Embed Size (px)
Citation preview

Clinical Radiology (1991) 43, 337-340
Chest Radiographs are Unreliable in Predicting Thrombi in the Left Atrium or its Appendage in Rheumatic Mitral Stenosis S. SHARMA, M. V. KUMAR*, S. AGGARWAL, V. M. REDDYt , U. KAUL*, M. RAJANI and P. V E N U G O P A L t
Department o f Cardiovascular Radiology, *Cardiology, and t Cardiothoracic and Vascular Surgery, Cardiothoracic Centre, Al l India Institute o f Medical Sciences, New Delhi
We have assessed the diagnostic accuracy of a flat or concave left mid-cardiac border (the region of the left atrial appendage) on conventional postero-anterior chest radiographs as a predictor of the presence of thrombi in the left atrium or its appendage in 80 patients with rheumatic mitral stenosis who subsequently underwent open-heart surgery. Forty-six patients (Group I) were found to have left atrial thrombus at surgery whereas 34 patients (Group II) showed no evidence of thrombosis. Only 22 of 46 patients in Group I showed a flat or concave left mid-cardiac border (sensitivity, 48%; specificity, 53%; positive predictive value, 58%). Furthermore in Group 1, the thrombus involved the left atrial appendage in 33 patients. In this subgroup only 14 patients showed a flat or concave left mid-cardiac border (sensitivity, 42%; specificity, 49 %; positive predictive value, 37 %). The presence of flatness or concavity in the left mid-cardiac border on conventional postero-anterior chest radiographs in patients with rheumatic mitral stenosis is an unreliable indicator of the presence of thrombi in the left atrium or its appendage. Sharma, S., Kumar, M.V., Aggarwal, S., Reddy, V.M., Kaul, U., Rajani, M. & Venugopal, P. (1991). Clinical Radiology 43, 337-340. Chest Radiographs are Unreliable in Predicting Thrombi in the Left Atrium or its Appendage in Rheumatic Mitral Stenosis
Thrombosis of the left atrium or its appendage is frequent in dominant rheumatic mitral valve stenosis and is said to occur in 22% of patients at surgery and in 35.8% of patients at autopsy (Nichols et al., 1962; Wallach et al., 1963). Most thrombi are small and occur in the vicinity of the appendage, but occasionally a large thrombus may extend along the posterior wall of the left atrium. It is important to pre-operatively localize the thrombus as this dictates the choice of surgery for mitral valve disease. Various imaging techniques including plain radiography, fluoroscopy, echocardiography, angiocardiography, computed tomography and scintigraphy have been uti- lized for the pre-operative localization of left atrial thrombi (Arendt and Cardon, 1949; Soloff and Zatuchni, 1956; Swanson and Steinberg, 1964; Lewis et al., 1965; Parker et al., 1965; Baue et al., 1968; Spangler and Okin, 1975; Cipriano and Guthaner, 1978; Colman et al., 1981; Nair et al., 1981; Schweizer et al., 1981; Matsuyama et al., 1983; Shrestha et al., 1983; Tomoda et al., 1983; Eriksson et al., 1984; Yamada et al., 1984; Hubbard et al., 1987).
Conventional plain chest radiography is simple, econo- mical and the most widely available imaging technique. It would be ideal if accurate pre-operative localization of left atrial thrombus could be made by plain radiography. It was initially reported that an undue prominence of the left mid-cardiac border (in the region of the left atrial appendage) in a patient with rheumatic mitral valve disease was suggestive of left atrial thrombosis (Arendt and Cardon, 1949). Subsequently, based on their experi- ence with 10 patients with surgically proven left atrial thrombi, Matsuyama et al. (1983) reported that the absence of convexity of the left mid-cardiac border in
Correspondence: Dr S. Sharma, Department of Radiodiagnosis, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, India.
patients with mitral valve disease was suggestive of thrombi in the left atrial appendage. This sign had a diagnostic accuracy of 66.7%.
