Embed Size (px)
Citation preview

Chapter02C.3.indd 378 11/02/14 1:07 PM

TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE
IN PARTIALLY IMMUNE INDIVIDUALS
Graham A.W. Rook
CHAPTER 2C.3
Clinical studies that are applied without taking into account the peculiarities of each geographical region can lose relevance.
‘Life can dawn three paces from the fire.’
Eppur si muoveJorge R. Bermúdez
To work without connectionÁngel RamírezOil on canvas; 66 3 67 cm
Chapter02C.3.indd 379 11/02/14 1:07 PM

Chapter02C.3.indd 380 11/02/14 1:07 PM

ABSTRACT Much of the TB in developing countries occurs in deprived individuals living in crowded conditions, stressed, malnourished, smoking and helminth-infected. Exposure to MTB tends to be high dose and repetitive over many weeks or months due to delayed diagnosis of cases within the family. Under these conditions the Th2 components of the response, already primed by environmental mycobacteria, tend to be exaggerated, therefore raised IL-4 and TGF-β are most striking in TB in developing countries. This combination of cytokines inhibits not only macrophage function, but also the “rescue” mechanisms that attempt to control the infection when macrophage function is compromised (apoptosis, cytotoxic T cells, and autophagy). IL-4 also contributes to TNF-mediated tissue damage, and IL-4, IL-13 and TGF-β play major roles in the pulmonary fibrosis that is a neglected aspect of TB. These functions of IL-4, 13 and TGF-β have been neglected because they are not usually involved, following low-dose infection in specific pathogen-free mice. However, the latter now appears to be a model that falls somewhere on the spectrum of human latent TB: the bacterial numbers (CFU) reach plateau, and the mice eventually “drown” because of the excessive volume of granuloma in very small lungs. When the conditions found in developing countries are mimicked by using higher infecting doses or appropriate combinations of mouse strain and MTB strain, a progressive increase in the CFU is seen, and the involvement of IL-4 and TGF-β is then readily demonstrated by immunotherapeutic approaches that deplete or inhibit either cytokine. Interestingly, in developing countries, the ratio of IL-4 to IL-4d2 (an inhibitory splice variant of IL-4) is emerging as a relevant biomarker of disease or susceptibility.
CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
Chapter02C.3.indd 381 11/02/14 1:07 PM

382 SECTION 2 MAin PlAyERs
INTRODUCTION TB remains one of the most serious and yet neglected global health problems. Most TB patients are located in developing countries, and there is an apparent need to focus on the immunology of the disease as it occurs where the problem is most severe. In an accompanying chapter entitled ‘The “Old Friends” hypothesis and TB: Impact on the development of new vaccines’ I have outlined some of the ways in which the immune systems of people living in deprived circumstances in developing countries differ from those living in rich Northern urban centres. These differences are manifested clinically as a switch from infectious disease, to increasing incidences of a variety of chronic inflammatory disorders such as allergies, autoimmunity and inflammatory bowel disease that are rare in developing countries (1). This dramatic shift in patterns of disease involves changes to the priming of regulatory circuits within the immune system that are described in the other chapter, together with an attempt to show how these insights can help us understand the unique problems of the developing countries’ environment. In this chapter, these arguments are briefly summarised, and some aspects of the immunology of TB in developing countries, and also in the mouse models that use high and low infectious challenge doses are outlined in the following sections.
TB IN DEVELOPING COUNTRIES The background to this discussion leans on the fact that in developing countries most of which are warm, humid and close to the equator, there is massive exposure to environmental mycobacteria that induce cross-reactive mixed Th1/Th2 and regulatory T cell responses (2–5). These responses are partially protective (6, 7), and tend to mask the effects of BCG in these environments, though BCG can be shown to provide similar protection to those who are not already sensitised to mycobacteria (6, 7). This protection, whether provided by BCG or by environmental mycobacteria, might be effective against sporadic low dose challenge in well-nourished, healthy citizens of Europe, and this accounts for the success of BCG trials in Europe. It can also be surprisingly effective for many months in developing country conditions. For example, in Gambia many individuals fail to even become latently infected despite prolonged close contact with open cases of TB (8, 9). However, such protection is not reliable in the presence of persistent, repetitive high dose challenge such as can result from crowded living conditions and delayed diagnosis of TB in family members sharing poor quality accommodation. Moreover, the tendency of persistent and repeated high challenge doses to overcome Th1-mediated immunity is increased by protein
Chapter02C.3.indd 382 11/02/14 1:07 PM

383 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
malnutrition (10, 11) and psychological stress (12–14), and smoking. Thus, in the next section the effects of low and high challenge doses on the immunology of TB in animal models will be discussed.
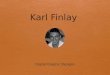
ANIMAL MODELS AfTER LOw DOSE CHALLENGE wITH MTB; LATENT DISEASE In most laboratories, when specific pathogen-free (SPF) mice are infected by aerosol with 100-200 living MTB, the organisms proliferate for about 3 weeks until a Th1 response develops (IFN-γ and TNF) (15, 16). Then, the proliferation ceases and the viable bacilli in the lung will reach a plateau. The animals eventually die, but this is due to the expanding granulomas and cellular infiltration, and in effect the animals are “drowned” (shown diagrammatically in Figure 2C.3.1). This probably does not represent a model of human disease. The mice die because they are very small animals, and the expanding granulomas rapidly reduce the lung tissue available for respiratory function, despite the effective control of bacterial growth. The air volume of the lungs of a relatively large mouse is about 300-400 microlitres. Therefore 200 granulomas will “drown” a mouse before they reach 1.5 mm in diameter (total of 353.4 microlitres, assuming that they are spherical), whereas these would not be noticed in a human. These low dose infection models, where bacterial proliferation ceases, are clearly models that represent a point somewhere on the spectrum of human latent TB, not of progressive disease.
100–200 mtb organisms by aerosol (Low dose challenge)
Cfu (bacteria) stop increasingNo interleukin 4 (Il–4)IL–4 gene knockout hasMouse “drowned” by cells in lung
no effect
Days since low dose aerosol challenge
Cfu
/lung
0 20 40 60 80 100
Figure 2C.3.1 Mouse models of TB that use low challenge doses, in specific pathogen-free laboratory mice
Note: The proliferation of organisms ceases when the Th1 response develops at about 3 weeks, but the mice eventually die by drowning in expanding granulomas and cellular infiltration. This is inevitable in such a small animal. Knocking out IL-4 or STAT-6 has no effect on the progress of the disease in these models.
Chapter02C.3.indd 383 11/02/14 1:07 PM

384 SECTION 2 MAin PlAyERs
However, this is the type of model that has been used for almost all studies of TB in Europe and the USA. This model has also served as the initial screening step for the selection of vaccine candidates. Interestingly, in models of this type, IL-4 plays no role at all (15). Functional deletion of the genes for signal transducer and activation of transcription 6 (Stat6), interleukin-4 receptor alpha chain (IL-4Rα), or IL-4 plus IL-13 (IL-4/IL-13) does not increase the resistance of mice to such low dose challenge (15).
ANIMAL MODELS AfTER HIGHER DOSE CHALLENGE wITH MTB; PROGRESSIVE DISEASE In some laboratories, the organisms do continue to proliferate after the Th1 response develops. Such laboratories are often using higher challenge doses of MTB (Figure 2C.3.2). When more than 105 MTB are given, either directly into the airways (intratracheal injection) (17, 18) or by intravenous injection (19, 20), a CFU plateau may be detectable at 3 weeks, but this is transient, and a few days later bacterial proliferation starts again, and in addition to granulomas, there is the occurrence of widespread pneumonia containing MTB. It is the extent of this pneumonia, rather than of granuloma, that correlates with death.
Importantly, this secondary growth of bacilli in the high dose challenge models is preceded by the appearance of lymphocytes expressing IL-4. However, the role of IL-4 has been controversial for two reasons. First, high dose challenge with mycobacteria is known to push the response towards Th2 (21, 22), but that does not prove that the IL-4 is involved in the pathogenesis of TB. Secondly, IL-4 is not involved in the pathogenesis of the low challenge dose model, as pointed out above (15). Nevertheless, it is now proven that IL-4 is directly involved in models where bacterial proliferation restarts after the plateau, as it occurs after higher dose challenge. In these models the infection is attenuated in mice with non-functional IL-4 genes (IL-4-/-) (17), and it can be partially treated by administering neutralising antibody to IL-4 (20). Interestingly, in wild type mice, the high dose infection is accompanied by a marked increase in levels of TGF-β (17). However in IL-4-/- mice there is a brief early peak of TGF-β, which then falls to very low levels (17). This has raised the possibility that neutralising the TGF-β would also treat the disease after high dose challenge (23). Administering recombinant soluble Type III TGF-β receptors have attenuated the disease, and reduced the expression of IL-4 (23). Thus, these two cytokines are inter-dependent in this model, and neutralising either TGF-β or IL-4 down-regulates the other. Interestingly, neutralising either IL-4 or TGF-β does not cure the animals, but reduces the bacillary load to a
Chapter02C.3.indd 384 11/02/14 1:07 PM

