Embed Size (px)
DESCRIPTION
Watson
Citation preview

Introduction: current conceptsand clinical decision making inelectrotherapyTim Watson
CHAPTER CONTENTS
Introduction 3
Current concepts inelectrotherapy 5
Models of electrotherapy 5
Electrotherapeutic windows 6
Clinical decision making inelectrotherapy 9
Conclusion 9
References 10
INTRODUCTION
Electrotherapy has a long-established place intherapy practice, being one of the mainstays ofprofessional activity over many years. The empha-sis on this mode of intervention has gone throughsignificant changes over time and, in current prac-tice, it is seen for the most part as an adjunct totreatment rather than as a means to an end in iso-lation. There are instances where it can be rightlyconsidered to be the focus of the treatment but thisis unusual and, arguably, the exception rather thanthe rule.
Given that many of the modalities that have beenused in the past have waned in popularity, and thatevery year new machines and new 'treatments'come to the marketplace, it can be difficult for thetherapist to know whether this 'new' treatment is infact new or just a revamped version of an alreadyexisting intervention. There are undoubtedly newinterventions and certainly new approaches toexisting treatments, driven by a demand frompatients,from manufacturers and from research.To claim that all current electrotherapy practice is'evidence based' would be naive, although there isroom. for debate as to what actually constitutesevidence-based practice, from where the evidenceis sourced and the role of individual experienceand that of colleagues in that process. Some ofthese issues will be explored in this introductorychapter.

4 INTRODUCTION AND SCIENTIFIC CONCEPTS
From the published and experiential evidence,it appears that electrotherapy can be clinicallyeffective and need not be written off as somethingthat is 'old fashioned' and that no longer deservesa place in the therapeutic tool kit. That it can beapplied in a clinically effective manner is evi-denced in the chapters that follow. That it can alsobe delivered in an ineffectual manner is somethingthat will be recognised by practitioners from manydisciplines. The evidence would suggest that whenthe appropriate modality is applied at the 'right'dose for the presenting problem, it can make a sig-nificant contribution to the improvement and wellbeing of the patient. The fact that it does not workin all cases is not surprising at all. This would be acommon feature of any therapy - whether manualtherapy, exercise or drug therapy. If one were to usea particular manual therapy technique for patient X,and the next day or the next week, when X returns,there was no improvement, it would not meanthat all manual therapy was a waste of time, oreven that the therapist was incompetent. There arepatients who fail to respond to therapy A, but dovery well with therapy B. The reasons for theseindividual differences are poorly understood, butcertainly add to the richness of clinical experience.If therapy was simply a matter of applying theright recipe to the patient presenting with a givenproblem, clinical practice would lose a deal of itsattractiveness. For any therapeutic intervention tobe effective there is the need for a clear assess-ment, a rationalisation of the problem(s), and theconstruction of a proposed treatment plan thatmatches the needs of the individual taking intoaccount their holistic circumstances, not just theirpresenting signs and symptoms. The applied inter-vention is that which is deemed to be most likelyto be effective. This is no guarantee that there willbe 100% success, but the best odds for a beneficialoutcome. The thinking therapist then re-evaluatesthe outcomes as the treatment progresses, modify-ing the treatment package in the light of theseresults. .
One of the problems with the application ofresearch in electrotherapy, as well as in other fields,is that the research tends to be somewhat reduc-tionist in approach. A clinical trial that evaluates,for example, the effect of ultrasound for patientswith a tear of the medial collateral ligament of the
knee, aims to construct a methodology that readilyidentifies the contribution that ultrasound makes tothe clinical outcome. By keeping all other treatmentparameters' constant' - the advice, exercise, manualtherapy, environment, number of treatment andtreatment intervals - the real effect of the ultra-sound therapy can be evaluated.
