Embed Size (px)
Citation preview

88
Chapter 4- Trends in Indian Health Insurance Industry

89
4.1 History and Global Perspective
Under the General Agreement on Trade in Services (GATS) of the World Trade
Organization (WTO) sector classification scheme, health insurance falls under the financial
services sector. Financial services are divided into two sectors: 1) insurance and 2) banking
and other financial services. Within insurance, there are four sub-sectors: a) life, accident
and health insurance, b) non-life insurance, c) reinsurance and retrocession, and, d) services
auxiliary to insurance, including broking and agency services. Despite the appearance of the
term "health insurance" under the first category, many country commitments affecting health
insurance services are in fact covered by the second category (non-life insurance). In India
health insurance is a part of non-life insurance sector. However, life insurance companies are
allowed to sell health insurance products. .
In India insurance is a federal subject and is governed by the Insurance Act 1938 and the
Insurance Regulatory and Development Authority Act, 1999. In India the Insurance business
is divided into four classes namely; a. Life insurance, b. Fire insurance, c. Marine insurance
and d. Miscellaneous insurance. Life insurers transact life insurance business and general
insurance transact the rest. Health insurance falls under the miscellaneous insurance business
but there is no clear demarcation as the same is also offered by the life insurance companies.
Globally, the history of general insurance can be traced back to the early civilization. As the
incidence of losses increased with the advancement of civilization, slowly the idea and
concept of risk pooling and loss sharing started taking roots. Historical facts show that the
Aryans through their cooperatives practiced the loss of profits insurances. The
Mediterranean merchants also practiced insurances from as early as the fourth century BC
through the issue of bottomry bonds, which is an advance of money in a ship during the
period of voyage, repayable on the arrival of the ship. The Code of Manu also indicates the
practice of marine insurance by Indian with their counter parts in Sri-Lanka, Egypt and
Greece23
.
23
The Institute of Chartered Accountants of India, ‗Principle and practice of general insurance‟,
2008.

90
When, talking about the history of health insurance in India, one will find that health
insurance is not of recent origin. One can argue that the concept of health insurance is there
since the beginning of the mankind. In the Vedic literature it‘s stated that people use to
sacrifice animals to Gods and in return expected good health. It is interesting to link this
activity with that of the current concept of health insurance i.e. to pay the premium (animal
sacrifice) to safeguard from ill health. However, in such situation there was no transfer of
risk in contractual terms. The concern for loss resulting from accident and illness can be
traced to ancient civilizations. In fact, one of the earliest forms of health insurance may have
been based on the ancient custom of paying the doctor while in good health and
discontinuing payment during periods of illness. The development of health insurance in
existing form in India is based on pattern followed in Europe and America. Also, health
Insurance or medical insurance schemes had developed in India due to industrial relations
problems between the employer and the employees. The Corporate Houses used to offer core
and non-core benefits to the employees. The insurance policies were granted to large
Corporate Houses purely on an accommodation basis. The cover usually offered to the
employees was in the nature of hospitalization and domiciliary treatment for dental and non-
surgical eye treatment.
Before examining the trends in the Indian health insurance industry, the global insurance
market was looked into. The market size of the global insurance industry which is measured
in terms of premium as a percent of global GDP was first studied, followed by studying the
data on insurance density and insurance penetration. This section is then followed by the
overview of the Indian healthcare system.
4.1.1 Market Share & Segmentation
The market size of the global insurance industry measured in terms of total premium stands
USD 4061bn in year 2007. The life insurance industry accounted for USD 2393bn, Non-life
accounted for USD 1668bn (Table 4.1). In the year 2007 the life insurance industry captures
59 percent of the total global insurance premium and the remaining 41 percent is captured by
the non-life insurance industry. The global premium as a percent of global GDP stands 7.48

91
percent. The total direct premium growth is 3.3 percent. The premium growth in non-life
sector is much less than that of the life insurance sector.
Table 4.1: Global insurance industry overview (market size), 2007
Global Insurance Industry
Amount Units Year Source
Total Gross Insurance Premiums 4061 Billion US$ 2007 Swiss Re
Global Premiums as percent of Global
GDP 7.48 Percent 2007 IMF
Global Life Insurance Premiums 2393 Billion US$ 2007 Swiss Re
Global Non-Life Insurance Premiums 1668 Billion US$ 2007 Swiss Re
Total Direct Premium Growth, 2007-2007 3.3 Percent 2007 Swiss Re
Growth in Life Insurance Premiums 5.4 Percent 2007 Swiss Re
Growth in Non-Life Insurance Premiums 0.7 Percent 2007 Swiss Re
4.1.2 Insurance density and penetration (international market)
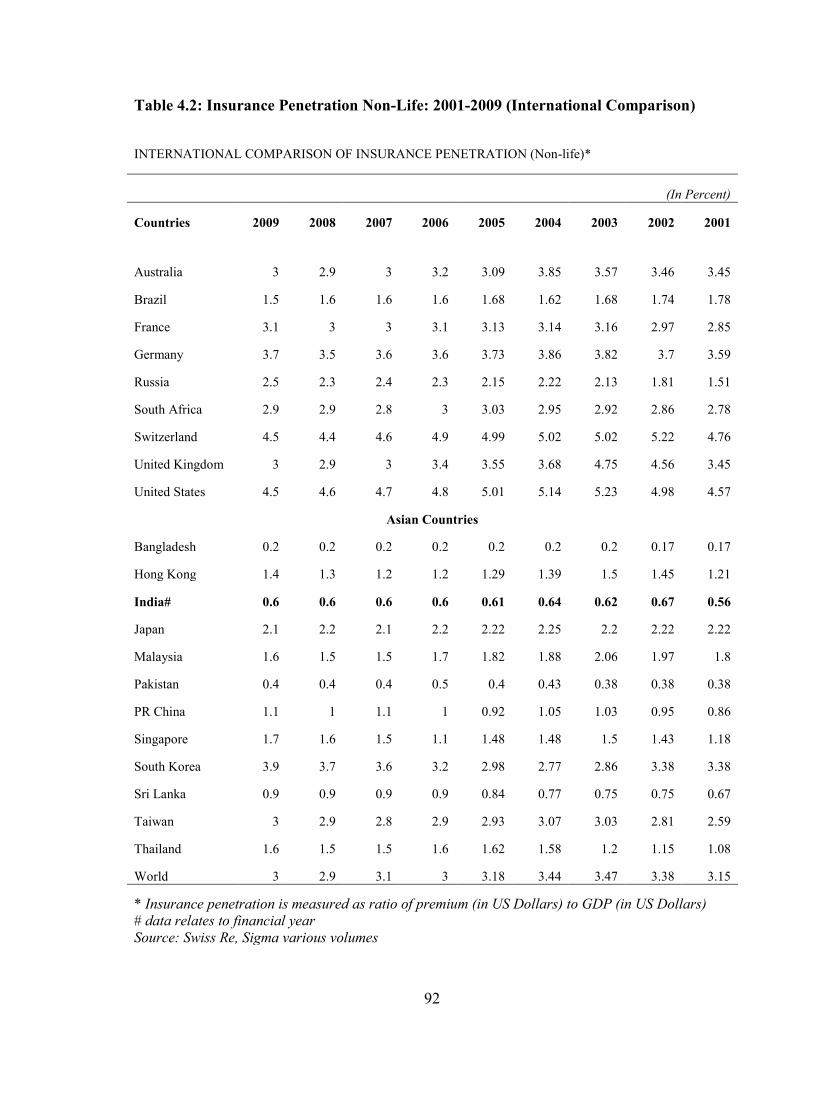
Table 4.2 and Table 4.3 depict the non-life international comparison of insurance penetration
and density24
. The insurance penetration in India has increased to 0.6 percent (2009) from
0.56 percent (2001). In India there had been an increase in insurance density from 2.4 to 6.7
during 2001 to 2009. India is one of the major contributor to the emerging market premium
as could be seen in the Figure 4.1 that reflect the additional premium volume from 2003-
2007 compared with the premium volume of 2002. India occupies seventh rank in the
emerging markets in terms of market share in non life insurance (Table 4.4). In non-life
insurance India‘s share is 3.7 percent and that of China is 17 percent in the year 2007.
24
Insurance penetration is measured in terms of premium as a percent of GDP and insurance density
is measured in terms of per capita premium.
92
Table 4.2: Insurance Penetration Non-Life: 2001-2009 (International Comparison)
INTERNATIONAL COMPARISON OF INSURANCE PENETRATION (Non-life)*
(In Percent)
Countries 2009 2008 2007 2006 2005 2004 2003 2002 2001
Australia 3 2.9 3 3.2 3.09 3.85 3.57 3.46 3.45
Brazil 1.5 1.6 1.6 1.6 1.68 1.62 1.68 1.74 1.78
France 3.1 3 3 3.1 3.13 3.14 3.16 2.97 2.85
Germany 3.7 3.5 3.6 3.6 3.73 3.86 3.82 3.7 3.59
Russia 2.5 2.3 2.4 2.3 2.15 2.22 2.13 1.81 1.51
South Africa 2.9 2.9 2.8 3 3.03 2.95 2.92 2.86 2.78
Switzerland 4.5 4.4 4.6 4.9 4.99 5.02 5.02 5.22 4.76
United Kingdom 3 2.9 3 3.4 3.55 3.68 4.75 4.56 3.45
United States 4.5 4.6 4.7 4.8 5.01 5.14 5.23 4.98 4.57
Asian Countries
Bangladesh 0.2 0.2 0.2 0.2 0.2 0.2 0.2 0.17 0.17
Hong Kong 1.4 1.3 1.2 1.2 1.29 1.39 1.5 1.45 1.21
India# 0.6 0.6 0.6 0.6 0.61 0.64 0.62 0.67 0.56
Japan 2.1 2.2 2.1 2.2 2.22 2.25 2.2 2.22 2.22
Malaysia 1.6 1.5 1.5 1.7 1.82 1.88 2.06 1.97 1.8
Pakistan 0.4 0.4 0.4 0.5 0.4 0.43 0.38 0.38 0.38
PR China 1.1 1 1.1 1 0.92 1.05 1.03 0.95 0.86
Singapore 1.7 1.6 1.5 1.1 1.48 1.48 1.5 1.43 1.18
South Korea 3.9 3.7 3.6 3.2 2.98 2.77 2.86 3.38 3.38
Sri Lanka 0.9 0.9 0.9 0.9 0.84 0.77 0.75 0.75 0.67
Taiwan 3 2.9 2.8 2.9 2.93 3.07 3.03 2.81 2.59
Thailand 1.6 1.5 1.5 1.6 1.62 1.58 1.2 1.15 1.08
World 3 2.9 3.1 3 3.18 3.44 3.47 3.38 3.15
* Insurance penetration is measured as ratio of premium (in US Dollars) to GDP (in US Dollars)
# data relates to financial year
Source: Swiss Re, Sigma various volumes

