Embed Size (px)
Citation preview

Resuscitation 50 (2001) 87–93
Changes of aortic dimensions as evidence of cardiac pumpmechanism during cardiopulmonary resuscitation in humans
Sung Oh Hwang a,*, Kang Hyun Lee a, Jun Hwi Cho a, Junghan Yoon b,Kyung Hoon Choe b
a Department of Emergency Medicine, Wonju College of Medicine, Yonsei Uni�ersity, 162 Ilsandong, Wonju 220-701, South Koreab Di�ision of Cardiology, Department of Internal Medicine, Wonju College of Medicine, Yonsei Uni�ersity, 162 Ilsandong,
Wonju 220-701, South Korea
Received 18 July 2000; received in revised form 18 July 2000; accepted 3 January 2001
Abstract
The mechanism of forward blood flow during cardiopulmonary resuscitation (CPR) remains controversial. We hypothesizedthat, if the heart acts as a pump, the proximal descending thoracic aorta would be distended during compression by forward bloodflow, and would be constricted or remained unchanged if blood flow is generated by increased intrathoracic pressure. Fourteenpatients with nontraumatic cardiac arrest underwent transesophageal echocardiography to verify changes in the descendingthoracic aorta during standard manual CPR. The aortic dimensions, including cross-sectional area and diameter at the end ofcompression and relaxation, were measured proximal to, and at the maximal compression site of the descending thoracic aorta.At the maximal compression site, deformation of the descending thoracic aorta was observed during compression in all patientsand the ratio of maximal to minimal diameter of the aorta (deformation ratio) decreased during compression compared withrelaxation (0.58�0.15 vs. 0.81�0.11, P=0.001). This suggests eccentric compression of the descending thoracic aorta byexternal chest compression. The deformation ratio of the descending thoracic aorta proximal to the maximal compression siteremained unchanged during compression and relaxation (1.0�0.88 vs. 1.0�0.9, P=0.345). The cross-sectional area of thedescending thoracic aorta proximal to the maximal compression site increased 15% on average during compression compared withrelaxation in 12 of 14 patients. In conclusion, deformation of the aorta at the maximal compression site and increase in thecross-sectional area of the proximal aorta suggests that cardiac pumping is the dominant mechanism in generating forward bloodflow during CPR in humans. © 2001 Elsevier Science Ireland Ltd. All rights reserved.
Keywords: Cardiac arrest; Cardiopulmonary resuscitation; External chest compressions
Resumo
O mecanismo que justifica o fluxo anterogrado do sangue durante a reanimacao cardiorespiratoria (RCR) permanececontroverso. Colocamos a hipotese de: se o coracao actua como uma bomba, a porcao proximal da aorta toracica deveriaapresentar-se distendida durante a fase de aumento da pressao intratoracica. Submeteream-se 14 doentes com paragemcardiorespiratoria (PCR) nao associada a trauma a ecocardiografia transesofagica, estudando as modificacoes da aorta toracicadescendente durante a execucao das manobras standard de RCR. Avaliaram-se as dimensoes da aorta, incluindo a areatransversal e o diametro no final da compressao e relaxamento quer no ponto de maior compressao da aorta toracica descendente,quer proximalmente. A avaliacao no ponto de maior compressao revelou deformacao da aorta descendente, quando dacompressao toracica, em todos os doentes e a razao entre o maior e o menor diametro da aorta (taxa de deformacao) diminuiudurante a compressao por comparacao com o perıodo de relaxamento (0.58 �0.15 vs. 0.81 �0.11, P=0.001). Estes dadossugerem uma compressao excentrica da aorta toracica descendente durante a fase de compressao cardıaca externa. A taxa dedeformacao da aorta toracica descendente, proximal ao ponto de maior compressao manteve-se inalterado quer durante acompressao quer no perıodo de relaxamento (1.0 �0.88 vs. 1.0 �0.9, P=0.345). A area de transseccao da aorta toracicadescendente, proximal ao ponto de maior compressao, aumentou em media 15%, na compressao comparativamente com a fase
www.elsevier.com/locate/resuscitation
* Corresponding author. Tel.: +82-33-7411611; fax: +82-33-7423030.E-mail address: [email protected] (S.O. Hwang).
