Embed Size (px)
Citation preview
© Macmillan Education Australia 2013 1 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Chapter 14: Anxiety disorder: specific phobia Learning activity suggested answers Learning Activity 14.1 (p. 564) 1 Explain the meaning of the term anxiety.
Explanation should refer to anxiety as:
• a state of physiological arousal,
• associated with feelings of apprehension, worry or uneasiness that something is wrong or that something unpleasant is about to happen.
2 Give an example of when anxiety may be (a) useful and (b) not useful.
Anxiety may be useful in the short term to deal with threatening or dangerous situations. Physiologically, it is like the fight–flight response and therefore makes us more alert, our reactions are faster and improves our ability to cope, e.g. the intense anxiety experienced as you step onto the ledge of a window 20 stories above ground may lead to you go back inside.
Anxiety may be not useful when it reduces/interferes with our ability to concentrate, learn, think clearly and logically, plan make accurate judgments, perform motor tasks (such as crossing a busy road and shooting for goal from a difficult angle) and our behaviour, e.g. experiencing intense anxiety while sitting at a desk in an office on the 20th floor that makes it impossible for a person to do their job is not helpful.
3 Explain the meaning of the term anxiety disorder with reference to three examples of anxiety disorders.
Anxiety disorder is a group of disorders characterised by chronic feelings of anxiety, distress, nervousness and apprehension or fear about the future, with a negative effect.
Answer should include names and descriptions of three of the DSM-‐IV-‐TR anxiety disorders listed in Box 14.1 on page 559.
4 In what way is anxiety experienced as a ‘normal’ part of everyday life different from the experience of anxiety that characterises an anxiety disorder?
Anxiety disorders are distinguished from ‘normal’, everyday anxiety in that anxiety disorders involve anxiety that:
• is more severe (intense),
• lasts longer (anxiety may persist for months instead of going away after the anxiety-‐provoking situation has passed), and
• significantly interferes with a person’s daily life and stops them doing what they want to do.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 2 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
5 What is phobia and how does it differ from an ordinary fear?
• A phobia is an excessive or unreasonable fear directed towards a particular object, situation or event that causes significant distress or interferes with everyday functioning.
• Differences between phobia and ordinary fear:
-‐ avoidance behaviour: People with a phobia typically go to extraordinary lengths to avoid any possible exposure to their phobic stimulus and even organise their whole life around it. This avoidance typically interferes with their day to day functioning. For example, a person with a phobia of thunder can spend so much time tracking the weather and rearranging schedules that it prevents them from attending to other priorities. In contrast, people with ordinary fears don’t like coming into contact with their feared object/situation but they usually won’t go to extraordinary lengths to avoid it.
-‐ appraisal of fear stimulus: People with a phobia typically overestimate the amount of risk in a feared situation and the degree of harm that will come from being in that situation (which is out of proportion to the actual reality of the danger) and underestimate how well they are able to cope with it. For example, a person with an ordinary fear of spiders will dislike exposure to a spider and might stay a safe distance if they encountered one, but a person with a phobia of spiders may think that if they come across a spider one it will attack them and they will die.
• Consequently, a person with a phobia will experience much greater anxiety and physiological arousal than a person with an ordinary fear when exposed to a feared situation/object, as well as a greater desire to avoid it.
6 List the three key characteristics of a specific phobia.
There key characteristics are:
• anxiety: exposure to the phobic stimulus almost invariably induces an immediate anxiety response;
• awareness: the person recognises that their fear is excessive or unreasonable;
• avoidance: the phobic situation is avoided or else is endured with intense anxiety or distress.
As with all other disorders in the DSM-‐IV-‐TR, the person’s anxiety and avoidance behaviour significantly interfere with their everyday life and causes them great distress.
7 According to the DSM, how long must a person’s fear of a specific object or situation have persisted for them to be diagnosed as having specific phobia?
A diagnosis of specific phobia is only made if the fear of the specific object or situation has persisted for at least six months.
8 For both of the following cases, identify the relevant DSM-‐IV-‐TR phobia category.
Case 1—Mina has a social phobia
Case 2—Kathryn has a specific phobia – animal subtype (dogs)
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 3 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
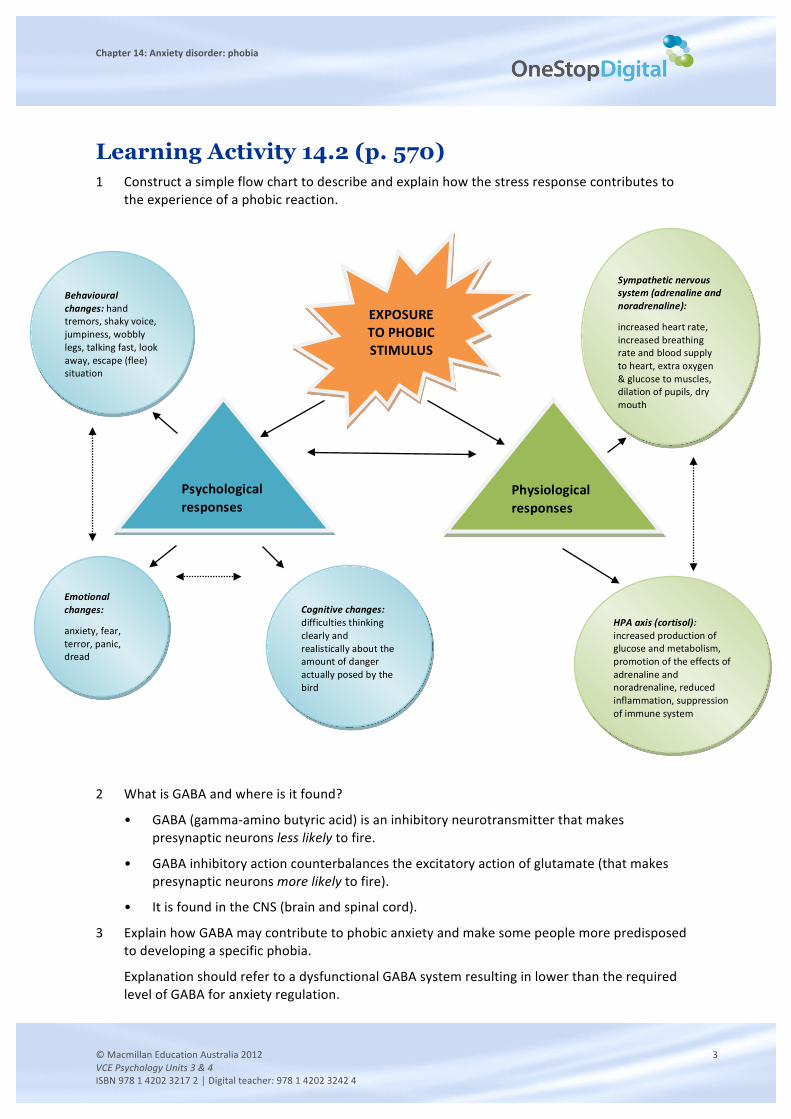
Learning Activity 14.2 (p. 570) 1 Construct a simple flow chart to describe and explain how the stress response contributes to
the experience of a phobic reaction.
2 What is GABA and where is it found?
• GABA (gamma-‐amino butyric acid) is an inhibitory neurotransmitter that makes presynaptic neurons less likely to fire.
• GABA inhibitory action counterbalances the excitatory action of glutamate (that makes presynaptic neurons more likely to fire).
• It is found in the CNS (brain and spinal cord).
3 Explain how GABA may contribute to phobic anxiety and make some people more predisposed to developing a specific phobia.
Explanation should refer to a dysfunctional GABA system resulting in lower than the required level of GABA for anxiety regulation.
EXPOSURE TO PHOBIC STIMULUS
(bird)
Psychological responses
Physiological responses
Behavioural changes: hand tremors, shaky voice, jumpiness, wobbly legs, talking fast, look away, escape (flee) situation
Emotional changes:
anxiety, fear, terror, panic, dread
Cognitive changes: difficulties thinking clearly and realistically about the amount of danger actually posed by the bird
HPA axis (cortisol): increased production of glucose and metabolism, promotion of the effects of adrenaline and noradrenaline, reduced inflammation, suppression of immune system
Sympathetic nervous system (adrenaline and noradrenaline):
increased heart rate, increased breathing rate and blood supply to heart, extra oxygen & glucose to muscles, dilation of pupils, dry mouth
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 4 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
4
a What are benzodiazepines?
• Benzodiazepines are a group of drugs commonly referred to as ‘minor tranquilisers’
• they have the effect of ‘calming down’ the body by reducing physiological arousal and promoting relaxation
• they are GABA agonists
• they are highly additive prescription drugs.
b Explain how benzodiazepines may be used to manage or treat phobic anxiety, ensuring you refer to their role as GABA agonists.
• when a person with a specific phobia encounters their phobic stimulus, their sympathetic nervous system and HPA axis are activated resulting in a highly aroused physiological state
• benzodiazepines are GABA agonists i.e. they mimic GABA’s inhibitory effects, therefore they reduce physiological arousal and promote relaxation
• for example, someone with a fear of flying may take a benzodiazepine tablet before getting on a plane
• benzodiazepines have therefore been successfully used to manage or treat phobic anxiety.
c In what way do studies with drugs that are GABA antagonists provide evidence of the role of GABA in phobic anxiety?
• Studies with drugs that are antagonists have found that they have the opposite effect on phobic anxiety
• GABA antagonists reduce GABA function and therefore produce anxiety symptoms
• for example, studies using primates have found that the physiological symptoms of anxiety can be induced when a benzodiazepine antagonist is administered.
Learning Activity 14.3 (p. 573) 1 What two key assumptions does the psychodynamic model make in explaining the development
of specific phobia and other mental disorders?
Key assumptions are:
• all mental disorders are caused by unresolved psychological conflicts of which we are not consciously aware, but which still have a considerable influence over our conscious thoughts and behaviours;
• unconscious psychological conflicts stem from early childhood experiences (e.g. infancy and early childhood such as the Oedipus complex), during which out instinctive impulses (‘urges’) and society’s view of what is ‘acceptable’ behaviour often clash.
2
a What is the Oedipal complex?
Explanation should refer to:
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 5 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• a developmental conflict that emerges during Freud’s phallic (third) stage of psychosexual development (4–5 years);
• it involves the unconscious, powerful, passionate love and desire that the male child develops toward his mother, and, fear that his father will become aware of this love and desire and punish him with castration.
