Embed Size (px)
Citation preview
1
CHAPTER 1
1.0 BACK GROUND INFORMATION
Antenatal booking is the first visit by a pregnant woman to the health facility for the purpose of
initiating antenatal care services. Early booking into antenatal is very cardinal because it provide
an opportunity for the health care provider to detect and treat pregnancy- related factors that may
lead into complications as well as increase positive patient outcomes. Currently Zambia has
recorded a reduction in maternal mortality rate which stand at 278 deaths per 100,000 live births.
This has been viewed as a reduction but the number is still alarming. Generally, identified factors
which contributes to maternal mortality includes: late antenatal booking, antepartum
haemorrhage, medical conditions such as (pregnancy induced hypertension, diabetes mellitus,
anaemia, cardiac conditions) early pregnancies (pregnancies in the under age), multiple
pregnancies unsafe abortions and many more. According to the latest update from the Zambia
national health demographic survey conducted in the year 2017, reveals that late antenatal
booking amongst pregnant women is the major contributing factor to maternal mortality. Being
the leading Couse of mortality, late antenatal registration if studied well and properly addressed,
may reduce maternal mortality.
Baker (2012) states that when a woman books early into antenatal care, it makes it feasible for
accurate estimation of gestational age. This will empower the health care provider with an
opportunity to evaluate the pregnant woman by identifying risk factors which should be
eliminated in order to promote a safe and healthy delivery. According to the safe motherhood
guidelines, it is advisable that a pregnant woman report to the health facility as soon as she feels
she is pregnancy for early identification and further technical health advice. This is also
highlighted in the World organization recommendations. Villar, J. (2002) recommend that
pregnant women should access ANC services as soon as they realize that they are pregnant and
this should be before twelve weeks of gestation. Any pregnant woman registering for her first
time after 12 weeks of gestation is considered to register late or late booking. This would mean
that such women may not have the opportunity to benefit from screening tests, antenatal
education and health advice, or supported decision-making regarding the place and choice of
delivery, Baker-(2012). Late booking has been linked to increased infant and maternal morbidity
2
and mortality. This is because such women, report to the health facilities with already developed
complications that may be difficulty to control or manage due to various factors.
Globally, women who do not utilize antenatal care services are about 45 million in which the
bigger number is in sub-Saharan Africa, WHO (2012). Antenatal care is key strategy to
improving maternal and infant health globally. However, data from a survey done in sub-Saharan
Africa showed that women often initiate ANC late, therefore they fail to meet the recommended
number of ANC visits, Pell. et al. (2013). In this case, it would mean that such women might
have already missed some appointments which were made or planned with the health care
provider. Such women reports to the health facilities with already developed complications
which comes other cost of management.
Despite antenatal care services being provided free of charge or sometimes at a minimal cost in
Zambia, very few women attend antenatal care by their fourth month of pregnancy as per safe-
motherhood guidelines. As stated earlier on, although Zambia has achieved reductions in
maternal mortality rates, the current levels, are still unacceptably high. Unless additional and
significant efforts are made, Zambia may not attain the desired sustainable development goal
(SDG) number 3 targets by the year 2030. There is thus need to re-examine current efforts and
approaches in order strengthen or propose other interventions which should aim at ensuring that
set targets are achieved. Nyambe (2015) state that, strategies on how to operationalize and scale
up these interventions is the challenge. Spotted factors that are associated with the high maternal
mortality rate (MMR) in Zambia to be specific include challenges to accessing services (1st and
2nd delays), cultural factors, poor referral system, transport difficulties late ANC booking and
other factors. Poor antenatal coverage contributes to high levels of maternal mortality. Narrowed
down to Mwansabombwe district, the situation is not deferent. Late antenatal booking among
pregnant women is as high as 60% of the total number of pregnant women who registered in the
1st and 2nd quarter of 2018 (Mwansabombwe District-HMIS 2018)
1.2 PROBLEM STATEMENT
Perspectives of pregnant women on late ANC registration have been extensively studied
globally, internationally and locally. Findings include: health systems related factors, patient
related, social – economic, individual perceptions and knowledge, HIV and AIDS among many
are found to be the leading cause. However, various recommendations have been made in
3
response to the findings such as deployment of various skilled personnel in the area of maternal
health to improve on human resource, increase and improvement of infrastructures, empowering
women and families and many more. These measures have been implemented in various
countries (Zambia inclusive) at various levels of obstetric care services successfully. Beside the
success in the implementation of such measure, the trend is still being observed in different
places more especially in rural places such as in Mwansabombwe district of Luapula province
Zambia. According to the desk reviewed data for the complete year of 2018, the catchment
population for the district was 55,478 representing (100%) based on Central Statistics Office’s
guide (CSO), 2,996 women registered for the first ANC registration representing 5.4% of the
total catchment population, 1029 pregnant women registered before 14 weeks of gestation
representing 34.5% and 1967 pregnant women registered after 14 weeks representing 65.7%. –
Zambia HMIS (2018). According to the guidelines 65.7% pregnant women registered late for
ANC services. Late ANC contribute largely to the maternal and prenatal mortality –Nkumbula et
al (2018). According to the Zambian daily mail dated 5th September 2019, the Zambian
government declared maternal and prenatal mortality as a public health emergency. Therefore,
prevention of maternal and prenatal mortality needs informed decisions from studies such as this
one which aimed at exploring women perspectives and further provide more information on how
pregnant women perceive late ANC booking. This study will largely provide evidences
pertaining to the women’s general perspective and perceptions concerning late ANC booking
which will help decision makers to make informed decisions that will help in the prevention of
complications that comes as a result of late ANC booking.
1.3.1 GENERAL OBJECTIVE
To determine the pregnant women’s perspectives towards late ANC registration in
Mwansabombwe rural district of Luapula province - Zambia.
1.3.2. SPECIFIC OBJECTIVES
Mwansabombwe district.
women in the district.
4
To investigate the level of awareness on dangers of late antenatal registration amongst
pregnant women in the district.
rative/managerial and policy level measures that
could be put in place to reduce late ANC registration in the district.
1.4. RESEARCH QUESTIONS
specific factors contributing to late antenatal care registration in the
district?
antenatal registration in the district?
munity, administrative/managerial and policy level
measures that could be put in place to reduce late ANC registration in the district?
1.5. STUDY SCOPE
This study was confined to the selected clinics while in Mwansabombwe district. Communities
including relevant local neighborhood health catchment zones while targeting women that have
given birth before who were the study participants.
1.6 THEORETICAL FRAMEWORK - HEALTH BELIEF MODEL
The following theoretical framework is extracted from the Health Believe Model (HBM) which
was developed by Godfrey Hochbaum, Irwin Rosenstock and Stephen Kegels in 1950 and
revised in 1974. Later improved by Leventhal, Rosenstock, (1960) improved again by Becker
(1974).It has been adopted to help analyzing data related to general and specific objectives stated
above. It will be used to analyze individual pregnant women perceptions, modifying factors and
likelihood of action factors- Rosenstock et al (1974). The model addresses the individual’s
perceptions of the threat posed by a health problem like susceptibility and severity as well as
factors influencing the decision as explained below:
5
PERCEIVED BENEFITS - This refers to a person's perception of the effectiveness of various
actions available to reduce maternal complications that comes as a result of late antenatal
registration – Rosenstock et al (1974). According to Rosenstock, the course of action a person
takes in preventing or curing an illness or disease relies on consideration and evaluation of both
perceived susceptibility and perceived benefit. This will help in determining women perception
of the effectiveness of their actions in order to reduce late ANC booking.
PERCEIVED BARRIERS – This refers to a person’s feelings on an obstacle to performing a
recommended health action – Rosenstock (1974). The model further states that, there is a wide
variation in a person's feelings of barriers, or impediments which lead to a cost/benefit analysis.
This will be applied to determine pregnant women perceptions on the obstacles which hinder
them from seeking early ANC registration. The model further states that, a person weighs the
effectiveness of the actions against the perceptions that it may be expensive, dangerous (e.g., side
effects), unpleasant (e.g., painful), time-consuming, or inconvenient.
PERCEIVED SUSCEPTIBILITY - This refers to a person's subjective perception of the risk
of acquiring an illness or disease. E.g. a person who sun bathes every day and does not believe
that he is at risk of skin cancer- Rosenstock (1974). This will help in understanding the women
perception on late ANC including the risk factors. The model further state that, if a person
believes he is at risk of an illness he is likely to do something about it. Hence if pregnant women
who register late for ANC believes they are at risk of complications, then they would suggest
something that they expected to do to prevent late ANC registration. Furthermore, Rosenstock
stated that, there is a wide variation in a person's feelings of personal vulnerability to an illness
or disease. Therefore, this will help in analyzing women perception involving their vulnerability
to late ANC registration.
SELF-EFFICACY - This refers to the level of a person's confidence in his or her ability to
successfully perform a behaviour – Rosenstock et al (1974). He further said that, Self-efficacy is
a construct in many behavioural theories as it directly relates to whether a person performs the
desired behaviour. This will help in assessing the pregnant women’s effort to start early ANC
booking.
6
CHAPTER 2
2.0. LITERATURE REVIEW
This section gave an account of what other researchers had contributed to understanding of
women perceptions towards late antenatal booking and the extent to which they have addressed
perceptions of women on late antenatal registration.
WOMEN PERSPECTIVES ON LATE ANTENATL CARE (ANC) REGISTRATION
PERCEIVED NEED TO KEEP EARLY PREGNANCY SECRET.
Keeping the pregnancy secret has been a trend in many societies especially in rural areas of
developing countries. This is due to various reasons of which some are related to religion,
tradition, culture and many more. According to the study conducted by Nelly (2019), most
women become so reluctant to disclose a pregnancy before 12 weeks gestation and initiation
antenatal due to cultural beliefs about vulnerability of pregnancy in the early stages and the need
to safeguard the pregnancy by keeping a secret from friends, family and the general public. Early
attendance of ANC services requires disclosure of the pregnancy and ANC booking therefore is
postponed until disclosure is inevitable – Nelly et al (2019).
PURPOSEFUL POSTPONEMENT OF ANC BY MULTIGRAVIDA WOMEN
It is said experience is the best teacher. This has sunk deep in most of our older women who
believe to know it all. After going through a lot of ANC sessions for the previous pregnancies
and mastered what happens at ANC clinics, they tend to postponed ANC booking and sometimes
not booking at all. Some consider themselves as experts reaching an extent of conducting
deliveries for the young ones at home. According to Annesa et al (2019), women with previous
pregnancies, especially older women, do not value ANC services in early pregnancies and
purposefully postponed ANC attendance. This is attributed to women perceived experience and
knowledge gained in prior pregnancies – Annesa et al (2019). Further, the study reveal that
negative ANC experiences during previous pregnancies such as congestions and being shouted at
by the staff among many, retained for too long at the facility luck of support especially those
women are not married and many more are important deterrent to early ANC attendance among
older women. As a result, women prefer to book late for ANC in order to avoid going through
the some experience.
7
PERCEIVED KNOWLEDGE ABOUT THE BENEFITS OF ANC
They say knowledge is power, because it empowers someone to be involved in carrying out a
particular activity willingly. With full knowledge about the benefits that comes with early ANC
registration pregnant women may be very much willing to participate in the early initiation of
ANC. According to Moola, most women who initiate ANC late do not perceive any benefits
from early ANC registration- Moola et al (2018). He further state that pregnant women believe
that ANC booking is only to receive the antenatal cards. The study further reveals that women
have a common perceptions that early booking led to more visits, hence prefer less visits by
postponing ANC attendance. Similar findings were reported in a study by Jewkes at al (2018)
where women did not perceive benefits of early booking and risks associated with late ANC
bookings. According to Jewkes, most pregnant women perceive pregnancy as natural
physiological process hence postponed ANC visits until any medical condition force them to
visit a health facility. According to Mayer and Harrison (2017), women do not perceive
pregnancy as an immediate health risk and their views are that, early booking is not necessary.
UNAVAILABILITY AND INACCESSIBILITY OF OBSTETRIC CARE SERVICES
Unavailability and inaccessibility of obstetric care services has been a challenge affecting most
developing countries. These include inadequate logistics such as drugs, inadequate infrastructure
leading into pregnant women covering very long distances to access obstetric care centers.
According to the study conducted by Onoya et al (2017), some pregnant women postponed their
ANC visits because of unavailability and inaccessibility of health services. Rural areas are
known to be poorly resourced and have fewer skilled health care workers. As a result, pregnant
women postponed their ANC visits in order to reduce on burdening the fewer health workers
who they feel are angered by too much pressure of work and reduce on the demand for logistics.
STIGMA RELATED PERCEPTIONS
Stigma related to HIV/AIDS is still a very big challenge in most countries. It is worse in rural
areas where sensitizations have not reached most of the people. Being a mandate that all
pregnant mothers have to be tested, most women shun ANC services for fear of being diagnosed.
According to the study conducted by Sibeko and Moodley, most women who are found to be
living with HIV are often reluctant to share the information with their partners and families.
They fear discrimination, stigma, violence, abandonment and other social consequences. Sibeko
8
further reveal that women becomes so reluctant to initiate early ANC clinics to avoid HIV test
because the HIV test is part of PMTCT, hence women postponed ANC visits to avoid HIV
testing because they fear losing their partners if they disclose their HIV statuses - Sibeko and
Moodley (2019).
INDIVIDUAL PERCEPTIONS AND KNOWLEDGE
Perception differ from person to person. Persons with more information or knowledge about
something perceives situations differently compared to those with low level of understanding or
with little information. Pregnant women with low levels of education perceives ANC services to
be of no value as compared to women who are educated. Haddrill said, experiences of past
pregnancies had a direct impact on the timing of ANC bookings – Haddrill et al (2017). In his
study, he found that pregnant women who had low levels of education postponed their ANC
visits because they did not perceive any benefit from early ANC booking. The study further
reveals that women with low levels of education who attended ANC in the previous pregnancy
did not do it again. As a result luck of basic education leads some of the pregnant women not to
perceive the pregnancy as requiring ANC and medical attention.
TRAVEL COST, LOSS OF INCOME AND WORK COMMITMENTS
Travel costs, loss of income and work commitments are among many factors that contribute to
pregnant women to perceiving ANC services being an option and not a priority- Mongwenyana
et al (2017). This is due to fear of getting tired as a result of covering long distances to access the
health facilities. Others believe that when they fall pregnant, that’s the time to moving around
looking for money to prepare for baby. This is common to the single women – Mathias et al
(2016). To some extent, even those who are married when they fall pregnant unexpectedly, they
go into panicking in order to prepare for what was not planned for. It is a well-known fact that
travelling cost in initiating ANC services for pregnant women remain adherent to subsequent
visits more especially in developing countries particularly in rural and remote areas –
Mongwenyana et al (2017). According to Mongwenyana, employed women straggle to book
early for ANC because of work commitments. He said, employed women from the communities
that they serve could not have maternity benefits or paid leave to attend ANC. As a result, unless
physically unwell, attending ANC is of lower priority compared to other pressing
9
responsibilities. Therefore, in order to save some money that could be used for transportation
women preferred to book late for ANC or even not book at all.
PARTNER NEGLECT AND LOSS OF SUPPORT
Partner neglect and loss of support is among challenges pregnant women faces in most countries
more especially in developing countries where the poverty levels are high. Both women in
marriages and those in relationships does everything possible to please their partners to the
extent of not booking for ANC if they are not told to do so. According to Isaac (2016) some
unmarried women’s opinion are that, fathers of the babies’ loose interest in them on early
disclosure of pregnancies. Therefore, many women do not want to disclose their pregnancy
because they fear loss of support from the partner. They tend to hide their pregnancy in a view to
delaying ANC registration that favors them to enjoy support from their partners – Isaac et al
(2016).
