Embed Size (px)
Citation preview

VALVULAR HEART DISEASE
274
ETIOLOGY AND PATHOGENESISRheumatic fever is responsible for a majority of
cases of mitral stenosis. The initial infection andits sequelae result in thickened valve leaflets andfusion of the commissure between the leaflets.Chordae tendineae are also affected and be-come thickened and shortened. Most valves thatare affected by rheumatic fever show abnormali-ties of all these structures. Few patients withrheumatic mitral valve disease have pure mitralstenosis; most patients have a combination ofstenosis and regurgitation. Approximately twothirds of the cases of mitral stenosis in the UnitedStates occur in women.
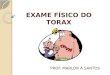
The normal mitral valve cross-sectional area indiastole is 4 to 6 cm2. Blood flow is impaired whenthe valve orifice is narrowed to less than 2 cm2,creating a pressure gradient with exertion. Avalve area smaller than 1 cm2 is considered criti-cal mitral stenosis and causes a gradient acrossthe valve at rest with chronically increased leftatrial pressures (Fig. 29-1).
Chronically increased pressures in the left atriumassociated with mitral stenosis result in left atrialenlargement and a predisposition for atrial fibrilla-tion. Valves affected by mitral stenosis are also vul-nerable to recurrent thrombosis and implantationof bacteria that lead to infective endocarditis.
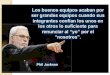
The hemodynamic effects of chronic mitralstenosis include pulmonary venous and arterialhypertension, right ventricular (RV) hypertrophyand failure, peripheral edema, ascites, andhepatic injury with cirrhosis (Fig. 29-2).
Numerous etiologies contribute to MR. These
include mitral valve prolapse, rheumatic heartdisease, cardiomyopathy with ventricular dila-tion, ischemic heart disease involving the papil-lary muscles, ischemic cardiomyopathy, bacteri-al or fungal endocarditis, and certain collagen–vascular diseases. Disease of any component ofthe mitral apparatus can cause a functional fail-ure of the valve.
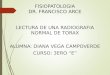
With moderate or severe MR, with left ven-tricular contraction in systole, blood is dis-charged into the left atrium, in addition to trav-eling its usual route through the aortic valve andinto the aorta. If the regurgitant volume is large,the left ventricle dilates to accommodateincreased volumes (Fig. 29-3). As MR continuesto progress, ventricular output capacity is chal-lenged, increased systemic afterload generateseven more regurgitation, and symptoms andother findings of MR occur (Fig. 29-4).
Infectious endocarditis, spontaneous rupture ofchordae tendineae, or ischemic injury of a papillarymuscle may cause acute loss of integrity of themitral valve and acute MR. In these cases, there isno adaptation of the left atrium or pulmonary vas-culature to the increased regurgitant volumes; sud-den onset of acute pulmonary edema may result.Aggressive use of afterload-reducing agents is theemergent treatment, but survival usually dependson emergency repair or replacement of the valve.
CLINICAL PRESENTATION Mitral Stenosis
Patients notice the effects of moderate (1–2 cm2) mitral stenosis with activity. With severe
Mitral valve leaflets consist of thin, pliable, fibrous material. The two leaflets—anterior and posteri-or—open by unfolding against the ventricular wall and close by apposition when the pressure in theleft ventricle becomes greater than that in the left atrium. Mitral stenosis occurs when the mitral valveleaflets become stiffened, calcified, and unable to fully open during diastole. This process ofteninvolves the chordae tendineae, in addition to the mitral valve leaflets. Mitral valve regurgitation (MR)occurs when the leaflets are unable to fully close in systole. In the United States, more than 20,000patients annually require surgery for manifestations of mitral stenosis and MR, and thousands morerequire monitoring and treatment.
Thomas R. Griggs
Chapter 29
Mitral Valve Disease