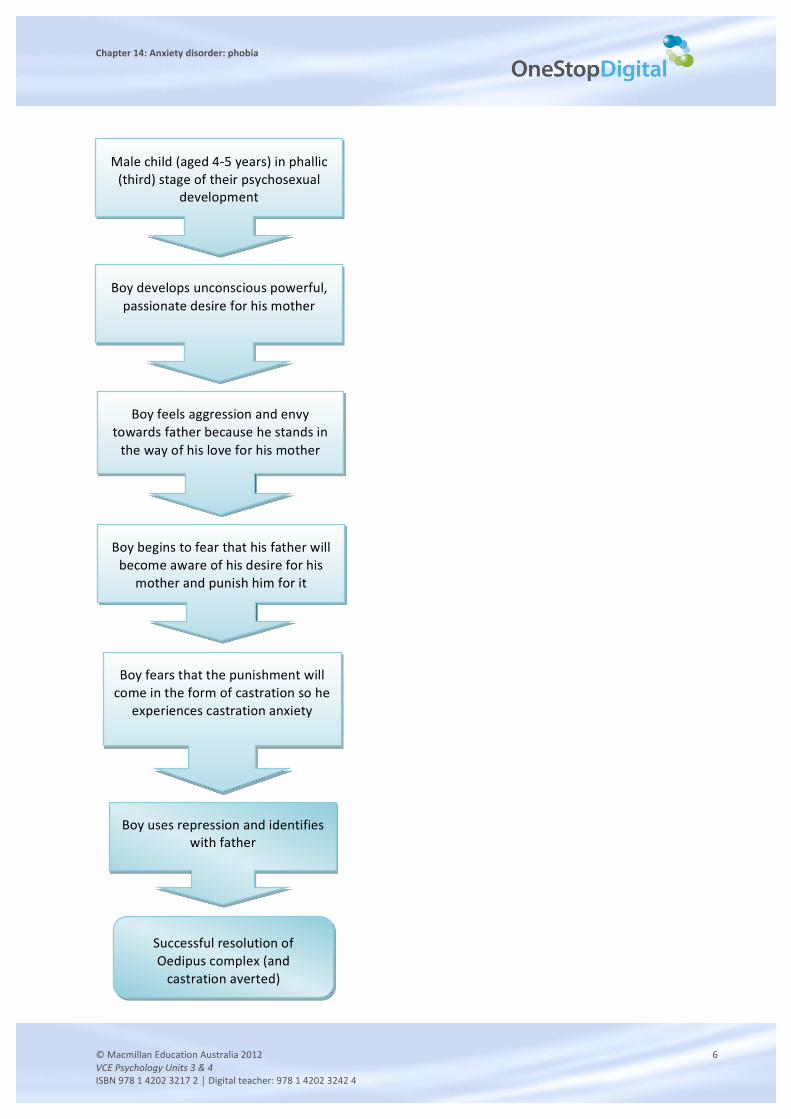
Use a simple flow chart to explain why the Oedipal complex occurs.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 6 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Male child (aged 4-‐5 years) in phallic (third) stage of their psychosexual
development
Boy develops unconscious powerful, passionate desire for his mother
Boy feels aggression and envy towards father because he stands in the way of his love for his mother
Boy begins to fear that his father will become aware of his desire for his
mother and punish him for it
Successful resolution of Oedipus complex (and castration averted)
Boy fears that the punishment will come in the form of castration so he
experiences castration anxiety
Boy uses repression and identifies with father
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 7 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
3 How does Freud’s psychodynamic model explain the development of a specific phobia?
Freud’s psychodynamic model proposes that:
• the development of a specific phobia is due to an unresolved Oedipus complex that arises during the phallic stage of a child’s development;
• a specific phobia develops when the Oedipus complex is not successfully resolved by the use of the defence mechanism called repression and another defence mechanism called displacement is used instead;
• when displacement is used, the anxiety caused by the unresolved Oedipus complex is displaced or ‘redirected’ away from the true source of the fear (the father) and onto a seemingly unimportant, irrelevant object or situation which then becomes the phobic stimulus;
• the male child can then deal with their unresolved conflict and the anxiety associated with it by avoiding the phobic stimulus.
4 According to Freud, why and how did Little Hans develop a phobia of horses?
Freud proposed that:
• Little Hans developed a specific phobia of horses because he was struggling to resolve his Oedipus complex;
• the anxiety and fear felt by Little Hans could not be expressed toward the real object of fear: his father;
• so, Little Hans used displacement and consequently ‘displaced’ his fear of his father onto horses, which symbolised or reminded him of his father and became the phobic stimulus;
• Freud believed that Little Hans’ fear of being bitten by a horse actually symbolised his fear of castration by his father.
5 To what extent does the psychodynamic model account for the development of phobias by girls?
The original psychodynamic model proposed by Freud does not account for the development of phobias by girls. Note that:
• Freud’s theory is well known for its gender bias;
• what happens to young girls in the phallic stage is not explained by Freud and the Oedipus complex cannot have the same outcome (i.e. a fear of castration cannot cause anxiety in a girl);
• Freud wrote that ‘the corresponding processes in the little girl are not known to us’ and he believed the Oedipus complex to be mainly masculine;
• it was Freud’s student Carl Jung who later proposed the Electra complex to describe a girl’s daughter–mother competition for psychosexual possession of father, i.e. the female equivalent of the Oedipus complex.
Learning Activity 14.4 (p. 575) 1 What key assumption does the behavioural model make in explaining the development of
specific phobia and other mental disorders?
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 8 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Key assumptions include:
• phobias are learned through experience and may be acquired, maintained or modified by environmental consequences such as rewards and punishment;
• classical conditioning processes play a role in the acquisition (or ‘development’) of a specific phobia and operant conditioning processes play a role in the persistence (or ‘maintenance’) of specific phobia;
• ‘abnormal’ or ‘dysfunctional’ ways of thinking, feeling and behaving are therefore learned through classical and operant conditioning processes (and can therefore also be modified).
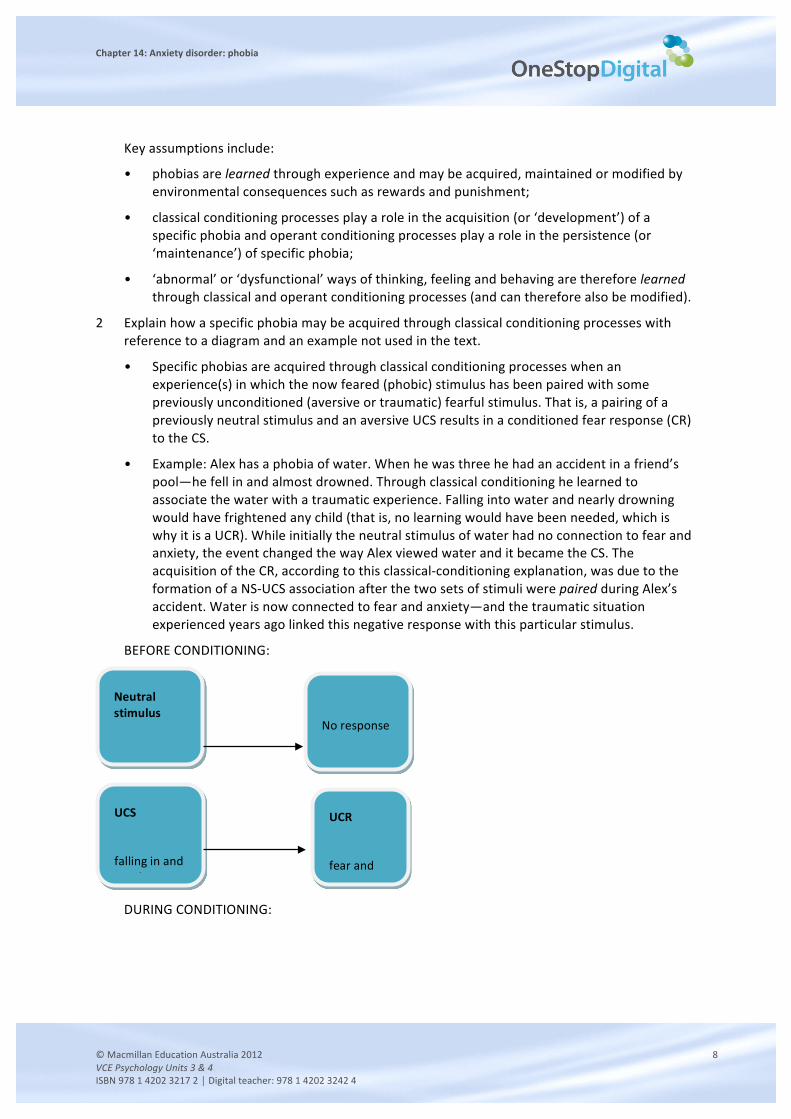
2 Explain how a specific phobia may be acquired through classical conditioning processes with reference to a diagram and an example not used in the text.
• Specific phobias are acquired through classical conditioning processes when an experience(s) in which the now feared (phobic) stimulus has been paired with some previously unconditioned (aversive or traumatic) fearful stimulus. That is, a pairing of a previously neutral stimulus and an aversive UCS results in a conditioned fear response (CR) to the CS.
• Example: Alex has a phobia of water. When he was three he had an accident in a friend’s pool—he fell in and almost drowned. Through classical conditioning he learned to associate the water with a traumatic experience. Falling into water and nearly drowning would have frightened any child (that is, no learning would have been needed, which is why it is a UCR). While initially the neutral stimulus of water had no connection to fear and anxiety, the event changed the way Alex viewed water and it became the CS. The acquisition of the CR, according to this classical-‐conditioning explanation, was due to the formation of a NS-‐UCS association after the two sets of stimuli were paired during Alex’s accident. Water is now connected to fear and anxiety—and the traumatic situation experienced years ago linked this negative response with this particular stimulus.
BEFORE CONDITIONING:
DURING CONDITIONING:
Neutral stimulus
water
No response
UCR
fear and anxiety
UCS
falling in and nearly
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 9 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
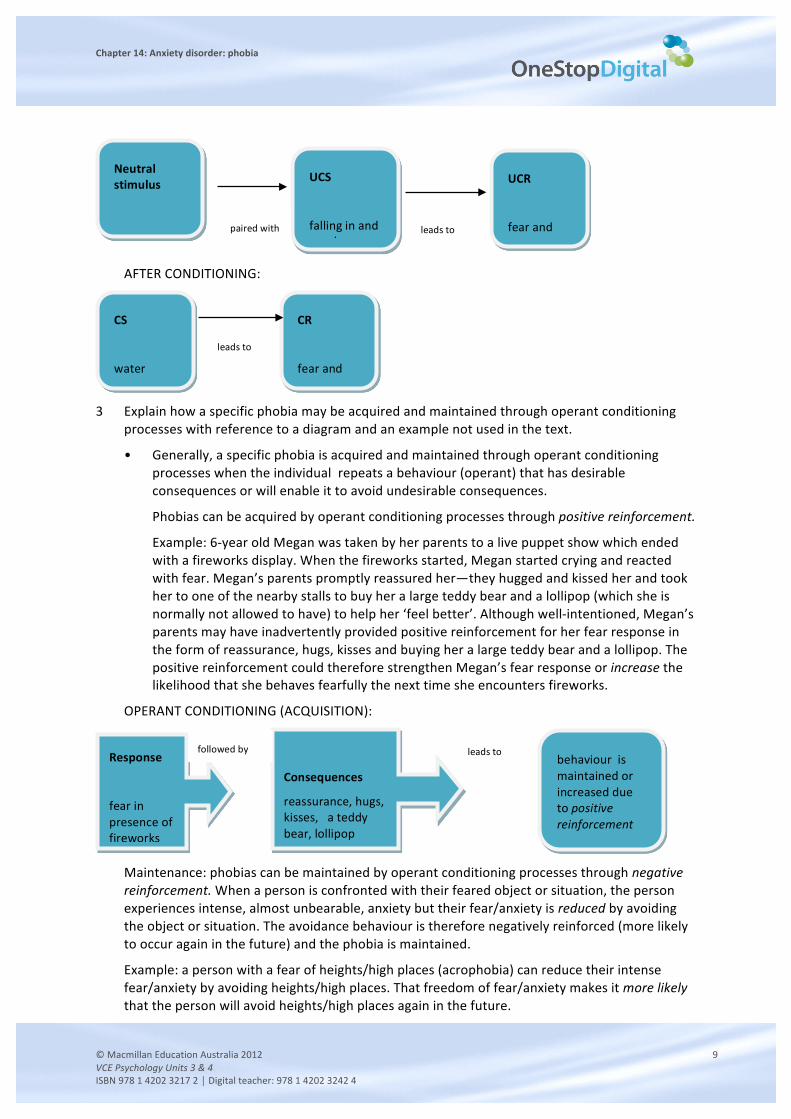
AFTER CONDITIONING:
3 Explain how a specific phobia may be acquired and maintained through operant conditioning
processes with reference to a diagram and an example not used in the text.