385 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
plateau, resembling the disease after low dose challenge (Figure 2C.3.2). More recently, these observations have been confirmed and extended using transgenic mice, over-expressing the dominant negative form of the type-II TGF-β receptor. These animals are remarkably resistant to TB (24). Moreover, when mice with established infection were treated with D4476 (full name:4-[4-(2,3-Dihydro-1,4-benzodioxin-6-yl)-5-(2-pyridinyl)-1H-imidiazol-2-yl]benzene) which can inhibit the TGF-β signalling pathway the drug was found to be therapeutic (24). In view of the striking interactions between the two cytokines, it will be exciting to see whether simultaneous inhibition of both IL-4 and TGF-β can have a more pronounced therapeutThese findings reveal three important facts:
1 High dose challenge induces a pattern of disease in which IL-4 and TGF-β are increased, even when there is no pre-induced Th2 response.
2 IL-4 and TGF-β are mutually dependent on each other, and each synergistically induces the other in mouse TB models.
3 In these models the IL-4 and TGF-β play a crucial role in enabling the continuing proliferation of MTB.
Interestingly, in Mexico (25) or Brazil (18) it is essential to give these larger challenge
High dose challenge (> 105 Mtb, intravenous or intra-tracheal)
Days since low dose aerosol challenge (i.v. or i.t.)
0 20 40 60 80 100
Cfu
/lung
High IL-4, and IL-13, &secondary rise in TGF-�
Can treat the progressive phaseinduced by high dose challenge by:-
Knocking out IL-4 ( )Blocking IL-4 with an natibodyPartially blocking TGF-Dominant negative TGF RIIInhibit TGF- signaling with D4476
M.vaccae
��
�
Figure 2C.3.2 Mouse models that use high challenge Doses (>105) of MTB, whether intravenous or intratracheal
Note: In sharp contrast to low-dose challenge (Figure 2C.3.1), in these high-dose models there is a secondary phase of bacterial proliferation, accompanied by raised IL-4 and TGF-β. These cytokines can be shown to be directly involved in this secondary phase of proliferation, because neutralising them, or blocking their signalling, causes bacterial proliferation to diminish or cease. This secondary phase of bacillary replication might be the murine equivalent of progressive TB in man in developing countries, where raised IL-4 and TGF-β are prominent.
Chapter02C.3.indd 385 11/02/14 1:07 PM

386 SECTION 2 MAin PlAyERs
doses that induce IL-4 and TGF-β, because 100-200 organisms can fail to cause disease. It has recently emerged that animals in the breeding rooms in both Brazil (26) and Mexico (Y. Lopez Vidal and R. Hernandez Pando, personal communication) are exposed to environmental mycobacteria. Thus, this resistance to low dose infection parallels that seen in human populations in the same developing countries’ environments (27), and is due to prior contact with mycobacteria. The observations outlined above suggest that high dose challenge helps to bias the response towards Th2, which blocks the protective response and allows bacterial replication and progressive disease to develop. The mechanisms are described below.
THE IMMUNOLOGY Of TB IN DEVELOPING COUNTRIES What is being suggested at this point, is that TB seen in developing countries is occurring in partially immune individuals, in whom the Th1 response has been incapacitated by repeated high dose challenge, and often exacerbated by malnutrition, smoking and stress. As shown above, in mice, high dose challenge leads to progressive disease via mechanisms involving IL-4 and TGF-β. What is the evidence that these mediators play a similar role in TB, in the populace of the developing countries?
Interleukin-4The most obvious difference between TB in rich and developing countries is the frequency of patients with high levels of IL-4. It is important to note that recent studies using microarrays do not provide meaningful data on this cytokine, because at the time of writing (December 2010), neither the Affymetrix nor the Illumina probes distinguish IL-4 from IL-4d2 (as will be discussed below). The expression of IL-4 is increased in some TB patients even in rich Northern countries, both in blood (28, 29) and in the lungs (29, 30). Interestingly the ½ life of mRNA encoding IL-4 is longer in the blood lymphocytes from TB patients, than from matched controls (31). However, TB accompanied by very high levels of IL-4 is characteristic of the developing countries where BCG fails (Figure 2C.3.3) [reviewed in (32)], which are precisely the areas where high loads of helminths and other features of the developing countries’ lifestyle prevail. Sometimes, TB in developing countries is accompanied by such high levels of IL-4 that it can be measured free in the serum by ELISA (33). This represents truly enormous levels that are not seen even in a Th2-mediated disorder such as atopic asthma in Europe.
Chapter02C.3.indd 386 11/02/14 1:07 PM

387 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
Figure 2C.3.3 The geographical location of TB patients with very high levels of IL-4
Note: Each symbol represents a published study, (reviewed in 32). The expression of IL-4 is increased in a percentage of patients in all countries when appropriate methods are used to distinguish between IL-4 and IL-4d2, but very high levels, often measurable in serum by ELISA, are characteristic of cavitatory TB in countries close to the equator. Note that the failure of BCG close to the equator is due to the conditions prevalent in the developing countries, and is not directly due to latitude.
Soluble IL-4 receptors (sIL-4R)sIL-4R is produced either by the secretion of an alternatively spliced variant by cells stimulated by IL-4, or by the proteolytic cleavage of the membrane-bound receptor after TCR engagement (34). At high concentrations, sIL-4R can inhibit the functions of IL-4. However, at low concentrations sIL-4R can prolong the plasma ½ life of IL-4, and also enhance its functions. sIL-4R has a lower affinity for IL-4 than the membrane form of the receptor, so sIL-4R can protect circulating IL-4, prolong its ½ life 10- to 20-fold, and pass it on to the membrane receptors (35). Therefore, the biological significance of changing sIL-4R levels is not clear. A recent study of pulmonary, meningeal and renal TB in Mexico has found that sIL-4R is abnormally low in all forms of the disease, and at all times (36). Despite the uncertainty surrounding the precise role of low sIL-4R levels, when set against the few existing studies in man, the result is provocative. Levels of sIL-4R are elevated in children with severe malaria (37) and in visceral leishmaniasis (38), but as we have found
Chapter02C.3.indd 387 11/02/14 1:07 PM

388 SECTION 2 MAin PlAyERs
in the Mexican TB patients (36), levels are abnormally low in subjects with stable asthma (39) or allergic rhinitis (40).
Interleukin 4delta2 (IL-4d2) There is a further, usually neglected complication. IL-4d2 is a splice variant of IL-4 that lacks the 16 amino acids encoded by exon 2. Assays that use antibodies, such as ELISAs, flow cytometry, or immunohistochemistry, might be measuring both, or either cytokine. This is yet to be known. Similarly, RT-PCR using primers based on sequences within exon 1 and exon 3 or 4 measure both mRNAs simultaneously, so the results cannot be interpreted. (Currently available microarray probes in the kits provided by Illumina and Affymetrix cannot be used because they measure IL-4 and IL-4d2 together). IL-4d2 seems to be present in most (perhaps all) species (41), including the mouse (42), and two groups have shown that the cloned molecule is a competitive antagonist of IL-4 (43, 44).
Since specific monoclonal antibodies have not yet been identified, the two forms can only be distinguished by RT-PCR, using appropriately re-designed primers. Using RT-PCR, we have previously established that in asthma there is a selective increase in the expression of IL-4, indicating a ‘classical’ Th2 response (45). By contrast, in the lungs of patients with systemic sclerosis, there is a selective increase in the expression of IL-4d2 (46). In TB the situation is more complex, with increased expression of both forms, but with a bias towards IL-4 in progressive disease (47, 48). During successful treatment, mRNA encoding IL-4 very slowly decreases, whereas the IL-4d2 mRNA is significantly increased by 6 months (48). The latter observation is confirmed recently (49). Using specific RT-PCR to investigate the expression of various mediators during the first week of treatment, expression of IL-4 has been decreased 4-fold while the expression of IL-4d2 has been increased 32-fold during this period. Interestingly, there is no change in the expression of IFN-γ or of other mediators during this first week (49).
The importance of IL-4 is supported by observations in latent TB infection. Approximately 5-10% of those exposed to MTB develop progressive disease within weeks. However, the other 90-95% develop latent infection that can be a stable state that lasts a lifetime. Expression of IL-4d2 mRNA is increased in unstimulated peripheral blood mononuclear cells from healthy donors who have established, stable latent TB, as defined by the presence of an IFN-γ response to ESAT-6, but no recent history of exposure to MTB has been noted. This has been shown by different methods in latently infected donors from Ethiopia and The Gambia (50, 51). This might indicate that a rise in IL-4d2 is a protective strategy that helps to block any
Chapter02C.3.indd 388 11/02/14 1:07 PM