OVERCROWDING AT THE CLINICS AND LONG QUEUES
Inadequate infrastructure in most developing nations result into congestions at the obstetric care
facilities and these discourages pregnant women from registering early for ANC services- Banda
(2011). In many countries mostly developing countries, women endure long waiting times and
sometimes turned away because of limited staff to attend to them - W.H.O. (2017) .In some
cases, clinics imposes daily quota and turn away women who come after the quota is reached –
Constance et al (2018). These among many other discouraging decisions make women to book
late so that they reduce on the contact and avoiding frequent disappointments.
SOCIAL ECONOMIC FACTORS
Social – economic factors remain a challenge impacting negatively in early ANC booking for the
pregnant women. According to Daniel et al (2017) women choose to seek antenatal care at the
time convenient for them depending on their social circumstances, community perceptions and
health care provider related issues. The social circumstances are financial dependence on others
and easy accessibility of health care facility. Financially insecure women find it difficult to make
their own informed decisions on their pregnancies. As a result pregnant women prefer to delay
ANC registration so that they give time for their partners or guardian who may be planning for
abortion. Early initiation of ANC services would make the pregnancy known to the public.
10
CHAPTER 3
3.1.0 RESEARCH METHODOLOGY
This section dealt with the means to answer the research questions and a justification as to why
this was the best available means.
3.1.1 RESEARCH DESIGN
This section provided a guide that was used to come up with the right answers to research
question. It is a systematically guides the processes the collected data, analysis and
interpretation. This qualitative study is aimed at exploring pregnant women’s personal
experiences about late ANC booking as well as their preferred actions and suggestions which
they feel when implemented by various stakeholders could help them register early for antenatal
care services thereby reducing maternal/neonatal mortalities related to late ANC registration.
3.1.2. SOURCE OF DATA
Data was collected directly from the participants (primary data) using a pretested structured
questionnaire that was administered through contact interview with the participants while in the
research area. Women’s perspectives on late ANC booking was assessed using a number of
questions organized in a questionnaire that was well designed. Three data collectors and one
supervisor was engaged during data collection period.
3.1.3. TARGET POPULATION
The target population which is the total group of individuals from which the sample was drown.
Participants are a group of people who took part in the study. The district has 6 operational
health facilities where reproductive health services are provided. These facilities have different
catchment populations which were targeted for this study. Of the six (6) only 5 facilities were
randomly selected for this study. 30 women from each randomly selected health facility were
picked to come up with a total of 150 participants who were interviewed. The study population
was composed of women aged 16 to 45 years who have delivered before to be interviewed
during primary data collection.
11
3.1.4. INCLUSION CRITERIA
Refers to the technique used to select eligible participants to be included in the study. And the
following were criterion.
-45 years were interviewed using the women’s questionnaire in
the selected catchment areas during the study.
rs period preceding the study.
ANC in their last pregnancy within five years preceding the study.
emale respondents who remembered the number of months their pregnancy was when they
first received ANC evidenced and those who answered appropriately to the question that was
asked on how many months pregnant they were when they first received ANC.
3.1.5. EXCLUSION CRITERIA
Refers to the technique used to exclude participant before the interview or before data analysis
based on certain factors as outlined below.
Female respondents who had not been pregnant during the five years preceding the study or
those who answered ‘NO’ to the question whether they had fallen pregnant during the five years
preceding this study.
analysis)
to be interviewed during the survey.
3.1.6. SAMPLE SIZE
This referred to the number of participants that were drawn from the total population for research
purposes. This included all women who met the inclusion and exclusion criteria that was, history
of a live birth during the five years preceding this study, attended ANC for their last pregnancy
which resulted in a live birth and could remember the number of months they had their first
antenatal care visit to the health facility. The total number of participants were 150.
12
3.1.7. DATA EXTRACTION AND CLEANING
All the information required for the analysis was obtained directly from the participants (primary
data). The individual recoding contained all the responses to the woman’s questionnaire used
during the data collection (interview). Only variables that were important for analysis were kept
as part of the data cleaning process.
The outcome variable was women’s perception on late ANC booking. The predictor variables
were checked for completeness and only those variables with complete information were
included for analysis. The predictor variables that were checked for completeness were the
respondent’s age, education level, number of years of education, previous pregnancies, number
of registered pregnancies, knowledge on the importance of early ANC booking economic status
and ideas on why some women register late for ANC and suggestions to the role of women in
reducing late ANC booking as well as health care satisfaction.
3.1.8 SAMPLING METHODOLOGY
Sampling referred to a technique in which a part or subset of a population (a sample) was
systematically selected for this study. The results from this sample were generalized onto the
entire population of the District. Systematic/interval sampling: Involves the selection of
participants at equal intervals. Every 5th participant was picked for the interview. Lists was
randomized and not in alphabetical.
3.1.9 RESEARCH INSTRUMENTS USED
The data was well collected using a structured questionnaire which was administered through
contact interview (one to one). Women’s perspectives on late ANC booking was assessed using a
number of questions. The questionnaire was prepared in English and then translated into
icibemba (local language) and later on it was translated back to English. The local language
version of questionnaire was used to collect data.
3.1.10. ETHICAL CONSIDERATION
Ethical approval was obtained from the relevant ethical committee to conduct a study (appendix
IV), while informed consent was obtained from the eligible participants. It was being made clear
to the participants before participation in the study. Furthermore, participant’s confidentiality
13
was well maintained throughout the study. Regarding participant’s consent form, information
was explained in the language that the participant understood using the information sheet.
Concerns and questions that the participant had were answered and clarified in simple terms by
using icibemba as a local for those who could read and write, managed to consent orally and
signed the consent form while those who could not read nor write, information were given by the
researcher and the research team members and the and then oral consent got and a thumb print
was used in place of signing on the consent form. No participant was forced to participate in the
study. In order to maintain confidentiality, no information regarding names of the participant was
obtained. Data was only used for the purpose of this study and not given to any person or
organization. Since there was a direct contact with the participant in the study, obvious injury to
the participant was considered and were avoided.
3.1.11. DATA ANALYSIS
Data analysis was done using SPSS software, version 16.0 SE (SPSS Corporation, TX, USA).
Firstly descriptive statistics were used to compare the variables, cross tabulation to determine the
overall distribution of predictor variables in determining women perception on late ANC
booking and then graphical presentation of the determined variables.
Data validity: in order to ensure validity, all variables were covered in the interview schedule.
The questions were clearly constructed to avoid ambiguities
RESULTS
Descriptive statistics of factors used to depict women perception on late ANC booking in
Mwansabombwe district. 150 women were interviewed and overall response rate was 92 per
cent. Of the eligible and successfully interviewed population of all females aged 16 to 49, only
the records of respondents that had completed the interview (n=138), including answering the
information on perception on late ANC booking were included in the final analysis. Of the 138
women47% (66) were in the age group of 26- 35 year which was the majority, 30.4% (42) were
in the age group of 16-25 years and 21.7% (30)women were in the age group of 36 to 45 which
was the least. The frequency distribution of predictor variables for determining women
perception on late ANC booking is summarized in the following tables which are coupled with
charts
14
CHAPTER 4
4.0 DATA PRESENTATION
This section gives out the research findings including their meaning or interpretation. This is
done through use of tables coupled with text/explanations to infer/illustrate aggregates or
strength/weakness of opinions or evidence against particular variable or research questions.
Tables will need to have a (table) number and title, and will be accompanied by a brief
explanations (below each table and on the same page) in terms of meaning or interpretation.
15
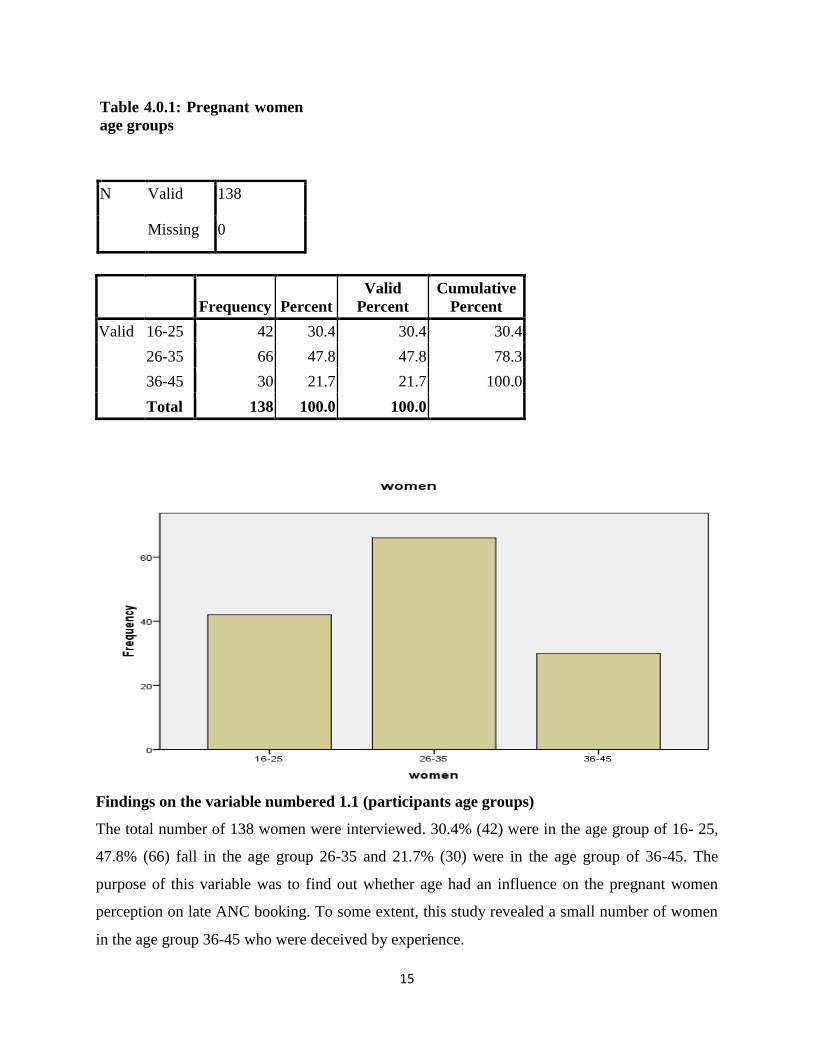
Table 4.0.1: Pregnant women
age groups
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 16-25 42 30.4 30.4 30.4
26-35 66 47.8 47.8 78.3
36-45 30 21.7 21.7 100.0
Total 138 100.0 100.0
Findings on the variable numbered 1.1 (participants age groups)
The total number of 138 women were interviewed. 30.4% (42) were in the age group of 16- 25,
47.8% (66) fall in the age group 26-35 and 21.7% (30) were in the age group of 36-45. The
purpose of this variable was to find out whether age had an influence on the pregnant women
perception on late ANC booking. To some extent, this study revealed a small number of women
in the age group 36-45 who were deceived by experience.
16
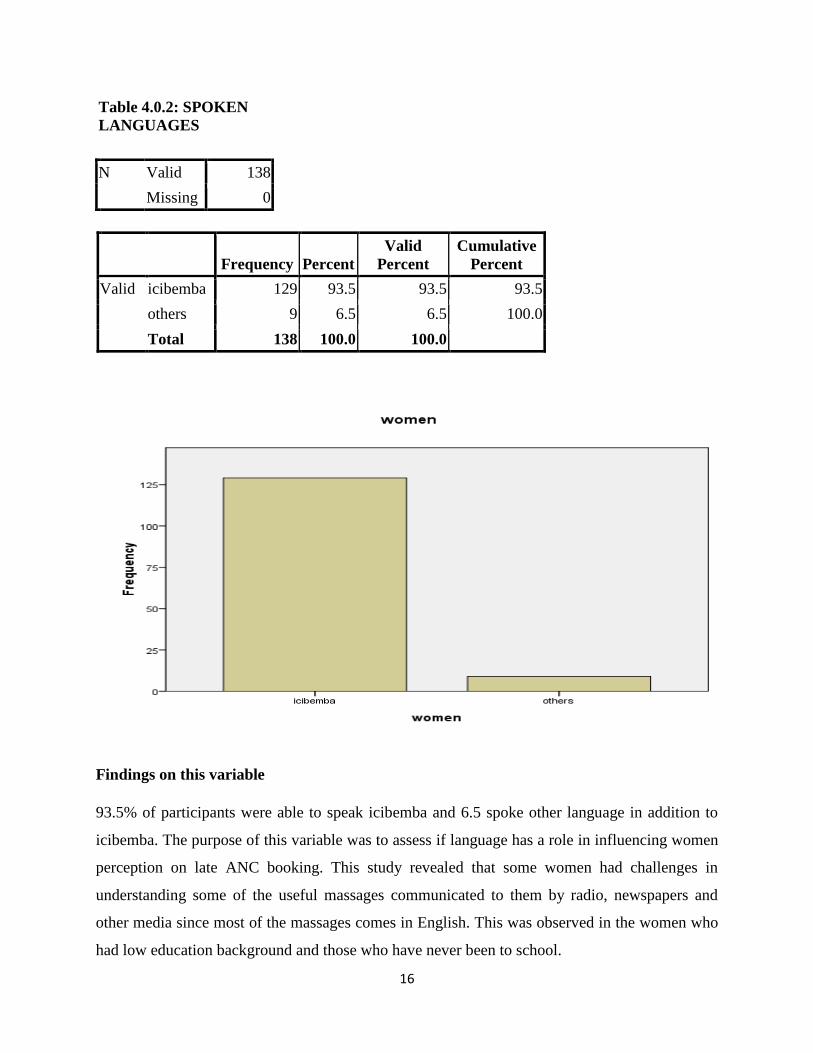
Table 4.0.2: SPOKEN
LANGUAGES
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid icibemba 129 93.5 93.5 93.5
others 9 6.5 6.5 100.0
Total 138 100.0 100.0
Findings on this variable
93.5% of participants were able to speak icibemba and 6.5 spoke other language in addition to
icibemba. The purpose of this variable was to assess if language has a role in influencing women
perception on late ANC booking. This study revealed that some women had challenges in
understanding some of the useful massages communicated to them by radio, newspapers and
other media since most of the massages comes in English. This was observed in the women who
had low education background and those who have never been to school.