• Generally, a specific phobia is acquired and maintained through operant conditioning processes when the individual repeats a behaviour (operant) that has desirable consequences or will enable it to avoid undesirable consequences.
Phobias can be acquired by operant conditioning processes through positive reinforcement.
Example: 6-‐year old Megan was taken by her parents to a live puppet show which ended with a fireworks display. When the fireworks started, Megan started crying and reacted with fear. Megan’s parents promptly reassured her—they hugged and kissed her and took her to one of the nearby stalls to buy her a large teddy bear and a lollipop (which she is normally not allowed to have) to help her ‘feel better’. Although well-‐intentioned, Megan’s parents may have inadvertently provided positive reinforcement for her fear response in the form of reassurance, hugs, kisses and buying her a large teddy bear and a lollipop. The positive reinforcement could therefore strengthen Megan’s fear response or increase the likelihood that she behaves fearfully the next time she encounters fireworks.
OPERANT CONDITIONING (ACQUISITION):
Maintenance: phobias can be maintained by operant conditioning processes through negative reinforcement. When a person is confronted with their feared object or situation, the person experiences intense, almost unbearable, anxiety but their fear/anxiety is reduced by avoiding the object or situation. The avoidance behaviour is therefore negatively reinforced (more likely to occur again in the future) and the phobia is maintained.
Example: a person with a fear of heights/high places (acrophobia) can reduce their intense fear/anxiety by avoiding heights/high places. That freedom of fear/anxiety makes it more likely that the person will avoid heights/high places again in the future.
Neutral stimulus
water
UCS
falling in and nearly
UCR
fear and anxiety
paired with leads to
CS
water
CR
fear and anxiety
leads to
Response
fear in presence of fireworks
Consequences
reassurance, hugs, kisses, a teddy bear, lollipop
behaviour is maintained or increased due to positive reinforcement
followed by leads to
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 10 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
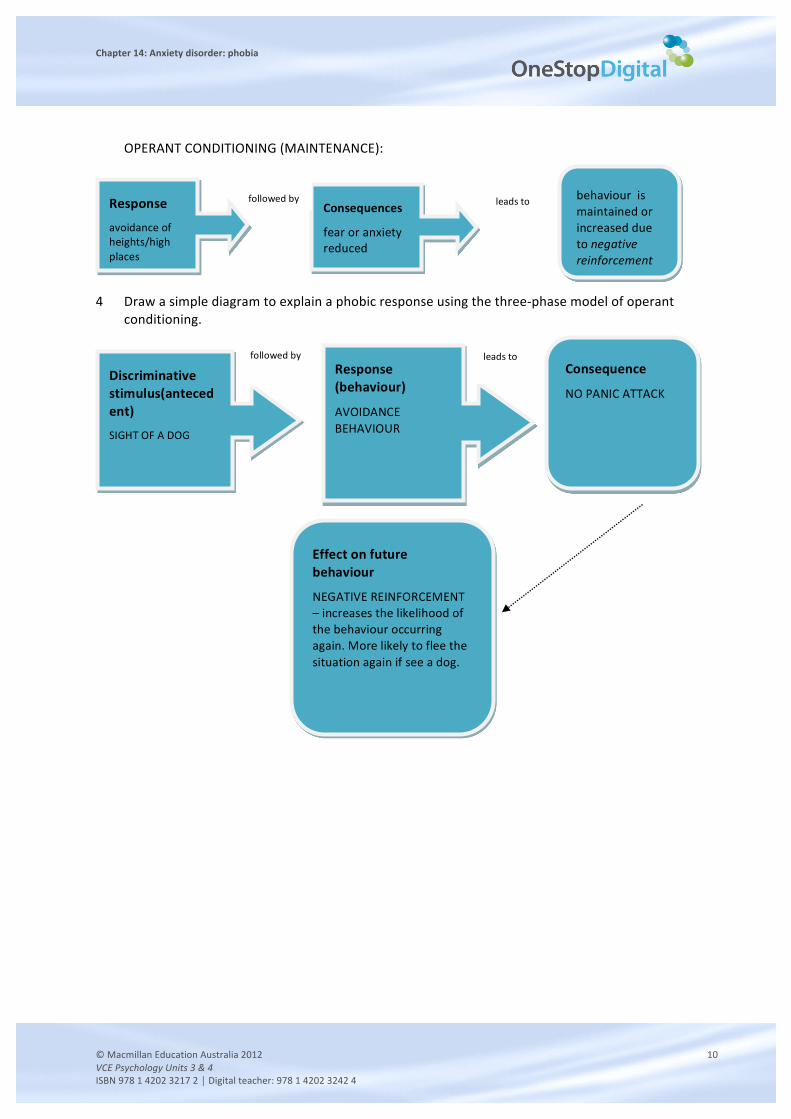
OPERANT CONDITIONING (MAINTENANCE):
4 Draw a simple diagram to explain a phobic response using the three-‐phase model of operant
conditioning.
Response
avoidance of heights/high places
Consequences
fear or anxiety reduced
behaviour is maintained or increased due to negative reinforcement
followed by leads to
Discriminative stimulus(antecedent)
SIGHT OF A DOG
Response (behaviour)
AVOIDANCE BEHAVIOUR
Consequence
NO PANIC ATTACK
leads to
Effect on future behaviour
NEGATIVE REINFORCEMENT – increases the likelihood of the behaviour occurring again. More likely to flee the situation again if see a dog.
followed by
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 11 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Learning Activity 14.5 (p. 576) Visual presentation on Little Albert’s and Little Hans’s specific phobias
Draw flow charts to compare and contrast the psychodynamic and behavioural explanations of how Little Albert and Little Hans may have developed their respective phobias. There should be four flow charts, organised in pairs, as follows:
• Little Hans: two flow charts, one summarising how his phobia developed through psychodynamic processes and the other how it developed through classical conditioning processes and was maintained through operant conditioning processes.
• Little Albert: two flow charts, one summarising how his phobia developed through psychodynamic processes and the other how it developed through classical conditioning processes and was maintained through operant conditioning processes.
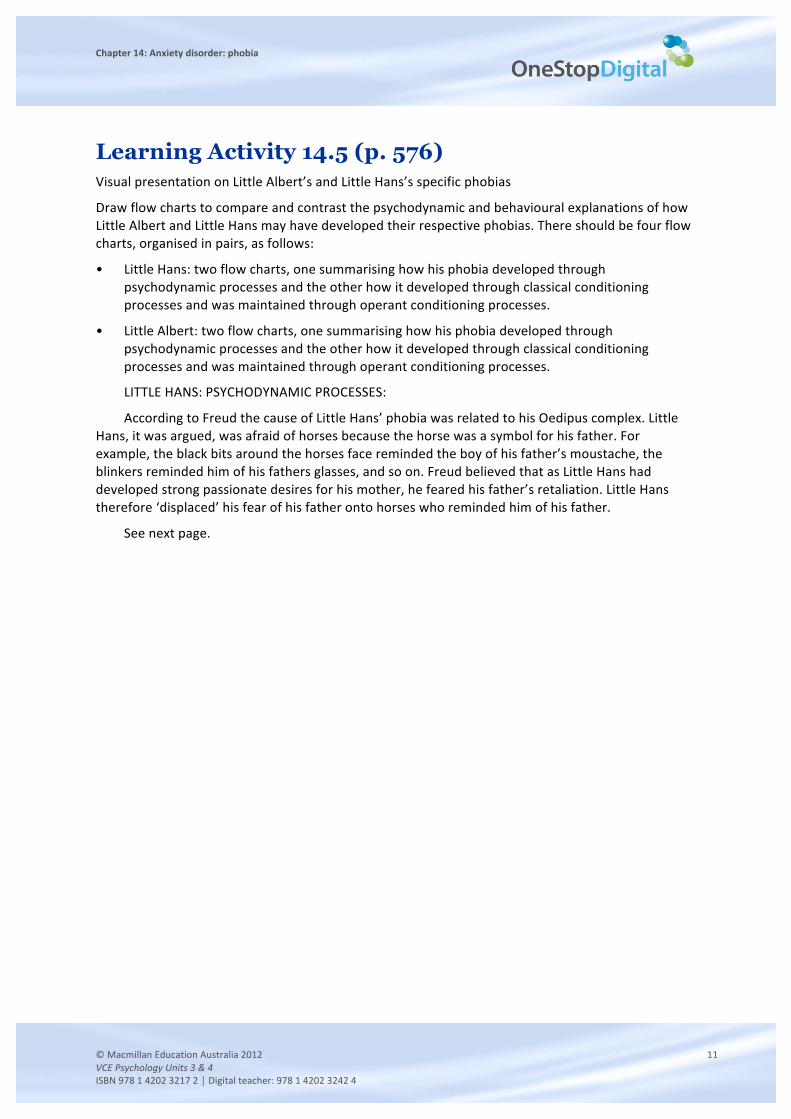
LITTLE HANS: PSYCHODYNAMIC PROCESSES:
According to Freud the cause of Little Hans’ phobia was related to his Oedipus complex. Little Hans, it was argued, was afraid of horses because the horse was a symbol for his father. For example, the black bits around the horses face reminded the boy of his father’s moustache, the blinkers reminded him of his fathers glasses, and so on. Freud believed that as Little Hans had developed strong passionate desires for his mother, he feared his father’s retaliation. Little Hans therefore ‘displaced’ his fear of his father onto horses who reminded him of his father.
