Embed Size (px)
Citation preview
Challenges in the management of
RRMM
Xavier Leleu
Hôpital la Milétrie, PRC, CHU
Inserm U1402 CIC
Laboratoire d’Immunologie Oncologie et dormance tumorale
Poitiers, France
Disclosures
• Honorarium, Grants/research support, and Consulting fees: Amgen, Bristol-Myers Squibb, Celgene, Janssen, Takeda, Novartis, Sanofi, Merck, Pierre Fabre
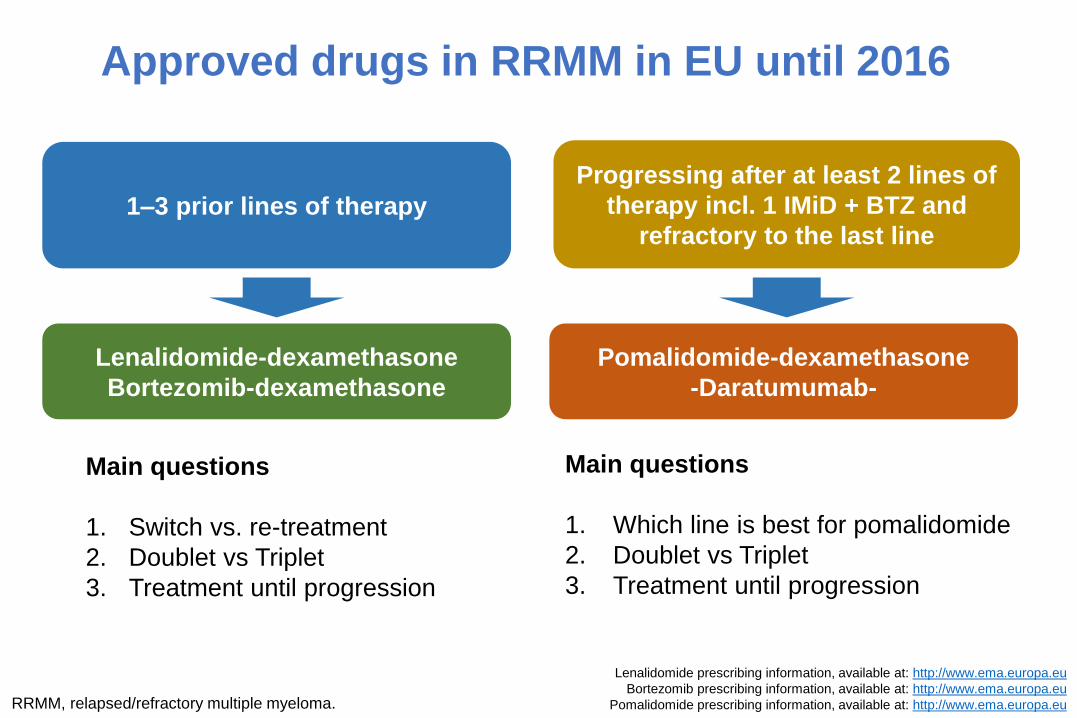
Main questions
1. Switch vs. re-treatment
2. Doublet vs Triplet
3. Treatment until progression
Main questions
1. Which line is best for pomalidomide
2. Doublet vs Triplet
3. Treatment until progression
1–3 prior lines of therapy
Progressing after at least 2 lines of
therapy incl. 1 IMiD + BTZ and
refractory to the last line
Lenalidomide-dexamethasone
Bortezomib-dexamethasone
Pomalidomide-dexamethasone
-Daratumumab-
Approved drugs in RRMM in EU until 2016
RRMM, relapsed/refractory multiple myeloma.
Lenalidomide prescribing information, available at: http://www.ema.europa.eu
Bortezomib prescribing information, available at: http://www.ema.europa.eu
Pomalidomide prescribing information, available at: http://www.ema.europa.eu
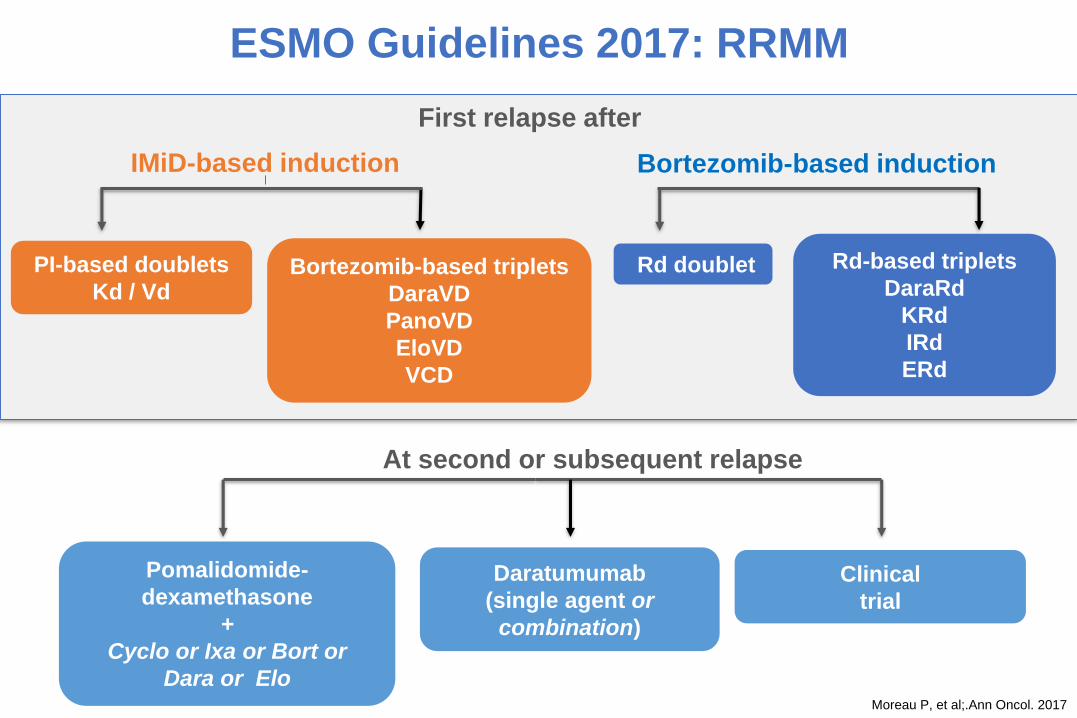
Pomalidomide-
dexamethasone
+
Cyclo or Ixa or Bort or
Dara or Elo
Daratumumab
(single agent or
combination)
Clinical
trial
At second or subsequent relapse
IMiD-based induction
PI-based doublets
Kd / VdBortezomib-based triplets
DaraVD
PanoVD
EloVD
VCD
Bortezomib-based induction
Rd-based triplets
DaraRd
KRd
IRd
ERd
Rd doublet
First relapse after
Moreau P, et al;.Ann Oncol. 2017
ESMO Guidelines 2017: RRMM
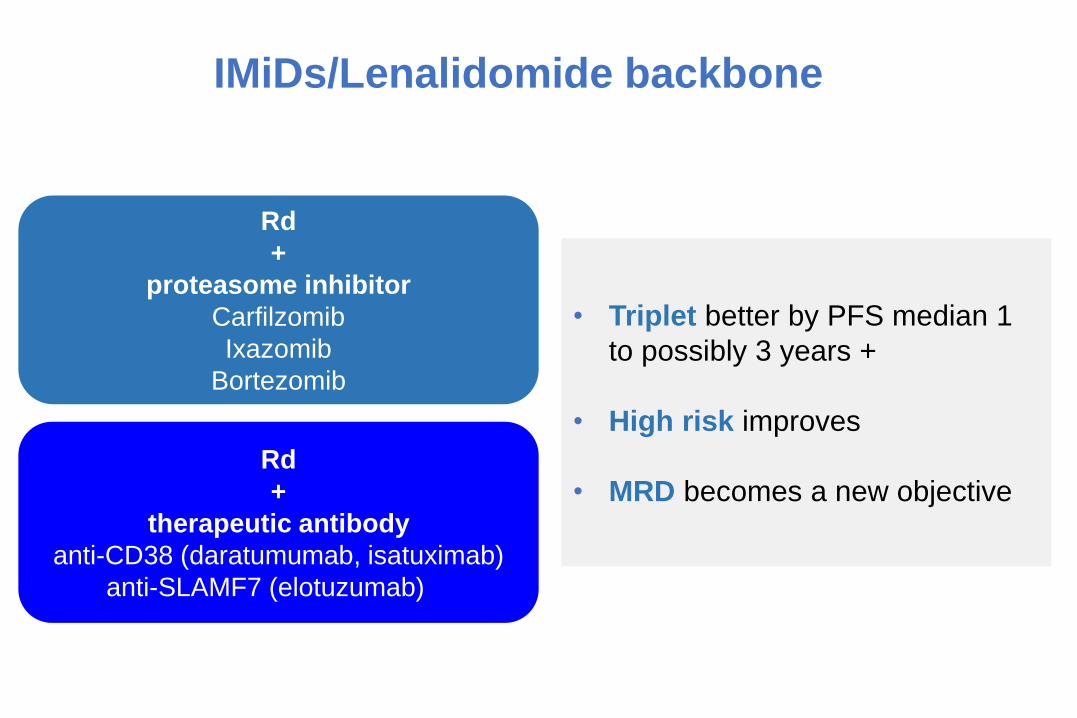
IMiDs/Lenalidomide backbone
Rd
+
proteasome inhibitor
Carfilzomib
Ixazomib
Bortezomib
Rd
+
therapeutic antibody
anti-CD38 (daratumumab, isatuximab)
anti-SLAMF7 (elotuzumab)
• Triplet better by PFS median 1
to possibly 3 years +
• High risk improves
• MRD becomes a new objective
K, carfilzomib; E, elotuzumab; I, ixazomib.
1. Dimopoulos MA, et al. N Engl J Med 2016; 375:1319-1331
2. Stewart AK, et al. N Engl J Med. 2015;372(2):142-152.
3. Lonial S, et al. N Engl J Med. 2015;373(7):621-631.
4. Dimopoulos MA, et al. Blood. 2015;126(23):Abstract 28.
5. Moreau P, et al. N Engl J Med. 2016;374(17):1621-1634.
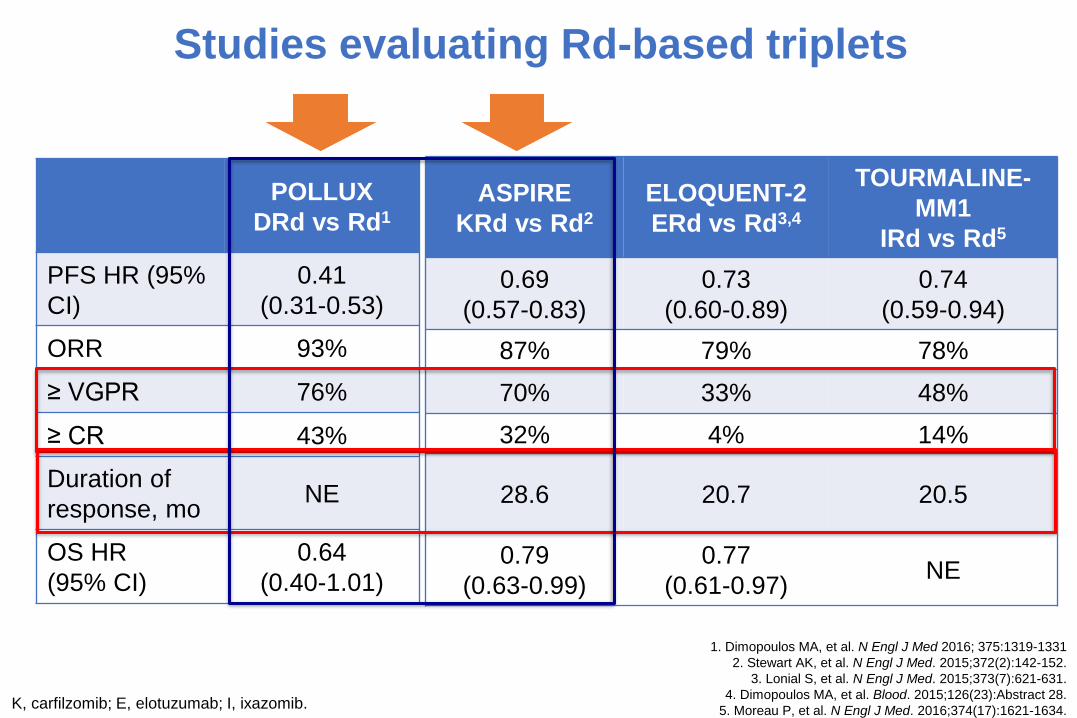
Studies evaluating Rd-based triplets
POLLUX
DRd vs Rd1
PFS HR (95%
CI)
0.41
(0.31-0.53)
ORR 93%
≥ VGPR 76%
≥ CR 43%
Duration of
response, moNE
OS HR
(95% CI)
0.64
(0.40-1.01)
ASPIRE
KRd vs Rd2
ELOQUENT-2
ERd vs Rd3,4
TOURMALINE-
MM1
IRd vs Rd5
0.69
(0.57-0.83)
0.73
(0.60-0.89)
0.74
(0.59-0.94)
87% 79% 78%
70% 33% 48%
32% 4% 14%
28.6 20.7 20.5
0.79
(0.63-0.99)
0.77
(0.61-0.97)NE
Stewart AK, et al. N Engl J Med 2015; 372:142-52
Dimopoulos MA, et al. N Engl J Med 2016; 375:1319-1331
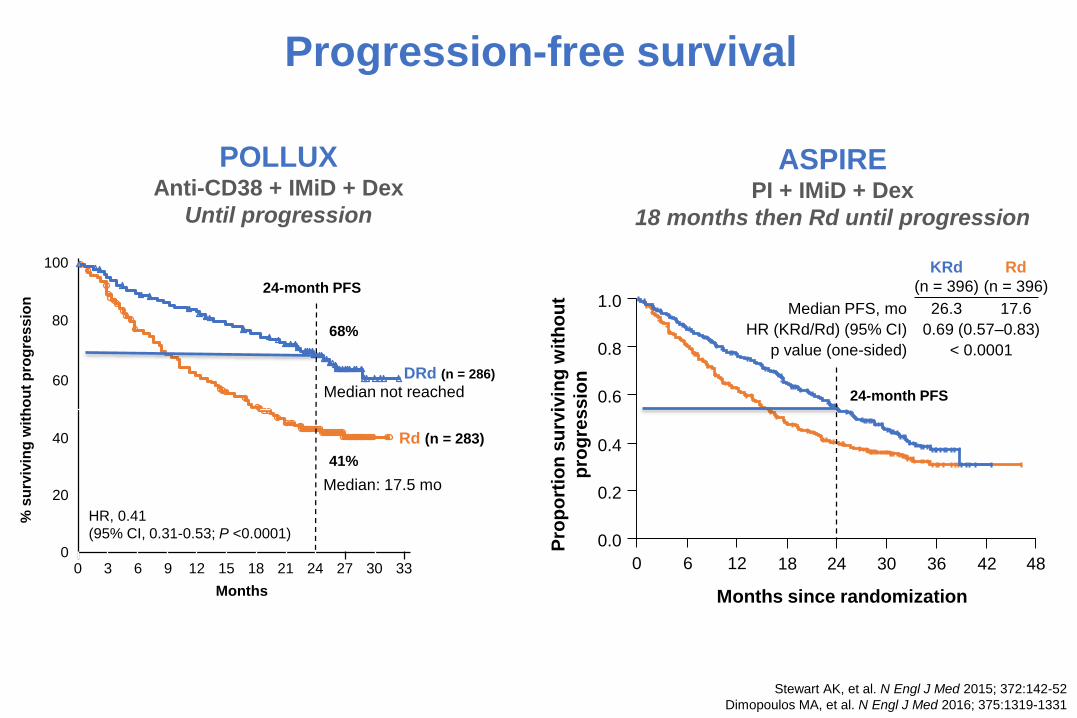
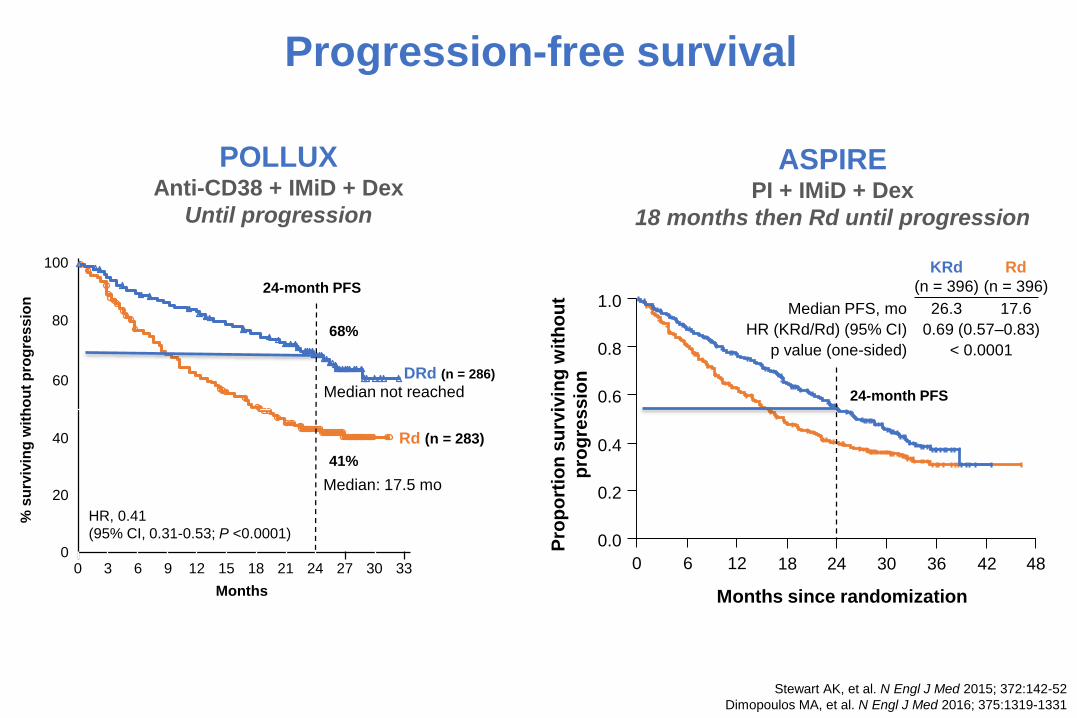
Progression-free survival
POLLUXAnti-CD38 + IMiD + Dex
Until progression
ASPIREPI + IMiD + Dex
18 months then Rd until progression
Rd
(n = 396)
KRd
(n = 396)
17.626.3
0.69 (0.57–0.83)
< 0.0001
Median PFS, mo
HR (KRd/Rd) (95% CI)
p value (one-sided)
0
0.2
0.6
1.0
Pro
po
rtio
n s
urv
ivin
g w
ith
ou
t
pro
gre
ss
ion
Months since randomization
0.8
0.4
0.0
6 18 24 30 36 42 4812
% s
urv
ivin
g w
ith
ou
t p
rog
res
sio
n
0
20
40
60
80
100
0 3 6 9 12 15 18 33
Months
21 24 30
Rd (n = 283)
DRd (n = 286)
27
24-month PFS
68%
41%
HR, 0.41
(95% CI, 0.31-0.53; P <0.0001)
Median: 17.5 mo
Median not reached 24-month PFS
Direct comparisons across trials is not intended and should not be inferred.