389 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
tendency of IL-4 to undermine effective immunity. The IL-4/IL-4d2 ratio might be a factor that determines whether latent TB progresses or remains latent (52).
TB and allergic disorders If progressive TB is associated with raised IL-4, while stable longstanding latent TB is associated with raised IL-4d2 (an inhibitor of IL-4), then we might expect evidence of different interactions between these two clinical states and allergic disorders. Similarly, if such a relationship were found, it would constitute evidence for the biological significance of the IL-4 in TB. Interestingly, an increase in IgE (53, 54) and increased sensitisation to common allergens can be demonstrated in TB patients (55). Moreover they have IgE antibody to MTB itself (56). (This striking point is often forgotten, as is the presence of equally IL-4-dependent IgG4 antibody (57, 58)). By contrast, in healthy populations with large tuberculin skin-test responses attributable to latent TB, there are reduced allergic responses and symptoms (59–61).These interactions have been extensively reviewed elsewhere (62).
TGF-β TGF-β levels would be expected to be high in TB in developing countries both because of the priming of regulatory cells already described, and because of secondary induction by IL-4, though it is not yet clear whether levels of TGF-β are also higher in TB in developing countries than in already developed ones. When both are measured in a place where IL-4 levels are high, cells from patients with the most advanced TB have shown the highest release of both IL-4 and TGF-β (33). Similarly serum levels of TGF-β are most strikingly raised in patients with advanced disease (63), and a rise is particularly characteristic of MDR patients in Brazil (64).
There are strong links between IL-4 and TGF-β. Th2 cytokines, including IL-4 and IL-13, enhance release and activation of TGF-β (65). Remarkably, when expression of TGF-β is followed throughout the course of the infection in a mouse model of pulmonary TB it is found that whereas in normal mice TGF-β expression rises to high levels by day 21 and stays high thereafter, in IL-4-/- mice there is an early peak at 7-14 days, followed by barely detectable expression of TGF-β from day 21 until day 120 when the experiment is terminated (17). Therefore, in the context of TB, as in asthma, IL-4 is a major controller of expression of TGF-β, and it will be interesting to see whether TGF-β is disproportionately raised in developing countries’ TB, in parallel with IL-4.
Chapter02C.3.indd 389 11/02/14 1:07 PM

390 SECTION 2 MAin PlAyERs
Excessive release of TGF-β has also been implicated in the pathogenesis of TB (33, 66), and it is abundant in tuberculous lung lesions (66). The mannose-capped lipoarabinomannan (ManLAM) of MTB is a potent inducer of TGF-β (67). Interestingly, human blood monocytes and alveolar macrophages produce bioactive TGF-β upon stimulation by MTB, so a signal from the organism is causing the activation of TGF-β, as well as its secretion (68). Bronchoalveolar lavage (BAL) cells from TB patients show spontaneous and simultaneous production of TGF-β and of the receptors TGF-βRI and TGF-βRII, required for its activity (69). Natural inhibitors of TGF-β restore T-cell responses of patients’ cells in vitro, and augment monocyte effector function against MTB (70).
Th2-associated chemokines Several chemokines are strongly associated with Th2 activity, but these have received little attention in TB. There are reports that MTB, BCG or specific recombinant antigens can induce the secretion of CCL2 from the peripheral blood mononuclear cells of TB patients (71, 72). Raised serum levels of CCL2 are seen in TB in Mexico (36, 73), but not in Pakistan (74) or Brazil (75). A recent study casts some light on these discordant results because CCL2 is most obvious in early disease (and in meningeal disease) and is inversely related to levels of CCL18, which rise with increasing disease duration. Thus, discordant data might be related to disease duration in different studies (36). Significantly, a single nucleotide polymorphism (SNP) that causes overproduction of CCL2 is the strongest genetic link with susceptibility to TB in both Mexico and Korea (73). The same SNP is associated with increased severity of atopic asthma symptoms in a European population (76). The effect of the CCL2 SNP on susceptibility to TB in Mexico appears to be very strong (77), and similar results have been reported in some (78, 79) but not all studies (80, 81), though in one case a link to a different SNP of the same chemokine has been found (82).
CCL2 is interesting in the context of TB immunology. It is produced by many cell types, including endothelial, fibroblasts, epithelial, smooth muscle, mesangial, astrocytic, monocytic and microglial cells (83). CCL2 regulates the migration and infiltration of monocytes, memory T lymphocytes and natural killer (NK) cells. It also has poorly studied anti-inflammatory roles dependent on the expression of its receptor (CCR2) in regulatory T cells (83, 84). CCL2 is often designated a Th2 chemokine because, in the mouse at least, CCL2 is both a cause and a consequence of Th2 bias. IL-4 induces the production of CCL2 (85), polarizes Th0 cells towards Th2 (86–88) and preferentially recruits Th2 cells (89). Moreover CCL2 appears to down-regulate the release of IFN-γ from murine Th1 cells (90). The same is usually
Chapter02C.3.indd 390 11/02/14 1:07 PM

391 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
true in man. IL-4 and IL-13 up-regulate the expression of CCL2 in human bronchial epithelial cells (89), and CCL2 is strikingly upregulated in biopsies from asthmatics (91). In sharp contrast, CCL2 downregulates the release of IL-12 from human macrophages (92), and low IL-12 is noted in the Mexican patients with the relevant SNP (73). Importantly, serum levels have been measured in a number of human diseases, and are characteristically raised more in Th2 or mixed Th1/Th2 disorders than in Th1-mediated disorders (93).
In another case, even stronger Th2-associated chemokine is CCL18, which is a marker of alternative macrophage activation (85, 94, 95). A recent study has measured levels of CCL18 in pulmonary, meningeal and renal TB in Mexico (36). Levels are strikingly raised in all disease types, and they increase with disease duration. The increase is least in meningeal TB which involves patients with very short clinical history, and highest in those pulmonary patients with very long history. We are not aware of any previous studies of CCL18 in TB, although there is one report that MTB can induce the expression of CCL18 in human macrophages (including alveolar) and DC in vitro (96). CCL18 is important in the current context because IL-4 and IL-13 induce expression of CCL18 in alveolar macrophages, DC and monocytes, whereas the expression is inhibited by IFN-γ (85, 94, 95). The CCL18 receptor is preferentially expressed on basophils and Th2 cells, for which CCL18 is a chemoattractant (94). Thus CCL18 is associated with allergic asthma. PBMC from asthmatics allergic to house dust mite cultured in the presence of Der p1 allergen secretes CCL18 after stimulation, whereas those from healthy donors do not (94). Similarly, CCL18 expression is associated with an atopic dermatitis phenotype when compared with other chronic inflammatory skin diseases (97).
Another major function of CCL18 is the regulation of fibrosis. In patients with fibrosing lung disease, spontaneous CCL18 production by alveolar macrophages is greatly increased and correlates with CCL18 serum concentrations. Changes in these concentrations closely correlate with changes in pulmonary function data at follow-up (95, 98). CCL18 shares several functional properties with TGF-b and up-regulates collagen production by lung fibroblasts via the same signalling pathways (95). The levels of CCL18 seen in long-term TB are similar to those seen in conditions with large Th2 components, such as bacterial pneumonias and dengue fever (36). The results suggest that as TB progresses, there is an increasing Th2 component that might contribute to the pulmonary fibrosis and to the deactivation of Th1-mediated effector pathways (36). It is of course, possible that MTB can trigger the release of CCL18 via pathways that do not involve Th2 cytokines.
Chapter02C.3.indd 391 11/02/14 1:07 PM

