Embed Size (px)
Citation preview

74
Objectives . The aim of this study was to determine the fre-quency and prognostic importance of ambulatory myocardialischemia and its association with cardiovascular risk factors inmen and women in the general population presenting for the firsttime with typical angina pectoris.
Background. Previous studies in selected "low" and "high"risk patients with stable coronary heart disease report a widerange in the frequency of ischemia (24% to 82%) and there is noagreement about whether ambulatory ischemia is of prognosticimportance for the generality of patients with stable angina .
Methods. Consecutive patients s70 years of age from a ran-domly selected population with no previous coronary heart diseasewere assessed prospectively, and 96 patients with typical anginaand 95 age-, gender- and practice-matched asymptomatic controlsubjects underwent 24-h ambulatory ST segment morltoring beforeantianginal therapy . All recordings were analyzed in blinded fash-ion. Follow-up evaluation of patients with angina to assess forrevascularization, myocardial infarction and death was undertakenat a mean of 15.8 months (range 7 to 30) after the initial evaluation .
Transient episodes of ischemic ST segment depression de-tected by continuous ambulatory electrocardiographic(ECG) monitoring have been extensively investigated, butthe true frequency and clinical importance of ambulatoryischemia in patients with stable coronary heart diseaseremain controversial . In selected hospital patients withpositive exercise tests and angiographic coronary arterydisease, some studies (1,2) reported the majority of patientswith angina to have ambulatory silent ischemia, but others(3) found this not to be the case . The proportion of patientswith stable angina in whom ambulatory ischemia is detectedranges from <25% (4,5) to >80% (1) . Gender differences inischemic activity have been poorly defined, and apart from
From the Department of Medicine, University of Southampton and theNational Heart and Lung Institute, University of London, London . UnitedKingdom. This work was supported in part by educational grants frontPreventive Cardiology Trust and the Jeffrey Fryer bequest . Bayer UK Ltdand Boehringer Ingelheim Ltd .
Manuscript received May 5, 1993 . revised manuscript received August 13,1993, accepted August 27, 1993 .
Address for correspondence ; Professor David A . Wood, National Heartand Lung Institute, Dovehouse Street, London SW3 6LY, United Kingdom .
©1994 by the American College of Cardiology
JACC Vol . 23 . No . IJanuary 1994 :74-81
Characteristics a Clinical Significance of Ambidatory MyocardialIschemia in Men and Women in the General Population PresentingWith Angina Pectoris
MANISH M. GANDHI, MRCP, DAVID A. WOOD, MSc, FRCP, FIONA C . LAMP E. MSc
Southampton and London, United Kingdom
Results . Transient episodes of ischemic ST segment depressionwere detected in 50 patients (52%) with angina and 9 controlsubjects (9%). In patients with angina, 159 episodes (71%) weresilent, median duration of ischemia was 66 min (range 1 to 782)and mean ± SID ST depression was 2.4 ± 1.1 mm. In logisticregression analysis, serum cholesterol (p < 0.05) and ischemia onexercise (p < 0.01) were independently associated with the pres-ence of ambulatory ischemia in men with angina, but only thelatter was significant in women ; this may reflect a differentpathophysinlogic basis for ambulatory ischemia in women. Duringfollow-up, there were 29 events. Kaplan-Meier survival analysisrevealed no significant difference in event-free survival betweenpatients with angina who did and did not have ischemic episodes(66% vs. 72%, p = NS).
Conclusions. This is the first study representative of newpatients with angina pectoris in the general population and showsthat ischemia during daily living activities is present in >50% ofthese patients but appears to be of no prognostic value .
(J Am Call Cardiol 1994;23:74-81)
smoking (6), the effect of cardiovascular risk factors isunclear .
There are conflicting reports about the prognostic impor-tance of ambulatory ischemia in patients with stable coro-nary heart disease. In selected patients with stable angina,ischemic episodes detected by ambulatory monitoring werepreviously reported (7-9) to be associated with a higher riskof subsequent fatal and nonfatal cardiac events, but morerecent studies (10,11) suggest that the reverse is true, with ahigher rate of myocardial infarction or cardiac death inpatients without than in those with ischemic changes onambulatory monitoring .
These differences in prevalence of ambulatory ischemiaand its prognostic significance may be due to careful patientselection, which results in arbitrary "low" and "high" riskstudy groups unrepresentative of the broad spectrum ofpatients with angina seen by most cardiologists-the "sick-est of the sick and the wellest of the well" (12) . A strikingfourfold difference in the annual rate of myocardial infarc-tion or death between two studies (8,10) that employeddifferent patient selection criteria supports this view. Resultsfrom studies that selected patients with long-standing angina(10), low work load exercise tests (7-9,13) and that included
0735-10971941$6.00

JACC Vol . 23, No . IJanuary 1994 :74-81
AMBULATORY ISCHEMIA AND ANGINA IN THE POPULATION
nonconsecutive referrals (8,10,13) cannot be extrapolated tothe generality of patients with angina pectoris . A physicianneeds to know the significance of ambulatory myocardialischemia in the type of patient with angina pectoris whopresents in clinical practice . if ischemia during daily activi-ties at the time of initial presentation and evaluation isfrequent, and if its presence can predict subsequent coro-nary events, then ambulatory monitoring would be valuablein risk stratification of new patients with angina .
