Improve cardiac output and cardiac index
• Reserved for patients with a dry-cold or wet-cold profile
• Risk-benefit profile not favorable
Inotropic agents:
Milrinone (Primacor)
Dobutamine (Dobutrex)
36
Inotropic Therapy
• Continuous IV infusions of Dobutamine, Dopamine
or Milrinone used as
�Bridge to transplantation
�Bridge to device therapy
�Symptom palliation
• ICDs should be implanted if the patient is going to be discharged on a continuous infusion unless inotrope is used for palliation
• Intermittent infusions NOT recommended
6/1/2015
13
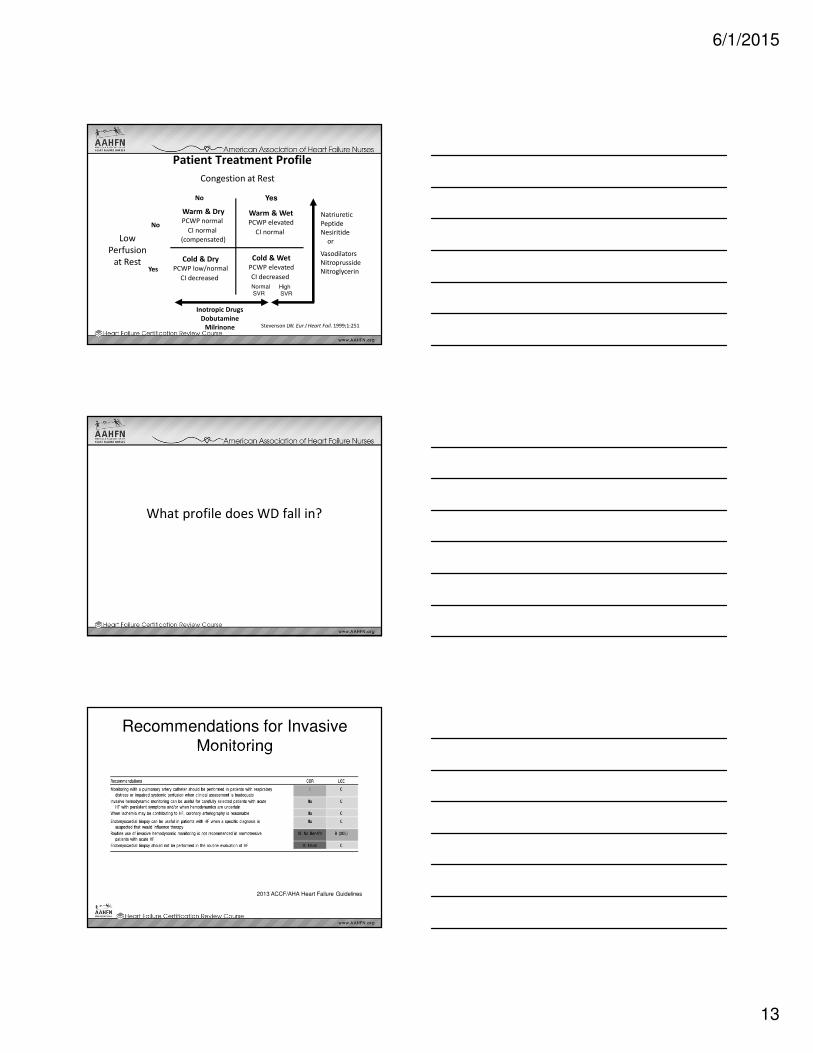
Patient Treatment Profile
Congestion at Rest
YesNo
Warm & DryPCWP normal
CI normal
(compensated)
Cold & WetPCWP elevated
CI decreased
Cold & DryPCWP low/normal
CI decreased
Vasodilators
Nitroprusside
Nitroglycerin
Inotropic Drugs
Dobutamine
Milrinone
NormalSVR
High SVR
Low
Perfusion
at Rest
No
Yes
Warm & WetPCWP elevated
CI normal
Natriuretic
Peptide
Nesiritide
or
Stevenson LW. Eur J Heart Fail. 1999;1:251
What profile does WD fall in?
Recommendations for Invasive Monitoring
2013 ACCF/AHA Heart Failure Guidelines

6/1/2015
14
Right Heart Catheterization
Normal Cardiac Pressures• Central venous pressure (CVP) -1-6 mm Hg
– Pressure of blood in the vena cava, near the right atrium
– Reflects the amount of blood returning to the heart
– Good approximation of right atrial pressure
• Right ventricular pressure
– Systolic – 15-30 mm Hg
– Diastolic – 0-5 mm Hg
• Pulmonary artery pressure
– Systolic – 15-30 mm Hg
– Diastolic – 4-12 mm Hg
• Pulmonary capillary wedge pressure (PCWP) 6-15 mm Hg
– Indirect pressure of left atrial pressure
– Pulmonary edema reflective of PCWP >25 mm Hg
• Left ventricular systemic pressure (systolic) 100-140 mm Hg
• Pulmonary vascular resistence (PVR)
– (PAP-PCWP)* 80 } / (CO) =150-250 dynes*sec/cm^5
– PAP- PCWP/ CO= PVR in wood units, normal 0.25-1.6
– An increase in PVR can result in RV failure
– Abnormally high PVR can be a contraindication to cardiac transplantation as it could cause RV dysfunction in the transplanted heart
• Systemic vascular resistance (SVR)– 80 X (PAP-CVP)/CO = <250 dynes-sec/cm-5
-1-6
15-30
0-5
15-30
4-12
100-140
Normal Results of a RHC
•Cardiac index (CI) is 2.8 to 4.2 liters per minute per square meter (of body surface
area)
• Pulmonary artery systolic pressure (PAS)
15 to 30 millimeters of mercury (mmHg)
• Pulmonary artery mean pressure (PAMP)
6 to 15 mmHg
• Pulmonary diastolic pressure (PAD) is 4
to 12 mmHg
• Pulmonary capillary wedge
pressure(PCWP) is 6 to 15 mmHg
• Right atrial pressure (RA) is -1 to 6 mmHg

6/1/2015
15
Definition of Advanced HF
2013 ACCF/AHA Heart Failure Guidelines
44
Advanced Heart Failure (HF)
• Defined as persistent symptoms (NYHA Class III or IV) that limit daily life despite routine therapy with agents of known benefit.
