Embed Size (px)
Citation preview

http://ajs.sagepub.com
MedicineAmerican Journal of Sports
DOI: 10.1177/0363546507308935 2008; 36; 523 originally published online Nov 8, 2007; Am. J. Sports Med.Crenshaw and James R. Andrews
Michael M. Reinold, Kevin E. Wilk, Leonard C. Macrina, Chris Sheheane, Shouchen Dun, Glenn S. Fleisig, Ken Players
Changes in Shoulder and Elbow Passive Range of Motion After Pitching in Professional Baseball
http://ajs.sagepub.com/cgi/content/abstract/36/3/523 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
On behalf of:
American Orthopaedic Society for Sports Medicine
can be found at:American Journal of Sports MedicineAdditional services and information for
http://ajs.sagepub.com/cgi/alerts Email Alerts:
http://ajs.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://ajs.sagepub.com/cgi/content/abstract/36/3/523#BIBLSAGE Journals Online and HighWire Press platforms):
(this article cites 33 articles hosted on the Citations
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from
The unique range of motion (ROM) characteristics of theshoulder in overhead throwing athletes have been welldefined.1-4,6,8,16,18,25,31 These studies have shown increasedexternal rotation (ER) and decreased internal rotation (IR)
at 90° of abduction in the throwing shoulder.1-4,6,8,16,18,25,31
Wright et al32 have documented a decrease in elbow exten-sion and flexion ROM in throwing athletes.
Wilk et al31 reported the shoulder passive ROM character-istics in 372 professional baseball players. The authorsreported a mean of 129° ± 10° of ER and 61° ± 9° of IR in thethrowing shoulder at 90° of abduction. The authors notedthat ER was 7° greater and IR was 7° less in the dominantarm when compared with the nondominant arm.The conceptof “total motion” was introduced in this article. Total motionis the total value of ER plus IR ROM (at 90° of abduction).The authors noted that there was not a significant differencein total motion bilaterally, despite alterations in ER and IR.
Changes in Shoulder and Elbow PassiveRange of Motion After Pitching inProfessional Baseball PlayersMichael M. Reinold,*†‡ PT, DPT, ATC, CSCS, Kevin E. Wilk,§ll PT, DPT,Leonard C. Macrina,§ MSPT, CSCS, Chris Sheheane,§ ATC, Shouchen Dun,ll MS,Glenn S. Fleisig,ll PhD, Ken Crenshaw,¶ ATC, CSCS, and James R. Andrews,ll# MDFrom the †Boston Red Sox Baseball Club, Boston, Massachusetts, ‡Massachusetts GeneralHospital, Department of Orthopedics, Sports Medicine Division, Boston, Massachusetts,§Champion Sports Medicine, Birmingham, Alabama, llAmerican Sports Medicine Institute,Birmingham, Alabama, ¶Arizona Diamondbacks Baseball Club, Phoenix, Arizona,and #Alabama Sports Medicine and Orthopedic Center, Birmingham, Alabama
Background: The overhead throwing athlete has unique range of motion characteristics of the shoulder and elbow. Numeroustheories exist to explain these characteristics; however, the precise cause is not known. Although it is accepted that range ofmotion is altered, the acute effect of baseball pitching on shoulder and elbow range of motion has not been established.
Hypothesis: There will be a reduction in passive range of motion immediately after baseball pitching.
Study Design: Controlled laboratory study.
Methods: Sixty-seven asymptomatic male professional baseball pitchers participated in the study. Passive range of motionmeasurements were recorded using a customized bubble goniometer for shoulder external rotation, shoulder internal rotation,total shoulder rotational motion, elbow flexion, and elbow extension on the dominant and nondominant arms. Testing was per-formed on the first day of spring training. Measurements were taken before, immediately after, and 24 hours after pitching.
Results: A significant decrease in shoulder internal rotation (–9.5°), total motion (–10.7°), and elbow extension (–3.2°) occurredimmediately after baseball pitching in the dominant shoulder (P < .001). These changes continued to exist 24 hours after pitch-ing. No differences were noted on the nondominant side.
Conclusion: Passive range of motion is significantly decreased immediately after baseball pitching. This decrease in range ofmotion continues to be present 24 hours after throwing. High levels of eccentric muscle activity have previously been observedin the shoulder external rotators and elbow flexors during pitching. These eccentric muscle contractions may contribute to acutemusculotendinous adaptations and altered range of motion. The results of this study may suggest a newly defined mechanismto range of motion adaptations in the overhead throwing athlete resulting from acute musculoskeletal adaptations, in addition topotential osseous and capsular adaptations.