The purpose of this study was therefore to prospectivelydetermine the frequency and prognostic significance of am-bulatory myocardial ischemia and its relation to cardiovas-cular risk factors in previously untreated patients presentingfor the first time with typical angina pectoris . Because theaim was to study a representative sample of patients withtypical angina drawn from the general population, the dem-onstration of positive findings on an exercise test or angio-graphic coronary artery disease was not a prerequisite . Theprevalence of ambulatory WOW is described in relation tothe frequency of ischemic ST segmcnt changes in age- andgender-matched asymptomatic persons drawn at randomfrom the same population .
Methods
Patients. A clinic for the evaluation of patients with chestpain was established in the noninvasive cardiology depart-ment of a teaching hospital (Royal South Hants) for thepurpose of this study . Seventeen of 64 family physicianpractices in the area of study (Southampton, United King-dorn), serving a registered population of 192,000, wererandomly selected and agreed to refer all new patients s70years age with suspected angina and no previous coronaryheart disease for evaluation. Patients whose chest pain wasconsistent with unstable angina or evolving myocardialinfarction that required hospital admission were not eligiblefor the study . From referrals between June 1990 and March1992, 110 consecutive patients presenting for the first timewith typical angina were eligible for the study . A diagnosis oftypical angina was made by a cardiologist when each of thefollowing criteria of an anatomically (14) and prognostically(15) validated definition were met : recurrent brief episodesof chest pain lasting up to 15 min precipitated by exertion orexertion and emotion, relieved by rest or nitroglycerin andwhose character and radiation were consistent with thediagnosis . No patient had a prior myocardial infarction or ahistory of any other manifestation of coronary heart diseaseor was taking long-acting antianginal medication . Patientswere excluded if they had baseline ECG abnormalitiesknown to influence the ST segment, such as left ventricularhypertrophy, bundle branch block or mitral valve prolapse,were on medical treatment likely to affect the ST segment orhad technically unsuitable ambulatory ECG recordings . Atotal of 96 patients who did not meet any of the exclusioncriteria underwent 24-h ambulatory ST segment monitoringbefore starting antianginal therapy . Six patients were taking
GANDHI ET AL
75
beta-adrenergic blocking agents for hypertension during themonitoring period .
Control subjects . For every eligible patient with typicalangina, one age-, gender- and practice-matched asymptom-atic subject was drawn at random from a computerizedrecord of the study population and invited to attend ascreening examination . Persons with a current or past his-tory of coronary heart disease or any of the exclusion criteriawere not studied. Thus, 95 of 110 eligible asymptomaticcontrol subjects underwent technically suitable 24-h ambu-latory ECG monitoring .
Permission for this study was granted by the hospital JointEthics Committee . Written informed consent was obtainedfrom all patients and healthy control subjects before enroll-ment .
Ambulatory eketracardlography . All patients and controlsubjects underwent continuous 24-h two-channel ambula-tory ST segment monitoring outside the hospital . Aftercareful skin preparation, pregelled electrodes were used torecord an anterior CM5 and an inferior bipolar lead onmagnetic tape with an amplitude-modulated dual-channelrecorder (Reynolds Tracker) that has a frequency responserange of 0.05 to 100 Hz in accordance with the AmericanHeart Association standards for evaluation of the ST seg-ment (16) . All recordings were calibrated with a 1-mV signalat the beginning of each tape . Baseline ECG recordings wereperformed for 30 s with the patient supine, in the right andleft lateral positions . standing and after hyperventilation toexclude postural ST segment changes . Patients and controlsubjects were asked to continue their usual daily activitiesduring the monitoring period . All patients were instructed topress an event marker on the recorder at the onset of anysymptoms and to maintain detailed angina diaries to recordthe time of each episode of pain, activity at the onset ofsymptoms and the use of sublingual nitrates . All tapes werevisually analyzed at 60-times normal speed with a ReynoldsPathfinder 111 system and areas of interest were printed outat 25 mm/s . The analysis was carried out without knowledgeof outcome, exercise test result and patient or controlsubject identity . An episode of significant ST segment de-piession was defined as >I -mm horizontal or downslopingST segment shift from baseline measured 0 .08 s after the Jpoint and persisting for ~ 1 min . An interval ? I min duringwhich the ST segment returned to baseline was required toseparate one episode from another . The total number andduration of episodes/24 h were recorded . For individualepisodes, the heart rate before onset, at onset and at peak STsegment change was recorded, as were the maximal degreeof ST segment change, duration of episode and associationwith any symptoms . Changes in the T wave vector alonewere not regarded as evidence of myocardial ischemia .