In view of these conflicting reports, we planned the present study in order to assess the predictive value of the presence or absence of a bulge in the left mid-cardiac border as an indicator of thrombosis of the left atrium or its appendage in a number of patients with rheumatic mitral stenosis.
MATERIALS A N D M E T H O D S
Pre-operative chest radiographs of 46 patients with rheumatic mitral stenosis who were proved to have thrombi in the left atrium and/or its appendage at surgery were retrospectively studied to assess the predictive value of the presence or absence of a bulge in the left mid- cardiac border (in the region of the left atrial appendage) as an indicator of the presence of left atrial thrombi. At the same time, immediate pre-operative chest radio- graphs of 34 patients with rheumatic mitral stenosis who underwent open-heart surgery and had no left atrial thrombi were also evaluated to serve as the 'control ' group. All the chest radiographs were assessed by two observers independently and without prior knowledge of the operative findings. Those excluded from the study were patients with associated mitral regurgitation (more than mild in grade), with a history of previous closed mitral valvotomy and those with suboptimal chest radio- graphs. Chest radiographs taken only in the immediate pre-operative period were included so as to minimize the time difference between chest radiographs and sub- sequent open-heart surgery.

338 CLINICAL RADIOLOGY
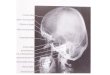
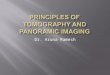
Fig. 1 -Convent ional chest postero-anterior radiograph in a patient with rheumatic mitral stenosis showing a bulge in the region of the left atrial appendage (arrow). The patient was subsequently found to have left atrial thrombosis at surgery (negative test).
STATISTICAL M E T H O D S
The result was considered as 'true positive' if both the chest radiograph and surgery were positive for thrombus, 'true negative' if both were negative for thrombus, 'false positive' if chest radiograph was positive but the surgery was negative for thrombus, and 'false negative' if the chest radiograph was negative but surgery was positive for thrombus.
The sensitivity, specificity and predictive accuracy were calculated as follows:
True positive Sensitivity = x 100
True positive + False negative
True negative Specificity= x 100
True negative + False positive
True positive Predictive accuracy = x 100
True positive + False positive
RESULTS
Pre-operative chest radiographs of a total of 80 patients with pure mitral stenosis or dominant mitral stenosis with up to mild mitral regurgitation and who subsequently underwent open-heart surgery were retrospectively ana- lysed. The patients were divided into two groups based on the presence or absence of left atrial thrombi at surgery.
Group I (those with evidence of left atrial thrombosis at