17
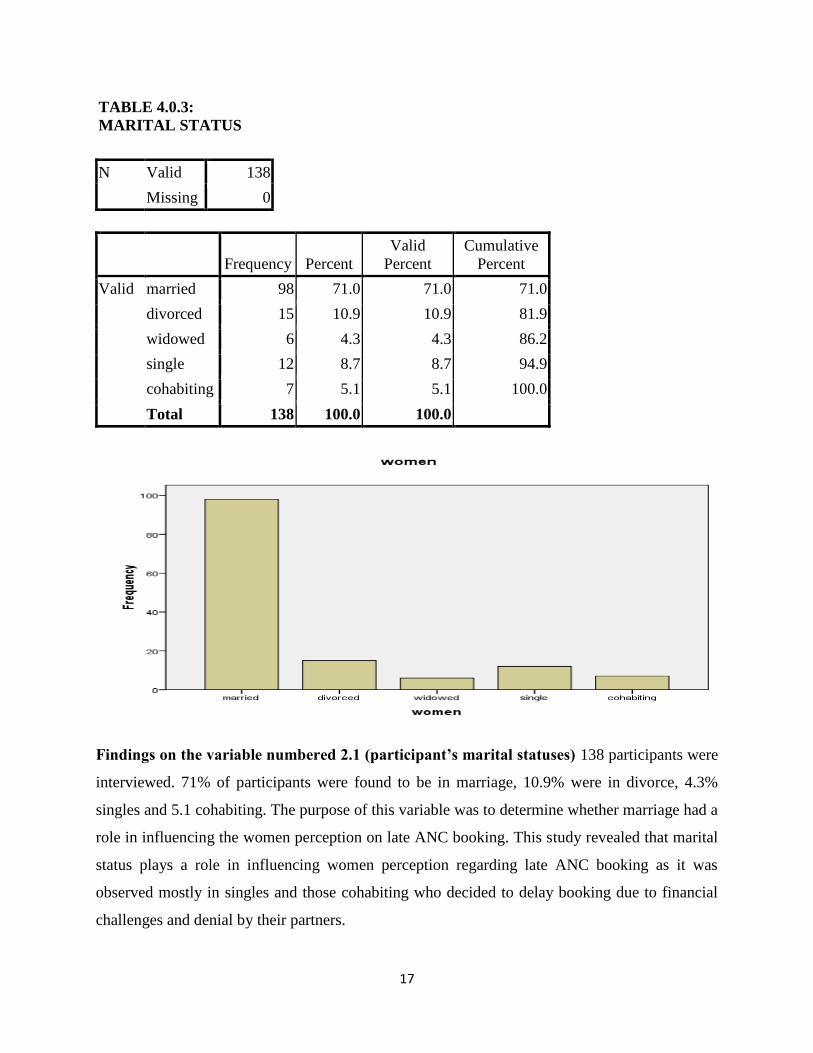
TABLE 4.0.3:
MARITAL STATUS
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid married 98 71.0 71.0 71.0
divorced 15 10.9 10.9 81.9
widowed 6 4.3 4.3 86.2
single 12 8.7 8.7 94.9
cohabiting 7 5.1 5.1 100.0
Total 138 100.0 100.0
Findings on the variable numbered 2.1 (participant’s marital statuses) 138 participants were
interviewed. 71% of participants were found to be in marriage, 10.9% were in divorce, 4.3%
singles and 5.1 cohabiting. The purpose of this variable was to determine whether marriage had a
role in influencing the women perception on late ANC booking. This study revealed that marital
status plays a role in influencing women perception regarding late ANC booking as it was
observed mostly in singles and those cohabiting who decided to delay booking due to financial
challenges and denial by their partners.
18
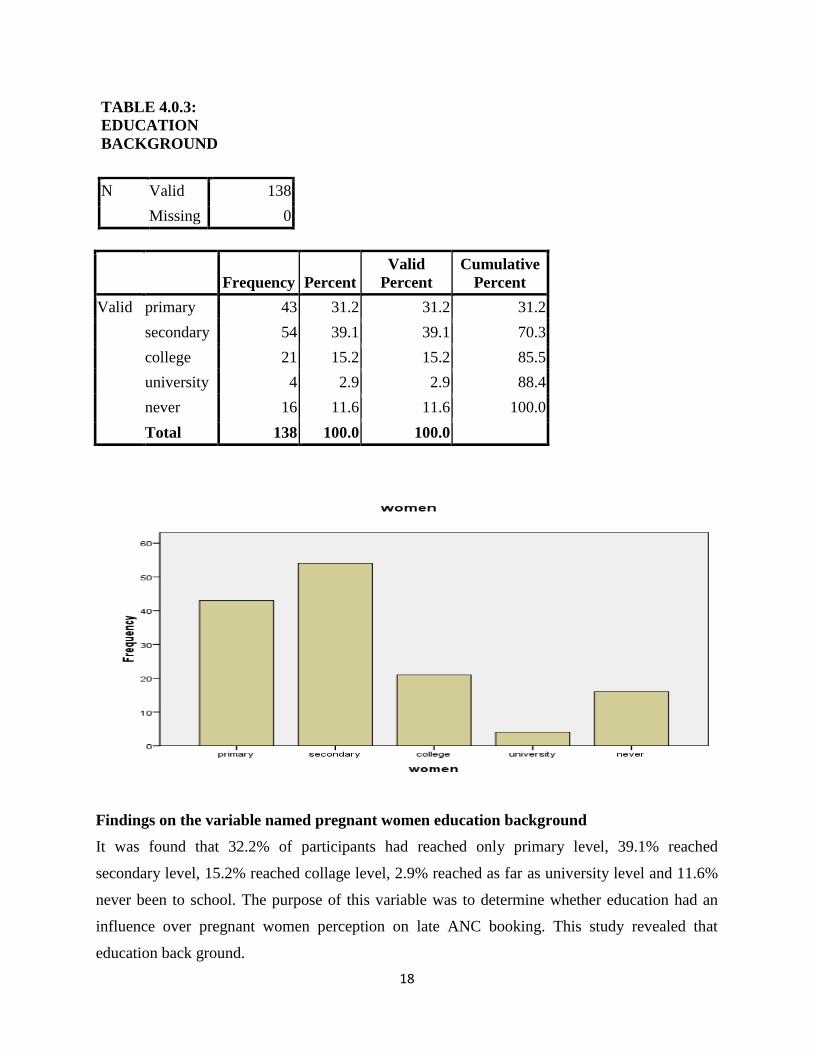
TABLE 4.0.3:
EDUCATION
BACKGROUND
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid primary 43 31.2 31.2 31.2
secondary 54 39.1 39.1 70.3
college 21 15.2 15.2 85.5
university 4 2.9 2.9 88.4
never 16 11.6 11.6 100.0
Total 138 100.0 100.0
Findings on the variable named pregnant women education background
It was found that 32.2% of participants had reached only primary level, 39.1% reached
secondary level, 15.2% reached collage level, 2.9% reached as far as university level and 11.6%
never been to school. The purpose of this variable was to determine whether education had an
influence over pregnant women perception on late ANC booking. This study revealed that
education back ground.
19
TABLE 4.0.4: ECONOMIC STATUS
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid formal employment 35 25.4 25.4 25.4
informal
employment 103 74.6 74.6 100.0
Total 138 100.0 100.0
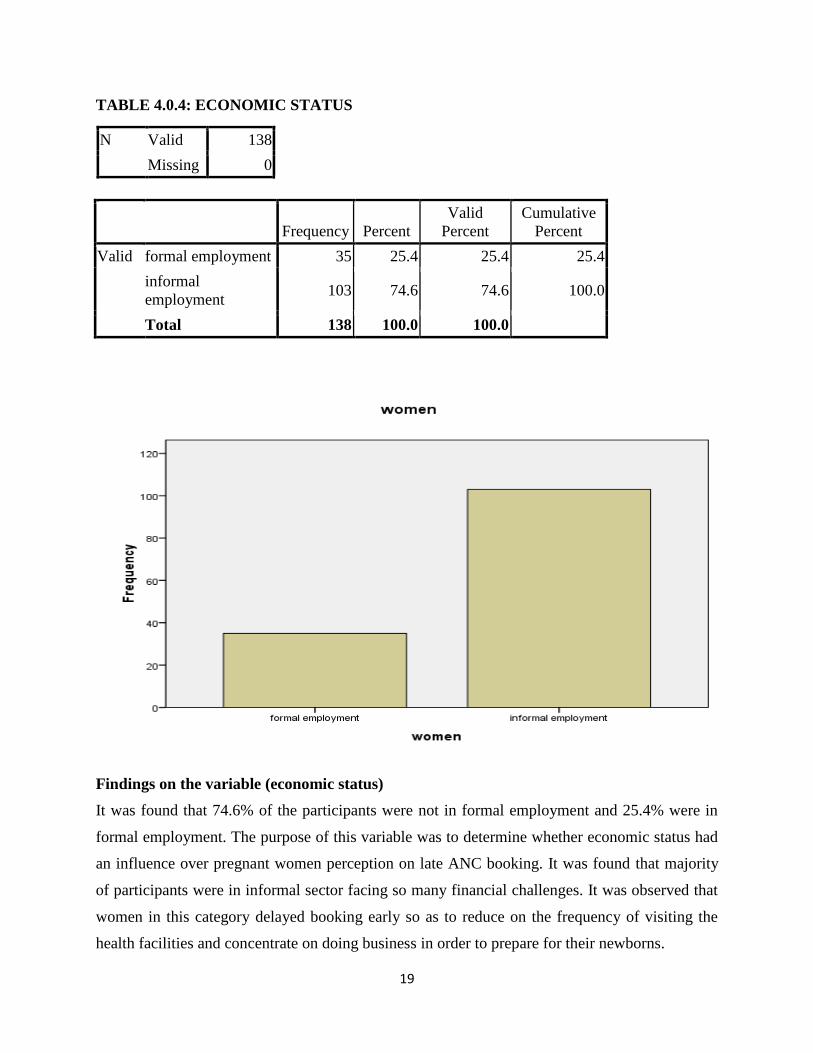
Findings on the variable (economic status)
It was found that 74.6% of the participants were not in formal employment and 25.4% were in
formal employment. The purpose of this variable was to determine whether economic status had
an influence over pregnant women perception on late ANC booking. It was found that majority
of participants were in informal sector facing so many financial challenges. It was observed that
women in this category delayed booking early so as to reduce on the frequency of visiting the
health facilities and concentrate on doing business in order to prepare for their newborns.
20
TABLE 4.0.5. NUMBER OF PREVIOUS PREGNANCIES
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 1 12 8.7 8.7 8.7
2 38 27.5 27.5 36.2
3 26 18.8 18.8 55.1
4+ 62 44.9 44.9 100.0
Total 138 100.0 100.0
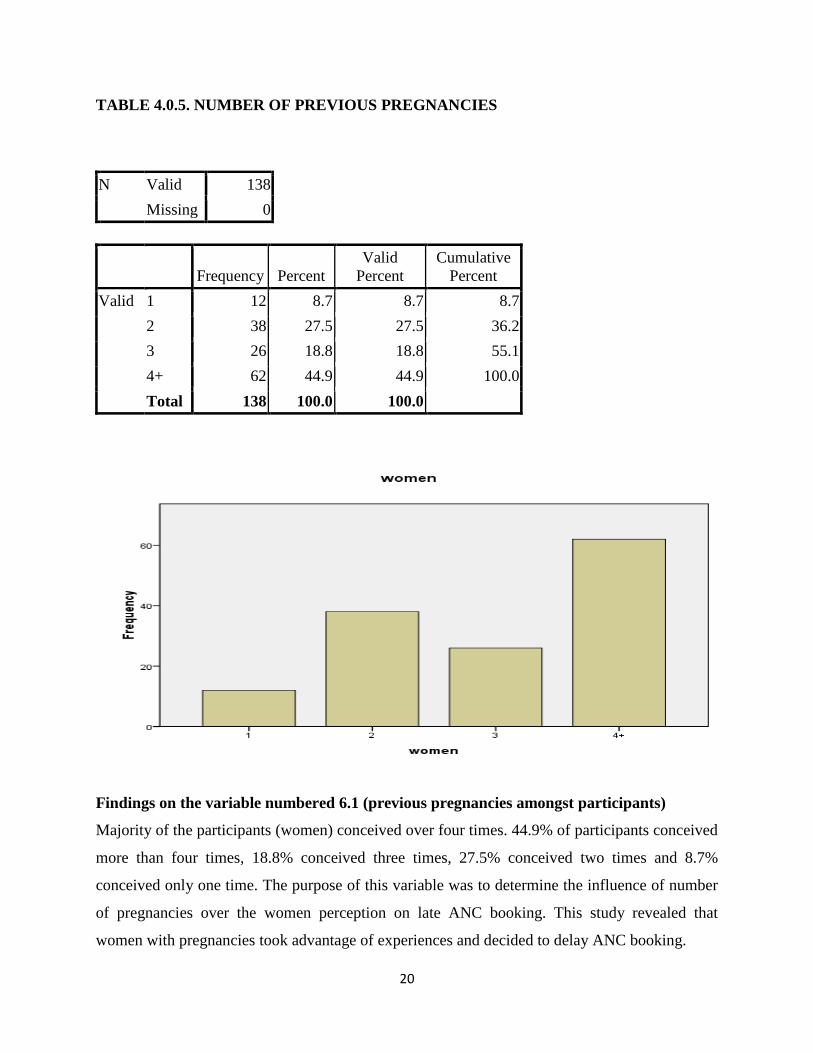
Findings on the variable numbered 6.1 (previous pregnancies amongst participants)
Majority of the participants (women) conceived over four times. 44.9% of participants conceived
more than four times, 18.8% conceived three times, 27.5% conceived two times and 8.7%
conceived only one time. The purpose of this variable was to determine the influence of number
of pregnancies over the women perception on late ANC booking. This study revealed that
women with pregnancies took advantage of experiences and decided to delay ANC booking.
21
TABLE 4.0.6: TERM PREGNANCIES
N Valid 138
Missing 0
Frequency Percent Valid Percent
Cumulative
Percent
Valid 1 (10/13 reported to reached
term 9 6.5 6.5 6.5
2 ((33/37 reported
pregnancies reached term 34 24.6 24.6 31.2
3 (22/26 reported pregnancies
reached term 32 23.2 23.2 54.3
4 (60/62 reported pregnancies
reached term 63 45.7 45.7 100.0
Total 138 100.0 100.0
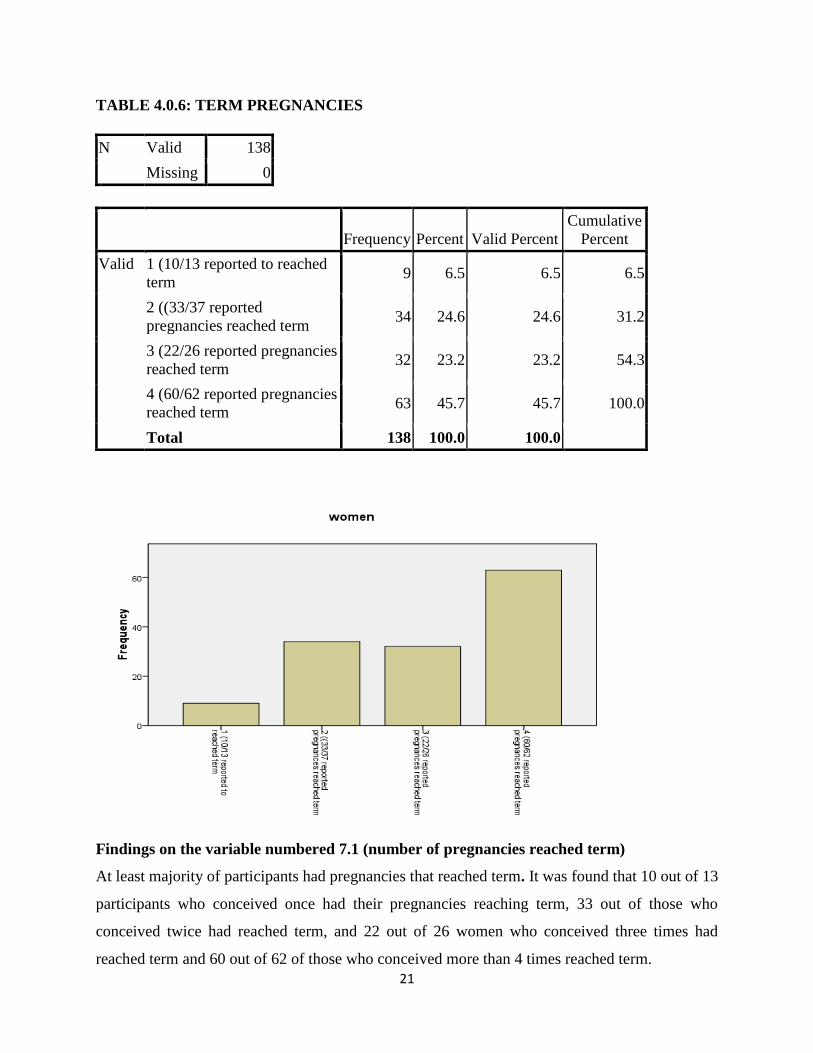
Findings on the variable numbered 7.1 (number of pregnancies reached term)
At least majority of participants had pregnancies that reached term. It was found that 10 out of 13
participants who conceived once had their pregnancies reaching term, 33 out of those who
conceived twice had reached term, and 22 out of 26 women who conceived three times had
reached term and 60 out of 62 of those who conceived more than 4 times reached term.