Dex, dexamethasone; LEN, lenalidomide; PI, proteasome inhibitor.
1. Dimopoulos MA, et al. N Engl J Med. 2016;375:1319-31.
2. Stewart AK, et al. N Engl J Med. 2015;372:142-52.
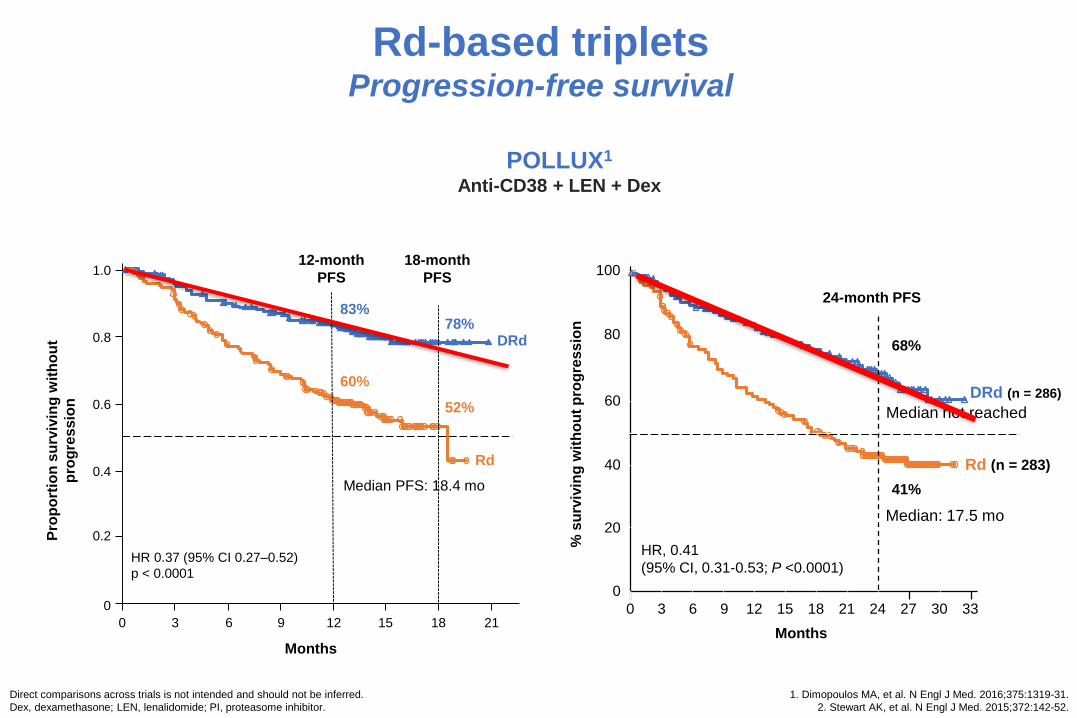
Rd-based tripletsProgression-free survival
POLLUX1
Anti-CD38 + LEN + Dex
Pro
po
rtio
n s
urv
ivin
g w
ith
ou
t
pro
gre
ss
ion
0
0.2
0.4
0.6
0.8
1.0
0 3 6 9 12 15 18 21
Rd
DRd
12-month
PFS
83%
60%
18-month
PFS
78%
52%
HR 0.37 (95% CI 0.27–0.52)
p < 0.0001
Median PFS: 18.4 mo
Months
% s
urv
ivin
g w
ith
ou
t p
rog
ressio
n0
20
40
60
80
100
0 3 6 9 12 15 18 33
Months
21 24 30
Rd (n = 283)
DRd (n = 286)
27
24-month PFS
68%
41%
HR, 0.41
(95% CI, 0.31-0.53; P <0.0001)
Median: 17.5 mo
Median not reached
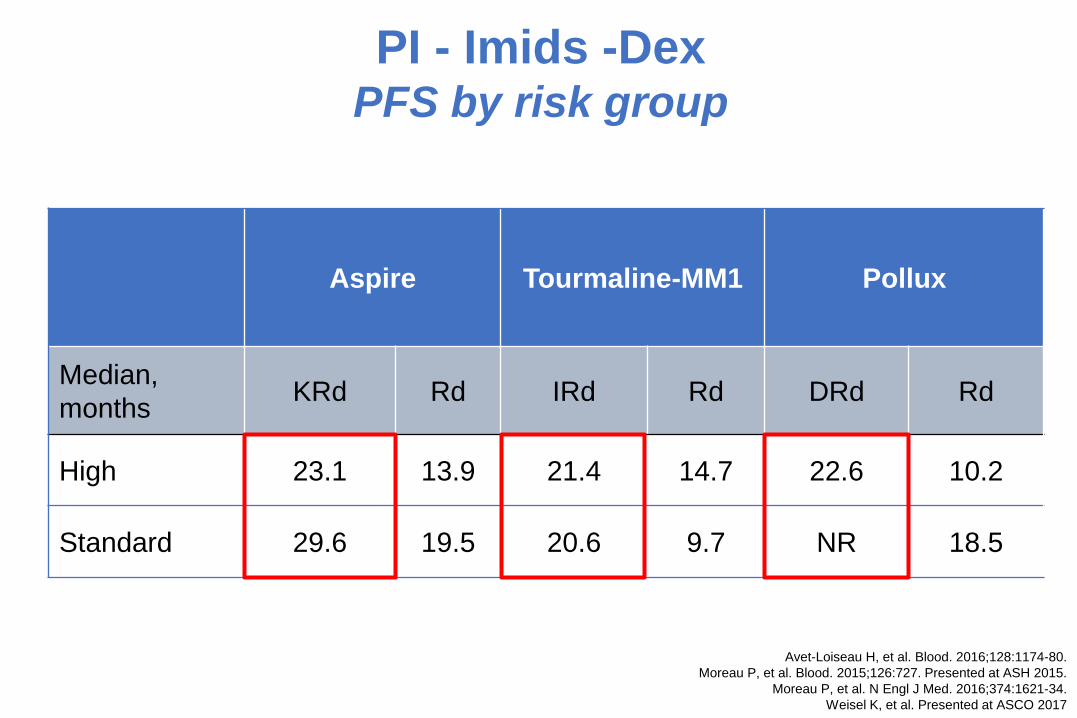
PI - Imids -DexPFS by risk group
Aspire Tourmaline-MM1 Pollux
Median,
monthsKRd Rd IRd Rd DRd Rd
High 23.1 13.9 21.4 14.7 22.6 10.2
Standard 29.6 19.5 20.6 9.7 NR 18.5
Avet-Loiseau H, et al. Blood. 2016;128:1174-80.
Moreau P, et al. Blood. 2015;126:727. Presented at ASH 2015.
Moreau P, et al. N Engl J Med. 2016;374:1621-34.
Weisel K, et al. Presented at ASCO 2017
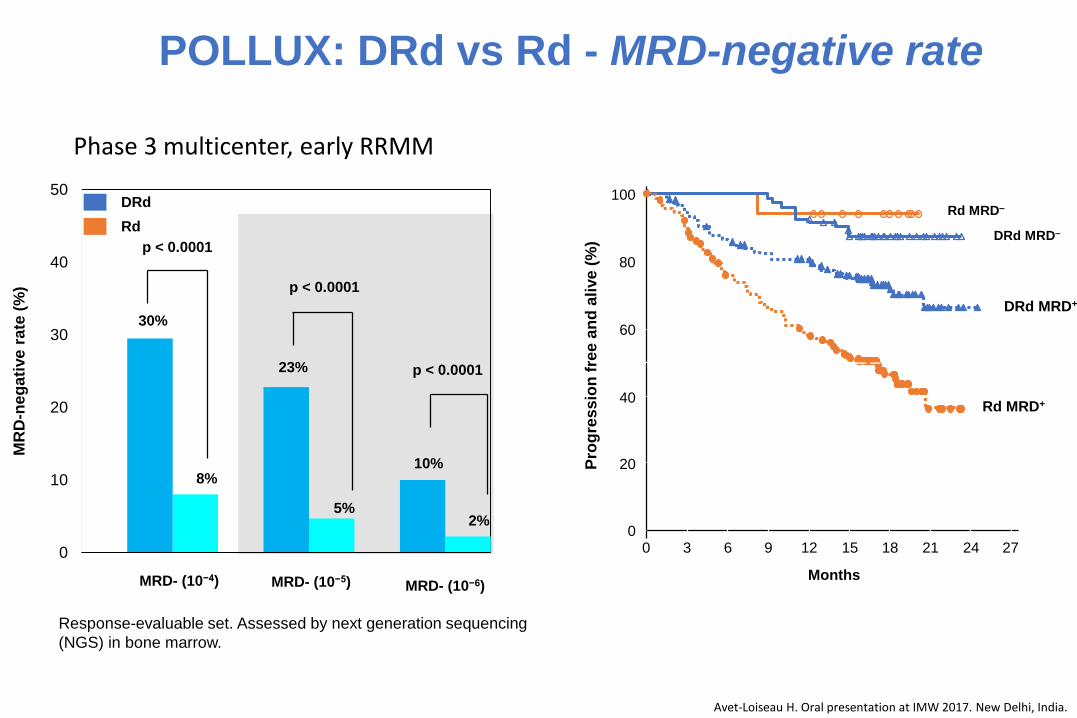
Response-evaluable set. Assessed by next generation sequencing
(NGS) in bone marrow.
Avet-Loiseau H. Oral presentation at IMW 2017. New Delhi, India.
