Embed Size (px)
Citation preview

doi:10.1152/jn.01091.2012 112:1447-1456, 2014. First published 11 June 2014;J NeurophysiolSuresh and William Zev RymerAneesha K. Suresh, Xiaogang Hu, Randall K. Powers, C. J. Heckman, Nina L.duration in stroke survivorsChanges in motoneuron afterhyperpolarization
You might find this additional info useful...
25 articles, 15 of which can be accessed free at:This article cites /content/112/6/1447.full.html#ref-list-1
including high resolution figures, can be found at:Updated information and services /content/112/6/1447.full.html
can be found at:Journal of Neurophysiologyabout Additional material and information http://www.the-aps.org/publications/jn
This information is current as of November 3, 2014.
American Physiological Society. ISSN: 0022-3077, ESSN: 1522-1598. Visit our website at http://www.the-aps.org/.(monthly) by the American Physiological Society, 9650 Rockville Pike, Bethesda MD 20814-3991. Copyright © 2014 by the
publishes original articles on the function of the nervous system. It is published 12 times a yearJournal of Neurophysiology
on Novem
ber 3, 2014D
ownloaded from
on Novem
ber 3, 2014D
ownloaded from

Changes in motoneuron afterhyperpolarization duration in stroke survivors
Aneesha K. Suresh,1 Xiaogang Hu,1 Randall K. Powers,2 C. J. Heckman,3,4,5 Nina L. Suresh,1
and William Zev Rymer3,4,6
1Sensory Motor Performance Program, Rehabilitation Institute of Chicago, Chicago, Illinois; 2Department of Physiology andBiophysics, University of Washington, Seattle, Washington; 3Department of Physical Medicine and Rehabilitation, FeinbergSchool of Medicine, Northwestern University, Chicago, Illinois; 4Department of Physical Therapy and Human MovementSciences, Northwestern University, Chicago, Illinois; 5Department of Physiology, Northwestern University, Chicago, Illinois;and 6Department of Biomedical Engineering, Northwestern University, Chicago, Illinois
Submitted 19 December 2012; accepted in final form 9 June 2014
Suresh AK, Hu X, Powers RK, Heckman CJ, Suresh NL,Rymer WZ. Changes in motoneuron afterhyperpolarization durationin stroke survivors. J Neurophysiol 112: 1447–1456, 2014. Firstpublished June 11, 2014; doi:10.1152/jn.01091.2012.—Hemisphericbrain injury resulting from a stroke is often accompanied by muscleweakness in limbs contralateral to the lesion. In the present study, weinvestigated whether weakness in contralesional hand muscle instroke survivors is partially attributable to alterations in motor unitactivation, including alterations in firing rate modulation range. Theafterhyperpolarization (AHP) potential of a motoneuron is a primarydeterminant of motoneuron firing rate. We examined differences inAHP duration in motoneurons innervating paretic and less impaired(contralateral) limb muscles of hemiparetic stroke survivors as well asin control subjects. A novel surface EMG (sEMG) electrode was usedto record motor units from the first dorsal interosseous muscle. ThesEMG data were subsequently decomposed to derive single-motorunit events, which were then utilized to produce interval (ISI) histo-grams of the motoneuron discharges. A modified version of intervaldeath rate (IDR) analysis was used to estimate AHP duration. Resultsfrom data analyses performed on both arms of 11 stroke subjects andin 7 age-matched control subjects suggest that AHP duration issignificantly longer for motor units innervating paretic muscle com-pared with units in contralateral muscles and in units of intactsubjects. These results were supported by a coefficient of variation(CV) analysis showing that paretic motor unit discharges have a lowerCV than either contralateral or control units. This study suggests thatafter stroke biophysical changes occur at the motoneuron level,potentially contributing to lower firing rates and potentially leading toless efficient force production in paretic muscles.
motor units; first dorsal interosseous; afterhyperpolarization; paresis;stroke
ONE OF THE MOST COMMON MOTOR impairments after stroke isparesis, or weakness for voluntary movement. While progres-sive changes in mechanical properties of paretic muscles, suchas muscle atrophy, metabolic changes, and connective tissueinfiltration, are prevalent and could contribute to paresis,changes at the spinal neuronal level may contribute as well.Indeed, understanding potential changes in the properties andcontrol of motoneurons could offer further insight into mech-anisms that may contribute to muscle weakness after stroke.Accordingly, our objective in this study is to assess the poten-tial contributions of changes in motoneuron properties to mus-cle weakness observed in many stroke survivors.
Earlier electrophysiological studies in stroke survivors havereported reductions of motor unit (MU) number, fibrillationand sharp waves, reduced compound muscle action potential(M wave) amplitude, and lower firing rates in motoneurons ofparetic muscles (Brown and Snow 1990; Dattola et al. 1993;Gemperline et al. 1995; McComas et al. 1973; Spaans andWilts 1982). Gemperline et al. (1995) reported lowered MUdischarge rates recorded from paretic biceps muscles of strokesurvivors compared with contralateral muscles at the sameforce level. While reduced firing rates could be a function ofdiminished descending drive following a cerebral lesion,changes in the electrical properties of the motoneuron couldalso contribute to the reduced MU firing rates (Gemperline etal. 1995).
The goal of the present study was to determine whetherchanges in a specific motoneuron property, the postspike afte-rhyperpolarization (AHP), contribute to the observed reduc-tions in mean firing rates. The AHP is a primary determinant ofmotoneuron firing rate, and any increase in its duration oramplitude could alter MU firing behaviors (Bakels and Kernell1993). The relative variability of discharge in motoneurons isdependent upon both the AHP size and time course, as well asthe amplitude and frequency content of concurrent synapticnoise. While statistical methods have been used to estimate theAHP duration in neurologically intact human subjects (Gossenet al. 2003; MacDonell et al. 2007; Matthews 1996, 2002),sparse data exist in stroke survivors. As of yet, no study hasperformed a systematic comparison between the paretic andcontralateral sides of stroke survivors in upper limbs (Ivanovaet al. 2014).