392 SECTION 2 MAin PlAyERs
An obvious hypothesis is that early release of CCL2 recruits Th2 cells, which then release Th2 cytokines such as IL-13 and IL-4, and further driving the local production of CCL18.
THE DETRIMENTAL ROLES Of IL-4, OTHER TH2 CYTOkINES, AND TGf-b IN TB There are good reasons why this combination of high Th2 cytokines and TGF-β would be expected to facilitate a secondary phase of bacterial proliferation (52, 99).
Effector mechanisms that control MTB MTB inhibits classical Th1-mediated macrophage activation, because it blocks phagosome maturation (100), lysosome fusion (101), presentation to Th1 cells (102, 103), and triggering via the IFN-γ receptor (104) (Figure 2C.3.4). IL-4 together with IL-13 further impair the macrophage function by inducing alternative macrophage activation (105). This involves numerous inappropriate changes, including enhanced iron uptake (106), and downregulated TLR-2 and TNF, accompanied by increased soluble TNF receptors, DC-SIGN and IL-10 (107, 108, Reviewed in 109). Similarly, TGF-β increases the apoptosis of T cells activated by mycobacterial antigens (110–112), and TGF-β enhances growth of MTB in macrophages (24, 113).
Figure 2C.3.4 MTB inhibits classical Th1-mediated macrophage activation, because it blocks phagosome maturation (100), lysosome fusion (101), presentation to Th1 cells (102, 103), and triggering via the IFN-γ receptor (104)
Chapter02C.3.indd 392 11/02/14 1:07 PM

393 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
In the progressive phase of the disease, the immune system therefore depends on several mechanisms that circumvent the failure of the infected phagososme, by promoting its uptake by a fresh macrophage, or directly exposing the bacteria to bactericidal peptides. These mechanisms are illustrated in Figure 2C.3.5, and include apoptosis, cytotoxic T cells, and autophagy. All of these mechanisms are susceptible to down-regulation by a combination of Th2 cytokines and TGF-β (Figure 2C.3.6) (24, 27, 114–116). Indeed, the ability of IL-4 plus TGF-β to impair development and function of cytotoxic lymphocytes is now a major topic in tumour immunology, because tumour-infiltrating lymphocytes can be isolated from the tumour, rendered non-susceptible to TGF-β, and returned to the host, when they can make their way back to the tumour, and destroy it (115–117).
Figure 2C.3.5 A summary of the mechanisms that protect from TB
Note: M. tuberculosis inhibits the classical pathway of cell-mediated immunity, as shown in Figure 2C.3.4. The immune system circumvents the problem of the incapacitated phagosome by means of apoptosis, cytotoxic lymphocytes, and autophagy. Each of these can result in the transfer of the organisms to a new fully functional phagosome, or to their exposure to microbicidal peptides.
Chapter02C.3.indd 393 11/02/14 1:07 PM

394 SECTION 2 MAin PlAyERs
Pulmonary fibrosis Fibrosis is a major complication of TB, which is easily the most important cause of pulmonary fibrosis globally. This might seem odd because IFN-γ opposes fibrosis. Indeed, in man, pulmonary fibrosis tends to be associated with Th2 responses (65). This is because Th2 cytokines, including IL-4 and IL-13, enhance the release and activation of TGF-β, and interestingly, when pulmonary TB is established in IL-4-/- mice there is markedly less TGF-β, and less fibrosis (17), whereas fibrosis is increased in tuberculous mice with enhanced Th2 activity (118). CCL18 shares several functional properties with TGF-β and up-regulates collagen production by lung fibroblasts via the same signalling pathways (95). The levels of CCL18 seen in long-term TB in Mexico are strikingly raised (36). Therefore, it is likely that CCL18 synergises with IL-4, IL-13 and TGF-β in the induction of the characteristic crippling fibrosis that accompanies long-term TB.
Figure 2C.3.6 IL-4 & IL-13 +TGF-β inhibit killing of MTB
Chapter02C.3.indd 394 11/02/14 1:07 PM

395 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
Tissue damage, IL-4 and the toxicity of TNF TNF-α is essential for protection (119), but is clearly toxic in patients with progressive TB, in whom symptoms are alleviated by reducing TNF-α levels (120). In the BALB/c mouse we have shown that toxicity of TNF-α during progressive pulmonary TB is dependent upon the presence of IL-4, and is absent from IL-4-/- mice (17). Toxicity of TNF-α is readily restored in tuberculous IL-4-/- mice by administering recombinant IL-4 (17). The involvement of IL-4 in the toxicity of TNF-α in inflammatory lesions dominated by Th1 cells has been observed in other infectious disease models (121–123). There are a number of possible contributory mechanisms. Firstly, IL-4 causes reduced apoptosis as discussed above, and therefore, there is likely to be a corresponding increase in necrosis; apoptotic cells are cleared without inflammation, but necrotic cells trigger further inflammatory reactions. Secondly, there is a large synergy between TNF-α and IL-4 in the induction of expression of VCAM-1 on endothelial cells (124, 125). This synergy results from a combination of transcriptional activation by TNF-α and the stabilization of resulting transcripts by IL-4 (125). Increased VCAM-1 will mediate increased cellular infiltration, and there is evidence that most of the cells present in TB lesions are irrelevant to immunity, and apparently involved in immunopathology rather than protection (126). Thirdly, when T cells are exposed simultaneously to IL-2 and to Th2 cytokines, they become resistant to suppression by glucocorticoid feedback because they express the β splice variant of the glucocorticoid receptor which does not bind glucocorticoids, but antagonizes the transactivating activity of the classic receptor (127). Thus, the usual negative feedback on inflammation is diminished, despite enhanced conversion of inactive cortisone to cortisol in the lesions of TB (128). These observations and mechanisms might explain why IL-4 is clearly associated with the extent of pulmonary cavitation (30, 47, 129).
CONCLUSIONS AND IMPLICATIONS In conclusion, it seems probable that most individuals in developing countries, where BCG fails, are partially immune to TB as a result of BCG vaccination and sensitisation by environmental mycobacteria (6). This immunity might be able to protect them from low dose challenge, and it is suggested that this is how BCG succeeds in rich Northern countries. Part of the apparent failure of BCG in developing countries is in fact a statistical artefact due to the increasing protection derived from contact with environmental mycobacteria, which narrows the gap between the incidences of TB in the vaccinated and non-vaccinated populations. However, by the age of 15-20 years essentially everyone in developing countries has this background response,
Chapter02C.3.indd 395 11/02/14 1:07 PM

396 SECTION 2 MAin PlAyERs
so the disease still thrives in this ‘protected’ group. This protection fails under the conditions that prevail in developing countries; 1) repeated high dose challenge due to overcrowding; 2) A pre-existing mixed Th1 and Th2 response to mycobacteria; 3) The psychological stresses of poverty; 4) Smoking. Under these conditions, repeated high dose challenge from untreated individuals sharing the same confined space might be able to drive enough IL-4, IL-13 and TGF-β to overcome the protective response, resulting in the characteristic ‘high IL-4’ TB seen in many developing countries (32, 33). There is however a paradox. There is a general agreement that “dose matters”, but the evidence suggests that in humans, even after high dose challenge there is usually only one primary lesion, and one Ghon focus. This implies that most of the loads of organisms that are taken in during high dose challenge play a role in the modulation and deviation of the immune system, but do not form the clone of bacteria that eventually proliferate and cause disease. Perhaps these immunomodulatory, but non-proliferating organisms are the lipid-rich dormant bacteria that form the majority of the sputum population (130).
There are major implications. First, models used to select vaccine candidates might need to involve high dose challenge of partially immune animals, in order to mimic the situation in the countries where a new vaccine is most needed. Secondly, it might be useful to document the two immune response patterns (i.e. low IL-4 TB versus high IL-4 TB) in the clinical trial areas, and in particular in trial participants who contract disease. It might be very difficult to vaccinate against TB resulting from high dose challenge in partially immune individuals. Finally, the immunology and genetics of TB occurring after high dose challenge in partially immune people are likely to be quite different from the immunology and genetics of susceptibility to sporadic low dose challenge in unvaccinated citizens of the USA (131).
REFERENCES
1. Rook GAW. 99th Dahlem Conference on infection, inflammation and Chronic inflammatory Disorders: Darwinian medicine and the ‘hygiene’ or ‘old friends’ hypothesis. Clin Exp immunol, 2010; 160: 70–9.
2. stewart GR, Boussinesq M, Coulson T, Elson l, nutman T, and Bradley JE. Onchocerciasis modulates the immune response to mycobacterial antigens. Clin Exp immunol, 1999; 117: 517–23.
3. Elliott AM, Hurst TJ, Balyeku Mn, Quigley MA, Kaleebu P, French n, et al. The immune response to Mycobacterium tuberculosis in HiV-infected and
Chapter02C.3.indd 396 11/02/14 1:07 PM