DRd
Rd
0
10
20
30
40
50
MR
D-n
eg
ati
ve
ra
te (
%)
MRD- (10−4) MRD- (10−5) MRD- (10−6)
30%
8%
p < 0.0001
23%
5%
p < 0.0001
10%
2%
p < 0.0001
Pro
gre
ss
ion
fre
e a
nd
ali
ve
(%
)
0
20
40
60
80
100
0 3 6 9 12 15 21 27
Months
2418
Rd MRD–
DRd MRD–
DRd MRD+
Rd MRD+
Phase 3 multicenter, early RRMM PFS
POLLUX: DRd vs Rd - MRD-negative rate
Weisel K et al., ASCO 2017
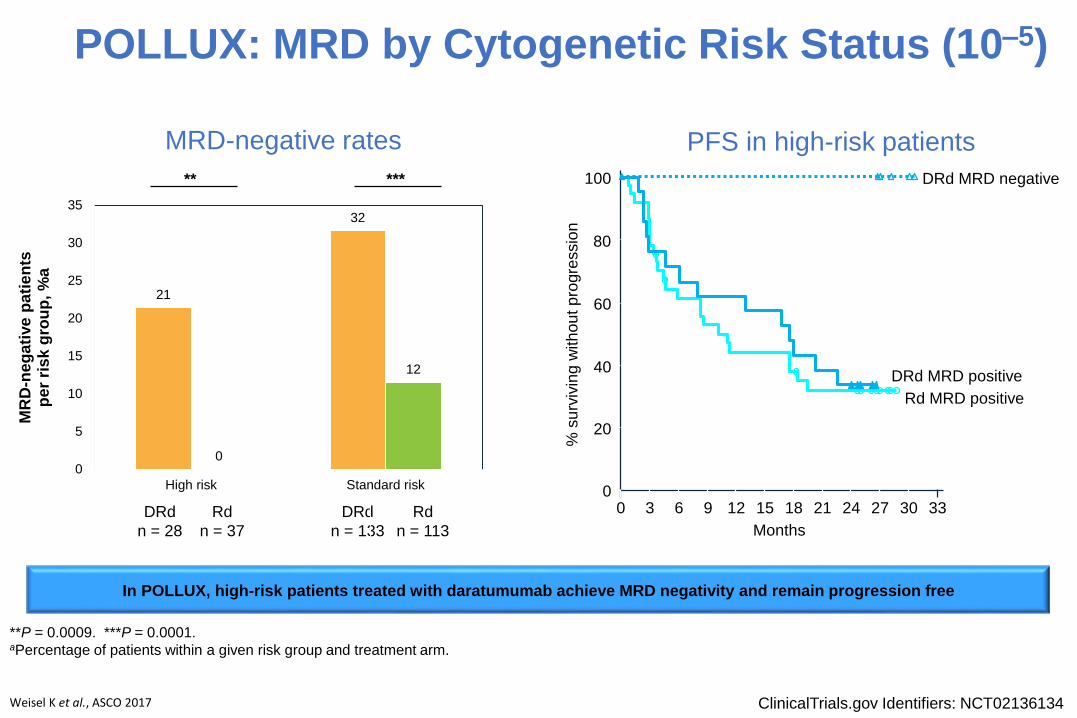
**P = 0.0009. ***P = 0.0001. aPercentage of patients within a given risk group and treatment arm.
21
32
0
12
0
5
10
15
20
25
30
35
High risk Standard risk
MR
D-n
eg
ati
ve
pa
tie
nts
p
er
ris
k g
rou
p,
%a
** ***
DRd
n = 28
Rd
n = 37
DRd
n = 133
Rd
n = 113
MRD-negative rates PFS in high-risk patients
% s
urv
ivin
g w
ith
ou
t p
rogre
ssio
n
0
20
40
60
80
100
0 3 6 9 12 15 18 33
Months
21 24
Rd MRD positive
DRd MRD negative
27
DRd MRD positive
30
In POLLUX, high-risk patients treated with daratumumab achieve MRD negativity and remain progression free
ClinicalTrials.gov Identifiers: NCT02136134
POLLUX: MRD by Cytogenetic Risk Status (10–5)
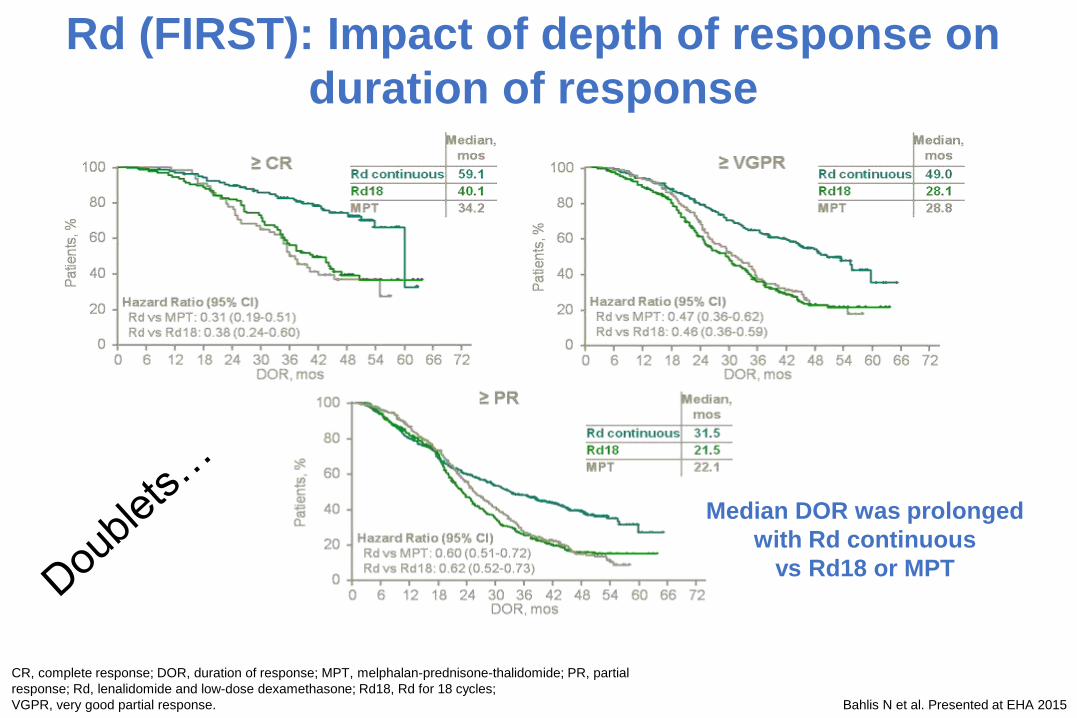
CR, complete response; DOR, duration of response; MPT, melphalan-prednisone-thalidomide; PR, partial
response; Rd, lenalidomide and low-dose dexamethasone; Rd18, Rd for 18 cycles;
VGPR, very good partial response. Bahlis N et al. Presented at EHA 2015
Rd (FIRST): Impact of depth of response on
duration of response
• Median DOR was prolonged
with Rd continuous
• vs Rd18 or MPT
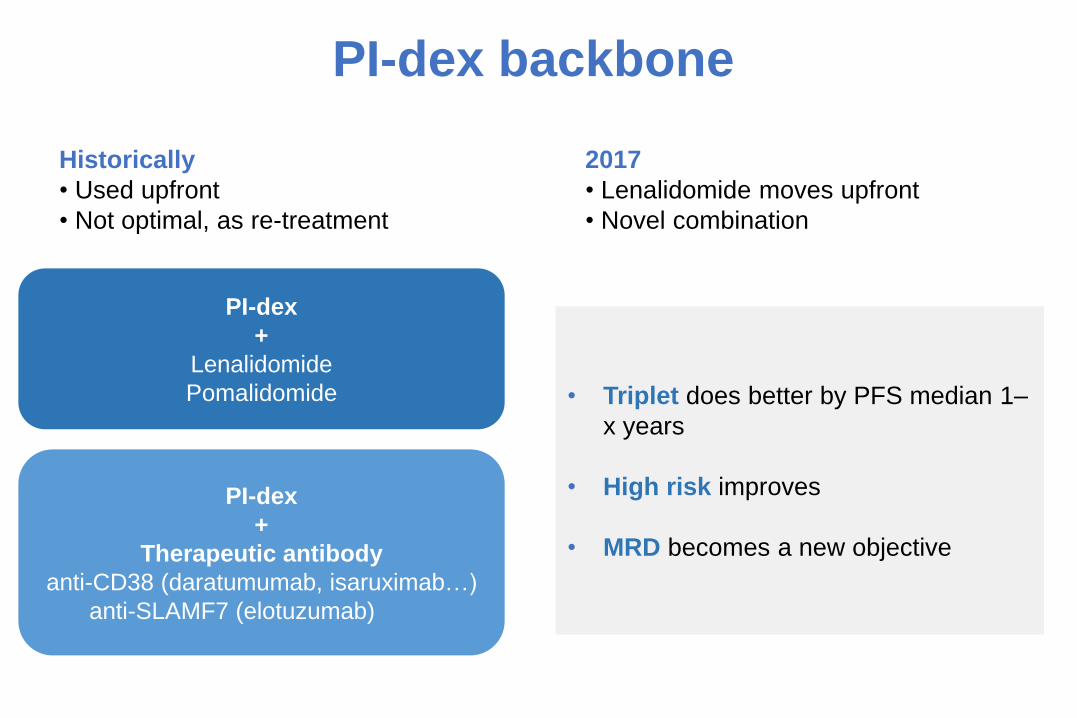
PI-dex backbone
PI-dex
+
Lenalidomide
Pomalidomide
PI-dex
+
Therapeutic antibody
anti-CD38 (daratumumab, isaruximab…)
anti-SLAMF7 (elotuzumab)
• Triplet does better by PFS median 1–
x years
• High risk improves
• MRD becomes a new objective
Historically
• Used upfront
• Not optimal, as re-treatment
2017
• Lenalidomide moves upfront
• Novel combination
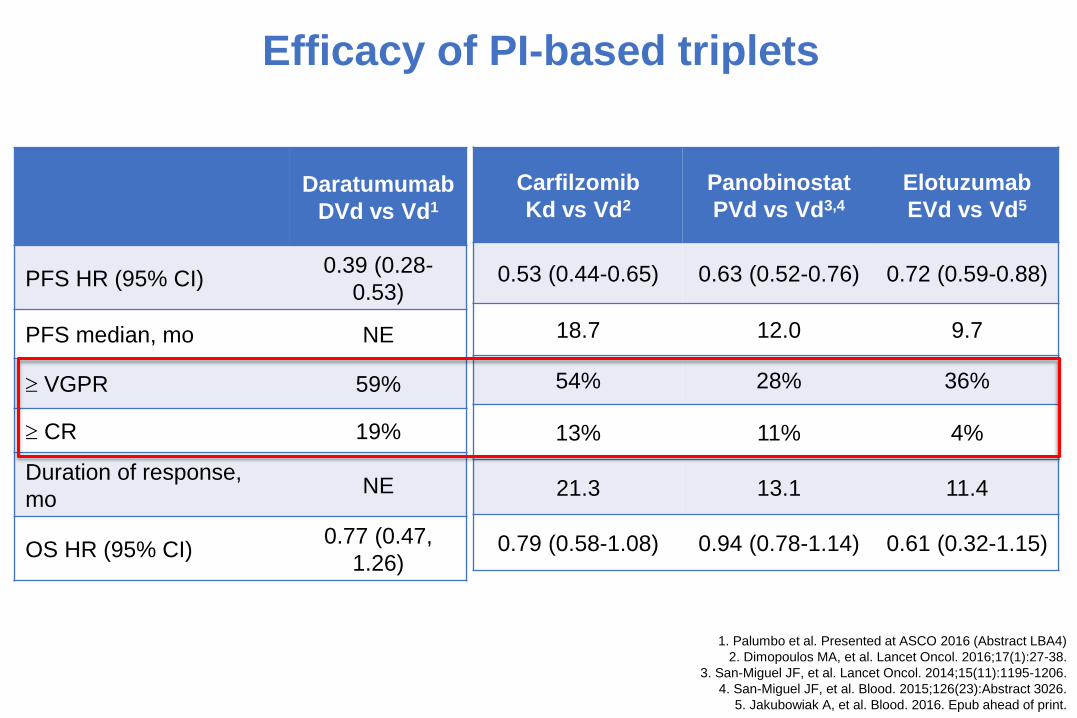
1. Palumbo et al. Presented at ASCO 2016 (Abstract LBA4)
2. Dimopoulos MA, et al. Lancet Oncol. 2016;17(1):27-38.
3. San-Miguel JF, et al. Lancet Oncol. 2014;15(11):1195-1206.
4. San-Miguel JF, et al. Blood. 2015;126(23):Abstract 3026.
5. Jakubowiak A, et al. Blood. 2016. Epub ahead of print.
Efficacy of PI-based triplets
Daratumumab
DVd vs Vd1
PFS HR (95% CI)0.39 (0.28-
0.53)
PFS median, mo NE
VGPR 59%
CR 19%
Duration of response,
moNE
OS HR (95% CI)0.77 (0.47,
1.26)
Carfilzomib
Kd vs Vd2
Panobinostat
PVd vs Vd3,4
Elotuzumab
EVd vs Vd5
0.53 (0.44-0.65) 0.63 (0.52-0.76) 0.72 (0.59-0.88)
18.7 12.0 9.7
54% 28% 36%
13% 11% 4%
21.3 13.1 11.4
0.79 (0.58-1.08) 0.94 (0.78-1.14) 0.61 (0.32-1.15)
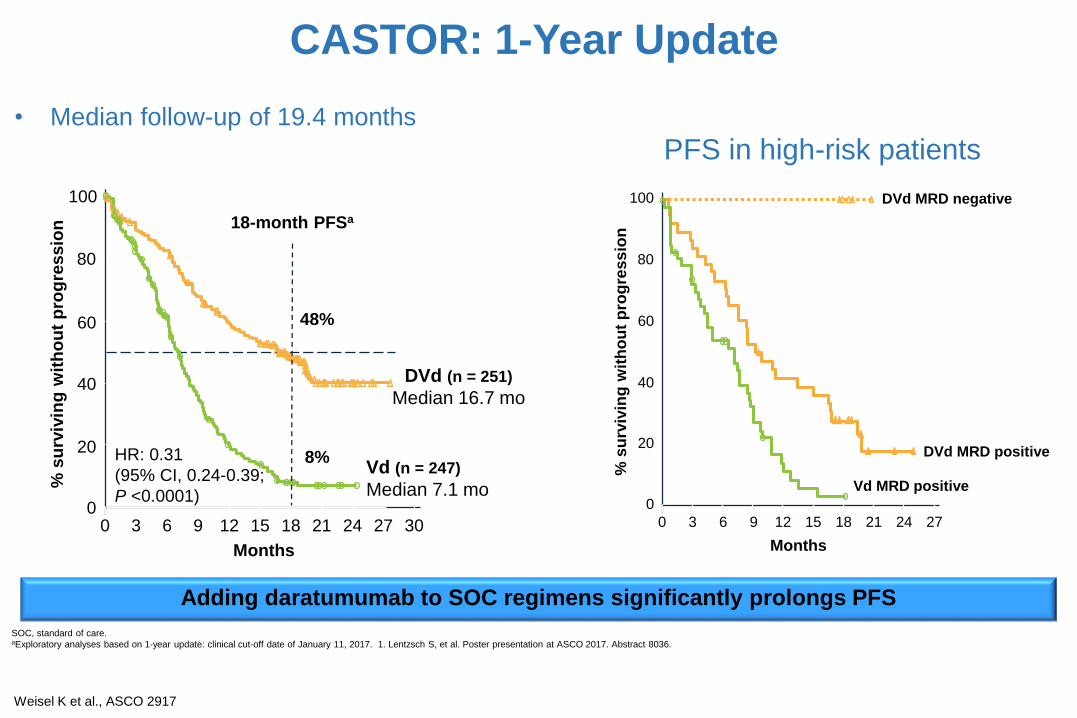
CASTOR: 1-Year Update
Weisel K et al., ASCO 2917
SOC, standard of care.aExploratory analyses based on 1-year update: clinical cut-off date of January 11, 2017. 1. Lentzsch S, et al. Poster presentation at ASCO 2017. Abstract 8036.