Currently, two methods of estimating AHP duration inhumans exist: interval death rate (IDR) analysis (Matthews1996) and variability analysis of interspike intervals (ISIs)(Piotrkiewicz 1999). Both methods have been validatedthrough animal models (Powers and Binder 2000). A study inwhich variability analysis compared average AHP duration ofMUs in biceps brachii between poststroke patients and healthycontrol subjects reported a lengthened AHP duration aftercerebral stroke (Liang et al. 2010). However, as the authorsstate, comparison of ISI variability between groups may havebeen confounded by a difference in spike generating modes:rhythmic firing mode (short interval range) versus occasionalspike mode (long interval range) (Calvin 1974). Rhythmicfiring mode is composed of spikes that fire regularly, usually inthe faster range of firing rates for a given MU. Occasionalspike mode is composed of spikes that fire irregularly, usually
Address for reprint requests and other correspondence: A. K. Suresh, SensoryMotor Performance Program, Rehabilitation Inst. of Chicago, 345 E Superior St.,Rm. 1378, Chicago, IL 60611 (e-mail: [email protected]).
J Neurophysiol 112: 1447–1456, 2014.First published June 11, 2014; doi:10.1152/jn.01091.2012.
14470022-3077/14 Copyright © 2014 the American Physiological Societywww.jn.org
on Novem
ber 3, 2014D
ownloaded from

in the slowest range of firing rates for a given MU. Resultsfrom this study also indicate that interval variability is signif-icantly different in paretic limbs compared with contralateral orcontrol limbs, suggesting that measuring AHP through vari-ability analysis may not be accurate.
Accordingly, the objective of our study was to assess AHPduration systematically, utilizing a modification of the IDRanalysis method during similar MU firing modes (Zijdewindand Thomas 2012), and to compare the results obtained fromparetic, nonparetic (contralateral), and control muscles. Todetermine whether distal limb muscles exhibit alterations inmotoneuron biophysical properties, we collected EMG datawith a novel, noninvasive surface electromyography (sEMG)sensor array (Delsys) from the first dorsal interosseous (FDI).The results of our study suggest that motoneuron/MU record-ings obtained from distal paretic muscles display significantlylonger AHP durations compared with contralateral muscles ofstroke survivors as well as comparable muscles in neurologi-cally intact persons.
METHODS
Subjects
Eleven chronic hemiparetic stroke subjects with moderate to severeweakness of the contralesional extremities were tested (see Table 1).The subjects were recruited from the outpatient clinics of the Reha-bilitation Institute of Chicago. Seven age-matched control subjectswere recruited as well. All participants gave informed consent viaprotocols approved by the Institutional Review Board at NorthwesternUniversity.
Stroke participants. Stroke participants were adults who had sus-tained a hemiparetic stroke at least 6 mo prior to experimental testing.We evaluated the ability of the participants to complete the specifiedfinger tasks as well as the ability to attain and maintain the experi-mental sitting posture and arm position, using several clinical assess-ment scales including the Fugl-Meyer scale and the Chedoke-McMas-ter hand assessment scale. A research physical therapist performed theclinical evaluation on both sides of our hemiparetic stroke subjects.
Neurologically intact participants. Our neurologically intact sub-jects were, on average, age matched to our stroke survivors. A clinicalassessment of our intact subjects was performed by the researchphysical therapist to affirm the lack of neurological impairment and/ormotor deficits.
Experimental Setup
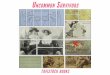
Study participants were seated upright in a Biodex chair with theirupper arm comfortably resting on a plastic support. To help standard-ize hand position as well as to minimize activity of unrecordedmuscles, the forearm was casted and placed in a ring-mount interfaceattached to an elbow rest; this rest was securely mounted withmagnetic stands to a heavy steel table. The right shoulder was placedin 45° of abduction and neutral rotation, the elbow in 60° of flexion,and the forearm in full pronation, and the wrist was held neutral withrespect to flexion/extension. The third through fifth digits were com-fortably splayed and strapped to the support surface. The first digitwas secured at a 45° angle to the second digit. The second digit wasplaced in line with the second metacarpal and the long axis of theforearm, creating a 0° or neutral (abduction/adduction) metacarpopha-langeal (MCP) joint angle. The proximal phalanx of the second digitwas cast and fixed to a ring-mount interface attached to a sixdegrees-of-freedom load cell (JR3, ATI) (Fig. 1A). The recordedforces from the x (abduction/adduction) direction were low-passfiltered (cutoff � 200 Hz) and digitized at a sampling frequency of 1kHz.
MU discharges from the FDI muscle were derived from a sEMGrecording using a surface sensor array (Delsys) as shown in Fig. 1B.The sensor consists of five slender cylindrical probes, located at thecorners and at the center of a 5 � 5-mm square (Fig. 1C). Pairwisedifferentiation of the five electrodes yields four channels of sEMGsignals (Fig. 1D). The sEMG sensor and a reference electrode wereconnected to four channels of a Delsys Bagnoli sEMG system. Thesignals were amplified and filtered with a bandwidth of 20–2,000 Hz.The signals were sampled at 20 kHz.
Procedures
Upon completion of the experimental setup, the subjects wereinstructed to perform a very small isometric abduction task with theirindex finger. MU recruitment was monitored both visually on acomputer screen and with auditory feedback from an analog speakerby the experimenter. Once a single unit was audibly and visuallyidentified, the participants were requested to maintain a relativelystable firing rate of a single MU at the lowest possible rate in order toensure that the ISI histogram included intervals longer than the AHPduration (see Data Analysis for further explanation). The subject wasgiven both visual and audio feedback of MU firings. To identify thelowest regular firing frequency for the MU, the subject was asked toincrease and decrease the level of effort until a sustained low rate offiring was achieved, and was then requested to maintain that unit firingat that rate for as long as possible. During this period, we alsomonitored for fatigue, by querying the subject as well as by monitor-ing the EMG signal. We monitored the EMG signal by ensuring thatthe isolated unit remained at a relatively stable firing rate and thatadditional units were not being recruited to maintain the same level ofeffort. The data for each MU were collected over several trials,allowing the subject to rest between trials.
All four sEMG channels as well as the force signal were monitoredonline via Spike2 (Cambridge Electronic Design) and subsequentlystored for processing. A minimum of four MUs were collected fromeach of the paretic and contralateral sides. Most stroke subjects weretested on both sides with the same protocol during one session, withthe paretic muscle tested first. Two subjects (subjects 1 and 5) weretested on separate days. The same protocol was repeated on arandomly selected side of control subjects.
