Embed Size (px)
Citation preview
Chartered Value Exchanges (CVEs)Chartered Value Exchanges (CVEs)
September 2008September 2008
CVEs may wish to tailor this slide deck for use CVEs may wish to tailor this slide deck for use with stakeholders in your community.with stakeholders in your community.
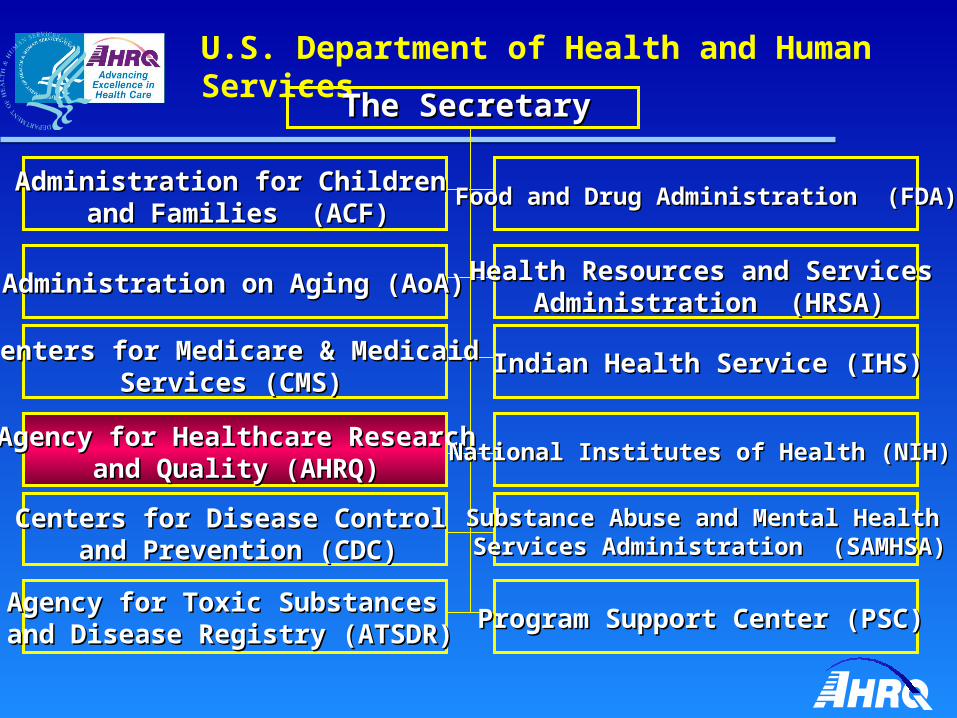
U.S. Department of Health and Human Services
The SecretaryThe Secretary
Administration for Children Administration for Children and Families (ACF)and Families (ACF)
Agency for Healthcare ResearchAgency for Healthcare Researchand Quality (AHRQ)and Quality (AHRQ)
Centers for Disease Control Centers for Disease Control and Prevention (CDC)and Prevention (CDC)
Agency for Toxic Substances Agency for Toxic Substances and Disease Registry (ATSDR)and Disease Registry (ATSDR) Program Support Center (PSC)Program Support Center (PSC)
Substance Abuse and Mental Health Substance Abuse and Mental Health Services Administration (SAMHSA)Services Administration (SAMHSA)
National Institutes of Health (NIH)National Institutes of Health (NIH)
Indian Health Service (IHS)Indian Health Service (IHS)
Health Resources and Services Health Resources and Services Administration (HRSA)Administration (HRSA)
Food and Drug Administration (FDA)Food and Drug Administration (FDA)
Centers for Medicare & MedicaidCenters for Medicare & MedicaidServices (CMS)Services (CMS)
Administration on Aging (AoA)Administration on Aging (AoA)

AHRQ’s Mission
Improve the quality, safety, efficiency and Improve the quality, safety, efficiency and effectiveness of health care for all Americanseffectiveness of health care for all Americans
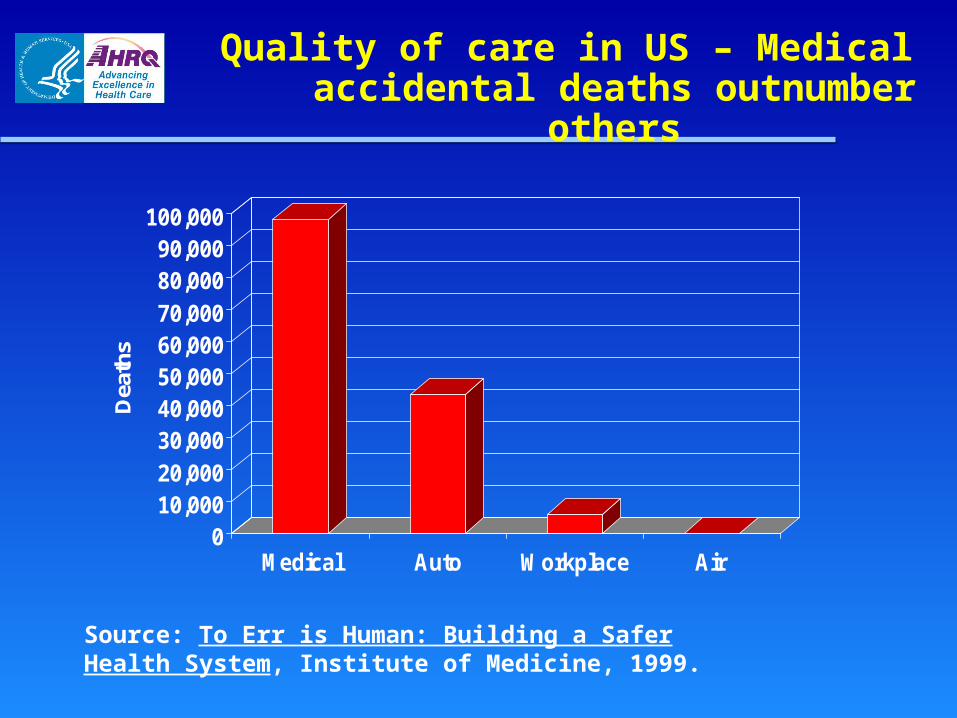
Quality of care in US – Medical accidental deaths outnumber others
010,00020,00030,00040,00050,00060,00070,00080,00090,000
100,000
Dea
ths
Medical Auto Workplace Air
Source: To Err is Human: Building a Safer Health System, Institute of Medicine, 1999.