93
Table 4.3: Insurance Density Non-Life: 2001-2009 (International Comparison)
INTERNATIONAL COMPARISON OF INSURANCE DENSITY (Non-Life)* (In US Dollars)
Countries 2009 2008 2007 2006 2005 2004 2003 2002 2001
Australia 1307.9 1348.6 1326.1 1191.9 1203.2 1186.3 912.1 695.5 628
Brazil 123.8 129.1 106.9 88.4 72.1 55.2 46.8 45 53.2
France 1289.4 1339.2 1219.3 1152.9 1093.9 1057.7 930.4 714.7 630.6
Germany 1518.7 1572.7 1427.9 1300.7 1268.4 1265.3 1120.8 891 809.9
Russia 276.4 268.1 203.3 146.9 116.5 89.6 64.3 43.5 32.6
South Africa 163.9 163.6 159.5 160.2 156.2 141 107.4 64.8 69.1
Switzerland 2852.1 2827.9 2581.7 2450.1 2480.3 2441.3 2228.5 1822.7 1627.1
United Kingdom 1051.2 1275.7 1383.2 1327.1 1311.9 1318 1441.4 1199.7 825.9
United States 2107.3 2177.4 2164.4 2134.2 2122 2062.6 1980.2 1799 1664
Asian Countries
Bangladesh 1.3 1.1 0.9 0.8 0.8 0.8 0.7 0.6 0.6
Hong Kong 417.5 380.8 341.3 331.6 331.7 332.9 348.7 345.1 295.5
India# 6.7 6.2 6.2 5.2 4.4 4 3.5 3 2.4
Japan 840.4 829.2 736 760.4 790.4 830.8 768 714.7 701.1
Malaysia 115 119.5 110.6 103 95.3 89.2 87.2 79.3 68.8
Pakistan 3.6 4 3.9 3.6 2.8 2.2 1.8 1.7 1.5
PR China 40 33.7 25.5 19.4 15.8 12.9 11.2 9.5 7.8
Singapore 645.6 630 531.2 341.2 392 365.4 320.3 300.6 245.8
South Korea 709.7 621 727.3 591.2 495.5 412.5 369.4 337.9 296.7
Sri Lanka 17.7 19.3 14.7 12.8 9.4 7.9 7.2 6.1 5.4
Taiwan 494.8 499.6 462.3 450.3 446.4 414.4 383.2 354.1 327.6
Thailand 62.7 64.9 58.9 50 44.4 41.3 27.6 23.1 19.8
World 253.9 264.2 249.6 224.2 219 220 202.5 175.6 158.3
* Insurance density is measured as ratio of premium (in US Dollar) to total population.
# data relates to financial year.
Source: Swiss Re, Sigma various volumes

94
Figure 4.1: Contribution to emerging market premium (growth 2003-2007)
111
38
24
5.8
5.0
3.4
3.3
3.1
2.0
2.0
21
4.0
0 50 100 150 200 250 300
Emerging Markets
India
Russia
South Africa
Mexico
Indonesia
bn USD (real at 2002 prices)
Premium volume 2002 Additional premium volume 2002-2007
Source: National insurance authorities, Swiss Re Economic Research & Consulting.
Table 4.4: Top 10 countries in non- life insurance (emerging markets)
Non-life insurance
2007 premium volume
(in USD milllion)
Share of emerging
markets
China 33,810 17.00 percent
Russia 28,973 14.60 percent
Brazil 20,501 10.30 percent
Mexico 9,763 4.90 percent
South Africa 8,345 4.20 percent
Poland 7,677 3.90 percent
India 7,402 3.70 percent
Turkey 7,201 3.60 percent
Venezuela 6,977 3.50 percent
Argentina 4,471 2.20 percent
Top 10 129,619 68.00 percent
Source: Insurance Information Bureau, IRDA

95
4.2 Overview of Indian healthcare system
The trends in the health insurance market are governed by multiple factors, one of which is
the nature and type of healthcare system existing in the given geography. For example, if the
healthcare system promotes out of pocket expenditures then there would be a large
percentage of population which would depend on private healthcare providers for their
medical needs. This will lead to higher demands for the private care and thus the cost of care
would increase must faster. A point will come when the healthcare cost would be so high
that it would become difficult for an average individual to afford health care cost. It will be
then that the health insurance companies would come into play and would try to apply the
principle of risk pooling and principle of large numbers. On the other side they would also
make efforts to bring down the cost of healthcare expenditure by contracting with healthcare
providers for better rates and also by monitoring the cost closely. Thus, it is important to
study the overview of the Indian healthcare system in context of the trends in the Indian
health insurance industry.
4.2.1 Determinants of Health
Before looking into the Indian healthcare system let‘s briefly examine the determinants of
health. As per World Health Organization a child born in a developing country is ten to
fifteen times more likely to die before reaching his first birthday than a child born in a
developed country. Similarly, the individual may expect to live up to fifty years compared to
eighty years in some developed countries. There has been this observation that during World
War II fighting in the same area in similar conditions more European soldiers developed
jaundice (Hepatitis A) as compared to Indian soldiers. So what determines whether a person
will fall ill or die? It is just being born or living in a particular geographical area or more
than that? Obviously it‘s more than that. Health is a multifactorial amalgamation of various
determinants. Some of the important determinants of health are examined and then linked
with the cover extended under health insurance policy. This determinant includes genetic,
environmental, socio-cultural, economic, health services, political system and technological
advancements. A brief description of these determinants is presented below.

96
4.2.1.1 Genetic- The positive health advocated by WHO implies that a person should be able
to express as completely as possible the potentialities of his genetic heritage. The
genetic makeup of each individual is unique and cannot be altered after conception.
The genetic constitution determines the health status to a great extent. It is may be
due to this reason that there are specific exclusions with respect to congenital illness
(both internal and external) in most of the health insurance policy. Now, the question
arises if the health insurance firms should be allowed to exclude any genetic
conditions in a person or not? The answer is not an easy one and one need to examine
this on a case to case basis and in lack of any specific regulations the decision
becomes more difficult.
4.2.1.2 Environmental- Environment may be internal or external. Internal environment is
dealt with by internal medicine. The external environment involves all that is external
to the individual. The external environment factors range from housing, water supply,
family structure and occupation. In health insurance the internal environment is
covered quite fairly. The only clause is that of hospitalization i.e. the insured need to
be hospitalized for a minimum of twenty four hours. However, there are few
exceptions where day care surgeries are covered due to advancement in medical
technology.
4.2.1.3 Socio-cultural- Social interactions with parents, peer groups, friends and siblings are
through school and mass media affects the life-style of individuals. Personal habits
like smoking, alcohol intake, drug abuse are developed through social interactions.
Obesity, drug addictions are few examples of medical problems resulting from social
causes. Life style can have a positive effect on health. Reduction of smoking,
avoiding red meat, regular exercise all contribute to a healthy life style. In health
insurance underwriting all these factors are kept in mind to measure the potential risk
of health and based on the life style of the individual necessary discounts or loading
is done in the base premium. Now a day‘s one can find that most of the health insurer
are focusing on the lifestyle of the customers and trying to bring positive health
outcomes by extending memberships to health clubs and exercise centers.

