Embed Size (px)
Citation preview

Charles L. Bennett MD PhD MPP
Planes, cars, oil spills, and pharmaceuticals-- common lessons for
preventing major safety tragedies

Limited size of clinical trials
Undetected toxicities at time of FDA approval
Many AEs identified after several years on the market
Barriers to Identifying Adverse Events

Postmarket Pharmacovigilance
Hampton, T. Postmarket “Pharmacovigilance” Program on Alert for Adverse Events from Drugs. JAMA, August 22/292007, 298 (8): 851-2.

Pharmacovigilance Organizations
Academic Organizations FDA Pharmaceutical
Manufacturers
Data Case assessments;Prospective data MedWatch Proprietary databases
Science Pathology; histology None None
Timeliness 1-2 years post approval 3 years or more 7-12 years
Dissemination Manuscripts; presentations Package inserts Dear Doctor letters
Network Broad; international Mostly internal Mostly internal
Funding R01-based; CERTs Internal Not known

Detect ADR signals
Investigate possible ADR occurrence
Analyze data
Disseminate results
Lessons Learned: The RADAR method
Bennett CL, Nebeker JR, Lyons EA, et al. The Research on Adverse Drug Events and Reports (RADAR) Project. JAMA 2005, 293:17, 2131-40.

Major RADAR Publications
Drug ADR N Publication
Bisphosphonates Osteonecrosis of the JawReview of
case series
Lancet Oncology 2008
Epoetin/ darbepoetin VTE and MortalityMeta-
analysisJAMA 2008
Sirolimus/paclitaxel coated cardiac stents
Thrombotic events 139 JAMA 2007
G-CSF/ GM-CSFAcute myeloid leukemia and myelodisplastic syndrome
16J Natl Cancer Inst
2007
Epoetin/ darbepoetin Venous thromboembolismMeta-
analysisJ Natl Cancer Inst
2006
Sirolimus/paclitaxel coated cardiac stents
Hypersensitivity reactions 6J Am Coll Cardiol
2006
Thalidomide/ lenalidomide
Venous thromboembolismMeta-
analysisJAMA 2006
Epoetin Pure Red-Cell Aplasia 9 N Engl J Med 2004
Clopidogrel Thrombotic thrombocytopenic
purpura13 N Engl J Med 2000
TiclopidineThrombotic thrombocytopenic
purpura21 Lancet 1998

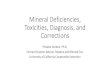
Mortality and Venous Thromboembolism Associated with Erythropoiesis
Stimulating Agents (ESAs)
Bennett CL, et al. Venous thromboembolism and mortality associated with recombinant erythropoietin and darbepoetin administration for the treatment of cancer-associated anemia. J Amer Med, 2008; 299(8):914-924.

Meta-analysis of mortality rates for 51 phase III oncology trials with 13,613 patients for ESAs versus placebo or control
HR= 1.10 (1.01, 1.20)
NOTE: Weights are from random effects analysis
Heterogeneity between groups: p = 0.133Overall (I-squared = 19.5%, p = 0.114)
Subtotal (I-squared = 0.0%, p = 0.536)
Cazzola_1995
Subtotal (I-squared = 21.1%, p = 0.108)
Chang_2007 (EPO-CAN-17)
N93-004_2004 (Grote)
P-174-2004
Dammacco_2001
Savonije_2004
Witzig_2005
Ten Bokkel_1998
Razzouk_2004
Vansteenkiste_2002
Henry_1995
EPO-CAN-15_2004
DAHANCA-10-2007
TRA
DA 232_2005 (Taylor)
DA 145_2007
Machtay_2004 (RTOG99-03)
EPO-GER22-2007
Thatcher b_1999
Ables_1993
Wright_2007 (EPO-CAN-20)
Hedenus_2003
Throuvalas_2000
Study ID
Coiff ier_2001
Gordon_2006
Mystakidou_2005
EPO-GBR-7_2004
Bamias_2003
WILKINSON_2006
Del Mastro_1997
Amgen 200010103_2007
INT-3_2004
Rose_1994
Osterborg_2005
BLOHMER_2007 (AGO/NOGG)
PREPARE-2007
Henke_2003
INT-1_2004
Oberhoff_1998
Case_1993
Osterborg_1996
Charu_2004
GOG-191_2007
MOEBUS_2007
Smith_2003
Vadhan-Raj_2004 (PR0003-006)
STRAUSS_2005
Kotasek_2003
Littlewood_2001
O'Shaughnessy_2005
Thatcher a_1999
Dunphy_1999
Leyland-Jones_2005 (INT-76)
AOC
1.10 (1.01, 1.20)
1.29 (1.00, 1.67)
0.37 (0.06, 2.27)
1.09 (0.99, 1.19)
0.88 (0.49, 1.59)
1.53 (0.65, 3.61)
0.41 (0.03, 5.76)
0.32 (0.11, 0.95)
0.98 (0.36, 2.67)
1.09 (0.83, 1.43)
1.01 (0.19, 5.31)
0.98 (0.14, 6.90)
0.78 (0.60, 1.01)
0.75 (0.28, 2.01)
2.70 (1.17, 6.23)
1.28 (0.97, 1.69)
0.85 (0.45, 1.60)
0.93 (0.82, 1.05)
1.41 (0.80, 2.49)
1.02 (0.60, 1.74)
1.26 (0.24, 6.60)
0.89 (0.41, 1.93)
1.84 (1.01, 3.35)
1.36 (0.98, 1.89)
0.13 (0.00, 332.66)
HR(mortality) (95% CI)
1.02 (0.38, 2.73)
0.67 (0.23, 2.00)
0.50 (0.05, 4.99)
1.07 (0.73, 1.57)
1.80 (0.53, 6.12)
4.54 (0.40, 51.20)
0.36 (0.05, 2.56)
1.43 (1.06, 1.92)
1.56 (0.42, 5.79)
1.68 (0.66, 4.29)
1.04 (0.80, 1.35)
0.67 (0.34, 1.33)
1.50 (0.96, 2.34)
1.39 (1.05, 1.84)
1.58 (0.32, 7.82)
0.61 (0.24, 1.55)
1.08 (0.44, 2.66)
1.02 (0.51, 2.04)
1.38 (0.44, 4.33)
1.25 (0.65, 2.41)
1.14 (0.77, 1.69)
3.96 (0.29, 54.12)
0.15 (0.00, 415.90)
1.16 (0.69, 1.95)
0.55 (0.11, 2.71)
0.81 (0.62, 1.06)
7.39 (0.15, 366.10)
0.49 (0.03, 8.71)
0.14 (0.00, 6.88)
1.37 (1.07, 1.75)
100.00
7.72
0.22
92.28
1.85
0.94
0.11
0.59
0.70
5.74
0.26
0.19
6.01
0.72
0.99
5.59
1.64
10.44
1.97
2.17
0.27
1.13
1.79
4.54
0.01
Weight
0.73
0.60
0.14
3.67
0.48
0.13
0.19
5.19
0.42
0.80
5.91
1.43
2.92
5.53
0.28
0.80
0.86
1.38
0.54
1.54
3.50
0.11
0.01
2.28
0.29
5.82
0.05
0.09
0.05
6.39
%
1.10 (1.01, 1.20)
1.29 (1.00, 1.67)
0.37 (0.06, 2.27)
1.09 (0.99, 1.19)
0.88 (0.49, 1.59)
1.53 (0.65, 3.61)
0.41 (0.03, 5.76)
0.32 (0.11, 0.95)
0.98 (0.36, 2.67)
1.09 (0.83, 1.43)
1.01 (0.19, 5.31)
0.98 (0.14, 6.90)
0.78 (0.60, 1.01)
0.75 (0.28, 2.01)
2.70 (1.17, 6.23)
1.28 (0.97, 1.69)
0.85 (0.45, 1.60)
0.93 (0.82, 1.05)
1.41 (0.80, 2.49)
1.02 (0.60, 1.74)
1.26 (0.24, 6.60)
0.89 (0.41, 1.93)
1.84 (1.01, 3.35)
1.36 (0.98, 1.89)
0.13 (0.00, 332.66)
HR(mortality) (95% CI)
1.02 (0.38, 2.73)
0.67 (0.23, 2.00)
0.50 (0.05, 4.99)
1.07 (0.73, 1.57)
1.80 (0.53, 6.12)
4.54 (0.40, 51.20)
0.36 (0.05, 2.56)
1.43 (1.06, 1.92)
1.56 (0.42, 5.79)
1.68 (0.66, 4.29)
1.04 (0.80, 1.35)
0.67 (0.34, 1.33)
1.50 (0.96, 2.34)
1.39 (1.05, 1.84)
1.58 (0.32, 7.82)
0.61 (0.24, 1.55)
1.08 (0.44, 2.66)
1.02 (0.51, 2.04)
1.38 (0.44, 4.33)
1.25 (0.65, 2.41)
1.14 (0.77, 1.69)
3.96 (0.29, 54.12)
0.15 (0.00, 415.90)
1.16 (0.69, 1.95)
0.55 (0.11, 2.71)
0.81 (0.62, 1.06)
7.39 (0.15, 366.10)
0.49 (0.03, 8.71)
0.14 (0.00, 6.88)
1.37 (1.07, 1.75)
100.00
7.72
0.22
92.28
1.85
0.94
0.11
0.59
0.70
5.74
0.26
0.19
6.01
0.72
0.99
5.59
1.64
10.44
1.97
2.17
0.27
1.13
1.79
4.54
0.01
Weight
0.73
0.60
0.14
3.67
0.48
0.13
0.19
5.19
0.42
0.80
5.91
1.43
2.92
5.53
0.28
0.80
0.86
1.38
0.54
1.54
3.50
0.11
0.01
2.28
0.29
5.82
0.05
0.09
0.05
6.39
%
ESA better Control better
15.1e-05 1 19684
MortalityMeta-analysis

