Embed Size (px)
Citation preview

Chapter 58Coronal Polish
Chapter 58Coronal Polish
Copyright 2003, Elsevier Science (USA).
All rights reserved. No part of this product may be reproduced or transmitted in any form or by any means, electronic or mechanical, including input into or storage in any information system, without permission in writing from the publisher.
PowerPoint® presentation slides may be displayed and may be reproduced in print form for instructional purposes only, provided a proper copyright notice appears on the last page of each print-out.
Produced in the United States of America
ISBN 0-7216-9770-4

Copyright 2003, Elsevier Science (USA). All rights reserved.
IntroductionIntroduction A technique used to remove plaque and
stains from the coronal surfaces of the teeth. A dental handpiece, a rubber cup, and an abrasive agent are used.
In some states, coronal polishing is delegated to registered or expanded-function dental assistants who have had special training in this procedure. Coronal polishing is strictly limited to the clinical crowns of the teeth. A coronal polish is NOT a substitute for an oral prophylaxis.
A technique used to remove plaque and stains from the coronal surfaces of the teeth. A dental handpiece, a rubber cup, and an abrasive agent are used.
In some states, coronal polishing is delegated to registered or expanded-function dental assistants who have had special training in this procedure. Coronal polishing is strictly limited to the clinical crowns of the teeth. A coronal polish is NOT a substitute for an oral prophylaxis.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Selective PolishingSelective Polishing Selective polishing is a procedure in which
only those teeth or surfaces with stain are polished.
The purpose of selective polishing is to avoid removing even small amounts of the surface enamel unnecessarily.
For some individuals, stain removal may cause dentinal hypersensitivity during and after the appointment.
Selective polishing is a procedure in which only those teeth or surfaces with stain are polished.
The purpose of selective polishing is to avoid removing even small amounts of the surface enamel unnecessarily.
For some individuals, stain removal may cause dentinal hypersensitivity during and after the appointment.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Benefits of Coronal PolishingBenefits of Coronal PolishingFluoride is better accepted into the enamel.Polishing prepares the teeth for placement of dental sealants.
Smooth tooth surfaces are easier for the patient to keep clean.
Formation of new deposits is slowed.Patients appreciate the smooth feeling and clean appearance.
Polishing prepares the teeth for placement of orthodontic brackets and/or bands.
Fluoride is better accepted into the enamel.Polishing prepares the teeth for placement of dental sealants.
Smooth tooth surfaces are easier for the patient to keep clean.
Formation of new deposits is slowed.Patients appreciate the smooth feeling and clean appearance.
Polishing prepares the teeth for placement of orthodontic brackets and/or bands.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Dental StainsDental Stains Stains of the teeth occur in three basic ways:
• Stain adheres directly to the surface of the tooth.
• Stain can be embedded in calculus and plaque deposits.
• Stain is incorporated within the tooth structure.
Before coronal polishing is undertaken to remove stains, it is important to distinguish between extrinsic and intrinsic stains.
Stains of the teeth occur in three basic ways:
• Stain adheres directly to the surface of the tooth.
• Stain can be embedded in calculus and plaque deposits.
• Stain is incorporated within the tooth structure.
Before coronal polishing is undertaken to remove stains, it is important to distinguish between extrinsic and intrinsic stains.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Extrinsic Stains Extrinsic Stains Occur on the external surfaces of the teeth
and may be removed by scaling and/or polishing.
Extrinsic stains are caused by certain substances such as tobacco, coffee, tea, red wine, certain drugs, and chromogenic (color-producing) bacteria.
Occur on the external surfaces of the teeth and may be removed by scaling and/or polishing.
Extrinsic stains are caused by certain substances such as tobacco, coffee, tea, red wine, certain drugs, and chromogenic (color-producing) bacteria.