97
4.2.1.4 Economic- Economic performance is the major factor in reducing morbidity,
increasing and improving life expectancy. Economic status determines the
purchasing power, quality of life, family size and disease pattern. It is one of the
crucial factors which determine which determine health seeking behavior. We have
seen in India how the central and state governments fund the health insurance
schemes for the poor who does not have the purchasing power.
4.2.1.5 Health Services- The health services must be equitably distributed, affordable and
socially acceptable. The health services can be offered at the primary, secondary and
tertiary level. It can also be bifurcated in terms of public and private space. From
health insurance perspective it is important to ensure that there is synergy between
the offering of the public and the private healthcare providers i.e. in places where
there is no public infrastructure; health insurance can be used as a mechanism to
deploy funds for the development of private health care services. This could be
practically seen in districts where RSBY policy has been launched.
4.2.1.6 Political System- The percentage of Gross National Product (GNP) spent on health is
a quantitative indicator of political commitment. To achieve the goal of health for all,
WHO has set the target of at least 5 percent expenditure of each country‘s GNP on
health care. India spends 3 percent of its GNP on health care. In addition to this it is
the political system which decides the investment of funds by the foreign players into
insurance sector. Currently, the FDI cap is of 26 percent in any insurance company.
However, the bill to raise the FDI limit to 49 percent is on its way and should be
passed given the current diplomatic pressures from the developed countries like US.
4.2.1.7 Technological advancements- There are many who suggest that improvement in
technology has lead to better health care outcomes. Whether, the health care cost has
risen or not due to technological advancement is not clearly know. In health
insurance this determinant is used to extend benefits to the customer by covering day
care treatments i.e. medical treatment and or surgical procedure which is undertaken
under general or local anesthesia in a hospital or a day care center in less 24 hours
because of technological advancement.
98
Thus we have seen that there are multiple determinants on one‘s health and how each one of
them is linked with the health insurance industry. Now, the overview of the Indian health
care system followed by healthcare financing is presented.
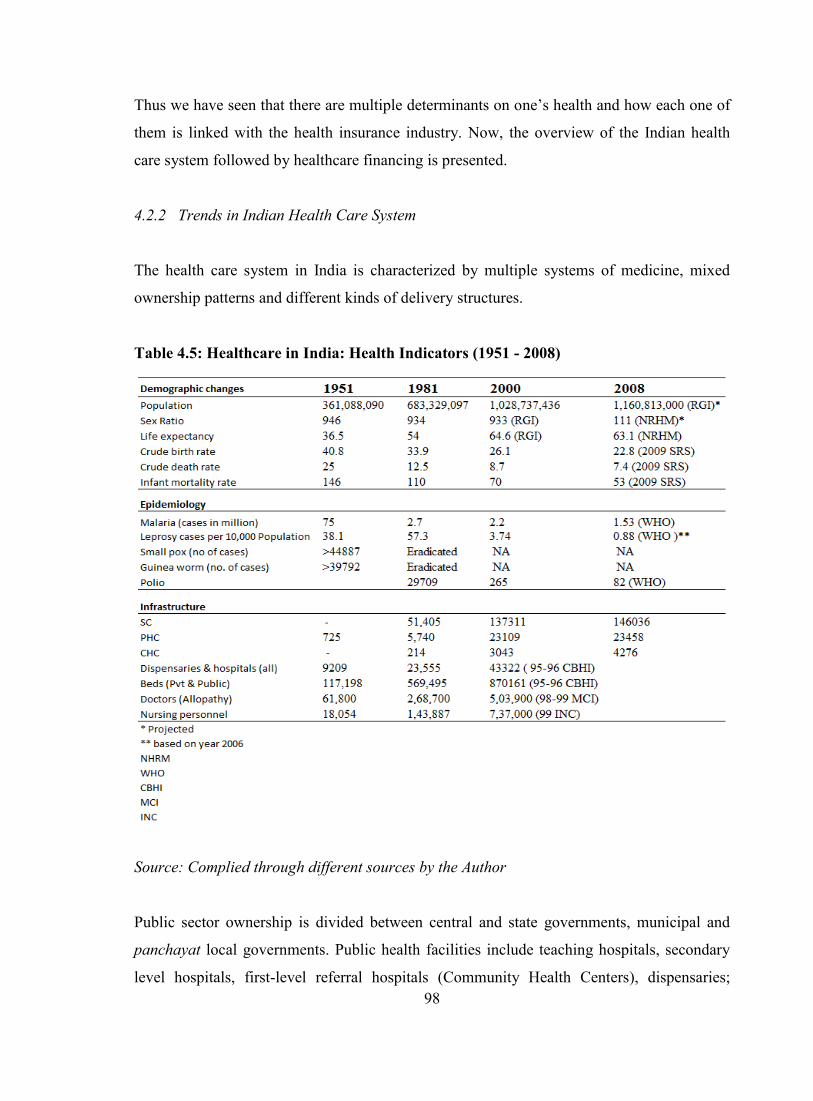
4.2.2 Trends in Indian Health Care System
The health care system in India is characterized by multiple systems of medicine, mixed
ownership patterns and different kinds of delivery structures.
Table 4.5: Healthcare in India: Health Indicators (1951 - 2008)
Source: Complied through different sources by the Author
Public sector ownership is divided between central and state governments, municipal and
panchayat local governments. Public health facilities include teaching hospitals, secondary
level hospitals, first-level referral hospitals (Community Health Centers), dispensaries;

99
Primary Health Centres (PHCs), Sub-Centres, and health posts. Also included are public
facilities for selected occupational groups like organized work force (ESI), defence,
government employees (CGHS), railways, post and telegraph and mines among others. The
private sector (for profit and not for profit) is the dominant sector with 50 percent of people
seeking indoor care and around 60 to 70 percent of those seeking ambulatory care (or
outpatient care) from private health facilities. While India has made significant gains in
terms of health indicators - demographic, infrastructural and epidemiological (see Table 4.5)
it continues to grapple with newer challenges.
The country is now in the midst of a dual disease burden of communicable and non-
communicable diseases. This is coupled with spiraling health costs, high financial burden on
the poor and erosion in their incomes. Around 24 percent of all people hospitalized in India
in a single year fall below the poverty line due to hospitalization. An analysis of financing of
hospitalization shows that large proportion of people; especially those in the bottom four
income quintiles borrow money or sell assets to pay for hospitalization25
. This situation
exists in a scenario where health care is financed through general tax revenue, community
financing, out of pocket payment and social and private health insurance schemes. India
spends about 4.9 percent of GDP on health26
.The total health expenditure in India is around
5 percent of GDP, with breakdown of public expenditure (0.9 percent); private expenditure
(4.0 percent). The private expenditure can be further classified as out-of-pocket (OOP)
expenditure (3.6 percent) and employees/community financing (0.4 percent). It is evident
that public health investment has been comparatively low. In fact as a percentage of GDP it
has declined from 1.3 percent in 1990 to 0.9 percent in 2010. Furthermore, the central
budgetary allocation for health (as a percentage of the total Central budget) has been
stagnant at 1.3 percent while in the states it has declined from 7.0 percent to 5.5 percent. In
light of the fiscal crisis facing the government at both central and state levels, in the form of
shrinking public health budgets, escalating health care costs coupled with demand for health-
care services, and lack of easy access of people from the low-income group to quality health
25
World Bank Report, 2002
26 World Health Report- India, 2002.

100
care, health insurance is emerging as an alternative mechanism for financing of health care in
India.
A population pyramid, also called an age structure diagram, is a graphical illustration that
shows the distribution of various age groups in a human population (typically that of a
country or region of the world), which ideally forms the shape of a pyramid when the region
is healthy. A great deal of information about the population broken down by age and sex can
be read from a population pyramid, and this can shed light on the extent of development and
other aspects of the population. A population pyramid also tells how many people of each
age range live in the area. There tends to be more females than males in the older age groups,
due to females' longer life expectancy. Figure 4.2, 4.3 and 4.4 depicts the population
pyramid by broad age-group, projected population pyramid 2001 and 2026 of India. In India
the demographic transition27
has been relatively slow but steady. As a result the country was
able to avoid adverse effects of too rapid changes in the number and age structure of the
population on social and economic development. In the period between1996 to 2016,
population in the age group greater than 60 yrs will increase from 62.3 to 112.9 million28
.
Figure 4.2: Percentage of population by broad age-groups: India 2001-2026
Source: Office of the Registrar General and Census Commissioner, India.
27 Demographic transition is the transition from a stable population with high mortality and fertility to
a stable population with low mortality and fertility. During the transition population growth and
changes in the age structure of the population are inevitable.
28 Source: Technical Group on Population Projections, Registrar General of India (RGI) 1996