Meta-analysis of mortality rates for 53 oncology trials with 14,164 patients for ESAs versus placebo or control (updated to include BRAVE study)
HR= 1.09 (95% CI, 1.01-1.18)
Updated MortalityMeta-analysis
NOTE: Weights are from random effects analysis
Heterogeneity between groups: p = 0.186
Overall (I-squared = 17.1%, p = 0.145)
Charu_2007
INT-1_2004
Leyland-Jones_2005 (INT-76)
Subtotal (I-squared = 20.4%, p = 0.111)
Study ID
O'Shaughnessy_2005
Henry_1995
PREPARE_2007
DAHANCA-10_2007
Thomas(GOG-191_2007)
EPO-GBR-7_2004
Rose_1994
Debus_2007 (EPO-GER22)
N93-004_2004 (Grote)
Glaspy_2007 (Amgen 200010103)
Vansteenkiste_2002
EPO-CAN-15_2004
Thatcher_1999b
Machtay_2004 (RTOG99-03)
Hedenus_2003
ten Bokkel Huinink_1998 (Reed_2005)
Strauss_2005
Gordon_2006
Vadhan-Raj_2004 (PR0003-006)
Littlewood_2001
DA 232_2005 (Taylor)
Kotasek_2003
INT-3_2004
Aapro_2008 (BRAVE)
Moebus_2007
Razzouk_2004
Osterborg_1996
TRA
Mystakidou_2005
Oberhoff_1998
Smith_2003
Chang_2007 (EPO-CAN-17)
Wright_2007 (EPO-CAN-20)
Ables_1993
Throuvalas_2000
Blohmer_2007 (AGO/NOGG)
DA 145_2007
Coiff ier_2001
Bamias_2003
P-174_2004
Henke_2003
Del Mastro_1997Dammacco_2001
Witzig_2005
Dunphy_1999
Subtotal (I-squared = 0.0%, p = 0.686)
AOC
Osterborg_2005
Case_1993
Cazzola_1995
Savonije_2005
Wilkinson_2006
Thatcher_1999a
Rosen_2003(phase II RCT)
1.09 (1.01, 1.18)
1.38 (0.44, 4.33)
1.58 (0.32, 7.82)
1.37 (1.07, 1.75)
1.09 (1.00, 1.18)
HR(mortality) (95% CI)
7.39 (0.15, 366.10)
0.75 (0.28, 2.01)
1.50 (0.96, 2.34)
1.28 (0.97, 1.69)
1.69 (0.76, 3.75)
0.98 (0.62, 1.56)
1.68 (0.66, 4.29)
1.02 (0.60, 1.74)
1.53 (0.65, 3.61)
1.22 (1.03, 1.45)
0.78 (0.60, 1.01)
2.70 (1.17, 6.23)
1.26 (0.24, 6.60)
1.41 (0.80, 2.49)
1.36 (0.98, 1.89)
1.06 (0.20, 5.53)
1.16 (0.69, 1.95)
0.67 (0.23, 2.00)
0.15 (0.00, 415.90)
0.81 (0.62, 1.06)
0.85 (0.45, 1.60)
0.55 (0.11, 2.71)
1.56 (0.42, 5.79)
1.07 (0.87, 1.32)
1.14 (0.77, 1.69)
0.98 (0.14, 6.90)
1.02 (0.51, 2.04)
0.51 (0.05, 4.99)
0.61 (0.24, 1.55)
3.96 (0.29, 54.12)
0.88 (0.49, 1.59)
1.84 (1.01, 3.35)
0.89 (0.41, 1.93)
0.13 (0.00, 332.66)
0.67 (0.34, 1.33)
0.93 (0.82, 1.05)
1.02 (0.38, 2.73)
1.80 (0.53, 6.12)
0.41 (0.03, 5.76)
1.39 (1.05, 1.84)
0.36 (0.05, 2.56)0.32 (0.11, 0.95)
1.09 (0.83, 1.43)
0.14 (0.00, 6.88)
1.19 (1.01, 1.40)
1.04 (0.80, 1.35)
1.08 (0.44, 2.66)
0.37 (0.06, 2.27)
1.15 (0.87, 1.53)
4.54 (0.40, 51.20)
0.49 (0.03, 8.71)
0.84 (0.45, 1.55)
100.00
0.42
0.22
5.65
89.82
Weight
0.04
0.56
2.38
4.85
0.84
2.22
0.62
1.73
0.73
8.23
5.27
0.77
0.20
1.56
3.84
0.20
1.83
0.46
0.01
5.08
1.29
0.22
0.32
6.69
2.88
0.15
1.08
0.11
0.62
0.08
1.47
1.42
0.88
%
0.01
1.12
10.32
0.56
0.37
0.08
4.79
0.150.45
5.00
0.04
10.18
5.16
0.66
0.17
4.71
0.10
0.07
1.35
1.09 (1.01, 1.18)
1.38 (0.44, 4.33)
1.58 (0.32, 7.82)
1.37 (1.07, 1.75)
1.09 (1.00, 1.18)
HR(mortality) (95% CI)
7.39 (0.15, 366.10)
0.75 (0.28, 2.01)
1.50 (0.96, 2.34)
1.28 (0.97, 1.69)
1.69 (0.76, 3.75)
0.98 (0.62, 1.56)
1.68 (0.66, 4.29)
1.02 (0.60, 1.74)
1.53 (0.65, 3.61)
1.22 (1.03, 1.45)
0.78 (0.60, 1.01)
2.70 (1.17, 6.23)
1.26 (0.24, 6.60)
1.41 (0.80, 2.49)
1.36 (0.98, 1.89)
1.06 (0.20, 5.53)
1.16 (0.69, 1.95)
0.67 (0.23, 2.00)
0.15 (0.00, 415.90)
0.81 (0.62, 1.06)
0.85 (0.45, 1.60)
0.55 (0.11, 2.71)
1.56 (0.42, 5.79)
1.07 (0.87, 1.32)
1.14 (0.77, 1.69)
0.98 (0.14, 6.90)
1.02 (0.51, 2.04)
0.51 (0.05, 4.99)
0.61 (0.24, 1.55)
3.96 (0.29, 54.12)
0.88 (0.49, 1.59)
1.84 (1.01, 3.35)
0.89 (0.41, 1.93)
0.13 (0.00, 332.66)
0.67 (0.34, 1.33)
0.93 (0.82, 1.05)
1.02 (0.38, 2.73)
1.80 (0.53, 6.12)
0.41 (0.03, 5.76)
1.39 (1.05, 1.84)
0.36 (0.05, 2.56)0.32 (0.11, 0.95)
1.09 (0.83, 1.43)
0.14 (0.00, 6.88)
1.19 (1.01, 1.40)
1.04 (0.80, 1.35)
1.08 (0.44, 2.66)
0.37 (0.06, 2.27)
1.15 (0.87, 1.53)
4.54 (0.40, 51.20)
0.49 (0.03, 8.71)
0.84 (0.45, 1.55)
100.00
0.42
0.22
5.65
89.82
Weight
0.04
0.56
2.38
4.85
0.84
2.22
0.62
1.73
0.73
8.23
5.27
0.77
0.20
1.56
3.84
0.20
1.83
0.46
0.01
5.08
1.29
0.22
0.32
6.69
2.88
0.15
1.08
0.11
0.62
0.08
1.47
1.42
0.88
%
0.01
1.12
10.32
0.56
0.37
0.08
4.79
0.150.45
5.00
0.04
10.18
5.16
0.66
0.17
4.71
0.10
0.07
1.35
ESA better Control better
15.1e-05 1 19684