Copyright 2003, Elsevier Science (USA). All rights reserved.
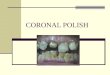
Fig. 58-1 A, Yellow and brown stain and marginal plaque.Fig. 58-1 A, Yellow and brown stain and marginal plaque.
Fig. 58-1 AFig. 58-1 A

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-1 B, Moderate tobacco stain on the lingual surfaces.Fig. 58-1 B, Moderate tobacco stain on the lingual surfaces.
Fig. 58-1 BFig. 58-1 B

Copyright 2003, Elsevier Science (USA). All rights reserved.
Intrinsic Stains Intrinsic Stains An internal discoloration of the tooth that
may be caused by exposure to medicine (e.g., tetracycline or excessive fluoride ingestion), or other causes during tooth development.
The dental assistant must be able to recognize these conditions because these stains cannot be removed by polishing or scaling.
An internal discoloration of the tooth that may be caused by exposure to medicine (e.g., tetracycline or excessive fluoride ingestion), or other causes during tooth development.
The dental assistant must be able to recognize these conditions because these stains cannot be removed by polishing or scaling.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-2 Intrinsic discoloration.Fig. 58-2 Intrinsic discoloration.
Fig. 58-2Fig. 58-2

Copyright 2003, Elsevier Science (USA). All rights reserved.
Methods of Removing Plaque and StainMethods of Removing Plaque and Stain
Air-powder polishing
• The air-powder polishing technique uses a specially designed handpiece with a nozzle that delivers a high-pressure stream of warm water and sodium bicarbonate.
Rubber cup polishing
• The most common technique for removing stains and plaque and polishing the teeth.
• A rubber polishing cup is rotated slowly and carefully by a prophy angle attached to the slow-speed handpiece.
Air-powder polishing
• The air-powder polishing technique uses a specially designed handpiece with a nozzle that delivers a high-pressure stream of warm water and sodium bicarbonate.
Rubber cup polishing
• The most common technique for removing stains and plaque and polishing the teeth.
• A rubber polishing cup is rotated slowly and carefully by a prophy angle attached to the slow-speed handpiece.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Rotary Equipment for Coronal PolishingRotary Equipment for Coronal Polishing Polishing cups
• Soft, webbed polishing cups are used to clean and polish the smooth surfaces of the teeth. The polishing cup attaches to the reusable prophy angle by either a snap-on or screw-on attachment.
Prophylaxis angle • Commonly called a prophy angle, attaches to the
slow-speed handpiece. • The reusable prophy angle must be properly
cleaned and sterilized after each use.• A disposable angle is discarded after a single
use.
Polishing cups • Soft, webbed polishing cups are used to clean and
polish the smooth surfaces of the teeth. The polishing cup attaches to the reusable prophy angle by either a snap-on or screw-on attachment.
Prophylaxis angle • Commonly called a prophy angle, attaches to the
slow-speed handpiece. • The reusable prophy angle must be properly
cleaned and sterilized after each use.• A disposable angle is discarded after a single
use.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Bristle BrushesBristle Brushes Bristle brushes are made from either
natural or synthetic materials and may be used to remove stains from deep pits and fissures of the enamel surfaces.
Bristle brushes can cause severe gingival lacerations and must be used with special care.
Brushes are not recommended for use on exposed cementum or dentin because these surfaces are soft and are easily grooved.
Bristle brushes are made from either natural or synthetic materials and may be used to remove stains from deep pits and fissures of the enamel surfaces.
Bristle brushes can cause severe gingival lacerations and must be used with special care.
Brushes are not recommended for use on exposed cementum or dentin because these surfaces are soft and are easily grooved.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Abrasives Abrasives Dental abrasives (polishing materials) are used
to remove stain and to polish natural teeth, prosthetic appliances, restorations, and castings.
Abrasives are available in extra coarse, coarse, medium, fine, and extra fine. The coarser the agent, the more abrasive the surface.
Even a fine-grit agent removes small amounts of the enamel surface.
The goal is to always use the abrasive agent that will produce the least amount of abrasion to the tooth surface.
Dental abrasives (polishing materials) are used to remove stain and to polish natural teeth, prosthetic appliances, restorations, and castings.
Abrasives are available in extra coarse, coarse, medium, fine, and extra fine. The coarser the agent, the more abrasive the surface.
Even a fine-grit agent removes small amounts of the enamel surface.
The goal is to always use the abrasive agent that will produce the least amount of abrasion to the tooth surface.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Factors That Influence Rate of AbrasionFactors That Influence Rate of Abrasion
The more agent used, the greater the degree of abrasion.
The lighter the pressure, the less abrasion.
The slower the rotation of the cup, the less abrasion.
The more agent used, the greater the degree of abrasion.
The lighter the pressure, the less abrasion.
The slower the rotation of the cup, the less abrasion.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Polishing StrokesPolishing Strokes Fill the polishing cup with the polishing agent and
spread it over several teeth in the areas to be polished.
Establish a finger rest, and place the cup almost in contact with the tooth.
The stroke should be from the gingival third toward the incisal third of the tooth.
Use the slowest speed, and then apply the revolving cup lightly to the tooth surface for 1 to 2 seconds.
Use light pressure to make the edges of the polishing cup flare slightly.
Use a patting, wiping motion and an overlapping stroke.
Fill the polishing cup with the polishing agent and spread it over several teeth in the areas to be polished.
Establish a finger rest, and place the cup almost in contact with the tooth.
The stroke should be from the gingival third toward the incisal third of the tooth.
Use the slowest speed, and then apply the revolving cup lightly to the tooth surface for 1 to 2 seconds.
Use light pressure to make the edges of the polishing cup flare slightly.
Use a patting, wiping motion and an overlapping stroke.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-5 Use overlapping strokes to ensure complete coverage of the tooth. Fig. 58-5 Use overlapping strokes to ensure complete coverage of the tooth.
Fig. 58-5Fig. 58-5