101
Figure 4.3: Projected population Pyramid: India-2001
Source: Office of the Registrar General and Census Commissioner, India.
Figure 4.4: Projected population Pyramid: India-2026
Source: Office of the Registrar General and Census Commissioner, India.
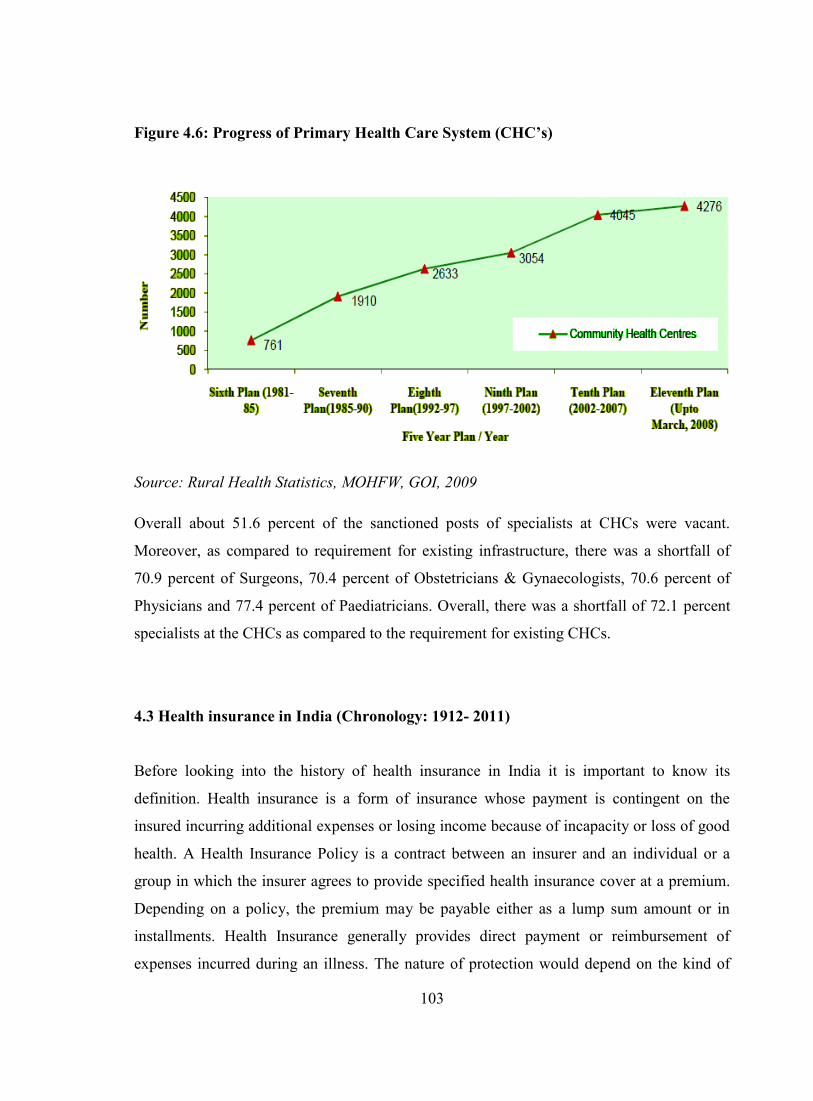
The Primary Health Care Infrastructure has been developed as a three tier system with Sub
Centre, PHC and CHC being the three pillars of Primary Health Care System. Progress of
Sub Centres, which is the most peripheral contact point between the Primary Health Care

102
System and the community, is a prerequisite for the overall progress of the entire system. A
look at the number of Sub Centres functioning over the years reveal that at the end of the
Sixth Plan (1981-85) there were 84,376 Sub Centres. The figure rose to 1, 30,165 at the end
of Seventh Plan (1985-90) and to 1, 45,272 at the end of Tenth Plan (2002-2007). As on
March, 2008 there were 1, 46,036 Sub Centres functioning in the country.
Figure 4.5: Progress of Primary Health Care System (PHC’s)
Source: Rural Health Statistics, MOHFW, GOI, 2009
Similar progress can be seen in the number of PHCs which was 9115 at the end of Sixth plan
(1981-85) and the figure almost doubled to 18671 at the end of Seventh Plan (1985-90) and
rose to 22370 at the end of Tenth Plan (2002-2007). As on March, 2008, there are 23458
PHCs functioning in the country (Figure 4.5). In accordance with the progress in the number
of SCs and PHCs, the number of CHCs has also increased from 761 at the end of Sixth Plan
(1981-85) to 1910 at the end of Seventh Plan (1985-90) and 4045 at the end of Tenth Plan
(2002-2007). As on March, 2008 there were 4276 CHCs functioning (Figure 4.6). According
to the figures of population based on 2001 Population Census, the shortfall in the rural health
infrastructure comes out to be of 20486 Sub Centres, 4477 PHCs and 2337 CHCs, ignoring
surplus in some States / UTs. The current position of specialists manpower at CHCs reveal
that as on March, 2008, out of the sanctioned posts, 55.3 percent of Surgeons, 48.2 percent
of Obstetricians & Gynaecologists, 54.5 percent of Physicians and about 47.2 percent of
Paediatricians were vacant.
103
Figure 4.6: Progress of Primary Health Care System (CHC’s)
Source: Rural Health Statistics, MOHFW, GOI, 2009
Overall about 51.6 percent of the sanctioned posts of specialists at CHCs were vacant.
Moreover, as compared to requirement for existing infrastructure, there was a shortfall of
70.9 percent of Surgeons, 70.4 percent of Obstetricians & Gynaecologists, 70.6 percent of
Physicians and 77.4 percent of Paediatricians. Overall, there was a shortfall of 72.1 percent
specialists at the CHCs as compared to the requirement for existing CHCs.
4.3 Health insurance in India (Chronology: 1912- 2011)
Before looking into the history of health insurance in India it is important to know its
definition. Health insurance is a form of insurance whose payment is contingent on the
insured incurring additional expenses or losing income because of incapacity or loss of good
health. A Health Insurance Policy is a contract between an insurer and an individual or a
group in which the insurer agrees to provide specified health insurance cover at a premium.
Depending on a policy, the premium may be payable either as a lump sum amount or in
installments. Health Insurance generally provides direct payment or reimbursement of
expenses incurred during an illness. The nature of protection would depend on the kind of

104
policy purchased and the cost and range of protection under that policy. Health insurance
could be either a personal scheme or a group scheme sponsored by an employer. Unlike life
insurance where there are only two parties i.e. the insured and the insurer, in the case of
health insurance there are three parties namely the insured, the insurer and the provider
(network hospital). There is also TPA which acts as an extended arm of the insurance
company and helps in claim processing, managing the hospital networks and at times helping
in enrollment of customers.
The generic features of insurance are equally applicable to the concept of health insurance.
Insurance primarily rests on the principle of pooling of risk associated with the same cause
i.e. health to share losses on some equitable basis. Insurance‘ whether it is health or any
other line of insurance, is a concept of sharing financial burden. Insurance follows a simple
statistical principle of ―diversity‖ or ―pooling of resources and sharing of risk‖. This means
that from out of a given population that is Insured, those needing the financial support by
way of a claim for loss is very small. Especially in the case of Health Insurance, it is less
than 5 percent of the total population covered in its current form. This in effect means that
out of the amount contributed by 100percent, financial claims are paid to only 5 percent.
This theory of diversity is an important factor in a country like India.
Thus, health insurance in a narrow sense would be ‗an individual or group purchasing health
care coverage in advance by paying a fee called premium.‘ In its broader sense, it would be
any arrangement that helps to defer, delay, reduce or altogether avoid payment for health
care incurred by individuals and households.
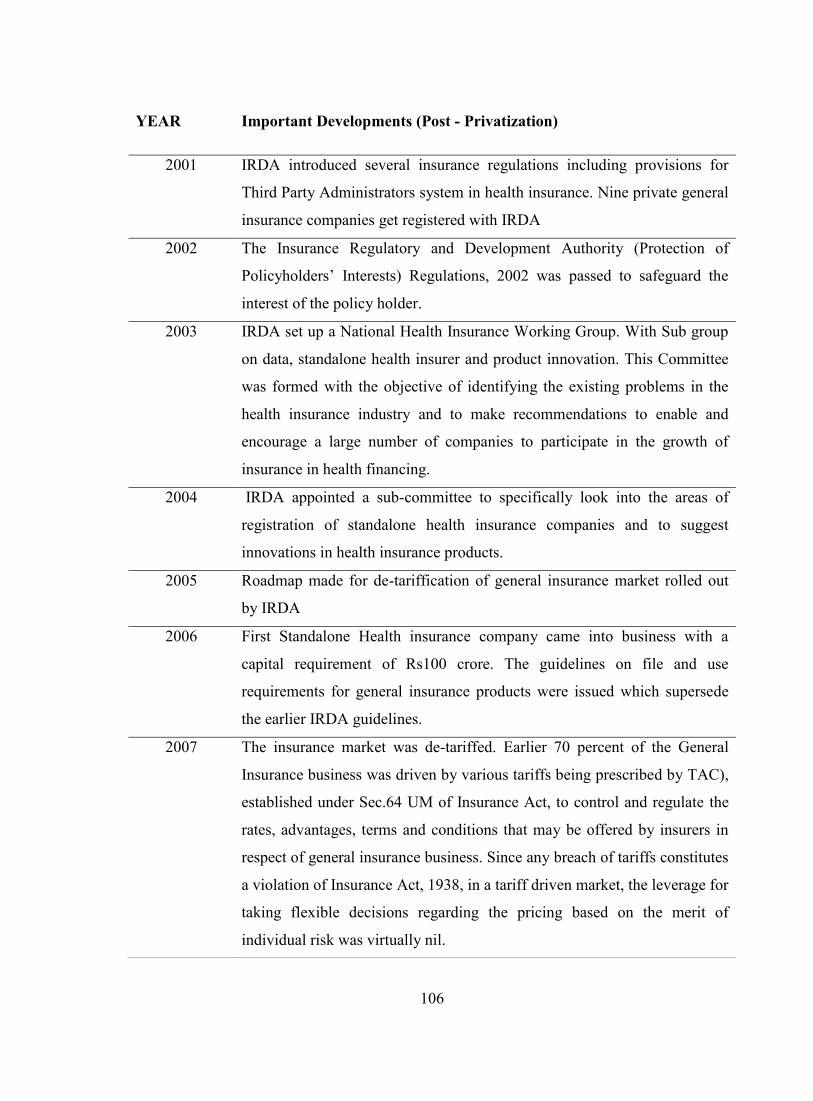
Taking into account various developments in and outside the insurance sector, showcasing
the developments in the field of insurance, including developments specific to health
insurance, with brief summaries are given in chronological order (see Table 4.6).