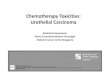
Meta-analysis of VTE rates in 38 phase III trials with 8,172 patients for ESAs versus placebo or control
HR= 1.57 (1.31,1.87)
VTEMeta-analysis
NOTE: Weights are from random effects analysis
Overall (I-squared = 0.0%, p = 0.901)
Ten Bokkel_1998a
Welch_1995
DA 145_2007
Smith_2003
Vadhan-Raj_2004 (PR0003-006)
EPO-CAN-15_2004
Bamias_2003
Henke_2003
Wright_2007 (EPO-CAN-20)
INT-3_2004
EPO-GBR-7_2004Machtay_2004 (RTOG99-03)
Wilkinson_2006
Cascinu_1994
Throuvalas_2000
Thatcher_1999a
Italian_1998GOG-191_2007
N93-004_2004 (Grote)
Charu_2007Rose_1994
Littlewood_2001
P-174_2004
Gordon_2006
Rosenzweig_2004
EPO-GER22_2007
Osterborg_1996a
Savonije_2004
Thatcher1999b
Study ID
Witzig_2005Leyland-Jones_2005 (INT-76)
Osterborg_2005
Osterborg_1996b
Abels_1993
Ten Bokkel_1998b
INT-1_2004
Razzouk_2004
Henry_1995
Dammacco_2001
Vansteenkiste_2002
Chang_2007 (EPO-CAN-17)
Case_1993
1.57 (1.31, 1.87)
1.96 (0.10, 38.79)
3.00 (0.13, 68.26)
1.53 (1.08, 2.18)
0.34 (0.02, 5.27)
3.74 (0.85, 16.56)
8.00 (1.93, 33.09)
0.33 (0.01, 8.05)
1.58 (0.59, 4.26)
0.75 (0.13, 4.20)
3.85 (0.49, 30.15)
4.93 (0.58, 41.73)4.93 (0.24, 100.89)
4.09 (0.54, 30.80)
. (., .)
2.79 (0.12, 65.66)
. (., .)
2.93 (0.12, 70.08)2.84 (0.81, 9.96)
0.97 (0.60, 1.59)
2.36 (0.13, 43.20)2.50 (0.55, 11.30)
1.38 (0.51, 3.75)
. (., .)
3.15 (0.17, 57.55)
8.40 (0.50, 142.27)
1.98 (0.97, 4.03)
2.71 (0.14, 54.32)
4.44 (0.57, 34.55)
2.56 (0.13, 51.05)
RR (95% CI)
1.47 (0.54, 4.05)1.47 (0.89, 2.40)
3.05 (0.13, 74.41)
1.53 (0.06, 36.23)
2.73 (0.11, 65.68)
3.56 (0.20, 62.58)
1.46 (0.15, 13.85)
2.95 (0.61, 14.28)
0.73 (0.27, 1.98)
5.51 (0.66, 45.98)
1.44 (0.47, 4.43)
1.36 (0.70, 2.62)
0.63 (0.11, 3.64)
100.00
0.35
0.32
25.84
0.42
1.42
1.56
0.31
3.21
1.06
0.74
0.690.35
%
0.77
0.00
0.32
0.00
0.312.00
13.16
0.371.38
3.16
0.00
0.37
0.39
6.23
0.35
0.75
0.35
Weight
3.0812.93
0.31
0.31
0.31
0.38
0.62
1.26
3.13
0.70
2.48
7.27
1.01
1.57 (1.31, 1.87)
1.96 (0.10, 38.79)
3.00 (0.13, 68.26)
1.53 (1.08, 2.18)
0.34 (0.02, 5.27)
3.74 (0.85, 16.56)
8.00 (1.93, 33.09)
0.33 (0.01, 8.05)
1.58 (0.59, 4.26)
0.75 (0.13, 4.20)
3.85 (0.49, 30.15)
4.93 (0.58, 41.73)4.93 (0.24, 100.89)
4.09 (0.54, 30.80)
. (., .)
2.79 (0.12, 65.66)
. (., .)
2.93 (0.12, 70.08)2.84 (0.81, 9.96)
0.97 (0.60, 1.59)
2.36 (0.13, 43.20)2.50 (0.55, 11.30)
1.38 (0.51, 3.75)
. (., .)
3.15 (0.17, 57.55)
8.40 (0.50, 142.27)
1.98 (0.97, 4.03)
2.71 (0.14, 54.32)
4.44 (0.57, 34.55)
2.56 (0.13, 51.05)
RR (95% CI)
1.47 (0.54, 4.05)1.47 (0.89, 2.40)
3.05 (0.13, 74.41)
1.53 (0.06, 36.23)
2.73 (0.11, 65.68)
3.56 (0.20, 62.58)
1.46 (0.15, 13.85)
2.95 (0.61, 14.28)
0.73 (0.27, 1.98)
5.51 (0.66, 45.98)
1.44 (0.47, 4.43)
1.36 (0.70, 2.62)
0.63 (0.11, 3.64)
100.00
0.35
0.32
25.84
0.42
1.42
1.56
0.31
3.21
1.06
0.74
0.690.35
%
0.77
0.00
0.32
0.00
0.312.00
13.16
0.371.38
3.16
0.00
0.37
0.39
6.23
0.35
0.75
0.35
Weight
3.0812.93
0.31
0.31
0.31
0.38
0.62
1.26
3.13
0.70
2.48
7.27
1.01
ESA better Control better
1.1 .2 .5 1 2 5 10 20 50