2001 IOM Report, Crossing the Quality Chasm
Scientific review documents the scale and gravity Scientific review documents the scale and gravity of quality problemsof quality problems
More than 70 publications cite quality problemsMore than 70 publications cite quality problems
……between the health care we have and the care between the health care we have and the care we could have lies not just a gap, but a chasmwe could have lies not just a gap, but a chasm..
Patients’ care often deficient, study says. Proper treatment given half the time. On average, doctors provide appropriate health care only half thetime, a landmark study of adults in 12 U.S. metropolitan areas suggests.
Medical Care Often Not Optimal Failure to Treat Patients Fully Spans Range of What Is Expected of Physicians and Nurses
Study: U.S.Doctors are not following the guidelines for ordinary illnesses
The American healthcare system,often touted as a cutting-edge leader in the world, suddenlyfinds itself mired in serious questions about the ability of itshospitals and doctors to deliverquality care to millions.
Medical errors corrodequality of healthcare system
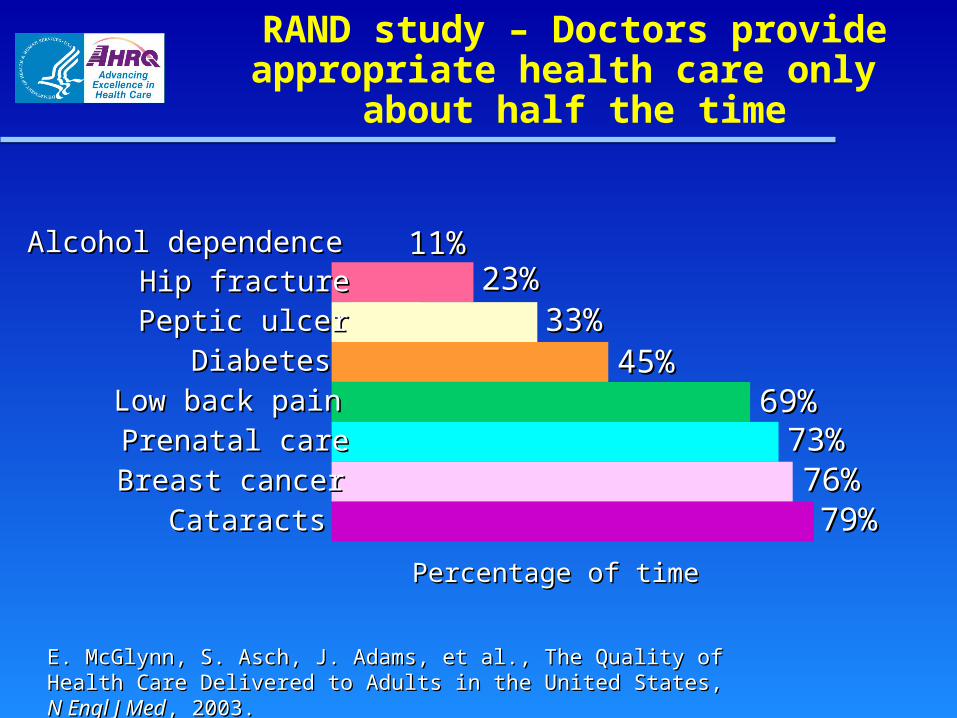
RAND study – Doctors provide appropriate health care only
about half the time
Percentage of timePercentage of time
Alcohol dependenceAlcohol dependence Hip fractureHip fracture
Peptic ulcerPeptic ulcer
DiabetesDiabetes
Low back painLow back pain
Prenatal carePrenatal care
Breast cancerBreast cancer
Cataracts Cataracts
11%11%23%23%
33%33%45%45%
69%69%73%73%76%76%79%79%
E. McGlynn, S. Asch, J. Adams, et al., The Quality of Health Care E. McGlynn, S. Asch, J. Adams, et al., The Quality of Health Care Delivered to Adults in the United States, Delivered to Adults in the United States, N Engl J MedN Engl J Med, 2003., 2003.