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-6 Stroke from the gingival third with just sufficient pressure to make the cup flare.Fig. 58-6 Stroke from the gingival third with just sufficient pressure to make the cup flare.
Fig. 58-6Fig. 58-6

Copyright 2003, Elsevier Science (USA). All rights reserved.
Positioning the PatientPositioning the Patient Adjust the dental chair so that the patient is
approximately parallel to the floor with the back of the chair raised slightly.
Adjust the headrest for patient comfort and operator visibility.
For the mandibular arch, position the patient's head with the chin down. When the mouth is open, the lower jaw should be parallel to the floor.
For access to the maxillary arch, position the patient's head with the chin up.
Adjust the dental chair so that the patient is approximately parallel to the floor with the back of the chair raised slightly.
Adjust the headrest for patient comfort and operator visibility.
For the mandibular arch, position the patient's head with the chin down. When the mouth is open, the lower jaw should be parallel to the floor.
For access to the maxillary arch, position the patient's head with the chin up.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-3 Disposable handpiece.Fig. 58-3 Disposable handpiece.
Fig. 58-3Fig. 58-3

Copyright 2003, Elsevier Science (USA). All rights reserved.
The Handpiece GraspThe Handpiece Grasp The handpiece and prophylaxis angle are
held in a pen grasp with the handle resting in the V-shaped area of the hand between the thumb and index finger.
A proper grasp is important because if the grasp is not secure and comfortable, the weight and balance of the handpiece can cause hand and wrist fatigue.
The handpiece and prophylaxis angle are held in a pen grasp with the handle resting in the V-shaped area of the hand between the thumb and index finger.
A proper grasp is important because if the grasp is not secure and comfortable, the weight and balance of the handpiece can cause hand and wrist fatigue.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-4 Handpiece grasp.Fig. 58-4 Handpiece grasp.
Fig. 58-4Fig. 58-4

Copyright 2003, Elsevier Science (USA). All rights reserved.
Handpiece OperationHandpiece Operation The rheostat (foot pedal) controls the speed
(rpm) of the handpiece.
The toe of the foot is used to activate the rheostat. The sole of the foot remains flat on the floor.
Apply a steady pressure with the toe on the rheostat to produce a slow, even speed.
Use a low-speed handpiece that operates to a maximum of 20,000 rpm.
Release the rheostat to prevent debris from splattering when the handpiece is removed from the tooth for more than a moment.
The rheostat (foot pedal) controls the speed (rpm) of the handpiece.
The toe of the foot is used to activate the rheostat. The sole of the foot remains flat on the floor.
Apply a steady pressure with the toe on the rheostat to produce a slow, even speed.
Use a low-speed handpiece that operates to a maximum of 20,000 rpm.
Release the rheostat to prevent debris from splattering when the handpiece is removed from the tooth for more than a moment.