Keywords: overhead throwing athlete; glenohumeral joint; capsule; internal impingement
523
*Address correspondences to Michael M. Reinold, PT, DPT, ATC, CSCS,Coordinator of Rehabilitation Research & Education, MGH SportsMedicine Center, Fenway Park, 4 Yawkey Way, Boston, MA 02215 (e-mail:[email protected]).
No potential conflict of interest declared.
The American Journal of Sports Medicine, Vol. 36, No. 3DOI: 10.1177/0363546507308935© 2008 American Orthopaedic Society for Sports Medicine
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from

524 Reinold et al The American Journal of Sports Medicine
These ROM characteristics have been shown by severalauthors in studies of baseball1-4,6 and tennis players.8
Although the altered ROM observed is currentlyaccepted as a physiological adaptation that occurs nor-mally in overhead throwing athletes, no study to date hasdocumented the acute effect of baseball pitching on ROM.Alterations in ROM as the result of baseball pitching mayhave implications for injury potential.19,27 Furthermore,understanding the acute effect of pitching on ROM mayassist in the evaluation of the injured players and thedesign of injury prevention stretching programs. Thus, thepurpose of the present study was to examine the acuteeffects of baseball pitching on ROM of the shoulder andelbow in professional athletes.
METHODS
Subjects
Sixty-seven professional baseball pitchers participated inthe study (mean age, 26 ± 4 years; height, 171 ± 5 cm;weight, 92 ± 10 kg). Fifty-one were right-hand dominant,and 16 were left-hand dominant. All subjects were asymp-tomatic of shoulder and elbow pain and demonstrated nosigns of injury at the time of testing. Subjects wereexcluded if they had undergone a previous surgery of theshoulder or elbow within the last 12 months before datacollection. All measurements were taken during the first 2days of spring training, before the beginning of practicesessions or the season. The subjects were advised of thenature of the procedure, and informed consent wasobtained before testing.
Testing Procedure
Measurements of bilateral passive shoulder ER and IR at90° of abduction and 10° of horizontal adduction alongwith elbow flexion and extension were assessed (Figures 1-4). The order of extremity and measurement performedwas randomized before data collection. Two examinerswere consistently used for all measurements, 1 to positionthe extremity (M.M.R.) and 1 to align and read thegoniometer (C. S.). Subjects were positioned in the supineposition with a towel roll placed between the arm and thetable. The examiner positioning the extremity was blindedto the results of the measurement.
The examiner passively moved the extremity to the endROM, and the position was held as the goniometer wasaligned and read. The ER and IR were performed with thetable stabilizing the scapula. For shoulder ER, elbow flexion,and elbow extension, the motion was stopped at the subject’send of available ROM when full capsular or bony end feelwas achieved. For shoulder IR, a combination of end feel andvisualization of compensatory movement was used to deter-mine the end of ROM. The extremity was moved until theshoulder was visualized to begin lifting off the table; motionwas stopped when this movement occurred. The humeralhead was not manually stabilized to avoid altering the nor-mal glenohumeral arthrokinematics during measurement.
A standard goniometer with an attached customized bub-ble inclinometer was used to ensure proper perpendicular
alignment of the goniometer. For shoulder measurement, thefulcrum of the goniometer was positioned over the olecranonprocess, with one arm of the device perpendicular to theground and the other arm aligned along the ulnar to theulnar styloid process.20 For elbow measurements, the ful-crum of the goniometer was positioned over the lateral epi-condyle of the humerus, with one arm of the device along thelength of the humerus to the tip of the acromion process andthe other arm along the length of the radius to the radial
Figure 1. Passive shoulder external rotation range of motionat 90° of abduction and 10° of horizontal adduction.
Figure 2. Passive shoulder internal rotation range of motionat 90° of abduction and 10° of horizontal adduction.
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from
Vol. 36, No. 3, 2008 Shoulder/Elbow Passive Range of Motion in Pitching 525
styloid process.20 Positive elbow extension was defined asmotion past 0° into hyperextension. Conversely, negativeelbow extension was defined as motion before 0°, such aswith an elbow flexion contracture.
Measurements were initially taken before any warm-up,exercise, or throwing program was performed. Subjectsthen warmed up with jogging for 5 minutes, generalizedfull-body stretching for 15 minutes, and a long-toss pro-gram up to 27.4 m for 10 minutes. Subjects then beganpitching from a standard pitching mound for 50 to 60pitches at full intensity. All ROM measurements wererepeated within 30 minutes of the conclusion of pitching.All measurements were repeated again on the dominantside using the same procedures 1 day (24 hours) after ini-tial testing before the subject performed any warm-upexercises or throwing.