• Patients with medication intolerance • Inability to uptitrate conventional medications• Decreasing dosage due to intolerance/side effects • One year mortality may be as high as 30-50% • Goals of therapy
– Symptom relief – Prevent re-hospitalization – Prolong survival – Improve quality of life as end of life approaches
Recommendations for Therapies in the
Hospitalized Patient
2013 ACCF/AHA Heart Failure Guidelines
6/1/2015
16
Case Study 1 : WD
• BMP: Na 130, K 4.0, BUN 20, Cr 1.6
• CBC: WBC 5.0, Hgb 11.5, Hct 32.3, plt 232
• Cardiac BNP: 1160
• Cardiac biomarkers (CK-MB, trop): normal
• 12 lead ECG: Sinus tachycardia, vent rate: 110 bpm, normal axis
• CXR: cardiomegaly
Hyponatremia
• Hyponatremia defined as serum sodium concentration <136 mmol/L
• Mild hyponatremia is seen in approximately 25% of patients with acute HF
• Hyponatremia poses significantly greater risk of death after discharge
• Reduction in cardiac output triggers hyponatremia.
• Hyponatremia is one of the strongest predictors for poor outcomes in HF patients
• Hyponatremia may be caused by multiple factors:
– RAAS: Aldosterone causes sodium and water retention.
– Antidiuretic Hormone, Vasopressin, ADH
– Impaired renal function leads to a decreased ability of the kidneys to excrete sodium and water.
• Efforts should be made to limit nephrotoxic medications and therapies such as
– Dye loads
– NSAIDS
– Antibiotics
Hyponatremia as a Prognostic Tool
W. H. Lee and M. Packer, “Prognostic importance of serum sodium concentration and its modification by converting-enzyme inhibition in patients with severe chronic heart failure,” Circulation, 1986.

6/1/2015
17
49
Therapy Options for Advanced HF
• Continuous intravenous inotropic medications
• Mechanical Circulatory Support
• Heart Transplantation
Mechanical Circulatory Support
• Temporary Devices
– Impella
– TandemHeart
– Centrimag
– ECMO
– IABP
• Long Term Devices
– VAD
– TAH
51
Mechanical Circulatory Support
• Indicated for patients who are on adequate medical therapy
but have:
– Hemodynamic concerns, symptomatic
– End organ dysfunction
– End stage cardiomyopathy
– Myocarditis
– Bridge to transplant
– Destination therapy
6/1/2015
18
52
Mechanical Circulatory Support
• Patient selection
– Appropriateness based on degree of illness
– Ability to successfully undergo surgery
– Ability to be discharged to home with adequate family
support for long term success
53
Heart Transplant
• Transplant community relies on United Network for Organ Sharing
(UNOS) for fair organ sharing
• Indications:
– NYHA IV on optimal medical therapy
– MVO2 < 14 % or <50 % predicted
– Reliable psychosocial support
– Insurance/financial resources to support life long immunosuppressive therapy
54
Heart Transplant
• Exclusion Criteria:
– Fixed Pulmonary Hypertension
– Active systemic infection
– Recent history of Cancer
– Obese with BMI > 35 – 40 (program specific)
– Documented history of noncompliance
– Life limiting disease other than HF
– End organ disease due to HF/poor perfusion
– Psychiatric illness that prevents compliance
– Active substance abuse
6/1/2015
19
Discharge Criteria for HF Patients
Recommendations for all patients with heart failure:
• Exacerbating factors addressed
• Optimal or at least near-optimal volume status achieved
• Transition from IV to oral diuretics successfully completed
• Patient & family education completed
• At least near-optimal pharmacologic therapy achieved
• Follow-up clinic visit scheduled, usually within 7 to 10 days
HFSA 2010 Comprehensive Heart Failure Practice Guideline
Discharge Criteria for Advanced HF/Recurrent
Admissions
Recommendations for patients with advanced HF /recurrent admissions for HF:
• Oral medications stable for 24 hours
• No IV vasodilator or inotropic agent needed during previous 24 hours
• Ambulation before discharge to assess functional capacity after therapy
• Referral for disease management
• Post discharge plans coordinated (eg, set of scales in home, visiting nurse or telephone follow-up scheduled for no later that 3 days after discharge)
HFSA 2010 Comprehensive Heart Failure Practice Guidelines
Recommendations for Hospital Discharge
2013 ACCF/AHA Heart Failure Guidelines

6/1/2015
20
Patient Education