Data Analysis
Spike2 was used to decompose and classify MUs with a templatematching algorithm based on amplitude and shape characteristics. ThesEMG trials were selected for further analysis on the basis of the
Table 1. Demographic information for stroke subjects
ID Sex Age, yrTime SinceStroke, yr FT C
PareticSide
1 M 46 13 24 3 L2 M 61 4 63 6 R3 F 53 3 63 7 R4 M 65 17 17 2 R5 M 66 9 16 4 L6 F 63 16 17 2 L7 F 58 5 38 4 R8 M 57 8 63 5 R9 F 58 5 56 4 R
10 F 59 23 22 2 R11 F 68 5 66 7 R
FT, arm motor Fugl-Meyer motor assessment (X/66); C, Chedoke-McMas-ter stroke assessment (hand).
1448 AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

following criteria: 1) �1,000 spikes were generated for a single MUand 2) the instantaneous firing rate variability during the steady-stateforce had a standard deviation (SD) of �0.5 pps.
Trains of single-MU action potentials were further analyzed inorder to compute the AHP duration estimates with a modified IDR
method (Matthews 1996) with code written in MATLAB (Math-Works). The modified IDR method is as follows.
As described by Matthews et al., in order to compensate for thelength of recordings as well as the high spike variability associatedwith low firing rates, each spike train was parsed into subpopulations
Fig. 1. Experimental setup, surface sensor array, surface EMG (sEMG) signals, and force display. A: brace and cast used to ensure that index finger was alignedwith the long axis of the forearm. B: placement of Delsys sensor array on first dorsal interosseous (FDI) muscle. C: 5 cylindrical probes of the sensor array locatedat the corners and center of a 5 � 5-mm square. D: pairwise differentiation of the 5 electrodes allows for 4 channels of sEMG signals.
1449AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

to ensure that ISI histograms represented a specific firing range. Eachspike train was divided into subpopulations derived from segmentsthat were spliced together based on a similar running mean firing rate,which was determined by averaging five spikes before and five spikesafter a targeted spike (Matthews 1996). The resulting interval histo-gram of the subpopulation of spikes was then generated based oninstantaneous intervals. Interval histograms (5-ms bins) thereby rep-resented a distinct mean firing rate distribution for a given MU.Changing bin size has two opposing effects on estimation accuracy.Increasing bin size reduces noise but also reduces resolution. Bin sizesof 5 ms are conventionally used for IDR analysis. All ISI histogramsthat consisted of at least 1,000 intervals (mean: 1,583 intervals, SD:521) were used for further analysis. ISI death rates were then calcu-lated, representing the probability (P) that a MU discharge willterminate a given ISI. The calculation of P is described by thefollowing equation:
P �
�ln�N0
N1��
bin width(1)
N0 is the sum of following bins in the interval histogram, includingthe bin whose P is being measured, and N1 is the sum of all followingbins excluding the bin whose P is being measured. The value P hasalso been called the interval death rate (IDR; Matthews 1996) becauseit represents the probability of a spike occurring (i.e., the interval“dying”) as a function of time from the previous spike. The final IDRplot eliminates the last 5% of P values, since the equation divergesquickly when remaining bin numbers are low.
To assess AHP duration, the interval at which the IDR plot reachesa clear “plateau” was determined. The probability of a spike occurringat short intervals is very low, because of the greater membranehyperpolarization and increased conductance due to the AHP. As theAHP decays, spike probability increases monotonically until itreaches a plateau at the completion of the AHP. Identification of theplateau phase is important because the start of the IDR plot plateaurepresents the time in the postspike interval after which the probabilityof spike occurrence is independent of the latency since the previousspike, and thus represents the time after which the AHP has con-cluded. The death rate plot terminates growth at the completion of theAHP because the membrane potential reaches a “steady state,” wherethe AHP no longer affects the probability of spike initiation (Mat-thews 1996; Zijdewind and Thomas 2012). Since IDR plots areconstrained by finite interval bins, the “plateau” period is oftencharacterized by erratic behavior resulting from low bin counts, wherevalues substantially deviate from the initial smooth trajectory of theIDR (Fig. 2).
As Fig. 2 indicates, this region can be readily identified by the pointat which the slope of the plot (qualitatively) reaches a mean of zero.To quantitatively estimate the beginning of the plateau region, theAHP termination interval was determined by performing a piecewiselinear regression fit to the trajectory of the IDR.
Control subject AHP estimates were calculated with modified IDRanalysis as well as ISI variability analysis. ISI variability analysisutilizes similar firing rate data and determines AHP duration throughthe relationship between mean interval and SD. AHP duration isquantified by the “turning interval,” which is where the SD substan-tially increases with mean interval (Piotrkiewicz et al. 2007; Powersand Binder 2000).
The Wilcoxon rank test was used to determine whether controlAHP estimate results were significantly different between ISI vari-ability analysis and modified IDR analysis. A previous study confirmsthat AHP estimate durations derived from modified IDR analysis andISI variability analysis are significantly correlated with each other(Zijdewind and Thomas 2012).
Additionally, we tested MUs from two control subjects to ensurethat AHP estimates did not change significantly with MU firing rate.Subjects were asked to hold steady firing of one MU over threedifferent firing rates. Modified IDR analysis was then performed onthese three separate recording trains to ensure that the AHP estimateswere independent of firing rate.
Statistical analysis. Paired t-tests were used to determine whetherAHP estimates and firing rates were significantly different betweenparetic and contralateral sides within subjects. Analysis of variance(ANOVA) with Bonferroni’s correction for multiple comparisons wasused to compare mean AHP estimate durations as well as mean firingrates among paretic, contralateral, and control MU populations.
MU trials were subsequently parsed into short 20- to 25-s trains andthen selected for further coefficient of variation (CV) analysis on thebasis of the following criteria: 1) �200 consecutive spikes weregenerated for a single MU; 2) the ISI train was determined to benormally distributed by the Lillifors test along with visualization ofthe ISI interval histogram; and 3) firing rates of each MU sample werewithin the range of 6–9 pps. With these three criteria, the data wereassumed to be stationary with sufficient samples to perform higher-order statistics on each MU train. Detailed explanations of thisanalysis are found in a previous study by Andreassen and Rosenfalck(1980).