22
TABLE 4.0.7 NUMBER OF PROTECTED PREGNANCIES
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid YES (protected
pregnancies during
ANC
112 81.2 81.2 81.2
NO Unprotected
pregnancies during
ANC
26 18.8 18.8 100.0
Total 138 100.0 100.0
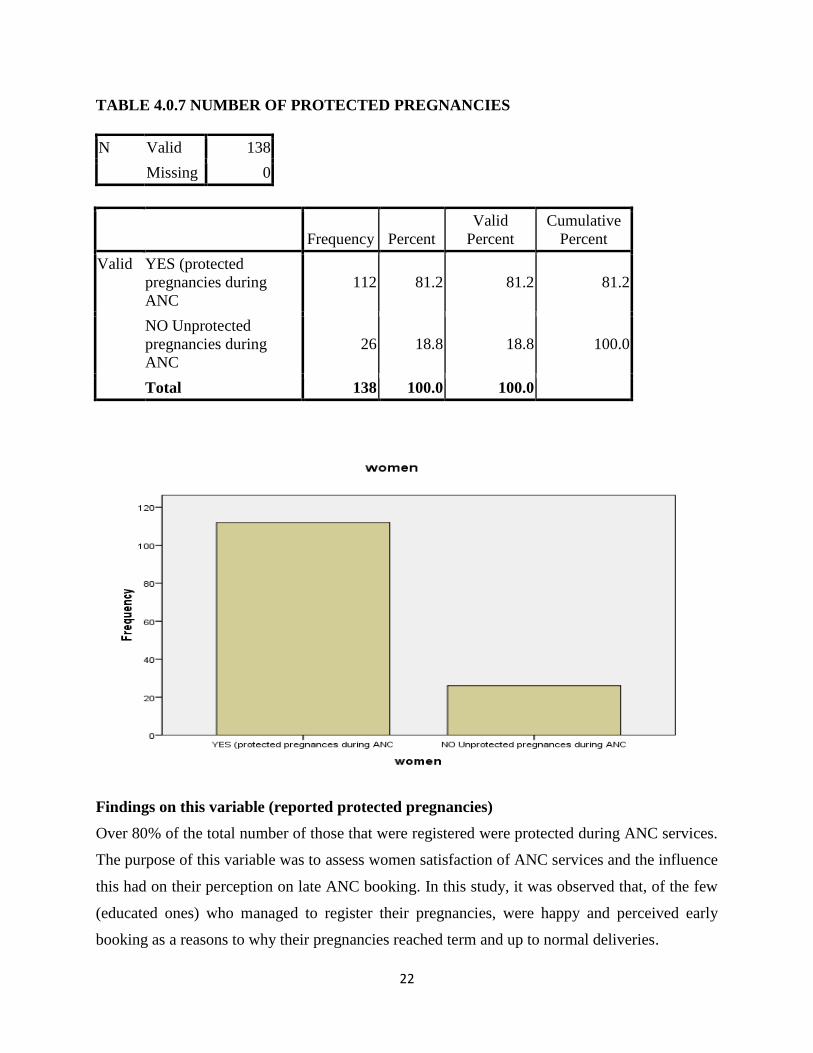
Findings on this variable (reported protected pregnancies)
Over 80% of the total number of those that were registered were protected during ANC services.
The purpose of this variable was to assess women satisfaction of ANC services and the influence
this had on their perception on late ANC booking. In this study, it was observed that, of the few
(educated ones) who managed to register their pregnancies, were happy and perceived early
booking as a reasons to why their pregnancies reached term and up to normal deliveries.
23
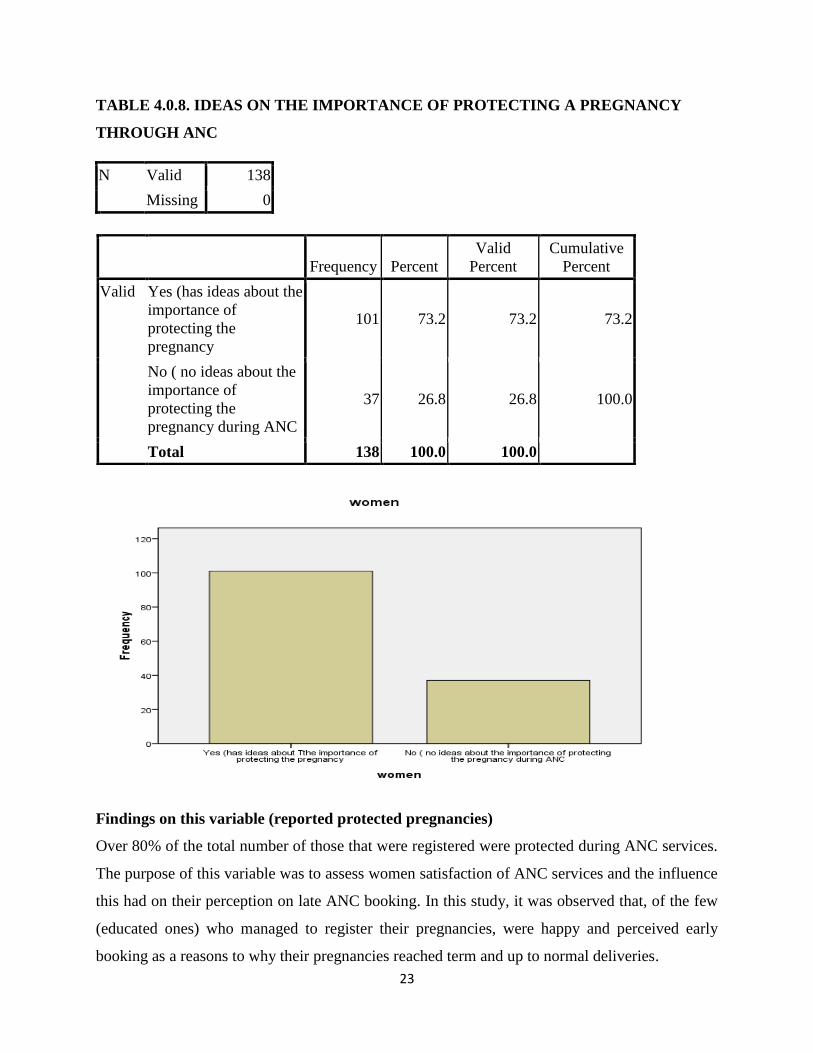
TABLE 4.0.8. IDEAS ON THE IMPORTANCE OF PROTECTING A PREGNANCY
THROUGH ANC
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid Yes (has ideas about the
importance of
protecting the
pregnancy
101 73.2 73.2 73.2
No ( no ideas about the
importance of
protecting the
pregnancy during ANC
37 26.8 26.8 100.0
Total 138 100.0 100.0
Findings on this variable (reported protected pregnancies)
Over 80% of the total number of those that were registered were protected during ANC services.
The purpose of this variable was to assess women satisfaction of ANC services and the influence
this had on their perception on late ANC booking. In this study, it was observed that, of the few
(educated ones) who managed to register their pregnancies, were happy and perceived early
booking as a reasons to why their pregnancies reached term and up to normal deliveries.
24
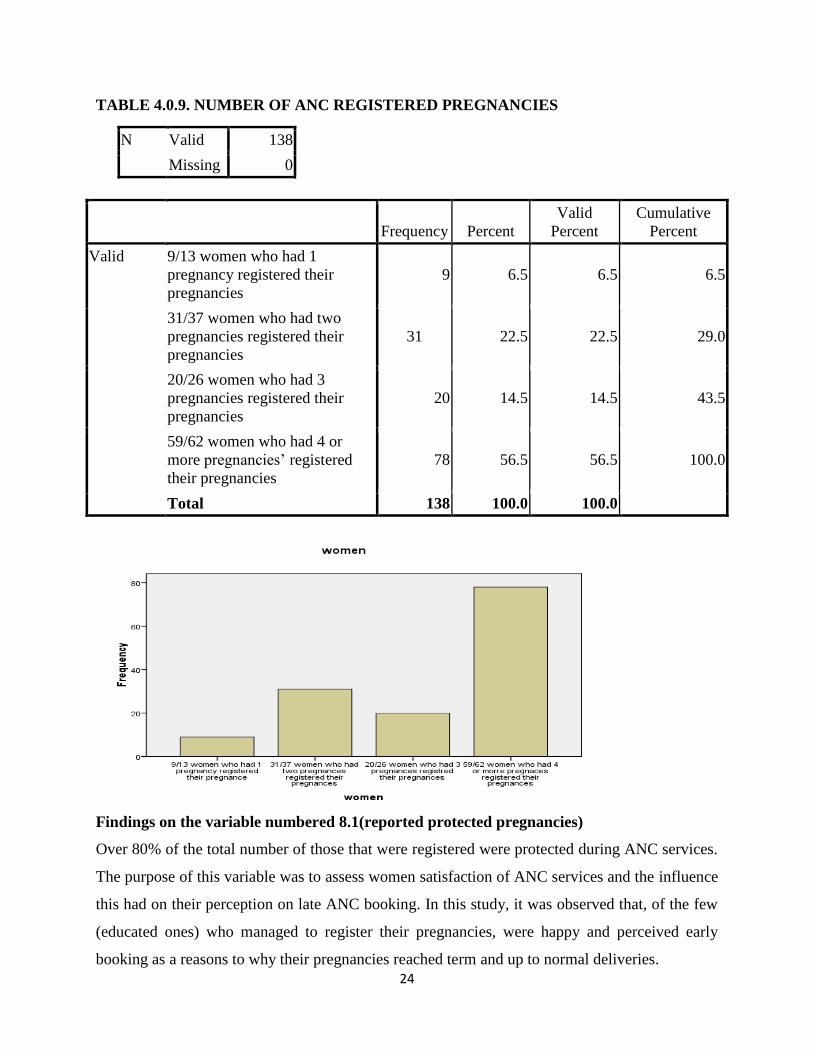
TABLE 4.0.9. NUMBER OF ANC REGISTERED PREGNANCIES
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 9/13 women who had 1
pregnancy registered their
pregnancies
9 6.5 6.5 6.5
31/37 women who had two
pregnancies registered their
pregnancies
31 22.5 22.5 29.0
20/26 women who had 3
pregnancies registered their
pregnancies
20 14.5 14.5 43.5
59/62 women who had 4 or
more pregnancies’ registered
their pregnancies
78 56.5 56.5 100.0
Total 138 100.0 100.0
Findings on the variable numbered 8.1(reported protected pregnancies)
Over 80% of the total number of those that were registered were protected during ANC services.
The purpose of this variable was to assess women satisfaction of ANC services and the influence
this had on their perception on late ANC booking. In this study, it was observed that, of the few
(educated ones) who managed to register their pregnancies, were happy and perceived early
booking as a reasons to why their pregnancies reached term and up to normal deliveries.
25
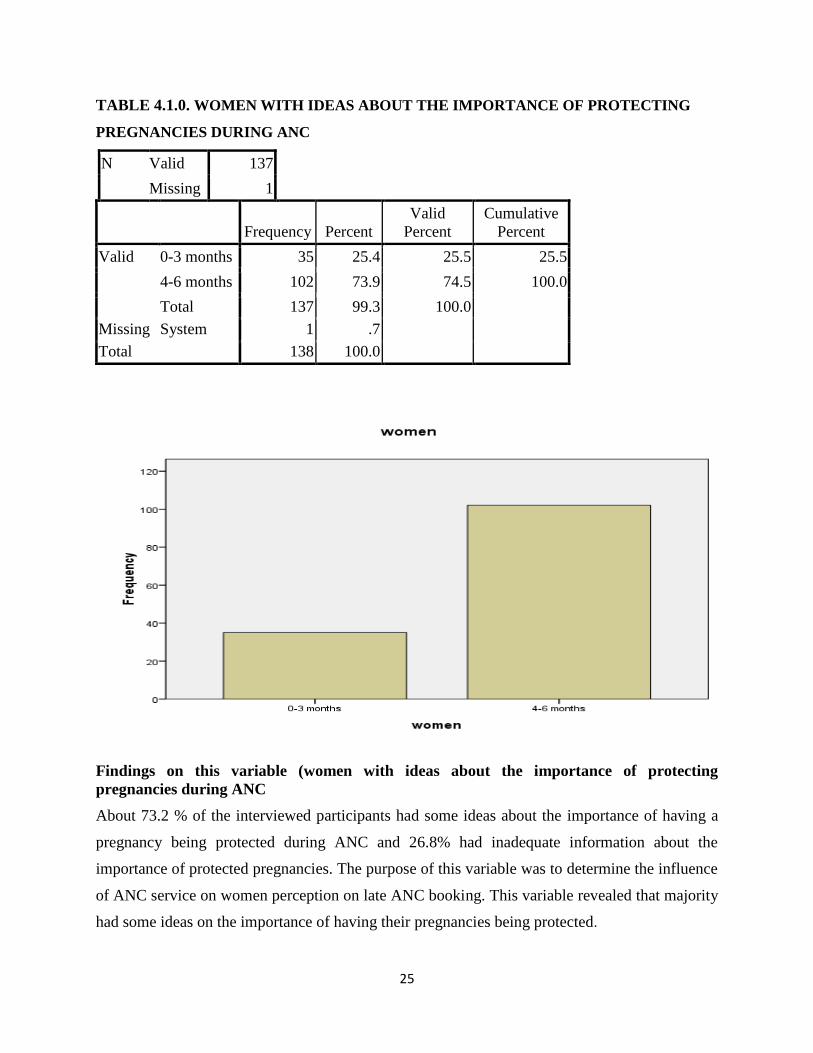
TABLE 4.1.0. WOMEN WITH IDEAS ABOUT THE IMPORTANCE OF PROTECTING
PREGNANCIES DURING ANC
N Valid 137
Missing 1
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 0-3 months 35 25.4 25.5 25.5
4-6 months 102 73.9 74.5 100.0
Total 137 99.3 100.0
Missing System 1 .7
Total 138 100.0
Findings on this variable (women with ideas about the importance of protecting
pregnancies during ANC
About 73.2 % of the interviewed participants had some ideas about the importance of having a
pregnancy being protected during ANC and 26.8% had inadequate information about the
importance of protected pregnancies. The purpose of this variable was to determine the influence
of ANC service on women perception on late ANC booking. This variable revealed that majority
had some ideas on the importance of having their pregnancies being protected.