• Salt Restriction (2 gm), avoid potassium-
salt based substitutes
• Fluid Restriction (2 liters /8 cups)
• Monitor daily weight
• Take medications as prescribed
• Notify healthcare provider with
temperature > 1000
• Alcoholic Restriction
• Exercise Training
• Monitoring use of NSAID’s
• Prevent infections (vaccinations)
Teaching Self-Care Maintenance
• Patient must be engaged in their management
• Knowledge is important in achieving treatment adherence but skill building is another essential component
• Assess potential barriers
• Once daily dosing if possible
• Always provide written instruction
• Follow up calls and visits improve adherence
• Do not assume patients’ take medications all of the time
Plans for WD’s Discharge
• Return to outpatient HF Clinic within 7 days
• Dietary education provided
• Self-care education
• Medication education
– Changed diuretic from furosemide to torsemide
– Added Bidil
6/1/2015
21
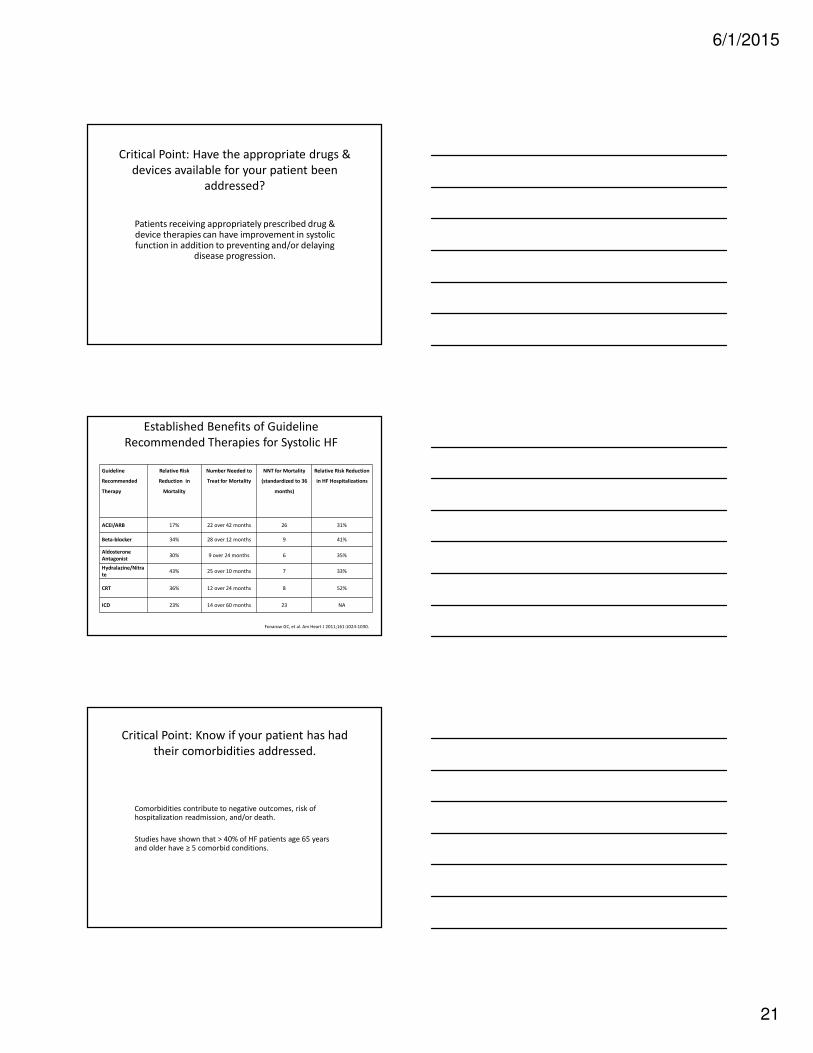
Critical Point: Have the appropriate drugs &
devices available for your patient been
addressed?
Patients receiving appropriately prescribed drug & device therapies can have improvement in systolic function in addition to preventing and/or delaying
disease progression.
Established Benefits of Guideline
Recommended Therapies for Systolic HF
Fonarow GC, et al. Am Heart J 2011;161:1024-1030.
Guideline
Recommended
Therapy
Relative Risk
Reduction in
Mortality
Number Needed to
Treat for Mortality
NNT for Mortality
(standardized to 36
months)
Relative Risk Reduction
in HF Hospitalizations
ACEI/ARB 17% 22 over 42 months 26 31%
Beta-blocker 34% 28 over 12 months 9 41%
Aldosterone
Antagonist30% 9 over 24 months 6 35%
Hydralazine/Nitra
te43% 25 over 10 months 7 33%
CRT 36% 12 over 24 months 8 52%
ICD 23% 14 over 60 months 23 NA
Critical Point: Know if your patient has had
their comorbidities addressed.
Comorbidities contribute to negative outcomes, risk of hospitalization readmission, and/or death.
Studies have shown that > 40% of HF patients age 65 years and older have ≥ 5 comorbid conditions.
6/1/2015
22
64
Anemia
• Estimated prevalence in 10-55% of HF patients; similar in
systolic and diastolic HF
• World Health Organization (WHO) definition is hemoglobin in
men<13gm/dL; women<12gm/dL
• Risk factors:
– Increased age
– Female
– Decreased body mass index (BMI)/ cachexia
– Use of rennin-aldosterone system blockers (ACE-I or ARB), beta
blockers
– Patients with more severe heart failure
– Chronic Kidney Disease
Managing Comorbid Conditions
• Anemia
– Severity may ↑the severity of HF
– Associated with:
• worsening symptoms of HF
• greater impairment in functional capacity
• ↓ survival
Nieminen et al, Eur Heart J. 2005; 26:384-416.
66
COPD
• Occurs in 11-52% in patients with HF
• Likely under-estimated since FEV1 is not routinely
performed to assess respiratory status
• HF and COPD presents diagnostic challenge and is
associated with worse outcomes
• Stable COPD is not a contraindication for beta-
blocker therapy

6/1/2015
23
67
Management of Diabetes Mellitus
Goal: HbA1c <7% (ACC/AHA Class IIb, Level of evidence A)
•Sulfonylurea associated with higher risk for HF than metformin
•Metformin- only diabetes drug with morbidity and mortality
benefit
�Concern for lactic acidosis in severe HF
�Contraindicated if creatinine >1.5 men;>1,4 in women
•Thiazolidinediones are associated with fluid retention
68
Neuropathic Pain and HF
• Pregabalin – analog of a neurotransmitter
– Exhibits analgesic, anticonvulsant and anxiolytic properties
– Potential side effects
• Dizziness and somnolence
• Peripheral edema 5-20%
• Weight gain 4-12%
– Food and Drug Administration (FDA) warning about possible
hypotension and edema especially if used with a TZD
– FDA cautions against use in NYHA class III or IV
Managing Comorbid Conditions
Cognitive impairment
– Seen as forgetfulness, attention & memory problems, and decreased
concentration
– Twice as likely in HF patients > 65 years of age
– In a study of elderly patients with HF:
• Only 50% could name their medications after receiving verbal and
written information
• 75% had forgotten to take their medications on some occasion
Cline et al. Eur J Heart Fail. 1999; 1: 145-149.