Summary of Mortality Hazard Ratios from Various Published Meta-analyses: Cancer Setting
Bohlius et al, J Clin Onc 2006
Wilson et al, Health Tech 2007
Seidenfeld et al, BCBS 2006
Bennett et al, JAMA 2008
Bohlius et al, Lancet 2009
No. of trials (No. of
patients)
42 (8,167) 28 (5,308) 35 (6,918) 51 (13,611) 53 (13,933)
HR for mortality (95% CI)
1.08 (0.99-1.18)
1.03 (0.92-1.16) 1.11 (0.99-1.23)
1.10 (1.01-1.20)
1.17 (1.06-1.30)

KDOQI 2007 guideline(non-dialysis patients)
KDOQI 2007 guideline (dialysis patients)
Phrommintikul 2007
RADAR report (unpublished)
No. of trials (No. of
patients)
8 (3,038) 4 (2,391) 9 (5,143) 3 (3,300)
HR for mortality (95%
CI)
1.01 (0.63,1.61) 1.12 (0.91,1.37) 1.17 (1.01, 1.35)
1.25 (1.07-1.45)
Summary of Mortality Rates from Various Meta-analyses: Chronic Kidney Disease Setting

Conflicts of Interest in Basic Science Studies:Evaluating Erythropoietin Effects
of Solid Tumor Cell Lines
Bennett CL, et al. Association between pharmaceutical support and basic science research on erythropoiesis-stimulating agents. Arch Intern Med, 2009; 170(16): 1490-1498.

• Senator Charles Grassley (R-IA) recently initiated conflict of interest probes against physicians at Harvard Medical School, Columbia University, and Emory University.
• Physician Payments Sunshine Act: requires transparency in relationships between physicians and pharmaceutical companies.
Prominent Conflict of Interest Cases

• Clinical studies have demonstrated that when investigators have financial relationships with pharmaceutical manufacturers, they are less likely to criticize the safety, efficacy, or cost-effectiveness of agents supplied by the manufacturers.
• No study has evaluated the effects of these financial relationships in the basic science setting.
Background

We investigated the relationship between manufacturer involvement and laboratory results in
studies of erythropoietin receptors (EpoRs) in cancer cells.
Study Objectives

• ESAs were approved in 1993 for use in the treatment of chemotherapy-associated anemia.
• Concerns were raised that the off-target effects might include stimulation of erythropoietin receptors (EpoRs) on cancer cells.
• Early adverse clinical evidence for ESA use: - BEST 2003 (breast cancer)
- ENHANCE 2003 (head and neck cancer)
Erythropoietin Stimulating Agents (ESAs)

• A MEDLINE database search was conducted (1988-June 2008).
• Studies investigating EpoR presence and ESA-induced signaling and/or changes in cellular function, in solid tumors, were evaluated.
• Conflicts of interest, laboratory results, funding sources, and affiliations were extracted.
Methods

• Academic studies without funding from ESA manufacturers; n=64
• Studies led by academic investigators who had received funding from ESA manufacturers; n=7
• Investigators employed by ESA manufacturers; n=3
Study Groups

Erythropoietin Receptors in Solid Tumors:Methods of Detection
Gene
Protein
Signal transduction
Function / Activity

Erythropoietin Receptors in Solid Tumors:Gene Level
• EpoR mRNA is detected in a wide variety of solid tumors.
• Studies have demonstrated an increase in EpoR mRNA levels upon stimulation with Epo.
Gene
Protein
Signal transduction
Function / Activity

Erythropoietin Receptors in Solid Tumors:Protein Level
• Cell surface expression of EpoR in solid tumors detected by immunohistochemistry, immunocytochemistry, immunoblot, etc.
Gene
Protein
Signal transduction
Function / Activity

Erythropoietin Receptors in Solid Tumors:Signaling
• EpoR stimulation by Epo induces the phosphorylation of signaling proteins involved in critical pathways regulating cell growth, apoptosis and angiogenesis.
• Signal transduction is detected in the PI3K-AKT, JAK-STAT and/or NF-kB pathways and varies among tumor types.
Gene
Protein
Signal transduction
Function / Activity

Erythropoietin Receptors in Solid Tumors:Cellular Function and Activity
• Activation of the Epo/EpoR-signaling axis by Epo administration results in changes in proliferation, apoptosis, invasion, and chemosensitivity.
Gene
Protein
Signal transduction
Function / Activity

0
20
40
60
80
100
Presence of the EpoR Erythropoietin-InducedSignaling Events
Erythropoietin-InducedChanges in Cellular
Function
Conclusion Identified
Per
cen
t o
f S
tud
ies
Iden
tify
ing
Co
ncl
usi
on
(%
) No COIAcademics with COIsInvestigators employed by ESA manufacturers
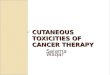
Comparison of Scientific Conclusions in Publications According to Funding Type
p= 0.009
p= 0.001
p= 0.007

0
10
20
30
40
50
60
70
Qualitative Conclusions “ESAsHarmful”
Qualitative Conclusions “ESAsBeneficial”
Conclusion Indentified
Per
cen
t o
f S
tud
ies
Iden
tify
ing
Co
ncl
usi
on
(%
) NO COIAcademics with COIsInvestigators employed by ESA manufacturers
Comparison of Scientific Conclusions in Publications According to Funding Type
p= 0.008
p< 0.04

Comparison of Scientific Conclusions in Presentations at Two National Meetings According to Funding Type
0
20
40
60
80
100
EpoR Presence Erythropoietin-Induced SignalingEvents
Erythropoietin-Induced Changes inCellular function
Conclusions Identified
Perc
ent
of P
rese
nter
s Id
enti
fyin
g Co
nclu
sion
s (%
)
No COI
Investigators employed by ESAmanufacturers
p<0.01 p<0.01 p<0.04

Association between pharmaceutical support and basic science research findings on ESAs: Comparison of findings before and after an NCI
workshop on this subject was convened