26
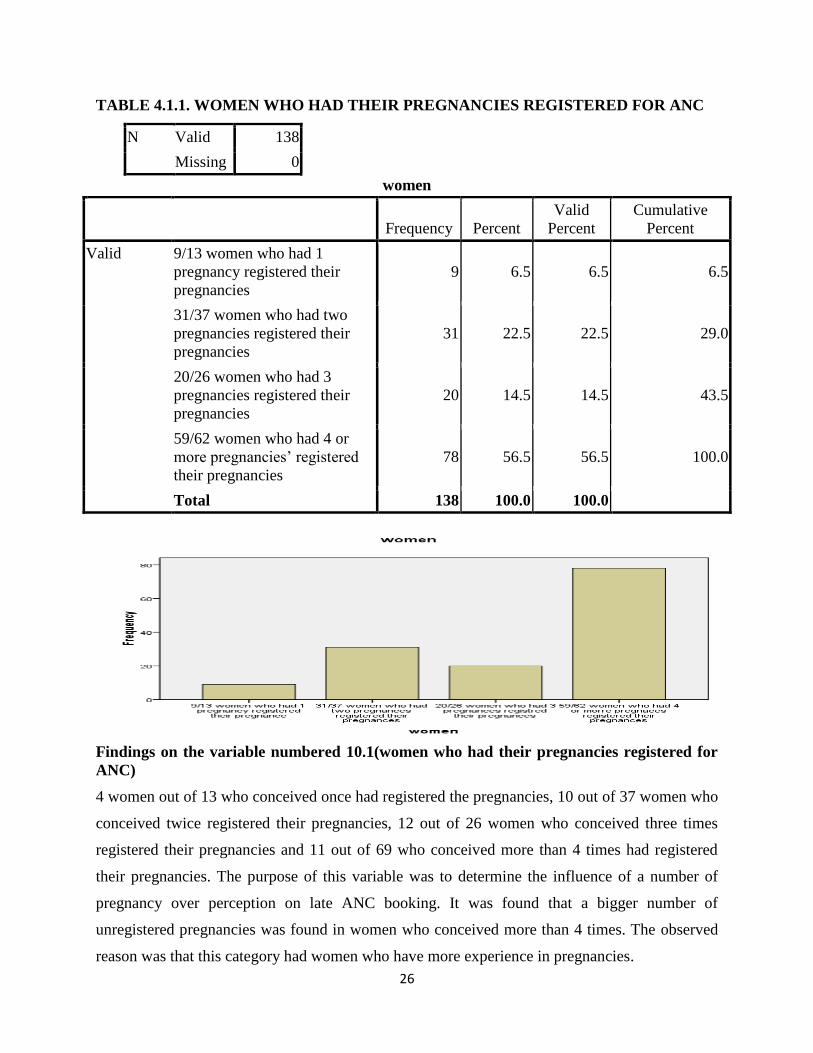
TABLE 4.1.1. WOMEN WHO HAD THEIR PREGNANCIES REGISTERED FOR ANC
N Valid 138
Missing 0
women
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 9/13 women who had 1
pregnancy registered their
pregnancies
9 6.5 6.5 6.5
31/37 women who had two
pregnancies registered their
pregnancies
31 22.5 22.5 29.0
20/26 women who had 3
pregnancies registered their
pregnancies
20 14.5 14.5 43.5
59/62 women who had 4 or
more pregnancies’ registered
their pregnancies
78 56.5 56.5 100.0
Total 138 100.0 100.0
Findings on the variable numbered 10.1(women who had their pregnancies registered for
ANC)
4 women out of 13 who conceived once had registered the pregnancies, 10 out of 37 women who
conceived twice registered their pregnancies, 12 out of 26 women who conceived three times
registered their pregnancies and 11 out of 69 who conceived more than 4 times had registered
their pregnancies. The purpose of this variable was to determine the influence of a number of
pregnancy over perception on late ANC booking. It was found that a bigger number of
unregistered pregnancies was found in women who conceived more than 4 times. The observed
reason was that this category had women who have more experience in pregnancies.
27
TABLE 4.1.2: EARLY BOOKING AMONGST THE SAMPLED PARTICIPANTS
N Valid 137
Missing 1
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 0-3 months 35 25.4 25.5 25.5
4-6 months 102 73.9 74.5 100.0
Total 137 99.3 100.0
Missing System 1 .7
Total 138 100.0
Findings in this variable (early booking amongst the sampled participants)
Findings revealed that 25.4% booked early for ANC and 73.9% booked late for ANC. The
purpose of this variable was to determine the general attitude of pregnant women over early
ANC booking which will further highlight on the general perception on late ANC booking. In
this study it was found that most women who booked, did so between 4th and 6th weeks
gestation.
28
TABLE 4.1.3. REASONS WHY SOME WOMEN REGISTER LATE FOR ANC
N Valid 137
Missing 1
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid 0-3 months 35 25.4 25.5 25.5
4-6 months 102 73.9 74.5 100.0
Total 137 99.3 100.0
Missing System 1 .7
Total 138 100.0
Findings on this variable (reasons why some women register late for ANC)
Among many reasons recorded, 40.6% of participants revealed economic challenges to be the
major factor that leads pregnant women to register late for ANC, 26.1 were personal related
reasons, 7.2% being traditional reasons and 26.1% to be other related reasons. The purpose of
this variable was to identify various reasons which influences women perception on late ANC
booking. It was found that economic factors were the major challenge that influences women
perception on late ANC booking. Majority decided to book late because they wanted to look for
finances to prepare for the new born baby.
29
TABLE 4.15: PREGNANT WOMEN PERCEPTION ON EARLY ANC BOOKING
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid positive 79 57.2 57.2 57.2
negative 59 42.8 42.8 100.0
Total 138 100.0 100.0
Findings on this variable (pregnant women perception on early ANC booking)
84.1% of participants showed wrong perception on early ANC booking due to various reasons
and only 15.9 to have a good perception. The purpose of this variable was to determine how
women perceive early ANC compared to late ANC booking. It was found that majority of
women perceived early ANC being a challenge because it forced them to book at the time they
were not ready to. This reason was recorded mainly to those who conceived unknowingly and
those who were cohabiting.
30
TABLE 4.1.6: PREGNANT WOMEN KNOWLEDGE ON THE IMPORTANCE OF ANC
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid high 25 18.1 18.1 18.1
average 22 15.9 15.9 34.1
low 91 65.9 65.9 100.0
Total 138 100.0 100.0
Findings on this variable (pregnant women knowledge on the importance of ANC)
Findings showed that majority 65.9% of the participants had inadequate information on the
importance of early ANC booking, 15.9% had some information and 18.1 had more information
on the importance of ANC. The purpose of this variable was to determine the influence of
knowledge level over women perception on late ANC booking. In this study it was found that
majority had inadequate information on the importance of ANC services.
31
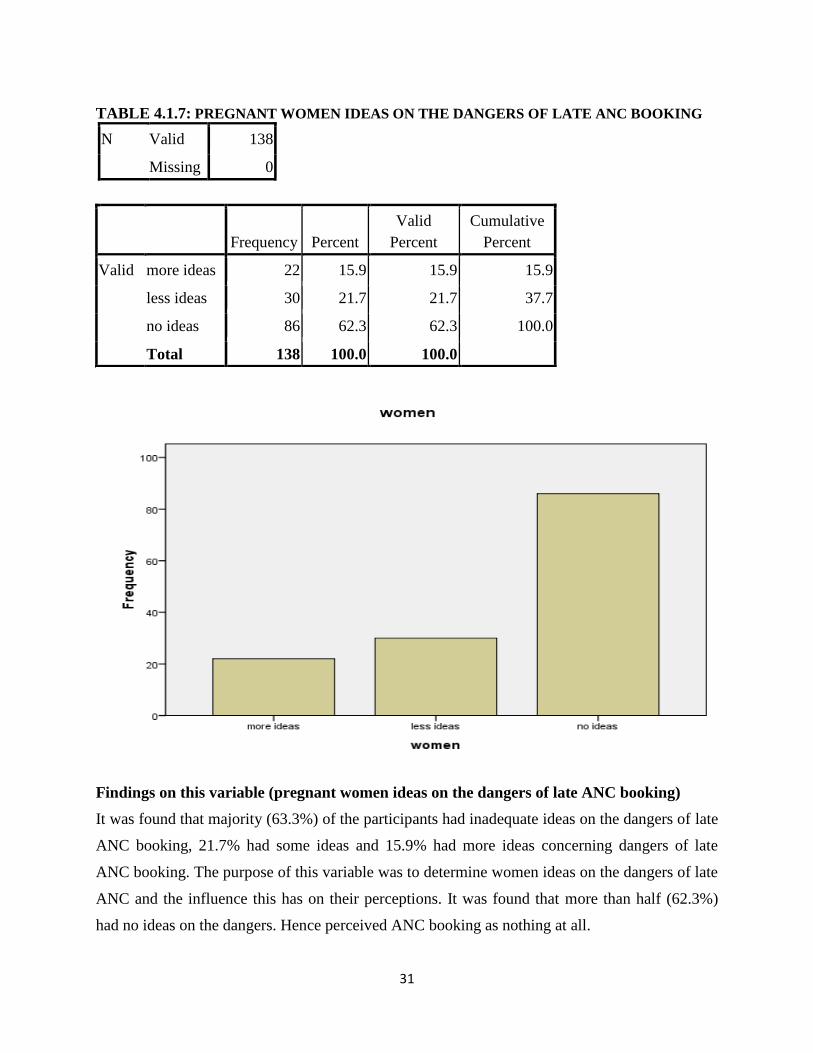
TABLE 4.1.7: PREGNANT WOMEN IDEAS ON THE DANGERS OF LATE ANC BOOKING
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid more ideas 22 15.9 15.9 15.9
less ideas 30 21.7 21.7 37.7
no ideas 86 62.3 62.3 100.0
Total 138 100.0 100.0
Findings on this variable (pregnant women ideas on the dangers of late ANC booking)
It was found that majority (63.3%) of the participants had inadequate ideas on the dangers of late
ANC booking, 21.7% had some ideas and 15.9% had more ideas concerning dangers of late
ANC booking. The purpose of this variable was to determine women ideas on the dangers of late
ANC and the influence this has on their perceptions. It was found that more than half (62.3%)
had no ideas on the dangers. Hence perceived ANC booking as nothing at all.
32
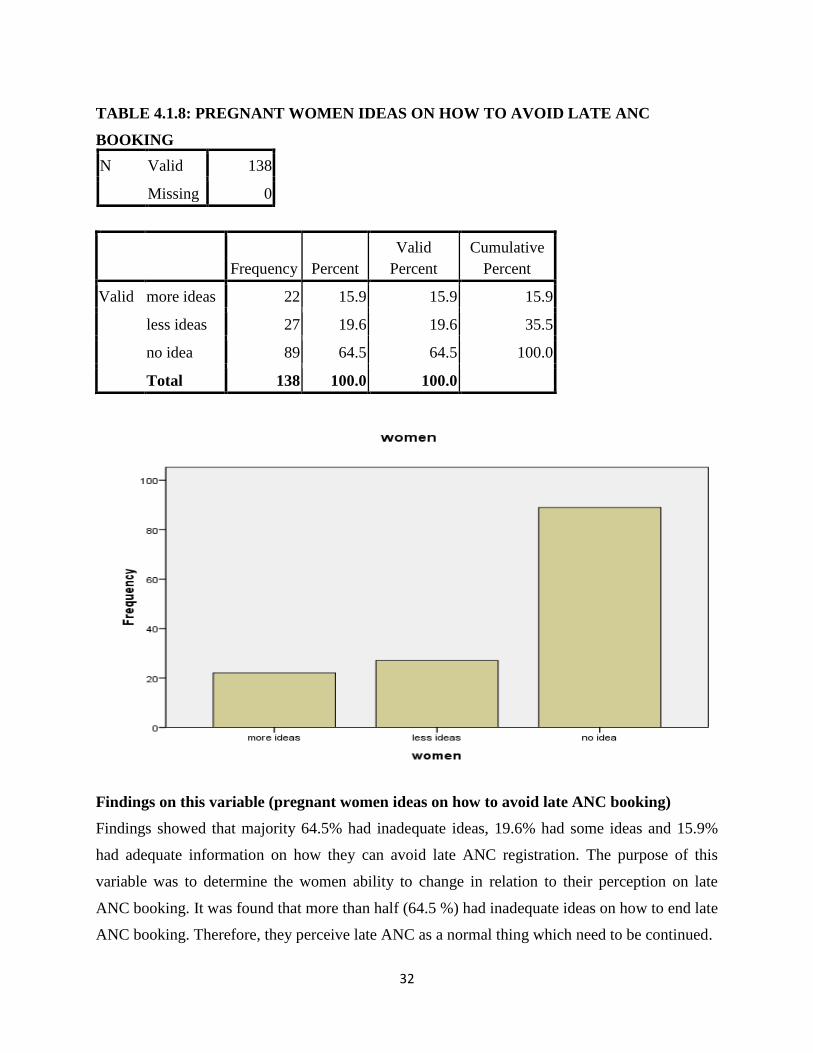
TABLE 4.1.8: PREGNANT WOMEN IDEAS ON HOW TO AVOID LATE ANC
BOOKING
N Valid 138
Missing 0
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid more ideas 22 15.9 15.9 15.9
less ideas 27 19.6 19.6 35.5
no idea 89 64.5 64.5 100.0
Total 138 100.0 100.0
Findings on this variable (pregnant women ideas on how to avoid late ANC booking)
Findings showed that majority 64.5% had inadequate ideas, 19.6% had some ideas and 15.9%
had adequate information on how they can avoid late ANC registration. The purpose of this
variable was to determine the women ability to change in relation to their perception on late
ANC booking. It was found that more than half (64.5 %) had inadequate ideas on how to end late
ANC booking. Therefore, they perceive late ANC as a normal thing which need to be continued.
33
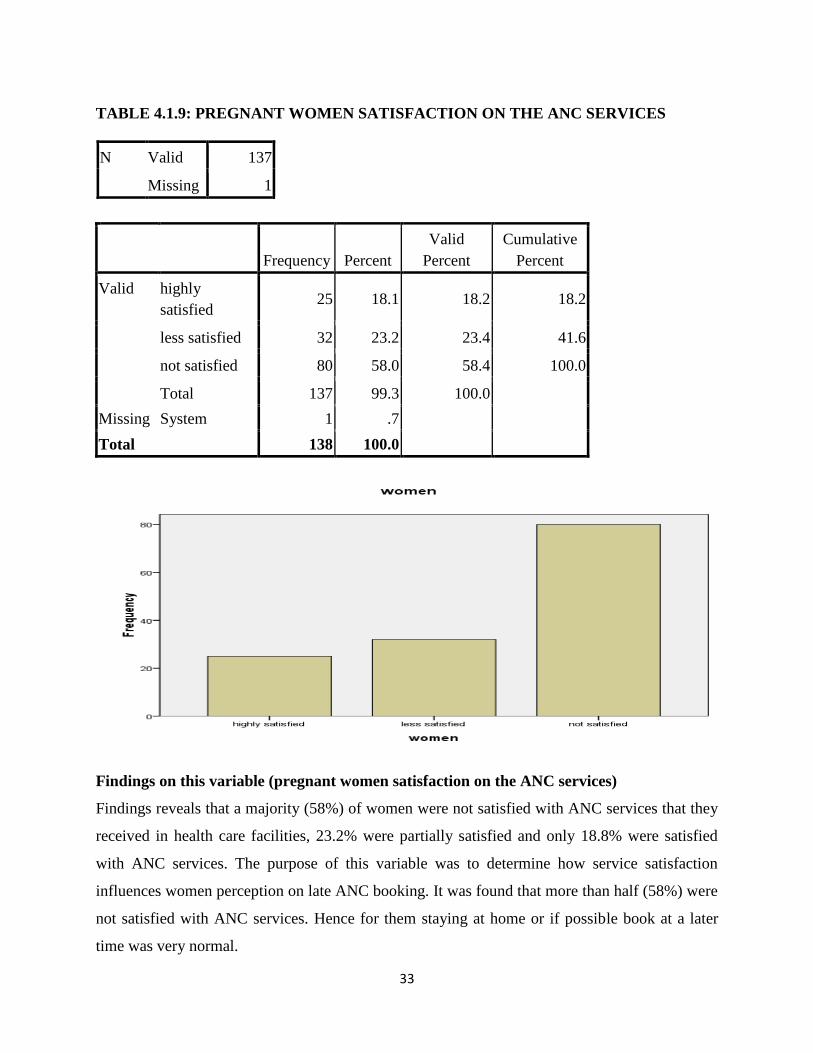
TABLE 4.1.9: PREGNANT WOMEN SATISFACTION ON THE ANC SERVICES
N Valid 137
Missing 1
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid highly
satisfied 25 18.1 18.2 18.2
less satisfied 32 23.2 23.4 41.6
not satisfied 80 58.0 58.4 100.0
Total 137 99.3 100.0
Missing System 1 .7
Total 138 100.0
Findings on this variable (pregnant women satisfaction on the ANC services)
Findings reveals that a majority (58%) of women were not satisfied with ANC services that they
received in health care facilities, 23.2% were partially satisfied and only 18.8% were satisfied
with ANC services. The purpose of this variable was to determine how service satisfaction
influences women perception on late ANC booking. It was found that more than half (58%) were
not satisfied with ANC services. Hence for them staying at home or if possible book at a later
time was very normal.