Exercise testing . All patients underwent maximal symp-tom-limited treadmill exercise testing according tc Bruceprotocol . Heart rate, blood pressure and 12-lead ECGs wererecorded before the start of the test, in the standing andsupine positions, after hyperventilation and at every 3 min

76
GANDHI E T AL.AMBULATORY )SCHEMIA AND ANGINA IN THE POPULATION
during exercise and recovery. Test end points dcal exhaustion, severe angina, dyspnea, ST segment de-pression >_4 nun, a decrease in blood pressure >20 mm Hg, 22%
complex ventricular arrhythmias, claudication or the patient'srequest. The maximal horizontal or downsloping ST segmentdepression at 0.08 s after the .1 point and the total exerciseduration were recorded .
Follow-up. Details of all deaths were obtained from theprimary care physicians . All patients were requested tocomplete a postal questionnaire up to 2 .5 years after entryinto the study. When questionnaires were not returned,details of clinical outcome were obtained by telephoneinterview or from the patient's physician . Information abouthospital attendance or admission was corroborated withhospital records to confirm the nature of any clinical eventand subsequent outcome. Events recorded were death fromany cause, myocardial infarction documented from a historyof chest pain associated with more than a twofold increase inserum cardiac enzymes and characteristic ECO changes orby the appearance of new pathologic Q waves, or perfor-mance of percutaneous transluntinat coronary angioplasty orcoronary artery bypass grafting. Results of ambulatory ECGmonitoring were not available to physicians caring for thepatients; therefore, decisions concerning revascularizationwere made independently .
Statistical analysis. Normally distributed data were sunl-marized by mean values and SD and skewed data by amedian and range, Comparisons among subgroups weremade using a chi-square test (without continuity correction)for categoric data and a i test for continuous data. TheMann-Whitney U test was used for comparison of nonnormally distributed data between subgroups . Logistic regres-sion analysis was used separately in men and women todetermine the independent association of clinical character-istics and exercise variables with ambulatory ischemic ac-tivity . A stepwise procedure was used to build the modelusing a cutoff of p = 0.05 to determine entry. Clinical variablesentered first in the analysis were frequency and duration ofsymptoms, age, gender, systolic and diastolic blood pressure,current cigarette smoking and serum cholesterol . Exercisevariables then added were presence of ischemia (ST segmentdepression ?I mm), peak rate-pressure product and totalexercise duration. Statistical significance was tested using thelikelihood ratio statistic . Survival curves were constructedusing the Kaplan-Meier technique to examine the cumulativeprobability of an adverse event (death, myocardial infarction,percutaneous transluminal coronary angioplasty or coronaryartery bypass grafting) in those with and without ambulatoryischemia and were compared by the log-rank method (17). Allanalyses were performed using Statistical Analysis System,version 6 (SAS Institute).
ResultsThe mean age ± SD of the 96 patients with typical angina
pectoris was 57.5 ± 9.9 years (range 34 to 70) ; 64 were male
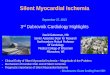
SID: silent only
48%
Figure 1 . Nature of ischemic ST segment depression (STD) in 96new patients presenting with angina pectoris from the generalpopulation .
JACC Vol. 23, No. IJanuary 1994 :74-81
and 32 female. Among the 95 asymptomatic healthy controlsubjects, the mean age was 56 .4 ± 9.6 years (range 35 to 71) ;59 were male and 36 female.
Ambulatory electrocardiographic monitoring n patientswith angina . Fifty (52%) of 96 patients with angina had oneor more episodes of significant ST segment depressionduring the 24-h monitoring period . The prevalence of ambu-latory ischemia was 53% in men, and 50% in women . Of atotal of 225 ischemic episodes recorded, 159 (71%) were notaccompanied by chest pain . There was no gender differencein the proportion of silent episodes (70% in men and 73% inwomen). Of the 159 silent episodes, 89 (56%) were detectedamong 13 patients (14%). Twenty-two percent of patientswith angina had silent episodes only, and 24% had both silentand painful episodes (Fig. 1) .
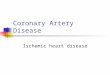
The distribution of the number of ischemic episodesrecorded in men and women was similar (Fig . 2). Amongpatients with ischemic ST segment depression, men had amedian of 3 episodes (range I to 15) and women a median of4.5 episodes (range I to 15) per 24-h period (p = NS). Inmen, the frequency of ambulatory ischemia increased withage. Only 31% (5 of 16) of men aged s50 years had transientischemic episodes compared with 60% (29 of 48) of men aged51 to 70 years (p < 0.05). There was no statistically signifi-cant difference between men and women in the duration(median 59 vs . 98 min) or extent (mean 2.4 vs. 2.5 mm) ofischemic ST segment change. In women, silent episodeslasted significantly longer than painful episodes (median 19vs. 11 min, p < 0.05), but in men, painful episodes tended tobe longer (median 14.5 vs. 10 min), (p = NS). However,there was a large variation among patients in the totalduration of ischemia (range I to 782 min [median 66])(Fig. 2) . The circadian distribution of ischemic episodes wassimilar in men and women, with a primary peak betweennoon and 6 PM (Fig. 3). Sixty-one percent of episodes in menand 70% in women were accompanied by an increase inheart rate at onset .