18-month PFSa
% s
urv
ivin
g w
ith
ou
t p
rog
ressio
n
0
20
40
60
80
0 3 6 9 12 15 18 30
Months
21 24 27
Median 16.7 mo
DVd (n = 251)
Vd (n = 247)
Median 7.1 mo
48%
8%HR: 0.31
(95% CI, 0.24-0.39;
P <0.0001)
100
Adding daratumumab to SOC regimens significantly prolongs PFS
• Median follow-up of 19.4 months
% s
urv
ivin
g w
ith
ou
t p
rog
res
sio
n
0
20
40
60
80
100
0 3 6 9 12 15 18 27
Months
21 24
Vd MRD positive
DVd MRD negative
DVd MRD positive
PFS in high-risk patients
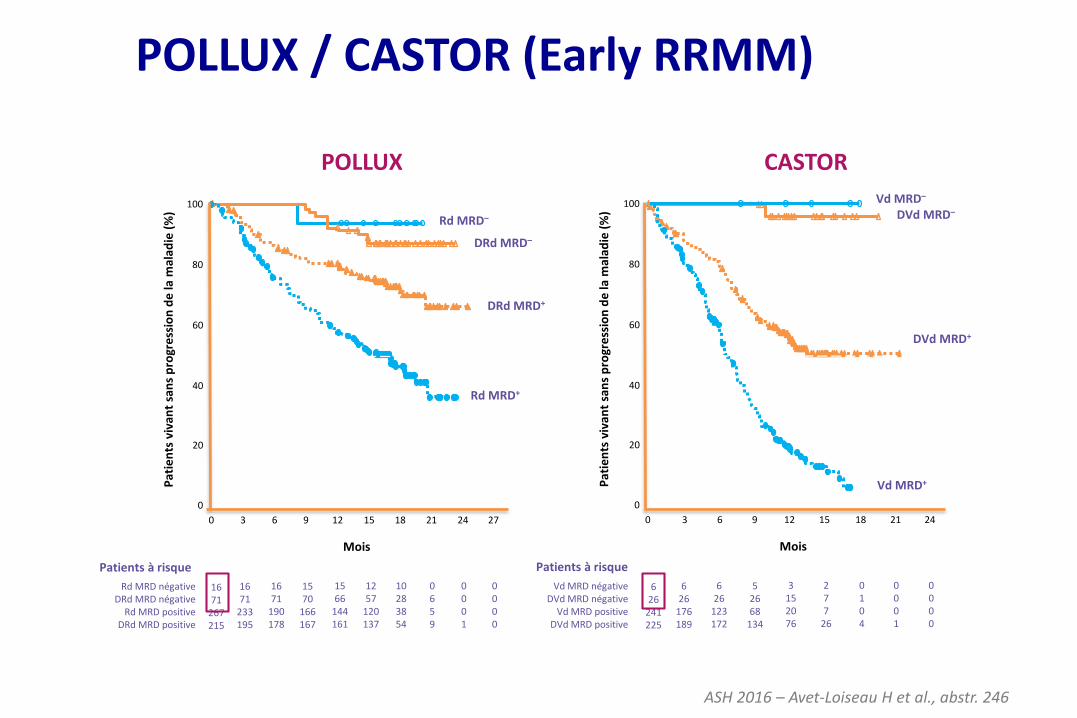
CASTORPOLLUX
Pat
ien
ts v
ivan
t sa
ns
pro
gre
ssio
n d
e la
mal
adie
(%)
0
20
40
60
80
100
0 3 6 9 12 15 18 24
Vd MRD négativeDVd MRD négative
Vd MRD positiveDVd MRD positive
Patients à risque
Mois
21
626
241225
626
176189
626
123172
52668
134
3152076
277
26
0104
0001
0000
Pat
ien
ts v
ivan
t sa
ns
pro
gre
ssio
n d
e la
mal
adie
(%)
0
20
40
60
80
100
0 3 6 9 12 15 21 27
Rd MRD négativeDRd MRD négative
Rd MRD positiveDRd MRD positive
Patients à risque
Mois
24
1671
267215
1671
233195
1671
190178
1570
166167
1566
144161
1257
120137
0659
0001
0000
18
10283854
Rd MRD–
DRd MRD–
DRd MRD+
Rd MRD+
Vd MRD–
DVd MRD–
DVd MRD+
Vd MRD+
Essais POLLUX / CASTOR (rechute)
ASH 2016 – Avet-Loiseau H et al., abstr. 246
POLLUX / CASTOR (Early RRMM)
Stewart AK, et al. N Engl J Med 2015; 372:142-52
Dimopoulos MA, et al. N Engl J Med 2016; 375:1319-1331
Progression-free survival
POLLUXAnti-CD38 + IMiD + Dex
Until progression
ASPIREPI + IMiD + Dex
18 months then Rd until progression
Rd
(n = 396)
KRd
(n = 396)
17.626.3
0.69 (0.57–0.83)
< 0.0001
Median PFS, mo
HR (KRd/Rd) (95% CI)
p value (one-sided)
0
0.2
0.6
1.0
Pro
po
rtio
n s
urv
ivin
g w
ith
ou
t
pro
gre
ss
ion
Months since randomization
0.8
0.4
0.0
6 18 24 30 36 42 4812
% s
urv
ivin
g w
ith
ou
t p
rog
res
sio
n
0
20
40
60
80
100
0 3 6 9 12 15 18 33
Months
21 24 30
Rd (n = 283)
DRd (n = 286)
27
24-month PFS
68%
41%
HR, 0.41
(95% CI, 0.31-0.53; P <0.0001)
Median: 17.5 mo
Median not reached 24-month PFS
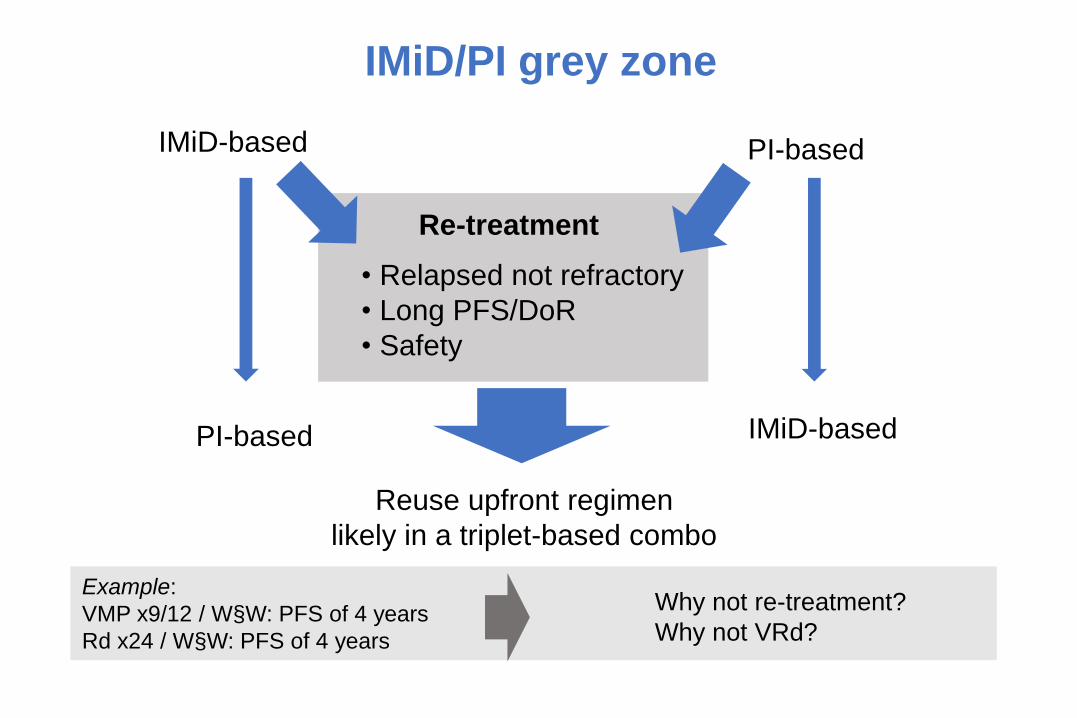
IMiD/PI grey zone
IMiD-based PI-based
IMiD-basedPI-based
Re-treatment
• Relapsed not refractory
• Long PFS/DoR
• Safety
Reuse upfront regimen
likely in a triplet-based combo
Example:
VMP x9/12 / W§W: PFS of 4 years
Rd x24 / W§W: PFS of 4 years
Why not re-treatment?
Why not VRd?
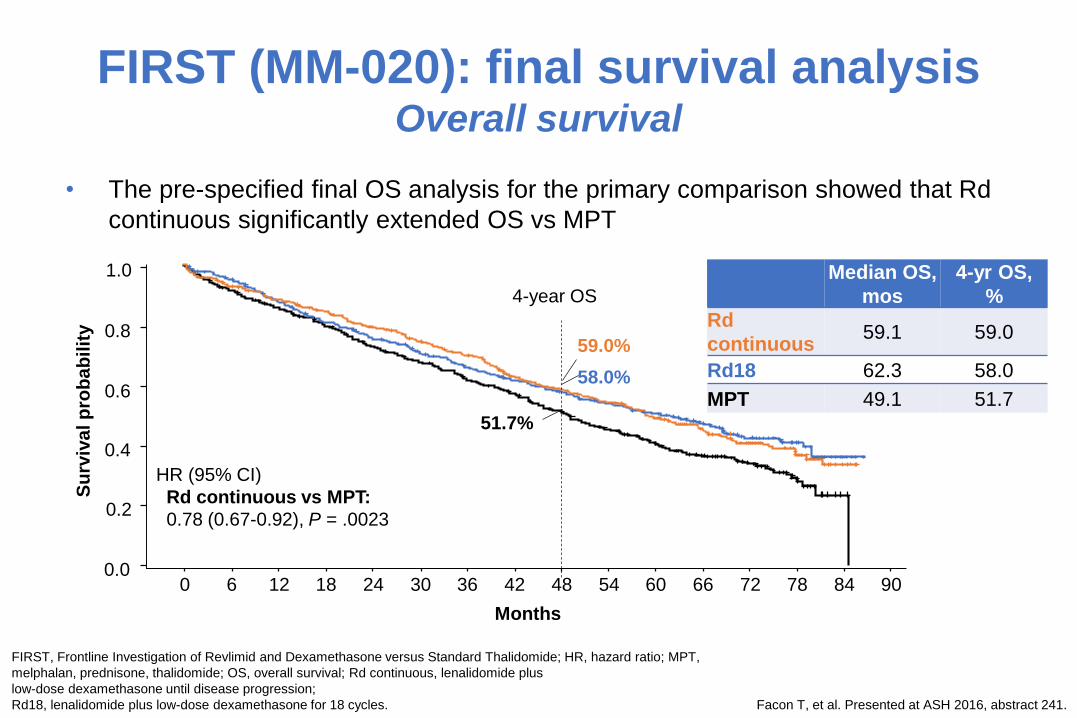
FIRST (MM-020): final survival analysisOverall survival
• The pre-specified final OS analysis for the primary comparison showed that Rd
continuous significantly extended OS vs MPT
FIRST, Frontline Investigation of Revlimid and Dexamethasone versus Standard Thalidomide; HR, hazard ratio; MPT,
melphalan, prednisone, thalidomide; OS, overall survival; Rd continuous, lenalidomide plus
low-dose dexamethasone until disease progression;
Rd18, lenalidomide plus low-dose dexamethasone for 18 cycles. Facon T, et al. Presented at ASH 2016, abstract 241.
Median OS,
mos
4-yr OS,
%
Rd
continuous59.1 59.0
Rd18 62.3 58.0
MPT 49.1 51.7
HR (95% CI)
Rd continuous vs MPT:
0.78 (0.67-0.92), P = .0023
1.0
0.8
0.6
0.4
0.2
0.00 6 12 18 24 30 36 42 48 54 6660 7872 9084
Months
Su
rviv
al p
rob
ab
ilit
y
4-year OS
59.0%
58.0%
51.7%
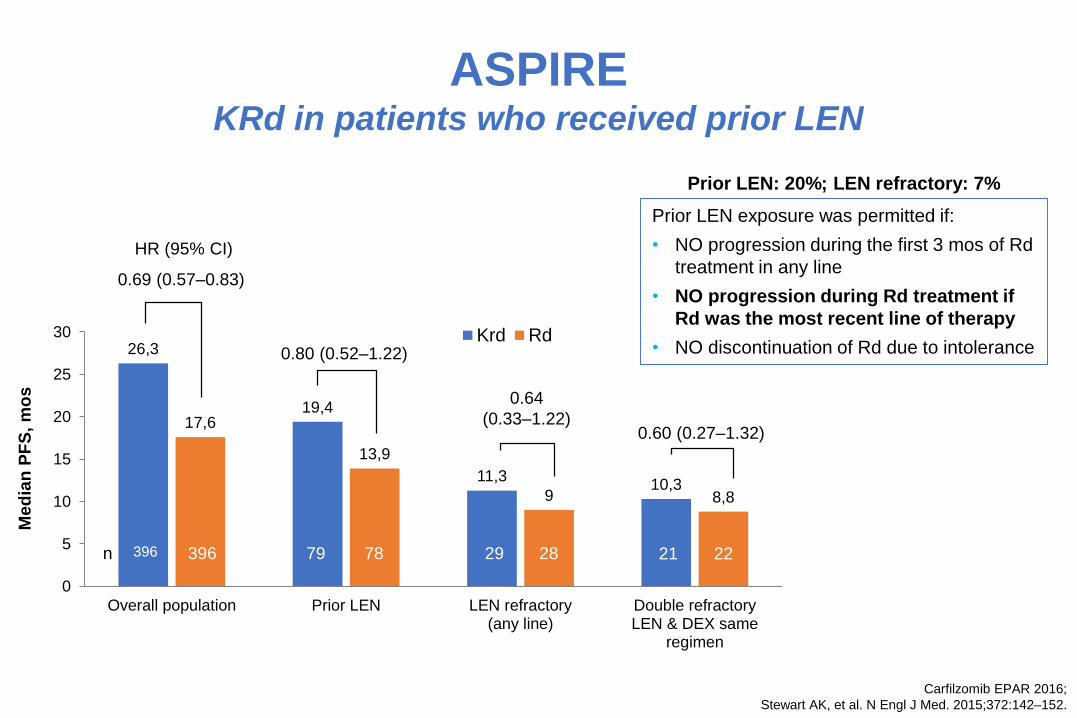
Carfilzomib EPAR 2016;
Stewart AK, et al. N Engl J Med. 2015;372:142–152.