Background Prior study evaluated associations between pharmaceutical-
industry funding and preclinical research Study of erythropoiesis stimulating agents (ESAs) found
academic researchers without industry support were more likely than others to identify detrimental effects of ESAs on tumor cells
Concurrently, a meta-analysis identified mortality risks when cancer patients received ESAs
2007 - the National Cancer Institute convened a workshop reviewing research of preclinical effects of ESAs on tumor growth
We updated our analyses of associations between funding source and ESA research findings following the workshop

Articles identified in MEDLINE and EMBASE databases (2008-2012) investigating preclinical findings for ESAs in the cancer setting were reviewed.
Possible outcomes:◦ EPO receptor detection◦ Signaling events◦ Cellular function◦ Qualitative conclusions
Methods

Outcomes were reported for the current and the earlier time-period according to funding source◦ investigators without ESA manufacturer funding [27 and 64
studies, respectively]◦ investigators with funding from manufacturers or who held an
ESA patent [5 and 7 studies, respectively]◦ investigators employed by ESA manufacturers [2 and 3
studies, respectively]

EpoR(s), Epo Receptor(s), OR Erythropoietin Receptor(s)
Cancer, Tumor, Malignancy, OR Carcinoma+
280 Total Articles
251 Articles were excluded:• Hematologic
malignancies• Single case reports• Investigators employed
contrived systems• Investigation did not
involve cancer• Experiments involved
tumor types for which evidence of changes in signaling upon Epo administration was not investigated in the literature
• Article was a review
Performed all combinations and used the search with most results
Erythropoietin Receptor + Cancer
280 Total Articles29 Included Articles
For each of the tumor types identified in the above searches, additional searches were run with “tumor type” + “EpoR” variant:
EpoR(s)
Erythropoietin Receptor(s)
BreastLung
ProstateCervical
EndometrialOvarianGlioma
Head and NeckNeuroblastoma
RenalPancreaticMelanoma
MesotheliomaColorectal
ColonEwing’s Sarcoma Family of
Tumors
AND
Erythropoietin+
First OR Last Author (from prior study)
4 Include
d ArticlesThe first and last author of each
previous article were searched for more recent publications
33 Total Articles

0
20
40
60
80
100
120
Effect of Impact Factor (</> 4) on Studies
0-4.00
4.0+
Per
cen
t o
f S
tud
ies
Academic Investigators without conflicts of interest: 16/24 and 8/24, respectivelyInvestigative teams comprised of primarily academic investigators, one or more authors has a conflict of interest: 0/3 and 3/3, respectivelyInvestigative teams comprised primarily of ESA manufacturer employees: 1/2 and 1/2, respectively

Old Results

Pres
ence
of th
e Epo
R
Eryth
ropo
ietin
-Indu
ced S
igna
ling E
vent
s
Eryth
ropo
ietin
-Indu
ced C
hang
es in
Cell
ular
Func
tion
Qualit
ative
Con
clusio
ns *E
SAs H
armfu
l*
Qualit
ative
Con
clusio
ns *E
SAs B
enefi
cial*
Qualit
ative
Con
clusio
ns *E
SAs N
eutra
l/No S
tatem
ent*
0
20
40
60
80
100
120
Percent of New Studies Identifying Varying Conclusion
Academic Investigators without conflicts of interest
Investigative teams comprised primarily of academic investigators, one or more authors has a conflict of interest
Investigative teams comprised primarily of ESA manufacturer employees
Basic Science Results Qualitative Conclusions
Presence of the EpoR: 25/26, 5/5, and 2/2, respectivelyErythropoietin-induced signaling events: 19/22, 2/2, and 0/2, respectivelyErythropoietin-induced chances in cellular function: 19/22, 2/3, and 0/2, respectivelyQualitative conclusions that ESAs were harmful: 20/26, 2/5, and 0/2, respectivelyQualitative conclusions that ESAs were beneficial: 0/26, 0/5, and 0/2, respectivelyQualitative conclusions that ESAs were neutral/no statement: 6/26, 3/5, and 2/2 respectively

Total
Presence of the EpoR Erythropoietin-Induced Signaling Events
Erythropoietin-Induced Changes in Cellular Function
Qualitative Conclusions *ESAs Harmful*
Qualitative Conclusions *ESAs Beneficial*
0
20
40
60
80
100
120
Academic Investigators without conflicts of interest
Investigative teams comprised primarily of academic investigators, one or more authors has a conflict of interest
Investigative teams comprised primarily of ESA manufacturer employees
Conclusion Identified
Per
cent
of S
tudi
es I
dent
ifyi
ng C
oncl
usio
n (%
) Qualitative ConclusionsBasic Science Results
Presence of the EpoR: 82/83, 8/10, and 3/5, respectivelyErythropoietin-induced signaling events: 50/55, 2/4, and 0/3, respectivelyErythropoietin-induced chances in cellular function: 49/61, 2/9, and 0/3, respectivelyQualitative conclusions that ESAs were harmful: 44/91, 2/12, and 0/5, respectivelyQualitative conclusions that ESAs were beneficial: 6/91, 3/12, and 0/5, respectively

Academic researchers with or without financial conflicts increasingly report detrimental effects of ESAs.
Concerns over potential financial conflicts of interest affecting basic science research are less apparent in academic versus pharmaceutical-owned laboratories.
Conclusions

• Antibody specificity
• Choice of controls; proprietary versus non-proprietary carrier protein
• Differences in biological threshold for identifying changes in cellular function of erythropoietin-exposed cancer cells
Criticisms of Findings Suggesting Harmful Effects of ESAs

In these basic science studies, pharmaceuticalsponsorship is associated with a decreasedlikelihood of identifying:
Presence of EpoR on solid cancer cell lines
Unfavorable signaling events upon ESA administration
Unfavorable changes in cellular function upon ESA administration
Summary of Results

• These findings are counter to the belief that basic science studies are not subject to variable interpretation.
• The observed relationship may extend to other basic science research studies.
• Only further analyses can confirm or deny these preliminary findings, but the implications are significant and additional studies in this area are warranted.
Future Implications of COI Study

Rituximab-associated Progressive multifocal leukoencephalopathy (PML)
Carson KR, Bennett CL, et al. Progressive multifocal leukoencephalopathy after rituximab therapy in HIV-negative patients: a report of 57 cases from the Research on Adverse Drug Events and Reports project. Blood, 2009; 113(20). 4834-4840.