397 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
uninfected adults in Uganda: application of a whole blood cytokine assay in an epidemiological study. int J Tuberc lung Dis, 1999; 3: 239–47.
4. Weir RE, Black GF, nazareth B, Floyd s, stenson s, stanley C, et al. The influence of previous exposure to environmental mycobacteria on the interferon-gamma response to bacille Calmette-Guerin vaccination in southern England and northern Malawi. Clin Exp immunol, 2006; 146: 390–9.
5. Fine PE. Variation in protection by BCG: implications of and for heterologous immunity. lancet, 1995; 346: 1339–45.
6. Radhakrishna s, Frieden TR, subramani R, and narayanan PR. influence of sex, age and non-tuberculous infection at intaake on the efficacy of BCG: reanalysis of 15 year data from a randomised control trial in south india. indian J Med Res, 2006; 123: 119–25.
7. Rook GA and Kim lU. Comments on the new analysis of the Chingleput BCG trial. indian J Med Res, 2006; 123: 103–6.
8. lienhardt C, Fielding K, sillah J, Tunkara A, Donkor s, Manneh K, et al. Risk factors for tuberculosis infection in sub-saharan Africa: a contact study in The Gambia. Am J Respir Crit Care Med, 2003; 168: 448–55.
9. lienhardt C, sillah J, Fielding K, Donkor s, Manneh K, Warndorff D, et al. Risk factors for tuberculosis infection in children in contact with infectious tuberculosis cases in the Gambia, West Africa. Pediatrics, 2003 111: e608–14.
10. Chan J, Tian y, Tanaka KE, Tsang Ms, yu K, salgame P, et al. Effects of protein calorie malnutrition on tuberculosis in mice. Proc natl Acad sci U s A, 1996; 93: 14857–61.
11. Rodriguez l, Gonzalez C, Flores l, Jimenez-Zamudio l, Graniel J, and Ortiz R. Assessment by flow cytometry of cytokine production in malnourished children. Clin Diagn lab immunol, 2005; 12:502–7.
12. Elenkov iJ. Glucocorticoids and the Th1/Th2 balance. Ann n y Acad sci, 2004; 1024: 138–46.
13. Agarwal sK and Marshall GD Jr. Glucocorticoid-induced type 1/type 2 cytokine alterations in humans: a model for stress-related immune dysfunction. J interferon Cytokine Res, 1998; 18: 1059–68.
Chapter02C.3.indd 397 11/02/14 1:07 PM

398 SECTION 2 MAin PlAyERs
14. Herberth G, Weber A, Roder s, Elvers HD, Kramer U, schins RP, et al. Relation between stressful life events, neuropeptides and cytokines: results from the lisA birth cohort study. Pediatr Allergy immunol, 2008; 19(8): 722–9.
15. Jung yJ, laCourse R, Ryan l, and north RJ. Evidence inconsistent with a negative influence of T helper 2 cells on protection afforded by a dominant T helper 1 response against Mycobacterium tuberculosis lung infection in mice. infect immun, 2002; 70: 6436–43.
16. Cooper AM and Khader sA. The role of cytokines in the initiation, expansion, and control of cellular immunity to tuberculosis. immunol Rev, 2008; 226: 191–204.
17. Hernandez-Pando R, Aguilar D, Garcia Hernandez Ml, Orozco H, and Rook GAW. Pulmonary tuberculosis in Balb/c mice with non-functional il-4 genes; changes in the inflammatory effects of TnF-a and in the regulation of fibrosis. Eur J immunol, 2004; 34: 174–83.
18. silva Cl, Bonato Vl, Coelho-Castelo AA, De souza AO, santos sA, lima KM, et al. immunotherapy with plasmid DnA encoding mycobacterial hsp65 in association with chemotherapy is a more rapid and efficient form of treatment for tuberculosis in mice. Gene Ther, 2005; 12: 281–7.
19. lowrie DB, Tascon RE, Bonato Vl, lima VM, Faccioli lH, stavropoulos E, et al. Therapy of tuberculosis in mice by DnA vaccination. nature, 1999; 400: 269–71.
20. Roy E, Brennan J, Jolles s, and lowrie DB. Beneficial effect of anti-interleukin-4 antibody when administered in a murine model of tuberculosis infection. Tuberculosis (Edinb), 2007; 88: 197–202.
21. Hernandez-Pando R, Pavon l, Arriaga K, Orozco H, Madrid-Marina V, and Rook GAW. Pathogenesis of tuberculosis in mice exposed to low and high doses of an environmental mycobacterial saprophyte. infect immun, 1997; 65: 3317–27.
22. Power CA, Wei G, and Bretscher PA. Mycobacterial dose defines the Th1/Th2 nature of the immune response independently of whether immunization is administered by the intravenous, subcutaneous, or intradermal route. infect immun, 1998; 66: 5743–50.
23. Hernandez-Pando R, Orozco-Esteves H, Maldonado HA, Aguilar-leon D, Vilchis-landeros MM, Mata-Espinosa DA, et al. A combination of a transforming
Chapter02C.3.indd 398 11/02/14 1:07 PM

399 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
growth factor-beta antagonist and an inhibitor of cyclooxygenase is an effective treatment for murine pulmonary tuberculosis. Clin Exp immunol, 2006; 144: 264–72.
24. Jayaswal s, Kamal MA, Dua R, Gupta s, Majumdar T, Das G, et al. identification of host-dependent survival factors for intracellular Mycobacterium tuberculosis through an siRnA screen. Plos Pathog, 2010; 6: e1000839.
25. Arriaga AK, Orozco EH, Aguilar lD, Rook GAW, and Hernandez Pando R. immunological and pathological comparative analysis between experimental latent tuberculous infection and progressive pulmonary tuberculosis. Clin Exp immunol, 2002; 128: 229–37.
26. lowrie DB. DnA vaccines for therapy of tuberculosis: where are we now? Vaccine, 2006; 24: 1983–9.
27. Rook GA, Hernandez-Pando R, and Zumla A. Tuberculosis due to high-dose challenge in partially immune individuals: a problem for vaccination? J infect Dis. 2009 199:613–8.
28. surcel HM, Troye-Blomberg M, Paulie s, Andersson G, Moreno C, Pasvol G, et al. Th1/Th2 profiles in tuberculosis based on proliferation and cytokine response of peripheral blood lymphocytes to mycobacterial antigens. immunology, 1994; 81: 171–6.
29. Dheda K, Chang Js, Breen RA, Haddock JA, lipman MC, Kim lU, et al. Expression of a novel cytokine, il-4delta2, in HiV and HiV-tuberculosis co-infection. Aids, 2005; 19: 1601–6.
30. Mazzarella G, Bianco A, Perna F, D’Auria D, Grella E, Moscariello E, et al. T lymphocyte phenotypic profile in lung segments affected by cavitary and non-cavitary tuberculosis. Clin Exp immunol, 2003; 132: 283–8.
31. Dheda K, Chang Js, Huggett JF, Kim lU, Johnson MA, Zumla A, et al. The stability of mRnA encoding il-4 is increased in pulmonary tuberculosis, while stability of mRnA encoding the antagonistic splice variant, il-4delta2, is not. Tuberculosis (Edinb), 2007; 87: 237–41.
32. Rook G, Dheda K, and Zumla A. Do successful tuberculosis vaccines need to be immunoregulatory rather than merely Th1-boosting? Vaccine, 2005; 23: 2115–20.
Chapter02C.3.indd 399 11/02/14 1:07 PM