The clinical reality is that it is the package of carethat is clinically effective (or not), rather than anyone individual component of it. If a patient hasreceived several forms of intervention (e.g. someadvice, electrotherapy, manual therapy and exer-cise coupled with appropriate advice and educa-tion) and comes back for the next session with animprovement, it is extraordinarily difficult to knowwhich elements of the treatment package (if any)were responsible for the change. It could be that allwere necessary in that particular combination; itcould be that one could have been safely omittedand the equivalent outcome would have beenachieved. .
When making a clinical decision, practitionerswill put together the package that in their opinionis most likely to be effective for that patient. Somepatients will not take advice well, others willalmost certainly not undertake the exercises that aresuggested, and others might have a strong aver-sion to the idea of electrical stimulation. The effec-tive package is the one that matches the patient'spresentation and the treatment context. Somepatients might be treated several times a weekwhereas others can only be seen once every 2 or 3weeks on a 'check-up' basis. Package tailoring isan essential skill for any therapist.
The current stage of research in electrotherapyand many other therapeutic fields is still at thepoint where the building blocks of these packagesare being evaluated. We might know, in absoluteterms, the effect of this particular treatment, at thisparticular dose on a specific problem in a con-trolled research environment. We might not knowwhat happens when the same therapy is used in adifferent combination - there are almost too manyvariables to evaluate at the current time.
The research evidence suggests that electrotherapycan be effective as an element of treatment. Furtherwork is needed to evaluate the combinations -or treatment packages - that are most effective.Practitioners will have, from their own experience,
Introduction: current concepts and clinical decision making in electrotherapy 5
ideas about combinations that are more or less effec-tive.This is the source of the richness of therapeuticexperience and until substantially more work hasbeen completed - both in the laboratory and in clin-ical practice, usingreductionist, holistic and prag-matic methodologies - the full story is unlikely toemerge.
The intention of this publication is to provide areview of the background, evidence and clinicalapplicability of various modalities in use. Theauthors of each chapter are writing because theyknow their subject and, although there might begaps in the knowledge that deserve to be filled,there is sufficient evidence out there from whichclinical decision making can be enhanced and fur-ther developments achieved.
CURRENT CONCEPTS INELECTROTHERAPY
, 0 matter which classification one uses, there isno one correct way to divide and categorise therange of electrotherapy modalities available. Onecould for example use a thermal/non-thermaldivision, but reading the literature on thermal vs.non-thermal vs. microthermal will soon demon-strate that this is an almost certainly flawed propo-sition. One could attempt to categorise by type ofapplied energy: light (e.g. laser, ultraviolet) versuselectricalstimulation (e.g. transcutaneous electrical
rve stimulation [TENS],interferential) versus thegh-frequency radiations (shortwave, microwave).trasound would have to sit in a category of itsm and biofeedback would not belong anywherethat, for the most part, it does not involve the
elivery of energy but enables the patient tospond to the behaviour of his or her body. This
~ -ision could also be challenged in that, forample, the effects of continuous shortwave are
~illli.larbut clinically different from those of pulsed_ ortwave. The fundamental energy might be thesame but the mode of delivery makes a substantial.. erence to the treatment outcome.
Furthermore, there is an issue with the inclusion~ new' therapies into the classification. Magneticerapy is a swiftly developing field although,e would suggest, still in its clinical infancy.uld it have a category of its own or should it be
incorporated with some forms of shortwave thatemploy and electromagnetic field?
The modalities covered in this text include thosethat are in common clinical use, and have beendivided into sections that reflect the type of energyemployed, for example, the thermal energies aregrouped as are various forms of electrical stimula-tion. The grouping of laser,ultrasound and biofeed-back does not imply a common energy type ormode of action,but rather their individuality.
MODELS OF ELECTROTHERAPY
All electrotherapy modalities - whether in currentuse, abandoned from the past or yet tobe 'invented'- actually follow a very straightforward modelthat is presented below. It is sufficiently robust toexplain current practice, yet sufficiently flexible toincorporate future developments. It has beenrefined over the years and will almost certainly besubject to further refinement in the future.