105
Table 4.6: Health insurance in India (Chronology: 1912- 2011)
YEAR Important Developments (Pre - Privatization)
1912 Insurance Act, 1912 passed, setting down rules and regulations specific to
insurance industry.
1923 Workman‘s Compensation Act passed, aims to provide workmen and/or
dependents some relief in case of accidents arising out of or in the course of
employment, causing death or disablement
1938 Insurance Act, 1938 passed, recognizing two categories, i.e. Life and non-
life (general) insurance. Led to an insurance wing being set-up, attached to
the Ministry of Finance.
1948 Employee‘s State Insurance (ESI) Act passed, providing protection to
workers & dependents in the organized sector for sickness, maternity, death
1954 The Central Government Health Scheme started in 1954, providing health
cover to employees of Central Government, MPs, Judges, Freedom Fighters
and their families.
1956 Life Insurance industry nationalized and Life Insurance Corporation of
India (LIC) set up subsequently.
1959 Mudaliar Committee constituted, recommended provision of long-range
health insurance policy for all and strengthening Primary Health Centers.
1972 General Insurance industry nationalized
1986 General Insurance Corporation of India (GIC) introduced mediclaim
insurance policy
1999 Insurance Regulatory and Development Authority (IRDA) Act passed
2000 W.e.f. Dec 2000, GIC became the National Re-insurer, its earlier role of co-
ordination between the four subsidiaries taken over by a new body, General
Insurance (Public Sector Companies) Association (GIPSA).
106
YEAR Important Developments (Post - Privatization)
2001 IRDA introduced several insurance regulations including provisions for
Third Party Administrators system in health insurance. Nine private general
insurance companies get registered with IRDA
2002 The Insurance Regulatory and Development Authority (Protection of
Policyholders‘ Interests) Regulations, 2002 was passed to safeguard the
interest of the policy holder.
2003 IRDA set up a National Health Insurance Working Group. With Sub group
on data, standalone health insurer and product innovation. This Committee
was formed with the objective of identifying the existing problems in the
health insurance industry and to make recommendations to enable and
encourage a large number of companies to participate in the growth of
insurance in health financing.
2004 IRDA appointed a sub-committee to specifically look into the areas of
registration of standalone health insurance companies and to suggest
innovations in health insurance products.
2005 Roadmap made for de-tariffication of general insurance market rolled out
by IRDA
2006 First Standalone Health insurance company came into business with a
capital requirement of Rs100 crore. The guidelines on file and use
requirements for general insurance products were issued which supersede
the earlier IRDA guidelines.
2007 The insurance market was de-tariffed. Earlier 70 percent of the General
Insurance business was driven by various tariffs being prescribed by TAC),
established under Sec.64 UM of Insurance Act, to control and regulate the
rates, advantages, terms and conditions that may be offered by insurers in
respect of general insurance business. Since any breach of tariffs constitutes
a violation of Insurance Act, 1938, in a tariff driven market, the leverage for
taking flexible decisions regarding the pricing based on the merit of
individual risk was virtually nil.

107
General insurance as a whole, developed with the industrial revolution in the West and with
the consequent growth of seafaring trade and commerce in the seventh century. In India too,
evidence of insurance in some form can be traced as early as from the Aryan period. The
British and some of the other foreign insurance companies through their agencies transacted
insurance business in India. The first general insurance company in India was the Triton
Insurance company Ltd., established in Calcutta in 1850 AD, with the British holding major
2008 Insurance Information bureau set up by IRDA (primarily working on Health
and motor data). General insurance Council for the first time defined the
"Pre-existing" clause and made it standard across the industry.
2009 The Renewability of Health insurance policies circular issued on 31st
March 2009 advises non-life insurers not to generally decline renewals
except for certain specified reasons. Detailed instructions on Health
Insurance for Senior Citizens stipulate that all health insurance products
filed on or after 1st July, 2009 must allow entry up to 65 years of age, and
also to make adequate dissemination of product information on websites.
Also, the FICCI report on Health Insurance released in July 2009 includes
Standard Treatment Guidelines for 21 common causes of hospitalization.
2010 The Preferred Provider Network (PPN) of hospitals introduced in July 2010
to offer cashless medical treatment following the initiative taken by the four
pubic insurers to bring discipline on the pricing of hospital services. The
health insurance market continues to be dominated by the four state-owned
general insurers, which together accounted for almost 60 percent of the
premiums.
2011 A key development was the announcement of portability of health
insurance policies by IRDA. The regulator has issued guidelines for the
arrangement to be effective from 1 July 2011, which will allow
policyholders to switch providers on the same policy terms, particularly
without losing the credit gained for pre-existing conditions in terms of
waiting period. Circular on ―De-Listing of Hospitals‖ and guidelines on
―Distance Marketing‖ also rolled out.

108
share. The first general insurance company by Indian promoters was the Indian Mercantile
Insurance company Ltd. started in Bombay in 1906-07.
Following the First World War, several foreign insurance companies started insurance
business in India, capturing about 40 percent of the insurance market in India at the time of
Independence. It was in the year 1912 that the ―insurance Act‖ was passed which was then
revised in the year 1932. This was under the revised Act that the Life and Non-life categories
were recognized. In India the general insurance is also known as ―Non-life‖. The health
insurance was a part of the non-life business; however, there was no clear demarcation then.
Even today both the life and the non-life companies are allowed to have health insurance
products.
The year 1940-1960 has witnessed the launch of the ESI and the CGHS schemes. These
schemes had the elements of health insurance concepts but were not placed with any
insurer29
.
In the year 1971, the government by an ordinance nationalized the general insurance
business, under the General insurance Nationalization Act, 1972 to ensure orderly and
healthy growth of the business. The then existing 107 companies were brought under the
aegis of GIC of India and were merged with the four public general insurance players
namely the National insurance company, the Oriental insurance company, the United
insurance company and the New India assurance company. These four public insurance
companies were distributed geographically and had their head offices at Kolkata, New-Delhi,
Chennai and Mumbai respectively. The primary reason for such division was to have wider
spread with regional focus. It was expected that the subsidiary companies would provide
effective competition to each other with the support from GIC. The GIC facilitated
coordination, competition and laid down standards for market conduct, customer service and
development of the market.
29
The current study excludes these two schemes as it would be a separate independent research area
in itself.