Thus only subgroups of MUs between all subjects for both thecontralateral and paretic sides were used for CV analysis. This is dueto the fact that the CV is a function of MU firing rate and only MUsthat demonstrated a firing rate of 6–9 pps (for at least 20–25 s) wereused for the calculation of CV. We chose 6–9 pps because this rangeallowed for the most inclusive representation of both contralateral andparetic MUs. Smaller samples from the original longer spike trains (upto 600 s) were taken since the long spike trains were usually nonsta-tionary and a stationary train of consecutive MU spikes is necessaryfor a CV analysis.
The CV was calculated, in order to assess normalized variability,with the following equation:
CV �SD�ISI�
Mean�ISI�� 100% (2)
ANOVA with Bonferroni’s correction for multiple comparisons wasused to determine whether mean CV values were significantly differ-ent among paretic, contralateral, and control MUs.
Linear regression analysis was performed on contralateral-to-pa-retic ratios of AHP estimates and firing rates. Additionally, linearregression analysis was performed on AHP estimates versus CV forcontralateral and paretic groups. To determine whether the regressionline between paretic and contralateral groups significantly differed, ananalysis of covariance (ANCOVA) was performed.
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
50 60 70 80 90 100 110 120 130
Dea
th R
ate
(%/m
s)
Time (ms)Fig. 2. Sample interval death rate plot from subject 3 (contralateral side); arrowindicates beginning of plateau phase and measure of afterhyperpolarization(AHP) duration. The estimate, or “termination interval,” is marked by theintersection of 2 fitted lines that provide the summed least-squares error. Anoperator indicates the intervals on which the piecewise linear regression isperformed due to the fact that the equation diverges quickly when remainingbin numbers are low. Dashed lines show piecewise linear regression results andcorresponding intersection of the 2 lines.
1450 AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

RESULTS
The objective of our study was to investigate whether theestimated duration of the AHP potential, a primary determinantof motoneuronal firing rate, was greater in MUs recorded fromcontralesional muscle of stroke survivors than in MUs drawnfrom the equivalent ipsilesional limb muscle. MU data col-lected from sEMG recordings of the FDI muscles of 11hemiparetic stroke subjects were analyzed using the modifiedIDR method. A total of 48 MUs were collected from thecontralateral side of 11 stroke survivors and 56 MUs from theparetic side of stroke survivors. Twenty-four MUs in total werecollected from seven control subjects. However, because of therequirements of the data analysis method, only 36 contralateralMUs, 39 paretic MUs, and 18 control MUs were furtheranalyzed for AHP duration estimation (all further reporting ison these subsets of units). The limiting factor in including aMU for AHP estimation utilizing the IDR method is that theanalysis is only valid on MUs with firing rate characteristicsthat exhibit a “plateau” in the IDR plot or an exponential decayin the ISI histogram. The rationale is that these features willonly emerge for firing rates of MUs for which the interval islargely governed by the AHP, which is generally true only atvery low discharge rates.
Subjects attempted to keep a single unit active for as long aspossible; MU recordings of �250 s were not used for furtheranalysis because of the low number of ISIs. The range ofrecording lengths for MUs retained for further analysis was ofthe order of 250–600 s. An average of 1,583 intervals wascollected from each single-unit recording train.
Contralateral and Paretic AHP Estimates Using ModifiedIDR Analysis
A comparison of AHP duration estimates for each strokesubject was performed with matched pairs, where computedestimates from single MUs were averaged from MUs derivedfrom each side separately. Matched-pairs comparisons wereperformed between the paretic and contralateral sides withinone subject, because of the heterogeneous nature of the strokepopulation. Our results show that, on average, the estimatedAHP duration was significantly longer in MUs recorded on theparetic side compared with the contralateral side (P � 0.05).Shown in Fig. 3 are sample interval histograms as well as IDRplots from one paretic unit and one contralateral unit from asingle subject, illustrating the differences in mean AHP dura-tion. The estimated AHP duration was 105 ms for the MU fromthe contralateral side versus 163 ms for the MU from theparetic side.
Figure 4 summarizes our results from all tested subjects.AHP duration values are obtained by averaging all the AHPestimates for all MUs (range of 2–6) collected for each subjectfor each side (paretic or contralateral) separately. We foundthat for 10 of the 11 tested subjects the average AHP durationestimate derived from the paretic side was longer than theaverage AHP duration estimate derived from the contralateralside (Fig. 4).
To ensure that parametric statistics were valid for thesecomparisons, the Lilliefors goodness-of-fit test was applied toAHP estimates of both sides. Our analysis shows that theestimates of AHP from both the paretic and contralateral sidesfollow an approximately normal distribution (P � 0.05). These
results indicate that a paired t-test is a valid statistical test forassessment of significant differences in AHP duration esti-mates between the two sides of a stroke subject.
AHP Estimates and Firing Rate of Control Subjects
All stroke subject data were pooled in order to analyzedifferences with age-matched control subjects. Comparisons ofmean AHP estimates as well as mean firing rates were per-formed with an ANOVA with Bonferroni’s correction formultiple comparisons between control MUs (18), contralateralMUs (36), and paretic MUs (39).
When compared at the � � 0.05 level, our results show thatAHP duration estimates were significantly shorter in controlMUs (mean: 125 ms; SD: 22 ms) compared with paretic MUs(mean: 147 ms; SD: 29 ms) as well as between contralateral(mean: 116 ms; SD: 27 ms) and contralesional “paretic” MUs.There were no significant differences in AHP duration esti-mates between control MUs and contralateral MUs. Results forMU mean firing rates also showed the same trend, in that therewere significant differences in mean MU firing rates for com-parisons made between contralateral (mean: 9.4 pps; SD: 2.0pps) and paretic (mean: 7.11 pps; SD: 1.2 pps) MUs as well as
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
50 100 150 200
Dea
th R
ate
(%/m
s)
Time Since Spike (ms)
Contralateral
Paretic
50 100 150 200 2500
20
40
60
80
100
120
Interval (ms)
Cou
nt
PareticContralateral
A
B
Fig. 3. Subject 1. A: interval histogram of spike train from a contralateral singlemotor unit (MU) and paretic single MU. B: corresponding interval death rateplots, with AHP estimate indicated by white triangle. Contralateral unit: meanfiring rate: 9.5 Hz, estimated AHP duration: 105.1 ms. No. of intervals: 1,093.Paretic unit: mean firing rate: 6.7 Hz, estimated AHP duration: 163.3 ms. No.of intervals: 1,044.