,5 ')~
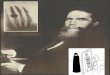
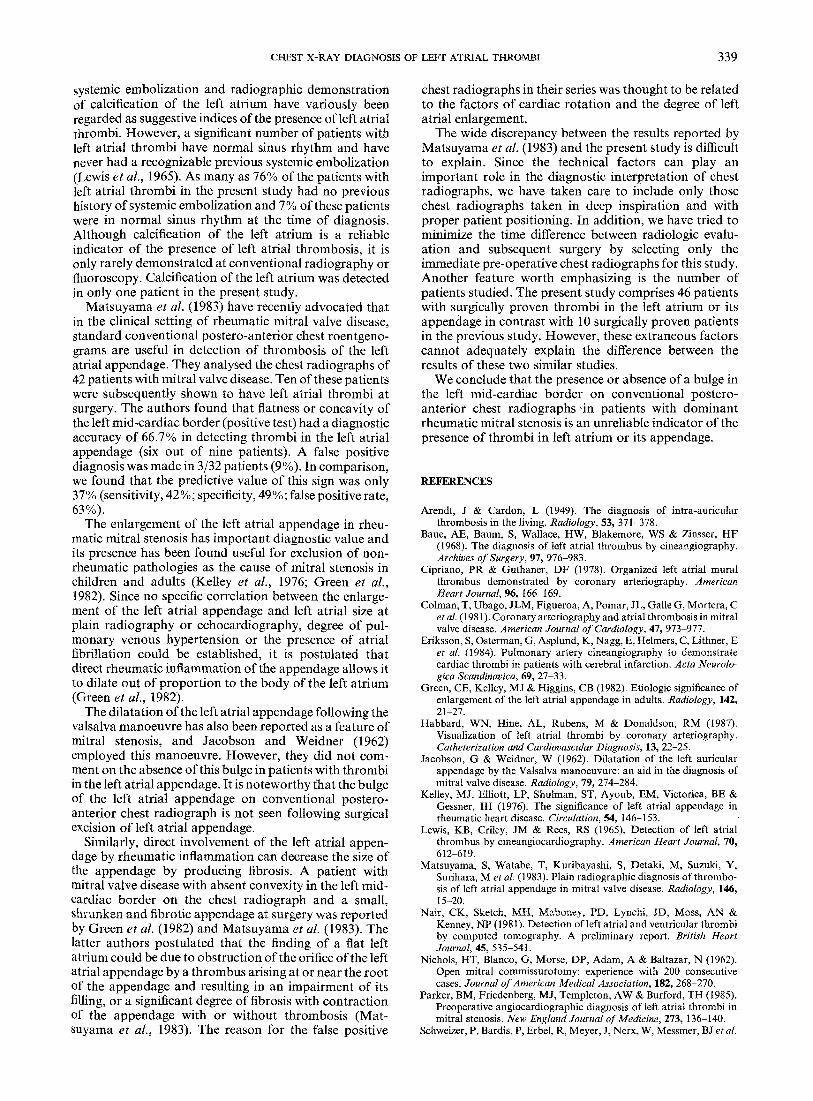
Fig. 2 - Conventional chest postero-anterior view m a patient with rheumatic mitral stenosis showing no bulge in the region of the left atrial appendage (arrow). The patient was subsequently shown to have left atrial thrombosis at surgery (positive test).
surgery) consisted of 46 patients. There were 34 males and ages ranged between 16 and 58 years (mean age 35.5 years). Forty-three of these patients were in atrial fibrilla- tion at the time of diagnosis (93%); a history of one or more embolic episodes was present in only 11 patients (24%). Twenty-four patients showed evidence of a bulge in the left mid-cardiac border (negative test) (Fig. 1) and 22 patients showed a flat or concave left mid-cardiac border (positive test) (Fig. 2). There were 34 patients in Group II (control group with no left atrial thrombi at surgery). Ages ranged between 16 and 52 years (mean age 30.5 years) and there were 21 males. Twenty of these patients were in atrial fibrillation at the time of diagnosis (59%). A bulge in the left mid-cardiac border (negative test) was seen in only 18 patients. The plain chest radiographic diagnosis of left atrial thrombi based on the absence of a bulge in the left mid-cardiac border (positive test), therefore, had a sensitivity of 48%; specificity of 53%, and predictive value of only 58%.
Further analysis of the 46 patients with thrombi in the left atrium showed that 33 patients had thrombi in the appendage with or without left atrial thrombosis and 13- patients had only left atrial thrombi. Among the 33 patients with appendage thrombi, 14 patients had a positive test and 19 patients a negative test. The predictive value of the plain radiograph in the diagnosis of appen- dage thrombi, therefore, was only 37% (sensitivity, 42%; specificity, 49%).
DISCUSSION
In patients with rheumatic mitral valve disease, the presence of atrial fibrillation, a history of previous
CHEST X-RAY DIAGNOSIS OF LEFT ATRIAL THROMBI 339
systemic embolization and radiographic demonstration of calcification of the left atrium have variously been regarded as suggestive indices of the presence of left atrial thrombi. However, a significant number of patients with left atrial thrombi have normal sinus rhythm and have never had a recognizable previous systemic embolization (Lewis et al., 1965). As many as 76% of the patients with left atrial thrombi in the present study had no previous history of systemic embolization and 7% of these patients were in normal sinus rhythm at the time of diagnosis. Although calcification of the left atrium is a reliable indicator of the presence of left atrial thrombosis, it is only rarely demonstrated at conventional radiography or fluoroscopy. Calcification of the left atrium was detected in only one patient in the present study.