109
In 1973 the general insurance industry was nationalized and with the liberalization of the
market, the four public players became autonomous and were directly answerable to the
Ministry of Finance as their owner. The General Insurance Corporation of India was
designated as the Indian Re-insurer.
In 1981, the Apex Body of Public Sector Insurance Companies i.e. GIC designed a limited
cover for individuals and families for covering their hospitalization needs. This was replaced
by a mediclaim policy in the year 1986 under a market agreement to provide insurance
benefits to individuals and groups under a group mediclaim policy. The then ‗Mediclaim‘
Insurance Policy provided reimbursement of medical expenses for hospitalization and
domiciliary hospitalization, but it does not cover OPD treatment. The sum that is assured
under this policy varies from Rs.15, 000 to Rs.5 lac. It was available to the people from the
age of 5 years to the age of 80 years. The children between the age of 3 months and 5 years
were covered with some additional premium. The minimum premium was Rs. 213 per
annum for the lowest sum assured, that is, Rs. 15,000 (for people below 35 years of age).
The highest premium was Rs. 17,156 per annum for people in the age group between 76
years and 80 years for the maximum sum assured, that is, up to Rs. 5 lac. There was a family
discount of 10 percent and some cumulative bonus if the previous year had been claim-free.
The scheme so introduced was modified in 1991 and 1996 in the light of experience and
suggestions received from the insuring public and medical fraternity. The benefit that was
provided under the mediclaim policy was on reimbursement basis only. Reimbursement of
the expenses was allowed by insurance companies on production of the required bills given
by the hospitals where the treatment was taken. This created the need for cashless payment
facility at hospitals, as it was difficult for an insured person to arrange for funds at the time
of admission in the hospital. Requests were made to GIC for introducing a system whereby,
payment could be made directly by the insurance company to the hospital where the
treatment was taken. Insurance companies entered into tie up with hospitals to provide such
benefit whereby an insured person could collect a certificate of his eligibility from an
insurance company and produce the same to the hospital for taking the treatment. The
settlement of the claims was directly made with the hospitals. This tie up with hospitals
failed in course of time in view of some reported cases wherein the hospital managed to get
110
claims reimbursement of such insured persons who took treatment for pre-existing
ailments30
.
As a part of the financial reforms in the year 1993 the Government of India appointed a
committee know as Malhotra Committee on reforms in the insurance sector. This committee
rightly recommended the opening up of insurance sector to competition stating that
introduction of competition will result in better customer service and new products. As the
insurance market was open in the year 2001, there were nine new entrants. Up to June 2011
there were 48 insurance companies licensed by IRDA and doing business in India (24 life
insurance companies and 24 non-life insurance companies and within non-life, there were
three specialist health insurance companies).
4.4 Major players and Performance
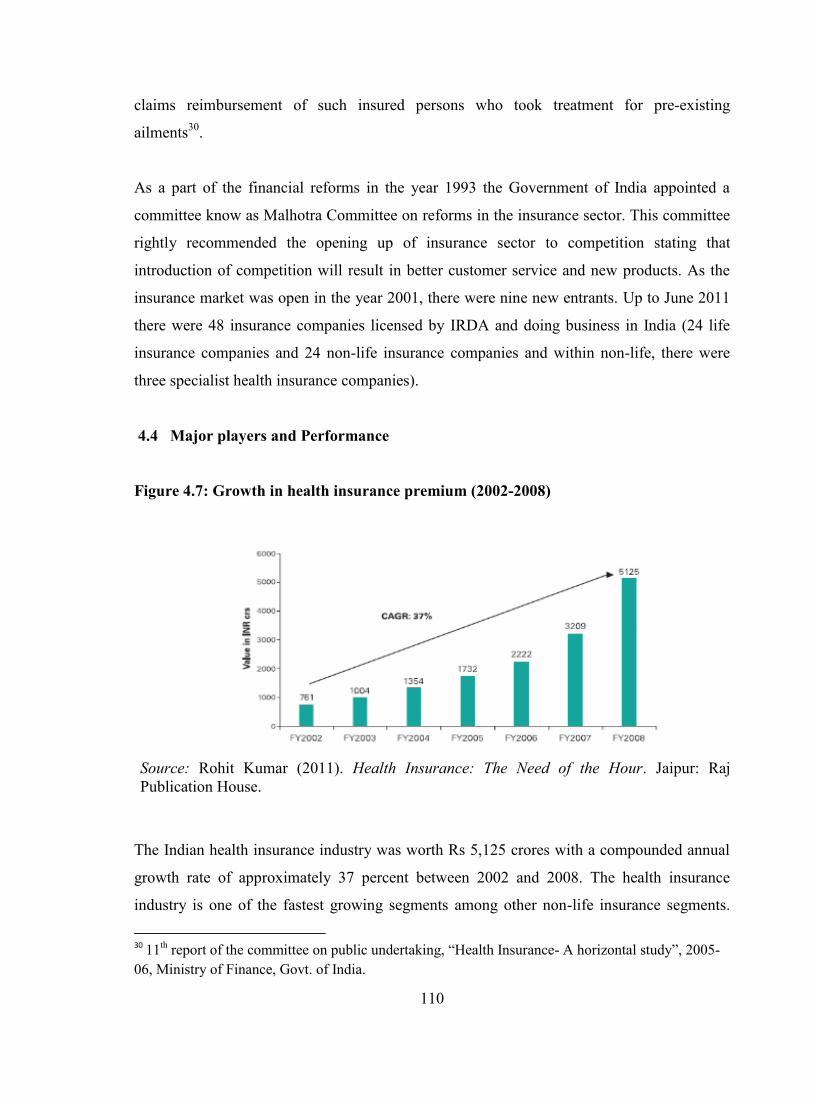
Figure 4.7: Growth in health insurance premium (2002-2008)
Source: Rohit Kumar (2011). Health Insurance: The Need of the Hour. Jaipur: Raj
Publication House.
The Indian health insurance industry was worth Rs 5,125 crores with a compounded annual
growth rate of approximately 37 percent between 2002 and 2008. The health insurance
industry is one of the fastest growing segments among other non-life insurance segments.
30
11th report of the committee on public undertaking, ―Health Insurance- A horizontal study‖, 2005-
06, Ministry of Finance, Govt. of India.
111
The Indian health insurance industry today is worth Rs 60,497 crores with a compounded
annual growth rate of approximately 42.3 percent expected between 2008 and 2015. Market
penetration will be three folds higher in 2015 (Figure 4.7).
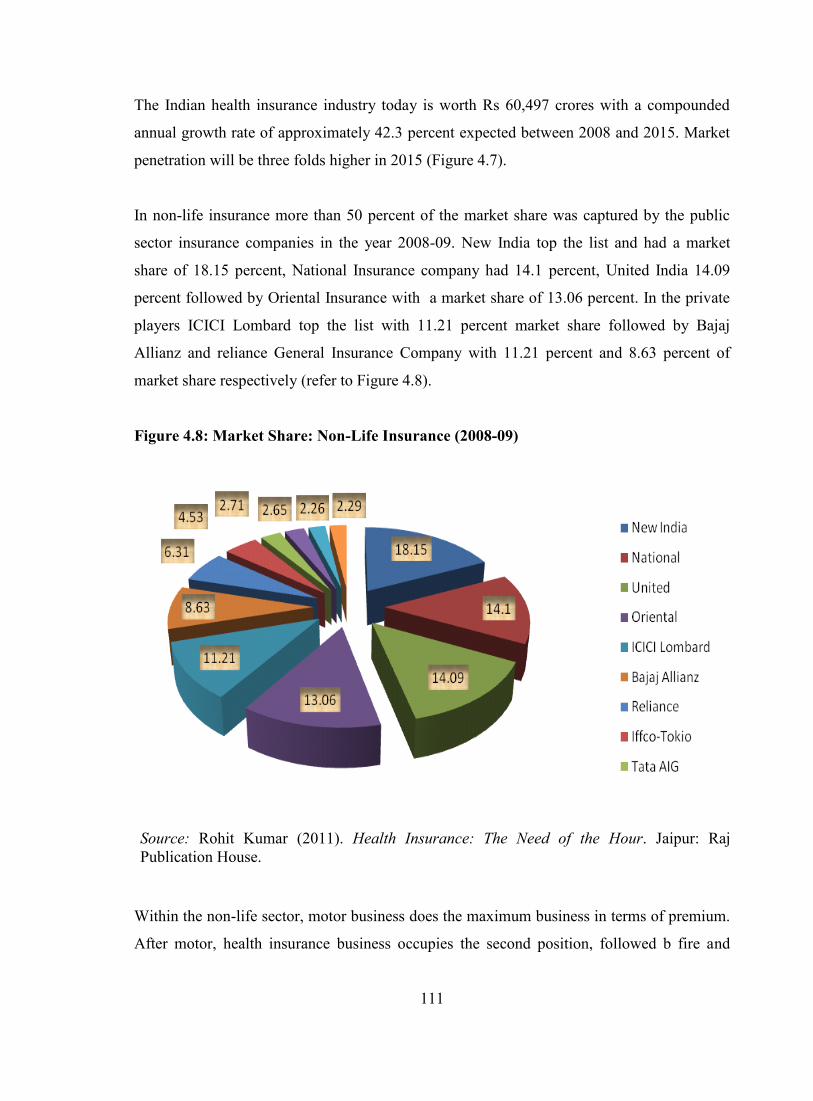
In non-life insurance more than 50 percent of the market share was captured by the public
sector insurance companies in the year 2008-09. New India top the list and had a market
share of 18.15 percent, National Insurance company had 14.1 percent, United India 14.09
percent followed by Oriental Insurance with a market share of 13.06 percent. In the private
players ICICI Lombard top the list with 11.21 percent market share followed by Bajaj
Allianz and reliance General Insurance Company with 11.21 percent and 8.63 percent of
market share respectively (refer to Figure 4.8).
Figure 4.8: Market Share: Non-Life Insurance (2008-09)
Source: Rohit Kumar (2011). Health Insurance: The Need of the Hour. Jaipur: Raj
Publication House.
Within the non-life sector, motor business does the maximum business in terms of premium.
After motor, health insurance business occupies the second position, followed b fire and

112
marine business. Across all these segments from 2007-08 to 2008-09 health insurance has
seen the maximum growth (refer Figure 4.9).
Figure 4.9: Non-Life insurance company- segment wise premium (2007and 2009)
Source: Rohit Kumar (2011). Health Insurance: The Need of the Hour. Jaipur: Raj
Publication House.
Figure 4.10: Market Share- Health Insurance (Earned premium 2008-09)
Source: Rohit Kumar, K. Rangarajan, and Nagarajan Ranganathan (2011). ―Health Insurance
in India—A Study of Provider‘s Perceptions in Delhi & the NCR,‖ Journal of Health
Management 13: 259-277.

