Embed Size (px)
DESCRIPTION
advance trauma life saving
Citation preview

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 1/28
Advanced Trauma Life Support 41
TWO
2Airway and VentilatoryManagement
CHAPTER
OBJECTIVES:
Upon completion of this chapter, the student will be able to identify actual or impending airway obstruction,explain the techniques of establishing and maintaining a patent airway, and conrm the adequacy of ventila-tion. Specically, the doctor will be able to:
A. Identify the clinical settings in which airway compromise is likely to occur.
B. Recognize the signs and symptoms of acute airway obstruction.
C. Describe the techniques to establish and maintain a patent airway and conrm the adequacy of ventila-tion and oxygenation, including pulse oximetry and carbon dioxide (CO
2) colorimetric monitoring.
D. Dene the term “denitive airway” and outline the steps needed to maintain oxygenation before, during,and after establishing a denitive airway.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 2/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
42 American College of Surgeons
I. INTRODUCTION
Inadequate delivery of oxygenated blood to the
brain and other vital structures is the quickest killerof the injured. Prevention of hypoxemia requires aprotected, unobstructed airway and adequate ven-tilation that must take priority over all other condi-tions. An airway must be secured, oxygen deliveredand ventilatory support provided. Supplementaloxygen must be administered to all trauma pa-tients.
Early preventable deaths from airway problems af-ter trauma often result from:
1. Failure to recognize the need for an airway.
2. Inability to establish an airway.3. Failure to recognize an incorrectly placed air-
way.
4. Displacement of a previously established air-way.
5. Failure to recognize the need for ventilation.
6. Aspiration of gastric contents.
Remember: Airway and ventilation are the rstpriorities.
II. AIRWAY
A. Problem Recognition
Airway compromise may be sudden and complete,insidious and partial, and progressive and/or recur-rent. Although often related to pain and/or anxiety,tachypnea may be a subtle but early sign of airwayor ventilatory compromise. Therefore, assessmentand frequent reassessment of airway patency andadequacy of ventilation are important. The patientwith an altered level of consciousness is at particu-lar risk for airway compromise and often requiresprovision of a denitive airway. The unconscious
head-injured patient, the patient obtunded fromalcohol and/or other drugs, and the patient withthoracic injuries may have compromised ventila-tory effort. In these patients, endotracheal intuba-tion is intended to (1) provide an airway, (2) deliversupplementary oxygen, (3) support ventilation, and(4) prevent aspiration. Maintaining oxygenationand preventing hypercarbia are critical in manag-ing the trauma patient, especially if the patient hassustained a head injury.
The doctor should anticipate vomiting in all injuredpatients and be prepared. The presence of gastriccontents in the oropharynx conrms a signicant
risk of aspiration with the patient’s very next breath.Immediate suctioning and rotation of the entire pa-tient to the lateral position are indicated.
1. Maxillofacial trauma
Trauma to the face demands aggressive airwaymanagement. The mechanism for this injury isexemplied by the unbelted passenger/driverwho is thrown into the windshield and dash-board. Trauma to the midface may producefractures/dislocations with compromise to thenasopharynx and oropharynx. Facial fractures
may be associated with hemorrhage, increasedsecretions, and dislodged teeth, causing addi-tional problems in maintaining a patent airway.Fractures of the mandible, especially bilateralbody fractures, may cause loss of normal sup-port. Airway obstruction results if the patient isin a supine position. Patients who refuse to liedown may be indicating difculty in maintainingtheir airway or handling secretions.
2. Neck trauma
Penetrating injury to the neck may result in vas-cular injury with signicant hemorrhage. Thismay result in displacement and obstruction of theairway. An urgent surgical airway may be neces-sary if this displacement and obstruction makeendotracheal intubation impossible. Hemorrhagefrom adjacent vascular injury may be massiveand operative control may be required.
Blunt or penetrating injury to the neck may causedisruption of the larynx or trachea, resulting inairway obstruction or severe bleeding into thetracheobronchial tree. A denitive airway is ur-gently required.
Neck injuries may cause partial airway obstruc-tion by disruption of the larynx and trachea orby compression of the airway from hemorrhageinto the soft tissues of the neck. Initially, a patientwith this type of serious airway injury may beable to maintain airway patency and ventilation.However, if airway compromise is suspected, adenitive airway must be established. To pre-vent extending an existing airway injury, anendotracheal tube must be inserted cautiously.When the patient loses airway patency, it may be

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 3/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 43
precipitous, and an early surgical airway usuallyis indicated.
3. Laryngeal trauma
Although fracture of the larynx is a rare injury,it can present with acute airway obstruction. It isindicated by the following triad:
a. Hoarseness
b. Subcutaneous emphysema
c. Palpable fracture
If the patient’s airway is totally obstructed orthe patient is in severe respiratory distress, anattempt at intubation is warranted. Flexible endo-
scopic-guided intubation may be helpful in thissituation, but only if it can be performed prompt-ly. If intubation is unsuccessful, an emergencytracheostomy is indicated, followed by operativerepair. However, a tracheostomy, when done un-der emergency conditions, is difcult to perform,may be associated with profuse bleeding, andmay be time-consuming. Surgical cricothyroid-otomy, although not preferred for this situation,may be a lifesaving option.
Penetrating trauma to the larynx or trachea isovert and requires immediate attention. Com-
plete tracheal transection or occlusion of theairway with blood or soft tissue can cause acuteairway compromise that requires immediatecorrection. These injuries are often associatedwith esophageal, carotid artery, or jugular veintrauma, as well as extensive tissue destructionsurrounding the area due to blast effect.
Noisy breathing indicates partial airway ob-struction that suddenly may become complete.Absence of breathing suggests that completeobstruction already exists. When the level ofconsciousness is depressed, detection of signi-
cant airway obstruction is more subtle. Laboredrespiratory effort may be the only clue to airwayobstruction and tracheobronchial injury.
If a fracture of the larynx is suspected, based onthe mechanism of injury and subtle physical nd-ings, computed tomography (CT) may help toidentify this injury.
During initial assessment of the airway, the “talk-ing patient” provides reassurance (at least for themoment) that the airway is patent and not com-
promised. Therefore, the most important earlymeasure is to talk to the patient and stimulate averbal response. A positive, appropriate verbal
response indicates that the airway is patent, ven-tilation is intact, and brain perfusion is adequate.Failure to respond or an inappropriate responsesuggests an altered level of consciousness orairway/ventilatory compromise.
B. Objective Signs—Airway Obstruction
1. Look to see if the patient is agitated or ob-tunded. Agitation suggests hypoxia, and obtun-dation suggests hypercarbia. Cyanosis indicateshypoxemia due to inadequate oxygenation andshould be sought by inspection of the nail beds
and circumoral skin. Look for retractions and theuse of accessory muscles of ventilation that, whenpresent, provide additional evidence of airwaycompromise.
2. Listen for abnormal sounds. Noisy breath-ing is obstructed breathing. Snoring, gurgling,and crowing sounds (stridor) may be associatedwith partial occlusion of the pharynx or larynx.Hoarseness (dysphonia) implies functional, la-ryngeal obstruction. The abusive or belligerentpatient may be hypoxic and should not be pre-sumed to be intoxicated.
3. Feel for location of the trachea and quicklydetermine if the trachea is midline.
III. VENTILATION
A. Problem Recognition
Assuring a patent airway is an important rst stepin providing oxygen to the patient but it is only arst step. An unobstructed airway is not likely tobenet the patient unless the patient also is ventilat-ing adequately. Ventilation may be compromised
by airway obstruction but also by altered ventila-tory mechanics or central nervous system (CNS)depression. If breathing is not improved by clearingthe airway, other etiologies must be sought. Directtrauma to the chest, especially with rib fractures,causes pain with breathing and leads to rapid, shal-low ventilation and hypoxemia. Elderly patientsand those with preexisting pulmonary dysfunctionare at signicant risk for ventilatory failure underthese circumstances. Intracranial injury may causeabnormal patterns of breathing and compromise