0300-9572/01/$ - see front matter © 2001 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0 3 0 0 -9572 (01 )00319 -7

S.O. Hwang et al. / Resuscitation 50 (2001) 87–9388
de relaxamento, em 12 dos 14 doentes. Em conclusao, a deformacao da aorta no ponto de maior compressao e o aumento da areade transseccao da aorta na regiao proximal, sugerem que o mecanismo de bomba toracica e o predominante na geracao de fluxosanguıneo anterogrado durante as manobras de reanimacao cardiorespiratoria, em humanos © 2001 Elsevier Science Ireland Ltd.All rights reserved.
Pala�ras cha�e: Paragem cardıaca; Reanimacao Cardio-Pulmonar; Compressao cardıaca externa
1. Introduction
Since external chest compression was introduced as amethod of providing an artificial circulation [1] for acardiac arrest patient, the question of whether bloodflow during cardiopulmonary resuscitation (CPR) re-sults from intrathoracic pressure fluctuation (thoracicpump mechanism) [2–4] or direct cardiac compression(cardiac pump mechanism) [5,6] has remained open.The controversies as to the mechanism of blood flowduring CPR are because the subject of research hasbeen performed with animal experimental models. Theresults of animal studies on the mechanisms of bloodflow during CPR are not necessarily applicable to hu-mans because the rib cage of animals is generallythicker anteroposteriorly and differently dispersed com-pared to humans. It is impossible to study the mecha-nism of blood flow during CPR in humans using thesame methods that are applied to animals because ofthe urgent need for resuscitation. Although it has beensuggested by some investigators that both cardiac andthoracic pumps may be involved [7,8], determining thedominant pump in humans will give insight for thedevelopment of new CPR methods.
To determine which mechanism drives blood flowduring CPR, we made the following assumptions; ifdirect compression of the heart plays a major role inproducing forward blood flow, the amount of bloodvolume flowing to the aorta should be proportionate tothe cardiac deformity caused by chest compression. Asin normal ventricular systole, the blood flow shouldincrease the diameter of the descending thoracic aortaduring compression systole. Conversely, if increasedintrathoracic pressure generates blood flow, the in-trathoracic pressure increase would reduce the size ofall intrathoracic vascular structures including the de-scending thoracic aorta. From this we hypothesizedthat the diameter of the descending thoracic aortawould be increased by forward blood flow if the heartacts as a pump, and be contracted or remain unchangedif increased intrathoracic pressure generates blood flowduring cardiac compression. The purpose of this studywas to investigate the mechanism of blood flow gener-ated by external chest compression in humans by ob-serving and analyzing changes in the descendingthoracic aorta during CPR.
2. Patients and methods
All patients over the age of 18 years with non-trau-matic cardiac arrest were enrolled in the study. Patientswho had structural heart diseases or aortic disease ontransesophageal echocardiography (TEE) were ex-cluded. The study was reviewed and approved by theHuman Investigation Committee of our institution. In-formed consent could not be obtained from the pa-tients, but verbal communication was made with afamily member present.
2.1. Cardiopulmonary resuscitation
The team performed CPR as soon as the patientarrived at the emergency room or just after the cardiacarrest developed. CPR was performed in accordancewith American Heart Association (AHA) guidelines [9].The rate of chest compression was 80 per min. Externalchest compressions were done by one of emergencyresidents. Ventilation with 100% oxygen was providedwith a self-inflating bag. One miligram of epinephrinewas injected into the antecubital vein in every 3 min.