See next page.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 12 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
4-‐year old Hans is in the phallic (third) stage of psychosexual development
Hans develops unconscious powerful, passionate desire for his mother
Hans feels aggression and envy towards father because he stands in the way of his love for his mother
Hans begins to fear that his father will become aware of his desire for his
mother and punish him for it
Hans tries to use repression and identify with father
Hans fears that the punishment will come in the form of castration so he
experiences castration anxiety
Repression does not work—unconscious desires are too strong
Hans uses displacement instead
Development of specific phobia of horses
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 13 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
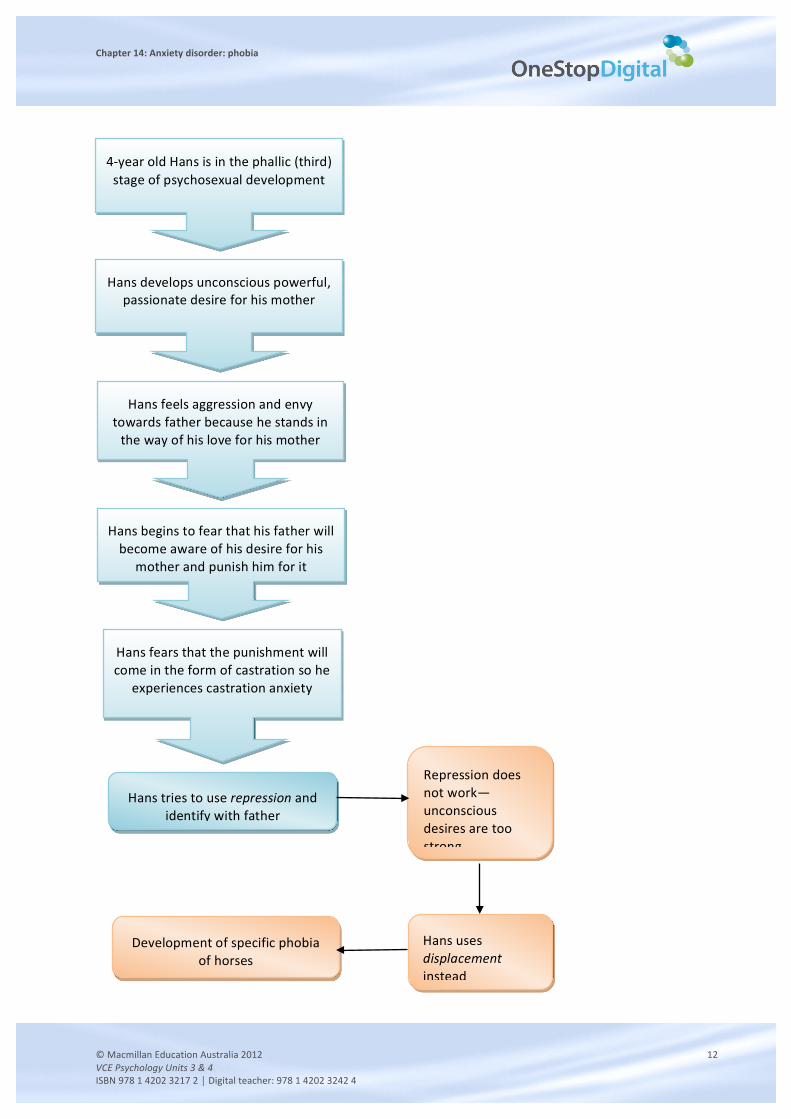
LITTLE HANS CLASSICAL CONDITIONING:
Little Hans first became afraid of horses after seeing and hearing a large horse fall and kick violently. In classical conditioning terms, the sight and sound of a horse falling was the unconditioned stimulus (UCS). The reflexive (automatic) distress elicited by this frightening situation was the unconditioned response (UCR). The sight and sound of a large horse falling and then violently struggling to get up (presumed dead), as well as the commotion that this would have caused among bystanders, would have been sufficient to frighten any child (that is, no learning would have been needed). While initially the neutral stimulus of horses had no connection to fear and anxiety, the event changed the way Hans viewed horses and horses became the CS. The acquisition of the CR, according to this classical-‐conditioning explanation, was due to the formation of a NS-‐UCS association after the two sets of stimuli were paired during Little Han’s walk with his mother. Therefore, it is possible to explain Freud's famous case in classical conditioning terms.
BEFORE CONDITIONING:
DURING CONDITIONING:
AFTER CONDITIONING:
LITTLE HANS OPERANT CONDITIONING:
Neutral stimulus
horse
No response
UCR
sight and sounds of fallen horse (presumed dead)
UCS
fear and anxiety
Neutral stimulus
horse
UCS
sight and sounds of fallen horse (presumed dead)
UCR
fear and anxiety
paired with
leads to
CS
horses
CR
fear and anxiety
leads to
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 14 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
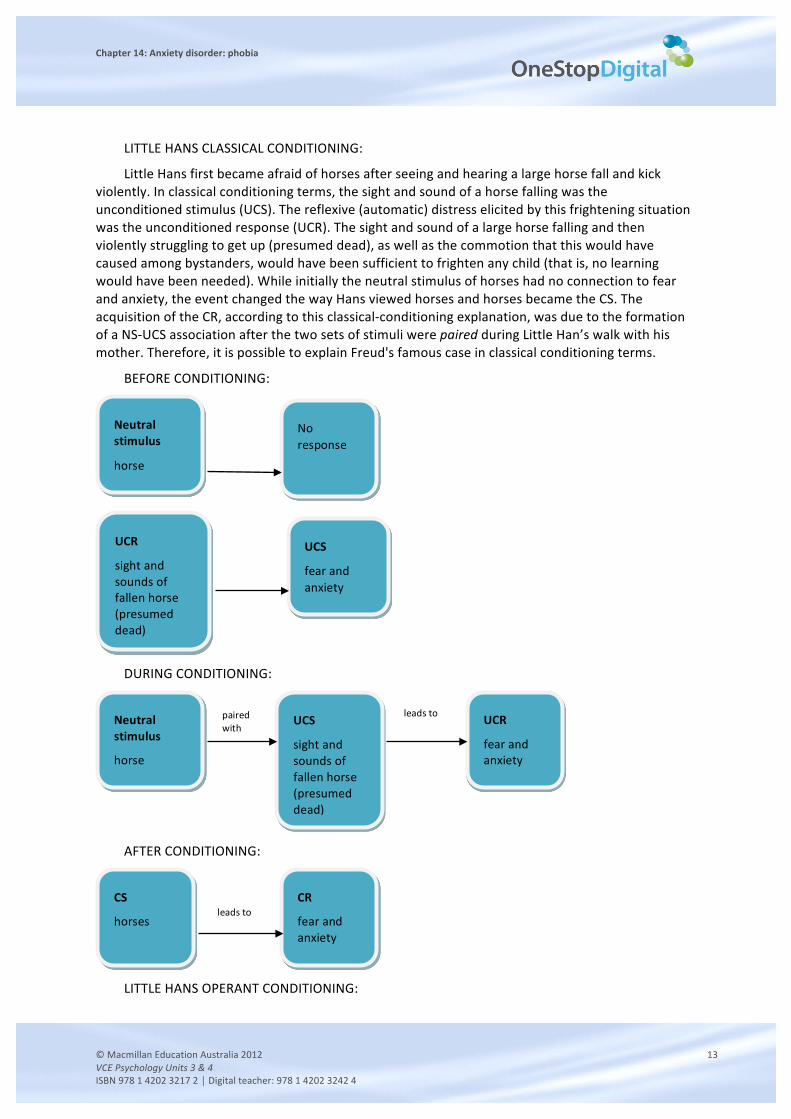
Little Hans specific phobia of horses was then maintained through operant conditioning, specifically, through negative reinforcement.
LITTLE ALBERT PSYCHODYNAMIC PROCESSES:
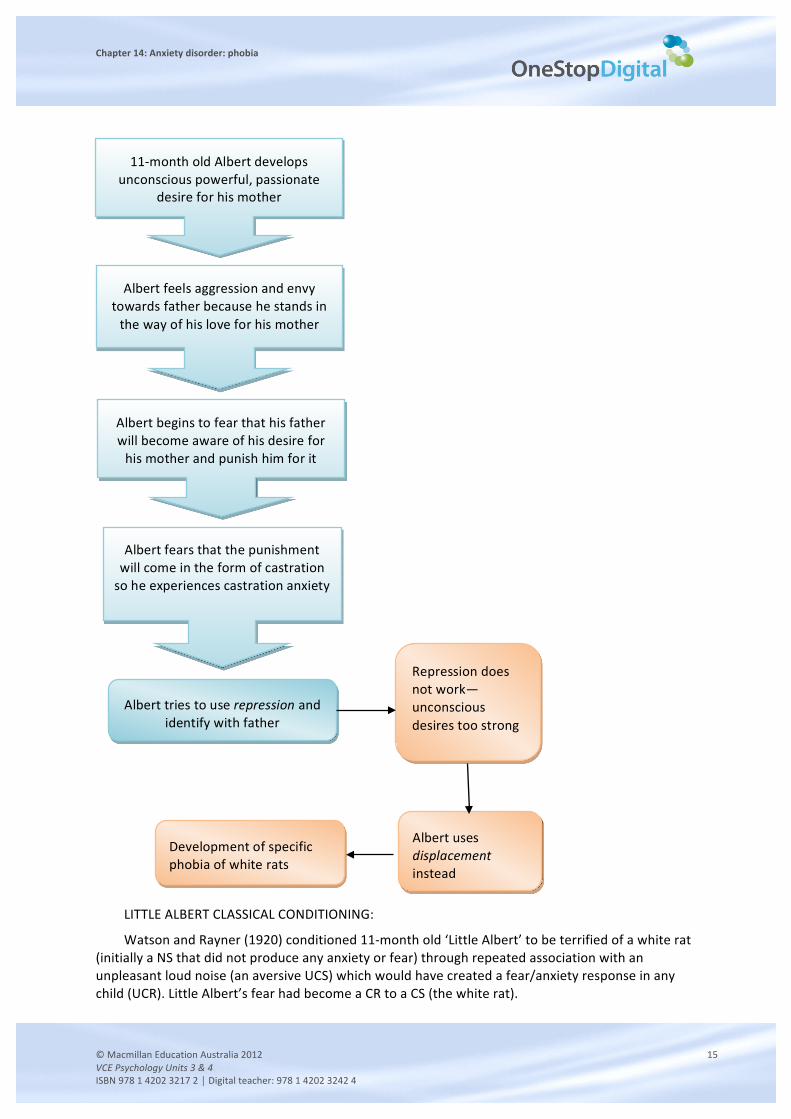
According to Freud, the cause of Little Albert’s phobia would be related to his Oedipus complex (which was experienced well ahead of the usual time as Albert was only 11 months old and therefore not in the phallic, or third, stage of his psychosexual development). Freud would argue that Little Albert was afraid of white rats because white rats were a symbol for his father. For example, Little Albert’s father may have had white hair or worn a white fluffy coat. Freud would have explained that as Little Albert had developed a strong unconscious desire for his mother, he feared his father’s retaliation. Little Albert therefore ‘displaced’ his fear of his father onto white rats who reminded him of his father.
See next page.