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 4/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
44 American College of Surgeons
adequacy of ventilation. Cervical spinal cord injurymay result in diaphragmatic breathing and interferewith the ability to meet increased oxygen demands.
Complete cervical cord transection, which sparesthe phrenic nerves (C-3, 4), results in abdominalbreathing and paralysis of the intercostal muscles.Assisted ventilation may be required.
B. Objective Signs—Inadequate Ventilation
1. Look for symmetrical rise and fall of the chestand adequate chest wall excursion. Asymmetrysuggests splinting or a ail chest and any laboredbreathing should be regarded as an imminentthreat to the patient’s oxygenation.
2. Listen for movement of air on both sides ofthe chest. Decreased or absent breath soundsover one or both hemithoraces should alert theexaminer to the presence of thoracic injury. (SeeChapter 4, Thoracic Trauma.) Beware of a rapidrespiratory rate—tachypnea may indicate airhunger.
3. Use a pulse oximeter. This device gives infor-mation regarding the patient’s oxygen saturationand peripheral perfusion, but does not assureadequate ventilation.
IV. MANAGEMENTThe assessment of airway patency and adequacy ofventilation must be done quickly and accurately.Pulse oximetry is essential. If problems are identiedor suspected, measures should be instituted imme-diately to improve oxygenation and reduce the riskof further ventilatory compromise. These includeairway maintenance techniques, denitive airwaymeasures (including surgical airway), and methodsto provide supplemental ventilation. Because all ofthese may require some neck motion, protection ofthe cervical spine must be provided in all patients,
especially if the patient has a known, unstable cer-vical spine injury or is incompletely evaluated andat risk. The spinal cord must be protected until thepossibility of a spinal injury has been excluded byclinical assessment and appropriate x-ray studies.
Patients wearing a helmet and requiring airwaymanagement should have the head and neck heldin a neutral position while the helmet is removed.This is a 2-person procedure. One person providesin-line manual immobilization from below while the
second person expands the helmet laterally and re-moves it from above. In-line manual immobilizationis reestablished from above and the patient’s head
and neck are secured during airway management.Removal of the helmet using a cast cutter while sta-bilizing the head and neck minimizes cervical spinemotion in the patient with a known cervical spineinjury.
Supplemental oxygen should be provided beforeand immediately after airway management mea-sures are instituted. A rigid suction device is essen-tial and should be readily available. Patients withfacial injuries may have associated cribriform platefractures and the use of soft suction catheters (or na-sogastric tube) inserted through the nose may result
in passage of the tube into the cranial vault.
A. Airway Maintenance Techniques
The tongue may fall backward and obstruct thehypopharynx if the patient has a decreased level ofconsciousness. This form of obstruction can be cor-rected readily by the chin-lift or jaw-thrust maneu-ver. The airway can then be maintained with an oro-pharyngeal or nasopharyngeal airway. Maneuversemployed to establish an airway might produce oraggravate cervical spine injury. Therefore, in-lineimmobilization of the cervical spine is essential dur-
ing these procedures.
1. Chin lift
The ngers of 1 hand are placed under the man-dible, which is gently lifted upward to bring thechin anterior. The thumb of the same hand lightlydepresses the lower lip to open the mouth. Thethumb also may be placed behind the lower inci-sors and, simultaneously, the chin gently lifted.The chin-lift maneuver should not hyperextendthe neck. This maneuver is useful for the traumavictim because it does not risk compromising a
possible cervical spine fracture or converting afracture without cord injury into one with cordinjury.
2. Jaw thrust
The jaw-thrust maneuver is performed by grasp-ing the angles of the lower jaw, one hand on eachside, and displacing the mandible forward. Whenthis method is used with the face mask of a bag-valve device, a good seal and adequate ventila-tion are achieved.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 5/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 45
3. Oropharyngeal airway
The oral airway is inserted into the mouth behindthe tongue. The preferred technique is to use atongue blade to depress the tongue and then in-sert the airway posteriorly. The airway must notpush the tongue backward and block, rather thanclear, the airway. This device must not be used inthe conscious patient because it may induce gag-ging, vomiting, and aspiration.
An alternative technique is to insert the oral air-way upside down, so its concavity is directed up-ward, until the soft palate is encountered. At thispoint, with the device rotated 180°, the concavityis directed caudad and the device is slipped intoplace over the tongue. This method should not beused for children, because the rotation of the de-vice may damage the mouth and pharynx.
4. Nasopharyngeal airway
The nasopharyngeal airway is inserted in 1 nostriland passed gently into the posterior oropharynx.The nasopharyngeal airway is preferred to theoropharyngeal airway in the responsive patientbecause it is better tolerated and less likely toinduce vomiting. It should be well lubricated,then inserted into the nostril that appears to beunobstructed. If obstruction is encountered dur-ing introduction of the airway, stop and try theother nostril. If the tip of the nasopharyngealtube is visible in the posterior oropharynx, it mayprovide safe passage of a nasogastric tube in thepatient with facial fractures.
5. Multilumen esophageal airway device
The multilumen esophageal airway device is usedby some prehospital personnel to achieve an air-way when a denitive airway is not feasible. Oneof the ports communicates with the esophagusand one with the airway. The personnel who usethese tubes are trained to observe which one is oc-cluding the esophagus and which will provide airto the trachea. The esophageal port is occluded bya balloon and the other port ventilated. A CO
2 de-
tector improves the accuracy with this apparatus.The multilumen esophageal airway device mustbe removed and/or a denitive airway providedby the doctor after appropriate assessment of theneeds of the patient.
6. Laryngeal mask airway (LMA)
The LMA does not provide a denitive airway.Proper placement of this device is difcult with-out appropriate training. Its role in the resuscita-tion of the injured patient has not been dened.When a patient has an LMA in place on arrivalin the emergency department, the doctor mustdecide after immediate assessment whether re-moval or replacement with an endotracheal tubeis necessary.
B. Denitive Airway
A denitive airway requires a tube present in thetrachea with the cuff inated, the tube connectedto some form of oxygen-enriched assisted ventila-tion, and the airway secured in place with tape.Denitive airways are of 3 varieties: orotrachealtube, nasotracheal tube, and surgical airway (cri-cothyroidotomy or tracheostomy). The decision toprovide a denitive airway is based on clinical nd-ings and includes (1) presence of apnea; (2) inabilityto maintain a patent airway by other means; (3) needto protect the lower airway from aspiration of bloodor vomitus; (4) impending or potential compromiseof the airway, eg, following inhalation injury, facialfractures, retropharyngeal hematoma, or sustainedseizure activity; (5) presence of a closed head injury
requiring assisted ventilation (GCS Score <8); and(6) inability to maintain adequate oxygenation byface-mask oxygen supplementation. (See Table 1,Indication for Denitive Airway, page 46.)
The urgency of the situation and circumstances de-termining the need for airway intervention dictatethe specic route and method to be used. Continuedassisted ventilation is aided by supplemental seda-tion, analgesics, or muscle relaxants, as indicated.The use of a pulse oximeter may be helpful in deter-mining the need for a denitive airway, the urgencyof the need, and, by inference, the effectiveness of
airway placement. Orotracheal and nasotracheal in-tubations are the methods used most frequently. Thepotential for concomitant c-spine injury is of majorconcern in the patient requiring an airway. Figure 1,Airway Algorithm, page 47, provides a scheme bywhich decisions for the appropriate route of airwaymanagement can be made.
C. Denitive Airway—Endotracheal Intubation
It is important to establish the presence or absence ofa cervical spine fracture. However, obtaining c-spine