2.2. Transesophageal echocardiography
TEE was performed during CPR just after comple-tion of tracheal intubation and injection of first dose ofepinephrine. One of the authors (H.S.O.) not directlyinvolved in the CPR introduced a multiplane trans-esophageal probe (5 MHz, Ultramark-9, AdvancedTechnology Laboratories Inc., USA) into the oesopha-gus to observe the heart and the descending thoracicaorta. Immediately after the transesophageal probe wasinserted, the heart and the aorta were briefly examinedto search for possible causes of cardiac arrest. Anypatient who had a morphologic abnormality on TEEwas excluded from the study. Left atrium– left ventricletwo-chamber views at 90 and 135° were used to inspectmitral and aortic valve closure, and a horizontal four-chamber view to evaluate the extent of left ventriclecompression. A longitudinal view of the descendingthoracic aorta was taken to identify the maximal com-pression site due to external chest compression and ahorizontal view was selected to observe deformation ofthe aorta and to measure the diameter and cross-sec-tional area of the aorta. Images of the descendingthoracic aorta were obtained at the point of the maxi-

S.O. Hwang et al. / Resuscitation 50 (2001) 87–93 89
mal compression site and at the descending thoracicaorta 5–10 cm above the maximal compression site. Allechocardiographic images were recorded with s-VHSvideotape.
2.3. Analysis of recorded images
The images recorded during CPR were analyzed by acardiac image analysis system (Imagevue, Novamicro-sonics Inc., USA). After freezing recorded images fromthe cardiac analysis system, calibration was made by aninternalized calibrator. Aortic diameter was measured,and the cross-sectional area was calculated by tracingsof the external wall of the aorta. Maximal diameter andminimal diameter were selected for each part of theaorta. The ratio of maximal diameter to minimal di-ameter (deformation ratio) was calculated to identifythe existence of aortic deformation at the maximalcompression point and the descending thoracic aortaproximal to the maximal compression point at the timeof compression and relaxation. The cross-sectional areaof the aorta was also measured to assess whether theaorta was dilated during compression. To determinewhether the mitral valve was closed during compres-sion, images from the left atrium– left ventricle two-chamber view and the horizontal four-chamber viewwere used. Change in left ventricular volume was deter-mined by subtracting end-systolic volume from end-diastolic volume. Left ventricular volume wascalculated by the area– length method [10]. Each mea-surement was calculated by taking the average value offive consecutive cycles from the recorded images.Analyses were performed and reviewed by an emer-gency physician (H.S.O.) and two cardiologists (J.Y.and K.H.C.). If there were any disagreements, theimage was reanalyzed.
2.4. Statistical analysis
Data were coded into a computerized data processingsoftware (SPSS for windows 8.0, SPSS Inc., Chicago,IL). Continuous variables were analyzed by paired t-test or Mann–Whitney U-tests if appropriate, andstatistical significance was noted at a P-value less than0.05. All data are presented as mean�SD.
3. Results
During the study period, 16 patients who sufferednon-traumatic cardiac arrest underwent TEE. However,only 14 patients were included in the analysis becauseone patient had an inadequate echocardiographic win-dow and one patient had aortic dissection.
Eight patients were men. The mean age was 67 years.Eleven patients had arrests in the field and three pa-tients had arrests in the emergency department. Table 1shows the characteristics of each patient. The averagetime from patient arrival to completion of probe inser-tion was 8�7 min. There was no difficulty in introduc-ing the TEE probe into the esophagus.
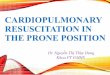
At the point of maximal compression, deformationsof the descending thoracic aorta were observed in allpatients during compression (Fig. 1). Gross morphol-ogy of the proximal descending thoracic aorta remainedunchanged during compression and relaxation.
At the maximal compression site, the minimal diame-ter of the descending thoracic aorta decreased by 37�17% during compression compared to the diameterduring relaxation, while maximal diameter of that in-creased by 9�11% during compression compared tothe diameter during relaxation. At the aorta proximalto maximal compression, minimal and maximal diame-ters of the descending thoracic aorta changed little
Table 1Patient dataa
Arrest timePlace of cardiac arrest Presumed etiologySex/age OutcomeCase Initial rhythm
Male/821 Out-of-hospital 10 Asystole Cardiac No ROSCMale/44 Out-of-hospital 202 Asystole No ROSCCardiac
CardiacVFFemale/543 15Out-of-hospital No ROSC15 VF Cardiac No ROSCOut-of-hospitalMale/664
Female/74 Emergency department 25 VF Survival dischargeNon-cardiacFemale/806 Out-of-hospital 32 Asystole Non-cardiac No ROSCFemale/82 Cardiac No ROSCOut-of-hospital 227 Asystole
Asystole Cardiac No ROSC8 Female/53 Out-of-hospital 22Asystole Cardiac No ROSC9 Male/88 Out-of-hospital 20
No ROSCCardiacAsystole2510 Out-of-hospitalMale/73PEA Non-cardiac No ROSCOut-of-hospital11 30Male/57
Female/82 Emergency department 112 VF Non-cardiac Died in 24 h13 Died in 24 hCardiacVF2Male/59 Emergency department
Male/41 Out-of-hospital 15 Asystole Cardiac Died in 24 h14
a VF, ventricular fibrillation; PEA, pulseless electrical activity; ROSC – return of spontaneous circulation.