113
Again in health insurance business the public sector insurance companies had more than 50
percent of the market share, measured in terms of earned premium (year 2008-09). However,
there was a difference in the ranking of public and private sector companies. The third rank
was occupied by ICICI Lombard. One of the interesting observations was that Star Health
insurance company (the first standalone health insurance company in India) had captured 11
percent of the overall market share (Figure 4.10). Thus, one can argue that standalone health
insurance companies are going to increase the level of competition within the health
insurance market and are here to stay.
On examining the latest data on market share for the period April-May 2011 it was observed
that ICIC Lombard had 29 percent of the market share, Star Health had 23 percent of the
market share followed by HDFC Ergo (9 percent), Royal Subdram (6 percent), Reliance
General (5 percent), IFFICO Tokio and Apollo Munich (4 percent each). Here, it is
interesting to note that the three standalone insurance companies captured some 28 percent
of the market share within the private insurance space (Figure 4.11). The customer segment
wise premium data is currently not available. However, the regulator had asked the insurers
and TPA‘s to start providing the health data on the basis of customer segment i.e retail,
corporate and mass business.
In the area of retail health product it was found that different levels of cover are being
offered by different insurance companies. In most of the cases the pre-existing disease was
not covered before fourth year from policy inception date (see table 4.7). It was also
observed that there were co-payment and sub-limit options being built-in in the product. This
may be primarily because to reduce the claim paid cost and also to offer retail health
insurance policy at a lower price.
The incurred claim ratio for both private and public sector companies for three consecutive
years i.e. 2006-07 to 2008-09 is presented in table 4.8. It was observed that the claim ratio
for public sector insurance companies was 20 to 15 percent higher than that of the private
players. One of the possible reasons for this difference could be because the public sector
insurance companies might be offering the health insurance product at a lower price to
corporate houses. In other words the public sector insurance companies might be subsidizing
the health insurance premium in lieu of premium received on other insurance product like
fire and marine business.

114
Figure 4.11: Market Share (Health Insurance) - Private Players (April -May -2011)
Source: Insurance Information Bureau, IRDA.
Table 4.7: Retail health insurance product- Market Comparison
Market Comparison (Retail policy)
Cover IL Bajaj Chola OIC Ntn'l Star
Hosp √ √ √ √ √ √Pre 30 60 60 30 30 30
Post 60 90 90 60 60
7% of hosp bill
max 7k
PED 5th 5th No NA 4th No
30 day √ √ √ √ √ √Named ailments 2 yrs 2 yrs 1 yr 2 yr 2 yr 1yr/ 2yr
Co-pay
We pay
full claims
10% co-
pay in non-
n/w
hospitals
10% for
Diab/Hyp &
25% if both.
Sub-limits
Only in
case of
cataract
Hernia/pile
s/cataratc
etc 10% of
SI
Room
Rent 1%
of SI, ICU
2% of SI
Room Rent
2% of SI max
4k
Two Year √SI 2L-4L 1L-10L 1L-10L 1L-5L 1L-5L
Entry Age 60 55 55/69 (for dependant parents)60 60 1L-5L
IL- ICICI Lombard, OIC- Oriental Insurance, Ntn‟l- National Insurance
Source: Author‟s compilation based on the study of the retails products (2009-10) offered by
selected insurance companies.

115
Table 4.8: Incurred Claim Ratio (2006-07 to 2009)
INCURRED CLAIMS RATIO (Percent)
YEAR 2008-09 2007-08 2006-07
PUBLIC 116.60 112.36 157.79
NEW INDIA 107.41 89.88 212.81
ORIENTAL 136.96 123.77 132.51
NATIONAL 111.27 118.01 131.47
UNITED 121.27 135.36 160.05
PRIVATE 85.33 94.81 103.42
ROYAL SUNDARAM 43.57 44.78 46.99
BAJAJ ALLIANZ 78.02 85.19 78.64
TATA AIG 46.71 74.93 61.69
RELIANCE 91.74 112.14 113.01
IFFCO TOKIO 122.23 121.14 152.89
ICICI LOMBARD 86.07 98.79 118.70
CHOLAMANDALAM 108.99 93.03 79.51
HDFC CHUBB 100.5 142.46 87.10
FUTURE GENERALI 141.12 Na Na
GRAND TOTAL 105.95 106.99 141.02
Source: Insurance Information Bureau, IRDA
However, subsidizing should get minimized due to de-tariffication of the general insurance
industry recently. The claim ratio for the public sector has shown improvement. From more
than 100 percent in 2006-07 it has come down to 85.33 percent. However, including both
public and private players the claim ratio is still more than 100 percent i.e. for 2008-09 it
was standing at 105.95 percent.

116
4.5 Current opportunities and threats
Insurance company today find themselves surrounded by a variety of challenges as they
work towards profitable growth and to compete in this dynamic industry. Across the industry
the insurance companies faces common challenges. The opportunity and threats includes the
following:
4.5.1 Governance and risk management: The record losses from Hurricanes Katrina,
Wilma and Rita have once again highlighted the scale of the risks faced by insurer‘s
in an increasingly complex and uncertain financial, geopolitical and climatic
environment. Model outputs are clearly critical in monitoring and controlling
aggregations and concentrations of risk. However, the largely unexpected gravity of
the losses and resulting pressure on reinsurance programmes have once again
underlined the importance of quality data, effective validation and calibration of
model outputs and, not least, the sense check of underwriting experience and
intuition. The development of Enterprise Risk Management (ERM)31
capabilities can
help to protect insurers from losses, earnings surprises and name risk and provide a
platform for strengthening governance, decision-making and regulatory compliance.
However, a recent study conducted by PricewaterhouseCoopers32
, revealed that many
insurers are finding it difficult to make headway in implementing and embedding
ERM in the face of continuing data, systems and governance challenges. However,
the study also found many examples of how insightful and effective management are
helping to overcome these technical and organizational hurdles and bring greater
clarity to insurers‘ ERM missions.
4.5.2 The growth imperative: To be succesful in the growth initiatives companies have
tried to design innovative bundles of good products and services. They have tried to
31
ERM programmes can help to safeguard businesses against losses, earnings surprises and name
risk. This includes strengthening the management of credit, market and other financial risks, along
with more effective controls over less quantifiable, though equally hazardous, non-financial risks
such as fraud, systems failure and breaches in compliance with regulatory and corporate guidelines
32 The report is available at:
http://www.pwc.com/extweb/pwcpublications.nsf/docid/2E4B06FB305460138525746C00625848.
117
cross sell by strengthening their relationship with agents and brokers and by
spreading their business in emerging markets like India and China.
4.5.3 Managing the complexities of compliance: In almost all the countries of the world the
insurance market is highly regulated. The degree may vary. Growing regulatory
requirements are bringing increased scrutiny to governance, information security,
monitoring and reporting process in insurance companies. Much of this change is
taking place in Europe by the advent of solvency II33
and in the United States with
the upcoming NIAC revised Model Audit Rule (MAR)34
. The effect of these
regulation are likely to be felt globally, as the evolving regulatory picture set the
canvas for industry best practices. There is an opportunity to use the regulatory
requirements as the catalyst to improve the overall management and build confidence
in the public eye.
4.5.4 Human Capital: Many insurers are facing mounting skills shortages. Yet, investment
in recruitment, training and career development often less than other financial
sectors. The primary focus can often be short-term demands rather than securing the
talent companies need to meet longer term strategic objectives. The effect of
demographic shifts, evolving aspirations and accelerating globalization are set to
transform the shape of the global labour market and could make it even harder for
insurers to attract and retain good people. In this competitive labour market,
33
Solvency II is the updated set of regulatory requirements for insurance firms that operate in the
European Union. It is based on economic principles for the measurement of assets and liabilities. It is
also a risk-based system as risk is measured on consistent principles and capital requirements depend
directly on this.
34 The National Association of Insurance Commissioners (NAIC) Annual Financial Reporting Model
Regulation, also known as the Model Audit Rule (MAR), requires that private insurance companies
with direct premiums written and assumed in excess of $500 million per year adopt corporate
governance and reporting standards. The Model Audit Rule, originally issued to drive consistency
across insurance regulators, was modified in 2006 and will take effect for the year ending 2010. The
new modifications within the Model Audit Rule are very similar to those of the Sarbanes-Oxley Act
of 2002 (SOX or Sarbanes-Oxley), which was issued in response to several high-profile fraudulent
financial reporting scandals at large public corporations. It was these scandals that caused there to be
a much greater emphasis placed on the accuracy of companies‘ financial statements and the method
in which they were assembled.
118
successful companies will need to develop a strategic approach to HR management
capable of anticipating and responding to evolving business needs and workforce
expectations. They will also need to identify and realize opportunities to differentiate
benefits, career development prospects and other key aspects of their employment
brand in both developed and emerging markets.
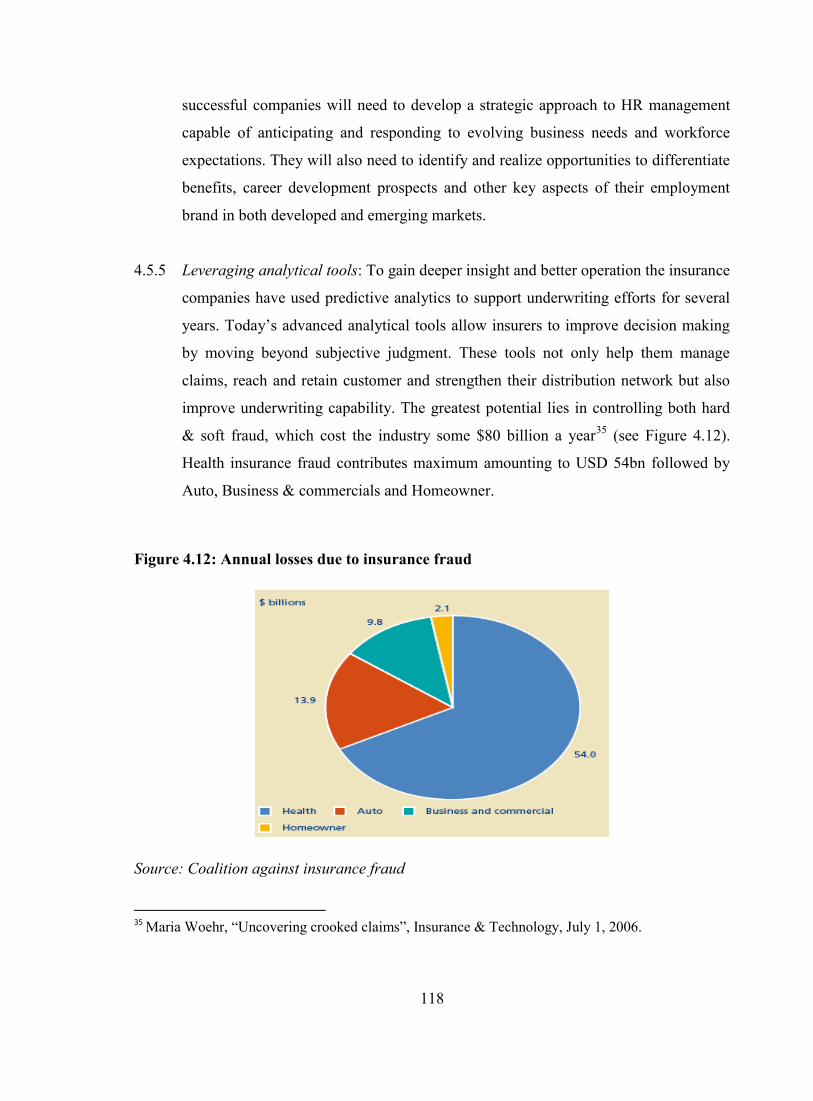
4.5.5 Leveraging analytical tools: To gain deeper insight and better operation the insurance
companies have used predictive analytics to support underwriting efforts for several
years. Today‘s advanced analytical tools allow insurers to improve decision making
by moving beyond subjective judgment. These tools not only help them manage
claims, reach and retain customer and strengthen their distribution network but also
improve underwriting capability. The greatest potential lies in controlling both hard
& soft fraud, which cost the industry some $80 billion a year35
(see Figure 4.12).
Health insurance fraud contributes maximum amounting to USD 54bn followed by
Auto, Business & commercials and Homeowner.
Figure 4.12: Annual losses due to insurance fraud
Source: Coalition against insurance fraud
35
Maria Woehr, ―Uncovering crooked claims‖, Insurance & Technology, July 1, 2006.