Response
avoidance of horses
Consequences
fear or anxiety reduced
Behaviour maintained or increased due to negative reinforcement
followed by
leads to
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 15 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
LITTLE ALBERT CLASSICAL CONDITIONING:
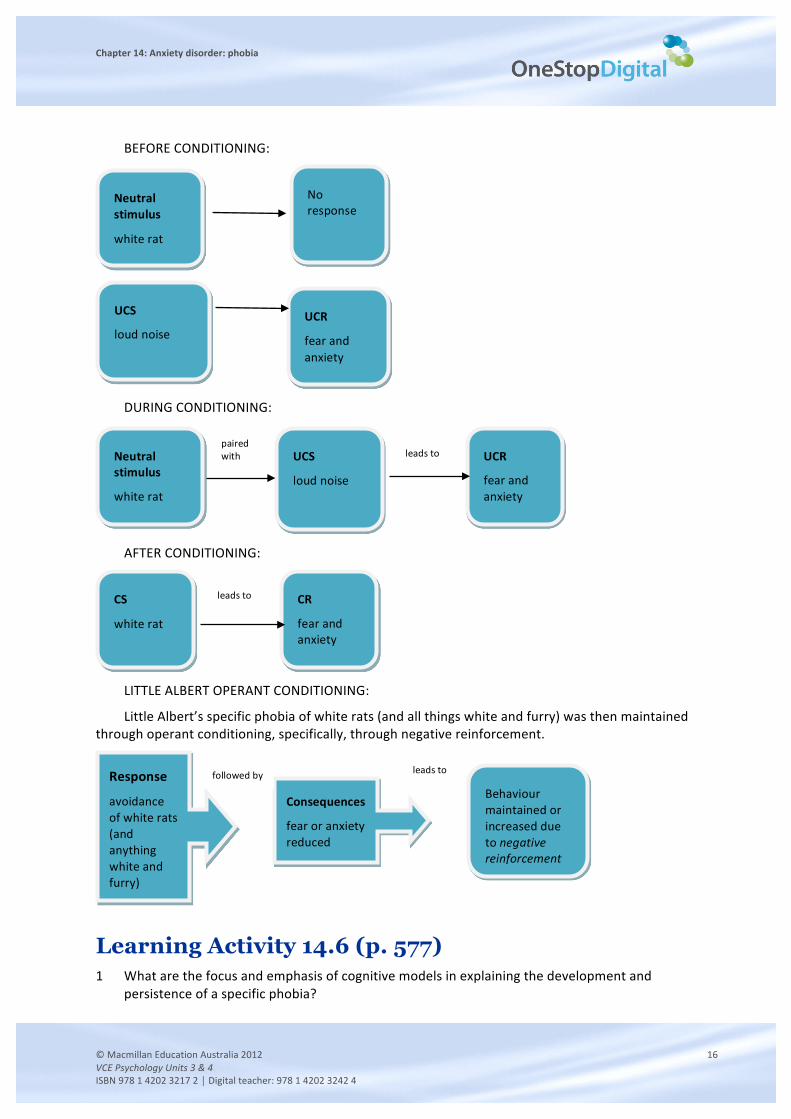
Watson and Rayner (1920) conditioned 11-‐month old ‘Little Albert’ to be terrified of a white rat (initially a NS that did not produce any anxiety or fear) through repeated association with an unpleasant loud noise (an aversive UCS) which would have created a fear/anxiety response in any child (UCR). Little Albert’s fear had become a CR to a CS (the white rat).
11-‐month old Albert develops unconscious powerful, passionate
desire for his mother
Albert feels aggression and envy towards father because he stands in the way of his love for his mother
Albert begins to fear that his father will become aware of his desire for his mother and punish him for it
Albert tries to use repression and identify with father
Albert fears that the punishment will come in the form of castration so he experiences castration anxiety
Repression does not work—unconscious desires too strong
Albert uses displacement instead
Development of specific phobia of white rats
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 16 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
BEFORE CONDITIONING:
DURING CONDITIONING:
AFTER CONDITIONING:
LITTLE ALBERT OPERANT CONDITIONING:
Little Albert’s specific phobia of white rats (and all things white and furry) was then maintained through operant conditioning, specifically, through negative reinforcement.
Learning Activity 14.6 (p. 577) 1 What are the focus and emphasis of cognitive models in explaining the development and
persistence of a specific phobia?
Neutral stimulus
white rat
No response
UCS
loud noise UCR
fear and anxiety
Neutral stimulus
white rat
UCS
loud noise
UCR
fear and anxiety
paired with leads to
CS
white rat
CR
fear and anxiety
leads to
Response
avoidance of white rats (and anything white and furry)
Consequences
fear or anxiety reduced
Behaviour maintained or increased due to negative reinforcement
followed by leads to
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 17 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• Focus: how the individual processes information and thinks about the phobic stimulus and related events (e.g. their perceptions, memories, beliefs, attitudes, appraisals and expectations).
• Emphasis: how and why people with a specific phobia have an unreasonable and excessive fear of a particular phobic stimulus.
2 What is cognitive bias?
A cognitive bias is a tendency to think in some kind of erroneous/mistaken or distorted way that involves an error(s) of judgment and faulty decision-‐making (and is therefore also referred to as a ‘mistake in thinking’ or cognitive distortion).
Note: In relation to phobias, cognitive biases make individuals more prone or vulnerable to experiencing fear and anxiety in response to a phobic stimulus.
3 Name, define and explain three types of cognitive bias that are associated with specific phobias. Give an example of each type of bias, other than an example used in the text.
Types of cognitive bias associated with specific phobias include:
attentional bias: the tendency to selectively attend to threat-‐related stimuli rather than to neutral stimuli, e.g. a person with a phobia of dogs may notice, upon arriving at a BBQ at a friend’s house, that there is a dog’s lead hanging on a coat hook in the hallway of the house—they are likely to be the first or only person to have noticed this;
memory bias: when recall or recognition is better for negative or threatening information than for positive or neutral information, e.g. a person with a dental phobia remembers the one and only time they had a frightening and painful dental experience but forgets all of the other times their dental experiences were not frightening or painful;
interpretive bias: the tendency to interpret or judge ambiguous stimuli and situations in a threatening manner, e.g. a person with a phobia of flying may interpret turbulence as a sign that the plane’s engine has failed so the plane is going to nose-‐dive and crash;
catastrophic thinking: the tendency to perceive objects or events as being far more threatening, dangerous or insufferable than they really are and will result in the worst possible outcome, e.g. a person with a phobia of bees may think that any bee they encounter will attack and kill them.
4 Briefly compare and contrast the cognitive, psychodynamic and behavioural models for explaining phobias, referring only to key assumptions.
Answer should highlight some of the following similarities/differences:
• all of the models provide an explanation for why someone develops a phobia, however they emphasise different reasons:
-‐ behavioural – phobias are learnt through classical and operant conditioning procedures
-‐ psychodynamic – phobias are caused by unresolved unconscious conflicts
-‐ cognitive – phobias are caused by faulty and irrational thinking
• in order to treat a phobia:
-‐ all of the models require a trusting and confiding therapeutic relationship
-‐ the psychodynamic model focuses on the earlier origins of the problem (i.e. the past) whereas cognitive and behavioural models focus the present (i.e. ‘here and now’)
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 18 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
-‐ cognitive and behavioural models adopt a structured, time-‐limited approach whereas psychodynamic models adopt a non-‐directive, open-‐ended approach
-‐ both cognitive and behavioural models use experiments/data collected from the environment whereas the psychodymanic model does not
-‐ both cognitive and behavioural models require the client to do ‘work’ outside/in between sessions (i.e. thought diary, behavioural experiments) whereas the psychodynamic model does not.
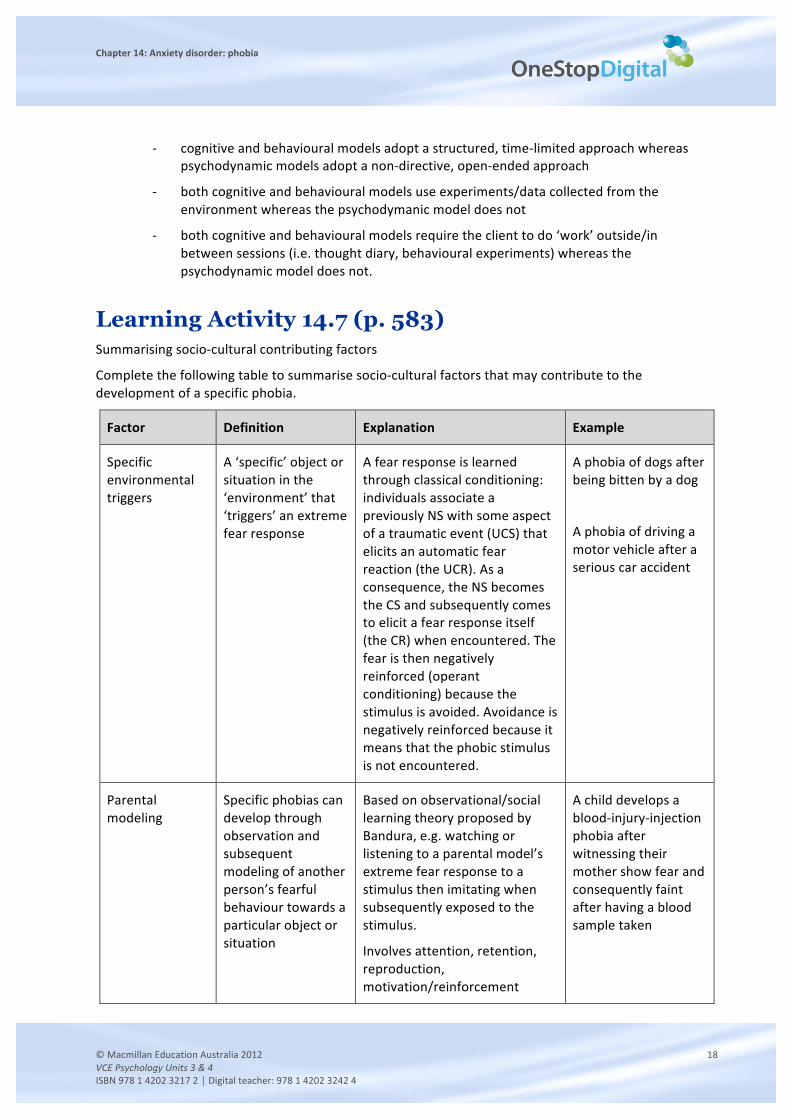
Learning Activity 14.7 (p. 583) Summarising socio-‐cultural contributing factors
Complete the following table to summarise socio-‐cultural factors that may contribute to the development of a specific phobia.
Factor Definition Explanation Example
Specific environmental triggers
A ‘specific’ object or situation in the ‘environment’ that ‘triggers’ an extreme fear response
A fear response is learned through classical conditioning: individuals associate a previously NS with some aspect of a traumatic event (UCS) that elicits an automatic fear reaction (the UCR). As a consequence, the NS becomes the CS and subsequently comes to elicit a fear response itself (the CR) when encountered. The fear is then negatively reinforced (operant conditioning) because the stimulus is avoided. Avoidance is negatively reinforced because it means that the phobic stimulus is not encountered.