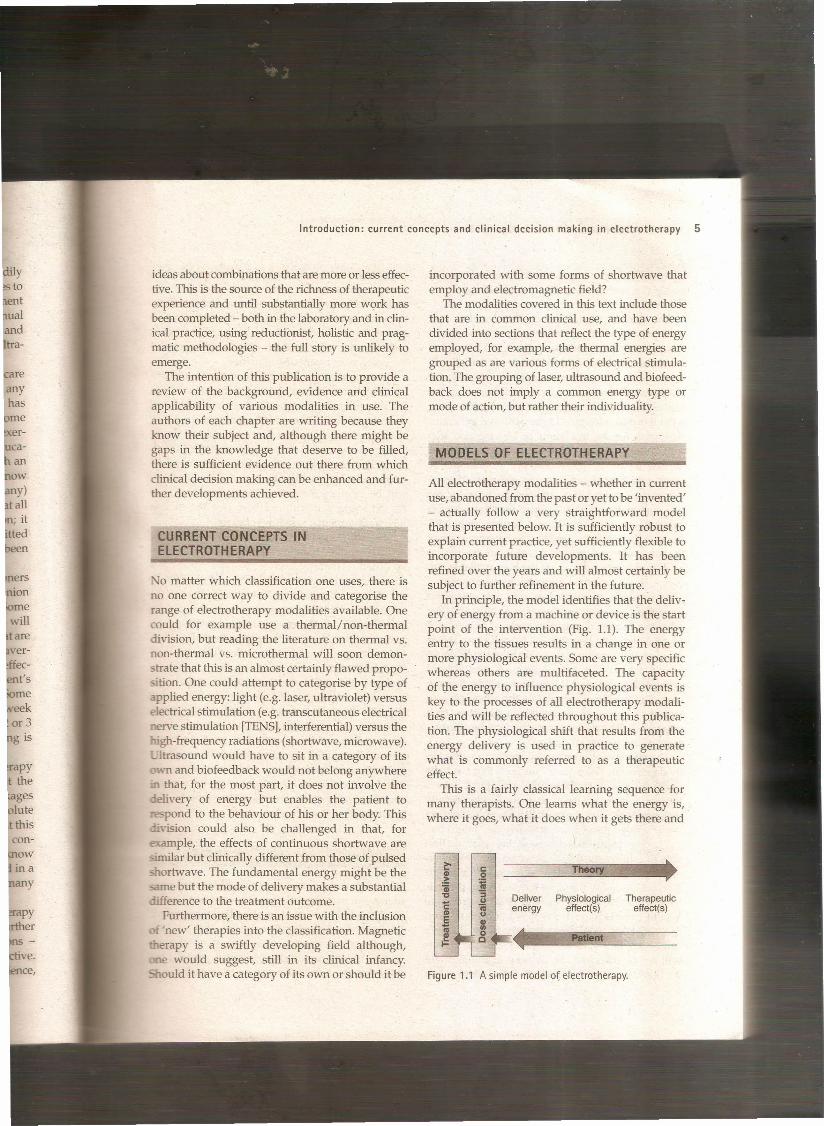
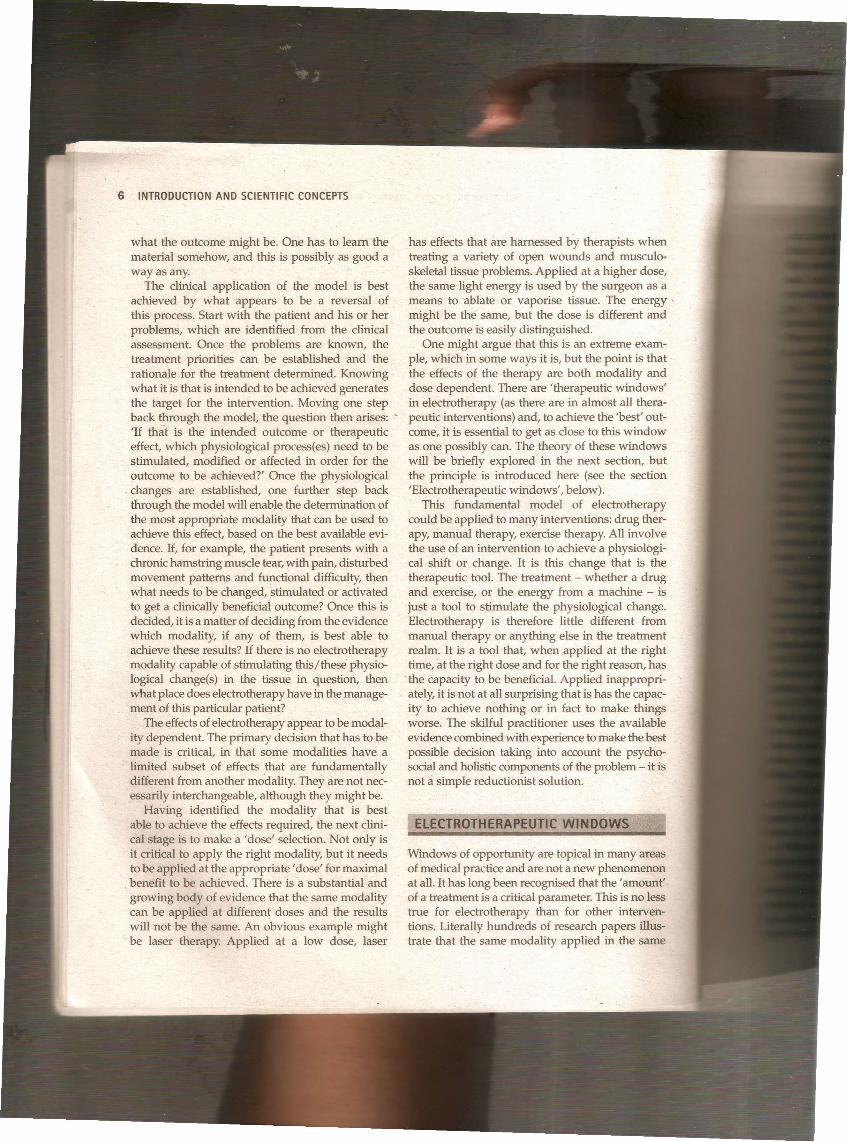
In principle, the model identifies that the deliv-ery of energy from a machine or device is the startpoint of the intervention (Fig. 1.1). The energyentry to the tissues results in a change in one ormore physiological events. Some are very specificwhereas others are multifaceted. The capacityof the energy to influence physiological events iskey to the processes of all electrotherapy modali-ties and will be reflected throughout this publica-tion. The physiological shift that results from theenergy delivery is used in practice to generatewhat is commonly referred to as a therapeuticeffect.
This is a fairly classical learning sequence formany therapists. One learns what the energy is,where it goes, what it does when it gets there and
Theory
Deliver Physiological Therapeuticenergy effect(s) effect(s)
Figure 1.1 A simple model of electrotherapy.
6 INTRODUCTION AND SCIENTIFIC CONCEPTS
what the outcome might be. One has to learn thematerial somehow, and this is possibly as good away as any.