6/1/2015
24
70
Arthritis
One of the top 10 co-morbidities in HF– Most common is osteoarthritis
Management
1. Physical therapy
2. Capsaicin topical (chronic pain only)
3. Lidocaine 5% patch – neuropathic pain
4. Glucosamine/chondroitin – 40%
patients have a clinical response
5. Intra-articular therapies
6. Narcotics
Staging Heart Failure:
Focus on Disease Progression
� Marked symptoms at rest despite maximal medical therapy (eg, those who
are recurrently hospitalized or cannot be safely discharged from the hospital without specialized interventions)
Refractory
end-stage HFD
� Known structural heart disease� Shortness of breath and fatigue
� Reduced exercise tolerance
Symptomatic HFC
� Previous MI� LV systolic dysfunction
� Asymptomatic valvular disease
Asymptomatic HFB
� Hypertension� CAD
� Diabetes mellitus� Family history of cardiomyopathy
High risk for developing
heart failure (HF)A
Patient DescriptionStage
Treatment Recommendations for Stage A HF
2013 ACCF/AHA Heart Failure Guidelines
6/1/2015
25
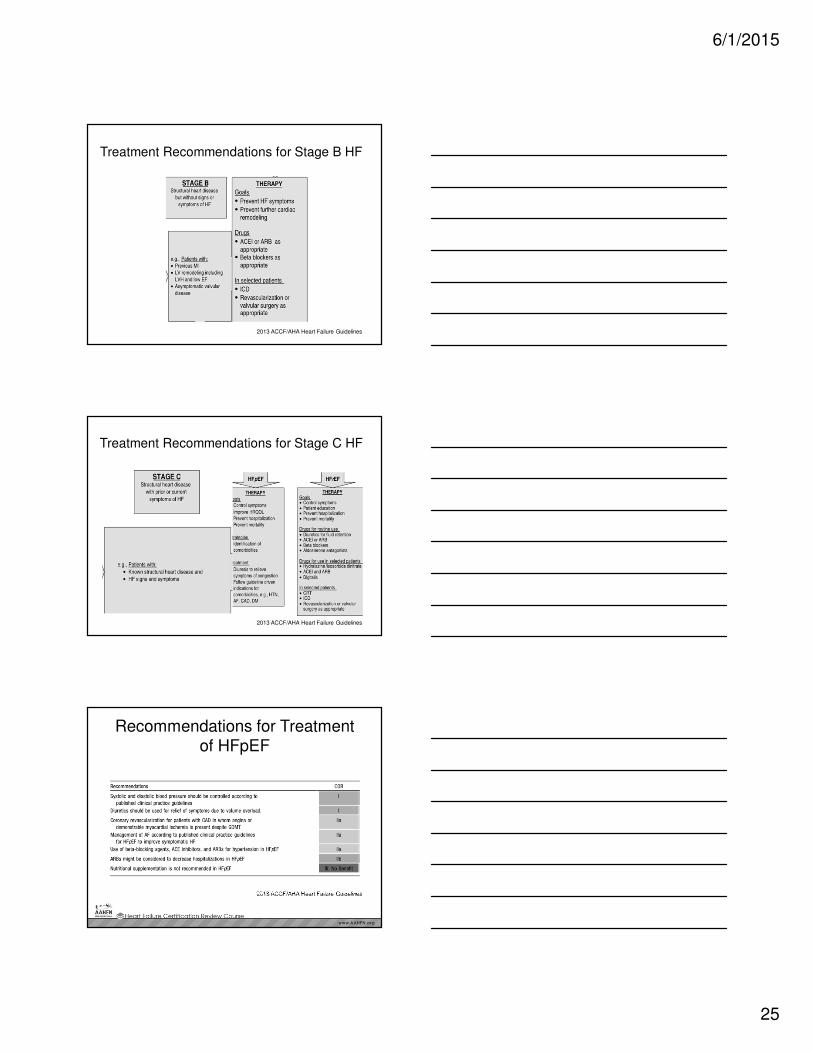
Treatment Recommendations for Stage B HF
2013 ACCF/AHA Heart Failure Guidelines
Treatment Recommendations for Stage C HF
2013 ACCF/AHA Heart Failure Guidelines
Recommendations for Treatment of HFpEF
2013 ACCF/AHA Heart Failure Guidelines

6/1/2015
26
Treatment Recommendations for Stage D HF
2013 ACCF/AHA Heart Failure Guidelines
Appendix
Guideline-Driven Medical Therapy for Systolic HF
77
Prevention: ACE-I • Blocks the conversion of angiotensin I to angiotensin II; prevents functional
deterioration
• Recommended for all heart failure patients
• Relieves symptoms and improves exercise tolerance
• Reduces risk of death and decreases disease progression
• Benefits may not be apparent for 1-2 months after initiation
ACE inhibitors are recommended for prevention of HF in patients at high risk for
this syndrome, including those with:
– Coronary artery disease
– Peripheral vascular disease
– Stroke
– Diabetes and other major risk factor Strength of Evidence = A
ACE inhibitors and beta blockers are recommended for all pts with prior MI.Strength of Evidence = A

6/1/2015
27
ACE Inhibitors Used in Clinical Trials
Generic Name Trade Name Initial Daily
Dose
Target Dose Mean Dose in
Clinical Trials
Captopril Capoten 6.25 mg tid 50 mg tid 122.7 mg/day
Enalapril Vasotec 2.5 mg bid 10 mg bid 16.6 mg/day
Fosinopril Monopril 5-10 mg qd 80 mg qd N/A
Lisinopril Zestril, Prinivil 2.5-5 mg qd 20 mg qd 4.5 mg/day, 33.2
mg/day*
Quinapril Accupril 5 mg bid 80 mg qd N/A
Ramipril Altace 1.25-2.5 mg qd 10 mg qd N/A
Trandolapril Mavik 1 mg qd 4 mg qd N/A
*No mortality difference between high and low dose groups, but 12% lower risk of death or
hospitalization in high dose group vs. low dose group. HFSA 2010 Practice Guideline
ACE-I Substitutions
It is recommended that other therapy be substituted for ACE inhibitors in the following circumstances:
– In patients who cannot tolerate ACE inhibitors due to cough, ARBs are recommended. Strength of Evidence = A
– The combination of hydralazine and an oral nitrate may be considered in such patients not tolerating ARBs.