ASPIRE KRd in patients who received prior LEN
Prior LEN: 20%; LEN refractory: 7%
Prior LEN exposure was permitted if:
• NO progression during the first 3 mos of Rd
treatment in any line
• NO progression during Rd treatment if
Rd was the most recent line of therapy
• NO discontinuation of Rd due to intolerance
HR (95% CI)
26,3
19,4
11,310,3
17,6
13,9
9 8,8
0
5
10
15
20
25
30
Overall population Prior LEN LEN refractory(any line)
Double refractoryLEN & DEX same
regimen
Krd Rd
396 79 29396 78 28
0.69 (0.57–0.83)
0.80 (0.52–1.22)
0.64
(0.33–1.22)
n 21 22
0.60 (0.27–1.32)
Med
ian
PF
S,
mo
s
Module 2 Part 2 data: Scenario C: Retreat with LEN (6/13)
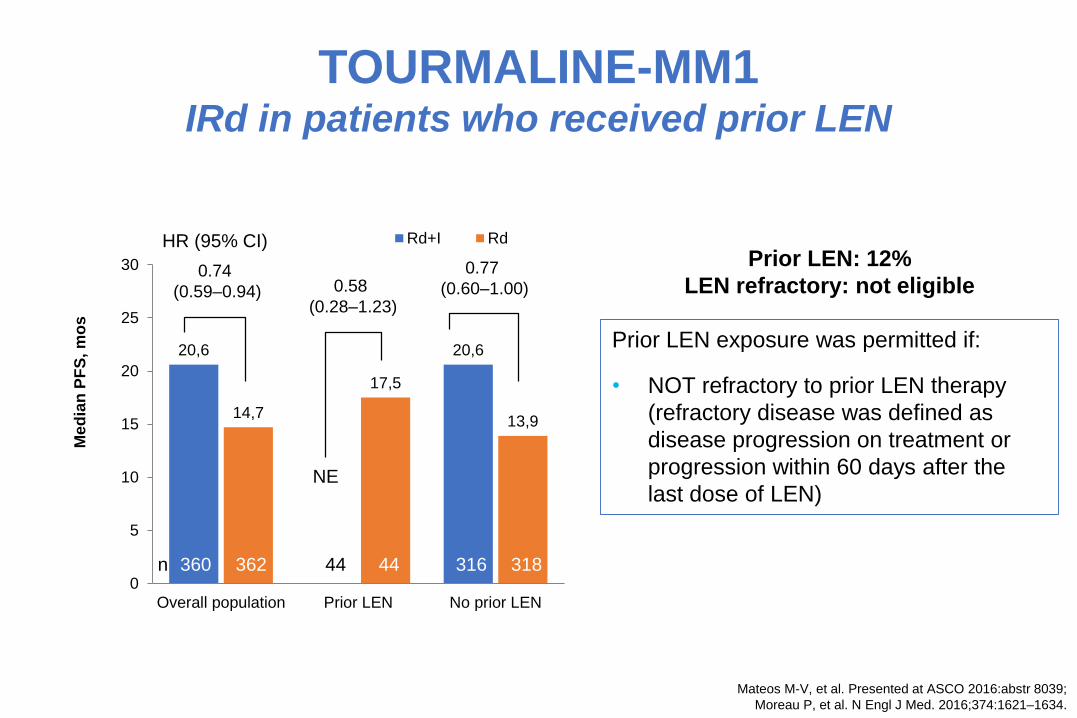
20,6 20,6
14,7
17,5
13,9
0
5
10
15
20
25
30
Overall population Prior LEN No prior LEN
Me
dia
n P
FS
, m
os
Rd+I Rd
Prior LEN: 12%
LEN refractory: not eligible
360 16362 318n
Mateos M-V, et al. Presented at ASCO 2016:abstr 8039;
Moreau P, et al. N Engl J Med. 2016;374:1621–1634.
TOURMALINE-MM1 IRd in patients who received prior LEN
4444 316
NE
0.74
(0.59–0.94) 0.58
(0.28–1.23)
HR (95% CI)
0.77
(0.60–1.00)
Prior LEN exposure was permitted if:
• NOT refractory to prior LEN therapy
(refractory disease was defined as
disease progression on treatment or
progression within 60 days after the
last dose of LEN)
Module 2 Part 2 data: Scenario C: Retreat with LEN (7/13)
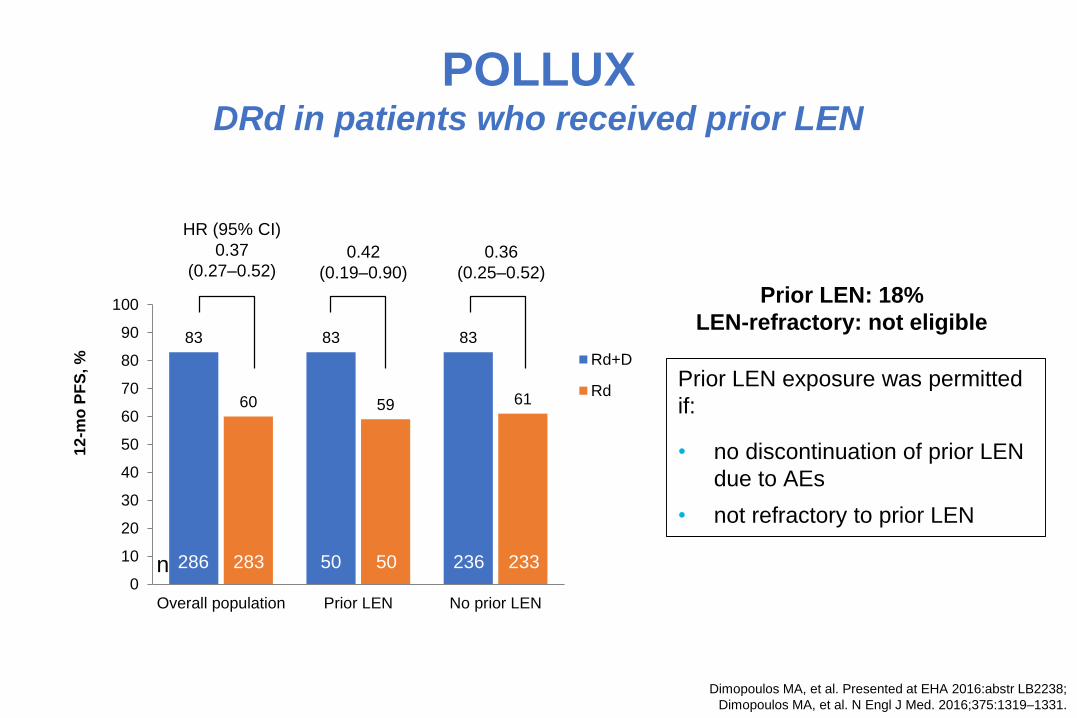
Dimopoulos MA, et al. Presented at EHA 2016:abstr LB2238;
Dimopoulos MA, et al. N Engl J Med. 2016;375:1319–1331.
POLLUXDRd in patients who received prior LEN
No prior
LEN
83 83 83
60 59 61
0
10
20
30
40
50
60
70
80
90
100
Overall population Prior LEN No prior LEN
12
-mo
PF
S, % Rd+D
Rd
0.36
(0.25–0.52)
0.42
(0.19–0.90)
HR (95% CI)
0.37
(0.27–0.52)
Prior LEN: 18%
LEN-refractory: not eligible
286 50 50283 236 233n
Prior LEN exposure was permitted
if:
• no discontinuation of prior LEN
due to AEs
• not refractory to prior LEN
Which triplet is the best choice
for my patient?
Selection criteria
• Efficacy: PFS/OS
• Safety
• QoL
• Cost
• Convenience (oral)
• Frontline therapy, depth and duration of first response
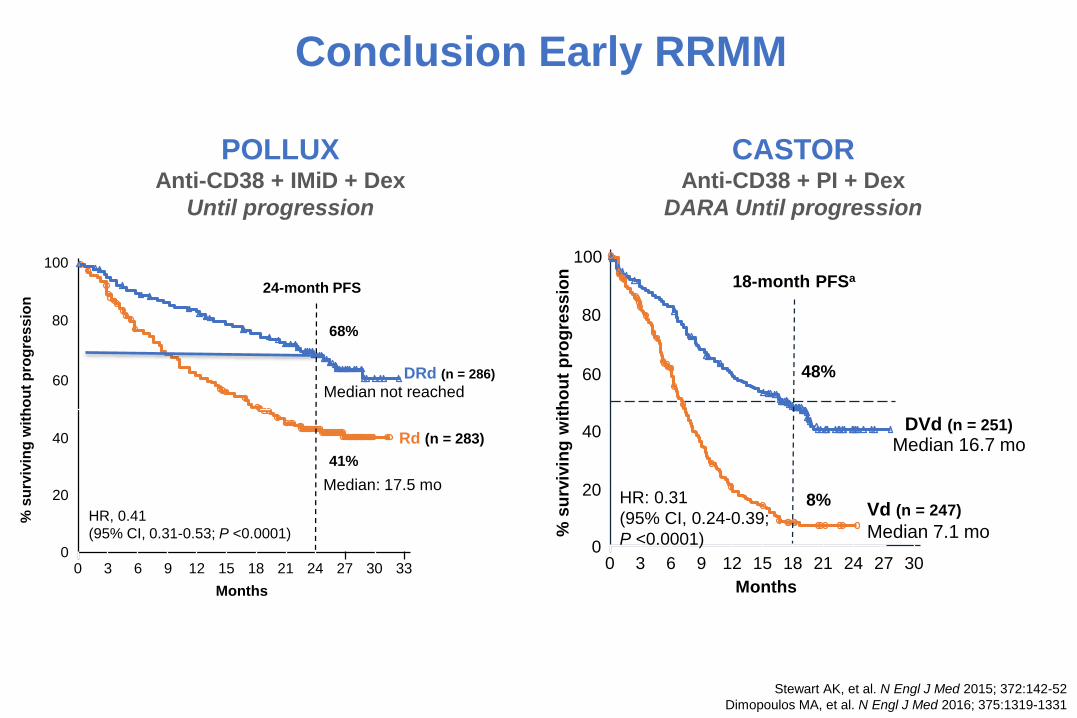
Stewart AK, et al. N Engl J Med 2015; 372:142-52
Dimopoulos MA, et al. N Engl J Med 2016; 375:1319-1331
Conclusion Early RRMM
POLLUXAnti-CD38 + IMiD + Dex
Until progression
% s
urv
ivin
g w
ith
ou
t p
rog
res
sio
n
0
20
40
60
80
100
0 3 6 9 12 15 18 33
Months
21 24 30
Rd (n = 283)
DRd (n = 286)
27
24-month PFS
68%
41%
HR, 0.41
(95% CI, 0.31-0.53; P <0.0001)
Median: 17.5 mo
Median not reached
18-month PFSa
% s
urv
ivin
g w
ith
ou
t p
rog
ressio
n0
20
40
60
80
0 3 6 9 12 15 18 30
Months
21 24 27
Median 16.7 moDVd (n = 251)
Vd (n = 247)
Median 7.1 mo
48%
8%HR: 0.31
(95% CI, 0.24-0.39;
P <0.0001)
100
CASTORAnti-CD38 + PI + Dex
DARA Until progression
NEED to optimize Pomalidomide-Dexamethasone?
1.Earlier is better
2.Combined is better
3.Be safe, stay safe, remain safe = be happy
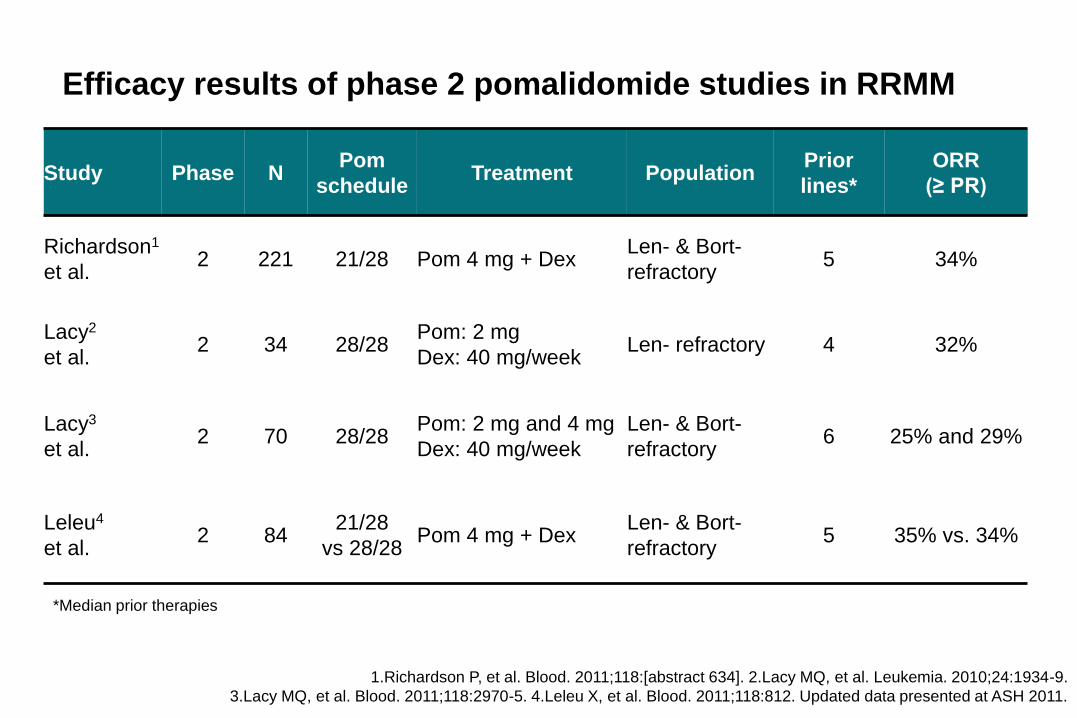
Efficacy results of phase 2 pomalidomide studies in RRMM
Study Phase NPom
scheduleTreatment Population
Prior
lines*
ORR
(≥ PR)
Richardson1
et al.2 221 21/28 Pom 4 mg + Dex
Len- & Bort-
refractory5 34%
Lacy2
et al.2 34 28/28
Pom: 2 mg
Dex: 40 mg/weekLen- refractory 4 32%
Lacy3
et al.2 70 28/28
Pom: 2 mg and 4 mg
Dex: 40 mg/week
Len- & Bort-
refractory6 25% and 29%
Leleu4
et al.2 84
21/28
vs 28/28Pom 4 mg + Dex
Len- & Bort-
refractory5 35% vs. 34%
1.Richardson P, et al. Blood. 2011;118:[abstract 634]. 2.Lacy MQ, et al. Leukemia. 2010;24:1934-9.
3.Lacy MQ, et al. Blood. 2011;118:2970-5. 4.Leleu X, et al. Blood. 2011;118:812. Updated data presented at ASH 2011.
*Median prior therapies
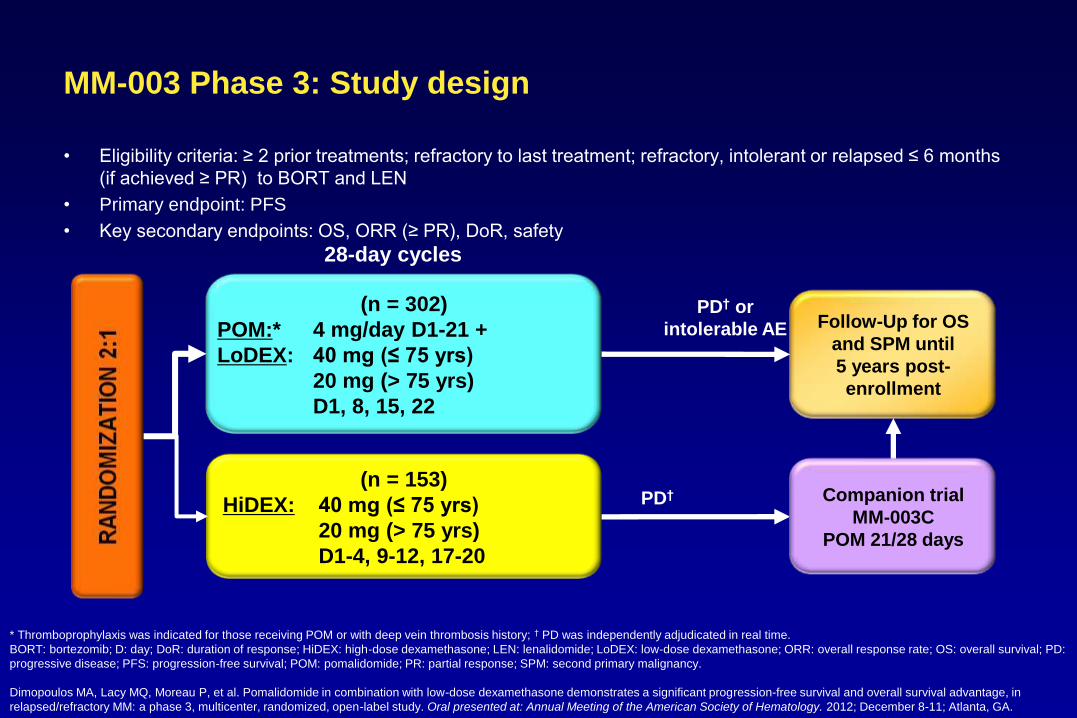
MM-003 Phase 3: Study design
• Eligibility criteria: ≥ 2 prior treatments; refractory to last treatment; refractory, intolerant or relapsed ≤ 6 months
(if achieved ≥ PR) to BORT and LEN
• Primary endpoint: PFS
• Key secondary endpoints: OS, ORR (≥ PR), DoR, safety
* Thromboprophylaxis was indicated for those receiving POM or with deep vein thrombosis history; † PD was independently adjudicated in real time.