Matsuyama et al. (1983) have recently advocated that in the clinical setting of rheumatic mitral valve disease, standard conventional postero-anterior chest roentgeno- grams are useful in detection of thrombosis of the left atrial appendage. They analysed the chest radiographs of 42 patients with mitral valve disease. Ten of these patients were subsequently shown to have left atrial thrombi at surgery. The authors found that flatness or concavity of the left mid-cardiac border (positive test) had a diagnostic accuracy of 66.7% in detecting thrombi in the left atrial appendage (six out of nine patients). A false positive diagnosis was made in 3/32 patients (9%). In comparison, we found that the predictive value of this sign was only 37 % (sensitivity, 42 %; specificity, 49 %; false positive rate, 63%).
The enlargement of the left atrial appendage in rheu- matic mitral stenosis has important diagnostic value and its presence has been found useful for exclusion of non- rheumatic pathologies as the cause of mitral stenosis in children and adults (Kelley et al., 1976; Green et al., 1982). Since no specific correlation between the enlarge- ment of the left atrial appendage and left atrial size at plain radiography or echocardiography, degree of pul- monary venous hypertension or the presence of atrial fibrillation could be established, it is postulated that direct rheumatic inflammation of the appendage allows it to dilate out of proportion to the body of the left atrium (Green et al., 1982).
The dilatation of the left atrial appendage following the valsalva manoeuvre has also been reported as a feature of mitral stenosis, and Jacobson and Weidner (1962) employed this manoeuvre. However, they did not com- ment on the absence of this bulge in patients with thrombi in the left atrial appendage. It is noteworthy that the bulge of the left atrial appendage on conventional postero- anterior chest radiograph is not seen following surgical excision of left atrial appendage.
Similarly, direct involvement of the left atrial appen- dage by rheumatic inflammation can decrease the size of the appendage by producing fibrosis. A patient with mitral valve disease with absent convexity in the left mid- cardiac border on the chest radiograph and a small, shrunken and fibrotic appendage at surgery was reported by Green et al. (1982) and Matsuyama et aL (1983). The latter authors postulated that the finding of a flat left atrium could be due to obstruction of the orifice of the left atrial appendage by a thrombus arising at or near the root of the appendage and resulting in an impairment of its filling, or a significant degree of fibrosis with contraction of the appendage with or without thrombosis (Mat- suyama et al., 1983). The reason for the false positive
chest radiographs in their series was thought to be related to the factors of cardiac rotation and the degree of left atrial enlargement.
The wide discrepancy between the results reported by Matsuyama et al. (1983) and the present study is difficult to explain. Since the technical factors can play an important role in the diagnostic interpretation of chest radiographs, we have taken care to include only those chest radiographs taken in deep inspiration and with proper patient positioning. In addition, we have tried to minimize the time difference between radiologic evalu- ation and subsequent surgery by selecting only the immediate pre-operative chest radiographs for this study. Another feature worth emphasizing is the number of patients studied. The present study comprises 46 patients with surgically proven thrombi in the left atrium or its appendage in contrast with 10 surgically proven patients in the previous study. However, these extraneous factors cannot adequately explain the difference between the results of these two similar studies.
We conclude that the presence or absence of a bulge in the left mid-cardiac border on conventional postero- anterior chest radiographs "in patients with dominant rheumatic mitral stenosis is an unreliable indicator of the presence of thrombi in left atrium or its appendage.
REFERENCES
Arendt, J & Cardon, L (1949). The diagnosis of intra-auricular thrombosis in the living. Radiology, 53, 371-378.
Baue, AE, Baum, S, Wallace, HW, Blakemore, WS & Zinsser, HF (1968). The diagnosis of left atrial thrombus by cineangiography. Archives of Surgery, 97, 976 983.
Cipriano, PR & Guthaner, DF (1978). Organized left atrial mural thrombus demonstrated by coronary arteriography. American Heart Journal, 96, 166 169.