400 SECTION 2 MAin PlAyERs
33. Dlugovitzky D, Bay Ml, Rateni l, Urizar l, Rondelli CF, largacha C, et al. in vitro synthesis of interferon-gamma, interleukin-4, transforming growth factor-beta and interleukin-1 beta by peripheral blood mononuclear cells from tuberculosis patients: relationship with the severity of pulmonary involvement. scand J immunol, 1999; 49: 210–7.
34. Blum H, Wolf M, Enssle K, Rollinghoff M, and Gessner A. Two distinct stimulus-dependent pathways lead to production of soluble murine interleukin-4 receptor. J immunol, 1996; 157: 1846–53.
35. Jung T, Wagner K, neumann C, and Heusser CH. Enhancement of human il-4 activity by soluble il-4 receptors in vitro. Eur J immunol, 1999; 29: 864–71.
36. Mendez A, Hernandez Pando R, Contreras s, Aguilar-leon D, and Rook GAW. CCl2, CCl18 and sil-4R in renal, meningeal and pulmonary TB; a 2 year study of patients and contacts. Tuberculosis (Edinb), 2011; 91(2): 140–5.
37. Perkmann T, Winkler H, Graninger W, Kremsner PG, and Winkler s. Circulating levels of the interleukin (il)-4 receptor and of il-18 in patients with Plasmodium falciparum malaria. Cytokine, 2005; 29: 153–8.
38. sang DK, Ouma JH, John CC, Whalen CC, King Cl, Mahmoud AA, et al. increased levels of soluble interleukin-4 receptor in the sera of patients with visceral leishmaniasis. J infect Dis, 1999; 179: 743–6.
39. schauer U, schmitt M, Muller s, Enssle K, Kurrle R, sundermann U, et al. soluble interleukin-4 receptor in atopic children. int Arch Allergy immunol, 1995; 108: 175–82.
40. Benson M, Wennergren G, Fransson M, and Cardell lO. Altered levels of the soluble il-1, il-4 and TnF receptors, as well as the il-1 receptor antagonist, in intermittent allergic rhinitis. int Arch Allergy immunol, 2004; 134: 227–32.
41. Gautherot i, Burdin n, seguin D, Aujame l, and sodoyer R. Cloning of interleukin-4 delta2 splice variant (il-4delta2) in chimpanzee and cynomolgus macaque: phylogenetic analysis of delta2 splice variant appearance, and implications for the study of il-4-driven immune processes. immunogenetics, 2002; 54: 635–44.
42. yatsenko OP, Filipenko Ml, Voronina En, Khrapov EA, sennikov sV, and Kozlov VA. Alternative splicing of murine interleukin-4 mRnA. Bull Exp Biol Med, 2004; 137: 179–81.
Chapter02C.3.indd 400 11/02/14 1:07 PM

401 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
43. Atamas sP, Choi J, yurovsky VV, and White B. An alternative splice variant of human il-4, il-4 delta 2, inhibits il- 4-stimulated T cell proliferation. J immunol, 1996; 156: 435–41.
44. Vasiliev AM, Vasilenko Rn, Kulikova nl, Andreev sM, Chikileva iO, Puchkova Gy, et al. structural and functional properties of il-4delta2, an alternative splice variant of human il-4. J Proteome Res, 2003; 2: 273–81.
45. seah GT, Gao Ps, Hopkin J, and Rook GAW. interleukin-4 and its alternatively spliced variant (il-4d2) in atopic asthmatics. Am J Resp Crit Care Med, 2001; 164: 1016–8.
46. sakkas li, Tourtellotte C, Berney s, Myers AR, and Platsoucas CD. increased levels of alternatively spliced interleukin 4 (il-4delta2) transcripts in peripheral blood mononuclear cells from patients with systemic sclerosis. Clin Diagn lab immunol, 1999; 6: 660–4.
47. seah GT, scott GM, and Rook GA. Type 2 Cytokine Gene Activation and its Relationship to Extent of Disease in Patients with Tuberculosis. J infect Dis, 2000; 181: 385–9.
48. Dheda K, Chang J-s, Breen RA, Kim lU, Haddock JA, Huggett JF, et al. in vivo and in vitro studies of a novel cytokine, interleukin-4delta2, in pulmonary tuberculosis. Am J Resp Crit Care Med, 2005; 172: 501–8.
49. siawaya JF, Bapela nB, Ronacher K, Beyers n, van Helden P, and Walzl G. Differential expression of il-4 and il-4{delta}2, but not TGF-{beta}, TGF-{beta}Rii, FOXP3, iFn-{gamma}, T-bet or GATA-3 mRnA in Fast and slow Responders to Anti-tuberculosis Treatment. Clin Vaccine immunol, 2008; 15: 1165–70.
50. Demissie A, Abebe M, Aseffa A, Rook GAW, Fletcher HA, Zumla A, et al. Healthy individuals that control latent infection with M. tuberculosis express high levels of Th1 cytokines and the il-4 antagonist il-4delta2. J immunol, 2004; 172: 6938–43.
51. Fletcher HA, Owiafe P, Jeffries D, Hill P, Rook GAW, Zumla A, et al. increased expression of mRnA encoding il-4 and its splice variant il-4d2 in cells from contacts of Mycobacterium tuberculosis in the absence of in vitro stimulation. immunology, 2004; 112: 669–73.
52. Rook GA, Hernandez-Pando R, Dheda K, and seah GT. il-4 in tuberculosis: implications for vaccine design. Trends immunol, 2004; 25:483–8.
Chapter02C.3.indd 401 11/02/14 1:07 PM

402 SECTION 2 MAin PlAyERs
53. Adams JF, scholvinck EH, Gie RP, Potter PC, Beyers n, and Beyers AD. Decline in total serum igE after treatment for tuberculosis. lancet, 1999; 353: 2030–3.
54. suzuki n, Kudo K, sano y, and ito K. Can Mycobacterium tuberculosis infection prevent asthma and other allergic disorders? int Arch Allergy immunol, 2001; 124: 113–6.
55. Ellertsen lK, Wiker HG, Egeberg nT, and Hetland G. Allergic sensitisation in tuberculosis and leprosy patients. int Arch Allergy immunol, 2005; 138: 217–24.
56. yong AJ, Grange JM, Tee RD, Beck Js, Bothamley GH, Kemeny DM, et al. Total and anti-mycobacterial igE levels in serum from patients with tuberculosis and leprosy. Tubercle, 1989; 70: 273–9.
57. sousa AO, salem Ji, lee FK, Vercosa MC, Cruaud P, Bloom BR, et al. An epidemic of tuberculosis with a high rate of tuberculin anergy among a population previously unexposed to tuberculosis, the yanomami indians of the Brazilian Amazon. Proc natl Acad sci U s A, 1997; 94: 13227–32.
58. Wilsher Ml, Hagan C, Prestidge R, Wells AU, and Murison G. Human in vitro immune responses to Mycobacterium tuberculosis. Tuber lung Dis, 1999; 79: 371–7.
59. shirakawa T, Enomoto T, shimazu s, and Hopkin JM. The inverse association between tuberculin responses and atopic disorder. science, 1996; 275: 77–9.
60. Obihara CC, Beyers n, Gie RP, Potter PC, Marais BJ, lombard CJ, et al. inverse association between Mycobacterium tuberculosis infection and atopic rhinitis in children. Allergy, 2005; 60: 1121–5.
61. Obihara CC, Kimpen Jl, Gie RP, lill sW, Hoekstra MO, Marais BJ, et al. Mycobacterium tuberculosis infection may protect against allergy in a tuberculosis endemic area. Clin Exp Allergy, 2006; 36: 70–6.
62. Rook GA, Hamelmann E, and Rosa Brunet l. Mycobacteria and allergies. immunobiology, 2007; 212: 461–73.
63. Fiorenza G, Rateni l, Farroni MA, Bogue C, and Dlugovitzky DG. TnF-alpha, TGF-beta and nO relationship in sera from tuberculosis (TB) patients of different severity. immunol lett, 2005; 98: 45–8.
Chapter02C.3.indd 402 11/02/14 1:07 PM