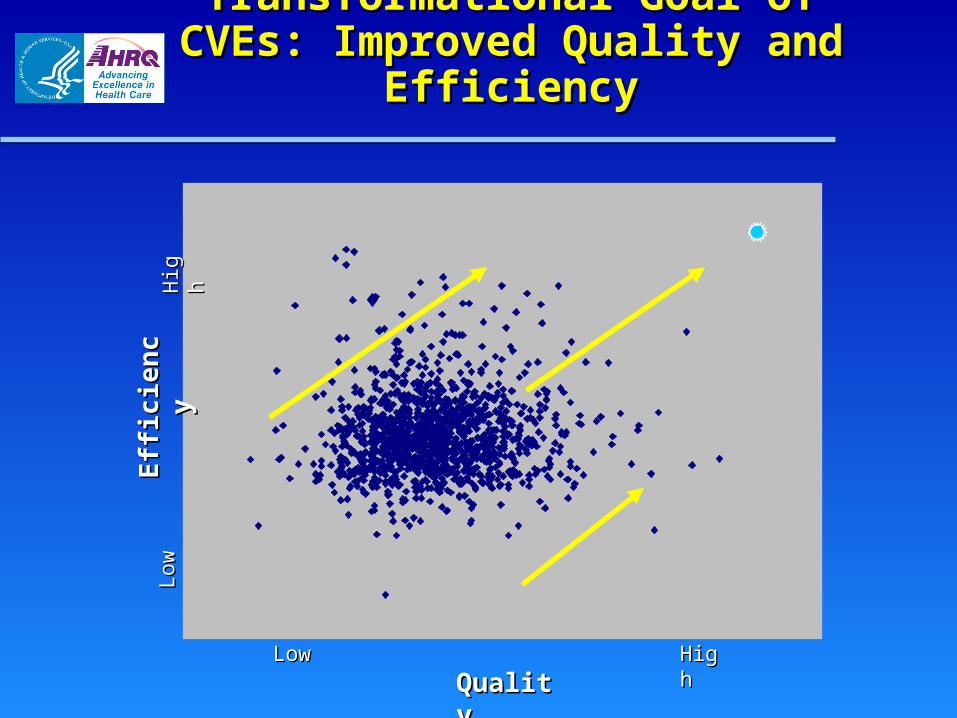
Transformational Goal of CVEs: Transformational Goal of CVEs: Improved Quality and EfficiencyImproved Quality and Efficiency
Low
Low
Hig
hH
igh
LowLow HighHigh
QualityQuality
Eff
icie
ncy
Eff
icie
ncy
What Will This Take?What Will This Take?
Good measures and dataGood measures and data
Strong local coalitionsStrong local coalitions
Evidence-based reporting, payment Evidence-based reporting, payment strategiesstrategies
Evidence, tools, strategies for improvementEvidence, tools, strategies for improvement
Collaboration across sitesCollaboration across sites
Focus of AHRQ Learning Focus of AHRQ Learning Network for CVEsNetwork for CVEs
Technical assistance content spans contemplation, Technical assistance content spans contemplation, design and implementation decisions across the design and implementation decisions across the following activities identified by user/stakeholders as following activities identified by user/stakeholders as high priority: high priority:
1.1. Collaborative leadership & sustainabilityCollaborative leadership & sustainability
2.2. Public at-large engagementPublic at-large engagement
3.3. Quality & efficiency measurementQuality & efficiency measurement
4.4. Public reportingPublic reporting
5.5. Provider incentivesProvider incentives
6.6. Consumer incentivesConsumer incentives
7.7. Capacity for improving qualityCapacity for improving quality
8.8. HIT/HIEHIT/HIE
AHRQ Learning Network Builds AHRQ Learning Network Builds on Secretary’s Value-Driven on Secretary’s Value-Driven
Health Care PrinciplesHealth Care Principles
1.1. All health care is “local”All health care is “local”
2.2. Transparency – accurate meaningful information on Transparency – accurate meaningful information on quality and cost – is key to provider improvement and quality and cost – is key to provider improvement and consumer engagementconsumer engagement
3.3. Collaboratives involving key stakeholder groups – public Collaboratives involving key stakeholder groups – public and private payers, providers, plans and consumers* – and private payers, providers, plans and consumers* – hold promise to foster requisite reformshold promise to foster requisite reforms
*and in some cases State data organizations, Quality Improvement *and in some cases State data organizations, Quality Improvement Organizations, and health information exchangesOrganizations, and health information exchanges
Improving Quality
The need for leadership has never been The need for leadership has never been greater. greater.
All public and private health care constituencies All public and private health care constituencies must commit to a shared agenda that can raise must commit to a shared agenda that can raise the quality of health care for all. the quality of health care for all.
-- 2001 IOM Report, -- 2001 IOM Report, Crossing the Quality ChasmCrossing the Quality Chasm