Strength of Evidence = C
– Patients intolerant to ACE inhibitors from hyperkalemia or renal insufficiency are likely to experience the same side effects with ARBs. In these cases, the combination of hydralazine and an oral nitrate should be considered.
Strength of Evidence = C
HFSA 2010 Practice Guideline
Angiotensin Receptor Blockers (ARB)
• Block AT1 receptors, which bind circulating angiotensin II
• ACEi remains the first choice for inhibition of the renin-
angiotensin-aldosterone system in systolic HF but ARBs are a
reasonable alternative
• ARBs should be used to treat patients who are ACEi intolerant
due to intractable cough or who develop angioedema

6/1/2015
28
ARBs Used in Clinical Trials
Generic Name Trade Name Initial Daily Dose Target Dose Mean Dose in
Clinical Trials
Candesartan Atacand 4-8 mg qd 32 mg qd 24 mg/day
Losartan Cozaar 12.5-25 mg qd 150 mg qd 129 mg/day
Valsartan Diovan 40 mg bid 160 mg bid 254 mg/day
HFSA 2010 Practice Guideline
Beta Blockers
• Cardioprotective effects due to blockade of excessive SNS stimulation
• In the short-term, beta blocker decreases myocardial contractility;
increase in EF after 1-3 months of use
• Long-term, placebo-controlled trials have shown symptomatic
improvement in patients treated with certain beta-blockers1
• When combined with conventional HF therapy, beta-blockers reduce
the combined risk of morbidity and mortality, or disease progression1
• Improve left ventricular function
• ↓ Symptoms of HF
• Improve exercise tolerance
• ↓ Mortality
• ↓ HospitalizationHFSA 2010 Practice GuidelineACCF/AHA 2009 HF Update
Beta Blockers
When to initiate:
• Stable or maximally compensated patients
• Avoid initiating in decompensated patients
• May be started before discharge in patients hospitalized for HF, provided they do not require inotropic therapy for HF 2013 ACCF/AHA Heart Failure Guidelines
Symptomatic ExacerbationContinuation of beta blocker therapy is recommended in most patients experiencing a symptomatic exacerbation of HF during chronic maintenance treatment, unless they develop cardiogenic shock, refractory volume overload, or symptomatic bradycardia.
Strength of Evidence = C
– Temporary dose reduction may be considered– Avoid abrupt discontinuation– Reinstate or gradually increase prior to discharge– Titrate dose to previously tolerated dose as soon as possible
HFSA 2010 Practice Guideline

6/1/2015
29
Beta Blockers
Concomitant Disease
Beta blocker therapy is recommended in the great majority of patients with HF and reduced LVEF—even if there is concomitant diabetes, chronic obstructive lung disease or peripheral vascular disease.
– Use with caution in patients with:
� Diabetes with recurrent hypoglycemia
� Asthma or resting limb ischemia.
– Use with considerable caution in patients with marked bradycardia (<55 bpm) or marked hypotension (SBP < 80 mmHg).
– Not recommended in patients with asthma with active bronchospasm. Strength of Evidence = C
HFSA 2010 Practice Guideline
Beta Blockers
Preserved LVEF
Beta blocker treatment is recommended in patients with HF and preserved LVEF who have:
– Prior MI Strength of Evidence = A
– Hypertension Strength of Evidence = B
– Atrial fib. requiring control of ventricular rate Strength of Evidence = B
The elderly
Beta-blocker and ACE inhibitor therapy is recommended as standard therapy in all elderly patients with HF due to LV systolic dysfunction.
Strength of Evidence = B
In the absence of contraindications, these therapies are also recommended in the very elderly (age > 80 years).
Strength of Evidence = C
HFSA 2010 Practice Guideline
Beta Blocker Overview
General considerations Initiate at low doses
Up-titrate gradually, generally no sooner than at 2 week intervals
Use target doses shown to be effective in clinical trials
Aim to achieve target dose in 8-12 weeks
Maintain at maximum tolerated dose
If symptoms worsen or
other side effects appear
Adjust dose of diuretic or concomitant vasoactive med.