BORT: bortezomib; D: day; DoR: duration of response; HiDEX: high-dose dexamethasone; LEN: lenalidomide; LoDEX: low-dose dexamethasone; ORR: overall response rate; OS: overall survival; PD:
progressive disease; PFS: progression-free survival; POM: pomalidomide; PR: partial response; SPM: second primary malignancy.
Dimopoulos MA, Lacy MQ, Moreau P, et al. Pomalidomide in combination with low-dose dexamethasone demonstrates a significant progression-free survival and overall survival advantage, in
relapsed/refractory MM: a phase 3, multicenter, randomized, open-label study. Oral presented at: Annual Meeting of the American Society of Hematology. 2012; December 8-11; Atlanta, GA.
(n = 302)
POM:* 4 mg/day D1-21 +
LoDEX: 40 mg (≤ 75 yrs)
20 mg (> 75 yrs)
D1, 8, 15, 22
Follow-Up for OS
and SPM until
5 years post-
enrollment
(n = 153)
HiDEX: 40 mg (≤ 75 yrs)
20 mg (> 75 yrs)
D1-4, 9-12, 17-20
28-day cycles
PD† or
intolerable AE
PD† Companion trial
MM-003C
POM 21/28 days
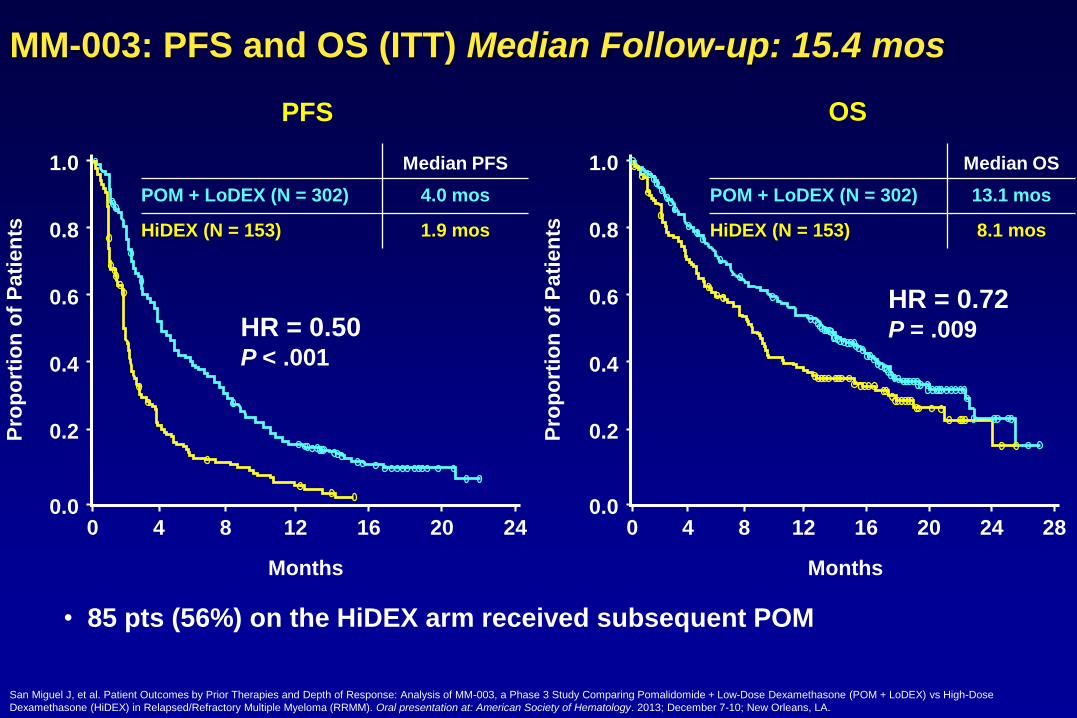
• 85 pts (56%) on the HiDEX arm received subsequent POM
MM-003: PFS and OS (ITT) Median Follow-up: 15.4 mos
0.0
0.2
0.4
0.6
0.8
1.0
4 8 12 16
HR = 0.50P < .001
20 240
Months
Pro
po
rtio
n o
f P
ati
en
ts
0.2
0.4
0.6
0.8
1.0
MonthsP
rop
ort
ion
of
Pati
en
ts4 8 12 16
HR = 0.72 P = .009
20 24 280.0
0
Median PFS
POM + LoDEX (N = 302) 4.0 mos
HiDEX (N = 153) 1.9 mos
Median OS
POM + LoDEX (N = 302) 13.1 mos
HiDEX (N = 153) 8.1 mos
PFS OS
San Miguel J, et al. Patient Outcomes by Prior Therapies and Depth of Response: Analysis of MM-003, a Phase 3 Study Comparing Pomalidomide + Low-Dose Dexamethasone (POM + LoDEX) vs High-Dose
Dexamethasone (HiDEX) in Relapsed/Refractory Multiple Myeloma (RRMM). Oral presentation at: American Society of Hematology. 2013; December 7-10; New Orleans, LA.
29
Registered at ClinicalTrials.gov as NCT01712789 and at EudraCT as 2012-001888-78.AE, adverse event; DoR, duration of response; IMWG, International Myeloma Working Group; LoDEX, low-dose dexamethasone; MM, multiple myeloma; ORR, overall response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; POM, pomalidomide; PR, partial response; SPM, second primary malignancy. Dimopoulos MA, et al. Haematologica. 2015;100 (suppl, abstr P273).
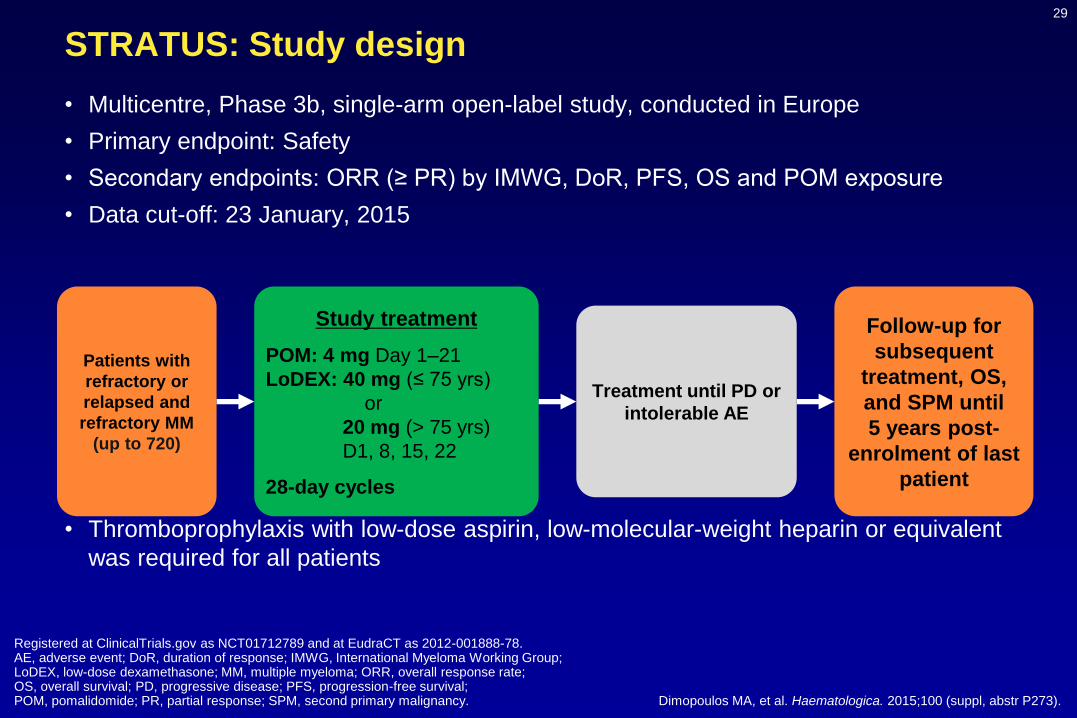
STRATUS: Study design
• Multicentre, Phase 3b, single-arm open-label study, conducted in Europe
• Primary endpoint: Safety
• Secondary endpoints: ORR (≥ PR) by IMWG, DoR, PFS, OS and POM exposure
• Data cut-off: 23 January, 2015
• Thromboprophylaxis with low-dose aspirin, low-molecular-weight heparin or equivalent
was required for all patients
Study treatment
POM: 4 mg Day 1–21
LoDEX: 40 mg (≤ 75 yrs)
or
20 mg (> 75 yrs)
D1, 8, 15, 22
28-day cycles
Treatment until PD or
intolerable AE
Patients with
refractory or
relapsed and
refractory MM
(up to 720)
Follow-up for
subsequent
treatment, OS,
and SPM until
5 years post-
enrolment of last
patient
30
BORT, bortezomib; CFZ, carfilzomib; CrCl, creatinine clearance; ECOG, Eastern Cooperative Oncology Group; ISS, International Staging System; LEN, lenalidomide; LoDEX, low-dose dexamethasone;POM, pomalidomide; SCT, stem cell transplant; THAL, thalidomide. Dimopoulos MA, et al. Haematologica. 2015;100 (suppl, abstr P273).
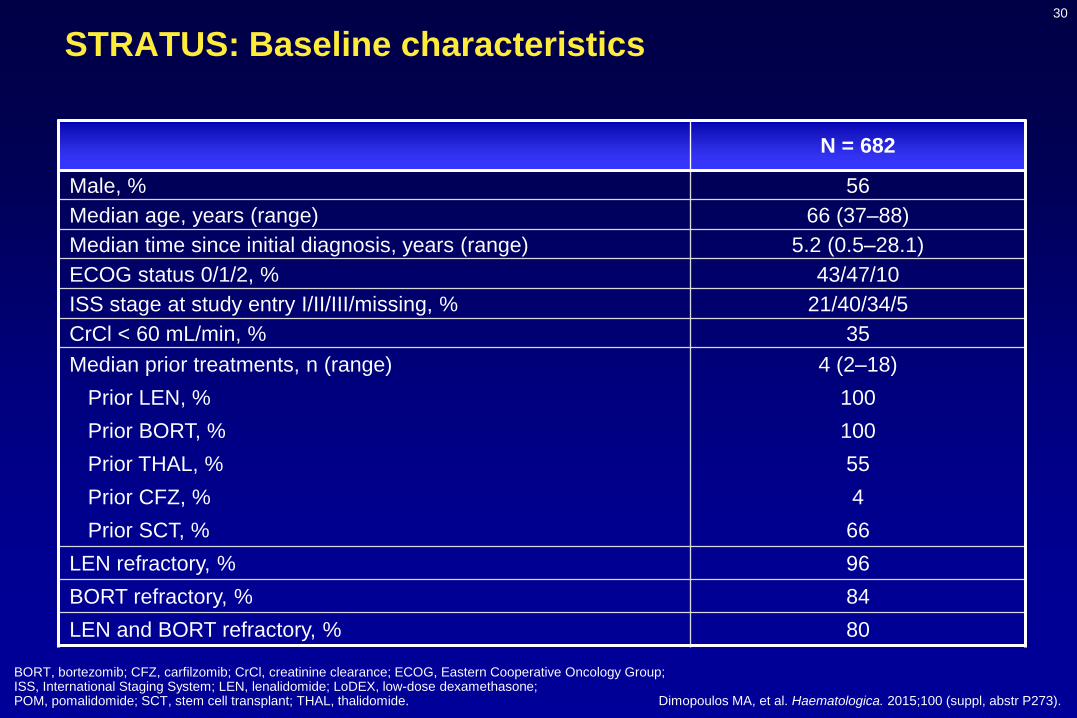
STRATUS: Baseline characteristics
N = 682
Male, % 56
Median age, years (range) 66 (37–88)
Median time since initial diagnosis, years (range) 5.2 (0.5–28.1)
ECOG status 0/1/2, % 43/47/10
ISS stage at study entry I/II/III/missing, % 21/40/34/5
CrCl < 60 mL/min, % 35
Median prior treatments, n (range) 4 (2–18)
Prior LEN, % 100
Prior BORT, % 100
Prior THAL, % 55
Prior CFZ, % 4
Prior SCT, % 66
LEN refractory, % 96
BORT refractory, % 84
LEN and BORT refractory, % 80
31
BORT, bortezomib; ITT, intent to treat; LEN, lenalidomide; OS, overall survival; PFS, progression-free survival. Dimopoulos MA, et al. Haematologica. 2015;100 (suppl, abstr P273).