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 6/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
46 American College of Surgeons
Table 1—Indications for Denitive Airway
NEED FOR AIRWAYPROTECTION NEED FOR VENTILATION
Unconscious Apnea• Neuromuscular paralysis• Unconscious
Severe maxillofacial fractures Inadequate respiratory efforts• Tachypnea• Hypoxia• Hypercarbia• Cyanosis
Risk for aspiration• Bleeding• Vomiting
Severe, closed head injury with needfor brief hyperventilation if acuteneurologic deterioration occurs
Risk for obstruction• Neck hematoma• Laryngeal, tracheal injury• Stridor
x-rays should not impede or delay establishing a de-nitive airway when one is clearly indicated. Thepatient who has a GCS Score of 8 or less requiresprompt intubation. If there is no immediate needfor intubation, x-ray of the cervical spine may beobtained. However, a normal lateral cervical spine
lm does not exclude a c-spine injury.
Note: The most important determinant of whetherto proceed with orotracheal or nasotracheal intu-bation is the experience of the doctor. Both tech-niques are safe and effective when performedproperly. Esophageal occlusion by cricoid pressureis useful in preventing aspiration and providing bet-ter visualization of the airway.
If the decision is made that orotracheal intubation isindicated, the 2-person technique with in-line cervi-cal spine immobilization should be used. If the pa-
tient is apneic, orotracheal intubation is indicated.
Following insertion of the orotracheal tube, the cuffshould be inated and assisted ventilation shouldbe instituted. Proper placement of the tube is sug-gested but not conrmed by hearing equal breathsounds bilaterally and detecting no borborygmi inthe epigastrium. The presence of gurgling noises inthe epigastrium with inspiration suggests esopha-geal intubation and warrants repositioning of thetube. A carbon dioxide (CO
2) detector (colorimetric
CO2 monitoring device) is indicated to help conrm
proper intubation of the airway. The presence ofCO
2 in exhaled air is an indication that the airway
has been successfully intubated, but does not assurethe correct position of the endotracheal tube. If CO
2
is not detected, esophageal intubation has occurred.
Proper position of the tube is best conrmed bychest x-ray, once the possibility of esophageal intu-bation is excluded. Colorimetric CO
2 indicators are
not useful for physiologic monitoring or assessingthe adequacy of ventilation. When the proper posi-tion of the tube is determined, it should be securedin place. If the patient is moved, tube placementshould be reassessed by auscultation of both laterallung elds for equality of breath sounds and by re-assessing for exhaled CO
2.
Nasotracheal intubation is a useful technique whenurgency of airway management precludes a cervical
spine x-ray. Blind nasotracheal intubation requiresspontaneous breathing. It is contraindicated in theapneic patient. The deeper the patient breathes, theeasier it is to follow the airow through the larynx.Facial, frontal sinus, basilar skull, and cribriformplate fractures are relative contraindications to na-sotracheal intubation. Evidence of nasal fracture,raccoon eyes, Battle sign, and possible cerebrospinaluid leaks (rhinorrhea or otorrhea) identify patientswith these injuries. Precautions regarding cervicalspine immobilization should be followed as withorotracheal intubation.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 7/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 47
FIGURE 1
Airway Algorithm
�
�
�
Patients who arrive at the hospital with an endotra-cheal tube in place must have the proper positionof the tube conrmed. This is important because thetube may have been inserted into the esophagus, amainstem bronchus, or dislodged during patient
transport from the eld or another hospital. A chestx-ray, CO2 monitoring, and physical examination
are essential to assess the position of the tube. Car-bon dioxide in the exhaled air will conrm that thetube is in the airway.
Patients with a cervical spine injury, severe arthri-tis of the cervical spine, a short muscular neck, ormaxillofacial/mandibular injury may be technicallydifcult to intubate. The use of a exible beropticendoscope may facilitate these difcult intubations.
The use of anesthetic, sedative, and neuromuscular-blocking drugs for endotracheal intubation in thetrauma patient is risky. In certain cases the needfor an airway justies the risk of these drugs. Thedoctor who uses these drugs must understand their
pharmacology, be skilled in the techniques of endo-tracheal intubation, and be able to obtain a surgicalairway if necessary. In many cases where an airwayis acutely needed during the primary survey, the useof paralyzing or sedating drugs is not necessary.
The technique for rapid-sequence intubation is asfollows:
1. Be prepared to perform a surgical airway inthe event that airway control is lost

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 8/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
48 American College of Surgeons
2. Preoxygenate the patient with 100% oxygen.
3. Apply pressure over the cricoid cartilage.
4. Administer a sedative (eg, etomidate, 0.3mg/kg or 30 mg, or midazolam 2 to 5 mg intrave-nously)
5. Administer 1 to 2 mg/kg succinylcholine in-travenously (usual dose, 100 mg).
6. After the patient relaxes, intubate the patientorotracheally.
7. Inate the cuff and conrm tube placement(auscultate the patient’s chest and determinepresence of CO
2 in exhaled air).
8. Release cricoid pressure.
9. Ventilate the patient.
Etomidate does not have a signicant effect on theblood or intracranial pressure. This drug does pro-vide adequate sedation, which is advantageous inthese patients. Etomidate or other sedatives must beused with great care to avoid loss of the airway asthe patient becomes sedated. Then, succinylcholine,which is a short-acting drug, should be adminis-tered. It has a rapid onset of paralysis of less than1 minute and duration of about 5 minutes or less.
The most dangerous complication of using sedationand neuromuscular blocking agents is the inabilityto establish an airway. If endotracheal intubation isunsuccessful, the patient must be ventilated with abag-valve-mask device until the paralysis resolves.Long-acting drugs are not used for this reason.Succinylcholine should not be used because of thepotential for severe hyperkalemia in the patient withpreexisting chronic renal failure, chronic paralysis,or chronic neuromuscular disease.
Induction agents, such as thiopental and sedatives,are dangerous to use in the hypovolemic trauma
patient. Small doses of diazepam or midazolamare appropriate to reduce anxiety in the paralyzedpatient. Flumazenil must be available to reverse thesedative effects after benzodiazepines have beenadministered. Practice patterns, drug preferences,and specic procedures for airway managementvary between institutions. The principle that the in-dividual utilizing these techniques be skilled in theiruse, knowledgeable of the inherent pitfalls associ-ated with rapid sequence intubation, and capableof managing the potential complications cannot beoverstated.
D. Denitive Airway—Surgical Airway
Inability to intubate the trachea is a clear indication
for creating a surgical airway. A surgical airway isperformed when edema of the glottis, fracture ofthe larynx, or severe oropharyngeal hemorrhageobstructs the airway and an endotracheal tube can-not be placed through the cords. A surgical cricothy-roidotomy is preferable to a tracheostomy for mostpatients requiring an emergency surgical airway. Asurgical cricothyroidotomy is easier to perform, isassociated with less bleeding, and requires less timeto perform than an emergency tracheostomy.
1. Jet insufation of the airway (See SkillsStation III, Cricothyroidotomy)
Insertion of a needle through the cricothyroidmembrane or into the trachea is a useful tech-nique in emergency situations that providesoxygen on a short-term basis until a denitiveairway can be placed. Jet insufation can providetemporary, supplemental oxygenation so thatintubation can be accomplished on an urgentrather than an emergent basis. The jet insufa-tion technique is performed by placing a large-caliber plastic cannula, #12- to #14-gauge (#16- to#18-gauge in children), through the cricothyroidmembrane into the trachea below the level of the
obstruction. The cannula is then connected towall oxygen at 15 L/minute (40 to 50 psi) witheither a Y-connector or a side hole cut in the tub-ing attached between the oxygen source and theplastic cannula. Intermittent insufation, 1 sec-ond on and 4 seconds off, can then be achievedby placing the thumb over the open end of theY-connector or the side hole. The patient can beadequately oxygenated for only 30 to 45 minutesusing this technique. However, only patients withnormal pulmonary function who do not have asignicant chest injury can be ventilated in thismanner. During the 4 seconds that the oxygen is
not being delivered under pressure, some exhala-tion occurs. Because of the inadequate exhalation,CO
2 slowly accumulates and limits the use of this
technique, especially in head-injured patients.
Jet insufation must be used with caution whencomplete foreign body obstruction of the glotticarea is suspected. Although high pressure mayexpel the impacted material into the hypophar-ynx where it can be readily removed, signicantbarotrauma may occur, including pulmonary