Copyright 2003, Elsevier Science (USA). All rights reserved.
The Fulcrum/Finger RestThe Fulcrum/Finger Rest The fulcrum provides stability for the operator
and must be placed in such a way as to allow for movement of the wrist and forearm.
The fulcrum is repositioned throughout the procedure as necessary.
The fulcrum may be either intraoral or extraoral, depending on a variety of circumstances such as:
• The presence or absence of teeth.• The area of the mouth being polished.• How wide the patient can open the mouth.
The fulcrum provides stability for the operator and must be placed in such a way as to allow for movement of the wrist and forearm.
The fulcrum is repositioned throughout the procedure as necessary.
The fulcrum may be either intraoral or extraoral, depending on a variety of circumstances such as:
• The presence or absence of teeth.• The area of the mouth being polished.• How wide the patient can open the mouth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Positioning of the OperatorPositioning of the Operator The operator's feet should be flat on the floor with
the thighs parallel to the floor.
The operator's arms should be at waist level and even with the patient's mouth.
When performing a coronal polish procedure, the right-handed operator generally begins by being seated at the 8 to 9 o'clock position.
When performing a coronal polish procedure, the left-handed operator generally begins by being seated at the 3 to 4 o'clock position.
The operator's feet should be flat on the floor with the thighs parallel to the floor.
The operator's arms should be at waist level and even with the patient's mouth.
When performing a coronal polish procedure, the right-handed operator generally begins by being seated at the 8 to 9 o'clock position.
When performing a coronal polish procedure, the left-handed operator generally begins by being seated at the 3 to 4 o'clock position.

Copyright 2003, Elsevier Science (USA). All rights reserved.
The Sequence of PolishingThe Sequence of Polishing The full mouth coronal polishing must be
done in a predetermined sequence to be certain that no area is missed.
The best sequence is based on the operator's preference and the individual needs of the patient.
The positions and fulcrums described in the following slides are for a right-handed operator.
The full mouth coronal polishing must be done in a predetermined sequence to be certain that no area is missed.
The best sequence is based on the operator's preference and the individual needs of the patient.
The positions and fulcrums described in the following slides are for a right-handed operator.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-7 Setup for coronal polishing.Fig. 58-7 Setup for coronal polishing.
Fig. 58-7Fig. 58-7

Copyright 2003, Elsevier Science (USA). All rights reserved.
Patient PreparationPatient Preparation Check the patient's medical history for any
contraindications to the coronal polish procedure.
Seat and drape the patient with a waterproof napkin. Ask the patient to remove any dental prosthetic appliance he or she may be wearing. Provide the patient with protective eyewear.
Explain the procedure to the patient and answer any questions.
Inspect oral cavity for lesions, missing teeth, tori, and so on.
Apply a disclosing agent to identify areas of plaque.
Check the patient's medical history for any contraindications to the coronal polish procedure.
Seat and drape the patient with a waterproof napkin. Ask the patient to remove any dental prosthetic appliance he or she may be wearing. Provide the patient with protective eyewear.
Explain the procedure to the patient and answer any questions.
Inspect oral cavity for lesions, missing teeth, tori, and so on.
Apply a disclosing agent to identify areas of plaque.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-8 Application of disclosing agent.Fig. 58-8 Application of disclosing agent.
Fig. 58-8Fig. 58-8