EtiologyJC polyomavirus infection>80% of cases seen in patients with HIVLatent JC virus in up to 80% of populationReactivation of JC virus not well understood
Non-HIV PMLHematologic malignancy
B-cell lymphoproliferative disorders Possible association with stem cell transplant and purine analog therapy
Chronic inflammatory diseases, solid organ transplant, sarcoidosis, advanced age
Progressive Multifocal Leukoencephalopathy (PML)

June 2004Warning about Hepatitis B reactivation added to package insert
February 2006Warning about other viral infections added to package insert
December 2006Letter to health professionals from manufacturer and FDA warning: PML seen
in two patients with lupusFebruary 2007
Black box warning added to package insert
Rituximab and viral reactivation(United States)

Cases were identified among rituximab-treated patients by clinicians from 12 cancer centers or academic hospitals (22 cases) or by reviewing FDA reports (11 cases), the manufacturer’s database (30 cases), and publications (18 cases; MeSH search terms: leukoencephalopathy, rituximab, immunosuppressed, lymphoma, and leukemia)
Unique data sources Clinical observation (n=7) Medical literature (n=14) FDA MEDWatch (n=14) Manufacturer (n= 23)
Inclusion criteria: Rituximab treatment AND Brain biopsy confirmation of PML OR Autopsy confirmation OR MRI evidence AND JC virus in CSF by PCR
Exclusion Diagnosis of HIV
Case Reports, Inclusion/Exclusion

Median Age (Years) 61 (range 30-89)
Sex (%) M: 48.3 F: 56.2
Median Doses Rituximab 6 (range 1-28)
Purine Analogue 26 patients
Stem Cell Transplant 6 (4 Auto, 2 Allo)
Findings
15 excluded for inadequate evidence of PML, 2 for diagnosis of HIV Patient Information (n=57)
Carson, Blood 2009

Additional Findings
Median time course (All patients, n=57)
1st rituximab to PML 16 months (range 1.0-90.0)
Last rituximab to PML 5.5 months (range 0.3-66.0)
PML diagnosis to death 2.0 months (0.4-122)
Previous and concomitant chemotherapy treatments
(range)
4 (1-14)
Carson, Blood 2009

Mental status changes or confusion 54.4% Focal motor weakness 33.3% Loss of coordination 24.6% Difficulty speaking 21.2% Vision changes 17.5%
Symptoms at diagnosis
Carson, Blood 2009

MRI Findings
Carson, Lancet Oncology 2009 (In press)

Inhibition of T-lymphocyte Trafficking by natalizumab and efalizumab
T- Lymphocyte
ICAM-1VCAM-1Selectins
Mucin
LFA-1
BLOOD FLOW
Selective adhesion molecule inhibitors
Node of RanvierMyelin internode
BRAIN TISSUE
Molecules not to scale.
Endothelial Basal lamina
VLA-4
Carson, Lancet Oncology 2009 (In press)

T-Lymphocyte count at PML diagnosis
Case No. Rituximab Indication Transplant CD4/CD8 CD4+ CD8+Purine analog exposure
1Diffuse large B-cell
lymphoma None N/A 68 N/A N
2Systemic lupus erythematosus None 1.25 71 57 N
3 Non-Hodgkin lymphoma Autologous 2.17 89 41 N
4Diffuse large B-cell
lymphoma None 0.39 94 243 N
5 Mantle cell lymphoma None 0.35 110 310 N
6 Follicular lymphoma None 0.29 152 532 N
7 Follicular lymphoma Autologous 0.23 234 1015 N
8Chronic lymphocytic
leukemia None 0.92 287 311 N
9 Mantle cell lymphoma Allogeneic 0.31 403 1309 N
10Marginal zone B-cell
lymphoma Autologous 0.21 551 2596 N
11Autoimmune hemolytic
anemia None 1.47 562 382 N
12 Follicular lymphoma None 0.30 570 1871 N
13Autoimmune hemolytic
anemia Allogenie 0.31 1059 3453 N
14Waldenstrom
macroglobulinemia None 0.34 2100 6200 Y
Carson, Blood 2009

Nine of ten with severe CD4 lymphopenia or low CD4/CD8 ratio
Abnormal CD4 counts or CD4/CD8 ratio possibly due to cytotoxic chemotherapy and not rituximab, based on clinical trial data
What about T-cell function after rituximab?
Summary of T-cell findings

Response in ITP associated with changes in T-cell compartment (Stasi et al, Blood 2007)
Modification of T-cell phenotype and cytokine profiles in patients with SLE and Evans’ syndrome (Tamimoto et al, Rheumatology Advanced Access 4/8/2008)
Rapid effect in multiple sclerosis suggests rituximab targets a process thought to be T-cell mediated (McFarland HF, NEJM 2/14/08)
Rituximab in autoimmune disorders

Through inhibition of T- and B-lymphocyte interactions, rituximab is contributing to viral reactivation and PML.
Criticism- Latent site of JC virus is in hematopoietic cells and likely B-lymphocytes. This may be how natalizumab causes PML
Hypothesis

5/5 bone marrow samples tested for JC in patients with PML, positive
2/86 bone marrow samples from MSD at NIH with no PML, positive
Odds-ratio not calculable
Epidemiology

Rituximab + chemotherapy increases risk of JC reactivation and PML◦ JC latent in CD34+ cells and early B-cells◦ Chemotherapy
mobilizes stem cells from bone marrowCauses quantitative T-cell depletion
◦ RituximabReduces qualitative T-cell responseB-cell depletion results in expansion of progenitor cells containing
latent JC
Revised Hypothesis

Retrospective Case-series Hypothesis is speculative and not verified in laboratory
model T-cell findings not yet shown to be significant in case-
control study
Limitations

Case-control study of T-cell markers after exposure to R-chemo and chemo without rituximab
Case-control study of marrow specimens from disease and treatment matched controls
Cohort study using large EMR or government database (VA, Kaiser, and/or Medicare)
Future Directions

Using methods of SONAR project, important hypotheses can be explored
Subsequent investigations allow clarification of issues raised by SONAR
Rituximab may be associated with multiple viral reactivation syndromes, screening and early detection could be helpful in prevention.
Conclusions

Ticlopidine- and clopidogrel-associated Thrombotic Thrombocytopenia Purpura (TTP)

Thrombotic Thrombocytopenic Purpura (TTP)
Clinical features• Microangiopathic hemolytic anemia• Thrombocytopenia• Microvascular thrombosis• Renal Failure• Neurological abnormalities
Epidemiology• Incidence may be rising
Increased awareness & diagnosis Increased exposure to TTP-associated agents
(ticlopidine, clopidogrel & prasugrel)

Among all clinically diagnosed TTP, 20% are drug-associated
Of all drug-associated TTP• Most frequent: ticlopidine • Next frequent: clopidogrel
• 1991: association of TTP with ticlopidine• 2000: association of TTP with clopidogrel
Drug-Associated Thrombotic Thrombocytopenic Purpura
Ticlopidine
Clopidogrel

Incidence & significance of thienopyridine-associated TTP
• Ticlopidine• Coronary artery stent: 1 in 1,500 to 1 in 5,000 patients• Cerebrovascular disease: 1 in 100,000 patients• 5 cases per year before development of stent procedures
• Stents: important contributing factor to occurrence of TTP Used by 100,000 in the U.S.
• Clopidogrel• 1 in 100,000 to 1 in 250,000 patients
Used by 6 million in the U.S.
Drug-Associated Thrombotic Thrombocytopenic Purpura

Ticlopidine-associated TTP in Coronary Stent Setting (Arch Intern Med, 1999)
Bennett CL, Davidson CD, et al. 1999. Thrombotic thrombocytopenic purpura associated with Ticlopidine in the setting of coronary artery stents and stroke prevention. Arch Intern Med 159: 2524-2528

Clopidogrel-Associated TTP (NEJM, 2000)
Bennett et al. 2000. Thrombotic Thrombocytopenia Purpura Associated with Clopidogrel. NEJM, 342 (24): 1773-77.
Of the 11 patients, 10 received clopidogrel <14 days before TTP onset.