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 9/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 49
rupture with tension pneumothorax. Low owrates (5 to 7 L/minute) should be used when per-sistent glottic obstruction is present.
2. Surgical cricothyroidotomy (See Skills StationIII, Cricothyroidotomy)
Surgical cricothyroidotomy is performed bymaking a skin incision that extends through thecricothyroid membrane. A curved hemostat maybe inserted to dilate the opening, and a small en-dotracheal tube or tracheostomy tube (preferably5 to 7 mm OD) can be inserted. When the endotra-cheal tube is used, the cervical collar can be reap-plied. One must be alert to the possibility that theendotracheal tube can become malpositioned andis easily advanced into a bronchus. Care must betaken, especially with children, to avoid damageto the cricoid cartilage, which is the only circum-ferential support to the upper trachea. Therefore,surgical cricothyroidotomy is not recommendedfor children under 12 years of age. (See Chapter10, Extremes of Age: A. Pediatric Trauma.)
In recent years percutaneous tracheostomy hasbeen reported as an alternative to open trache-ostomy. This is not a safe procedure in the acutetrauma situation, because the patient’s neck mustbe hyperextended to properly position the headto perform the procedure safely. Percutane-ous tracheostomy requires the use of a heavyguidewire and sharp dilator, or a guidewire andmultiple dilators. This may be dangerous and/ortime-consuming, depending on the type of equip-ment used.
E. Airway Decision Scheme
The airway decision scheme (Figure 1, Airway Al-gorithm, page 47) applies only to the patient who isin acute respiratory distress (or apneic) and in needof an immediate airway, and in whom a cervicalspine injury is suspected by mechanism of injury orphysical examination. The rst priority is to assurecontinued oxygenation with maintenance of cervicalspine immobilization. This is accomplished initiallyby position (ie, chin lift or jaw thrust) and prelimi-nary airway techniques (ie, oropharyngeal airwayor nasopharyngeal airway) already discussed.
In the patient who is still showing some respira-tory effort, a nasotracheal tube may be passed ifthe doctor is skilled in this technique. Otherwise, an
orotracheal tube should be passed while a secondperson provides in-line immobilization. If neither anasotracheal nor an orotracheal tube can be inserted
and the patient’s respiratory status is in jeopardy, acricothyroidotomy should be performed.
In the apneic patient, in-line immobilization shouldbe maintained by 1 person and orotracheal intuba-tion should be performed by another. If severe max-illofacial injury precludes nasotracheal intubationand orotracheal intubation cannot be achieved forany reason, a cricothyroidotomy is indicated.
Oxygenation and ventilation must be maintainedbefore, during, and immediately upon completionof insertion of the denitive airway. Prolonged peri-ods of inadequate or absent ventilation and oxygen-ation should be avoided.
F. Oxygenation
Oxygenated inspired air is best provided via a tight-tting oxygen reservoir face mask with a ow rateof 11 L/minute. Other methods (eg, nasal catheter,nasal cannula, nonrebreather mask) can improveinspired oxygen concentration.
Because changes in oxygenation occur rapidly andare impossible to detect clinically, pulse oximetryshould be used when difculties are anticipated in
intubation or ventilation. This includes the transportof the critically injured patient. Pulse oximetry is anoninvasive method to continuously measure oxy-gen saturation (O
2 sat) of arterial blood. It does not
measure the partial pressure of oxygen (PaO2) and,
depending on the position of the oxyhemoglobindissociation curve, the PaO
2 may vary widely. (See
Table 2, Approximate PaO2 Versus O
2 Hemoglobin
Saturation Levels, page 50.) However, a measuredsaturation of 95% or greater by pulse oximetry isstrong corroborating evidence of adequate, periph-eral arterial oxygenation (PaO
2 >70 mm Hg or 9.3
kPa). Pulse oximetry requires intact peripheral per-fusion and cannot distinguish oxyhemoglobin fromcarboxyhemoglobin or methemoglobin, which limitsits usefulness in the severely vasoconstricted patientand in the patient with carbon monoxide poison-ing. Profound anemia (hemoglobin <5 g/dL) andhypothermia (<30ºC or 86ºF) decrease the reliabilityof the technique. However, in most trauma patientspulse oximetry is not only useful, but also continu-ous monitoring of oxygen saturation provides animmediate assessment of therapeutic interventions.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 10/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
50 American College of Surgeons
(See Skills Station II, Airway and Ventilatory Man-agement: VII., Pulse, Oximetry Monitoring, at theconclusion of this chapter.)
G. Ventilation
Effective ventilation can be achieved by bag-valve-face mask techniques. However, 1-person ventila-tion techniques, using a bag-valve mask, are lesseffective than 2-person techniques in which bothhands can be used to assure a good seal. Bag-valve-mask ventilation should be performed by 2 peoplewhenever possible.
Intubation of the hypoventilated and/or apneic pa-tient may not be successful initially and may requiremultiple attempts. The patient must be ventilatedperiodically during prolonged efforts to intubate.The doctor should practice taking a deep breathwhen intubation is rst attempted. When the doctormust breathe, the attempted intubation should beaborted and the patient ventilated.
With intubation of the trachea accomplished, as-sisted ventilation should follow using positive-pres-sure breathing techniques. A volume- or pressure-regulated respirator can be used, depending onavailability of the equipment. The doctor should bealert to the complications secondary to changes inintrathoracic pressure, which can convert a simplepneumothorax to a tension pneumothorax, or evencreate a pneumothorax secondary to barotrauma.
H. Pitfalls
1. The inability to intubate the patient expedi-ently or to provide a surgical airway results in
hypoxia and patient deterioration. Rememberthat performing a needle cricothyroidotomy with
jet insufation may provide the time necessary to
establish a denitive airway.2. Trauma patients may vomit and aspirate.Functional suction equipment must be immedi-ately available, and the doctor should ensure asecure, patent airway in all trauma patients.
3. Gastric distention may occur when ventilatingthe patient with a bag-valve-mask device, whichmay result in the patient vomiting and aspirat-ing. It also may cause distention of the stomachagainst the vena cava, resulting in hypotensionand bradycardia.
4. Equipment failure may occur at the most inop-portune time and cannot always be anticipated,eg, the light on the laryngoscope burns out, the la-ryngoscope batteries are weak, the endotrachealtube cuff leaks, or the pulse oximeter does notfunction properly.
V. SUMMARY
A. Actual or impending airway obstruction shouldbe suspected in all injured patients.
B. With all airway maneuvers, the cervical spinemust be protected by in-line immobilization.
C. Clinical signs suggesting airway compromiseshould be managed by securing a patent airway andproviding adequate oxygen-enriched ventilation.
Table 2—Approximate PaO2 Versus O
2 Hemoglobin Saturation Levels
PaO2 LEVELS
O2 HEMOGLOBIN
SATURATION LEVELS
90 mm Hg 100%
60 mm Hg 90%
30 mm Hg 60%
27 mm Hg 50%