The clinical application of the .model is bestachieved by what appears to be a reversal ofthis process. Start with the patient and his or herproblems, which are identified from the clinicalassessment. Once the problems are known, thetreatment priorities can be established and therationale for the treatment determined. Knowingwhat it is that is intended to be achieved generatesthe target for the intervention. Moving one stepback through the model, the question then arises: .'If that is the intended outcome or therapeuticeffect, which physiological process(es) need to bestimulated, modified or affected in order for theoutcome to be achieved?' Once the physiological
. changes are established, one further step backthrough the model will enable the determination ofthe most appropriate modality that can be used toachieve this effect,based on the best available evi-dence. If, for example, the patient presents with achronic hamstring muscle tear,with pain, disturbedmovement patterns and functional difficulty, thenwhat needs to be changed, stimulated or activatedto get a clinically beneficial outcome? Once this isdecided, it is a matter ofdeciding from the evidencewhich modality, if any of them, is best able toachieve these results? If there is no electrotherapymodality capable of stimulating this/these physio-logical change(s) in the tissue in question, thenwhat place does electrotherapy have in the manage-ment of this particular patient?
The effectsof electrotherapy appear to be modal-ity dependent. The primary decision that has to bemade is critical, in that some modalities have alimited subset of effects that are fundamentallydifferent from another modality, They are not nec-essarily interchangeable, although they might be.
Having identified the modality that is bestable to achieve the effects required, the next clini-cal stage is to make a 'dose' selection. Not only isit critical to apply the right modality, but it needsto be applied at the appropriate' dose' for maximalbenefit to be achieved. There is a substantial andgrowing body of evidence that the same modalitycan be applied at different doses and the resultswill not be the same. An obvious example mightbe laser therapy. Applied at a low dose, laser
has effects that are harnessed by therapists whentreating a variety of open wounds and musculo-skeletal tissue problems. Applied at a higher dose,the same light energy is used by the surgeon as ameans to ablate or vaporise tissue. The energy'might be the same, but the dose is different andthe outcome is easily distinguished.
One might argue that this is an extreme exam-ple, which in some ways it is, but the point is thatthe effects of the therapy are both modality anddose dependent. There are 'therapeutic windows'in electrotherapy (as there are in almost all thera-peutic interventions) and, to achieve the 'best' out-come, it is essential to get as close to this windowas one possibly can. The theory of these windowswill be briefly explored in the next section, butthe principle is introduced here (see the section'Electrotherapeutic windows', below) .
This fundamental model of electrotherapycould be applied to many interventions: drug ther-apy, manual therapy, exercise therapy. All involvethe use of an intervention to achieve a physiologi-cal shift or change. It is this change that is thetherapeutic tool. The treatment - whether a drugand exercise! or the energy from a machine - isjust a tool to stimulate the physiological change.Electrotherapy is therefore little different frommanual therapy or anything else in the treatmentrealm. It is a tool that, when applied at the righttime, at the right dose and for the right reason, hasthe capacity to be beneficial. Applied inappropri-ately, it is not at all surprising that is has the capac-ity to achieve nothing or in fact to make thingsworse. The skilful practitioner uses the availableevidencecombined with experienceto make the bestpossible decision taking into account the psycho-socialand holistic components of the problem - it isnot cl simple reductionist solution.
ElECTROTH ERAPEUTIC WIN DOWS
Windows of opportunity are topical in many areasof medical practice and are not a new phenomenonat all. It has long been recognised that the 'amount'of a treatment is a critical parameter. This is no lesstrue for electrotherapy than for other interven-tions. Literally hundreds of research papers illus-trate that the same modality applied in the same
Introduction: current concepts and clinical decision making in electrotherapy 7
circumstances, but at a different 'dose', will pro-duce a different outcome. The illustrations used inthis section are deliberately taken from cell, ani-mal and clinical research studies with variousmodalities to illustrate the breadth of the princi-ple. Furthermore, the examples used are notintended to criticise the researchers reportingthese results. Knowing where the window 'is not'is possibly as important as knowing where it is.
Given the research evidence, there appear to beseveral aspects to this issue. Using a very straight-forward model, there is substantial evidence, forexample, that there is an amplitude, window orstrength window. An energy delivered at a particu-lar amplitude has a beneficial effect, whereas thesame energy at a lower amplitude-might have nodemonstrable effect. The laser example above is asimple extension of this case - one level will pro-duce a distinct cellular response whereas a higherdose can be considered to be destructive. Karu(1987)demonstrated and reported these principlesrelated to laser energy and the research producedsince has served to reinforce the concept (Vincket a12003).