JACC Vol . 23 . No . IJanuary 1994 :74-81
0
0
1
2-5
6-10
11-15
Number of tsehent!c episodes per 24 hours
1-30
31-60
61-120 121-180 aver 180
Duration of ischenia (m9rnutes)
Figure 2. Number of ischemic episodes (top) and duration of isch-emia (bottom) recorded by 24-h ambulatory electrocardiographicmonitoring in men and women in the general population presentingwith angina pectoris .
Ischemic ST segment depression in asymptematic control
subjects . Among the 95 age-, gender- and practice-matchedhealthy asymptotnatic control subjects who underwent 24-hambulatory monitoring, significant ischemic ST segment
Figure 3. Circadian distribution of 225 ischemic episodes in men andwomen with angina .
30-
25-figfig
male
temale
./i
0-3
3-6
6-9 9-12 12-15 15-18 18-21 21-24
Time of day (hours)
GANDHI ET AL .
77AMBULATORY ISCHEMIA AND ANGINA IN THE POPULATION
Table 7 . Baseline Clinical Characteristics of Angina Patients Withand Without Ambulatory Ischcmia
*p = 0 .05 . tp < 0 .001 . Values presented are mean value ± SD or percentof p atients . S T I = ST segment depression .
depression was detected in 7 (12%) of 59 men and 2 (6%) of36 women. The mean age of the nine subjects with ischemicchanges was 64 .3 ± 4 .6 years . A total of 21 episodes weredetected during 2 .453 h of monitoring, and their circadiandistribution was similar to that of patients with angina, withan afternoon peak between noon and 6 PM when 52% of theepisodes were recorded . The median duration of episodeswas 26 min (range 4 to 193), and the mean extent of STsegment depression was 2 .5 ± 0.9 mm .
tschLmic activity, cardiac risk factors and symptoms .Table I shows the baseline clinical and exercise test charac-teristics of patients with angina with and without ambulatoryischemia . There wore no significant differences between thetwo groups in frequency and duration of angina, gender ormajor cardiovascular risk factors . Patients with isehemia onambulatory monitoring tended to be older and had a higherprevalence of exercise-induced ST segment depression, buttotal exercise duration and the peak rate-pressure productdid not differ significantly between the two groups .
When the two groups were compared separately bygender, significantly higher values for age, serum cholesteroland prevalence of exercise-induced ST segment depression
Table 2 . Association of Ambulatory Ischemia and ClinicalCharacteristics in Men by Univariate and Multivariate Analyses
CI = confidence interval ; ST I = ST segment depression .
ST I(n = 50)
No ST I.(n = 46)
Mean age lyr) 59 .4 ± 9 .2 55 .5 - IQ3*Male (r) h8 65Cigarette smoker (%) 28 37Hypertension (%n) 52 48Serum cholesterol (mgidl) 290 t 54 275 t i0Diabetes {%) 8 9Symptoms
Frequency a once daily (%) 36 33Duration <1 month (c) 44 46
ExerciseSa y - i mm 87 38tDuration (min) 6 .3 ± 2 .5 7.1 t 2 .8}tale-pressure product (x10 3 ) 27 .7 ± 5 .8 29 ± 5 .8
UnivariateST J
to = 34)No ST I
pIn = 30)
Value
Mean age (yr) 60.3 54.4 0 .02Serum cholesterol (mgldl) 294 255 0 .004Exercise ST I al mm 1%c) 84 38
< 0.001
Multivariate Relative Risk (95%r Cl) p Value
Serum cholesterol 1 .9 (1 .0-3 .4) 0.02
Exercise ST I aI mm 6 .6 (1 .8-24_ I) 0.003

78
1
0 .9
syc0 0 .6Oa 0...- 0 .4
4E 0 .2U 0.1
0.8
0 .7
0
GANDHI ET AL .AMBULATORY ISCHEMIA AND ANGINA IN THE POPULATION
January 1994 : 7 4 -81
Follow-up ldays)
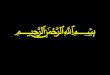
Figure 4 . Kaplan-Meier survival curves comparing cumulative pro-portion of patients with angina surviving without cardiac events(death, nonfatal myocardial infarction, percutaneous transluminalcoronary angioplasty or coronary artery bypass grafting) during amean follow-up period of 15 .8 months for 50 patients with ischemia(triangles, solid line) and 46 patients without ischemia (circles,dashed line) as detected by ambulatory electrocardiographic moni-toring . STD = ST segment depression.
were found in men with ambulatory ischemia (Table 2), butonly the latter was significantly higher in women . A stepwisemultiple logistic regression analysis adjusting for age con-firmed the independent association of serum cholesterollevel and exercise-induced ischemia with ambulatory isch-emic activity in men (Table 2) .