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 11/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 51
D. A denitive airway should be inserted if there isany doubt on the part of the doctor as to the integrityof the patient’s airway.
E. A denitive airway should be placed early afterthe patient has been ventilated with oxygen-en-riched air, and prolonged periods of apnea must beavoided.
F. Airway management requires assessment andreassessment of airway patency, tube position, andventilatory effectiveness.
G. The selection of orotracheal or nasotrachealroutes for intubation is based on the experience andskill level of the doctor.
H. Surgical airway is indicated whenever an airwayis needed and intubation is unsuccessful.
BIBLIOGRAPHY
1. Aprahamian C, Thompson BM, Finger WA, etal: Experimental cervical spine injury model:evaluation of airway management and splint-ing techniques. Annals of Emergency Medicine1984; 13(8):584–587.
2. Bergen JM, Smith DC: A review of etomidatefor rapid sequence intubation in the emergency
department. Journal of Emergency Medicine 1997; 15(2): 221–230.
3. Brantigan CO, Grow JB Sr: Cricothyroidotomy:Elective use in respiratory problems requiringtracheotomy. Journal of Thoracic and Cardio-vascular Surgery 1976; 71:72–81.
4. Danzl DF, Thomas DM: Nasotracheal intuba-tion in the emergency department. Critical CareMedicine 1980; 8(11):667–682.
5. Frame SB, Simon JM, Kerstein MD, et al: Per-cutaneous transtracheal catheter ventilation(PTCV) in complete airway obstructions canine
model. Journal of Trauma 1989; 29(6):774–781.
6. Fremstad JD, Martin SH: Lethal complicationfrom insertion of nasogastric tube after severebasilar skull fracture. Journal of Trauma 1978;18:820–822.
7. Guildner CV: Resuscitation—opening the air-way. A comparative study of techniques foropening an airway obstructed by the tongue.
Journal of American College of EmergencyPhysicians 1976; 5:588–590.
8. Iserson KV: Blind nasotracheal intubation. An-nals of Emergency Medicine 1981; 10:468.
9. Jorden RC, Moore EE, Marx JA, et al: A compari-son of PTV and endotracheal ventilation in anacute trauma model. Journal of Trauma 1985;25(10):978–983.
10. Kress TD, et al: Cricothyroidotomy. Annals ofEmergency Medicine 1982; 11:197.
11. Levinson MM, Scuderi PE, Gibson RL, et al:Emergency percutaneous and transtrachealventilation. Journal of American College ofEmergency Physicians 1979; 8(10):396–400.
12. Majernick TG, Bieniek R, Houston JB, et al:Cervical spine movement during orotracheal in-tubation. Annals of Emergency Medicine 1986;15(4):417–420.
13. Seshul MB Sr, Sinn DP, Gerlock AJ Jr: The AndyGump fracture of the mandible: a cause of re-spiratory obstruction or distress. Journal ofTrauma 1978; 18:611–612.
14. Walter J, Doris PE, Shaffer MA: Clinical pre-sentation of patients with acute cervical spineinjury. Annals of Emergency Medicine 1984;13(7):512–515.
15. Yeston NS: Noninvasive measurement of bloodgases. Infections in Surgery 1990; 90:18–24.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 12/28
CHAPTER 2
AIRWAY AND VENTILATORY MANAGEMENT
52 American College of Surgeons

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 13/28
Advanced Trauma Life Support 53
SKILLS STATION II
II Airway and Ventilatory Management
SKILLS STATION
OBJECTIVES:
Performance at this station will allow the participant to evaluate a series of clinical situations and to acquirethe cognitive skills related to decision making in airway and ventilatory management. The student will prac-tice and demonstrate the following skills on adult and infant intubation manikins.
1. Insert oral and nasal pharyngeal airways.
2. Using both oral and nasal routes, intubate the trachea of an adult intubation manikin (within the guide-lines listed), provide effective ventilation, and utilize the CO
2 colorimetric device to aid in determining
proper placement of the endotracheal tube.
3. Intubate the trachea of an infant intubation manikin with an endotracheal tube within the guidelineslisted, and provide effective ventilation.
4. Relate the indications of trauma to airway management when performing oral endotracheal intubationand nasotracheal intubation.
5. Using a pulse oximeter:
a. Discuss the purpose of pulse oximetry monitoring.
b. Demonstrate the proper use of the device.
c. Discuss the indications for its use, its functional limits of accuracy, and reasons for malfunction orinaccuracy.
d. Interpret accurately the pulse oximeter monitor readings and relate their signicance to the care ofthe trauma patient.
PROCEDURES:Eight procedures for acute airway management are outlined in Skills Station II:
1. Oropharyngeal airway insertion
2. Nasopharyngeal airway insertion
3. Ventilation without intubation
4. Orotracheal intubation
5. Nasotracheal intubation

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 14/2854 American College of Surgeons
SKILLS STATION II
6. Infant endotracheal intubation
7. Pulse oximetry
8. Carbon dioxide detection