There are many examples of amplitude win-dows in the electrotherapy-related literature, andin some instances, the researchers have not set outto evaluate window effects but have none the lessdemonstrated their existence. Papers by Larsenet al (2005)measuring ultrasound parameter manip-ulation in tendon healing, Aaron et al (1999)investi-gating electromagnetic field strengths, Goldmanet al (1996)considering the effectsof electrical stim-ulation in chronicwound healing, Rubin et al (1989)investigating electromagnetic field strength andosteoporosis and Cramp et al (2002)comparing dif-ferent forms of TENS and its influence on localblood flow all provide evidence in this field.
Along similar lines, frequency windows are alsoapparent. A modality applied at a specific fre-quency (pulsing regimen) might have a ineasurablebenefit, whereas the same modality applied usinga different pulsing profile might not appear toachieve equivalent results.
Electrical stimulation frequency windows havebeen proposed and there is clinical and laboratoryevidence to suggest that there are frequency-dependent responses in clinical practice. TENSapplied at frequency X appears to have a different
outcome to TENS applied at frequency Y in anequivalent patient population. Studies by Hanet al (1991),Kararmaz et al (2004)and Sluka et al(2005)are among the many that have demonstra-ted frequency-dependent effects of TENS. Severalauthors have appeared to demonstrate that fre-quency parameters are possibly less critical, espe-cially in clinical practice, and Chapters 16 and 17,on TENS and interferential therapy, include usefuldiscussion on these issues. Frequency windows'are not confined to TENS treatments and there areexamples from other areas, including electromag-netic fields (Blackman et al 1988), ultrasound(Schafer et al 2005) and interferential (Noble et al2000).
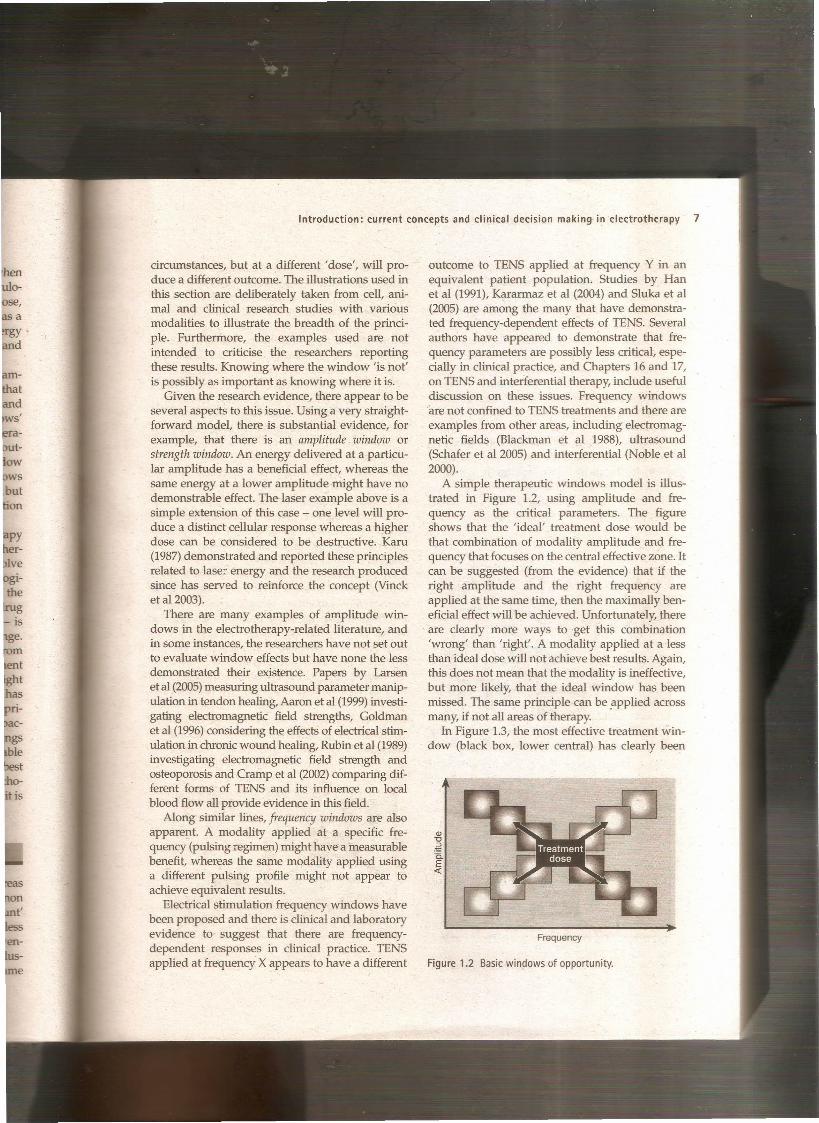
A simple therapeutic windows model is illus-trated in Figure 1.2, using amplitude and fre-quency as the critical parameters. The figureshows that the 'ideal' treatment dose would bethat combination of modality amplitude and fre-quency that focuses on the central effective zone. Itcan be suggested (from the evidence) that if theright amplitude and the right frequency areapplied at the same time, then the maximally ben-eficial effect will be achieved. Unfortunately, thereare clearly more ways to get this combination'wrong' than 'right'. A modality applied at a lessthan ideal dose will not achieve best results. Again,this does not mean that the modality is ineffective,but more likely, that the ideal window has beenmissed. The same principle can be .applied acrossmany, if not all areas of therapy.