S.O. Hwang et al. / Resuscitation 50 (2001) 87–9390
Fig. 1. Changes in gross morphology of the descending thoracic aorta during CPR: Horizontal views of the descending thoracic aorta at themaximal compression area show that anterior wall of the aorta is being compressed during compression (A) and restored to it’s original shapeduring relaxation (B).
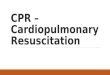
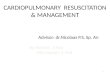
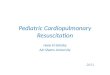
during compression as compared to relaxation (7�8% in minimal diameter and 3�5% in maximal di-ameter). At the site of maximal compression, thedeformation ratio of the descending thoracic aorta de-creased during compression compared with relaxation(0.58�0.15 vs. 0.81�0.11, P=0.001), which suggestseccentric compression of the descending thoracic aortaby external chest compression during CPR (Fig. 2).At the point proximal to the maximal compressionsite, the deformation ratio of the descending thoracicaorta remained unchanged during compression andrelaxation (1.0�0.88 vs. 1.0�0.9, P=0.345) (Fig. 3).At the point proximal to the maximal compressionsite, the cross-sectional area of the descending tho-
racic aorta increased during compression compared torelaxation in 12 patients while cross-sectional area re-mained unchanged in two patients (Fig. 4). The aver-age increase in the cross-sectional area was 15�12%compared to the relaxation period.
Left-ventricular volume was 45�34 ml during re-laxation and 26�30 ml during compression. It wasdifficult to acquire an optimal image plane to measureleft-ventricular volume during compression and relax-ation because the heart swung markedly with pre-cordial compression. The mitral valve was closed dur-ing compression and the aortic valve was open brieflyduring the early phase of compression in all pa-tients.
Fig. 2. Deformation ratio (minimal diameter/maximal diameter) of the descending thoracic aorta at the maximal compression area during thecompression and relaxation period of CPR. Decrease in deformation ratio during compression suggests eccentric compression of the aorta byexternal chest compression.

S.O. Hwang et al. / Resuscitation 50 (2001) 87–93 91
Fig. 3. Deformation ratio (minimal diameter/maximal diameter) of the descending thoracic aorta proximal to the maximal compression areaduring the compression and relaxation period of CPR. Deformation ratio remains unchanged, which suggests proximal descending thoracic aortadoes not have morphologic change by external chest compression.
4. Discussion
In this study, we found that the descending thoracicaorta was eccentrically compressed at the site of maxi-mal compression in all patients enrolled in this studyand the cross-sectional area of the aorta proximal tothe compressed area increased during CPR in mostpatients. Eccentric deformation of the descending tho-racic aorta during compression is considered to happenbecause the heart is displaced posteriorly when thesternum is compressed, and the displaced heart com-presses the descending thoracic aorta. Dilatation of theproximal descending aorta during compression suggeststhat aortic volume increases when blood flows from theheart into the aorta due to chest compression. Thisfinding supports the cardiac pump theory that forwardblood flow is due to direct compression of the heartbetween the sternum and the vertebral column duringchest compression. The hemodynamic mechanism ofchest compression, postulated by researchers [11,12]who insist on the thoracic pump mechanism, is that it isnot due to a direct cardiac compression effect but
predominantly due to the elevation of the gradientbetween the intrathoracic and extrathoracic pressure. Ifit is true that the consequence is a result of the pressuregradient only, without an effect from direct cardiaccompression, the elevated intrathoracic pressure proba-bly should exert the same pressure on the entire tho-racic descending aorta. Therefore, there should beneither deformation nor dilatation of the descendingthoracic aorta during compression if circulation is aresult of the thoracic pump mechanism.