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 15/28
CHAPTER 2—SKILLS STATION II
Airway and Ventilatory Management AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 55
INTERACTIVE SKILLS PROCEDURES
Airway and Ventilatory Management
Note: Standard precautions are required whenever caring for the trauma patient.
Note: Scenarios are incorporated into the performance of some of these skills. The scenarios to be presentedare included at the conclusion of the procedures. (See IX, Skills Scenarios.)
I. OROPHARYNGEAL AIRWAY INSERTION
A. This procedure is for temporary ventilation of the unconscious patient while preparing to intubate thepatient.
B. Select the proper-sized airway. The correctly sized airway will extend from the corner of the patient’smouth to the external auditory canal.
C. Open the patient’s mouth with either the chin-lift maneuver or the crossed-nger technique (scissorstechnique).
D. Insert a tongue blade on top of the patient’s tongue far enough back to depress the tongue adequately,being careful not to gag the patient.
E. Insert the airway posteriorly, gently sliding the airway over the curvature of the tongue until the device’sange rests on top of the patient’s lips. The airway must not push the tongue backward and block the air-way.
F. Remove the tongue blade.
G. Ventilate the patient with a bag-valve-mask device.
II. NASOPHARYNGEAL AIRWAY INSERTION
A. This procedure is used when the patient would gag on an oropharyngeal airway.
B. Assess the nasal passages for any apparent obstruction (eg, polyps, fractures, hemorrhage).
C. Select the appropriately sized airway.
D. Lubricate the nasal pharyngeal airway with a water-soluble lubricant or tap water.
E. Insert the tip of the airway into the nostril and direct it posteriorly and toward the ear.
F. Gently insert the nasal pharyngeal airway through the nostril into the hypopharynx with a slight rotatingmotion, until the ange rests against the nostril.
G. Ventilate the patient with a bag-valve-mask device.
III. BAG-VALVE-MASK VENTILATION—2-PERSON TECHNIQUE
A. Select the appropriately sized mask to t the patient’s face.
B. Connect the oxygen tubing to the bag-valve device, and adjust the ow of oxygen to 12 L/minute.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 16/28
CHAPTER 2—SKILLS STATION II
AIRWAY AND VENTILATORY MANAGEMENT Airway and Ventilatory Management
56 American College of Surgeons
C. Assure that the patient’s airway is patent and secured by previously described techniques.
D. The rst person applies the mask to the patient’s face, ascertaining a tight seal with both hands.
E. The second person ventilates the patient by squeezing the bag with both hands.
F. The adequacy of ventilation is assessed by observing the patient’s chest movement.
G. The patient should be ventilated in this manner every 5 seconds.
IV. ADULT OROTRACHEAL INTUBATION
A. Assure that adequate ventilation and oxygenation are in progress, and that suctioning equipment is im-mediately available in the event that the patient vomits.
B. Inate the cuff of the endotracheal tube to ascertain that the balloon does not leak, then deate the cuff.
C. Connect the laryngoscope blade to the handle, and check the bulb for brightness.
D. Have an assistant manually immobilize the head and neck. The patient’s neck must not be hyperextendedor hyperexed during this procedure.
E. Hold the laryngoscope in the left hand.
F. Insert the laryngoscope into the right side of the patient’s mouth, displacing the tongue to the left.
G. Visually identify the epiglottis and then the vocal cords.
H. Gently insert the endotracheal tube into the trachea without applying pressure on the teeth or oral tis-sues.
I. Inate the cuff with enough air to provide an adequate seal. Do not overinate the cuff.
J. Check the placement of the endotracheal tube by bag-valve-to-tube ventilation.
K. Visually observe chest excursions with ventilation.
L. Auscultate the chest and abdomen with a stethoscope to ascertain tube position.
M. Secure the tube. If the patient is moved, the tube placement should be reassessed.
N. If endotracheal intubation is not accomplished within seconds or in the same time required to hold yourbreath before exhaling, discontinue attempts, ventilate the patient with a bag-valve-mask device, and tryagain.
O. Placement of the tube must be checked carefully. A chest x-ray is helpful to assess the position of the tube,
but it cannot exclude esophageal intubation.
P. Attach a CO2 colorimetric device to the endotracheal tube between the adapter and the ventilating device.
Use of the colorimetric device provides a reliable means of conrming the position of the endotracheal tubein the airway.
Q. Attach a pulse oximeter device to one of the patient’s ngers (intact peripheral perfusion must exist) tomeasure and monitor the patient’s oxygen saturation levels. Pulse oximetry is useful to monitor oxygen satu-ration levels continuously and provides an immediate assessment of therapeutic interventions.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 17/28
CHAPTER 2—SKILLS STATION II
Airway and Ventilatory Management AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 57
V. ADULT NASOTRACHEAL INTUBATION
Remember: Blind nasotracheal intubation is contraindicated in the apneic patient and whenever severe mid-
face fractures or suspicion of basilar skull fracture exist.
A. If a cervical spine fracture is suspected, leave the cervical collar in place to assist in maintaining immobi-lization of the neck.
B. Assure that adequate ventilation and oxygenation are in progress.
C. Inate the cuff of the endotracheal tube to ascertain that the balloon does not leak, then deate the cuff.
D. If the patient is conscious, spray the nasal passage with an anesthetic and vasoconstrictor to anesthetizeand constrict the mucosa. If the patient is unconscious, it is adequate to spray the nasal passage only with avasoconstrictor.
E. Have an assistant maintain manual immobilization of the head and neck.
F. Lubricate the nasotracheal tube with a local anesthetic jelly and insert the tube into the nostril.
G. Guide the tube slowly but rmly into the nasal passage, going up from the nostriI (to avoid the large infe-rior turbinate) and then backward and down into the nasopharynx. The curve of the tube should be alignedto facilitate passage along this curved course.
H. As the tube passes through the nose and into the nasopharynx, it must turn downward to pass throughthe pharynx.
I. Once the tube has entered the pharynx, listen to the airow emanating from the endotracheal tube. Ad-vance the tube until the sound of the moving air is maximal, suggesting location of the tip at the opening ofthe trachea. While listening to air movement, determine the point of inhalation and advance the tube quickly.If tube placement is unsuccessful, repeat the procedure by applying gentle pressure on the thyroid cartilage.
Remember, intermittently ventilate and oxygenate the patient.
J. Inate the cuff with enough air to provide an adequate seal. Avoid overination.
K. Check the placement of the endotracheal tube by bag-valve-to-tube ventilation.
L. Visually observe chest excursion with ventilation.
M. Auscultate the chest and abdomen with a stethoscope to ascertain tube position.
N. Secure the tube. If the patient is moved, the tube placement should be reassessed.
O. If endotracheal intubation is not accomplished within 30 seconds or in the same time required to holdyour breath before exhaling, discontinue attempts, ventilate the patient with a bag-valve-mask device, and
try again.
P. Placement of the tube must be checked carefully. A chest x-ray may be helpful to assess the position of thetube, but it cannot exclude esophageal intubation.
Q. Attach a CO2 colorimetric device to the endotracheal tube, between the adapter and the ventilating device.
The use of this device provides a reliable means of conrming the position of the endotracheal tube in thetrachea.
R. Attach a pulse oximeter device to one of the patient’s ngers (intact peripheral perfusion must exist) tomeasure and monitor the patient’s oxygen saturation levels. Pulse oximetry is useful to monitor oxygen satu-ration levels continuously, and provides an immediate assessment of therapeutic interventions.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 18/28
CHAPTER 2—SKILLS STATION II
AIRWAY AND VENTILATORY MANAGEMENT Airway and Ventilatory Management
58 American College of Surgeons
Complications of Orotracheal and Nasotracheal Intubation
1. Esophageal intubation, leading to hypoxia and death
2. Right mainstem bronchus intubation, resulting in ventilation of the right lung only, collapse of the left lung 3. Inability to intubate, leading to hypoxia and death
4. Induction of vomiting, leading to aspiration, hypoxia, and death
5. Trauma to the airway, resulting in hemorrhage and potential aspiration
6. Chipping or loosening of the teeth (caused by levering of the laryngoscope blade against the teeth)
7. Rupture leak of the endotracheal tube cuff, resulting in loss of seal during ventilation, and necessitating reintuba-tion
8. Conversion of a cervical vertebral injury without neurologic decit to a cervical cord
9. Injury with neurologic decit
VI. INFANT OROTRACHEAL INTUBATION
A. Ensure that adequate ventilation and oxygenation are in progress.
B. Select the proper-sized uncuffed tube, which should be the same size as the infant’s nostril or little n-ger.
C. Connect the laryngoscope blade and handle; check the light bulb for brilliance.
D. Hold the laryngoscope in the left hand.
E. Insert the laryngoscope blade in the right side of the mouth, moving the tongue to the left.
F. Observe the epiglottis, then the vocal cords.
G. Insert the endotracheal tube not more than 2 cm past the cords.
H. Check the placement of the tube by bag-valve-to-tube ventilation.
I. Check the placement of the endotracheal tube by observing lung inations and auscultating the chest andabdomen with a stethoscope.
J. Secure the tube. If the patient is moved, the tube placement should be reassessed.
K. If endotracheal intubation is not accomplished within 30 seconds or in the same time required to holdyour breath before exhaling, discontinue attempts, ventilate the patient with a bag-valve-mask device, andtry again.
L. Placement of the tube must be checked carefully. A chest x-ray may be helpful to assess the position of thetube, but it cannot exclude esophageal intubation.
M. Attach a CO2colorimetric device to the endotracheal tube, between the adapter and the ventilating device.
The use of this device provides a reliable means of conrming the position of the endotracheal tube in thetrachea.
N. Attach a pulse oximeter device to one of the patient’s ngers (intact peripheral perfusion must exist) tomeasure and monitor the patient’s oxygen saturation levels. Pulse oximetry is useful to monitor oxygen satu-ration levels continuously, and provides an immediate assessment of therapeutic interventions.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 19/28
CHAPTER 2—SKILLS STATION II
Airway and Ventilatory Management AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 59
VII. PULSE OXIMETRY MONITORING
The pulse oximeter is designed to measure oxygen saturation and pulse rate in peripheral circulation. This
device is a microprocessor that calculates the percentage saturation of oxygen in each pulse of arterial bloodthat ows past a sensor. It also calculates the heart rate at the same time.
The pulse oximeter works by a low-intensity light beamed from a light-emitting diode (LED) to a photodiodethat is a light receiver. Two thin beams of light, one red and the other infrared, are transmitted through bloodand body tissue, a portion of which is absorbed by the blood and body tissue. The photodiode measures thatportion of the light that passes through the blood and body tissue. The relative amount of light absorbedby oxygenated hemoglobin differs from that absorbed by nonoxygenated hemoglobin. The microprocessorevaluates these differences in the arterial pulse and reports the values as calculated oxyhemoglobin satura-tion (%SaO
2). Measurements are reliable and correlate well when compared with a cooximeter that directly
measures hemoglobin saturation (SaO2).
The accuracy of the pulse oximeter is unreliable when there is poor peripheral perfusion. This may be due tovasoconstriction, hypotension, a blood pressure cuff that is inated above the sensor, hypothermia, and other
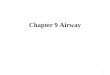
FIGURE 2
PaO2 (mm Hg) and Hemoglobin Saturation Relationship
�
�
�
�
�
�
�
��
�
�

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 20/28
CHAPTER 2—SKILLS STATION II
AIRWAY AND VENTILATORY MANAGEMENT Airway and Ventilatory Management
60 American College of Surgeons
causes for poor blood ow. Severe anemia may likewise inuence the reading. Signicantly high levels ofcarboxyhemoglobin or methemoglobin may cause abnormalities, and circulating dye (eg, indocyanine greenand methylene blue) may interfere with the measurement. Excessive patient movement, other electrical de-
vices, or intense ambient light may cause malfunction of this device.Using a pulse oximeter requires knowledge of the particular device being used. Various sensors are appro-priate for different patients. The ngertip and earlobe are common sites where sensors are applied; however,both of these areas may be subject to vasoconstriction. The ngertip (or toe tip) of an injured extremity orbelow a blood pressure cuff should not be used.
When analyzing results of a pulse oximeter, evaluate the initial readings. Does the pulse rate correspondto the electrocardiogram monitor? Is the oxygen saturation appropriate? If the pulse oximeter is giving lowreadings or if they are very poor readings, look for a physiologic cause, not a mechanical one.
The relationship between partial pressure of oxygen in arterial blood (PaO2) and %SaO
2 is shown in Figure 2,
page 59. The sigmoid shape of this curve indicates that the relationship between %SaO2and PaO
2is nonlinear.
This is particularly important in the middle range of this curve, where small changes in PaO2 will effect large
changes in saturation. Remember, the pulse oximeter measures arterial oxygen saturation, not arterial oxy-gen partial pressure. (See Table 2, Approximate PaO
2 Versus O
2 Hemoglobin Saturation Levels in Chapter 2,
Airway and Ventilatory Management, page 50.)
Standard blood gas measurements report both arterial oxygen pressure (PaO2) and calculated hemoglobin
saturation (%SaO2). When oxygen saturation is calculated from blood gas PaO
2, the calculated value may
differ from the oxygen saturation measured by the pulse oximeter. This difference may occur because anoxygen saturation value that has been calculated from the blood gas PaO
2 has not necessarily been correctly
adjusted for the effects of variables that shift the relationship between PaO2 and saturation. These variables
include temperature, pH, PaCO2 (partial pressure of carbon dioxide), 2,3-dpg (diphosphoglycerates), and the
concentration of fetal hemoglobin.
VIII. END-TIDAL CO2 DETECTORSWhen a patient is intubated, it is essential to check the position of the endotracheal tube. If carbon dioxide isdetected in the exhaled air, the tube is in the airway. Colorimetric end-tidaI CO
2detectors should be readily
available in each emergency department. They can rapidly detect the presence of CO2 in the exhaled air.
Colorimetric devices use a chemically treated indicator strip that generally reects the CO2level. At very low
levels of CO2, eg, atmospheric air, the indicator turns purple. At higher CO
2 1evels, eg, 2% to 5%, the indica-
tor turns yellow. A tan color indicates detection of CO2 levels that are generally lower than those found in the
exhaled tracheal gases.
It is important to note that, on a rare occasion, patients with gastric distention may have elevated CO2 levels
in their esophagus. These elevated levels clear rapidly after several breaths, and the results of this colorimet-ric test should not be used until after at least 6 breaths. If the colorimetric device still shows an intermediate
range, 6 additional breaths should be taken or given. If the patient sustains a cardiac arrest and has no cardiacoutput, CO
2 is not delivered to the lungs. In fact, with cardiac asystole, this may be a way of determining if
cardiopulmonary resuscitation is adequate.
The colorimetric device is not used for the detection of elevated CO2 levels. Similarly, it is not used to detect
a main stem bronchial intubation. Physical examination and a chest x-ray are still required to determine thatthe endotracheal tube is properly positioned in the airway. In a noisy emergency department or when thepatient is transported several times, this device is extremely reliable in differentiating between tracheal andesophageal intubation.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 21/28
CHAPTER 2—SKILLS STATION II
Airway and Ventilatory Management AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 61
IX. SKILLS SCENARIOS
A. Scenario #1
A 22-year-old man is an unrestrained passenger in a motor vehicle that collides head-on into a retaining wall.He has a strong odor of alcohol on his breath. At the time of the collision, he hits the windshield and sustainsa scalp laceration. At the injury scene he is combative and his GCS Score is 11. His blood pressure is 120/70mm Hg, heart rate is 100 beats/minute, and respirations are 20 breaths/minute. A semirigid cervical collaris applied and he is immobilized on a long backboard. He is receiving oxygen via a high-ow oxygen mask.Shortly after his arrival in the emergency department, he begins to vomit.
B. Scenario #2
The patient described in the rst scenario is now unresponsive and is endotracheally intubated. He is beingventilated with 100% oxygen. Part of his evaluation includes a CT scan of his brain. After he is transported toradiology for the scan, the pulse oximeter reveals 82% SaO
2.
C. Scenario #3
A 3-year-old unrestrained, front-seat passenger is injured when the car crashes into a stone wall. The child isunconscious at the injury scene. In the emergency department, bruises to the forehead, face, and chest wallare noted. There is blood around the mouth. Blood pressure is 105/70 mm Hg, heart rate is 120 beats/minute,and respirations are rapid and shallow. The child’s GCS Score is 8.
D. Scenario #4
A 35-year-old man sustains blunt chest trauma during a single motor-vehicle collision. In the emergencydepartment, he is alert and has evidence of a right chest wall contusion. He has point tenderness and fracturecrepitus of several right ribs. His GCS Score is 14. He is immobilized with a semirigid cervical spine collar andis on a long backboard. High-ow oxygen is being administered via a face mask.