Clinical outcome. Follow-up was complete for 93 (97%)of 96 patients with angina . The remaining three patients hadmoved without leaving a forwarding address. During a meanfollow-up period of 15 .8 months (range 7 to 30), there werethree deaths, eight myocardial infarctions, seven coronaryartery bypass graft operations and I I coronary angioplastyprocedures . Seventeen patients (34%) with ambulatory isch-emia experienced adverse events compared with 12 patients(26%) with no ischemia . Kaplan-Meier actuarial analysis ofcumulative survival (Fig. 4) revealed no significant differ-ence in event-free survival between patients with and with-out ischemia (66% vs . 72%, p = NS1 . Slightly more patientswith ambulatory ischemia experienced the combined endpoints of death or myocardial infarction compared withpatients with no ischemia (14% vs . 9%, p = NS) .
Survival was also compared in relation to duration ofischemia. Eight (31%) of 26 patients with >60 min ofischemia during 24-h ambulatory monitoring experiencedevents compared with 21 (31%) of 67 patients with <60 minof ischemia or no ischemia. The overall event-free survivalin both groups was identical (69%) .
DiscussionThis prospective study is the first to investigate the
frequency and prognostic importance of ambulatory myocar-
JACC Vol. 23, No. I
dial ischernia in a representative sample of patients in thegeneral population presenting for the first time with stableangina. Patient selection is critical to all scientific clinicalinvestigations because it determines the generalizability ofresults . Previous studies have included a variable number ofpatients with prior myocardial infarction (7 .9-11,13) orrevascularization (7,10,13), are based on predominantlymale patients (8,9) with a low work load positive exercisetest (7-9,13) or angiographically proven coronary arterydisease (8,11) and have all recruited patients referred to aspecialist center. With an increasing number of selectioncriteria, the spectrum of patients included becomes narrowerand the term "consecutive patients" has no meaning whenthe population from which they are drawn is not known . Toavoid these sources of bias, the present study was designedto investigate the frequency and prognosis of ambulatoryischemia in a representative sample of new patients withangina from the general population typical of those whopresent in clinical practice . None of the patients hadpreviously diagnosed coronary heart disease, and entrywas not limited to patients with exercise-induced ischemia atlow work loads or proved angiographic coronary arterystenoses .
Prevalence and characteristics . ischemia during daily liv-ing activities was detected in about half of all patients in thisgeneral population sample in whom angina pectoris was thefirst manifestation of coronary heart disease . There was nodifference in the extent or duration of ischemia between menand women. The prevalence of ambulatory ischemia inwomen in the present study was 50% compared with only22% in a recently reported (5) cohort of 121 women withcoronary artery disease who underwent 48 h of ambulatorymonitoring. The lower prevalence in that study may havebeen due to the inclusion of only selected women with mildor no symptoms, some of whom may have had a previousmyocardial infarction (18), whereas the present study wasrepresentative of all women in the general population c70years of age presenting with angina pectoris . Compared withasymptomatic control subjects, womcn with angina had asignificantly higher prevalence of ischemic ST segment de-pression during daily living ; therefore, the ambulatory mon-itor findings cannot be regarded as false positive pathophys-iologic changes even if the prevalence of significant coronaryartery stenoses may be lower than that in men with ischemia(19). The mechanism responsible for ST segment depressionin women with angina may be different from that in men (20) .
Ambulatory ST segment depression was detected in 9%of apparently healthy subjects. This ending may reflectunderlying asymptomatic coronary artery disease becauseall subjects were >55 years of age and at a higher risk forfuture cardiac events (21,22) . The reported frequency ofischemic ST segment changes in selected healthy personsranges from 2% in hospital workers (23) to 30% in volunteerpolicemen (24) . In the only other study of population-basedhealthy subjects (25), the reported prevalence of 12% wassimilar to that in the present study .

JACC Vol . 23 . No . I GANDHI ET AL
19January 1994 :74-81
AMBULATORY ISCHEMIIA AND ANGINA IN THE POPULATION
Among new patients with angina pectoris, there werelarge differences in the number of transient ischemic epi-sodes and the duration of ischemia recorded over a 24-hperiod. This inherent variability of ambulatory ischemia,which has been quantified in patients with chronic stableangina (26), emphasizes the need for caution when interpret-ing data regarding therapeutic antfischemic effects, particu-larly if criteria to take account of this variability are not used(27) .
A circadian variation in the frequency of transient isch-emic episodes was evident in both men and women . Aprimary peak in the afternoon rather than in the morninghours in the current study is similar to observations inpatients taking beta-blockers (29), but is at variance withfindings in monitored patients receiving no treatment, inwhom the primary peak of ischen - ic episodes appeared to bein the morning hours (29) . Although these differences couldarise from the intrinsic variability of ambulatory ischemia,they might also be due to the influence of environmentalfactors that can modify the circadian pattern of heart ratechange (30) . Thus, patients with established chronic stableangina may modify their daily activity pattern to avoid peaksin daytime stress, whereas the early afternoon peak in newpatients in the present study probably reflects continuingoccupational stress . The latter explanation is supported by asimilar primary afternoon peak in the number of episodes ofST segment depression in the asymptomati,, control group .In any case, the significance of the peaks in ambulatoryischemic activity in relation to coronary events remainsspeculative because neither a direct causal relation nor amodification of outcome by medical intervention has beendemonstrated .