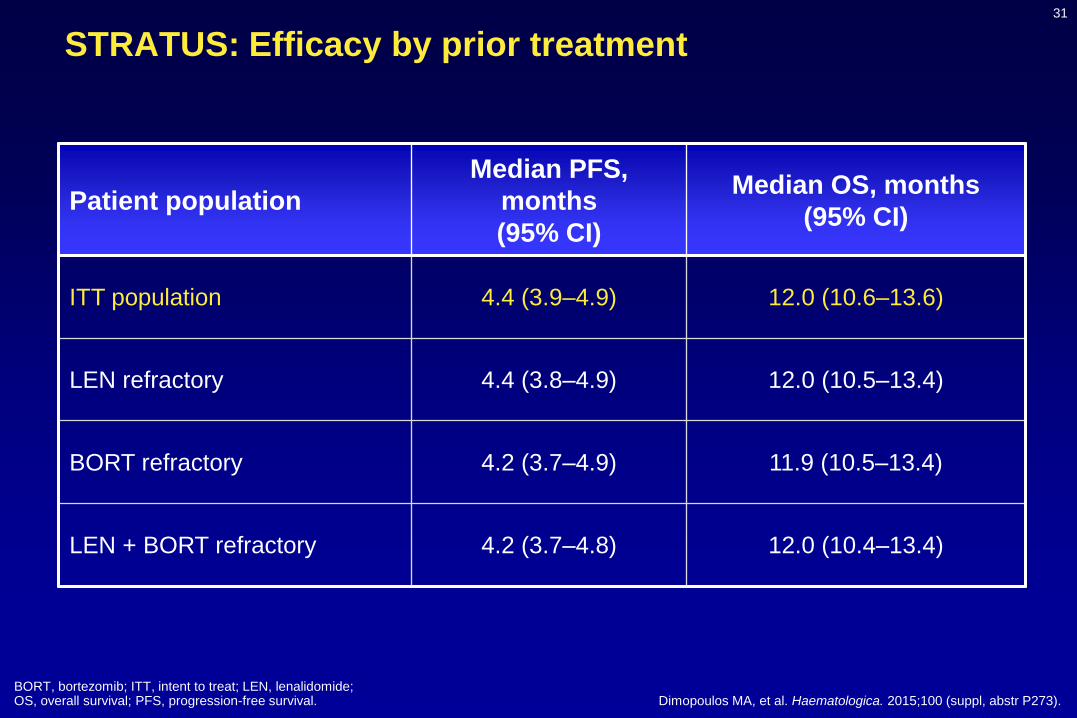
STRATUS: Efficacy by prior treatment
Patient population
Median PFS,
months
(95% CI)
Median OS, months
(95% CI)
ITT population 4.4 (3.9–4.9) 12.0 (10.6–13.6)
LEN refractory 4.4 (3.8–4.9) 12.0 (10.5–13.4)
BORT refractory 4.2 (3.7–4.9) 11.9 (10.5–13.4)
LEN + BORT refractory 4.2 (3.7–4.8) 12.0 (10.4–13.4)
32
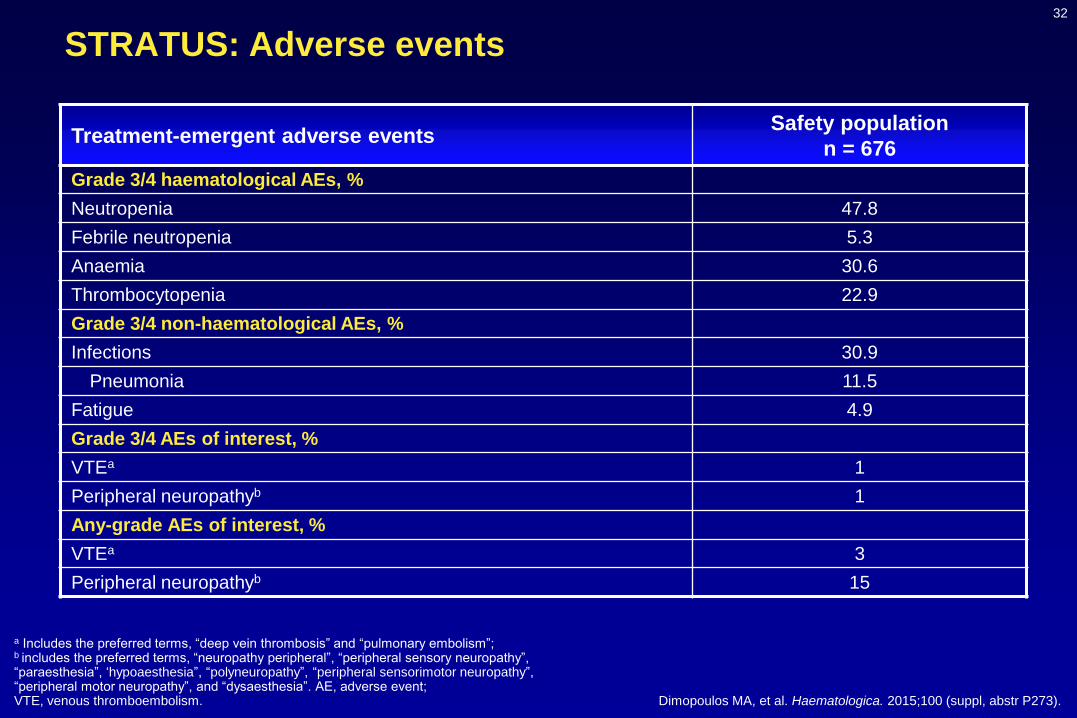
a Includes the preferred terms, “deep vein thrombosis” and “pulmonary embolism”; b includes the preferred terms, “neuropathy peripheral”, “peripheral sensory neuropathy”, “paraesthesia”, ‘hypoaesthesia”, “polyneuropathy”, “peripheral sensorimotor neuropathy”, “peripheral motor neuropathy”, and “dysaesthesia”. AE, adverse event; VTE, venous thromboembolism. Dimopoulos MA, et al. Haematologica. 2015;100 (suppl, abstr P273).
STRATUS: Adverse events
Treatment-emergent adverse eventsSafety population
n = 676
Grade 3/4 haematological AEs, %
Neutropenia 47.8
Febrile neutropenia 5.3
Anaemia 30.6
Thrombocytopenia 22.9
Grade 3/4 non-haematological AEs, %
Infections 30.9
Pneumonia 11.5
Fatigue 4.9
Grade 3/4 AEs of interest, %
VTEa 1
Peripheral neuropathyb 1
Any-grade AEs of interest, %
VTEa 3
Peripheral neuropathyb 15
Switch
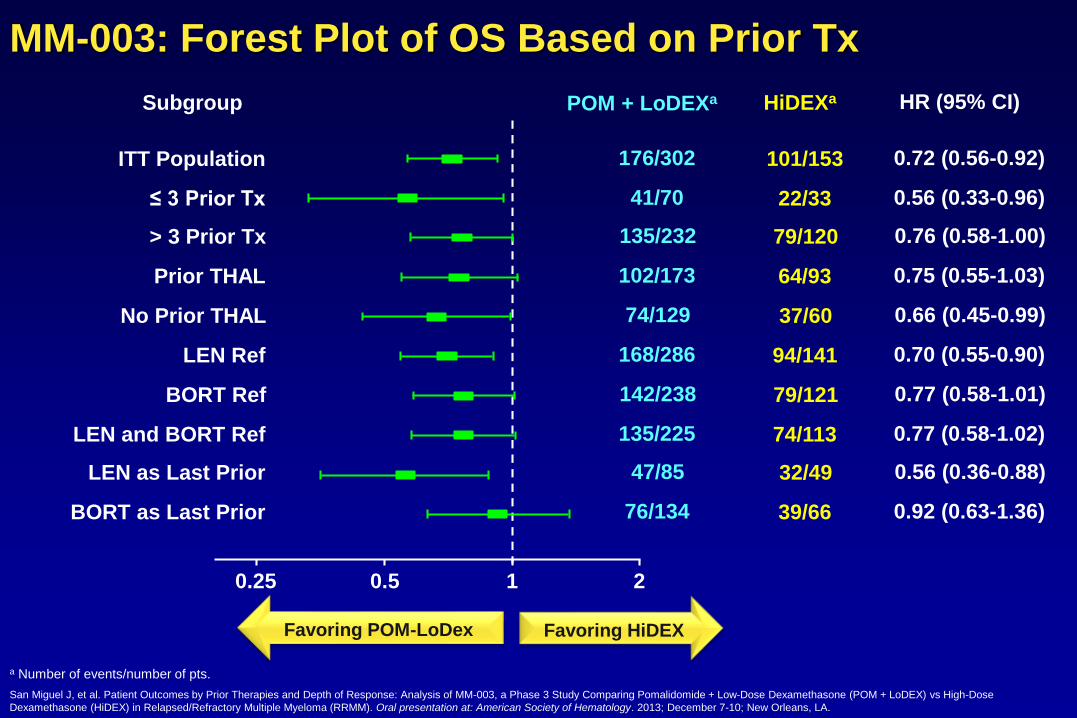
MM-003: Forest Plot of OS Based on Prior Tx
a Number of events/number of pts.
Subgroup HiDEXa HR (95% CI)
0.72 (0.56-0.92)
0.56 (0.33-0.96)
0.76 (0.58-1.00)
0.75 (0.55-1.03)
0.66 (0.45-0.99)
0.70 (0.55-0.90)
0.77 (0.58-1.01)
0.77 (0.58-1.02)
0.56 (0.36-0.88)
0.92 (0.63-1.36)
101/153
22/33
79/120
64/93
37/60
94/141
79/121
74/113
32/49
39/66
176/302
41/70
135/232
102/173
74/129
168/286
142/238
135/225
47/85
76/134
ITT Population
≤ 3 Prior Tx
> 3 Prior Tx
Prior THAL
No Prior THAL
LEN Ref
BORT Ref
LEN and BORT Ref
LEN as Last Prior
BORT as Last Prior
POM + LoDEXa
0.25 0.5 1 2
Favoring POM-LoDex Favoring HiDEX
San Miguel J, et al. Patient Outcomes by Prior Therapies and Depth of Response: Analysis of MM-003, a Phase 3 Study Comparing Pomalidomide + Low-Dose Dexamethasone (POM + LoDEX) vs High-Dose
Dexamethasone (HiDEX) in Relapsed/Refractory Multiple Myeloma (RRMM). Oral presentation at: American Society of Hematology. 2013; December 7-10; New Orleans, LA.
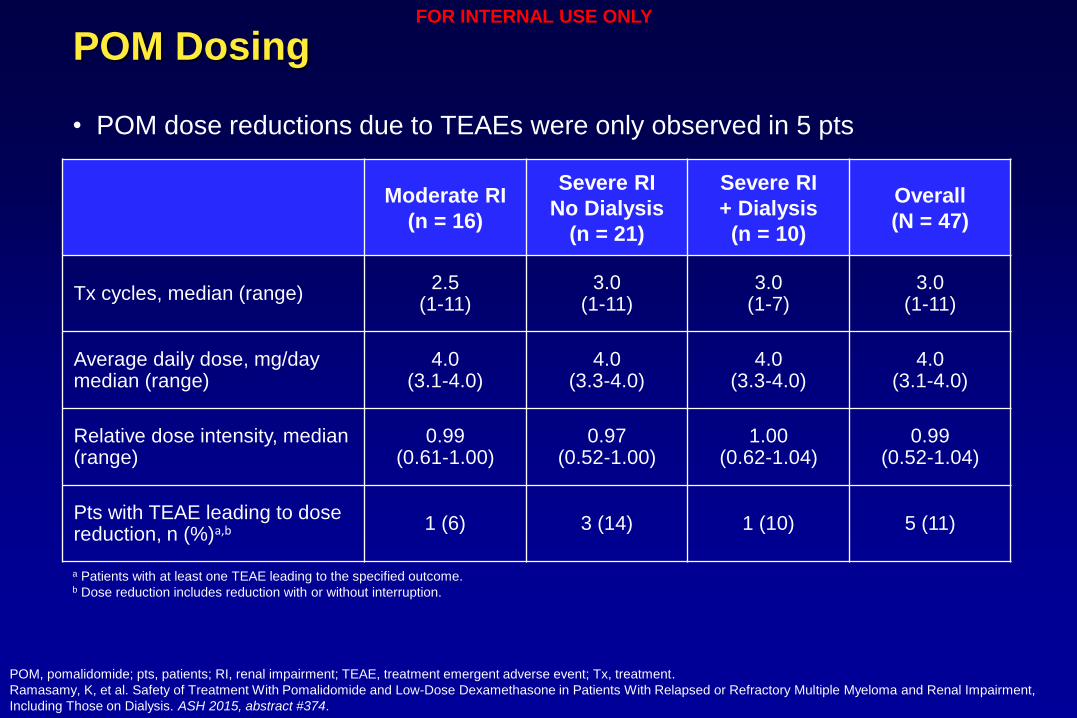
Pomalidomide and Kidney
Moderate RI
(n = 16)
Severe RI
No Dialysis
(n = 21)
Severe RI
+ Dialysis
(n = 10)
Overall
(N = 47)
Tx cycles, median (range)2.5
(1-11)3.0
(1-11)3.0
(1-7)3.0
(1-11)
Average daily dose, mg/day median (range)
4.0(3.1-4.0)
4.0(3.3-4.0)
4.0(3.3-4.0)
4.0(3.1-4.0)
Relative dose intensity, median (range)
0.99(0.61-1.00)
0.97(0.52-1.00)
1.00(0.62-1.04)
0.99(0.52-1.04)
Pts with TEAE leading to dose reduction, n (%)a,b 1 (6) 3 (14) 1 (10) 5 (11)
POM Dosing
POM, pomalidomide; pts, patients; RI, renal impairment; TEAE, treatment emergent adverse event; Tx, treatment.
Ramasamy, K, et al. Safety of Treatment With Pomalidomide and Low-Dose Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma and Renal Impairment,
Including Those on Dialysis. ASH 2015, abstract #374.
• POM dose reductions due to TEAEs were only observed in 5 pts
a Patients with at least one TEAE leading to the specified outcome.b Dose reduction includes reduction with or without interruption.
FOR INTERNAL USE ONLY
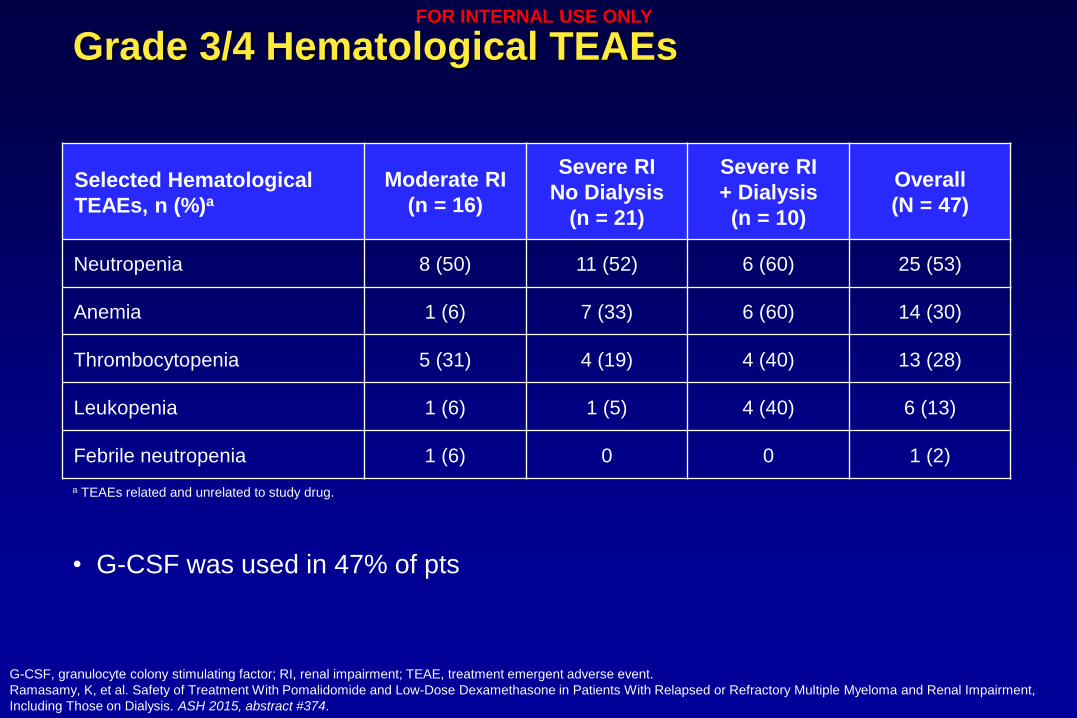
Grade 3/4 Hematological TEAEs
Selected Hematological
TEAEs, n (%)a
Moderate RI
(n = 16)
Severe RI
No Dialysis
(n = 21)
Severe RI
+ Dialysis
(n = 10)
Overall
(N = 47)
Neutropenia 8 (50) 11 (52) 6 (60) 25 (53)
Anemia 1 (6) 7 (33) 6 (60) 14 (30)
Thrombocytopenia 5 (31) 4 (19) 4 (40) 13 (28)
Leukopenia 1 (6) 1 (5) 4 (40) 6 (13)
Febrile neutropenia 1 (6) 0 0 1 (2)
G-CSF, granulocyte colony stimulating factor; RI, renal impairment; TEAE, treatment emergent adverse event.
