-
Chapter 5 - Mechanisms of Injury Physical process responsible
for a given action, reaction or result
-
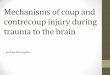
Why is it necessary to determine the mechanism of
injuries?Important for the diagnosis, rehabilitation and prevention
of injuries
-
Injury MechanismDepends persons perspectiveMechanism often acts
in combinationEstablish cause and effect relationshipSport medicine
classificationContact or impactdynamic overloadoverusestructural
vulnerabilityinflexibilitymuscle inbalancerapid growth
-
Mechanical LoadingLoads greater than physiological lead to
injuriesChronic injuriescumulative traumarepetitive stressAcute
injuries
-
Principles of InjuriesCatch-all termsshinsplintstennis
elbowjumpers kneeLevel of dysfunctioncatastrophic
injuriesProgressionuntreated or lack to time to heal lead to more
severe injuries
-
Assessment of SeverityClinical classificationshelp assign common
characteristics to injuriesSeverity linked to amount of tissue
damageMild & moderate: partial disruption, tissue is able to
accept loads
Ligamentsgrade 1 mildnegligible structuralminimal time lossgrade
2 moderatepartial ruptureswelling tendernessup to 6 wk timegrade 3
severecomplete, gross swelling, 8 wk min
-
Injury PrinciplesMicro vs macrotraumaPrimary: direct consequence
of traumaSecondaryinjury surface after original traumaaccommodation
to primary injury (adaptation of loads)Tissue structure
-
Contributing factorsAgeacute injuries: youngchronic:
olderGenderGeneticsFitness levelNutritionPsychologicalHuman
interactionFatiguephysical & mentalEnvironment
Equipmentprotectivecontributes to injuriesPrevious
injuryDiseaseDrugsRehabilitationAnthropometricsSkill
levelExperiencePain
-
Tissue InjuryInflammation: pathological processvascular
responseincrease capillary permeability (swelling)Pain: swelling
related pressure on nerve endings (more in confined spaces)
-
Tissue InjuryVasodilatory phaseflow of fluid/plasma proteins
into tissuePlasma proteinsfibrinogenFunctionsdilutes &
inactivates toxinsnutrients to inflammatory cellsantibodies,
proteins
Control of inflammationChemicals mediatorshistamine, serotonin,
bradykin, prostagladins, plasmin etc.Other CellsPhagocytes (fungal
and bacterial infection)Lymphocytes (antigens)
-
Why inflammation?Bodys first line of defense against
injuries
-
BoneAny conditions that affects osteocyte
performanceOsteonecrosis: cessation of blood flowvessel
disruptionocclussioninjury or pressure to arterial walls matrix,
bone strength likelihood of fracture
-
BoneOsteoporosisMajor public health issueAffect mostly
trabercular boneBone of axial skeletonMultifactorClinical
conditions
-
BoneFracture (break): applied loads exceeds bones ability
Resistancematerial propertiesgeometryanisotropic
effectsporosityType of loadingacute vs chronic
-
FracturesIndirect or directRisk and type of
boneDiagnosissiteextent of injuryconfigurationfragments
(displaced)environmental (open closed)complicationsetiological
-
FracturesHealing phases:inflammationunion of bony ends
(3wk)callus remodeling (6 wks)
-
Articular CartilageExcessive loadingloss of cartilage
matrixchondral fracturesosteochondral fractureInability to
repair
-
Articular CartilageAOnon inflammatoryweight bearing
jointsdeterioration of ACosteophytes formationcartilage
fibrillationArtificial Jointscemented or non
-
FibrocartilageDistributes forces at jointsShock absorberImprove
joint fitmenisciintervertebral disks
-
TendonForce transferInjuriesdirect (cuts)indirect (excessive
loads applied to unit)Musculotendinous injuries: StrainMild,
moderate, severesevere: precede by microdamage
-
TendonRepetitive overloading: inflammatory response or
tendinitisAlso could affect tendon sheath, peritenon
etc.HealingInflammationSynthesis of collagen and GAG (matrix)Cyclic
loading (2-3 wk)Progressive stress
PeritenonitisTendinosis (intratendinous degeneration dut ot
atrophy)Tendinitis (Symptomatic degeneration vascular disruption
and inflammation
-
LigamentsLigament injuriessprainpartial tearscomplete
tearsHealingbleeding & inflammation (fibrin, fibroblas scar
cells)proliferation of building material (scar tissue)matrix
remodeling smaller fiberslack organization
-
Muscle InjuriesAcute muscular strainoverstreching or
overloadingforce, rate, applicationmoderate:partial tearsevere:
complete tear, hemorrage, swellingcontusionsintramuscular
bleedingmyositis ossificansexercise induced injuryDOMS 24-72 hr
after exerciseeccentric
-
SkinAbrasionsContusionsPenetrating woundsobscure deeper
damageLacerationsInfectionExcessive bleeding
-
Nervous tissueNot musculoskeletalGreatest potential for
dysfunctionInjurieschemicalthermalischemicmechanicalentrapment
trauma: compressive or tensileTemporary or complete axonal
discontinuityMotor impairment can lead to secondary injuries
-
Nervous Tissue
Degree
Mechanism
Effect
First degree
Low compression or acute high compression
Conduction block, no axonal discontinuity
Second degree
Pinching or crunching
Prolonged pressure
Axonal interruption, wallerian degeneration, nerve supporting
structure intact (recovery ok)
Third degree
Any of the above
Loss of continuity, damage to axons and sheath, loss of sensory
and motor. Slow recovery
Fourth degree
Loss of all tissue except epineurial tissue, surgical repair
Fifth degree
Severance of nerve trunk
Incomplete regeneration, if occurs, needs surgical repair
-
Nervous TissueCompartment or entrapments of nerves or
vesselsIncrease pressure transmittedEnclosed
spacingSymptonsnumbness, tingling & paindecreased vessel
perfusionInflammation: positive feedback loop
-
Joint InjuriesExcessive loadingDislocation (luxation)Partial
dislocation (subluxation)SynovitisArthritisOARAGouty