Since Kouwenhoven et al. [1] suggested direct cardiaccompression as the mechanism of forward blood flow,there have been many debates on the role of the heartduring CPR. Among the investigations to define themechanism of blood flow, only a few [8,13–16] wereperformed on humans because of the urgent need forresuscitation. Recently, TEE was introduced to investi-gate the mechanism of blood flow during CPR inhuman because it provides high-resolution images ofthe thoracic cardiovascular structures and can be per-formed without interrupting external chest compres-sion. TEE has been found to be a useful tool to study
Fig. 4. Cross-sectional area of the descending thoracic aorta proximal to the maximal compression area. Cross-sectional area increased duringprecordial compression in 12 of 14 patients.

S.O. Hwang et al. / Resuscitation 50 (2001) 87–9392
the mechanism of blood flow during CPR by investiga-tion of mitral valve motion, flow direction by Dopplerechocardiography [13–15] and the haemodynamic ef-fect of new CPR techniques [16]. TEE studies to datehave focused on the position of the mitral valve and thedirection of blood flow during chest compression. How-ever, consistent analysis has yet to be established. Thefocus of interest in this paper was to analyse changes inthe descending thoracic aorta, which are easily ob-served by TEE, as indirect evidence of the cardiacpump mechanism during CPR. Nieman et al. [17] re-ported in their angiographic observations that aorticdiameter decreased during precordial compression inexperimental animals. Guerci et al. [18] also studiedchanges in aortic dimensions to define the pump whichwas operative during external chest compression. Theyreported that they carried out angiograms during CPRin dogs and found a decrease in the diameter of thethoracic aorta during compression. They pointed outthat decreases in the size of the aorta suggested thoracicpump mechanism because the aorta would be distendedif the heart were squeezed. Their results were the veryopposite to that observed in this study. There are twodifferent points between Guerci’s and our study. Theirobservations were made in an animal experiment usingdogs while our study was done with humans. This leadsto results that are not comparable, because the thoraciccage of animals such as dogs have a different structurecompared with human. Dogs have a longer antero-pos-terior diameter than bilateral and a narrower anteriorchest wall surface than humans. The heart and aorta,located in the posterior part of the thoracic cage, arehardly pressed down on chest compression, in animals.In our study, chest compression in human leads tocompression of the descending thoracic aorta providingevidence of cardiac compression because the heart islocated just in front of the thoracic aorta. Moreover,the proximal descending thoracic aorta was dilatedduring chest compression, supporting the theory thatcirculation in human CPR is predominantly made bycardiac compression. The second different point be-tween the two studies was the method used to detectchanges in aortic dimension. Guerci et al. observed theaorta by means of angiograms while TEE was chosenfor our study. Eccentric compression of the aorta mightbe shown an angiography at certain angle, as if theaorta was constricted during the compression systole.On the other hand, TEE can provide a close inspectionof the cross-sectional area as well as the shape of thevascular deformation.
The duration of resuscitation affects the mechanismof CPR [19]. While the cardiac pump plays a predomi-nant role in early CPR, the thoracic pump might bemore important when the heart becomes less compliantas the duration of cardiac arrest or resuscitation at-tempt is prolonged [20]. It is not known when and how
the thoracic pump becomes more predominant than thecardiac pump during resuscitation. Timing of observa-tions may affect our conclusions regarding mechanismof blood flow. Our observation was done during theearly phase of resuscitation attempt, so that the cardiacpump would dominate the thoracic pump at this pe-riod. There might be the possibility that thoracic pumpdominates in two patients with prolonged resuscitationwhose cross-sectional area of the aorta remained un-changed. However, most of patients showed an increasein cross-sectional area of the aorta although they had awide range of resuscitation duration. This finding sug-gests that the haemodynamic effect of the cardiac pumpmay persist for a relatively long period duringresuscitation.