The present study investigated the relation between themajor cardiovascular risk factors and ischemic activity dur-ing daily living in patients with angina . In men, an elevatedserum cholesterol level was positively associated with thepresence of ambulatory ischemic activity independent of ageand baseline clinical characteristics . A similar relation wasnot evident in women . Although the incidence of coronaryheart disease and prevalence of angiographic coronary ar-tery stenoses are both positively associated with total cho-lesterol in women <50 years of age, this relation has notbeen demonstrated in older women (31,32) and there is noassociation between serum cholesterol and risk of suddendeath (33). In contrast, the independent association of raisedcholesterol levels with ischemic activity in men might under-lie an important pathophysiologic basis because cholesterollevel is independently associated in men of all ages <70years with both the short- and long-term increased risk ofsudden unexpected death (33) .
Ambulatory ischemla and prognosis. In this study ofpatients presenting for the first time with angina pectoris inthe general population, there was no statistically significantdifference in event-free survival between those with andwithout ambulatory ischemia . Ambulatory ischemia re-mained prognostically unimportant even after women were
excluded from the analysis . The findings of previous reportsare contradictory . Ambulatory ischarria predicts adversecoronary events in some selected patients with stable coro-nary disease (7-9,13), but not in others (10,11) . Deedwaniaand Carabajal (9) showed an independent association ofsilent ischemia with cardiac mortality in patients receivingmedical treatment for angina, but unlike the current study ofentirely new patients, the duration of symptoms in theirstudy population of men with low work load positive exer-cise tests ranged from 2 to 42 years . By contrast, ambulatoryischemia was found to be of no prognostic significance in 172patients with stable angina selected nonconsecutively fromtwo centers (10) . In that study, the combined event rate formyocardial infarction and death was in fact twofold higher inpatients with no detectable ischemia on ambulatory moni-toring compared with those with ischemia . A similar trendtoward an increased event rate in patients without ischemiawas also found in a recent study by Quyyumi et al . (11) inasymptomatic or mildly symptomatic patients with coronaryartery disease . They used multiple criteria based on coro-nary angiography and exercise testing to select 116 low riskpatients, but because selection was based on coronaryanatomy determined a mean of 2 years before enrollment,they could not include patients who had experienced anadverse event in the interim period nor allow for any changein coronary anatomy during the 2 years after initial angiog-raphy. Furthermore, their method (11) of defining low riskusing coronary anatomy and radionuclide ventriculographymay not be entirely appropriate because in five of sixpatients . the most significant lesion at baseline angiographywas not in the vessel that was totally occluded at the time ofa subsequent acute clinical event, and the infarcted region infour of five patients did not show ischemic dysfunction at thetime of baseline radionuclide ventriculography .
When patient selection is based on positive exercise testsat low work loads, the prognostic importance of ambulatorymonitoring may be exaggerated because exercise-inducedischemia at low work loads not only predicts the presence ofambulatory ischemia (34), but also is independently associ-ated with an adverse outcome (35) . In such studies, patientswith a high probability of having ischemia recorded on ambu-latory monitoring are therefore also the ones most likely toexperience a cardiac event . It is not surprising that in studiesthat based patient selection on a positive exercise test, ambu-latory ischemia appeared to have prognostic value (7-9), but inthose that did not (10, 11), including the current study, ambu-latory ischemia did not discriminate between patients with anadverse outcome . Exercise-induced ischemia probably resultspredominantly from increased demand across fixed, narrowlumen, flow-limiting stenoses associated with severe coronaryatheroma, whereas ischernic episodes during ambulatory mon-itoring may also occur at rest and at lower levels of exercisebecause of vasoconstriction and a reduction in coronary flowreserve associated with milder coronary artery disease (36) .Thus, ischemia in patients with a low work load exercise testthat is mainly "demand" related may be prognostically impor-

gQ
GANDHI ET AL .AMBULATORY ISCHEMIA AND ANGINA IN THE POPULATION
taut, but ambulatory ischemic ST segment depression that also
References
occurs at rest because of altered vasomotor tone and vasocon-striction may have less prognostic importance .