Reliability
A pilot study was performed before data collection toassess the test-retest intratester reliability of the gonio-metric methodology of this study. Ten asymptomatic malesubjects (mean age, 28.3 years; height, 180 cm; weight, 88kg) were measured once in all 4 positions by the sameexaminers used in the main study. All 4 measurements
were randomly repeated on 5 consecutive days to assesstest-retest intratester reliability. The order of tests per-formed was randomized. All subjects refrained from par-ticipating in any overhead throwing sports during thetesting period.
To examine the rest-retest reliability, intraclass correlationcoefficients (ICC3,1) were calculated on shoulder ER, shoulderIR, elbow flexion, and elbow extension using data collected inthe pilot study. Single-measure intraclass correlation resultswere 0.8115 for shoulder IR, 0.8740 for shoulder ER, 0.9053for elbow flexion, and 0.9740 for elbow extension.
Data Analysis
For the dominant side, a 1-way repeated-measures analy-sis of variance was performed for each of the 4 variables toevaluate the differences in ROM before, immediately after,and 24 hours after throwing. When a statistical signifi-cance was detected, post hoc paired t tests were conductedto test for significance of pairwise comparisons. For thenondominant side, a paired-samples t test was performedfor each of the 4 variables to evaluate the difference ofROM before and after pitching. A significance level of P <.01 was adopted to control for type I error. All statisticalanalyses were performed using SPSS 10.0 (SPSS ScienceInc, Chicago, Ill).
Figure 4. Passive elbow extension range of motion.
Figure 3. Passive elbow flexion range of motion.
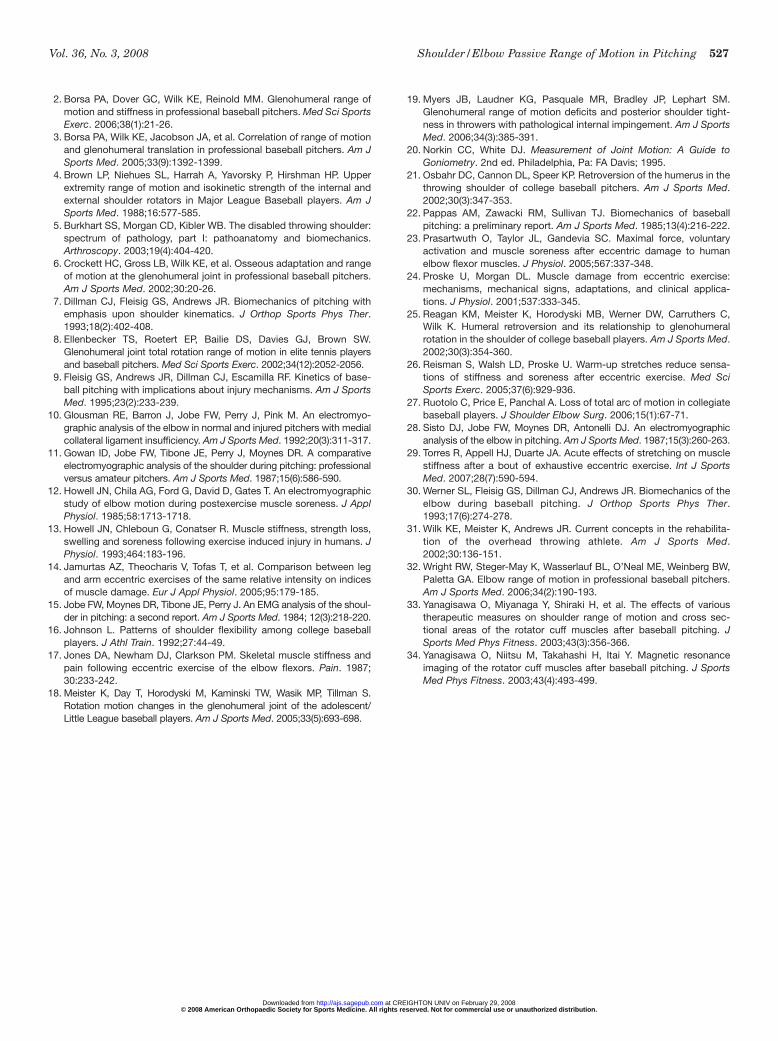
TABLE 1Range of Motion Before, After, and 24 Hours After
Pitching in the Dominant Arma
24 Hours P for Before After After ANOVA
ShoulderER 136.5 ± 9.8 135.3 ± 9.3 136.5 ± 9.0 .213IR 54.1 ± 11.4 44.6 ± 11.9b 46.5 ± 10.0b <.001b
TM 190.6 ± 14.6 179.9 ± 13.7b 182.9 ± 11.5b <.001b
ElbowFlexion 144.9 ± 7.1 144.7 ± 5.9 145.8 ± 5.8 .264Extension –5.1 ± 9.5 –8.3 ± 8.8b –7.7 ± 8.9b <.001b
aData are mean degrees ± SD. ANOVA, analysis of variance; ER,external rotation; IR, internal rotation; TM, total motion.