We cannot say that, from our results, the cardiacpump is the only mechanism of blood flow generatedby standard CPR in humans. We can say that anincrease in aortic cross-sectional area during compres-sion suggests a cardiac pump mechanism as the domi-nant mechanism in generating blood flow in humans.Recent studies [13,15,21,22] using TEE provided evi-dence that support a cardiac pump mechanism, whilemost studies [2–4] that favour the thoracic pump havebeen performed in animals.
There are several limitations to this study. First, weonly assessed aortic dimensions during CPR. Eventhough we observed the cardiac chambers, we could notassess changes in the descending thoracic aorta as wellas in the cardiac chambers and valves simultaneously.Simultaneous observation of the aorta and the heartmay be needed to find the relationship between changesin the aortic dimensions and cardiac valve motions.There is still a debate as to whether closure of themitral valve suggests direct compression of the leftventricle during compression systole [23]. It is impossi-ble to observe the heart and the aorta at the samemoment with TEE. Second, we could not measureintracavitary pressures including that in the left ventri-cle and the aorta. Therefore, we could not investigatethe time sequences of pressure rise in the left ventricleand the aorta, which may help to verify the pumpdriving blood flow. Third, we could not measure bloodflow (this is not feasible during CPR in humans), sothat we could not correlate morphologic changes of theaorta with blood volume transferred from the left ven-tricle to the aorta. Fourth, the compression force couldnot be measured during CPR. Higher compressionforces might produce direct cardiac compression[24,25]. However, excessive compression forces mustnot be administered because residents of emergencydepartments perform precordial compression accordingto AHA guidelines. Fifth, we could not compare aorticdimensions throughout the entire duration of CPR thataffects the mechanism of blood flow because of theclinical situation. Further studies are needed to verify

S.O. Hwang et al. / Resuscitation 50 (2001) 87–93 93
the effect of CPR duration on mechanism of bloodflow.
Continuing controversy regarding mechanism ofblood flow during CPR in humans may be attributed tothe results of previous experimental studies that havebeen performed with animal that have differentanatomical structures. The increase in the cross-sec-tional area of the aorta observed in this study suggeststhat the cardiac pumping is the dominant mechanism ingenerating blood flow during CPR in humans eventhough thoracic pump is also operative.
References
[1] Kouwenhoven WB, Jude JR, Knickerbocker GG. Closed chestcardiac massage. J Am Med Assoc 1960;173:1063–7.
[2] Halperin HR, Tsitlik JE, Guerci AD, Mellits ED, Levin HR, ShiAY, et al. Determinants of blood flow to vital organs duringcardiopulmonary resuscitation in dogs. Circulation 1986;73:539–50.
[3] Halperin HR, Tsitlik JE, Beyar R, Chandra N, Guerci AD.Intrathoracic pressure fluctuations move blood during CPR:comparison of hemodynamic data with predictions from a math-ematical model. Ann Biomed Eng 1987;15:385–403.
[4] Rudifoff MT, Maughan WL, Effron M, Freund P, WeisfeldtML. Mechanisms of blood flow during cardiopulmonary resusci-tation. Circulation 1980;61:345–52.
[5] Feneley MP, Maier GW, Gaynor JW, Gall SA, Kisslo JA, DavisJW, et al. Sequence of mitral valve motion and transmitral bloodflow during manual cardiopulmonary resuscitation in dogs. Cir-culation 1987;76:363–75.
[6] Deshmukh HG, Weil MH, Gudipati CV, Trevino RP, Bisera J,Rackow EC. Mechanism of blood flow generated by precordialcompression during CPR. I. Studies on closed chest precordialcompression. Chest 1989;95:1092–9.
[7] Paradis NA, Martin GB, Goetting MG, Rosenberg JM, RiversEP, Appleton TJ, et al. Simultaneous aortic, jugular bulb, andright atrial pressures during cardiopulmonary resuscitation inhumans. Insights into mechanisms. Circulation 1989;80:361–8.
[8] Porter TR, Ornato JP, Guard CS, Roy VG, Burns CA, NixonJV. Transesophageal echocardiography to assess mitral valvefunction and flow during cardiopulmonary resuscitation. Am JCardiol 1992;70:1056–60.