A phobia of dogs after being bitten by a dog
A phobia of driving a motor vehicle after a serious car accident
Parental modeling
Specific phobias can develop through observation and subsequent modeling of another person’s fearful behaviour towards a particular object or situation
Based on observational/social learning theory proposed by Bandura, e.g. watching or listening to a parental model’s extreme fear response to a stimulus then imitating when subsequently exposed to the stimulus.
Involves attention, retention, reproduction, motivation/reinforcement
A child develops a blood-‐injury-‐injection phobia after witnessing their mother show fear and consequently faint after having a blood sample taken
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 19 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Transmission of threat information
The delivery of information from parents, other family members, teachers, peers, the media etc. about the potential threat or danger of a particular object or situation.
Threat information may increase beliefs about the danger posed by a particular stimulus. If a subsequent interaction with the stimulus is encountered, this is likely to produce a fear reaction.
A child develops a phobia of clowns (that persists into adulthood) after after watching the movie 'It' by Stephen King
A person develops a phobia of lightning after watching a documentary about fatal lightning strikes
Learning Activity 14.10 (p. 590) 1 Briefly explain what cognitive behavioural therapy (CBT) is.
Cognitive behavioural therapy is a type of psychological therapy that combines (or ‘blends’) cognitive and behavioural therapies to help people manage mental health problems and disorders:
• cognitive therapy focuses on the role of cognitions (thoughts, beliefs and attitudes) in determining emotions and behaviour;
• behavioural therapy is the clinical application of learning theories such as classical and operant conditioning and deals directly with maladaptive behaviours such as avoidance and reduced activity levels.
2 What is the key assumption of CBT?
Key assumption of CBT: The way people feel and behave is largely a product of the way they think.
3 What does CBT not aim to do?
CBT does not aim to persuade someone that their current way of thinking about an object or situation is wrong, irrational or too negative.
4 In what two ways does CBT differ from psychodynamic therapy?
Key differences include:
CBT does not involve ‘talking freely’ or dwelling on events in a person’s past to gain an insight into their psychological state;
CBT is relatively short-‐term, structured and focused on the ‘here and now’.
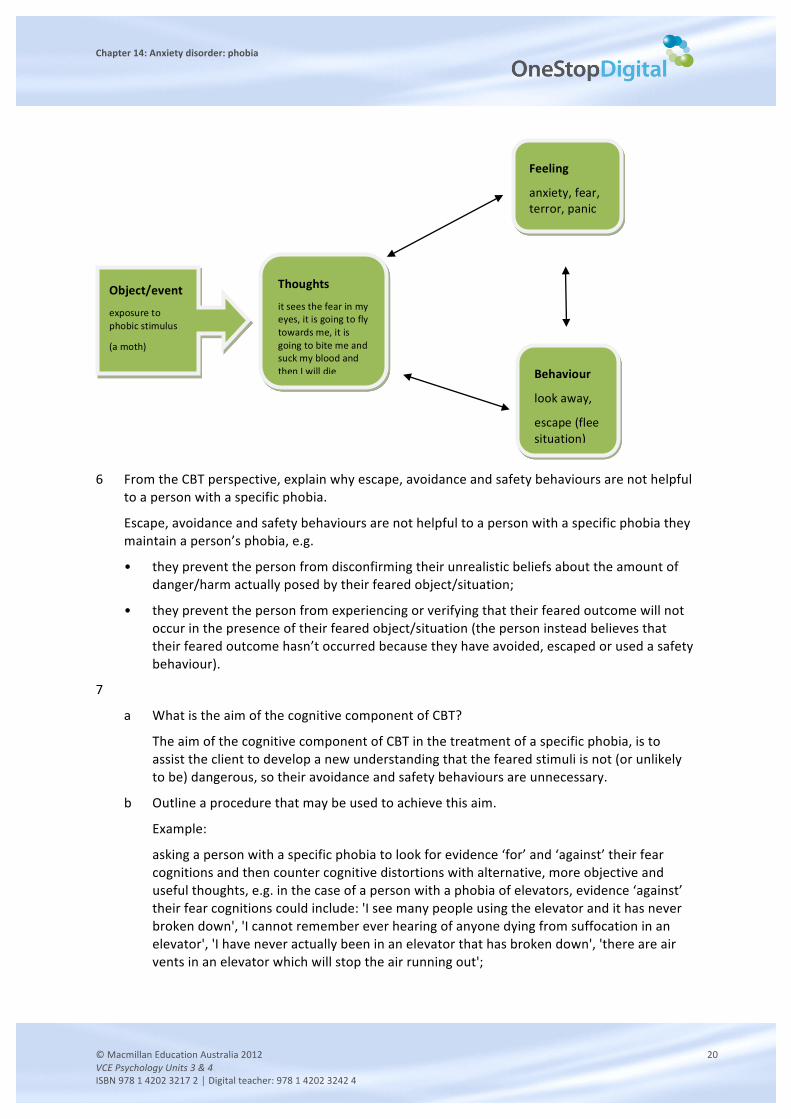
5 Draw a version of the diagram in figure 14.16 to explain how a specific phobia is acquired from the perspective of a mental health professional who uses CBT.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 20 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
6 From the CBT perspective, explain why escape, avoidance and safety behaviours are not helpful
to a person with a specific phobia.
Escape, avoidance and safety behaviours are not helpful to a person with a specific phobia they maintain a person’s phobia, e.g.
• they prevent the person from disconfirming their unrealistic beliefs about the amount of danger/harm actually posed by their feared object/situation;
• they prevent the person from experiencing or verifying that their feared outcome will not occur in the presence of their feared object/situation (the person instead believes that their feared outcome hasn’t occurred because they have avoided, escaped or used a safety behaviour).
7
a What is the aim of the cognitive component of CBT?
The aim of the cognitive component of CBT in the treatment of a specific phobia, is to assist the client to develop a new understanding that the feared stimuli is not (or unlikely to be) dangerous, so their avoidance and safety behaviours are unnecessary.
b Outline a procedure that may be used to achieve this aim.
Example:
asking a person with a specific phobia to look for evidence ‘for’ and ‘against’ their fear cognitions and then counter cognitive distortions with alternative, more objective and useful thoughts, e.g. in the case of a person with a phobia of elevators, evidence ‘against’ their fear cognitions could include: 'I see many people using the elevator and it has never broken down', 'I cannot remember ever hearing of anyone dying from suffocation in an elevator', 'I have never actually been in an elevator that has broken down', 'there are air vents in an elevator which will stop the air running out';
Thoughts
it sees the fear in my eyes, it is going to fly towards me, it is going to bite me and suck my blood and then I will die
Feeling
anxiety, fear, terror, panic
Behaviour
look away,
escape (flee situation)
Object/event
exposure to phobic stimulus
(a moth)
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 21 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• gathering accurate information or receiving psycho-‐education from their mental health professional about their phobic stimulus, e.g. that although huntsman spiders are very big and hairy and look very dangerous, they are in fact harmless.
8
a What is the aim of the behavioural component of CBT?
The aim of the behavioural component of CBT in the treatment of a specific phobia is to change any behaviours that are maladaptive (i.e. not helpful or even harmful).
b Outline a procedure that may be used to achieve this aim.
Procedure should refer to the client engaging in one or more behavioural experiments, e.g.
• behavioural experiments are planned experiential activities undertaken by clients in or between CBT sessions;
• their purpose is to help the client ‘test out’ the accuracy of their thoughts about the phobic stimulus, i.e. how harmful or dangerous the object/situation really is;
• it is hoped that at the conclusion of the experiment, clients come to realise that the likelihood of some terrible catastrophe occurring is in fact exaggerated.
Learning Activity 14.11 (p.590) Visual presentation on CBT
Example:
Sally has a moth phobia. She hates how slowly they fly, in seemingly arbitrary circles, and appear to make no attempt to avoid humans. In fact, according to Sally, they purposefully fly into people’s houses in order to terrify the occupants. Sally is disgusted and feels physically sick whenever she thinks about how their soft bodies turn into a kind of paste when they are squashed and the way they make large, visible silhouettes when they land. She believes that if she comes into contact with a moth it would see the fear in her eyes, adjust its flight path so that it flies directly towards her and then bite her (and she will die a long and painful death).
As part of her CBT, Sally was asked to gather accurate facts about moths. She discovered that only one type of moth (the Tiger Moth) is ‘poisonous’ (but only if it’s eaten and even then the quantity it not enough to kill a human) and none are ‘venomous’ (i.e. they do not secrete or transmit a venom if they were to bite you). She also found out that moths are nocturnal, which means that she is very unlikely to encounter one during daylight hours. With the help of the mental health professional, a behavioural experiment was set up. Before the experiment, Sally predicted that any exposure to a moth would result in her experiencing significant physical harm. She further believed that if she touched a moth, it would bite her and she would die. During the experiment, Sally tested out her beliefs by exposing herself to a moth and touching one. At the end of the experiment, Sally had touched a moth and not only did it not hurt her, it actually died in her hands after she touched it. Sally realised that it was moths that were fragile, not her.
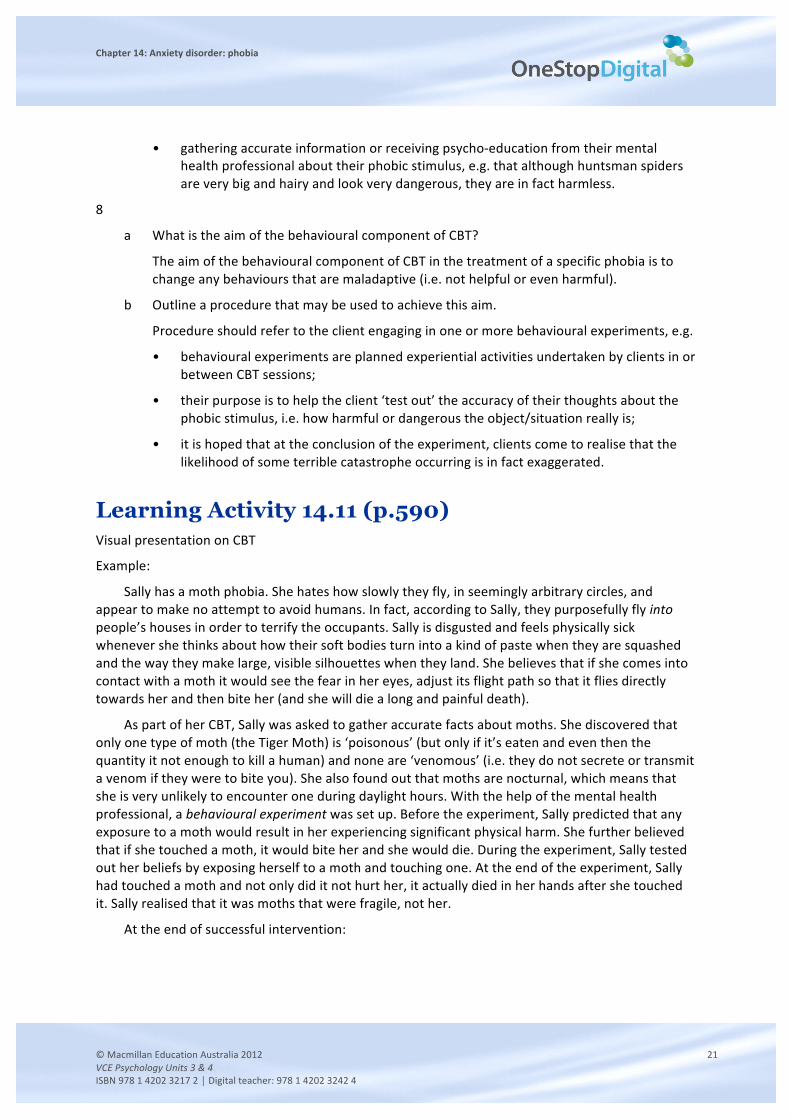
At the end of successful intervention:
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 22 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Learning Activity 14.12 (p. 596) 1 What is systematic desensitisation?