bSignificantly different than before throwing (P < .01).
TABLE 2Range of Motion Before and After Pitching in the
Nondominant Arma
P for Paired-Before After Samples t Test
ShoulderER 124.2 ± 9.1 125.3 ± 8.6 .320IR 63.1 ± 14.3 63.5 ± 13.1 .712TM 187.3 ± 16.9 188.8 ± 17.3 .339
ElbowFlexion 146.5 ± 6.8 146.3 ± 5.8 .715Extension 2.2 ± 5.2 1.6 ± 5.5 .212
aData are mean degrees ± SD. ER, external rotation; IR, internalrotation; TM, total motion.
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from

526 Reinold et al The American Journal of Sports Medicine
RESULTS
The results for the dominant and nondominant shouldercan be found in Tables 1 and 2, respectively. There was asignificant reduction (P < .001) in dominant shoulder IR(–9.5°), total motion (–10.7°), and elbow extension (–3.2°)after pitching that remained present at 24 hours afterpitching. No statistically significant differences wereobserved on the nondominant shoulder.
DISCUSSION
It is well recognized and reported that ROM adaptationsare normal in the overhead throwing athlete. However, theprecise cause of this adaptation has not been established.Numerous theories regarding the altered ROM patternobserved in overhead throwing athletes have beenreported.1-3,5,6,18,19,21,25,31 Several authors have documentedhumeral retroversion in the thrower’s shoulder and attrib-ute the altered ROM to bony adaptations.6,21,25 Someauthors have theorized that the excessive ER and limitedIR are due to anterior capsular laxity and posterior cap-sule tightness,5 although no clinical studies to date haveshown this to be present. This theory of posterior capsulartightness has come into question from other researcherswho have identified that ROM in baseball pitchers, specif-ically a loss of IR, does not correlate with an alteration inposterior glenohumeral translation.2,3
Anecdotally, it is the authors’ experience that baseballplayers often describe generalized tightness in the muscu-lature of their posterior shoulders and elbow flexors afterpitching. The muscles responsible for ER of the shoulderand flexion of the elbow exhibit high eccentric muscleactivity10,11,15,28 during the throwing motion as the shoul-der internally rotates between 6000 and 7000 deg/s7,9,22
and the elbow extends between 2000 and 5000 deg/s.9,30
Furthermore, Yanagisawa et al34 have shown long-lastingincreased signal on T2-weighted MRIs of the supraspina-tus, infraspinatus, and teres minor muscles after baseballpitching. The authors attribute these findings to muscledamage that resulted from eccentric muscle contractions.
Previous studies examining the effect of repetitive eccen-tric contractions have shown a subsequent loss of joint ROMin both the upper and lower extremities after testing.14,23,26
There are several postulated theories regarding this phe-nomenon, including a stretch-activated release of Ca2+ inmuscle fibers,13 shortening of parallel noncontractile ele-ments in the muscle,12,17 and a loss of motion due to aneccentric induced local inflammatory response and soft-tissue edema exerting strain on perimysial and epimysialconnective tissue elements.13 Regardless of the mechanism,eccentric muscular contractions have been correlated to arise in passive muscular tension and a loss of joint ROM.24
The results of the current study show a significant reduc-tion in the amount of shoulder IR, total motion, and elbowextension ROM immediately after pitching. Although ROMwas beginning to show a trend toward returning to baselinevalues, this significantly altered motion was still present 24hours after pitching. These motions all involved high levelsof eccentric muscle activity during pitching compared with
the motions of shoulder ER and elbow flexion, which did notdemonstrate changes in ROM after pitching. These findingsmay suggest that the altered ROM characteristics in base-ball pitchers may be at least partially explained by adapta-tions of the soft-tissue musculature due to the high level ofeccentric contractions observed during pitching, in additionto potential underlying bony or capsular adaptations.