34
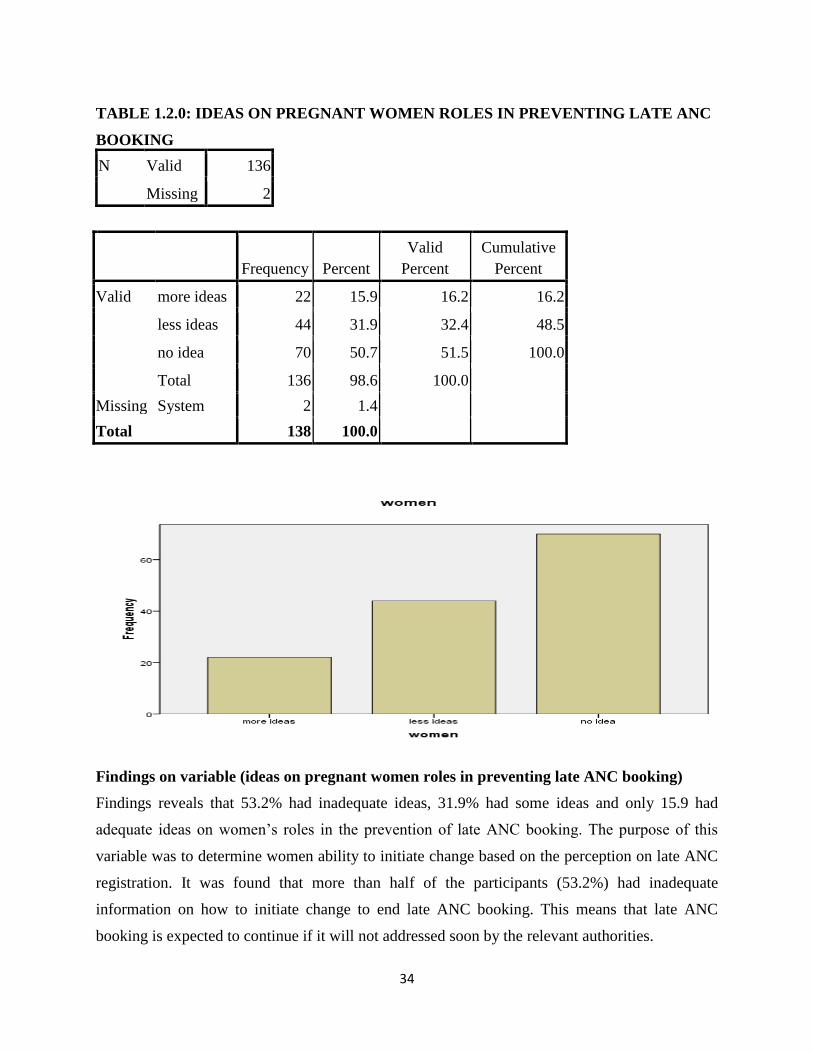
TABLE 1.2.0: IDEAS ON PREGNANT WOMEN ROLES IN PREVENTING LATE ANC
BOOKING
N Valid 136
Missing 2
Frequency Percent
Valid
Percent
Cumulative
Percent
Valid more ideas 22 15.9 16.2 16.2
less ideas 44 31.9 32.4 48.5
no idea 70 50.7 51.5 100.0
Total 136 98.6 100.0
Missing System 2 1.4
Total 138 100.0
Findings on variable (ideas on pregnant women roles in preventing late ANC booking)
Findings reveals that 53.2% had inadequate ideas, 31.9% had some ideas and only 15.9 had
adequate ideas on women’s roles in the prevention of late ANC booking. The purpose of this
variable was to determine women ability to initiate change based on the perception on late ANC
registration. It was found that more than half of the participants (53.2%) had inadequate
information on how to initiate change to end late ANC booking. This means that late ANC
booking is expected to continue if it will not addressed soon by the relevant authorities.
35
CHAPTER 5
5.0. DISCUSSION
A high proportion of women who perceived late ANC booking not being a problem was found in
the category of women with lower education background, those who have never been to school,
those with no idea of the importance of early ANC booking, those with inadequate financial
resources and those who are unsatisfied with ANC services in health facilities. Similar results in
a study in London done using routinely collected data showed that women who are not well
sensitized were more likely to book for ANC late, similar to the findings reported here (Baker
and Rajah, 2012, Emelieh et al., 2014). The reasons for this is unclear but it is reasonable to
think that women who may not see a good reason of early registration for ANC services may not
know or understand the importance of booking early for ANC meaning they will have wrong
perceptions on early ANC. Women with inadequate financial resources on the other hand may be
more likely to book late for ANC. This is because they may take the period when they become
pregnant as the time for them to start moving up and down to look for the resources for
preparation (Emelieh et al., 2014). In addition, unmarried, women aged 16 to 19 years may feel
ashamed to disclose their pregnancies or be uncomfortable going for ANC without their partners
and thus perceives delay in booking for ANC as a favor. Some of this might be related to
availability and affinity of health promotion messages regarding child and maternal survival. In
the present it was thus not surprising to find that women exposed to the media tended to book
early suggesting that they may have heard health promotional messages that modified
perceptions positively their understanding on the role of early ANCs in both child and maternal
survival (Nyambe et al 2006).
It looks reasonable that, the unmarried may perceive late ANC booking as a favor or not perceive
early ANC booking with much attention as shown in this study. Various barriers to early ANC
booking may surround unplanned pregnancies more especially for women who are just
cohabiting or who are not yet made up their mind whether to be with their partners or not.
Results similar to the findings in this study were seen in a study done in the Copperbelt province
of Zambia which showed that women with unplanned pregnancy were 4.4 times more likely to
perceive late ANC booking as a usual thing compared to those with planned pregnancies (Banda
et al., 2012). A survey done in Tanzania similarly showed that women with unplanned
36
pregnancies were two times more likely to book for ANC late compared to women with planned
pregnancies (Exavery et al., 2013). The question, which arises, is whether the women will
develop a good perception on early ANC booking. If they will, when and what role do they need
to play in order for them to initiate the change. Do the health promotion messages cater for many
with wrong perceptions on late ANC booking? These and more questions are among topics
which need to be looked at in the future studies. While it sounds logical that women with
inadequate information about the importance of early ANC booking, the results from this study
did not support this reasoning. What this may be telling us is that women may be aware of the
consequences that comes with late ANC booking but my fail to do away with it due to various
reasons. If women with inadequate information about the benefits of early ANC booking, would
most likely be ashamed to book for ANC early, as they would fear being questioned why they
never register early.
In this study, evidence was provided that women with low education background had a wrong
perception on late ANC booking and are more likely to book for ANC late than women with
high education back ground. This is supported by studies done in Nigeria, New Zealand Uganda
and a systematic review of literature from African countries which similarly showed that women
with higher education are more likely to book for ANC early because of a good perception that
they have toward early ANC service (Simkhada et al., 2008, Ebeigbe and Igberase, 2010,
Oladokun et al., 2010, Corbett et al., 2014). This may be attributed to differences in perceiving
late booking for ANC as well as the levels of understanding on the importance of early ANC
booking among the different levels of education of women (Baker and Rajasingam, 2012,
Emelumadu et al., 2014). This suggests that women with higher education are more likely to read
newspapers and watch television more frequently than less educated or not educated women.
37
CHAPTER 6
6.0 CONCLUSION AND RECOMMENDATION
In this study, it was found that majority of women are still perceiving late ANC booking as a
usual practice which provide favor to many (wrong perception). This is still a problem in the
district suggesting that a large proportion of pregnant women perceive late ANC booking not
being a problem there by missing an opportunity to have early detection and preventing any
possible complications of pregnancy and the unborn fetus. These observations further shows that
this challenge is concentrated in women with little or no education or those with inadequate
information about the importance of early ANC booking and those women who are not in
marriage. The concentration of this problem in lower or no education groups may be an
illustration of existing inequalities which might further explain past and present limitations in
health promotion messages meant to mitigate this challenge. This could also have strategic
hindrances in planned interventions aimed at enhancing both maternal and child survival. There
is thus urgent need to re-pack health promotion message to specifically target these population
sub-groups.
6.1 RECOMMENDATIONS
From the findings in this study, it’s recommended that women should be educated beyond
primary and secondary level, women should be empowered with some life skills to enable them
being self-reliant and not depending on others for financial help. Have access to family planning
methods and should be able to use them. To support this, the health promotion packages that
encourage pregnant women to develop a good perception on early ANC booking must be
repackaged to suit women’s differential background characteristics that account for their
differences in education status, age and parity as observed in this study. This is critical as these
factors may have been missed in past maternal survival strategies in this population. If we look at
this as a right for the women, an obligation for policy makers and a responsibility for primary
care workers, we may save many lives, and consequently save millions of dollars currently
incurred in current maternal health strategies. There is need to conduct a similar study using a
deferent sources of data and places in order to compare and analyze trends in women perception
on late ANC booking at inter-provincial level.

38
6.3 LIMITATIONS
One limitation in this study include the small sample size which has been taken to represent the
district. However, this study was not linked to evaluations of associated maternal survival
strategies, it is difficult to estimate the effect of this limitation. Other limitations were that some
variables of interest like education of the partner and age of the partner had significantly missing
data and could not be included in the analysis and certain questions could only be answered
using other qualitative method approach and were thus not included in this analysis. This study
only asked women with previous live births in the five years preceding the survey questions
about perceptions on late ANC and this may be a source of bias because those women without
live births may be the ones with wrong perceptions in booking early for ANC. Despite these
limitations, the observed results were from a representative high-powered population based
sample of women in the district and hence point to a significant problems associated with
women’s perceptions on late ANC booking which are difficult to ignore.
39
REFERENCES
Bbaale, E. 2017. Factors influencing timing and frequency of antenatal care in Uganda. AMJ 4,
8, 431-438. Available at: http//dx.doi.org/10.4066/AMJ.2017.729
Central Statistical Office (CSO), Ministry of Health (MOH), Tropical Diseases research Centre
(TDRC), University of Zambia and Macro International Inc., 2016. Zambia Demographic and
Health Survey 2014. Calverton, Maryland: CSO and Macro International
Central Statistical Office (CSO) [Zambia], Ministry of Health (MOH) [Zambia] and ICF
International, 2014. Zambia Demographic and Health Survey 2012-2014. Rockville, Maryland,
USA: Central Statistics Office, Ministry of Health, and ICF International
Corbett, S., Chelimo, C. & Okesene-gafa, K. 2014. Barriers to early initiation of antenatal care
in a multi-ethnic sample in South Auckland, New Zealand. N Z Med J, 127, 53-61.
Cresswell, J. A., YU, G., Hatherall, B., Morris, J., Jamal, F., Harden, A. & Renton, A. 2013.
Predictors of the timing of initiation of antenatal care in an ethnically diverse urban cohort in
the UK. BMC Pregnancy Childbirth, 13, 103.
Ebeigbe, P. N. & Igberase, G. O. 2010. Reasons given by pregnant women for late initiation of
antenatal care in the Niger delta, Nigeria. Ghana Med J, 44, 47-51.
Exavery, A., Kante, A. M., Hingora, A., Mbaruku, G., Pemba, S. & Phillips, J. F. 2013. How
mistimed and unwanted pregnancies affect timing of antenatal care initiation in three districts in
Tanzania. BMC Pregnancy Childbirth, 13, 35.
Makasa, M., Fylkesnes, K., Michelo, C., Kayeyi, N., Chirwa, B. & Sandoy, I. 2012.
Declining syphilis trends in concurrence with HIV declines among pregnant women in Zambia:
observations over 14 years of national surveillance. Sex Transm Dis, 39, 173-81.
Ministry of Health, 2015. Health for the Poorest Population Project (unpublished)
Ministry of Health, 2015. HMIS Instructions and Procedures Reference Materials, Zambia
Ministry of Health, 2014. HMIS Instructions and Procedures Reference Materials, Zambia
Ministry of Health (MOH), 2014. Zambia Antenatal Clinic Sentinel Surveillance Report 2017-
2018
40
Neumann, W.L., (2014). Social Research Methods: Qualitative and Quantitative Approaches
(3rd edition). London: Allyn & Bacon.
Newhouse, J., (2015). Free for All Lessons from the RAND Health Insurance Experiment.
Harvard University Press. ISBN 0-674-31846-3.
Nichols, F.H & Zwelling, E., (2016). Maternal-Newborn Nursing: Theory and Practice. W.B.
Saunders. London.
Nielsen, B.B., Lijestrand, J., Thilsted, S., H. Joseph and Hedegard, M. (2015) Characteristics of
antenatal care attendees in a rural population in Tamil, N South India: A community-based
cross-sectional study. Perinatal Epidemiological Research Unit, Department of Gynecology and
Obstetrics, University Hospital of Aarhus, N, Denmark.
NOFAS-UK (National Organization on fetal Alcohol Syndrome UK), 2015. Online Available:
http//www.nofas-uk.org/index.asp.
Nohr, E.A., Vaeth, M, Bech, B.H, Henriksen, T.B., Cnattingius, S., Olsen, J. (2017). Maternal
obesity and neonatal mortality according to subtypes of preterm birth. Obstetric Gynecology.
2017 November; 110(5):1083-90.
O’Callaghan, M. F., Bororkowski J. G, Whitman TL, Maxwell S. E & Keogh D., (2017). A
Model of Adolescent Parenting: The Role of Cognitive Readiness to Parent. Journal of Research
on Adolescence, 9(2): 203–225
Oiler, C.J. (2018). ‘The Phenomenological Approach in Nursing Research’, Nursing Research,
31 (3): 178-181.
Okuku, D., (2016). Access to and utilization of antenatal care services in Uganda. Affiliation:
Regional Institute of Population studies, University of Ghana. Legon, Ghana.
Owolabi. A.T., Fatusi, A.O., Kuti, O., Adeyemi, A., Faturoti, S.O., Obiajuwa, P.O., (2018).
Maternal complications and perinatal outcomes in booked and unbooked Nigerian mothers.
Singapore Medical Journal J 49(7): 526-531.
Parmar, V.R., Grover, N., Kaushik, R. Neonatal mortality rate: relationship to birth weight and
gestational age. Indian J Pediatr. (2018) May-June; 65 (3):429-33.
41
Patton, M. (1990). Qualitative evaluation and research methods. (pp. 169-186). Beverly Hills,
CA: Sage.
Perloff J. D and Jaffee K D: Late entry in prenatal care: The neighborhood context. Social work.
1999, 44; 116.
Myer, I. & Harrison, A. 2003. Why do women seek antenatal care late? Perspectives from rural
South Africa. Journal of Midwifery & Women's Health, 48, 268-272.
National Institute for Health and Clinical Excellence (NICE). Antenatal care. 2008. Available at
http://www.nice.org.uk/guidance/CG62 (accesses on 25th November 2016)
Nwosu, B. O., Ugboaja, J. O., Obi-Nwosu, A. L., Nnebue, C. C. & Ifeadike, C. O. 2017.
Proximate determinants of antenatal care utilization among women in southeastern Nigeria.
Niger J Med, 21, 196-204.
Geta, M.B. and Yallew, W. W., Early Initiation of Antenatal Care and Factors Associated with
Early Antenatal Care Initiation at Health Facilities in Southern Ethiopia. Hindawi Advances in
Public Health, 2017.