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Right Posterior Quadrant, Buccal Aspect Maxillary Right Posterior Quadrant, Buccal Aspect Sit in the 8 to 9 o'clock position.
Have the patient tilt his head up and turn slightly away from you.
Hold the dental mirror in your left hand. Use it to retract the cheek or for indirect vision of the more posterior teeth.
Establish a fulcrum on the maxillary right incisors.
Sit in the 8 to 9 o'clock position.
Have the patient tilt his head up and turn slightly away from you.
Hold the dental mirror in your left hand. Use it to retract the cheek or for indirect vision of the more posterior teeth.
Establish a fulcrum on the maxillary right incisors.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-9 Polishing the buccal surfaces of the maxillary right quadrant.Fig. 58-9 Polishing the buccal surfaces of the maxillary right quadrant.
Fig. 58-9Fig. 58-9

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Right Posterior Quadrant, Lingual Aspect Maxillary Right Posterior Quadrant, Lingual Aspect Remain seated in the 8 to 9 o'clock
position.
Have the patient turn his head up and toward you.
Hold the dental mirror in your left hand. Direct vision in this position and the mirror provides a view of the distal surfaces.
Establish a fulcrum on the lower incisors and reach up to polish the lingual surfaces.
Remain seated in the 8 to 9 o'clock position.
Have the patient turn his head up and toward you.
Hold the dental mirror in your left hand. Direct vision in this position and the mirror provides a view of the distal surfaces.
Establish a fulcrum on the lower incisors and reach up to polish the lingual surfaces.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Anterior Teeth, Facial Aspect Maxillary Anterior Teeth, Facial Aspect
Remain in the 8 to 9 o'clock position.
Position the patient's head tipped up slightly and facing straight-ahead. Make necessary adjustments by turning the patient's head slightly either toward or away from you.
Use direct vision in this area.
Establish a fulcrum on the incisal edge of the teeth adjacent to the ones being polished.
Remain in the 8 to 9 o'clock position.
Position the patient's head tipped up slightly and facing straight-ahead. Make necessary adjustments by turning the patient's head slightly either toward or away from you.
Use direct vision in this area.
Establish a fulcrum on the incisal edge of the teeth adjacent to the ones being polished.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-10 Polishing the facial surfaces of the maxillary anterior teeth. Fig. 58-10 Polishing the facial surfaces of the maxillary anterior teeth.
Fig. 58-10Fig. 58-10

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Anterior Teeth, Lingual Aspect Maxillary Anterior Teeth, Lingual Aspect
Remain in the 8 to 9 o'clock position or move to the 11 to 12 o'clock position.
Position the patient's head so it is tipped slightly upward.
Use the mouth mirror for indirect vision and to reflect light on the area.
Establish a fulcrum on the incisal edge of the teeth adjacent to the ones being polished.
Remain in the 8 to 9 o'clock position or move to the 11 to 12 o'clock position.
Position the patient's head so it is tipped slightly upward.
Use the mouth mirror for indirect vision and to reflect light on the area.
Establish a fulcrum on the incisal edge of the teeth adjacent to the ones being polished.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-11 Polishing the lingual surfaces of the maxillary anterior teeth.Fig. 58-11 Polishing the lingual surfaces of the maxillary anterior teeth.
Fig. 58-11Fig. 58-11