1451AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

those between paretic and control MUs (mean: 8.2 pps; SD: 2.1pps).
In contrast, there were no significant differences in firingrates recorded from contralateral versus control MUs. Thesevalues represent averages taken over the entire subject popu-lation. Because of the heterogeneous nature of the strokepopulation, it is difficult to determine limits of high or lowfiring rates. Although we show average firing rates over theentire population of MUs collected, firing rate values varyconsiderably between subjects, as demonstrated in the SDs ofthese measures. As a result, comparisons between the controland paretic sides within each stroke subject better reflectindividual poststroke physiological changes.
Validation of Modified IDR Method
To validate our modified IDR method, we compared AHPduration estimates derived from this method with estimatesderived with the ISI variability analysis (Piotrkiewicz 1999) forthe control subjects only. Using the Wilcoxon paired differencetest (P � 0.511) we found that the AHP duration estimatescomputed with the modified IDR method were not significantlydifferent from estimates computed with the ISI variability
analysis (mean: 120 ms; SD 24 ms). Furthermore, both meth-ods have been validated in animal models, as described in aprevious study (Powers and Binder 2000). Additionally, aprevious study has verified the correlation between the modi-fied IDR method and ISI variability analysis (Zijdewind andThomas 2012). Modified IDR analysis was chosen as thepreferred analysis method for the present study because of theinherent lower MU firing rates exhibited in paretic muscle(Gemperline et al. 1995). For such low firing rates, ISI vari-ability analysis may not offer an accurate comparison of AHPestimates, since the variability of the ISI is strongly influencedby mean interval values (Liang et al. 2010).
Relationship Between AHP Estimates and ClinicalAssessments
We also examined the relationship between our experimen-tally derived parameters in paretic and nonparetic muscle andthe experimental and clinical assessments of weakness. Foreach stroke subject, we computed the ratios between the pareticand contralateral sides for both AHP duration estimates andmean MU firing rates. Maximum voluntary contraction forces(MVCs) were also recorded on the paretic and contralateral
0
50
100
150
200
250
1 2 3 4 5 6 7 8 9 10 11
AH
P D
urat
ion
Estim
ate
(ms)
Subject Number
Contralateral Paretic
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 10 11
Firin
g R
ate
(pps
)
Subject Number
A
B
Fig. 4. Results that illustrate average AHPestimates (A) and firing rates (B) (over 2–6MUs) on the contralateral and paretic sides foreach individual subject. Error bars representSE for each subject. A matched-pairs statisti-cal comparison suggests that contralateralAHP duration estimates were significantly lessthan paretic AHP duration estimates (P �0.05). Contralateral side: subject 1, 4 units;subjects 2–6, 3 units; subject 7, 2 units; sub-ject 8: 5 units; subject 9: 3 units; subject 10, 4units; subject 11, 3 units. Paretic side: subject1, 6 units; subject 2, 3 units; subject 3, 5 units;subject 4, 6 units; subject 5, 6 units; subject 6,3 units; subjects 7–11, 2 units.
1452 AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

side from 8 of 11 subjects, and the force ratio between bothsides was also calculated. Table 2 displays these results foreach subject. The computed MVC ratios did not significantlycorrelate with the computed MU firing rate ratio or AHPduration estimate ratios, and there was no apparent trend.
We then attempted to find correlations between these ratiosderived from experimental measures and the various clinicalmeasures obtained from each subject. Our results show thatAHP estimate ratios and firing rate ratios between paretic andcontralateral MUs did not correlate with clinical assessmentscores (Fugl-Meyer and Chedoke). Overall, the only visibletrend was between the ratios of paretic and contralateral AHPduration estimates and the respective MU firing rates. Figure 5shows that as the ratio between paretic and contralateral firingrate increases, the ratio between paretic and contralateral AHPduration decreases. These data suggest that the longer AHPduration is correlated with lower firing rates in paretic muscle.
Coefficient of Variation
It was reported in earlier reduced animal studies that theAHP acts to reduce the variability of the motoneuronal firingrate (Brownstone et al. 1992; Manuel et al. 2006; Powers andBinder 2000). To determine whether this relation was alsopresent in our human experiments, the relationship betweenAHP duration and the CV of the MU firing rate was investi-gated. With shorter data samples from the long MU trains
acquired for AHP estimation, the spike train CV for MUsderived from both the paretic and contralateral sides wascomputed. Only statistically stationary spike trains can be usedfor CV analysis, and therefore the record length used for thisanalysis was necessarily shorter than that utilized for AHPduration estimation. Because of data analysis requirements (seeMETHODS), a total of 10 single MUs were analyzed from thecontralateral side of eight stroke survivors and 29 single MUsfrom the paretic side, a subset of the MUs used for AHPanalysis. For each single MU, an average of two “trials,” ortwo separate consecutive intervals of �200 counts were ana-lyzed. Seventeen MUs in total were collected from sevencontrol subjects, with an average of two trials per MU. Asdescribed in METHODS, these data were sampled from the originallengthy spike trains of 250–600 s used for AHP duration esti-mates—and represent consecutive spike trains of �20–30 s.
The CV was calculated for all contralateral, paretic, andcontrol MU samples. Results showed that there was a signifi-cant difference between control and paretic units, betweencontralateral and paretic units, as well as between contralateraland control units. CV distributions illustrate that control unitshad the highest CV, followed by contralateral and then pareticunits. Results also show that for all the data, CV decreases asfiring rate (computed over the 25–30 s) increases for a givenMU. As described above, the discharge rate for all analyzedunits was in the range of 6–9 pps. Figure 6 compares therelation between CV and estimated AHP duration for contralat-eral and paretic MUs. This plot shows that as the AHP durationincreases, the CV for the unit decreases.