Thickened, calcified, stenotic mitral valve demonstrated in echocardiographic study at left
Mitral stenosis, viewed from below and left: Minor rheumatic involvement of aortic valve
Thickened stenotic mitral valve: Anterior cusp has typical convexity; enlarged L. atrium; “jet lesion” on L. ventricular wall
Enlargement of R. ventricle with some thickening of wall resulting from mitral stenosis; pulmonary artery enlarged and thickened with scattered plaques of atheromas
Echocardiogram demonstrating mitral stenosis. Valve located between left atrium (LA) and left ventricle (LV) is thickened, with reduced orifice and intense signal due to excessive calcium.
RV
LV AO
LA
RV
LVAO
LA
Mitral Stenosis
VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
275
Figure 29-1

VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
276
Pathophysiology and Clinical Aspects of Mitral Stenosis
Elevated “wedge” pressure
HemoptysisPulm. arteriolar constriction and/or sclerosis
Elevated pulm.-artery pressurePulmonary atherosclerosis
Dyspnea
Pulmonary congestion
Edema
Elevated pulm. venous pressure
Elevated L. atrial pressureFibrillation frequently
Thrombosis (embolism)
L. atrium enlarged
Diminished L. ventricular filling
Fixed left-heart output
Pulmonary fibrosisParasternal lift
R. ventricle dilated
Hypertrophy
Failure
Liver enlarged, tender
(Ascites)
Portal circulation
Systemic circulation
Slight cyanosis
(Portal hypertension)
Elevated venous pressure Edema
L. ventricular pressure
L. atr ia l pres sure
Diastolic–presystolic rumbling murmur 4th. L. interspace
I Sounds II Opening snap I
Gradient
L. atrial abnormality (P “mitral”) and evidence of R. ventricular hypertrophy (S in leads I and V5, R in V1)
Atrial fibrillation
R
S
I aVR V1 V2 V3
II
III
aVL
aVF
V4 V5 V6
S
Figure 29-2

In time, left ventricle dilates to accommodate increased volume.
Left atrial enlargement due to mitral regurgitationShortened,
thickened mitral cusps
Color Doppler study demonstrating systolic aortic outflow (blue/red) and multicolored jet of regurgitant flow through incompetent mitral valve into left atrium (LA)
Systolic aortic outflow
Diagram of mitral regurgitation shown in Doppler color study at left
RV
LVAO
LA
RV
LVAO
LA
Mitral insufficiency: Mitral valve viewed from below; marked shortening of posterior cusp, with only slight
commissural fusion, and little fusion and shortening of
chordae tendineae
Calcific plate at anterolateral commissure of mitral valve, contributing to insufficiency
Regurgitant jet through incompetent mitral valve
Mitral RegurgitationFigure 29-3
VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
277

VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
278
Pathophysiology and Clinical Aspects of Mitral Regurgitation
Elevated “wedge” pressure
Pulmonary arteriolar constriction
Pulmonary artery dilated; pressure elevated
Dyspnea
Pulmonary congestion
Edema
Elevated pulm.-vein pressure
Systolic regurgitation
Diminished L.-heart output
R. ventricle slightly enlarged
Failure
L. atrium enlarged (fibrillation common)
Soft, blowing pansystolic murmur at apex
I Sounds II
IIII
Lifting apex beat
L. ventricle dilated
Hypertrophy
Failure
Portal circulation
Systemic circulation
L. ventricular pressure
L. atrial pressure
L. and R. ventricular enlargementElectrocardiographic evidence of l. ventricular hypertrophy (large S in V1, large R in V4) and minor atrial abnormality (broad P)
Figure 29-4

VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
279
stenosis, dyspnea with minimal exertion andparoxysmal nocturnal dyspnea may occur. Insome cases, a sudden, dramatic onset of atrial fib-rillation produces the first symptoms, occasionallyresulting in fatal pulmonary edema. When thedevelopment of atrial fibrillation is clinically silent,the initial event may be a stroke or other throm-boembolic event. The classic presentation ofsevere cor pulmonale with ascites and edema israrely seen today except in medically underservedpopulations. Mitral valve disease increases the riskfor bacterial endocarditis, which should always beconsidered when symptoms worsen in a previ-ously stable patient with mitral valve disease.
Auscultation of symptomatic mitral stenosis ischaracterized by a loud first heart sound, anopening snap after the second heart sound, anda low-pitched diastolic murmur with presystolicaccentuation if the patient is in sinus rhythm.The opening snap is the sound generated bysudden full opening of the mitral valve. It canreflect the severity of the pressure gradientacross the mitral valve because greater left atrialpressures generate earlier opening than do less-er ones. Therefore, the shorter the interval fromA2 to opening snap, the greater the pressuregradient, and the more severe the stenosis.
The characteristic diastolic, low-frequency“rumble” or murmur associated with mitral steno-sis is best heard at the apex, with the patient in theleft lateral decubitus position and the bell overthe point of maximal ventricular intensity. Therumble occurs throughout diastole, with accentu-ation in late diastole (presystole) in patients whohave preserved normal sinus rhythm. This mur-mur can be difficult to hear and is soft and briefwhen the mitral stenosis is minor. Therefore,heightened awareness of possible mitral stenosisis necessary. If the murmur is inaudible during thismaneuver, it can be accentuated by having thepatient exercise before auscultation. This murmursequence—loud first sound, opening snap, anddiastolic rumble—is quite specific for mitral steno-sis. Murmurs that mimic mitral stenosis includethe Austin Flint murmur with aortic regurgitation,mitral diastolic murmurs in patients with largeintracardiac shunts, and occasionally murmursthat are caused by a left atrial myxoma. However,none have all three components of classic mitralstenosis.
Electrocardiographic changes in mitral steno-sis may range from minor ST-segment and T-waveabnormalities to electrocardiographic evidenceof severe pulmonary hypertension and RVenlargement. The ECG pattern of left atrial andRV enlargement is a classic indicator. Atrial fib-rillation is common.
Mitral RegurgitationEven severe MR may be clinically silent. Many
cases are discovered during routine examina-tions when the characteristic murmur is noticed.Symptoms usually begin as dyspnea on exer-tion. Patients may also present with acute pul-monary edema or evidence of RV failure. Sud-den decompensation can occur with the onsetof atrial fibrillation or the development of bacte-rial endocarditis.
With MR, palpation may be normal or mayshow a displaced, sustained left ventricular (LV)impulse with a rapid filling wave. On ausculta-tion, the most prominent feature is a high-pitched holosystolic murmur that usually radi-ates to the axilla. The intensity may not correlatewith the severity of the MR; even highly severeMR can be associated with virtually no murmur.ECG changes in MR are nonspecific and are pri-marily changes of LV hypertrophy and strain;atrial fibrillation is common.
DIFFERENTIAL DIAGNOSISPrimary pulmonary diseases (pneumonia,
tuberculosis, chronic obstructive lung disease,and pulmonary thromboembolism) have pre-sentations similar to that of mitral valve disease:dyspnea on exertion or pulmonary edema. Dys-pnea may also be present in chronic interstitialpulmonary diseases, pulmonary hypertension,and malignancies that involve the chest. Heartdiseases to consider are ischemic heart disease,congenital heart disease, dilated cardiomyopa-thy, and hypertrophic cardiomyopathy. Chronicpericardial disease with restriction can cause RVfailure that mimics the pulmonary hypertensionassociated with mitral valve disease.
DIAGNOSTIC APPROACHMany pulmonary diseases can be differenti-
ated from mitral valve disease by means ofchest imaging, including both radiography and

VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
280
computerized tomographic scanning. When aninitial evaluation has focused the differentialdiagnosis on mitral valve disease, the most help-ful clinical tool is echocardiography (see alsochapter 4). In rheumatic mitral valve disease,echocardiography can demonstrate thickening,calcification, poor mobility of the valve, andthickening of subvalvular structures. The degreeof valvular stenosis or regurgitation can be esti-mated using Doppler ultrasonography. Whennecessary, the anatomy of the valve and sub-valvular apparatus can be further defined bytransesophageal echocardiography. The goals ofechocardiography are to evaluate the severity ofthe stenosis or regurgitation, the mobility of thevalve, the involvement of subvalvular structures,and the degree of calcification and to detectintracardiac thrombi. Echocardiography pro-vides information about LV contractile functionand an accurate estimation of pulmonary arterypressure and RV function. It can also identifybacterial and fungal vegetations, intracardiacmasses (especially left atrial myxoma), and intra-ventricular septal defects, all conditions that cancomplicate the diagnosis of mitral valve disease.
Cardiac catheterization is indicated in the fewpatients with a questionable diagnosis and inthose patients for whom surgical treatment iscontemplated. Catheterization is performed toquantify the mitral valve area; document key ele-ments of hemodynamics, such as cardiac outputand systemic resistance; define the degree of pul-monary hypertension; and to determine whethercoexistent coronary artery disease is present.
MANAGEMENT AND THERAPYAsymptomatic patients with mild, uncompli-
cated mitral valve disease may require only pro-phylaxis for endocarditis. In symptomaticpatients, diuretics can help to reduce pulmonarycongestion. With mitral stenosis, the time forventricular filling is critically important; HRshould be maintained as low as is practical witha β-blocker or a calcium channel blocker, suchas verapamil or diltiazem. Patients with atrial fib-rillation must be treated with warfarin anticoag-ulation unless it is contraindicated.
Symptomatic mitral stenosis can be improvedby means of percutaneous balloon mitral valvo-tomy, surgical valvotomy, or surgical replace-
ment of the mitral valve. Various criteria areused to determine the timing of surgery, rangingfrom the development of symptoms in a patientwith known severe mitral stenosis to the newdiagnosis of severe mitral stenosis in a youngperson. In selected patients, in whom there is lit-tle valvular calcification, little involvement of thesubvalvular apparatus, and minimal or no mitralvalve regurgitation, percutaneous balloon valvo-tomy is the treatment of choice. Longitudinalstudies have documented event-free survival tobe greater than 70% at 7 years.
Open valvotomy is a repair procedure thatinvolves direct visualization by the surgeon,allowing for débridement of the valve structureand reconstruction of subvalvular apparatus.Because the approach used also allows for valvereplacement, in patients who are questionablecandidates for valvotomy, the decision can bemade during surgery whether repair or replace-ment is the most appropriate choice. Mitralvalve replacement continues to be an alterna-tive for patients with severe mitral stenosis andis especially appropriate for patients with signifi-cant MR (see chapter 34).
The timing of surgical intervention for patientswith MR is critical. In most cases, MR is well tol-erated, and the patient is asymptomatic formany years. Delaying surgery as long as possi-ble avoids the trauma, expense, and risk of sur-gery. However, every effort must be made toproceed with surgery before ventricular func-tion has degenerated. Assessments of LV sys-tolic function involve measurement of the ejec-tion fraction. The reduced wall tension andafterload of MR allow the ejection fraction to bepreserved late into the course of the disease;therefore, any decrement in ejection fractionmay represent a considerable decrease inmyocardial functional reserve. In general, mitralvalve surgery should be considered in a patientwith known moderate to severe MR when thepatient is symptomatic or there is objective evi-dence of decreased LV function.
Valve repair for severe MR improves mortalityand decreases the frequency of complications.Valves must be relatively free of calcificationand have pliable leaflets with chordae tendineaethat can be separated, reinforced, or reattachedas needed. Placement of a reinforcing mitral ring

Adhesion of mitral valve cusp to ventricular wall resulting from vegetations on undersurface of valve
Bacterial vegetations first appear along “contact line” of mitral valve but spread to involve atria and chordae tendineae with subsequent rupture and shrinkage of the latter.
Perforation of aortic valve cusp
Bacterial perforation of anterior mitral cusp
Late sequelae of bacterial endocarditis may result in mitral regurgitation via destruction of mitral valve cusps or by widening of annular valve ring due to left ventricular enlargement due to aortic insufficiency.
Left ventricular hypertrophy
Thickening and erosion of mitral valve with stumps of ruptured chordae tendineae resulting in valvular incompetence, regurgitation, and atrial enlargement
Valve adhesion to ventricular wall
Acute Chronic
Vegetations of bacterial endocarditis on underside as well as atrial surface of mitral valve
Bacterial Endocarditis in Mitral Valvular DiseaseFigure 29-5
VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
281