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Left Posterior Quadrant, Buccal AspectMaxillary Left Posterior Quadrant, Buccal Aspect Sit in the 9 o'clock position.
Position the patient's head tipped upward and turned slightly toward you to improve visibility.
Use the mirror to retract the cheek and for indirect vision.
Rest your fulcrum finger on the buccal occlusal surface of the teeth toward the front of the quadrant.
Alternative: Rest your fulcrum finger on the lower premolars and reach up to the maxillary posterior teeth.
Sit in the 9 o'clock position.
Position the patient's head tipped upward and turned slightly toward you to improve visibility.
Use the mirror to retract the cheek and for indirect vision.
Rest your fulcrum finger on the buccal occlusal surface of the teeth toward the front of the quadrant.
Alternative: Rest your fulcrum finger on the lower premolars and reach up to the maxillary posterior teeth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Maxillary Left Posterior Quadrant, Lingual AspectMaxillary Left Posterior Quadrant, Lingual Aspect Remain in the 8 to 9 o'clock position.
Have the patient turn his head away from you.
Use direct vision in this position. Hold the mirror in your left hand and use for a combination of retraction and reflecting light.
Establish a fulcrum on the buccal surfaces of the maxillary left posterior teeth or on the occlusal surfaces of the mandibular left teeth.
Remain in the 8 to 9 o'clock position.
Have the patient turn his head away from you.
Use direct vision in this position. Hold the mirror in your left hand and use for a combination of retraction and reflecting light.
Establish a fulcrum on the buccal surfaces of the maxillary left posterior teeth or on the occlusal surfaces of the mandibular left teeth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Left Posterior Quadrant, Buccal Aspect Mandibular Left Posterior Quadrant, Buccal Aspect
Sit in the 8 to 9 o'clock position.
Have the patient turn his head slightly toward you.
Use the mirror to retract the cheek and for indirect vision of distal and buccal surfaces.
Establish a fulcrum on the incisal surfaces of the mandibular left anterior teeth and reach back to the posterior teeth.
Sit in the 8 to 9 o'clock position.
Have the patient turn his head slightly toward you.
Use the mirror to retract the cheek and for indirect vision of distal and buccal surfaces.
Establish a fulcrum on the incisal surfaces of the mandibular left anterior teeth and reach back to the posterior teeth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Left Posterior Quadrant, Lingual Aspect Mandibular Left Posterior Quadrant, Lingual Aspect
Remain in the 9 o'clock position.
Have the patient turn his head slightly away from you.
For direct vision, use the mirror to retract the tongue and reflect more light to the working area.
Establish a fulcrum on the mandibular anterior teeth and reach back to the posterior teeth.
Remain in the 9 o'clock position.
Have the patient turn his head slightly away from you.
For direct vision, use the mirror to retract the tongue and reflect more light to the working area.
Establish a fulcrum on the mandibular anterior teeth and reach back to the posterior teeth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-12 Polishing the lingual surfaces of the mandibular left quadrant.Fig. 58-12 Polishing the lingual surfaces of the mandibular left quadrant.
Fig. 58-12Fig. 58-12

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Anterior Teeth, Facial Aspect Mandibular Anterior Teeth, Facial Aspect Sit in either the 8 to 9 o'clock position or in the 11
to 12 o'clock position.
As necessary, instruct the patient to make adjustments in his head position by turning either toward or away from you or by tilting his head up or down.
Use your left index finger to retract the lower lip. Both direct and indirect vision can be used in this area.
Establish a fulcrum on the incisal edges of the teeth adjacent to the ones being polished.
Sit in either the 8 to 9 o'clock position or in the 11 to 12 o'clock position.
As necessary, instruct the patient to make adjustments in his head position by turning either toward or away from you or by tilting his head up or down.
Use your left index finger to retract the lower lip. Both direct and indirect vision can be used in this area.
Establish a fulcrum on the incisal edges of the teeth adjacent to the ones being polished.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Anterior Teeth, Lingual Aspect Mandibular Anterior Teeth, Lingual Aspect Sit in either the 8 to 9 o'clock position or at the 11 to
12 o'clock position.
As necessary, instruct the patient to make adjustments in his head position by turning either toward or away from you or by tilting his head up or down.
Use the mirror for indirect vision, to retract the tongue, and to reflect light onto the teeth. Direct vision is often used in this area when the operator is seated in the 12 o’clock position, but indirect vision can also be helpful.
Establish a fulcrum on the mandibular cuspid incisal area.
Sit in either the 8 to 9 o'clock position or at the 11 to 12 o'clock position.
As necessary, instruct the patient to make adjustments in his head position by turning either toward or away from you or by tilting his head up or down.
Use the mirror for indirect vision, to retract the tongue, and to reflect light onto the teeth. Direct vision is often used in this area when the operator is seated in the 12 o’clock position, but indirect vision can also be helpful.
Establish a fulcrum on the mandibular cuspid incisal area.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-13 Polishing the lingual surfaces of the mandibular anterior teeth.Fig. 58-13 Polishing the lingual surfaces of the mandibular anterior teeth.
Fig. 58-13Fig. 58-13