Continue titration to target after symptoms return to baseline
If up-titration continues to
be difficult
Prolong titration interval
Reduce target dose
Consider referral to a HF specialist
HFSA 2010 Practice Guideline
6/1/2015
30
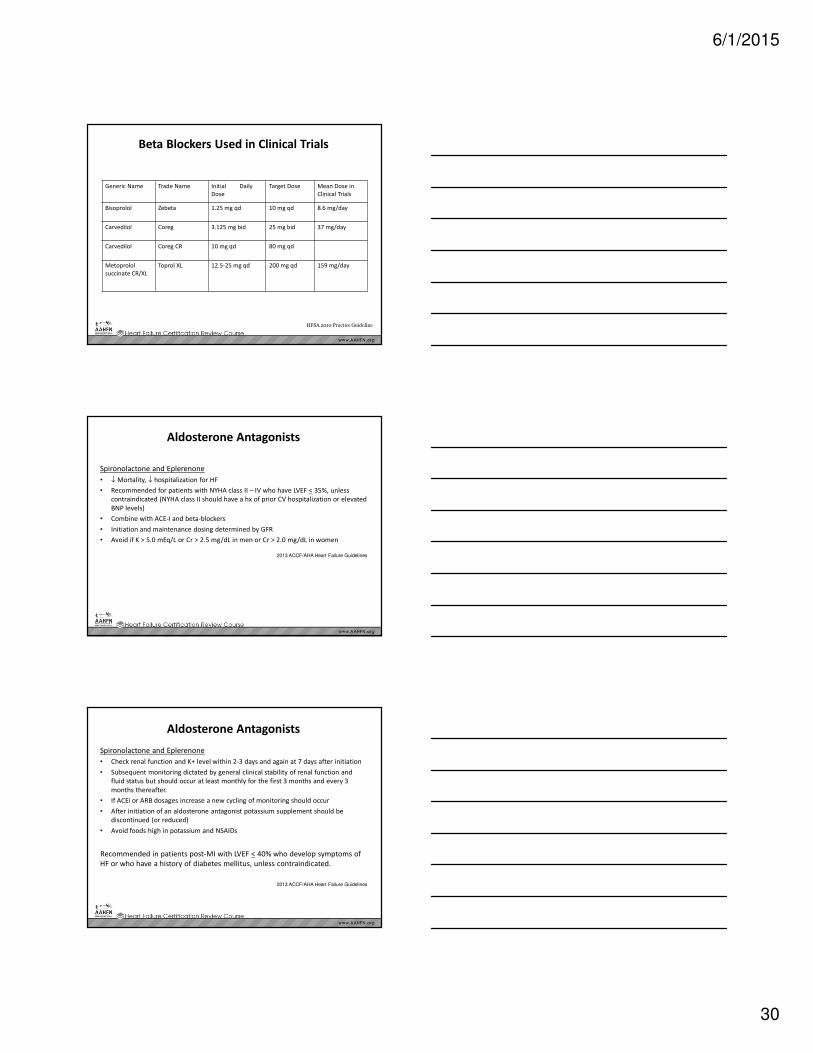
Beta Blockers Used in Clinical Trials
Generic Name Trade Name Initial Daily
Dose
Target Dose Mean Dose in
Clinical Trials
Bisoprolol Zebeta 1.25 mg qd 10 mg qd 8.6 mg/day
Carvedilol Coreg 3.125 mg bid 25 mg bid 37 mg/day
Carvedilol Coreg CR 10 mg qd 80 mg qd
Metoprolol
succinate CR/XL
Toprol XL 12.5-25 mg qd 200 mg qd 159 mg/day
HFSA 2010 Practice Guideline
Aldosterone Antagonists
Spironolactone and Eplerenone
• ↓ Mortality, ↓ hospitalization for HF
• Recommended for patients with NYHA class II – IV who have LVEF < 35%, unless
contraindicated (NYHA class II should have a hx of prior CV hospitalization or elevated
BNP levels)
• Combine with ACE-I and beta-blockers
• Initiation and maintenance dosing determined by GFR
• Avoid if K > 5.0 mEq/L or Cr > 2.5 mg/dL in men or Cr > 2.0 mg/dL in women
2013 ACCF/AHA Heart Failure Guidelines
Aldosterone Antagonists
Spironolactone and Eplerenone
• Check renal function and K+ level within 2-3 days and again at 7 days after initiation
• Subsequent monitoring dictated by general clinical stability of renal function and
fluid status but should occur at least monthly for the first 3 months and every 3
months thereafter.
• If ACEi or ARB dosages increase a new cycling of monitoring should occur
• After initiation of an aldosterone antagonist potassium supplement should be
discontinued (or reduced)
• Avoid foods high in potassium and NSAIDs
Recommended in patients post-MI with LVEF < 40% who develop symptoms of
HF or who have a history of diabetes mellitus, unless contraindicated.
2013 ACCF/AHA Heart Failure Guidelines
6/1/2015
31
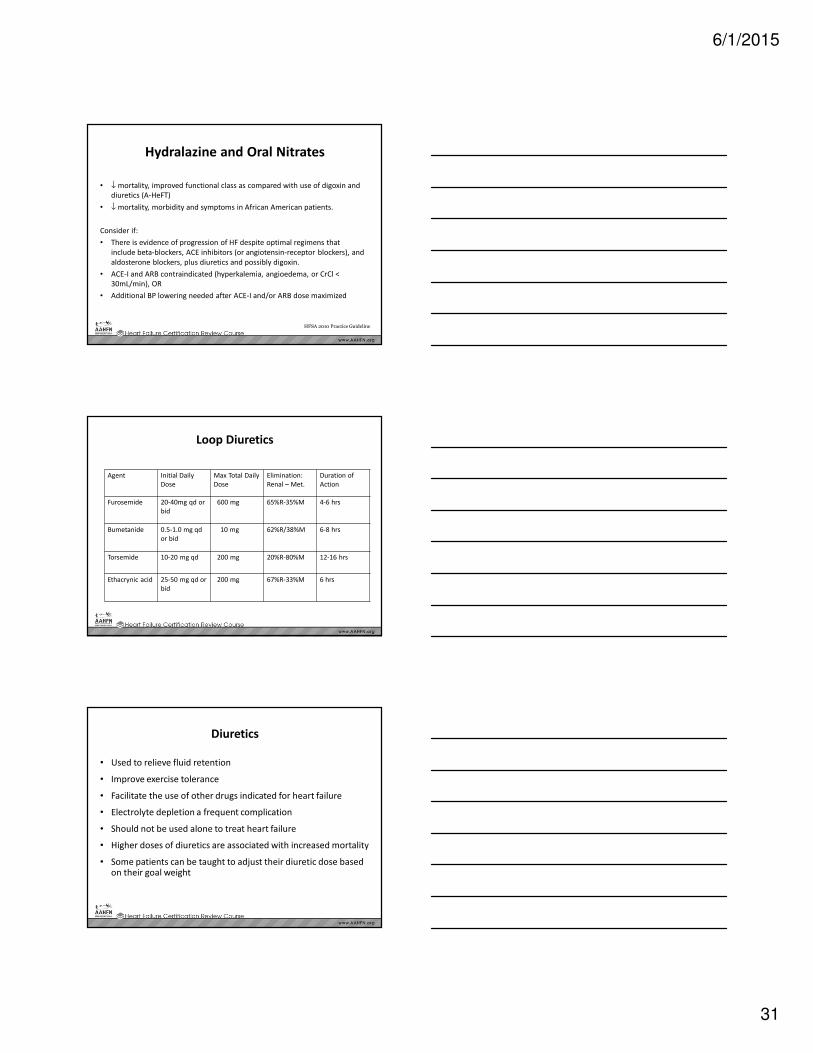
Hydralazine and Oral Nitrates
• ↓ mortality, improved functional class as compared with use of digoxin and
diuretics (A-HeFT)
• ↓ mortality, morbidity and symptoms in African American patients.