VALVULAR HEART DISEASE
MITRAL VALVE DISEASE
282
is frequently included in the repair. Advantages ofvalve repair over replacement are that it providespatients with functional subvalvular components,including the papillary muscles, and that the nat-ural tissues in the valve are much more resistantto thrombogenicity than any artificial surface,obviating the use of warfarin anticoagulant.
Mitral regurgitation resulting from dilated car-diomyopathy is an especially troublesome prob-lem that is caused by dilation of the mitral ringand ventricles and results in anatomic deformityof the relation of the papillary muscles and chor-dae tendineae to the mitral valve leaflets. Theresulting MR increases the need for ejection vol-ume and decreases forward blood flow. In thissituation, repair or replacement of the mitralvalve may fail to improve symptoms and is asso-ciated with an extremely high risk of operativedeath. New percutaneous approaches for mitralvalve repair in this circumstance are currently inclinical trials to determine safety and efficacy.
Coronary heart disease can cause MR bymeans of several mechanisms. The mitral valve istethered to papillary muscles that are dependenton myocardial blood flow. Acute ischemia to thearea providing blood flow to the papillary mus-cles can cause temporary MR. Infarction of thepapillary muscle will cause permanent failure ofthe subvalvular apparatus. Acute myocardialinfarction that involves a papillary muscle causessevere, acute, life-threatening MR, with mortalityrates of nearly 30% if not surgically and emer-gently corrected. In some circumstances, aninfarction results in rupture of the tip of the papil-lary muscle with acute MR. This is almost alwaysfatal unless surgically corrected. Finally, patientswith extensive myocardial scarring caused by pre-vious infarction and associated dilation of theventricle, ischemic cardiomyopathy, can havesevere MR because of dilation of the mitral ringand abnormal alignment of the papillary muscles,chordae tendineae, and valve leaflets.
Any structural abnormality of the valve canresult in flow aberrations that promote depositionof microthrombi. These can be the nidus for a bac-terial or fungal infection with simultaneous sep-
ticemia, resulting in further damage associatedwith endocarditis (Fig. 29-5). Endocarditis canaffect valve competency because of interferencein valve function by vegetations or by destructionor fenestration of the valve leaflets. Althoughendocarditis is usually managed with antibiotics,the damage effected by the bacteria is permanent,as is the resultant MR. Indications for surgery aftercured bacterial endocarditis are identical to thosefor other causes for MR. In addition, acute surgicalcare is indicated for extremely large vegetations,when heart failure is otherwise unmanageable,when a myocardial abscess is documented, andfor patients with persistent bacteremia.
FUTURE DIRECTIONSImproving worldwide morbidity and mortality
associated with rheumatic heart disease necessi-tates better systems of hygiene and improvedprophylactic treatment of streptococcal infec-tion, especially the current drug-resistant strains.The prevalence of MR will increase as the popu-lation ages, spurring improvements in severalareas: imaging with more accurate estimates ofventricular reserve, surgical technology withearly repair of severely regurgitant valves, bal-loon valvotomy with improved patient selectionand equipment, and minimally invasive surgicaltechniques with reduced recovery time and mor-bidity. Better treatment for atrial fibrillation andimproved therapies for prevention of thrombosiswill greatly improve the quality of life for patientswith mitral valve disease and valve prostheses.
REFERENCESBonow RO, Carabello B, de Leon AC Jr, et al. ACC/AHA guide-
lines for the management of patients with valvular heart dis-ease: A report of the American College of Cardiology/Amer-ican Heart Association Task Force on Practice Guidelines(Committee on Management of Patients With ValvularHeart Disease). J Am Coll Cardiol 1998;32:1486–1588.
Enriquez-Sarano M. Timing of mitral valve surgery. Heart2002;87:79–85.
Marcus RH, Sareli P, Pocock WA, et al. The spectrum ofsevere rheumatic mitral valve disease in a developingcountry: Correlations among clinical presentation, surgi-cal pathologic findings, and hemodynamic sequelae. AnnIntern Med 1994;120:177–183.