DISCUSSION
The objective of our study was to assess whether the AHPperiod in human motoneurons, estimated from MU recordings,is longer in MUs recorded from the paretic side of hemipareticstroke survivors compared with MUs from the nonparetic sideof stroke survivors. To achieve this objective, we analyzed datadrawn from long-duration recordings derived from the FDImuscles in both paretic and contralateral limbs. Our goal wasto understand whether lower MU firing rates, often reported inparetic muscles in stroke, were partially attributable to a longeraverage motoneuron AHP duration. To derive such AHP du-ration estimates, we utilized a (novel) modified IDR analysis toestimate AHP duration and a novel, noninvasive surface elec-trode to record MU activity.
Table 2. Ratios of paretic to contralateral values for MVC, firing rate, and AHP estimate
Subject MVC Paretic, N MVC Contralateral, N MVC Ratio Firing Rate Ratio AHP Estimate Ratio
1 14 40 0.35 0.74 1.332 30 39 0.77 0.77 1.283 26 65 0.40 0.69 1.304 N/C N/C N/C 0.78 1.195 6.7 22 0.30 0.80 1.106 13.2 31 0.43 0.67 1.627 N/C N/C N/C 0.62 1.338 17.7 31 0.57 0.99 1.009 N/C N/C N/C 0.90 1.33
10 8.25 37 0.22 0.85 1.0811 13.6 33 0.41 0.85 1.33
Ratio data are ratios of paretic to contralateral values for maximum voluntary contraction force (MVC, N), firing rate (pps), and afterhyperpolarization (AHP)estimate (ms). N/C indicates that data were not collected.
y = -1.06x + 2.07 R² = 0.39
0.0
0.2
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
0.5 0.6 0.7 0.8 0.9 1.0 1.1
AH
P es
timat
es -
Pare
tic:C
ontr
alat
eral
Firing Rate estimates - Paretic: Contralateral
Fig. 5. Relationship between paretic-to-contralateral ratio of AHP estimate vs.firing rate estimate for each subject. Plot shows a negative (slope: �1.06)trend, with an R2 value of 0.388. This plot illustrates that as the ratio betweenparetic and contralateral firing rate increases, the ratio between paretic andcontralateral AHP estimates decreases. Therefore, we can infer that longerAHP durations contribute to the lower firing rates exhibited in paretic MUs.
1453AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

The main result of our study is that in all 11 of ourhemiparetic stroke subjects the estimated mean AHP durationwas significantly longer in MUs from the affected side com-pared with the nonparetic (contralateral) side, and this findingwas upheld in group data comparisons as well. Additionally,the AHP duration estimates were longer in MUs derived fromparetic muscles compared with MUs recorded from neurolog-ically intact controls. No significant differences were observedin comparisons of AHP duration derived from nonparetic(contralateral) MUs with neurologically intact MUs. Our find-ings also show that CV differs significantly among paretic,contralateral, and control units, with the MUs derived from theparetic side exhibiting the lowest CV. The relationship be-tween firing rate and CV differs among these groups as well.
The longer AHP duration estimates on the paretic side areconsistent with findings from an earlier study in which in-creased AHP durations were reported for MUs recorded fromparetic biceps brachii compared with those recorded fromneurologically intact individuals (Piotrkiewicz et al. 2007).Thus it appears that MUs derived from both distal and proxi-mal paretic (upper limb) muscle exhibit systematic alterationsin AHP duration. A recent study in lower limb muscle in strokesurvivors further supports our results (Ivanova et al. 2014).
Our CV analysis also supports this conclusion, albeit indi-rectly. Presumably because of the presence of a longer AHP,the CV is decreased in paretic units compared with contralat-eral and control units. A lower CV indicates that spikes aretriggered over a more limited range of times around the meanISI, consistent with a longer AHP. Our CV results support theAHP estimate conclusions in that paretic MUs exhibit longerAHPs with lower CVs, while contralateral/control MUs exhibitshorter AHPs with higher CVs. These CV results are notmerely a reflection of the firing rate differences betweengroups, because we ensured that the range of firing rates waskept similar among groups. Additionally, given that generallythe CV of a MU decreases with increased firing rates, theopposite effect would actually be expected with the previouslyshown firing rate differences between the tested groups. Thisphenomenon was also reported earlier in cat preparations(Brownstone et al. 1992; Manuel et al. 2006; Powers andBinder 2000). Figure 6 further supports this conclusion, show-
ing that there is a clear negative trend between CV value andAHP for single contralateral as well as paretic MUs. The tworegression lines between paretic and contralateral groups arenot significantly different, suggesting that the relationshipbetween AHP and CV is similar in both sides and that thelower CV seen in paretic MUs is a function of their longerAHPs.
The AHP also has a significant impact on the slope of therelation between firing rate and injected current (Manuel et al.2006; Miles et al. 2007; Mottram et al. 2009), i.e., on theinput-output gain of the motoneuron. The larger and longer theAHP, the lower the input-output gain. Thus the increased AHPduration seen in this study may account in part for the tendencyfor there to be lower firing rates in paretic MUs of strokesurvivors over a range of contraction levels (Gemperline et al.1995; Mottram et al. 2009).
Our modified IDR analysis may be better suited to compar-isons of AHP durations in stroke survivors than other publishedmethods, as it eliminates the potentially confounding impact ofcomparing AHP estimates at significantly different firing rates,a point also discussed in a previous study (Piotrkiewicz et al.2007). ISI variability analysis is governed by the overallvariability of the spike train, which is directly influenced byfiring rate. Our modified IDR analysis does not rely on thevariability of the spike train. Instead, IDR analysis is governedby the “termination probability” of interimpulse intervals.Additionally, in this study we were able to test both the pareticand contralateral sides of the same subject and directly com-pare how the AHP duration estimate differs within an individ-ual. This is important, given the heterogeneous stroke popula-tion and the variation of therapeutic measures experienced byeach individual subject.
The use of a novel surface electrode for MU recordingsallowed us to record from the same MUs for lengthy periods,up to 7 min in several instances. We can be confident aboutMU identification because we selected large-amplitude units,whose MU action potential shape remained stable. We werealso able to record from the same MU after a brief rest periodprovided for the subjects. On the negative side, we werelimited to recordings of low-threshold MUs.