Kisuule I, Kaye DK, Najjuka F, Ssematimba SK, Arinda A, Nakitende G, et al., Timing and
reasons for coming late for the first antenatal care visit by pregnant women at Mulago hospital,
Kampala Uganda. BMC Pregnancy and Childbirth 2013. 13(121).
Lilungulu A.G., Matovelo D., and Gesase A, Reported Knowledge, Attitude and Practice of
Antenatal Care Services among Women in Dodoma Municipal, Tanzania. Journal of Pediatrics
and Neonatal Care, 2016. 4(1).
Adekanle DA and Isawumi AI, Late Antenatal Care Booking and Its Predictors among Pregnant
Women in South Western Nigeria. Online journal of health and allied sciences March 2018. 7(1).
Tesfaye G, Loxton D, Chojenta C, Semahegn A, Smith R., Delayed initiation of antenatal care
and associated factors in Ethiopia: a systematic review and meta-analysis. Reproductive Health,
2017. 14(150).
Elvis E. Tarkang, Francis B. Zotor. Application of the Health Belief Model (HBM) in HIV
Prevention: A Literature Review. Central African Journal of Public Health. Vol. 1, No. 1, 2015,
pp. 1-8. doi: 10.11648/j.cajph.20150101.11. [email protected] (E. E. Tarkang)
42
World Health Organization (WHO). 2014. WHO Policy Brief for the Implementation of
Intermittent Preventive Treatment of Malaria in Pregnancy Using Sulfadoxine-Pyrimethamine
(IPTp-SP).Geneva,Switzerland:WHO(January).
http://www.who.int/malaria/publications/atoz/iptp-sp-updated-policy-brief-24jan2014.pdf?ua=1
Okunlola MA, Owonikoko KM, Fawole AO et al .Gestational age at antenatal booking and
delivery outcome. Afr J Med Sci 2018; 37(2):165 -169.
Adekanle D A, Isawumi A I. Late antenatal care booking and its predictors among pregnant
women in South Western Nigeria. Online Journal of Health and Allied Sciences 2018; 7(1):4-7
Ebeigbe P N, Igberase GO. Antenatal Care: A comparison of demographic and Obstetric
Characteristics of early and late attendees in the Niger delta, Nigeria. Med Sci Monit 2015;
11(11): 52932.
Kiwuwa MS and Mufubenga P. Use of antenatal care, maternity services, intermittent
presumptive treatment and insecticide treated nets by pregnant women in Luwero district,
Uganda. Malar J 2018; 7:44.
Mrisho M, Obrist B, Schulenburg A J et al. The use of antenatal and postnatal care: perspectives
and experiences of women and health care providers in rural southern Tanzania. BMC Pregnancy
Childbirth 2017; 9:10.
Kupek E, Petrous S, Vause S, Maresh M Clinical, Provider and Socio demographic predictors of
late initiation of ANC in England and Wales. Br J Obst Gynae 2017; 109(3):265-273.
Rowe RE, Magee H, Quigley M A et al. Social and ethnic differences in attendance for
antenatal care in England. Public Health 2018; 122(12):1363 -1372.
Adeyemi AB, Makinde ON, Ajenifuja K O et al. Determinants of antenatal booking time in
Southwestern Nigeria setting. West Afr J Med.2017; 26(4):293-297
Olusanya O, Okpere E, Ezimokhai M. The importance of social class in voluntary fertility
control in a developing country. West Afr J Med 1985; 4:4.
Gharoro EP, Igbafe AA. Antenatal care: some characteristics of the booking visit in a major
Teaching hospital in the developing world. Med Sci Monit 2016; 6(3):519-522.
43
Chisholm D K. Factors associated with late booking for antenatal care in Central Manchester.
Public Health 2016; 103(6):459-466.
Office for National Statistics, United Kingdom. The National statistics socioeconomic
classification (NS-SEC).2018
Say, L., Chou, D., Gemmill, A., Tuncalp, Ö, Moller, A.B., Daniels, J., Gülmezoglu, A.M.,
Temmerman, M. & Alkema, L. (2014) Global Causes of Maternal death: A WHO Systematic
Analysis. Lancet Global Health 2: e323-e333.
Tariku, A., Melkamu, Y. & Kebede Z. (2015) previous utilization of service does not improve
timely booking in antenatal care: Cross sectional study on timing of antenatal care booking at
public health facilities in Addis Ababa. Ethiopian Journal Health Development 24: 226-233.
TDH-MIS (2016) Tanzania Demographic and Health Survey and Malaria Indicator Survey.
Ministry of Health, Community Development, Gender, Elderly and Children (Tanzania
Mainland), Ministry of Health (Zanzibar), National Bureau of Statistics, Office of the Chief
Government Statistician, and ICF. Dar es Salaam, Tanzania and Rockville, Maryland, USA.
TDHS (2011) Tanzania Demographic and Health Survey 2013-15. National Bureau of Statistics
and ICF Macro. Calverton, Maryland, USA.
Uji, A.B., Efiok, E.E., Etenikang, A.S., Obinna, N.C., Chinedum, N.E. & Egor, O.S. (2017)
Obstetric characteristics of women attending antenatal clinic in a tertiary hospital in Nigeria.
Sky Journal of Medicine and Medical Sciences 5(2): 15-19.
WHO (2016) Provision of Focused Antenatal Care for Pregnant Women. World Health
Organization, Geneva.
Glaser BG, Strauss AL. The discovery of grounded theory: Strategies for qualitative research
New York: Aldine de Gruyter, 1994.
44
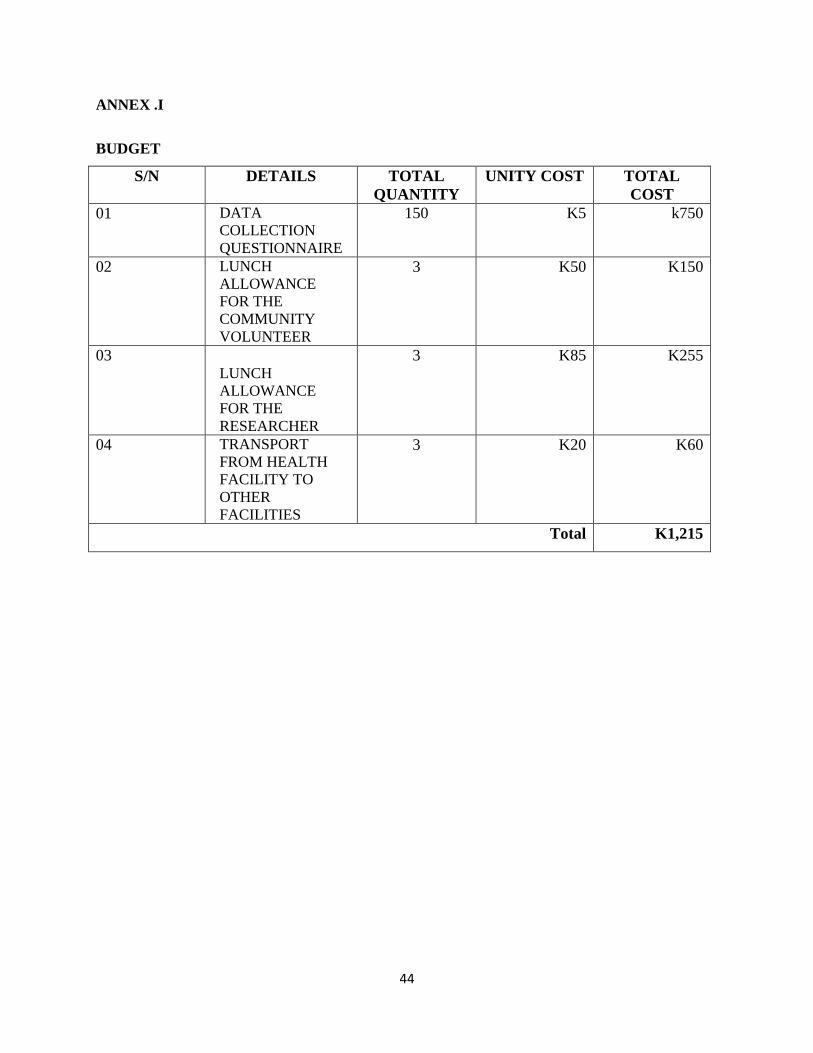
ANNEX .I
BUDGET
S/N DETAILS TOTAL
QUANTITY
UNITY COST TOTAL
COST
01 DATA
COLLECTION
QUESTIONNAIRE
150 K5 k750
02 LUNCH
ALLOWANCE
FOR THE
COMMUNITY
VOLUNTEER
3 K50 K150
03 LUNCH
ALLOWANCE
FOR THE
RESEARCHER
3 K85 K255
04 TRANSPORT
FROM HEALTH
FACILITY TO
OTHER
FACILITIES
3 K20 K60
Total K1,215
45
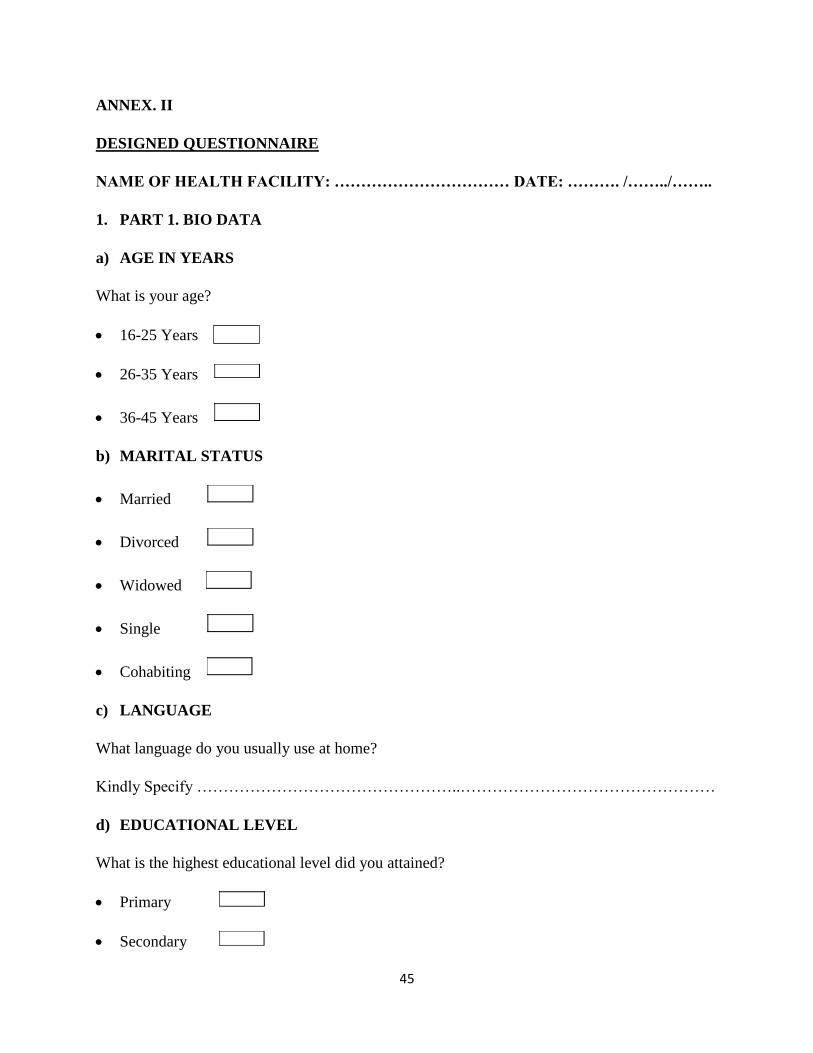
ANNEX. II
DESIGNED QUESTIONNAIRE
NAME OF HEALTH FACILITY: …………………………… DATE: ………. /……../……..
1. PART 1. BIO DATA
a) AGE IN YEARS
What is your age?
16-25 Years
26-35 Years
36-45 Years
b) MARITAL STATUS
Married
Divorced
Widowed
Single
Cohabiting
c) LANGUAGE
What language do you usually use at home?
Kindly Specify …………………………………………..…………………………………………
d) EDUCATIONAL LEVEL
What is the highest educational level did you attained?
Primary
Secondary
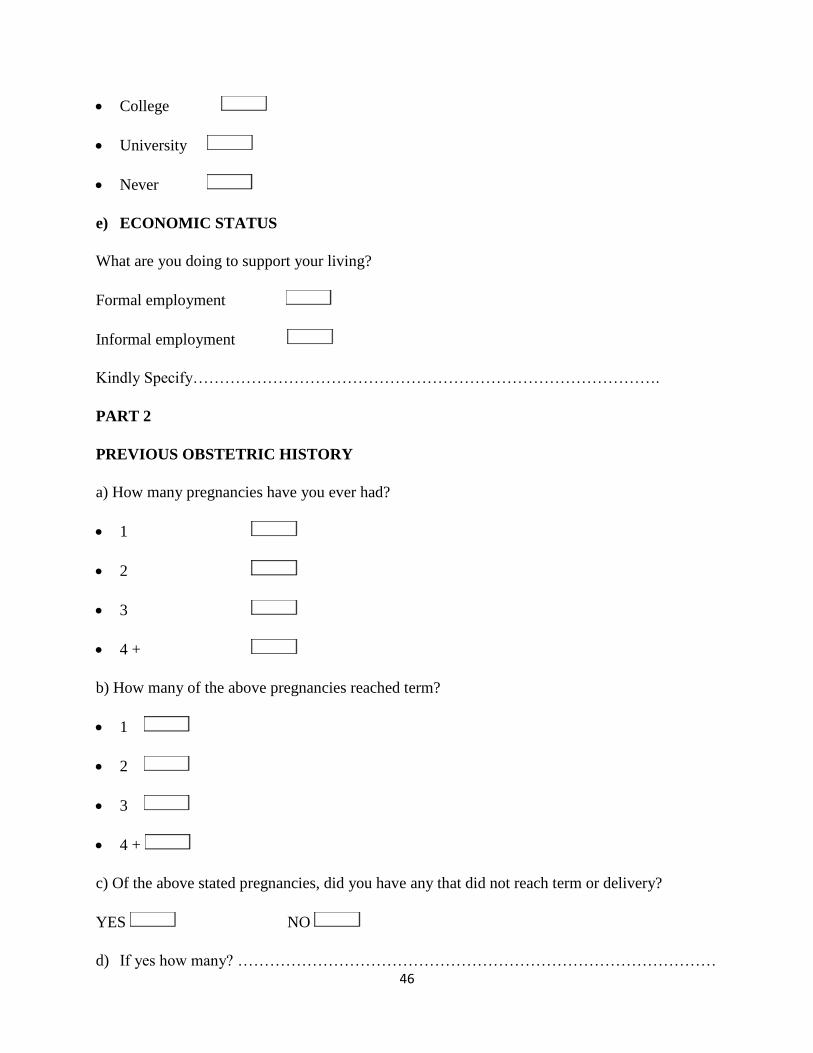
46
College
University
Never
e) ECONOMIC STATUS
What are you doing to support your living?
Formal employment
Informal employment
Kindly Specify…………………………………………………………………………….
PART 2
PREVIOUS OBSTETRIC HISTORY
a) How many pregnancies have you ever had?
1
2
3
4 +
b) How many of the above pregnancies reached term?
1
2
3
4 +
c) Of the above stated pregnancies, did you have any that did not reach term or delivery?