Recently, reports have shown that baseball pitchers withdocumented rotator cuff internal impingement and painfulshoulders exhibit decreased IR in their total motion arcs.19,27
Based on the results of these studies, as well as the resultsof the current study, we hypothesize that although an acutedecrease in ROM may be a normal physiological response,baseball pitchers may be more susceptible to shoulder injuryif they continue to pitch with decreased IR and total motion.The cumulative effects of eccentric microtrauma in the base-ball pitcher may contribute to the pathological loss of shoul-der IR and elbow extension ROM.
Clinically, acute static stretching after eccentric muscleactivity has been shown to minimize loss of ROM.29 Thus,therapeutic techniques for injury prevention, such as stretch-ing,26,29 light shoulder exercise,33 and ice,33 may be performedin an attempt to restore the athlete’s normal or preactivityROM before having to pitch again. Future studies should beperformed to prospectively assess this hypothesis.
Our ROM methods, including the use of a customized bub-ble goniometer, have shown good intratester reliability(0.8115-0.9740). Furthermore, because of the inherent SD ofmeasurement associated with goniometry, we also usedstrict criteria to define significant results (P < .01) to mini-mize the chance of a type I statistical error. Testing was notperformed during game situations. Although the currentstudy demonstrated that ROM continues to be reduced at 24hours after pitching, other authors have documented alteredmotion patterns of the upper and lower extremities for up to4 days after various eccentric activities.13,14 Although base-ball players often pitch with 24 hours of rest (relief pitchersdo this routinely; starting pitchers may not compete everyday yet often throw daily), future studies should continue toexplore the duration of altered ROM after pitching, with andwithout therapeutic intervention.
CONCLUSION
The primary findings of the current study were that shoul-der IR, total motion, and elbow extension ROM are signif-icantly reduced immediately after baseball pitching. Thisdecrease in ROM continued to be present 24 hours afterpitching. The altered ROM corresponds with the musclegroups that show high eccentric activity during the act ofpitching. This suggests that the altered ROM characteris-tics in baseball pitchers may be at least partially explainedby soft-tissue musculotendinous adaptations due to muscledamage after eccentric contractions.
REFERENCES
1. Bigliani LU, Codd TP, Connor PM, Levine WN, Littlefield MA, HersonSJ. Shoulder motion and laxity in the professional baseball player. AmJ Sports Med. 1997;25:609-613.
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from
Vol. 36, No. 3, 2008 Shoulder/Elbow Passive Range of Motion in Pitching 527
2. Borsa PA, Dover GC, Wilk KE, Reinold MM. Glenohumeral range ofmotion and stiffness in professional baseball pitchers. Med Sci SportsExerc. 2006;38(1):21-26.
3. Borsa PA, Wilk KE, Jacobson JA, et al. Correlation of range of motionand glenohumeral translation in professional baseball pitchers. Am JSports Med. 2005;33(9):1392-1399.
4. Brown LP, Niehues SL, Harrah A, Yavorsky P, Hirshman HP. Upperextremity range of motion and isokinetic strength of the internal andexternal shoulder rotators in Major League Baseball players. Am JSports Med. 1988;16:577-585.
5. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder:spectrum of pathology, part I: pathoanatomy and biomechanics.Arthroscopy. 2003;19(4):404-420.
6. Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and rangeof motion at the glenohumeral joint in professional baseball pitchers.Am J Sports Med. 2002;30:20-26.
7. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching withemphasis upon shoulder kinematics. J Orthop Sports Phys Ther.1993;18(2):402-408.
8. Ellenbecker TS, Roetert EP, Bailie DS, Davies GJ, Brown SW.Glenohumeral joint total rotation range of motion in elite tennis playersand baseball pitchers. Med Sci Sports Exerc. 2002;34(12):2052-2056.
9. Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of base-ball pitching with implications about injury mechanisms. Am J SportsMed. 1995;23(2):233-239.
10. Glousman RE, Barron J, Jobe FW, Perry J, Pink M. An electromyo-graphic analysis of the elbow in normal and injured pitchers with medialcollateral ligament insufficiency. Am J Sports Med. 1992;20(3):311-317.
11. Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparativeelectromyographic analysis of the shoulder during pitching: professionalversus amateur pitchers. Am J Sports Med. 1987;15(6):586-590.
12. Howell JN, Chila AG, Ford G, David D, Gates T. An electromyographicstudy of elbow motion during postexercise muscle soreness. J ApplPhysiol. 1985;58:1713-1718.