Study Objectives ◦ To describe clinical and laboratory findings for a large cohort of patients
with thienopyridine-associated thrombotic thrombocytopenic purpura (TTP).
Methods◦ Clinical reports of TTP associated with clopidogrel and ticlopidine were
identified from medical records, published case reports, and FDA case reports (n=128).
◦ Duration of thienopyridine exposure, clinical and laboratory findings, and survival were recorded.
◦ ADAMTS13 activity and inhibitor were measured for a subset of individuals.
Thienopyridine-associated TTP
Bennett CL, Kim B, Zakarija A, et al. Two mechanistic pathways of thienopyridine-associated thrombotic thrombocytopenia purpura: Results from the SERF-TTP Research Group and the RADAR Project. J Am Coll Cardiol 2007; 50 (12): 1138-43.

279 articles identified in MEDLINE, EMBASE, the public website of the FDA and abstracts from national scientific conferences from 1991 to 2010 using terms: TTP, ticlopidine, clopidogrel, TTP
215 articles reviewed
138 articles on ticlopidine-associated TTP
67 articles on clopidogrel-associated TTP
Articles were excluded if they were in a language other than English and if there were duplicates (N=64)
29 articles reviewed
Articles were excluded if they did not include details on pharmacology, epidemiology, laboratory or basic science studies (N=176)

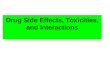
Latency difference of Thienopyridine-Associated TTP
days
Per
cent
age
of p
atie
nts
with
TTP
0 5 10 15 20 25 30 35 40 45 50
010
2030
4050
6070
8090
0
Time to Onset
ADAMTS13 Non deficient n=13
ADAMTS13 deficient n=26
▲Figure 1. LeftThienopyridine-Associated TTP Onset: ADAMTS13 Deficient versus ADAMTS13 Non-Deficient (p>0.05).
days
Per
cent
age
of p
atie
nts
with
TT
P
0 5 10 15 20 25 30 35 40 45 50
010
2030
4050
6070
8090
0
Time to Onset
Clopidogrel n=35
Ticlopidine n=93
▲Figure 1. RightThienopyridine-Associated TTP Onset: Ticlopidine versus Clopidogrel (p=0.0016).
Bennett CL, Kim B, Zakarija A, et al. Two mechanistic pathways of thienopyridine-associated thrombotic thrombocytopenia purpura: Results from the SERF-TTP Research Group and the RADAR Project. J Am Coll Cardiol 2007; 50 (12): 1138-43.
Time on Onset Differences in thienopyridine-associated TTP

Survival rates were associated with access to TPE and duration of thienopyridine exposure.
Survival with TPE Survival without TPE
All Patients (N=128)* 81.6 % 50.0 %
Ticlopidine (N=93) * 85.5 % 45.8 %
Ticlopidine Rx < 14 days (N=9) 100.0 % 100.0 %
Ticlopidine Rx > 14 days (N=84) 84.1 %* 38.1 %*
Clopidogrel (N=35) 72.4 % 66.7 %
Clopidogrel Rx < 14 days (N=26) 70.0 % 66.7 %
Clopidogrel Rx > 14 days (N=9) 77.8 %
Thienopyridine Rx < 14 days (N=35) 76.9 % 77.8 %
Thienopyridine Rx > 14 days (N=93) 83.3 %* 38.1 %*
Bennett CL, Kim B, Zakarija A, et al. Two mechanistic pathways of thienopyridine-associated thrombotic thrombocytopenia
purpura: Results from the SERF-TTP Research Group and the RADAR Project. J Am Coll Cardiol 2007; 50 (12): 1138-43.
Outcomes for Thienopyridine-Associated TTP Cases Based on Access to Therapeutic Plasma Exchange therapy (TPE).

Idiopathic vs. Thienopyridine Associated TTP
ADAMTS13 activity and clinical characteristics of idiopathic and thienopyridine-associated TTP cases
ADAMTS13 Activity (≤10%)
Normal ADAMTS13 Activity (>10%)
Idiopathic (n=30)
Thienopyridine (n=26)
Idiopathic (n=24)
Thienopyridine (n=14)
Age (years) 40** 67** 46** 62**
Sex (%female) 83%* 54%* 96%** 43%**
Platelet count (mean) 20,900** 9,269** 51,458 37,000
Platelet count <20,000/mm3
60%** 96%** 29% 36%
Creatinine (mean) 1.4** 2.2** 3.7 2.9
Creatinine >2.5 mg/dl 7% 19% 48% 36%
Neurologic Dysfunction 53% 69% 52% 43%
Total IgG autoantibodies to ADAMTS13 (prior to TPE)
100% N/A 65% (n=23)
N/A
*p<0.05; **p< 0.001 for comparisons between idiopathic and thienopyridine associated TTP in each ADAMTS13 cohort. Note: Total numbers of patients (n) are provided where information are not available for the entire cohort.

ADAMTS13 activity, neutralizing autoantibodies, and outcomes of idiopathic and thienopyridine-associated TTP cases
ADAMTS13 Activity (≤10%) Normal ADAMTS13 Activity (>10%)
Idiopathic (n=30)
Thienopyridine (n=26)
Idiopathic (n=24)
Thienopyridine (n=14)
Neutralizing autoantibodies to ADAMTS13 (prior to TPE) Ticlopidine Clopidogrel
79%*
100%* (n=23)
100% (n=2)
39%
N/A0% (n=6)
Neutralizing autoantibodies to ADAMTS 13 (measured at remission)
46% N/A 29% N/A
% cases ADAMTS13 level 11-50%
0% 0% 33% 79%
30-day survival 97% 85% 96% 57%
1-year relapse 33% 8% 13% 0%
*p<0.05; **p< 0.001 for comparisons between idiopathic and thienopyridine associated TTP in each ADAMTS13 cohort. Note: Total numbers of patients (n) are provided where information are not available for the entire cohort.
Idiopathic vs. Thienopyridine Associated TTP

Ticlopidine vs. ClopidogrelClinical characteristics of ticlopidine vs clopidogrel associated TTP
CasesTiclopidine (n=30) Clopidogrel no relapse (n=8)
Age (years) 68 58
Platelet count <20,000/mm3 90% 13%
Creatinine >2.5 mg/dl 20% 50%
Neurologic Dysfunction 60% 50%
Neutralizing autoantibodies to ADAMTS 13 (at presentation)
100% 0%
% cases ADAMTS13 ≤10% 80% 0%
% cases ADAMTS13 level 11-50% 20% 63%
Duration of Thienopyridine Use:
Percent < 2 weeks 0% 50%
Percent 2-12 weeks 100% 25%
Percent > 12 weeks 0% 25%
Percent received TPE 83% 100%
Survival after TPE 85% (n=26) 50% (n=8)
30-day survival 80% 50%
1-year relapse 0% 0%