403 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
64. Castro AZ, Diaz-Bardalez BM, Oliveira EC, Garcia RC, Afi une JB, Paschoal iA, et al. Abnormal production of transforming growth factor beta and interferon gamma by peripheral blood cells of patients with multidrug-resistant pulmonary tuberculosis in Brazil. J infect, 2005; 51: 318–24.
65. lee CG, Homer RJ, Zhu Z, lanone s, Wang X, Koteliansky V, et al. interleukin-13 induces tissue fibrosis by selectively stimulating and activating transforming growth factor beta(1). J Exp Med, 2001; 194: 809–21.
66. Toossi Z, Gogate P, shiratsuchi H, young T, and Ellner JJ. Enhanced production of TGF-beta by blood monocytes from patients with active tuberculosis and presence of TGF-beta in tuberculous granulomatous lung lesions. J immunol, 1995; 154: 465–73.
67. Dahl KE, shiratsuchi H, Hamilton BD, Ellner JJ, and Toossi Z. selective induction of transforming growth factor beta in human monocytes by lipoarabinomannan of Mycobacterium tuberculosis. infect immun, 1996; 64: 399–405.
68. Aung H, Wu M, Johnson Jl, Hirsch Cs, and Toossi Z. Bioactivation of latent transforming growth factor beta1 by Mycobacterium tuberculosis in human mononuclear phagocytes. scand J immunol, 2005; 61: 558–65.
69. Bonecini-Almeida MG, Ho Jl, Boechat n, Huard RC, Chitale s, Doo H, et al. Down-modulation of lung immune responses by interleukin-10 and transforming growth factor beta (TGF-beta) and analysis of TGF-beta receptors i and ii in active tuberculosis. infect immun, 2004; 72: 2628–34.
70. Hirsch Cs, Ellner JJ, Blinkhorn R, and Toossi Z. in vitro restoration of T cell responses in tuberculosis and augmentation of monocyte effector function against Mycobacterium tuberculosis by natural inhibitors of transforming growth factor beta. Proc natl Acad sci U s A, 1997; 94: 3926–31.
71. Hasan Z, Cliff JM, Dockrell HM, Jamil B, irfan M, Ashraf M, et al. CCl2 responses to Mycobacterium tuberculosis are associated with disease severity in tuberculosis. Plos One, 2009; 4: e8459.
72. Ruhwald M, Bjerregaard-Andersen M, Rabna P, Eugen-Olsen J, and Ravn P. iP-10, MCP-1, MCP-2, MCP-3, and il-1RA hold promise as biomarkers for infection with M. tuberculosis in a whole blood based T-cell assay. BMC Res notes, 2009; 2: 19.
Chapter02C.3.indd 403 11/02/14 1:07 PM

404 SECTION 2 MAin PlAyERs
73. Flores-Villanueva PO, Ruiz-Morales JA, song CH, Flores lM, Jo EK, Montano M, et al. A functional promoter polymorphism in monocyte chemoattractant protein-1 is associated with increased susceptibility to pulmonary tuberculosis. J Exp Med, 2005; 202: 1649–58.
74. Hasan Z, Jamil B, Khan J, Ali R, Khan MA, nasir n, et al. Relationship between circulating levels of iFn-gamma, il-10, CXCl9 and CCl2 in pulmonary and extrapulmonary tuberculosis is dependent on disease severity. scand J immunol, 2009; 69: 259–67.
75. Alessandri Al, souza Al, Oliveira sC, Macedo GC, Teixeira MM, and Teixeira Al. Concentrations of CXCl8, CXCl9 and sTnFR1 in plasma of patients with pulmonary tuberculosis undergoing treatment. inflamm Res, 2006; 55: 528–33.
76. szalai C, Kozma GT, nagy A, Bojszko A, Krikovszky D, szabo T, et al. Polymorphism in the gene regulatory region of MCP-1 is associated with asthma susceptibility and severity. J Allergy Clin immunol, 2001; 108: 375–81.
77. Alcais A, Fieschi C, Abel l, and Casanova Jl. Tuberculosis in children and adults: two distinct genetic diseases. J Exp Med, 2005; 202: 1617–21.
78. Buijtels PC, van de sande WW, Parkinson s, Petit Pl, van der sande MA, van soolingen D, et al. Polymorphism in CC-chemokine ligand 2 associated with tuberculosis in Zambia. int J Tuberc lung Dis, 2008; 12: 1485–8.
79. Xu ZE, Xie yy, Chen JH, Xing ll, Zhang AH, li BX, et al. Monocyte chemotactic protein-1 gene polymorphism and monocyte chemotactic protein-1 expression in Chongqing Han children with tuberculosis. Zhonghua Er Ke Za Zhi, 2009; 47: 200–3.
80. Chu sF, Tam CM, Wong Hs, Kam KM, lau yl, and Chiang AK. Association between RAnTEs functional polymorphisms and tuberculosis in Hong Kong Chinese. Genes immun, 2007; 8: 475–9.
81. Jamieson sE, Miller En, Black GF, Peacock Cs, Cordell HJ, Howson JM, et al. Evidence for a cluster of genes on chromosome 17q11-q21 controlling susceptibility to tuberculosis and leprosy in Brazilians. Genes immun, 2004; 5: 46–57.
82. Thye T, nejentsev s, intemann CD, Browne En, Chinbuah MA, Gyapong J, et al. MCP-1 promoter variant -362C associated with protection from pulmonary tuberculosis in Ghana, West Africa. Hum Mol Genet, 2009; 18: 381–8.
Chapter02C.3.indd 404 11/02/14 1:07 PM

405 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
83. Deshmane sl, Kremlev s, Amini s, and sawaya BE. Monocyte chemoattractant protein-1 (MCP-1): an overview. J interferon Cytokine Res, 2009; 29: 313–26.
84. Bruhl H, Cihak J, schneider MA, Plachy J, Rupp T, Wenzel i, et al. Dual role of CCR2 during initiation and progression of collagen-induced arthritis: evidence for regulatory activity of CCR2+ T cells. J immunol, 2004; 172: 890–8.
85. Mantovani A, sica A, sozzani s, Allavena P, Vecchi A, and locati M. The chemokine system in diverse forms of macrophage activation and polarization. Trends immunol, 2004; 25: 677–86.
86. Gu l, Tseng s, Horner RM, Tam C, loda M, and Rollins BJ. Control of TH2 polarization by the chemokine monocyte chemoattractant protein-1. nature, 2000; 404: 407–11.
87. Karpus WJ, lukacs nW, Kennedy KJ, smith Ws, Hurst sD, and Barrett TA. Differential CC chemokine-induced enhancement of T helper cell cytokine production. J immunol, 1997; 158: 4129–36.
88. nakajima H, Kobayashi M, Pollard RB, and suzuki F. Monocyte chemoattractant protein-1 enhances HsV-induced encephalomyelitis by stimulating Th2 responses. J leukoc Biol, 2001; 70: 374–80.
89. ip WK, Wong CK, and lam CW. interleukin (il)-4 and il-13 up-regulate monocyte chemoattractant protein-1 expression in human bronchial epithelial cells: involvement of p38 mitogen-activated protein kinase, extracellular signal-regulated kinase 1/2 and Janus kinase-2 but not c-Jun nH2-terminal kinase 1/2 signalling pathways. Clin Exp immunol, 2006; 145: 162–72.
90. Owen Jl, lopez DM, Grosso JF, Guthrie KM, Herbert lM, Torroella-Kouri M, et al. The expression of CCl2 by T lymphocytes of mammary tumor bearers: role of tumor-derived factors. Cell immunol, 2005; 235: 122–35.
91. sousa AR, lane sJ, nakhosteen JA, yoshimura T, lee TH, and Poston Rn. increased expression of the monocyte chemoattractant protein-1 in bronchial tissue from asthmatic subjects. Am J Respir Cell Mol Biol, 1994; 10: 142–7.
92. Braun MC, lahey E, and Kelsall Bl. selective suppression of il-12 production by chemoattractants. J immunol, 2000; 164: 3009–17.
Chapter02C.3.indd 405 11/02/14 1:07 PM

406 SECTION 2 MAin PlAyERs
93. Gu D, Chen Z, Zhao H, Du W, Xue F, Ge J, et al. T(h)1 (CXCl10) and T(h)2 (CCl2) chemokine expression in patients with immune thrombocytopenia. Hum immunol, 2010; 71(6): 586–91.
94. de nadai P, Charbonnier As, Chenivesse C, senechal s, Fournier C, Gilet J, et al. involvement of CCl18 in allergic asthma. J immunol, 2006; 176: 6286–93.
95. Prasse A and Muller-Quernheim J. non-invasive biomarkers in pulmonary fibrosis. Respirology, 2009; 14: 788–95.
96. Ferrara G, Bleck B, Richeldi l, Reibman J, Fabbri lM, Rom Wn, et al. Mycobacterium tuberculosis induces CCl18 expression in human macrophages. scand J immunol, 2008; 68: 668–74.
97. Pivarcsi A, Gombert M, Dieu-nosjean MC, lauerma A, Kubitza R, Meller s, et al. CC chemokine ligand 18, an atopic dermatitis-associated and dendritic cell-derived chemokine, is regulated by staphylococcal products and allergen exposure. J immunol, 2004; 173: 5810–7.
98. Kodera M, Hasegawa M, Komura K, yanaba K, Takehara K, and sato s. serum pulmonary and activation-regulated chemokine/CCl18 levels in patients with systemic sclerosis: a sensitive indicator of active pulmonary fibrosis. Arthritis Rheum, 2005; 52: 2889–96.
99. Rook GA, Dheda K, and Zumla A. immune responses to tuberculosis in developing countries: implications for new vaccines. nat Rev immunol, 2005; 5: 661–7.
100. Malik ZA, Denning GM, and Kusner DJ. inhibition of Ca(2+) signaling by Mycobacterium tuberculosis is Associated with Reduced Phagosome-lysosome Fusion and increased survival within Human Macrophages. J Exp Med, 2000; 191: 287–302.
101. Deretic V, singh s, Master s, Harris J, Roberts E, Kyei G, et al. Mycobacterium tuberculosis inhibition of phagolysosome biogenesis and autophagy as a host defence mechanism. Cell Microbiol, 2006; 8: 719–27.
102. Mariotti s, Teloni R, iona E, Fattorini l, Giannoni F, Romagnoli G, et al. Mycobacterium tuberculosis subverts the differentiation of human monocytes into dendritic cells. Eur J immunol, 2002; 32: 3050–8.
Chapter02C.3.indd 406 11/02/14 1:07 PM