13. Howell JN, Chleboun G, Conatser R. Muscle stiffness, strength loss,swelling and soreness following exercise induced injury in humans. JPhysiol. 1993;464:183-196.
14. Jamurtas AZ, Theocharis V, Tofas T, et al. Comparison between legand arm eccentric exercises of the same relative intensity on indicesof muscle damage. Eur J Appl Physiol. 2005;95:179-185.
15. Jobe FW, Moynes DR, Tibone JE, Perry J. An EMG analysis of the shoul-der in pitching: a second report. Am J Sports Med. 1984; 12(3):218-220.
16. Johnson L. Patterns of shoulder flexibility among college baseballplayers. J Athl Train. 1992;27:44-49.
17. Jones DA, Newham DJ, Clarkson PM. Skeletal muscle stiffness andpain following eccentric exercise of the elbow flexors. Pain. 1987;30:233-242.
18. Meister K, Day T, Horodyski M, Kaminski TW, Wasik MP, Tillman S.Rotation motion changes in the glenohumeral joint of the adolescent/Little League baseball players. Am J Sports Med. 2005;33(5):693-698.
19. Myers JB, Laudner KG, Pasquale MR, Bradley JP, Lephart SM.Glenohumeral range of motion deficits and posterior shoulder tight-ness in throwers with pathological internal impingement. Am J SportsMed. 2006;34(3):385-391.
20. Norkin CC, White DJ. Measurement of Joint Motion: A Guide toGoniometry. 2nd ed. Philadelphia, Pa: FA Davis; 1995.
21. Osbahr DC, Cannon DL, Speer KP. Retroversion of the humerus in thethrowing shoulder of college baseball pitchers. Am J Sports Med.2002;30(3):347-353.
22. Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseballpitching: a preliminary report. Am J Sports Med. 1985;13(4):216-222.
23. Prasartwuth O, Taylor JL, Gandevia SC. Maximal force, voluntaryactivation and muscle soreness after eccentric damage to humanelbow flexor muscles. J Physiol. 2005;567:337-348.
24. Proske U, Morgan DL. Muscle damage from eccentric exercise:mechanisms, mechanical signs, adaptations, and clinical applica-tions. J Physiol. 2001;537:333-345.
25. Reagan KM, Meister K, Horodyski MB, Werner DW, Carruthers C,Wilk K. Humeral retroversion and its relationship to glenohumeralrotation in the shoulder of college baseball players. Am J Sports Med.2002;30(3):354-360.
26. Reisman S, Walsh LD, Proske U. Warm-up stretches reduce sensa-tions of stiffness and soreness after eccentric exercise. Med SciSports Exerc. 2005;37(6):929-936.
27. Ruotolo C, Price E, Panchal A. Loss of total arc of motion in collegiatebaseball players. J Shoulder Elbow Surg. 2006;15(1):67-71.
28. Sisto DJ, Jobe FW, Moynes DR, Antonelli DJ. An electromyographicanalysis of the elbow in pitching. Am J Sports Med. 1987;15(3):260-263.
29. Torres R, Appell HJ, Duarte JA. Acute effects of stretching on musclestiffness after a bout of exhaustive eccentric exercise. Int J SportsMed. 2007;28(7):590-594.
30. Werner SL, Fleisig GS, Dillman CJ, Andrews JR. Biomechanics of theelbow during baseball pitching. J Orthop Sports Phys Ther.1993;17(6):274-278.
31. Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilita-tion of the overhead throwing athlete. Am J Sports Med.2002;30:136-151.
32. Wright RW, Steger-May K, Wasserlauf BL, O’Neal ME, Weinberg BW,Paletta GA. Elbow range of motion in professional baseball pitchers.Am J Sports Med. 2006;34(2):190-193.
33. Yanagisawa O, Miyanaga Y, Shiraki H, et al. The effects of varioustherapeutic measures on shoulder range of motion and cross sec-tional areas of the rotator cuff muscles after baseball pitching. JSports Med Phys Fitness. 2003;43(3):356-366.
34. Yanagisawa O, Niitsu M, Takahashi H, Itai Y. Magnetic resonanceimaging of the rotator cuff muscles after baseball pitching. J SportsMed Phys Fitness. 2003;43(4):493-499.
© 2008 American Orthopaedic Society for Sports Medicine. All rights reserved. Not for commercial use or unauthorized distribution. at CREIGHTON UNIV on February 29, 2008 http://ajs.sagepub.comDownloaded from