Sources of Error
A modified IDR analysis was used in order to best accom-modate the constraints experienced in our stroke survivorstudies. The full IDR analysis requires several lengthy record-ing trains from one MU (300 s or more) in order to estimate anAHP trajectory. For this study, we were primarily interested inestimating AHP duration, since the IDR analysis of AHPtrajectory is based in “noise units,” which cannot be quantifiedin the human population. Focusing solely on estimating AHPduration allowed for less data collection from each MU, which,in turn, permitted increased inclusion of many stroke subjectswho might have been unable to meet the more stringentrecording requirements associated with other estimation meth-ods.
Previous studies have illustrated the stability of the IDRanalysis-derived AHP estimate within the same unit over arange of MU firing rates, a result that also follows from thetheoretical basis of the IDR analysis (Gossen et al. 2003;MacDonell et al. 2007; Matthews 1996; Powers and Binder
y = -0.05x + 21.65R² = 0.40
y = -0.08x + 23.13R² = 0.40
0
5
10
15
20
25
0 50 100 150 200 250
Coe
ffici
ent o
f Var
iatio
n
AHP Estimate (ms)
Contralateral
Paretic
Fig. 6. Single MUs: contralateral and paretic. For each unit, the averagecoefficient of variation (CV) value vs. average AHP estimate is plotted. Bothcontralateral and paretic units show that as AHP duration increases, CVdecreases.
1454 AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

2000). The IDR analysis will only converge for intervals (in aMU spike train) that are longer than the AHP, effectively atrelatively low MU firing rates.
The reliability of the AHP estimates computed from the IDRmethod is dependent on whether the firing rate of the MU is ina range in which the IDR plot would plateau, or in other wordsin a range in which the ISI duration was longer than the actualAHP duration (Piotrkiewicz et al. 2007). Thus our AHP esti-mates for control, contralateral, and paretic muscle were com-puted at slightly different firing rates, since firing rates requiredfor a robust estimate (for a convergence of the IDR plot) weregenerally lower in paretic muscle than in control or contralat-eral muscle, which in turn would be expected for a longer AHPduration, assuming that the method accurately reflects theactual AHP duration.
Although we tried to make our AHP estimates at comparableMU firing rates, the lower firing rates were not always attain-able for our control subjects, or for the contralateral side of ourstroke subjects, and consequently almost half of the MU datacollected could not be analyzed. In addition, even though wewere able to record from MU trains at higher discharge rates onthe paretic side, these data were discarded because of noncon-vergence of the IDR analysis. Nonetheless, given our resultsfrom different firing rate levels in our control subjects, as wellas the theoretical framework for the AHP estimates (Matthews1996) and earlier animal model validations for IDR analysis(Powers and Binder 2000), we believe that we were able toobtain reliable AHP duration estimates for comparisons be-tween control, contralateral, and paretic muscle.
The IDR method utilizes firing rates low enough such that asignificant number of the ISIs are longer than the AHP dura-tion. A probability function (illustrated through the IDR plot)can then reliably predict when the interval will most likely be“terminated.” The IDR plot plateaus at the time point of theAHP duration. The AHP is a determinant of firing rate, and itis an intrinsic motoneuron property that is not modulated byfeedback control (Lee and Mitchell 2012). Therefore, weexpect that an increase in AHP duration is not a result of MUfiring rate modulation, and instead contributes to the observeddecreases in firing rate (although our arguments are based oncorrelations only) . Animal model validation of modified IDRanalysis may offer robust results supporting the hypothesis thata lengthened AHP contributes to lower MU discharge rates inhemispheric stroke.
Mechanisms Contributing to Observed Longer AHP inParetic MUs
There are a number of possible mechanisms that could causea significant increase in AHP duration in paretic MUs. Onepossibility is that increases in AHP duration may result fromchanges in activity of specific neuromodulator pathways fol-lowing stroke. The AHP trajectory is controlled by both po-tassium and calcium conductances, each of which is alsoinfluenced by CNS neuromodulators. For example, monoam-inergic and cholinergic agents control specific calcium-sensi-tive channels within the neuron, and therefore any modifica-tions to these neuromodulator pathways can affect AHP-relatedconductance changes. For example, acetylcholine is able toactivate muscarinic receptors, triggering a calcium-sensitivecationic current, which may also impact calcium-sensitive
potassium channels. Neuromodulators such as GABA, gluta-mate, epinephrine, and norepinephrine also have specific ef-fects on L-type calcium conductances and may therefore indi-rectly affect potassium conductances. Further investigation ofthese various neuromodulator actions could offer insight intowhich pathways contribute to changes in AHP duration. Thisinformation can potentially be used to pharmacologically targetspecific channels or conductances and, consequently, the AHPduration.
Functional Implications: Relation Between Motor UnitFiring Rates and Motor Unit Force Production
Although we have demonstrated systematic increases inAHP duration, it is still unclear as to the overall impact of anincrease in AHP duration on muscle force generation. Previousstudies have shown that muscle force increases both in pro-portion to MU recruitment and with increases in MU firingrates (Conwit et al. 1999). The AHP is a primary determinantof motoneuron firing rate, and therefore shortening the AHPcould lead to higher firing rates and, potentially, to increasedand more efficient force production. Ultimately, the effect ofchanges in firing rate depend on the MU twitch contractionproperties, and especially on the relaxation phase, since thiswill govern the degree of tetanic fusion and overall contractileefficiency. Our present findings show that the ratio of paretic tocontralateral MVC does not correlate with the ratio of pareticto contralateral firing rate, or with AHP duration. This is mostlikely due to the fact that the measured force was maximalvoluntary force and the measured firing rate was submaximal,if not the slowest possible firing rates.
As discussed above, a number of other factors may contrib-ute to muscle paresis, and the AHP duration may be just one ofmany. This may be why we cannot find a consistent correlationbetween AHP duration changes and MVC changes. Addition-ally, longer AHP duration may be a compensatory response tovarious other impairments following stroke, such as changes inmuscle properties, disorderly MU recruitment, or decreaseddescending drive.