Colman, T, Ubago, JLM, Figueroa, A, Pomar, JL, Galle G, Mortera, C et al. (1981). Coronary arteriography and atrial thrombosis in mitral valve disease. American Journal of Cardiology, 47, 973-977.
Eriksson, S, Osterman, G, Asplund, K, Nagg, E, Helmers, C, Lithner, E et al. (1984). Pulmonary artery cineangiography to demonstrate cardiac thrombi in patients with cerebral infarction. Acta Neurolo- gica Scandinaviea, 69, 27-33.
Green, CE, Kelley, MJ & Higgins, CB (1982). Etiologic significance of enlargement of the left atrial appendage in adults. Radiology, 142, 21-27.
Habbard, WN, Hine, AL, Rubens, M & Donaldson, RM (1987). Visualization of left atrial thrombi by coronary arteriography. Catheterization and Cardiovascular Diagnosis, 13, 22-25.
Jacobson, G & Weidner, W (1962). Dilatation of the left auricular appendage by the Valsalva manoeuvure: an aid in the diagnosis of mitral valve disease. Radiology, 79, 274-284.
Kelley, M J, Elliott, LP, Shulman, ST, Ayoub, EM, Victorica, BE & Gessner, IH (1976). The significance of left atrial appendage in rheumatic heart disease. Circulation, 54, 146-153.
Lewis, KB, Criley, JM & Rees, RS (1965). Detection of left atrial thrombus by cineangiocardiography. American Heart Journal, 70, 612-619.
Matsuyama, S, Watabe, T, Kuribayashi, S, Detaki, M, Suzuki, Y, Surihara, Met aL (1983). Plain radiographic diagnosis of thrombo- sis of left atrial appendage in mitral valve disease. Radiology, 146, 15-20.
Nair, CK, Sketch, MH, Maboney, PD, Lynchi, JD, M~ss, AN & Kenney, NP (1981). Detection of left atrial and ventricular thrombi by computed tomography. A preliminary report. British Heart Journal, 45, 535-541.
Nichols, HT, Blanco, G, Morse, DP, Adam, A & Baltazar, N (1962). Open mitral commissurotomy: experience with 200 consecutive cases. Journal o f American Medical Association, 182, 268-270.
Parker, BM, Friedenberg, MJ, Templeton, AW & Burford, TH (1985). Preoperative angiocardiographic diagnosis of left atrial thrombi in mitral stenosis. New England Journal of Medicine, 273, 136-140.
Schweizer, P, Bardis, P, Erbel, R, Meyer, J, Nerx, W, Messmer, BJ et al.

340 CLINICAL RADIOLOGY
(1981). Detection of left atrial thrombi by echocardiography. British Heart Journal, 45, 148 156.
Shrestha, NK, Moreno, PL, Narcise, FV, Torres, L & Callenga, HB (1983). Two dimensional echocardiographic diagnosis of left atrial thrombus in rheumatic heart disease. A clinicopathologic study. Circulation, 67, 341-347.
Soloff, LA & Zatuchni, J (1956). The angiocardiographic diagnosis of left atrial thrombus. Circulation, 14, 25-32.
Spangler, RD & Okin, JT (1975). Echocardiographic demonstration of a left atrial thrombus. Chest, 67, 716-721.
Swanson, GE & Steinberg, I (1964). Roentgen features of the atrial appendage. American Journal of Radiology, 91, 311-320.
Tomoda, H, Hoshiai, M, Puruya, H, Kuriboyashi, S, Ootaki, M, Matsuyama, Se t al. (1983). Evaluation of intracardiac thrombus with computed tomography. American Journal of Cardiology, 51, 843-852.
Wallach, JB, Lukash, L & Angrist, AA (1963). Interpretation of the incidence of mural thrombi in the left auricle and appendage with particular reference to mitral commissurotomy. American Heart Journal, 45, 252-254.
Yamada, M, Haki, N, Ishikawa, K, Yoshima, H, Hata, S, Okkube, Met al. (1984). Detection of left atrial thrombi in men using indium-111 labelled autologous platelets. British Heart Journal, 51, 298-305.