[9] Guidelines for cardiopulmonary resuscitation and emergencycardiac care. Emergency Cardiac Care Committee and Subcom-mittee, American Heart Association. Part II. Adult Basic LifeSupport and Part III. Adult Advanced Cardiac Life Support.JAMA 1992;268:2184–241.
[10] Schiller NB, Shah PM, Crawford M, DeMaria A, Devereux R,Feigenbaum H, et al. Recommendations for quantitation of theleft ventricle by two-dimensional echocardiography. American
Society of Echocardiography Committee on Standards, Subcom-mittee on Quantitation of Two-Dimensional Echocardiograms. JAm Soc Echocardiogr 1989;2:358–67.
[11] Criley JM, Niemann JT, Rosborough JP, Ung S, Suzuki J. Theheart is a conduit in CPR. Crit Care Med 1981;9:373–4.
[12] Chandra NC, Tsitlik JE, Halperin HR, Guerci AD, WeisfeldtML. Observations of hemodynamics during human cardiopul-monary resuscitation. Crit Care Med 1990;18:929–34.
[13] Higano ST, Oh JK, Ewy GA, Seward JB. The mechanism ofblood flow during closed chest cardiac massage in humans:transesophageal echocardiographic observations. Mayo ClinProc 1990;65:1432–40.
[14] Ma MH, Hwang JJ, Lai LP, Wang SM, Huang GT, Shyu KG,et al. Transesophageal echocardiographic assessment of mitralvalve position and pulmonary venous flow during cardiopul-monary resuscitation in humans. Circulation 1995;92:854–61.
[15] Redberg RF, Tucker KJ, Cohen TJ, Dutton JP, Callaham ML,Schiller NB. Physiology of blood flow during cardiopulmonaryresuscitation. A transesophageal echocardiographic study. Circu-lation 1993;88:534–42.
[16] Cohen TJ, Tucker KJ, Lurie KG, Redberg RF, Dutton JP,Dwyer KA, et al. Active compression–decompression. A newmethod of cardiopulmonary resuscitation. J Am Med Assoc1992;267:2916–41.
[17] Nieman JT, Rosborough JP, Hausknecht M, Garner D, CrileyJM. Pressure-synchronized cineangiography during experimentalcardiopulmonary resuscitation. Circulation 1981;64:985–91.
[18] Guerci AD, Halperin HR, Beyar R, Beattie C, Tsitlik JE,Wurmb EC, et al. Aortic diameter and pressure-flow sequenceidentify mechanism of blood flow during external chest compres-sion in dogs. J Am Coll Cardiol 1989;14:790–8.
[19] Swart GL, Mateer JR, DeBehnke DJ, Jameson SJ, Osborn JL.The effect of compression duration on hemodynamics duringmechanical high-impulse CPR. Acad Emerg Med 1994;1:430–7.
[20] Takino M, Okada Y. Firm myocardium in cardiopulmonaryresuscitation. Resuscitation 1996;33:101–6.
[21] Kuhn C, Juchems R, Frese W. Evidence for the ‘cardiac pumptheory’ in cardiopulmonary resuscitation in man by trans-esophageal echocardiography. Resuscitation 1991;22:275–82.
[22] Pell AC, Guly UM, Sutherland GR, Steedman DJ, Bloomfield P,Robertson C. Mechanism of closed chest cardiopulmonary re-suscitation investigated by transesophageal echocardiography. JAccid Emerg Med 1994;11:139–43.
[23] Halperin HR, Weiss JL, Guerci AD, Chandra N, Tsitlik JE,Brower R, et al. Cyclic elevation of intrathoracic pressure canclose the mitral valve during cardiac arrest in dogs. Circulation1988;78:754–60.
[24] Maier GW, Tyson GS Jr., Olsen CO, Kernstein KH, Davis JW,Conn EH, et al. The physiology of external cardiac massage:high-impulse cardiopulmonary resuscitation. Circulation1984;70:86–101.
[25] Hackl W, Simon P, Mauritz W, Steinbereithner K. Echocardio-graphic assessment of mitral valve function during mechanicalcardiopulmonary resuscitation in pigs. Anesth Analg1990;70:350–6.
.