Finally, our subject population consisted of chronic strokesurvivors, varying from 3 to 23 yr after stroke. MVC ratiosbetween the paretic and contralateral side may be influenced byusage of the paretic limb, by medication, as well as bytherapeutic interventions experienced by each individual sub-ject. These variables were not consistent between subjects,especially given the broad range of 3–23 yr after stroke. Forfuture studies, the recruitment of acute stroke subjects mayminimize the number of confounding variables.
ACKNOWLEDGMENTS
We acknowledge Brian Jeon and April Leung for their technical assistance.
GRANTS
This research was supported by National Institute of Neurological Disordersand Stroke R01 Grant NS-062200.
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the author(s).
1455AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from

AUTHOR CONTRIBUTIONS
Author contributions: A.K.S. and X.H. performed experiments; A.K.S.analyzed data; A.K.S., R.K.P., C.J.H., N.L.S., and W.Z.R. interpretedresults of experiments; A.K.S. and X.H. prepared figures; A.K.S. drafted manu-script; A.K.S., X.H., R.K.P., C.J.H., and W.Z.R. edited and revised manuscript;A.K.S., X.H., R.K.P., C.J.H., N.L.S., and W.Z.R. approved final version ofmanuscript; R.K.P., C.J.H., N.L.S., and W.Z.R. conception and design ofresearch.
REFERENCES
Andreassen S, Rosenfalck A. Regulation of the firing pattern of single motorunits. J Neurol Neurosurg Psychiatry 43: 897–906, 1980.
Bakels R, Kernell D. Matching between motoneurone and muscle unitproperties in rat medial gastrocnemius. J Physiol 463: 307–324, 1993.
Brown WF, Snow R. Denervation in hemiplegic muscles. Stroke 21: 1700–1704, 1990.
Brownstone RM, Jordan LM, Kriellaars DJ, Noga BR, Shefchyk SJ. Onthe regulation of repetitive firing in lumbar motoneurones during fictivelocomotion in the cat. Exp Brain Res 90: 441–455, 1992.
Calvin WH. Three modes of repetitive firing and the role of threshold timecourse between spikes. Brain Res 69: 341–346, 1974.
Conwit RA, Stashuk D, Tracy B, McHugh M, Brown WF, Metter EJ. Therelationship of motor unit size, firing rate and force. Clin Neurophysiol 110:1270–1275, 1999.
Dattola R, Girlanda P, Vita G, Santoro M, Roberto ML, Toscano A,Venuto C, Baradello A, Messina C. Muscle rearrangement in patients withhemiparesis after stroke: an electrophysiological and morphological study.Eur Neurol 33: 109–114, 1993.
Gemperline JJ, Allen S, Walk D, Rymer WZ. Characteristics of motor unitdischarge in subjects with hemiparesis. Muscle Nerve 18: 1101–1114, 1995.
Gossen ER, Ivanova TD, Garland SJ. The time course of the motoneuroneafterhyperpolarization is related to motor unit twitch speed in humanskeletal muscle. J Physiol 552: 657–664, 2003.
Ivanova TD, Knorr S, Macdonell CW, Pollock CL, Garland SJ. Motoneu-rone afterhyperpolarisation time-course following stroke. Clin Neurophysiol125: 544–551, 2014.
Lee RH, Mitchell CS. Revisiting the role of spike afterhyperpolarization andspike threshold in motoneuron current-frequency gain. J Neurophysiol 107:3071–3077, 2012.
Liang LY, Chen JJ, Wang YL, Jakubiec M, Mierzejewska J, PiotrkiewiczM. Changes in spinal motoneuron “fastness” in post-stroke spastic patients.J Med Biol Eng 30: 17–22, 2010.
MacDonell CW, Ivanova TD, Garland SJ. Reliability of the interval deathrate analysis for estimating the time course of the motoneurone afterhyper-polarization in humans. J Neurosci Methods 162: 314–319, 2007.
Manuel M, Meunier C, Donnet M, Zytnicki D. The afterhyperpolarizationconductance exerts the same control over the gain and variability ofmotoneurone firing in anaesthetized cats. J Physiol 576: 873–886, 2006.
Matthews PB. Relationship of firing intervals of human motor units to thetrajectory of post-spike after-hyperpolarization and synaptic noise. J Physiol492: 597–628, 1996.
Matthews PB. Measurement of excitability of tonically firing neurones testedin a variable-threshold model motoneurone. J Physiol 544: 315–332, 2002.
McComas AJ, Sica RE, Upton AR, Aguilera N. Functional changes inmotoneurones of hemiparetic patients. J Neurol Neurosurg Psychiatry 36:183–193, 1973.
Miles GB, Hartley R, Todd AJ, Brownstone RM. Spinal cholinergic in-terneurons regulate the excitability of motoneurons during locomotion. ProcNatl Acad Sci USA 104: 2448–2453, 2007.
Mottram CJ, Suresh NL, Heckman CJ, Gorassini MA, Rymer WZ.Origins of abnormal excitability in biceps brachii motoneurons of spastic-paretic stroke survivors. J Neurophysiol 102: 2026–2038, 2009.
Piotrkiewicz M. An influence of afterhyperpolarization on the pattern ofmotoneuronal rhythmic activity. J Physiol (Paris) 93: 125–133, 1999.
Piotrkiewicz M, Kudina L, Mierzejewska J, Jakubiec M, Hausmanowa-Petrusewicz I. Age-related change in duration of afterhyperpolarization ofhuman motoneurones. J Physiol 585: 483–490, 2007.
Powers RK, Binder MD. Relationship between the time course of theafterhyperpolarization and discharge variability in cat spinal motoneurones.J Physiol 528: 131–150, 2000.
Sidney S, Rosamond WD, Howard VJ, Luepker RV. The “heart disease andstroke statistics—2013 update” and the need for a national cardiovascularsurveillance system. Circulation 127: 21–23, 2013.
Spaans F, Wilts G. Denervation due to lesions of the central nervous system.An EMG study in cases of cerebral contusion and cerebrovascular accidents.J Neurol Sci 57: 291–305, 1982.
Zijdewind I, Thomas CK. Firing patterns of spontaneously active motor unitsin spinal cord-injured subjects. J Physiol 590: 1683–1697, 2012.
1456 AHP DURATION IN STROKE SURVIVORS
J Neurophysiol • doi:10.1152/jn.01091.2012 • www.jn.org
on Novem
ber 3, 2014D
ownloaded from