YES NO
d) If yes how many? ………………………………………………………………………………
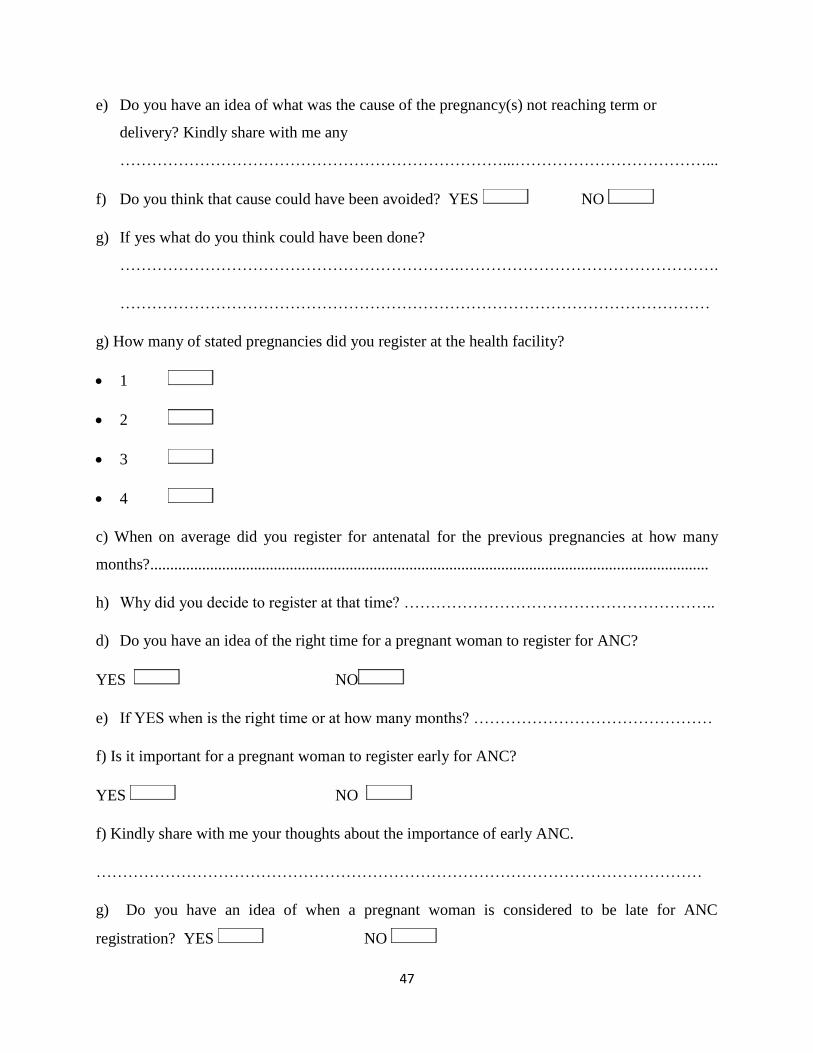
47
e) Do you have an idea of what was the cause of the pregnancy(s) not reaching term or
delivery? Kindly share with me any
………………………………………………………………...………………………………...
f) Do you think that cause could have been avoided? YES NO
g) If yes what do you think could have been done?
……………………………………………………….………………………………………….
…………………………………………………………………………………………………
g) How many of stated pregnancies did you register at the health facility?
1
2
3
4
c) When on average did you register for antenatal for the previous pregnancies at how many
months?............................................................................................................................................
h) Why did you decide to register at that time? …………………………………………………..
d) Do you have an idea of the right time for a pregnant woman to register for ANC?
YES NO
e) If YES when is the right time or at how many months? ………………………………………
f) Is it important for a pregnant woman to register early for ANC?
YES NO
f) Kindly share with me your thoughts about the importance of early ANC.
……………………………………………………………………………………………………
g) Do you have an idea of when a pregnant woman is considered to be late for ANC
registration? YES NO
48
i) If yes kindly share with me when? …………………………………...………………………..
………………………………………………………………………………………………………
k) Do you have an idea of why some women register late for antenatal?
YES NO
l) If yes, kindly share with me any?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
m) Do you have an idea of any danger(s) associated with late ANC registration to a pregnant
woman?
YES NO
n) If yes, kindly share with me any?
…………………………………………………………………..…………………………………..
o) Is it okay for a pregnant woman to register late for antenatal care services?
YES NO
Kindly share your thought with me
………………………………………………………………………………………………………
………………………………………………………………………………………………………
p) Do you have an idea of anything that could be done to help you and other pregnant women to
be registering early for ANC? YES NO
p) If yes what would you suggest………………………………………………………………......
………………………………………………………………………………………………………
………………………………………………………………………………………………………
49
PART 3. HEALTH CARE SERVICE SATISFACTION
a) How far is the health facility from your household? ……………………………..……………
b) Are you comfortable with the distance? YES NO
c) Are you comfortable with the health care services offered at your nearest health facility in
relation to ANC? YES NO
d) If NO, what suggestions can you give in order to help the health care service providers to
improve on their service provision? ……………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
e) On the other hand what role should the women and community play to avoid late ANC
registration?
1. Women:…………………………………………………………………………………………
2. Community:…………………………………………………………………………………….
………………………………………………………………………………………………………
f) Do you have some questions that you would like to ask me concerning the conversation I had
with you?
………………………………………………………………………………………………….
I WOULD LIKE TO THANK YOU SINCERELY FOR YOUR TIME AND
COOPERATION.
THANK YOU AND GOD BLESS
50
ANNEX. III
DESIGNED QUESTIONNAIRE (BEMBA VERSION)
ISHINA LYACIPATAL: …………………………… DATE: ………. /……../……..
2. PART 1. BIO DATA
f) Iciimo mumyaka
Bushe muli nemyaka iyakufyalwa iinga?
16-25 Years
26-35 Years
36-45 Years
g) Ukuupwa
mwalyupwa
mwalilekna
mwalifwila
tamwaupwa
tamulaba pamo
h) ICILIMI
Bushe ciliminshi mubomfya pang’anda?
Mukwai kuti mwanjebako
……………………………………………………………………………………
i) Amasambilio Bushe mwapelele mugeredi shani?
Amasambililo yanono
Museconale
51
Amasambililo yapamulu
j) UKUBOMBA
Bushe mulimonshi mubomba pakuti mulessunga ulupwa?
Mulaibombela mwebeene?
Kwaliba uko muboma ?
Nga kuli umulimo umbi uyo mubombako, kuti mwalanda
mukwai…………………………………………………………………………….
ICIPUTULWA CALENGA BUBILI
UBUFYASHI MUNSHITA YAKUNUMA
a) Bushe mwakwatapo amafumo yanga?
1
2
3
4 +
b) Pali aya mafumo mwalanda bushe niyanga mwalembeshepo ku cipatala ?
1
2
3
4 +
c) Pali ayamafumo mwalanda, bushe bushe mwalikwetepo ayakumashe imyeshi ikumi
YES NO
j) Nga cakuti mwaliikwatapo bushe niyannga?
………………………………………………………………………………
52
k) Bushe finshi mwaishibapo ifyalengele ukuti ayo mafumo yonaike?
……………………………………………………………………..............................................
l) Bushe filya fyacike kwena kuti fyacingiliwa
m) YES NO
n) Nga cakuti mwasuminisha landenipo inshila imofye?
………………………………………………………………………………………………………
k) bushe mafumo yanga mwalembeshepo pali yalya ayo mwakweete?
1
2
3
4
c) Bushe mumafumo yonse ayo mwakwete, niyanga ayo mwalembeshepo kucipatala elo
pamyeshi inga?
………….................................................................................................................................
o) Bushe ninshi mwasaliile ukulembesha pali iyo myesnhsi?…………………………………
f) Bushe mwalishiba imyeshi iyapelwa ukulembeseshapo ifumo?
YES NO
g) Nga cakuti mwalishiba , bushe niinga? ………………………………………
f) Bushe cikankala ukulembesha ifumo?
YES NO
f) Bushe bukankalanshi ubwaba mukulembesha ifumo.
……………………………………………………………………………………………………
g) Bushe nililali umunte engebwa ukuti nabangilila ukulembesha ifumo kucipatala? Bushe
mwalishiba? YES NO
53
p) Naga cakuti mwalishiba, nipamyeshi iinga?…………………………………………………
k) Bushe mwalishiba nililali umuntu engebwa ukuti naceelwa ukulembesha ifumo kucipatala?
YES NO
l) Ngacakuti mwalishiba nililali?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
m) Bushe mwalishiba amafya yesa ngacakuti umuntu aceelwa ukulembesha ifumo?
YES NO
n) Naga mwalishiba, landenipo ubwafya bumofye
……………………………………………………………………………………………………..
o) Bushe caliwama namayo ukuceelwa ukulembesha ifumo?
YES NO
Mukwai landeni naine ifyo mwaishibapo
………………………………………………………………………………………………………
p) Bushe finshi ifingafwaikwa ukwafwilisha banamayo ukulembesha bwangu amafumo, bushe
pali ifyo mwaishibapo? YES NO
p) Nga cakuti mwalishibapo fimo landeni naine mukwai
………………………………………………………………………………………………………
………………………………………………………………………………………………………
ICIPUTLWA CALENGA FITATU (3). IMIBOMBELE YABABOMFI BACIPATALA
g) Bushe paleepa shani apo mwikala naapabela icipatala? ………………………………………
h) Bushe mulasekelamo mumibombele yababomfi bapacipatala? YES NO
i) Bushe mwalitemwa imibombele yababomfi bapacipatala?
j) YES NO
54
k) Nga cakuti tamwasekelamo, finshi mwingatemwa ukutila balecita pakuti banamayo
balelembesha bwangu?
………………………………………………………………………………………………………
………………………………………………………………………………………………………
………………………………………………………………………………………………………
l) Mulubali lumbi, finshi banamayo nabekala mushi balingile ukucita pakuti belcelwa
ukulembesha?
Banamayo………………………………………………………………………………………
Abekala mushi …………………………………………………………………………………
m) Bushe namukwatako iliipusho pafryo twalanshanya mukwai?
………………………………………………………………………………………………….
KUTI NATEMWA UKUMITOOTELA APAKALMBA PAKUIPEELA MULI UKU
KULANSHANYA.
LESA AMIPAALE APAKALAMBA

55
ANNEX .III
NOTIFICATION LATTER
Dear Participant,
My name is MUSONDA ALEX, a student pursuing a degree in nursing and midwifery sciences
at Cavendish University Zambia in Lusaka.
Questions will be asked to help in obtaining data that will help in coming up with
recommendations that will contribute to the reduction of maternal/neonatal mortality related to
late ANC booking.
The study will ensure strict confidentiality. There are no known risks. You may not immediately
benefit from the study but the information will help to understand the prevailing outcomes and
explain the women perceptions on late ANC booking so as to improve maternal and unborn child
survival.
Your participation is completely voluntary. You are free to withdraw at any time and this will
not affect the level of care you and your family including the community receive in any way.
If you agree to take part, please sign the consent form which will allow us to interview you if you
chose to be part of the study.
In case you need some clarification you can contact me on the address below.
MUSONDA ALEX
CELL: 0978140199.
Email: [email protected]
56
ANNEX .IV
CONSENT FORM (ENGLISH VERSION)
EXPLORING WOMEN PERSPECTIVES ON LATE ANC BOOKING IN
MWANSABOMBWE RURAL DISTRICT OF ZAMBIA.
I have read and understood all the information concerning late ANC booking and what this Study
is all about is clear to me. I therefore voluntarily consent to take part in this study.
Participants’ name: ______________________________________________________________
Signature: __________________________ Date: __________________________________
Right Thumb Print: ___________________ Date: __________________________________
WITNESS
Name: ________________________________________________________________________
Signature: ________________________ Date: _____________________________________
Right Thumb Print: _________________ Date: _____________________________________
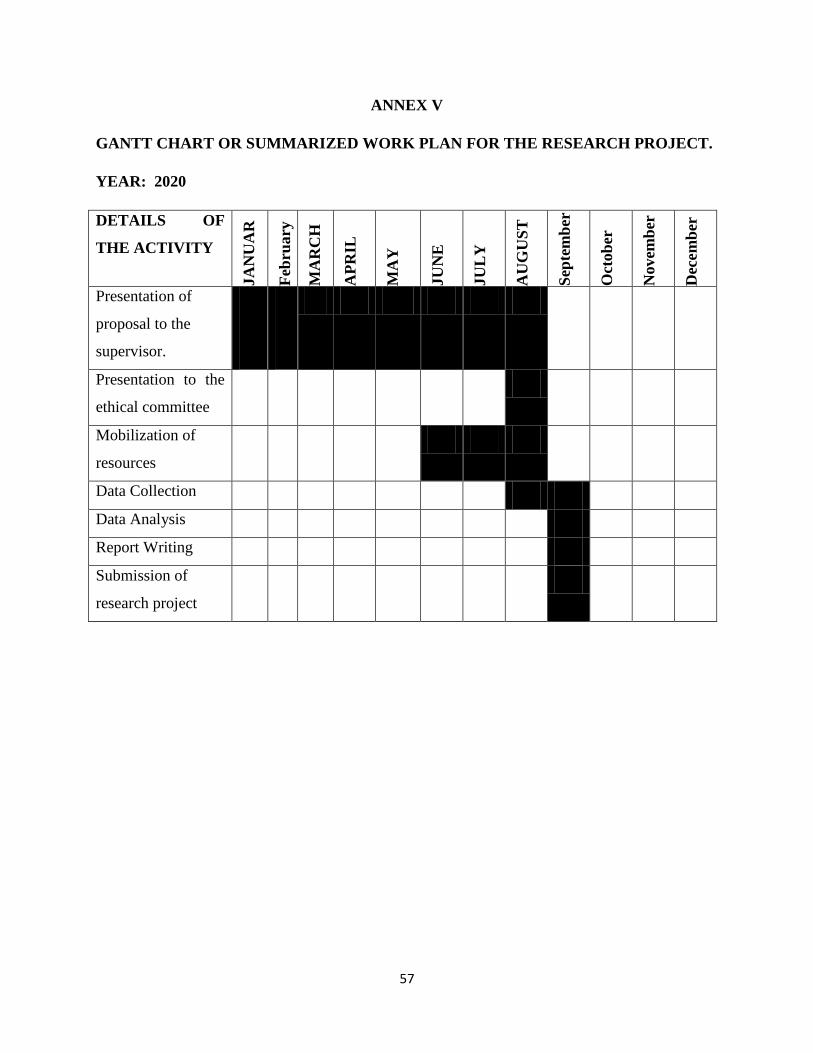
57
ANNEX V
GANTT CHART OR SUMMARIZED WORK PLAN FOR THE RESEARCH PROJECT.
YEAR: 2020
DETAILS OF
THE ACTIVITY JA
NU
AR
Y
Feb
ruary
MA
RC
H
AP
RIL
MA
Y
JU
NE
JU
LY
AU
GU
ST
Sep
tem
ber
Oct
ob
er
Novem
ber
Dec
em
ber
Presentation of
proposal to the
supervisor.
Presentation to the
ethical committee
Mobilization of
resources
Data Collection
Data Analysis
Report Writing
Submission of
research project
58
ANNEX VI
CONSENT FORM (BEMBA VERSION)
UKUFWAILISHA IMITONTONKANISHISHE YABANA-CIFYASHI PAMULANDU
WAKUCEELWA MUMILEMBESESHE YAMAFUMO MUFIAPATA MUMUSUMBA
WAMWANSABOOMBWE ICITUNGU CA LWAPULA.
Ine nabelenga nokwishiba ifya pamulandu wabana-cifyashi ukuceelwa mumilembeseshe
yamafumo. Eico ndeibimba muli uku kulanshanya mukuipeleshafye ukwabula amalipilo.
Ishina lyabaibimbilemo:
___________________________________________________________________________
ukusaina: __________________________ Date: __________________________________
ukufwatiak: ___________________ Date: _______________________________________
BAKAMBONE
ishina: ________________________________________________________________________
ukusaina: ________________________ Date: _____________________________________
ukufwatika: _________________ Date: ___________________________________________
59
ANNEX VII
60
ANNEX VIII