119
Given the above opportunities and challenges the top executives of the insurance companies
are quite optimistic about the future growth of insurance industry.
In April 2009, the Economist Intelligence Unit surveyed, on behalf of KPMG International,
315 global insurance executives from around the world. The respondents were split among
life insurance (42 percent), non-life insurance (49 percent) and reinsurance (9 percent)
companies or divisions. The Key findings of the survey were as under:
i. Over half of respondents see positive prospects for growth in the next 12 months.
ii. While respondents believe themselves to be well-capitalized, and rating themselves
highly in terms of effectiveness across most risk management activities, there is a
clear sense that a greater focus on both capital management and risk management
would be warranted.
iii. Two thirds of companies have appointed board level risk committees.
There is limited appetite for incremental spend, with almost half the respondents expecting
to improve performance without increasing resources.
The global insurance industry is bound to contribute towards the growth of world economy
and will keep evolving in the way the other financial markets have done in the past. The
study of the global insurance market reveals that there is a level of saturation reached in the
industrialized countries and the focus has moved to the emerging markets like China and
India.
4.6 Legal & regulatory aspects of health insurance
The Constitution of India has a federal structure i.e. it provides for distribution of powers
between the Union and the States. It enumerates the powers of the Parliament and State
Legislatures in three lists, namely Union list, State list and Concurrent list. As insurance is
included in the Union list, the parliament has the exclusive legislative empowerment to
regulate the insurance industry in India. Thus, the laws with reference to insurance are
uniform throughout the territories of India.

120
As we have seen earlier, the insurance industry (both life and general) has gone through the
complete cycle from being a free market, to nationalization and then again opened for private
players. The common thread connecting this cycle is the legal framework, which has also
undergone a sea change. However, The Insurance Act of 1938 along with various
amendments over the years continues till date to be the definitive piece of legislation on
insurance and controls both life insurance and general insurance.
The general insurance business was nationalized with effect from January 1, 1973, through
the introduction of the General Insurance Business (Nationalisation) Act, 1972 (―GIC Act‖).
Under the provisions of the GIC Act, the shares of the existing Indian general insurance
companies and undertakings of other existing insurers were transferred to the GIC to secure
the development of the general insurance business in India and for t he regulation and control
of such business. The GIC was established by the Central Government in accordance with
the provisions of the Companies Act, 1956 (―Companies Act‖) in November 1972 and it
commenced business on January 1, 1973. Prior to 1973, there were a hundred and seven
companies, including foreign companies, offering general insurance in India. These
companies were amalgamated and grouped into four subsidiary companies of GIC viz. the
National Insurance Company Ltd. (―National Co.‖), the New India Assurance Company Ltd.
(―New India Co.‖), the Oriental Insurance Company Ltd. (―Oriental Co.‖), and the United
India Assurance Company Ltd. (―United Co.‖). GIC undertakes mainly re-insurance
business apart from aviation insurance. The bulk of the general insurance business of fire,
marine, motor and miscellaneous insurance business is under taken by the four subsidiaries.
It was in the year 1993, the Government of India set up an eight-member committee chaired
by Mr. R. N. Malhotra (commonly called as the Malhotra Committee), a former Governor of
India's apex bank, the Reserve Bank of India to review the prevailing structure of regulation
and supervision of the insurance sector and to make recommendations for strengthening and
modernizing the regulatory system. The Committee submitted its report to the Indian
Government in January 1994. Two of the key recommendations of the Committee included
the privatization of the insurance sector by permit ting the entry of private players to enter
the business of life and general insurance and the establishment of an Insurance Regulatory
Authority.

121
The Indian Parliament passed the Insurance Regulator y and Development Act,
1999 (―IRDA Act‖) on December 2, 1999 with the aim ―to provide for the establishment of
an Authority, to protect t he interests of the policy holders, to regulate, promote and ensure
orderly growth of the insurance industry and to amend the Insurance Act, 1938, the Life
Insurance Corporation Act, 1956 and the General Insurance Business (Nationalization) Act,
1972‖.
IRDA has been entrusted with the duty to regulate, promote and ensure the orderly growth of
the insurance and re-insurance business in India. In addition to this, it has been conferred
with numerous powers and functions which include prescribing regulations on the
investments of funds by insurance companies, regulating maintenance of the margin of
solvency, adjudication of disputes between insurers and intermediaries, supervising the
functioning of the Tariff Advisory Committee, specifying the percentage of premium income
of the insurer t o finance schemes for promoting and regulating professional organizations
and specifying the percentage of life insurance business and general insurance business to be
undertaken by the insurer in the rural or social sector.
The broad regulatory framework for health insurance business in India includes: Deposits;
Investments; Valuation of Assets Liabilities and Solvency Margins; Submission of Returns;
Actuary; Insurance Advertisements; Obligations to the Rural and Social Sector; Assignment
and Nomination; Foreign Exchange laws; Taxation laws and Stamp Duty.
In the month of February 2011, IRDA had rolled out the regulation on portability of health
insurance to safeguard the interest of the policyholders. The gist of guidelines is given
below:
All insurers issuing health insurance policies shall allow for credit gained by the
insured for pre existing conditions in terms of waiting period when insured switches
from one insurer to another or from one plan to another, provided the previous policy
has been maintained without break.

122
This credit shall be limited to the sum assured (including bonus) under the previous
policy.
When policyholder is switching from one insurer to other, Insurers shall process the
proposal with speed and efficiency and all decisions thereof shall be communicated
in writing within a reasonable period not exceeding 15 days from receipt of proposal
by the insurer.
If the policy results into discontinuance because of any delay by the insurer in
accepting the proposal, the insurer shall not treat the policy as discontinuance and
shall allow portability.
Insurers shall clearly draw the attention of the policyholder in the policy contract and
the promotional material like prospectus, sales literature etc.
Insurer to share the entire database including the claim details of the policies where
the policyholders has opted for portability with their counterparts where requested.
All applications for the portability shall be acknowledged by the insurers within three
working days.
Having looked into the external environment including the trends in the Indian health
insurance industry it becomes quite evident that the health insurance sector is growing at a
fast pace and so is the level of competition. The key developments in the Indian health
insurance industry had taken place post the privatization. There are multiple initiatives taken
by the regulator to improve the growth and built trust among the minds of the policyholders.
The standalone health insurance companies are here to stay and are increasing their market
share on a year to year basis. The detariffication of the insurance industry will help reduce
the subsidization offered in health insurance However, currently the health insurance
industry has a claim ratio of more than 100 percent and to ensure that the business is
profitable one needs to develop strategies for synergy among insurers and providers, and in
doing so it is important to understand the attitude, interest and concerns of the different
stakeholders. The health insurance industry is highly regulated unlike the healthcare industry
and it is important to meet the needs and expectations of different stakeholders.