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 22/28
CHAPTER 2—SKILLS STATION II
AIRWAY AND VENTILATORY MANAGEMENT Airway and Ventilatory Management
62 American College of Surgeons

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 23/28
Advanced Trauma Life Support 63
SKILLS STATION III
OBJECTIVES:
Performance at this station will allow the student to practice and demonstrate the techniques of needle crico-thyroidotomy and surgical cricothyroidotomy on a live, anesthetized animal; a fresh human cadaver; or ananatomic human body manikin. Specically, the student will be able to:
1. Identify the surface markings and structures to be noted when performing needle and surgical crico-thyroidotomies.
2. Discuss the indications and complications of needle and surgical cricothyroidotomies.
3. Perform needle and surgical cricothyroidotomies on a live, anesthetized animal; a fresh human ca-daver; or an anatomic human body manikin as outlined in this skills station.
PROCEDURES:
1. Needle cricothyroidotomy
2. Surgical cricothyroidotomy
IIICricothyroidotomy
SKILLS STATION

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 24/2864 American College of Surgeons
SKILLS STATION III

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 25/28
CHAPTER 2—SKILLS STATION III
Cricothyroidotomy AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 65
INTERACTIVE SKILLS PROCEDURES
Cricothyroidotomy
Note: Standard precautions are required whenever caring for the trauma patient.
I. NEEDLE CRICOTHYROIDOTOMY
A. Assemble and prepare oxygen tubing by cutting a hole toward one end of the tubing. Connect the otherend of the oxygen tubing to an oxygen source, capable of delivering 50 psi or greater at the nipple, and assurefree ow of oxygen through the tubing.
B. Place the patient in a supine position.
C. Assemble a #12- or #14-gauge, 8.5-cm, over-the-needle catheter to a 6- to 12-mL syringe.
D. Surgically prepare the neck, using antiseptic swabs.
E. Palpate the cricothyroid membrane, anteriorly, between the thyroid cartilage and cricoid cartilage. Stabi-lize the trachea with the thumb and forenger of 1 hand to prevent lateral movement of the trachea duringthe procedure.
F. Puncture the skin in the midline with a #12- or #14-gauge needle attached to a syringe, directly over thecricothyroid membrane (ie, midsagittal). A small incision with a #11 blade facilitates passage of the needlethrough the skin.
G. Direct the needle at a 45º angle caudally, while applying negative pressure to the syringe.
H. Carefully insert the needle through the lower half of the cricothyroid membrane, aspirating as the needleis advanced.
I. Aspiration of air signies entry into the tracheal lumen.
J. Remove the syringe and withdraw the stylet while gently advancing the catheter downward into posi-tion, being careful not to perforate the posterior wall of the trachea.
K. Attach the oxygen tubing over the catheter needle hub, and secure the catheter to the patient’s neck.
L. Intermittent ventilation can be achieved by occluding the open hole cut into the oxygen tubing with yourthumb for 1 second and releasing it for 4 seconds. After releasing your thumb from the hole in the tubing,passive exhalation occurs. Note: Adequate PaO
2 can be maintained for only 30 to 45 minutes, and CO
2 accu-
mulation may occur more rapidly.
M. Continue to observe lung inations and auscultate the chest for adequate ventilation.
Complications of Needle Cricothyroidotomy
1. Inadequate ventilations leading to hypoxia and death
2. Aspiration (blood)
3. Esophageal laceration
4. Hematoma
5. Posterior tracheal wall perforation

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 26/28
CHAPTER 2—SKILLS STATION III
AIRWAY AND VENTILATORY MANAGEMENT Cricothyroidotomy
66 American College of Surgeons
6. Subcutaneous and/or mediastinal emphysema
7. Thyroid perforation
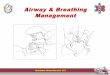
II. SURGICAL CRICOTHYROIDOTOMY (See Figure 3, Surgical Cricothyroidotomy, page 67)
A. Place the patient in a supine position with the neck in a neutral position. Palpate the thyroid notch, crico-thyroid interval, and the sternal notch for orientation. Assemble the necessary equipment.
B. Surgically prepare and anesthetize the area locally, if the patient is conscious.
C. Stabilize the thyroid cartilage with the left hand and maintain stabilization until the trachea is intubated.
D. Make a transverse skin incision over the cricothyroid membrane, and carefully incise through the mem-brane transversely.
E. Insert the scalpel handle into the incision and rotate it 90° to open the airway. (A hemostat or tracheal
spreader also may be used instead of the scalpel handle.)
F. Insert an appropriately sized, cuffed endotracheal tube or tracheostomy tube (usually a #5 or #6) into thecricothyroid membrane incision, directing the tube distally into the trachea.
G. Inate the cuff and ventilate the patient.
H. Observe lung inations and auscultate the chest for adequate ventilation.
I. Secure the endotracheal or tracheostomy tube to the patient to prevent dislodging.
J. Caution: Do not cut or remove the cricoid and/or thyroid cartilages.
Complications of Surgical Cricothyroidotomy 1. Aspiration (eg, blood)
2. Creation of a false passage into the tissues
3. Subglottic stenosis/edema
4. Laryngeal stenosis
5. Hemorrhage or hematoma formation
6. Laceration of the esophagus
7. Laceration of the trachea
8. Mediastinal emphysema
9. Vocal cord paralysis, hoarseness

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 27/28
CHAPTER 2—SKILLS STATION III
Cricothyroidotomy AIRWAY AND VENTILATORY MANAGEMENT
Advanced Trauma Life Support 67
Thyroid notch
Thyroid cartilage
Cricothyroid membrane
Indent
Trachea
Cricoid cartilage
FIGURE 3
Surgical Cricothyroidotomy

7/17/2019 CHAPTER 2 - Airway and Ventilatory Management
http://slidepdf.com/reader/full/chapter-2-airway-and-ventilatory-management 28/28
CHAPTER 2—SKILLS STATION III
AIRWAY AND VENTILATORY MANAGEMENT Cricothyroidotomy