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Right Quadrant, BuccalAspectMandibular Right Quadrant, BuccalAspect
Sit in the 8 o'clock position.
Have the patient turn his head slightly away from you .
Use the mirror to retract tissue and reflect light. The mirror may also be used to view the distal surfaces in this area.
Establish a fulcrum on the lower incisors.
Sit in the 8 o'clock position.
Have the patient turn his head slightly away from you .
Use the mirror to retract tissue and reflect light. The mirror may also be used to view the distal surfaces in this area.
Establish a fulcrum on the lower incisors.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Fig. 58-14 Polishing the mandibular right quadrant, buccal aspect.Fig. 58-14 Polishing the mandibular right quadrant, buccal aspect.
Fig. 58-14Fig. 58-14

Copyright 2003, Elsevier Science (USA). All rights reserved.
Mandibular Right Quadrant, Lingual AspectMandibular Right Quadrant, Lingual Aspect
Remain in the 8 o'clock position.
Have the patient turn his head slightly toward you.
Retract the tongue with the mirror.
Establish a fulcrum on the lower incisors.
Remain in the 8 o'clock position.
Have the patient turn his head slightly toward you.
Retract the tongue with the mirror.
Establish a fulcrum on the lower incisors.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Flossing After Coronal PolishingFlossing After Coronal Polishing Dental floss and tape have two purposes after coronal
polishing.
• The first is to polish the interproximal tooth surfaces.
• The second is to remove any abrasive agent or debris that may be lodged in the contact area.
Place abrasive on the contact area between the teeth, and work the floss or tape through the contact area with a back-and-forth motion.
A floss threader can be used to pass the floss under any fixed bridgework to gain access to the abutment teeth.
Dental floss and tape have two purposes after coronal polishing.
• The first is to polish the interproximal tooth surfaces.
• The second is to remove any abrasive agent or debris that may be lodged in the contact area.
Place abrasive on the contact area between the teeth, and work the floss or tape through the contact area with a back-and-forth motion.
A floss threader can be used to pass the floss under any fixed bridgework to gain access to the abutment teeth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Evaluation of PolishingEvaluation of Polishing There is no remaining disclosing agent on
any of the tooth surfaces.
The teeth are glossy and reflect light from the mirror uniformly.
There is no evidence of trauma to the gingival margins or any other soft tissues in the mouth.
There is no remaining disclosing agent on any of the tooth surfaces.
The teeth are glossy and reflect light from the mirror uniformly.
There is no evidence of trauma to the gingival margins or any other soft tissues in the mouth.

Copyright 2003, Elsevier Science (USA). All rights reserved.
Patient InstructionsPatient Instructions Most patients are self-conscious about
stains on their teeth and appreciate any tips you can give them as to how to they can keep their teeth as white as possible.
It is important to educate patients about the cause of stains.
When the stains are intrinsic, the dentist may want you to discuss possible cosmetic dental care options to satisfy their desire for attractive and stain-free teeth.
Most patients are self-conscious about stains on their teeth and appreciate any tips you can give them as to how to they can keep their teeth as white as possible.
It is important to educate patients about the cause of stains.
When the stains are intrinsic, the dentist may want you to discuss possible cosmetic dental care options to satisfy their desire for attractive and stain-free teeth.
![MSK CT PROTOCOL[2] - jefferson.edu · AC joint. SHOULDER Coronal Imaging Plane Coronal Imaging Plane •Prescribe coronal plane off of axial images parallel to supraspinatus muscle](https://img.pdfslide.us/doc/110x75/5d645f8588c9930e728b6075/msk-ct-protocol2-ac-joint-shoulder-coronal-imaging-plane-coronal-imaging.jpg)