Consider if:
• There is evidence of progression of HF despite optimal regimens that
include beta-blockers, ACE inhibitors (or angiotensin-receptor blockers), and
aldosterone blockers, plus diuretics and possibly digoxin.
• ACE-I and ARB contraindicated (hyperkalemia, angioedema, or CrCl <
30mL/min), OR
• Additional BP lowering needed after ACE-I and/or ARB dose maximized
HFSA 2010 Practice Guideline
Loop Diuretics
Agent Initial Daily
Dose
Max Total Daily
Dose
Elimination:
Renal – Met.
Duration of
Action
Furosemide 20-40mg qd or
bid
600 mg 65%R-35%M 4-6 hrs
Bumetanide 0.5-1.0 mg qd
or bid
10 mg 62%R/38%M 6-8 hrs
Torsemide 10-20 mg qd 200 mg 20%R-80%M 12-16 hrs
Ethacrynic acid 25-50 mg qd or
bid
200 mg 67%R-33%M 6 hrs
Diuretics
• Used to relieve fluid retention
• Improve exercise tolerance
• Facilitate the use of other drugs indicated for heart failure
• Electrolyte depletion a frequent complication
• Should not be used alone to treat heart failure
• Higher doses of diuretics are associated with increased mortality
• Some patients can be taught to adjust their diuretic dose based on their goal weight
6/1/2015
32
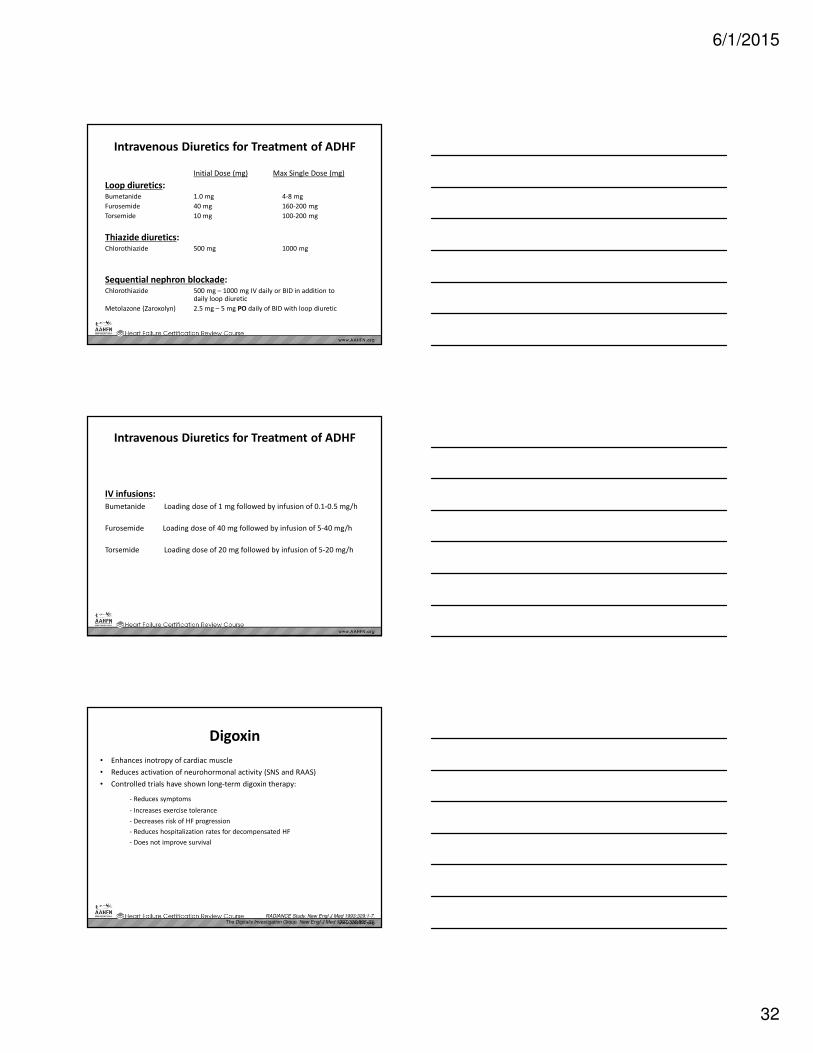
Intravenous Diuretics for Treatment of ADHF
Initial Dose (mg) Max Single Dose (mg)
Loop diuretics:Bumetanide 1.0 mg 4-8 mg
Furosemide 40 mg 160-200 mg
Torsemide 10 mg 100-200 mg
Thiazide diuretics:Chlorothiazide 500 mg 1000 mg
Sequential nephron blockade:Chlorothiazide 500 mg – 1000 mg IV daily or BID in addition to
daily loop diuretic
Metolazone (Zaroxolyn) 2.5 mg – 5 mg PO daily of BID with loop diuretic
Intravenous Diuretics for Treatment of ADHF
IV infusions:
Bumetanide Loading dose of 1 mg followed by infusion of 0.1-0.5 mg/h
Furosemide Loading dose of 40 mg followed by infusion of 5-40 mg/h
Torsemide Loading dose of 20 mg followed by infusion of 5-20 mg/h
Digoxin
• Enhances inotropy of cardiac muscle
• Reduces activation of neurohormonal activity (SNS and RAAS)
• Controlled trials have shown long-term digoxin therapy:
- Reduces symptoms
- Increases exercise tolerance
- Decreases risk of HF progression
- Reduces hospitalization rates for decompensated HF
- Does not improve survival
RADIANCE Study. New Engl J Med 1993;329:1-7.The Digitalis Investigation Group. New Engl J Med 1997;336:525-33.