Study limitations . In common with previous studies (7--11,13) assessing the prognostic importance of ambulatoryischemia in which the number of patients with stable anginaenrolled ranged from 56 (8) to 172 (10), the number ofpatients in our study was small; therefore all studies lackadequate statistical power . The 95% confidence interval forthe observed difference in event rates of 6% between pa-tients with and without ambulatory ischemia in this study is-l3% to +25% . A much larger study would be required todetect with confidence a clinically important difference of,say, 15% . A longer duration of follow-up may also reveal astatistically significant difference in survival, but the prog-nostic value of ambulatory monitoring in predicting theobjective end points of myocardial infarction and deathdiminishes over time (13) ; therefore, it is likely that anydifference in survival between patients with and withoutischemia would also diminish with time .
As discussed earlier, the use of an exercise test to selectpatients for coronary angiography could have increased thechances of an association between ambulatory ischemia andrevascularization procedures . This would have resulted in ahigher event rate in patients with ambulatory ischemia .Therefore, this bias, if anything, strengthens the conclusionof this study in relation to the lack of prognostic importanceof ambulatory ischemia .
To evaluate t.Ne importance of ambulatory ischemia innew patients with typical angina representative of those seenin clinical practice, cardiac catheterization was not requiredfor entry to the study and therefore some patients might nothave had significant coronary artery stenosis . However,comparisons with asymptomatic control subjects, especiallyin women, put the reported prevalence of ischemia inpatients with angina into perspective .
Clinical implications . This study shows that transientischemic episodes occur on ambulatory ECG monitoring in>50°Jo of patients from a representative sample of the generalpopulation presenting for the first time with typical angina.The pathophysiology of ambulatory ischemic changes maybe different in men and women, and for men ischemicactivity during daily living was independently and positivelyassociated with serum cholesterol . In new unselected pa-tients with typical angina, ambulatory ST segment monitor-ing did not identify a subgroup at increased risk of death,myocardial infarction or future revaseularization . Therefore,its routine use in clinical practice for risk stratification in thegenerality of patients presenting for the first time with anginapectoris is not recommended .
Invaluable support for this study from the following in Southampton isgratefully acknowledged: all staff or Noninvasive Cardiology, Royal SouthHants Hospital, the 117 participating family physicians, and Avis Scamle-bury, who prepared the manuscript,
2 .
3 .
4 .
5 .
6.
7 .
8 .
9 .
10 .
11 .
12 .13.
14.
15.
16.
17.
18.
19 .
20.
21 .
22.
23.
JACC Voi . 23, No . 1January 1994 :74-81
I . Cecchi A, Dovellini E, Marchi F . Pucchi P. Santaro G . Fazzint P . Silentmyocardial ischemia during ambulatory electrocardiographic monitoringin patients with effort angina. J Am Coll Cardiol 1983 :1 :934-9 .Shea MJ, Deanfield J, Wilson R, De Landsheere C. Jones T . Selwyn A.Transient ischemia in angina pectoris : frequent silent events with every-day activities . Am J Cardiol 1985 :56:34E-8E .Mulcahy D, Keegan P, Crean P, et al . Silent myocardial ischemia inchronic stable angina : a study of its frequency and characteristics in 150patients . Br Heart J 1988 ;60:417-23 .Von Arnim T, Hofiing B, Schreiber M . Characteristics of episodes of STelevation or ST depression during ambulatory monitoring in patientssubsequently undergoing coronary angiograph ; . Br Heart J 1985 ;54:484-8 .Thadani U, Hill J, Cohn P, et al . Prevalence and frequency distribution ofambulant silent ischemia in asymptomatic and minimally symptomaticwomen with CAD labstracil . Circulation 1992 ;86 Suppl 1 :1-115 .Barry J . Mead K, Nobel E, et al . Effect of smoking on the activity ofischemic heart disease. JAMA 1989 ;261 :398-402 .Rocco M. Nobel E, Campbell S, et al . Prognostic importance of myacar-diai ischemia detected by ambulatory monitoring in patients with stablecoronary artery disease . Circulation 1988 ;78:877-84 .Tzivani D, Weisz G, Gavish A, Zin D, Keren A, Stern S . Comparison ofmortality and myocardial infarction rates in stable angina pectoris withand without ischemic episodes during daily activities . Am J Cardiol1989 ;63 :273-6.Deedwania P, Carabajal E . Silent ischemia during daily life as anindependent predictor of mortality in stable angina . Circulation 1990 ;81 :743-56.Mulcahy D, Parameshwar J, Holdright D, et al . Value of ambulatory STsegment monitoring in patients with chronic stable angina : Does