Characteristics of Idiopathic TTP Cases by ADAMTS13 Activity and Presence of Neutralizing Antibody to ADAMTS13
ADAMTS13 Activity (≤10%) ADAMTS13 Activity (>10%)
Neutralizing Antibody at Presentation
Present (n=23)
Not Present (n=6)
Present (n=10) Not Present (n=14)
Age (years) 38 43 48 45
Sex (%female) 87% 67% 100.0% 92.3%
Platelet count (mean) 19,261 24,000 38,400 60,786
Platelet count <20,000/mm3 65% 50% 30.0% 28.6%
Creatinine (mean) 1.27 1.70 3.66 10.49
Creatinine >2.5 mg/dl 4% 20% 50.0% 42.9%
Neurologic Dysfunction 52% 67% 40.0% 61.5%
Neutralizing autoantibodies to ADAMTS 13 (measured at remission)
60%* (n=20) 0%* 50.0% 18.2%
% cases ADAMTS13 level 11-50%
0% 0% 50.0% 21.4%
30-day survival 95%(n=22) 100% 100.0% 92.9%
1-year relapse 57% 17% 25.0% 0.0%

Most ticlopidine-associated TTP cases”- occur after 2 weeks of drug exposure, - ADAMTS13 deficient, - 100% have ADAMTS13 autoantibodies at presentation but do not
relapse - immune-mediated involving neutralizing antibodies to ADAMTS-13.
Clopidogrel-associated TTP cases:- occur within days of drug exposure, - do not exhibit ADAMTS13 deficiency, - does not have ADAMTS13 autoantibodies at presentation but do not
relapse- less responsive to TPE- may be a direct result of endothelial damage,
Ticlopidine- vs. Clopidogrel-associated TTP
Bennett CL, Kim B, Zakarija A, et al. Two mechanistic pathways of thienopyridine-associated thrombotic thrombocytopenia purpura: Results from the SERF-TTP Research Group and the RADAR Project. J Am Coll Cardiol 2007; 50 (12): 1138-43.

Thrombotic Thrombocytopenic Purpura (TTP) Patients Associated
with Ticlopidine
Bennett CL, Georgantopoulos P, Matsumoto M, Rock G, Fujimura Y, et al. Thrombotic thrombocytopenic purpura (TTP) patients associated with ticlopidine: A review of 22 cases in Japan. (Under Review).

Matsumoto (n= 186)
Bennett (n=22) this paper
Bennett (n= 98)
Tsai (n=7) Steinhubl (n=19)
Country Japan Japan United States United States United States
% female 55.1% 45.50% 46.6% 70.0% 30.0%
Median Age (yrs)*
54 (8 mos-87)*
69 (41- 89)* 64.2 (11.1= SD)
57 (42-89) 62 (38-75)
Plt < 20k/mm3 100.0% 96.0% (23/24) 71.9% 100.0% 89.4%
Hgb < 9 g/dl 75.0% 72.7% 26.9% 42.3% 66.7%
Cr > 2.5 mg/dl*
75.8% 18.1% 30.1% NA 47.0%
Neurologic abnormality
79.0% 63.6% 73.1% 70.0% 73.7%
Median days ticlopidine (range)
Not applicable 27.5 (14 -36) 21 (7-112) 21 (14-56) 21 (14-28)
Characteristics of ticlopidine-associated TTP in Japan and the United States
*p<0.05 for comparison between acquired idiopathic TTP

Matsumoto (n= 186)
Bennett (n=22) this paper
Bennett (n= 98)
Tsai (n=7) Steinhubl (n=19)
Survival 84.3% 91.03% 84.9% 100.0% 78.9%
% Therapeutic plasma exchange (TPE)
Not available 63.6% 74.2% 100.0% 68.4%
Survival w/o TPE Not available 66.70% 42.1% Not available
33.3%
Survival w/ TPE* 83.9%* 100.0%* 81.7% 100.0% 100.0%
% w/ ADAMTS13:AC deficiency (<10%)
100.0% 100.0% 100.0% 83.3% Not available
% with ADAMTS13 inhibitors
97.8% 100.0% Not available
100.0% Not available
Characteristics of ticlopidine-associated TTP in Japan and the United States
*p<0.05 for comparison between acquired idiopathic TTP

Idiopathic TTP and thienopyridine-associated TTP represent distinct clinical syndromes.
Ticlopidine- and clopidogrel-associated TTP are also distinct clinical syndromes.
Measurement of ADAMTS13 activity as well as ADAMTS13 auto-antibodies provides important information that characterizes the two different mechanistic pathways for thienopyridine-associated TTP syndromes.
TTP: Conclusions

Gadolinium-Associated Nephrogenic Systemic Fibrosis
Bennett CL, Qureshi ZP, Sartor AO, Norris LB, Murday A, Xirasagar S, Thomsen HS. Gadolinium Induced Nephrogrenic Systemic Fibrosis, the Rise and Fall of an Iatrogenic Disease. Clinical Kidney Journal, 2012; 5: 82-88.

Overview:◦The first cases of nephrogenic systemic sclerosis were
initially identified by Cowper et al. in 1997 and published in 2000.
◦Fifteen patients on hemodialysis presented with thickening and hardening of the skin and scleromyxedema-like features.
◦This condition can be quite disabling because the skin tightening and musculo-tendinous involvement result in joint contractures that can reduce the range of motion of joints.
Nephrogenic Systemic Fibrosis: Introduction

Clinical Appearance of NSF

Clinical Appearance of NSF

Systemic Involvement in NSF

Clinical Subtypes of Nephrogenic Systemic Fibrosis: a proposed classification scheme
Subtype Description Percentage of previously reported patients (n=100)
NFD progression
1 New-onset acute renal failure or acute decompensation in CKD
25 May be transient
2 Pneumonia like disorder, followed by acute renal failure
6 Usually transient
3 Surgical procedure (often vascular) or acute blood loss, followed by acute renal failure
18 May be transient
4 Kidney transplant 34 May be transient
5 Chronic kidney disease, unknown trigger
3 Usually chronic
6 Thrombotic event, renal failure may prewdate or follow the event
12 May be transient
7 Brain tumor 1 Unknown

Number of Cases in FDA database of GBCA-associated NSF by Year (With Confirmed Event Date)
Num
ber
of C
ases
• Grobner’s report (2005)• First FDA report: summarizes Danish findings and
indicates that the FDA is investigating (2006)• FDA advisory warns of GBCA administration to
persons with CKD stage 4-5 (2007)• Black-box warnings issued (2008)
* Indicates a linear chelating agent
Key Events (US):

Results of Advisories
Swift but uncoordinated efforts led to identifying and disseminating information GBCA-associated NSF
Nearly a 70% drop in US cases from 1997 to 1998◦The US still accounts for the vast majority of NSF
cases worldwide
The absence of a centralized registry of NSF cases resulted in variable quality and quantity of case reports

Data Sources
The individual safety databases in this study will be derived from:◦FDA’s MedWatch: European Medicines Agency ;
Published case reports and case series◦International Registry maintained at the Yale
University School of Medicine◦Medical record reviews◦Safety reports collated by 23 product safety law firms◦Safety reports obtained from two of the manufacturers
of GCCAs

Methodology

Project Objectives regarding GBCA- associated NSF
Report on the long-term outcome of persons with NSF. We hope to adjudicate weather NSF is a class- or product-specific
toxicity (as we did with Epo-associeated PRCA)
Bennett CL, Luminari S, Nissenson AR, et al. Pure red-cell aplasia and epoetin therapy. N Engl J Med 2004; 351:1403-8.