6/1/2015
33
97
Other Meds Frequently Prescribed
• Electrolyte supplements: Potassium and magnesium
supplementation as needed with monitoring of serum
electrolytes to assess response to therapy.
• Statins: Patients with HF often have co-morbid conditions that
necessitate the use of statin therapy (diabetes, coronary artery
disease, cerebrovascular disease, peripheral vascular disease).
Statin therapy should be prescribed based on current guidelines
for these conditions.
98
Accreditation Agencies for HF Certification
• The Joint Commission Disease-specific Certificationoffers basic and advanced certification:
– For advanced certification, a center must already have achieved Get With The Guidelines Bronze Level and work towards meeting standards
• The Society of Chest Pain Centers:
– Accreditation that includes a collaborative approach providing resources, education, feedback towards improving gaps in processes of care.
• The Healthcare Accreditation Colloquium
– The Colloquium centers its approach around accreditation as an opportunity for improvement of relationships, processes, systems, and outcomes for HF patients.
99
Quality Improvement
• Quality improvement is a process of purposeful change toward meeting accepted quality standards for a health care population.
• Quality improvement teams
– Employ quality of care performance indicators that are described in clinical practice guidelines
– Use data for measuring progress
– Ensure ways to evaluate and address gaps in the quality of care
– Repeat evaluations or audits over time to ensure the care level is maintained and continually evaluated for further improvement

6/1/2015
34
100
The Nurse’s Role Quality Improvement
• Know the indicators being used to measure quality in one’s work environment
• Be familiar with mechanisms to capture data and report on the quality indicators for HF (Core Measures)
• Participate in quality improvement meetings and projects• Identify disparities or gaps in clinical management of HF
patients.• Incorporate evidence-based practices and professional
guideline recommendations when managing patients with HF.
• Use a collaborative (interdisciplinary) framework when planning actions for quality improvement.
• Assist with achieving accreditation or certification for specialty HF services to gain recognition for quality improvement processes and improved outcomes.
101
Measuring Outcomes• Structural indicators are those indicators that relate to the
organization and delivery of care
• Examples of structural indicators that may improve quality of HF care include:
– Telephone support and telemonitoring
– Electronic health records as a means of communication and data collection
– Access to providers- family practice, cardiologists, HF specialist
– Access to healthcare for minority/marginal or high risk groups (older patients, multiple co-morbid conditions, ethnic groups and women
– Mechanisms to support and evaluate patient adherence and health literacy
102
Inpatient Process of Care Indicators
• Core Measures for HF as adopted by The Joint Commission and Centers for Medicare and Medicaid in the United States have been established as indicators for inpatient processes of care since May 2001.
– Documentation on the medical record that left ventricular systolic function (LVEF) was evaluated before arrival, during hospitalization, or is planned after discharge.
– HF patients with LVEF < 40% are prescribed an angiotensin converting enzyme (ACE) inhibitor or an angiotensin receptor blocker (ARB) unless a contraindication is documented.
6/1/2015
35
103
Core Measures for HF
Discharge instructions are to be provided in writing to patients/caregivers at time of discharge from hospital addressing all of the following:
• Activity level
• Diet
• Discharge medications
• Follow-up appointment
• Weight monitoring
• What to do if symptoms worsen
104
Get with the Guidelines-HF
• Developed by the American Heart Association
– offers educational opportunities, national and local recognition, and support with a data management tool for tracking clinical details for internal and external comparison.
– Hospitals can purchase the data management tool and manual.
– Clinical teams are supported to educate staff and implement care based on the latest HF guidelines.
105
Hospital to Home (H2H)
• National quality improvement to reduce unnecessary readmissions for cardiovascular patients through national networking and learning initiatives
• H2H’s goal is to reduce all-cause readmission rates by 20% among patients discharged with HF or acute MI by December 2012
• Core concepts: medication management post-discharge, early follow-up, symptom management
• Although care that prevents readmission occurs largely outside hospitals, it starts in hospitals
6/1/2015
36
106
Institute for Healthcare Improvement (IHI)
• Offers education and tools for implementation of core processes for improving the treatment of HF.
• Tools and recommended steps for the “ideal transition home” focus on these four components:
– Enhanced admission assessment for post-discharge needs (e.g. caregivers, medication reconciliation).
– Enhanced teaching and learning – how to tailor patient/family education
– Patient and family-centered handoff communication (e.g. medication reconciliation, critical elements to communicate to families, physicians, and other involved agencies.
– Post-acute care follow-up – inclusion of home care or telephone follow-up for high or moderately high risk patients.





















![NANCY M. ALBERT, PhD, CCNS, CHFN, CCRN, NE-BC, FAHA, … · 2015-11-12 · Clinical Ladder: What's in a Name? [Manuscript in development; Presented locally]. 2009. Coach. The Importance](https://img.pdfslide.us/doc/110x75/5f77612265d88a0b146a3e34/nancy-m-albert-phd-ccns-chfn-ccrn-ne-bc-faha-2015-11-12-clinical-ladder.jpg)