measure-ment of the "total ischemic burden" assist with management? Br Heart J1992 ;67 :47-52.Quyyumi A, Panza J, Diodati J, Callahan T, Bonow R . Epstein S .Prognostic implications of myocardial ischemia during daily life in lowrisk patients with coronary artery disease . J Am Coll Cardiol 1993 ;21 :loo-B.Diamond G. Monkey business leditoriall . Am J Cardiol 1986:57 :471-5.Yeung A, Barry J, Orav J, Bonassin E. Ruby K, Selwyn A . Effects ofasymptomatic ischemia on long-term prognosis in chronic stable coronarydisease . Circulation 1991 ;83 :1598-604.Weiner D, Ryan T, McCabe C, et al . Correlations among history ofangina, ST segment response and prevalence of coronary artery disease inthe Coronary Artery Surgery Study (CASS) . N Engl J Med 1979 ;301 ;230-5.Murabito J, Anderson K, Kannel W, Evans J, Levy D . Risk of coronaryheart disease in subjects with chest discomfort : the Framingham HeartStudy . Am J Med 1990 ;89:297-302 .Pipberger HV, Arzbaecher RC, Berson AS, et al . Recommendations forstandardization of leads and of specifications for instruments in electro-cardiogtaphy and vectorcardiography: report or the Committee on Elec-trocardiogmphy, American Heart Association . Circulation 1975 ;52 :11-31 .Armitage P, Berry G. Statistical Methods in Medical Research . 2nd ed .Oxford: Blackwell Scientific, 1987:428 .Pepine C, Cohn P, Deedwania P, et al . The prognostic and economicimplications of a strategy to detect and treat asymptomatic ischemia : theAtenolol Silent [schema Trial (ASIST) protocol . Clin Cardiol 1911 ;14 :457-62 .Welch C, Proudfit W, Sheldon W . Coronary arteriographic findings in1,000 women under age 50. Am J Cardiol 1975 ;35 :211-5 .Maseri A, Crea F, Kaski J, Crake T . Mechanisms of angina pectoris insyndrome X. J Am Coll Cardiol 1991 ;17 :499-506 .Hedblad B, Juul-Moller S, Svensson K, et al . Increased mortality in menwith ST segment depression during 24h ambulatory long-term ECGrecording . Eur Heart J 1989 ;10 :149-58 .Flog J, Kennedy H . Long-term prognostic significance of ambulatoryelectrocardiographic findings in apparently healthy subjects >60 years ofage . Am J Cardiol 1992 ;70:748-51 .Deanfield 1, Ribiero P, Oakley K, Krikler S, Selwyn A . Analysis of STsegment changes in normal subjects : implications for ambulatory moni-toring in angina pectoris . Am J Cardiol 1984 ;54 :1321-5 .

JACC Vol . 23 . No . IJanuary 1994:74-81
24. Armstrong W. Jordan J, Morris S. McHenry P . Prevalence and magnitudeof ST segment and T wave abnormalities in normal men during continuousambulatory electrocardiography . Am J Cardiol 1982 :49 :1638-42 .
25. Kohli R, Cashman P . Lahiri A . Raftery E . The ST segment of theambulatory electrocardiogram in a normal population . Br Heart J 1988 :60:4-16 .
26 . Nabel E, Barry J . Rocco M, et al . Variability of transient myocardialischemia in ambulatory patients with coronary artery disease . Circulation1987 ;78 :60-7 .
27 . Redl A . Rudolf W . Spontaneous variability of ischemic episodes duringeveryday activities : role of ST Holler monitoring in assessment oftreatment . Herz 1990 ;15 :253-8 .
28. IJeedwania P, Carhajal E. Prevalence and patterns of silent myocardialischemia during daily life in stable angina patients receiving: conventionalantianginal therapy . Am J Cardiol 1990 ;85 :1090-6.
29. Hausman D, Nikutta P . Trappe J-J, Daniel W, Wenzlaff P . Lichtlen P.Circadian distribution of the characteristics of ischemic episodes inpatients with stable coronary artery disease . Am I Cardiol 1990 :66 :668-72 .
30 . Mulcahy D, Keegan J, Fingret A, ei al . Circadian variation of heart rate
GANDF I FT AL .
81AMBULATORY ISCHEIv1IA AND ANGINA IN THE POPULATION
is affected by environment : a study of continuous electrocardiographicmonitoring in members of a symphony orchestra . Br Heart J 1990:64 :388-92 .
31 . Kannel WB, Castelli WP .. Gardon T. Serum cholesterol lipoproteins andthe risk of coronary heart disease . Ann !nteru Med 1971 :74 :1-12 .Vlietstra R . Frye R, Kronmal R . et al . Risk factors and angiographiccoronary artery disease : a report from the Coronary Artery Surgery StudyICASSI . Circulation 1980 :62 :254-61 .
33 . Cupples LA. Gagnon D. Kannel W . Long and short term risk of suddencoronary death . Circulation 1992;85 Suppl 1 :1-11-8 .
34. Panza J, Quyyumi A, Diodati J, Callahan T, Epstein S . Prediction of thefrequency and duration of ambulatory myocardial ischemia in patientswith stable coronary artery disease by determination of the ischemicthreshold from exercise testing : importance of the exercise protocol .J Am Coll Cardiol 1991 ;17 :657-63-
35. Weiner D, Ryan T. McCabe C, et al . Prognostic importance of a clinicalprofile and exercise lest in medically treated patients with coronary arterydisease, J Am Coll Cardiol 1984 :3 :772-9.
36 . Cohn PF. Mechanisms of myocardial ischemia . Am J Cardiol 1992 ;70 :14G-8G .