In Figure 1.3, the most effective treatment win-dow (black box, lower central) has clearly been
Frequency
Figure 1.2 Basic windows of opportunity.

8 INTRODUCTION AND SCIENTIFIC CONCEPTS
missed by the delivered treatment (upper left) andhence whatever the effect of the therapy, it will failto be maximally effective.
The situation is complicated by the apparentcapacity of the windows to 'move' with thepatient's condition. The position of the therapeuticwindow in the acute scenario appears to be differ-ent from the window position for the patient witha chronic version of the same problem. A treat-ment dose that might be very effective for an acuteproblem may fail to be beneficial with a chronicpresentation.
In Figure 1.4, the effective 'acute window'shown in the left-hand picture is in a differentposition to the most effective 'chronic window'shown in the right-hand picture.
Given the rapidly increasing complexity seen inthis simple two-parameter model (amplitude and
ID"0
.~0.E«
Frequency
Figure 1.3 Treatment dose 'missing' the window.
ID"0
~0.E«
Frequency
Figure 1.4 Moving acute (A) and chronic (B) windows.
frequency) with two levels of condition (acute andchronic), it is easy to see how difficult clinical real-ity might be. As the volume of published workcontinues to increase, new results can be includedin the existing framework, and this helps toidentify where the windows are (positive researchoutcomes) and where they are not (negative out-comes). If this methodology is pursued, it is inter-esting to note how the effective treatments clusterwhen plotted, adding weight to the therapeuticwindows theory.
Assuming that there are likely to be more thantwo variables to the real-world model, some com-plex further work needs to be invoked. There isalmost certainly an energy- or time-based window(e.g. Hill et al 2002)and then another factor basedon treatment frequency (number of sessions a weekor treatment intervals). Workcontinues in our own,and other, research units to identify the more andless critical parameters for each modality across arange of clinical presentations.