Systematic desensitisation:
• a kind of behaviour therapy that aims to replace an anxiety response with a relaxation response when an individual with a specific phobia confronts their feared stimulus;
• applies classical conditioning principles in a process that involves unlearning the association between anxiety and a specific object /situation and relearning feelings of relaxation (and safety) with that particular object/situation.
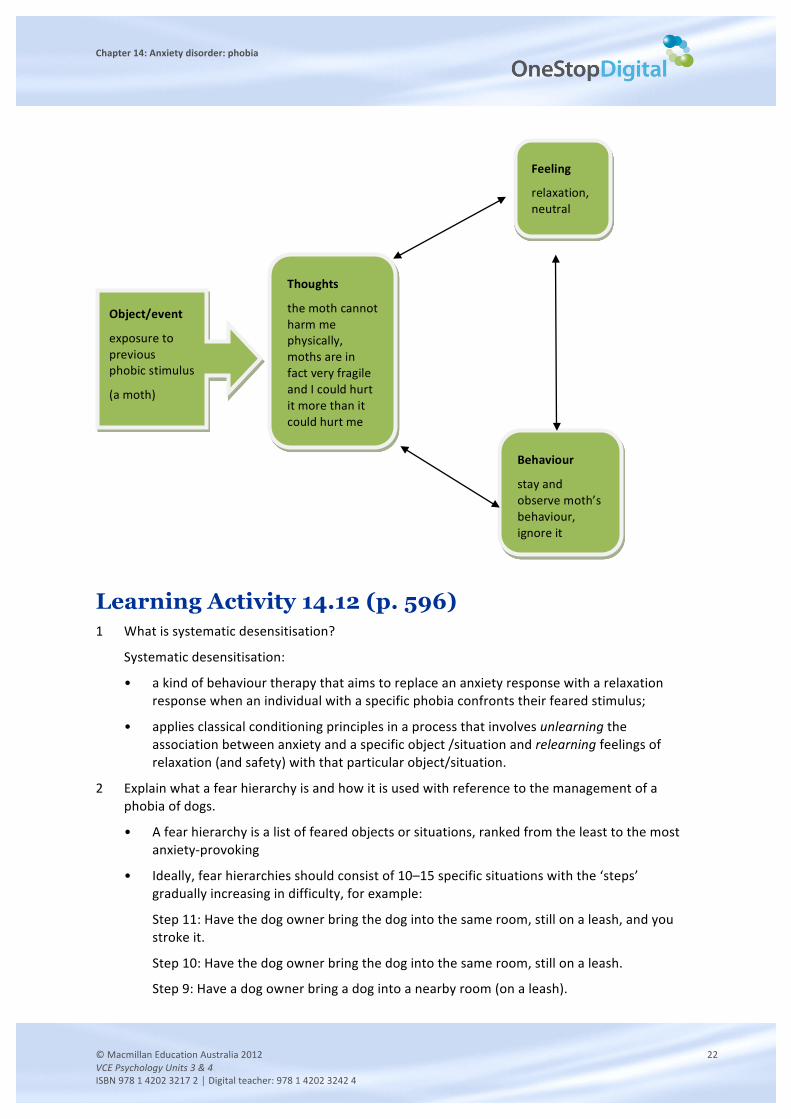
2 Explain what a fear hierarchy is and how it is used with reference to the management of a phobia of dogs.
• A fear hierarchy is a list of feared objects or situations, ranked from the least to the most anxiety-‐provoking
• Ideally, fear hierarchies should consist of 10–15 specific situations with the ‘steps’ gradually increasing in difficulty, for example:
Step 11: Have the dog owner bring the dog into the same room, still on a leash, and you stroke it.
Step 10: Have the dog owner bring the dog into the same room, still on a leash.
Step 9: Have a dog owner bring a dog into a nearby room (on a leash).
Thoughts
the moth cannot harm me physically, moths are in fact very fragile and I could hurt it more than it could hurt me
Feeling
relaxation, neutral
Behaviour
stay and observe moth’s behaviour, ignore it
Object/event
exposure to previous phobic stimulus
(a moth)
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 23 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
Step 8: Look at dogs from further out from the doorway.
Step 7: Look at dogs from a doorway.
Step 6: Look at dogs through a partly-‐opened window.
Step 5: Look at dogs through a closed window.
Step 4: Look at videos of dogs.
Step 3: Look at photos of dogs.
Step 2: Read information about dogs.
Step 1: Draw a dog on a piece of paper.
• The client then works their way upward through the hierarchy one ‘step’ at a time (starting at Step 1) whilst being encouraged to relax.
• No advancement is made to the next step until complete relaxation is achieved.
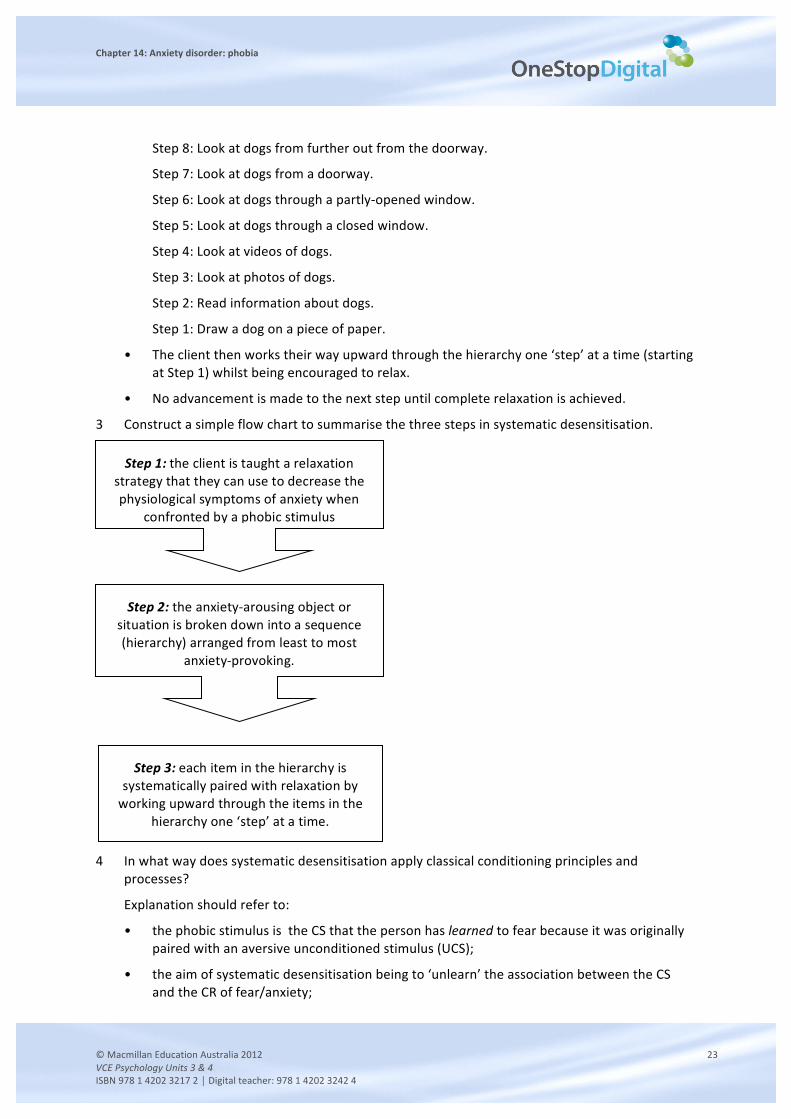
3 Construct a simple flow chart to summarise the three steps in systematic desensitisation.
4 In what way does systematic desensitisation apply classical conditioning principles and
processes?
Explanation should refer to:
• the phobic stimulus is the CS that the person has learned to fear because it was originally paired with an aversive unconditioned stimulus (UCS);
• the aim of systematic desensitisation being to ‘unlearn’ the association between the CS and the CR of fear/anxiety;
Step 1: the client is taught a relaxation strategy that they can use to decrease the physiological symptoms of anxiety when
confronted by a phobic stimulus
Step 2: the anxiety-‐arousing object or situation is broken down into a sequence (hierarchy) arranged from least to most
anxiety-‐provoking.
Step 3: each item in the hierarchy is systematically paired with relaxation by working upward through the items in the
hierarchy one ‘step’ at a time.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 24 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• the fact that by pairing the successive approximations of the CS with a new relaxation response that is incompatible with the emotions and the physical arousal associated with their current CR, the person’s fear/anxiety is gradually reduced and relieved;
• the fact that systematic desensitisation therefore involves gradually replacing the CR (fear/anxiety) with a new CR (relaxed state) and the fear response is extinguished i.e. replaces ‘spider=fear’ with ‘spider=relax’.
5 Helena has a fear of flying. Together with her therapist, she has constructed a fear hierarchy. Put the steps of her fear hierarchy in the most likely order that she would approach them using systematic desensitisation.
MOST ANXIETY PROVOKING Taking off
The plane taxiing to the runway
Watching the flight attendants do the safety drill
Being asked to fasten her seatbelt
The doors closing
Boarding the plane
Going into the departure lounge
Checking in
Arriving at the airport
Travelling to the airport in a taxi
Packing her luggage
Booking her plane ticket on the Internet
LEAST ANXIETY PROVOKING Thinking about travelling by plane
6
a What is flooding?
When used as a treatment for specific phobias, flooding is a technique that involves bringing the person into contact with the most-‐feared object or situation straight away and keeping them in contact with it until their fear disappears.
b What is the underlying assumption of this technique?
The assumption underlying this technique is that a high level of autonomic arousal is impossible to sustain (‘you can’t scream forever’) and eventually the feelings of panic subside, thereby enabling the person to experience their most prominent phobic stimulus in the absence of anxiety and come to learn that it is actually quite harmless
7 In what way does flooding apply classical conditioning principles and processes?
Explanation should refer to:
the phobic stimulus is the CS that the person has learned to fear because it was originally paired with an aversive unconditioned stimulus (UCS);
the aim of flooding is to extinguish the unwanted Conditioned Response (anxiety/fear/terror) by exposing the person, in one ‘massive dose’, to the Conditioned Stimulus (e.g. pigeon)
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 25 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
flooding therefore breaks the association between the CS and CR.