407 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
103. Wolf AJ, linas B, Trevejo-nunez GJ, Kincaid E, Tamura T, Takatsu K, et al. Mycobacterium tuberculosis infects dendritic cells with high frequency and impairs their function in vivo. J immunol, 2007; 179: 2509–19.
104. Arko-Mensah J, Julian E, singh M, and Fernandez C. TlR2 but not TlR4 signalling is critically involved in the inhibition of iFn-gamma-induced killing of mycobacteria by murine macrophages. scand J immunol, 2007; 65: 148–57.
105. Gordon s. Alternative activation of macrophages. nat Rev immunol, 2003; 3: 23–35.
106. Kahnert A, seiler P, stein M, Bandermann s, Hahnke K, Mollenkopf H, et al. Alternative activation deprives macrophages of a coordinated defense program to Mycobacterium tuberculosis. Eur J immunol, 2006; 36: 631–47.
107. Essner R, Rhoades K, McBride WH, Morton Dl, and Economou Js. il-4 down-regulates il-1 and TnF gene expression in human monocytes. J immunol, 1989; 142: 3857–61.
108. Joyce DA and steer JH. il-4, il-10 and iFn-gamma have distinct, but interacting, effects on differentiation-induced changes in TnF-alpha and TnF receptor release by cultured human monocytes. Cytokine, 1996; 8: 49–57.
109. Rook GA. Th2 cytokines in susceptibility to tuberculosis. Curr Mol Med, 2007; 7: 327–37.
110. Hernandez-Garay M and Mendez-samperio P. Transforming growth factor-beta decreases survival of Mycobacterium bovis-activated T cells. Arch Med Res, 2003; 34: 20–5.
111. Mendez-samperio P, Hernandez-Garay M, and Garcia-Martinez E. induction of apoptosis in bacillus Calmette-Guerin-activated T cells by transforming growth factor-beta. Cell immunol, 2000; 202: 103–12.
112. Hirsch Cs, Johnson Jl, Okwera A, Kanost RA, Wu M, Peters P, et al. Mechanisms of apoptosis of T-cells in human tuberculosis. J Clin immunol, 2005; 25: 353–64.
113. Hirsch Cs, yoneda T, Averill l, Ellner JJ, and Toossi Z. Enhancement of intracellular growth of Mycobacterium tuberculosis in human monocytes by transforming growth factor-beta 1. J infect Dis, 1994; 170: 1229–37.
Chapter02C.3.indd 407 11/02/14 1:07 PM

408 SECTION 2 MAin PlAyERs
114. Harris J, De Haro sA, Master ss, Keane J, Roberts EA, Delgado M, et al. T helper 2 cytokines inhibit autophagic control of intracellular Mycobacterium tuberculosis. immunity, 2007; 27: 505–17.
115. Chen Ml, Pittet MJ, Gorelik l, Flavell RA, Weissleder R, von Boehmer H, et al. Regulatory T cells suppress tumor-specific CD8 T cell cytotoxicity through TGF-beta signals in vivo. Proc natl Acad sci U s A, 2005; 102: 419–24.
116. Olver s, Groves P, Buttigieg K, Morris Es, Janas Ml, Kelso A, et al.Tumor-derived interleukin-4 reduces tumor clearance and deviates the cytokine and granzyme profile of tumor-induced CD8+ T cells. Cancer Res, 2006; 66: 571–80.
117. Khazaie K and von Boehmer H. The impact of CD4+CD25+ Treg on tumor specific CD8+ T cell cytotoxicity and cancer. semin Cancer Biol, 2006; 16: 124–36.
118. Wangoo A, sparer T, Brown in, snewin VA, Janssen R, Thole J, et al. Contribution of Th1 and Th2 Cells to Protection and Pathology in Experimental Models of Granulomatous lung Disease. J immunol, 2001; 166: 3432–9.
119. Keane J, Gershon s, Wise RP, Mirabile-levens E, Kasznica J, schwieterman WD, et al. Tuberculosis associated with infliximab, a tumor necrosis factor alpha-neutralizing agent. n Engl J Med, 2001; 345: 1098–104.
120. Tramontana JM, Utaipat U, Molloy A, Akarasewi P, Burroughs M, Makonkawkeyoon s, et al.Thalidomide treatment reduces tumor necrosis factor alpha production and enhances weight gain in patients with pulmonary tuberculosis. Mol Med, 1995, 1: 384–97.
121. lawrence CE, Paterson JC, Higgins lM, MacDonald TT, Kennedy MW, and Garside P. il-4-regulated enteropathy in an intestinal nematode infection. Eur J immunol, 1998; 28: 2672–84.
122. Wynn TA, Cheever AW, Jankovic D, Poindexter RW, Caspar P, lewis FA, et al. An il-12-based vaccination method for preventing fibrosis induced by schistosome infection. nature, 1995; 376: 594–6.
123. Pina A, Valente-Ferreira RC, Molinari-Madlum EE, Vaz CA, Keller AC, and Calich Vl. Absence of interleukin-4 determines less severe pulmonary paracoccidioidomycosis associated with impaired Th2 response. infect immun, 2004; 72: 2369–78.
Chapter02C.3.indd 408 11/02/14 1:07 PM

409 CHAPTER 2C.3TB IN DEVELOPING COUNTRIES DUE TO HIGH-DOSE CHALLENGE IN PARTIALLY IMMUNE INDIVIDUALS
124. Kotowicz K, Callard RE, Friedrich K, Matthews DJ, and Klein n. Biological activity of il-4 and il-13 on human endothelial cells: functional evidence that both cytokines act through the same receptor. int immunol, 1996; 8: 1915–25.
125. iademarco MF, Barks Jl, and Dean DC. Regulation of vascular cell adhesion molecule-1 expression by il-4 and TnF-alpha in cultured endothelial cells. J Clin invest, 1995; 95: 264–71.
126. Kaushal D, schroeder BG, Tyagi s, yoshimatsu T, scott C, Ko C, et al. Reduced immunopathology and mortality despite tissue persistence in a Mycobacterium tuberculosis mutant lacking alternative sigma factor, sigH. Proc natl Acad sci U s A, 2002; 99: 8330–5.
127. leung Dy and szefler sJ. new insights into steroid resistant asthma. Pediatr Allergy immunol, 1998; 9: 3–12.
128. Baker RW, Walker BR, shaw RJ, Honour JW, Jessop Ds, lightman sl, et al. increased cortisol-cortisone ratio in acute pulmonary tuberculosis. Am J Respir Crit Care Med, 2000; 162: 1641–7.
129. van Crevel R, Karyadi E, Preyers F, leenders M, Kullberg BJ, nelwan RH, et al. increased Production of interleukin 4 by CD4+ and CD8+ T Cells from Patients with Tuberculosis is Related to the Presence of Pulmonary Cavities. J infect Dis, 2000; 181: 1194–7.
130. Garton nJ, Waddell sJ, sherratt Al, lee sM, smith RJ, senner C, et al. Cytological and transcript analyses reveal fat and lazy persister-like bacilli in tuberculous sputum. Plos Med, 2008; 5: e75.
131. Golub JE, Cronin WA, Obasanjo OO, Coggin W, Moore K, Pope Ds, et al. Transmission of Mycobacterium tuberculosis through casual contact with an infectious case. Arch intern Med, 2001; 161: 2254–8.
Chapter02C.3.indd 409 11/02/14 1:07 PM