One research style that has proved to be helpfulin this context is to test a treatment on non-injuredsubjects in the laboratory using a variety of doses,and then to take the same protocol out into theclinical environment and repeat the testing proce-dure with real patients with particular clinicalproblems. Preliminary results indicate that thereare distinct differences between the responses on'normal' and 'injured' tissues at equivalent dosesand further work is essential to maximise ourunderstanding of these behaviours. Research thatdemonstrates significant effect in a laboratorystudy might, or might not, transfer directly to
ID"0
~0.E«
Frequency

Introduction: current concepts and clinical decision making in electrotherapy 9
the clinical environment. Recent work with pulsedshortwave therapy (AI Mandil & Watson 2006)clearly demonstrated a different magnitude ofphysiological effect when the same 'treatment'was delivered to asymptomatic subjects in the lab-oratory and real patients in a clinical setting: thephysiological changes were similar, but of a differ-ent magnitude.
CLINICAL DECISION MAKING INELECTROTHERAPY
When it comes to making a clinical decision withregard to electrotherapy as a component of treat-ment (and taking into account the precedingsections), it can be seen that the effects of the inter-vention appear to be both modality and dosedependent (at least to some extent), and thus bothelements need to be taken into account. The firstdecision needs to be with regards to the modality,as this is the primaryconcem; the secondary deci-ion, although still of importance is that of dosage.
This having been said, it is important to remem-ber that the use of electrotherapy in clinical prac-tice is a matter if its integration into the wholetreatment programme. Rarely is electrotherapyalone the most beneficial way forward. There aretimes when this might be the case, but they are theexception rather than the rule. Some patients-'ould gain nothing significant from the additionof a modality into their treatment programme,
"hereas others would derive considerable gains.Electrotherapy has, in the past, probably been ano 'erused intervention. Its current incorporationinto clinical practice is more e.vidence based andselective, and hence should be more effective.
The detailed chapters in this text examine the-idence base for each of the modalities covered
and, within that evidence, the ·areas where themodality has the capacity to be effective and those
.here there is insufficient evidence at the presentnme. A commonly cited phrase that is important
this context relates to the difference between ak of evidence as opposed to an evidence of lack; in
ther words, there are many areas of practice,. eluding several areas in electrotherapy, wherethere is a substantiai lack of evidence - it is simply
t there - whereas in other areas there is evidence
that demonstrates a lack of effect. In the formercircumstance, the clinician might have to make aclinical decision based on experience and expertopinion in the absence of published research. Inthe latter circumstances, the clinician who takesaccount of the available evidence would refrainfrom adopting that particular clinical approach infavour of another.
If it were simply a matter of learning a set of rulesor guidelines, the use of electrotherapy in practicemight appear to be somewhat simpler but, in reality,there are (at present at least) no rule sets that wouldgovern any possible clinical scenario, and thereforeclinical decision making remains an art with a scien-tificbias, or a science with an integrated art, depend-ing on which philosophy you follow. Whicheverone of these it is, the employment of electrotherapyinto current clinical practice cannot be reduced to asimple rule set, and possibly it never will. The evi-dence will continue to close the gaps, although,inevitably, by closing down one gap, another willbecome apparent, and hence further research will beneeded.
The individual chapters in this text aim to iden-tifythe key issues about each modality, examinethe evidence for their effects and relate this to clin-ical practice. None of the chapters aims to provideclinical recipes, but will enable practitioners toevaluate the available evidence in order to facili-tate their clinical decision making.
CONCLUSION
Incorporation of electrotherapy modalities intoclinical intervention programmes can result in sig-nificant benefit for the patient. Used unwisely, it isat best an inefficient use of resources and at worst,can easily have effects that are neither wanted norbeneficial. Critical clear thinking, an understand-ing of the capacity of the various modalities toinfluence the tissues combined with the joined-upthinking that links this aspect of practice with oth-ers such as manual therapy and exercise therapycan result in gains for the patient. Patients who areroutinely denied electrotherapy because the clini-cian does not believe it to be effective would seem,based on the evidence presented in this text, to bedenied potential benefit.