8 In what three ways can systematic desensitisation and flooding be carried out?
• In real-‐life (‘in vivo’)
• using visual imagery (their imagination)
• using virtual reality.
9
a How are systematic desensitisation and flooding similar when used in management of a specific phobia?
Both are behavioural techniques that require the person to ‘face their fear’ i.e. expose the person to their phobic stimulus.
b How do systematic desensitisation and flooding differ when used in management of a specific phobia?
They expose the person to their phobic stimulus in different ways. Flooding forces the person to face their phobic stimulus immediately and deliberately elicits a massive amount of anxiety. Whereas systematic desensitisation exposes the person to their phobic stimulus gradually and tries to prevent anxiety occurring.Flooding is also faster as eliminating the phobia than systematic desensitisation – flooding has known to be effective in only one session, whereas systematic desensitisation takes place over a number of sessions.
c Is flooding more or less ethically acceptable than systematic desensitisation? Explain your answer.
During flooding, the person is prevented from making their usual escape and is forced to stay and face their fear. It could be argued that flooding is less ethically acceptable than systematic desensitisation as it evokes considerable distress, is potentially traumatic and cruel, its ‘ends do not justify its means’, and that clients are better off suffering from their phobia than undergoing this form of treatment.
However, flooding is not less ethically acceptable than systematic desensitisation if the psychologist obtains Informed Consent from the client before undertaking it. According to the APS Code of Ethics, “Psychologists must fully inform clients regarding the psychological services they intend to provide; explain the nature and purpose of the procedures they intend using; and clarify the reasonably foreseeable risks, adverse effects, and possible disadvantages of the procedures they intend using”.
Before undertaking flooding, it would therefore be necessary for psychologists to spend time providing the client with a clear rationale for its use and a detailed explanation of its requirements. If this is done (and presumably it would be), it will satisfy the ethical principle of informed consent.
10 Sebastian has a phobia of cats.
a How could systematic desensitisation be used to assist Sebastian to overcome his phobia?
First, Sebastian would be taught relaxation strategies e.g. slow breathing technique
Next, Sebastian and his psychologist would construct a fear hierarchy, with items ranked from least to most anxiety provoking. E.g. top of the hierarchy, and most anxiety provoking, might be holding a cat in his arms.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 26 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
With the help of his psychologist, Sebastian would then work up his fear hierarchy, one step at a time, while using his relaxation techniques. He would not progress to the next step until complete relaxation had been achieved.
b How could flooding be used to assist Sebastian to overcome his phobia?
Sebastian could be put into a room with one hundred cats and the doors and windows closed. Sebastian would not be let out of the room until his body went into a relaxed/exhausted state.
Learning Activity 14.13 (p. 597) Evaluation of research by Gilroy and colleagues (2000)
1 What was the aim of the research?
The aim of the research was to compare the effectiveness of computer-‐aided vicarious exposure and systematic desnsitisation in the treatmentof spider phobia.
2 What was the hypothesis?
Both the live exposure and computer treatment conditions will lead to significant decreases in spider phobia symptoms, whereas the relaxation condition would remain at around the pre-‐treatment level and that any observed improvement in phobic symptoms would be maintained for 3-‐month..
Note: May be stated as two hypotheses, as described in the text.
3
a Who were the participants in the research?
45 females, all diagnosed with a spider phobia. Their mean age was 33.11 years.
b Why might the researchers have chosen this particular sample?
• use participants who have formally been diagnosed as having spider phobia
• females only may be to control sex/gender as a possible confounding variable
4 Identify the operationalised IV(s) and DV(s).
IV – the type of treatment given (computer-‐aided vicarious exposure vs live systematic desensitisation vs progressive muscle relaxation)
DVs – scores on various subjective and behavioural measures of phobic symptoms
5 Identify the experimental and control groups.
E1: computer-‐aided vicarious exposure E2:live systematic desensitisation
C: progressive muscle relaxation
6 Did the results of the experiment support the hypothesis? Explain your answer.
• The results supported the hypothesis that both the live exposure and computer treatment conditions will lead to significant decreases in spider phobia symptoms as both groups showed a substantial reduction in their phobic symptoms (including ( behavioural avoidance of spiders) for up to 3 months after the conclusion of the treatment sessions.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 27 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• However, the relaxation placebo group unexpectedly showed improvements on a number of the dependent variables.
7 What is a possible explanation for why Group 2 did so much better on the BAT than Group 1 post-‐treatment?
Due to the probable similarity between their treatment method (systematic desensitisation) and the steps on the BAT i.e. Group 2’s ‘treatment’ had probably consisted of working through the BAT steps.
8 The treatment given to Group 3 was a placebo.
a What does this mean?
The participants in this group were given a ‘fake treatment’ (to control beliefs/expectations of treatment acorss all groups).
b What were the participants of Group 3 likely to have been told by the researchers about the treatment they were receiving as part of the study?
• Participants would not have been informed that their treatment was a placebo i.e. they would have been told/led to believe that they were fully participating in the study like all the other participants and receiving a genuine treatment for their spider phobia.
c What particular ethical issue is relevant to this?
• An ethical issue of particular relevance to this specific study is ‘use of deception’ and the need for the researchers to ensure that participants did not suffer any distress from the research study .
9 Why was the double-‐blind procedure used in the 2003 follow-‐up study?
To control experimenter bias i.e. so that the researchers (experimenters) remained unbiased and objective and did not unintentionally influence the results of the experiment in order to support the hypothesis.
Learning Activity 14.14 (p. 597) Read the article ‘Scare Tactics’ on pages 561-‐562 and answer the following questions with reference to information in the article and the text.
1 How accurately does the article explain the meaning of phobia?
• The article provides information about the prevalence of specific phobias (10% of the population) and some of the subtypes as outlined in the DSM (i.e. animal, nature, situations, injection/blood/injury).
• The article also provides a good description and many examples via case studies about how specific phobias can interfere with people’s lives and impair their daily functioning.
• The article does not provide a definition of phobia per se.
2 According to the article, why do people with ‘obscure’ phobias tend to not seek treatment?
• More obscure phobias tend to be easy to avoid, so unless it is interfering with their lives, for the most part, they will put up with it.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 28 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• Things have to get ‘pretty bad’ before people with obscure phobias will consult a psychologist.
3 How accurate do you think this statement is?
• Assuming psychologist Montgomery is quoted correctly, reasonable accuracy may be inferred given the authoritative source.
• In addition to the reasons given above, there may also be an element of embarrassment that prevents people from consulting a mental health professional about a phobia of something obscure (e.g. phobia of peas, zips or cutlery), especially given the person is aware that their phobia is irrational.
4 In what ways did John’s specific phobia impair his everyday life? Why?
• Impairments:
-‐ he couldn’t walk from a building to his car or put his rubbish out if there was any thunder in the distance;
-‐ he was an avid golfer who could not play golf anymore (‘a golf course was the last place a golfer wants to be in the middle of a thunderstorm’)—he’d run off the course at the first rumble of thunder;
-‐ he was unable to carry on his day-‐to-‐day activities because he was constantly checking his lightning detector and spent so much time looking at the Bureau of Meterology’s website;
-‐ affecting his interactions with his wife as during storms, he’d spend his time locked in his bathroom with his iPod on, he’d turn all of electrical equipment in the house and draw the curtains.
• Why?
John most likely thought that he would definitely be struck down by lightning and killed if he was outside during a thunderstorm.
5 Explain how John’s thunderstorm phobia and Eyvonne’s bird phobia may have developed in terms of a:
a behavioural model:
• John:
John first became afraid of thunderstorms after he watched a documentary about fatal lightning strikes and this was intensified when some firecrackers unexpectedly went off near him at the Melbourne Showgrounds and sent a shower of ashes into the crowd.
-‐ In classical conditioning terms, the sight and sound of the firecrackers unexpectedly going off was the unconditioned stimulus (UCS). The reflexive (automatic) response elicited by this unexpected situation was the unconditioned response (UCR). While initially the neutral stimulus of thunder had no connection to fear and anxiety, the event changed the way he viewed thunder and thunder became the CS. The acquisition of the CR, according to this classical-‐conditioning explanation, was due to the formation of a NS-‐UCS association after the two sets of stimuli were paired during John’s outing at the Melbourne showgrounds.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 29 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• Eyvonne:
-‐ It is not known whether there was any particular negative encounter with a bird that precipitated her phobia.
-‐ In classical conditioning terms, a negative experience with a bird (e.g. a bird swooping down and trying to take something out of her hand) would have been the unconditioned stimulus (UCS). The reflexive (automatic) response elicited by this unexpected situation was the unconditioned response (UCR). While initially the neutral stimulus of birds had no connection to fear and anxiety, the event would have changed the way she viewed birds and birds became the CS.
b cognitive model:
• John:
He would have a number of cognitive distortions. In particular, he would be overestimating the amount of danger and threat posed by thunderstorms, e.g. that he will be struck by lightning and die.
• Eyvonne:
She would have a number of cognitive distortions. In particular, she would be overestimating the amount of danger and threat actually posed by birds and underestimating her ability to cope, e.g. if a bird flaps near her or flies by she is likely to think that it will swoop down and attack her, causing her physical harm, and she would be powerless to do anything about it.
c socio-‐cultural model:
John:
He developed his phobia of thunderstorms via transmission of threat information (after watching a documentary about fatal lightning strikes).
Eyvonne:
She may have developed her phobia of birds through one of the following:
-‐ a specific environmental trigger, e.g. following a negative/traumatic experience with a bird);
-‐ parental modeling, e.g. her parents were fearful of birds and she modeled this;
-‐ transmission of threat information, e.g. after watching a horror film about birds, such as Hitchcock’s The Birds or a documentary showing birds acting aggressively, eating carcasses etc.
6 What biological explanation of phobias is proposed in the article?
• That phobias are caused by the ‘amygdala, the threat-‐warning device buried deep in the brain, which can overact in situations it perceives to be risky’.
• The fact that people with phobias know their fears are irrational is due to ‘the separation of the cerebellum, the thinking part of the brain, from the emotional part of the brain—the thinking part says this is stupid but nevertheless the other part of the brain is still active so you can’t subjugate it.
7 Suggest how GABA may be contributing to Edan’s jewellery phobia.
Chapter 14: Anxiety disorder: phobia
© Macmillan Education Australia 2012 30 VCE Psychology Units 3 & 4 ISBN 978 1 4202 3217 2 │ Digital teacher: 978 1 4202 3242 4
• Eden could have a dysfunctional GABA system, i.e. a failure to produce, release or receive the correct amount of GABA transmission in the brain).
• The resulting low level of GABA could lead to higher levels of anxiety because there is not enough GABA to adequately regulate Edan’s anxiety or arousal levels.