Ramasamy, K, et al. Safety of Treatment With Pomalidomide and Low-Dose Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma and Renal Impairment,
Including Those on Dialysis. ASH 2015, abstract #374.
• G-CSF was used in 47% of pts
a TEAEs related and unrelated to study drug.
FOR INTERNAL USE ONLY
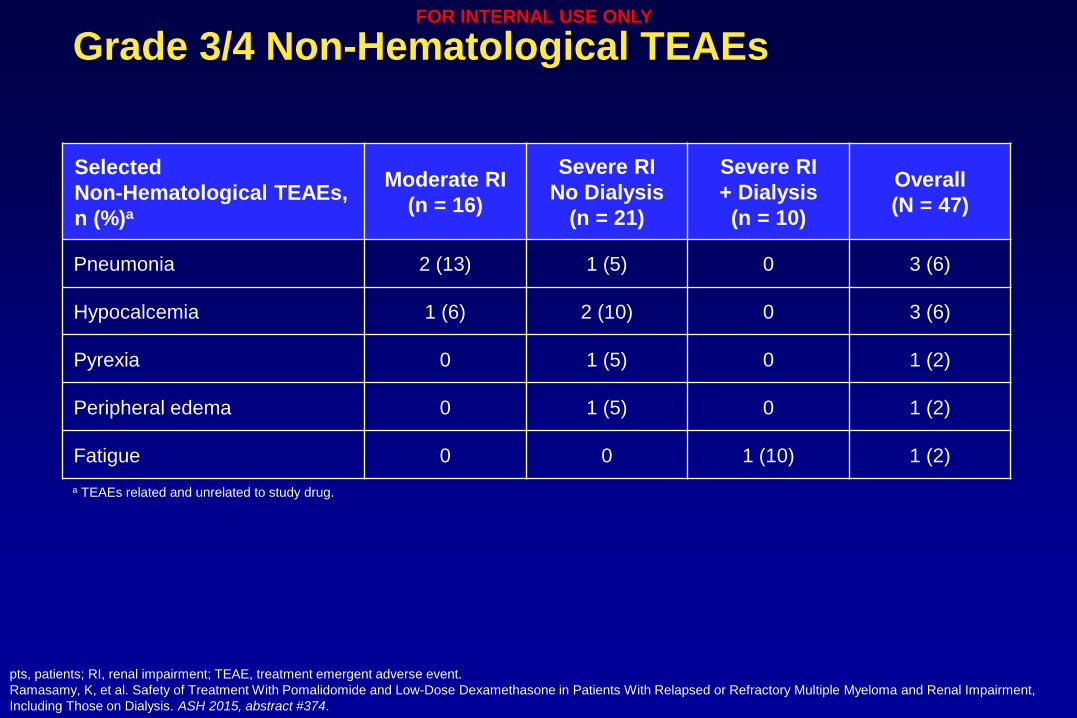
Grade 3/4 Non-Hematological TEAEs
pts, patients; RI, renal impairment; TEAE, treatment emergent adverse event.
Ramasamy, K, et al. Safety of Treatment With Pomalidomide and Low-Dose Dexamethasone in Patients With Relapsed or Refractory Multiple Myeloma and Renal Impairment,
Including Those on Dialysis. ASH 2015, abstract #374.
Selected
Non-Hematological TEAEs,
n (%)a
Moderate RI
(n = 16)
Severe RI
No Dialysis
(n = 21)
Severe RI
+ Dialysis
(n = 10)
Overall
(N = 47)
Pneumonia 2 (13) 1 (5) 0 3 (6)
Hypocalcemia 1 (6) 2 (10) 0 3 (6)
Pyrexia 0 1 (5) 0 1 (2)
Peripheral edema 0 1 (5) 0 1 (2)
Fatigue 0 0 1 (10) 1 (2)
a TEAEs related and unrelated to study drug.
FOR INTERNAL USE ONLY
39
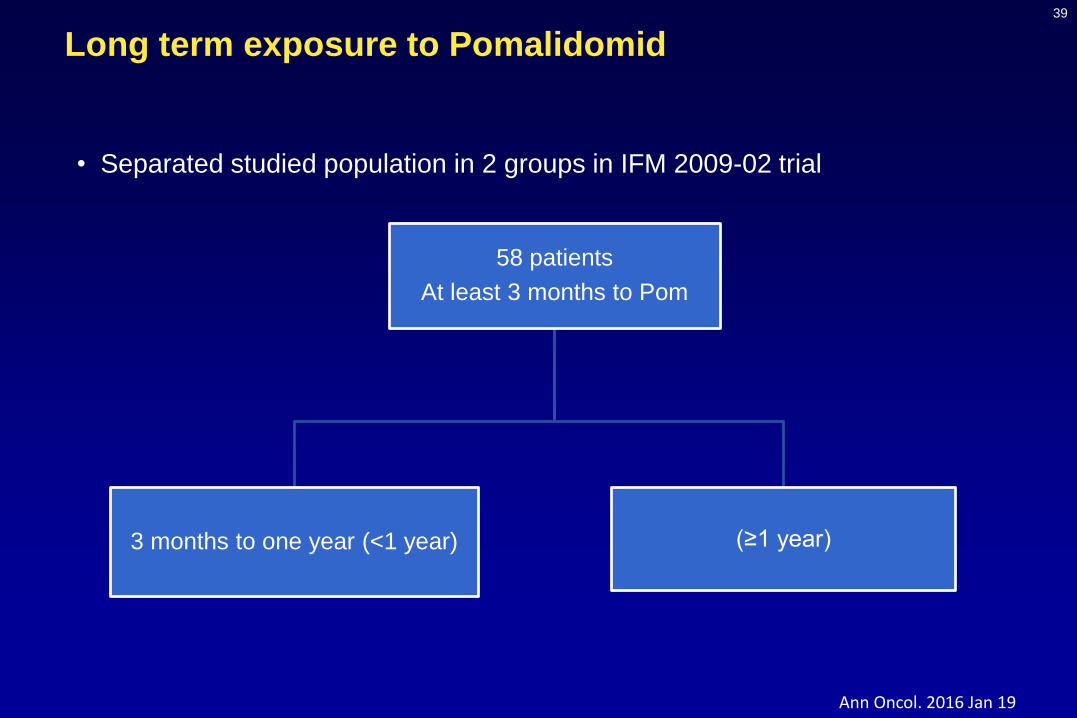
• Separated studied population in 2 groups in IFM 2009-02 trial
Long term exposure to Pomalidomid
58 patients
At least 3 months to Pom
3 months to one year (<1 year) (≥1 year)
Ann Oncol. 2016 Jan 19
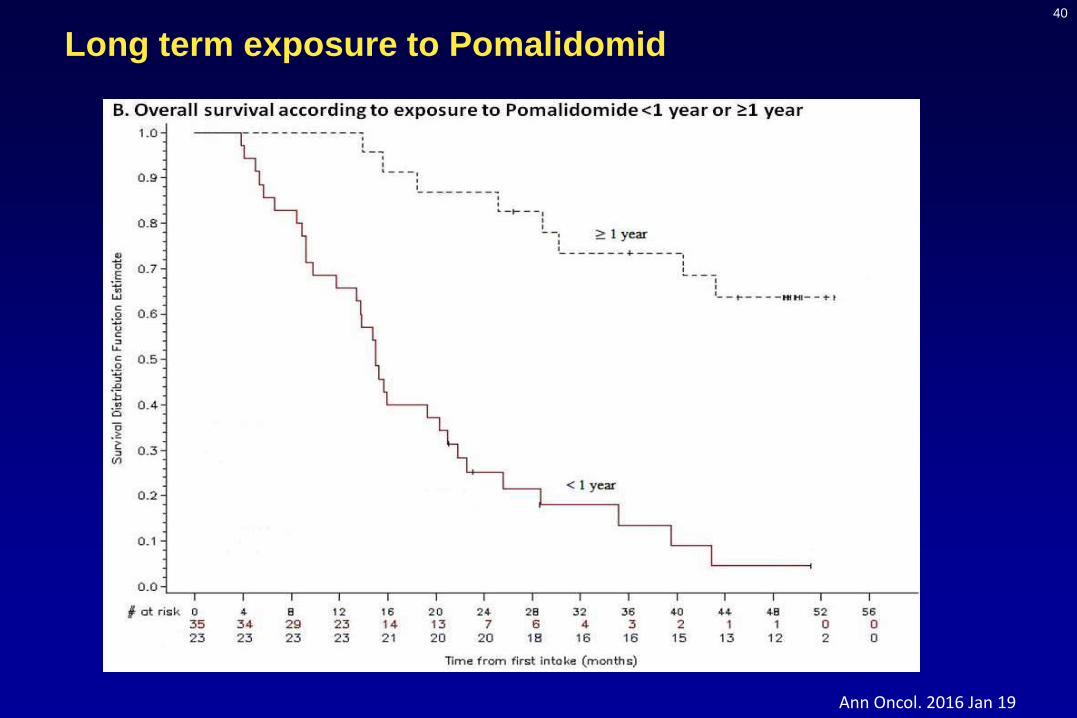
40
Long term exposure to Pomalidomid
Ann Oncol. 2016 Jan 19
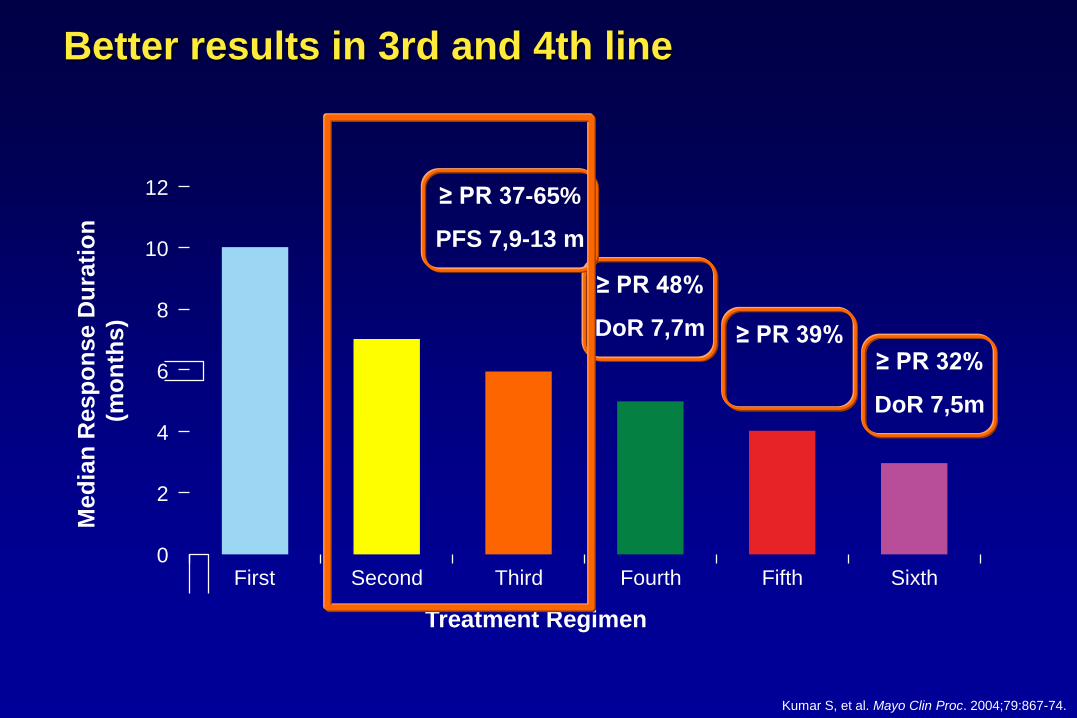
Better results in 3rd and 4th line
Treatment Regimen
Med
ian
Resp
on
se D
ura
tio
n
(mo
nth
s)
12
8
4
2
0
6
10
First Third SixthSecond Fourth Fifth
Kumar S, et al. Mayo Clin Proc. 2004;79:867-74.Kumar S, et al. Mayo Clin Proc. 2004;79:867-74.
≥ PR 32%
DoR 7,5m
≥ PR 39%
≥ PR 48%
DoR 7,7m
≥ PR 37-65%
PFS 7,9-13 m
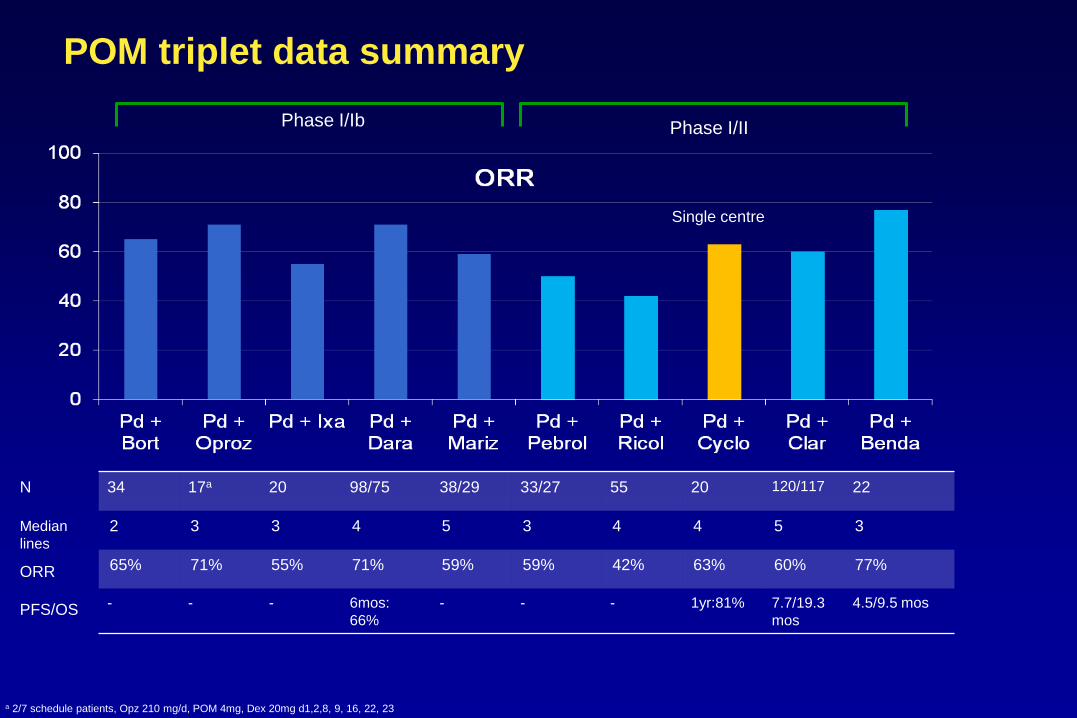
POM triplet data summary
34 17a 20 98/75 38/29 33/27 55 20 120/117 22
2 3 3 4 5 3 4 4 5 3
65% 71% 55% 71% 59% 59% 42% 63% 60% 77%
- - - 6mos:
66%
- - - 1yr:81% 7.7/19.3
mos
4.5/9.5 mos
N
Median
lines
ORR
PFS/OS
Phase I/IIPhase I/Ib
Single centre
a 2/7 schedule patients, Opz 210 mg/d, POM 4mg, Dex 20mg d1,2,8, 9, 16, 22, 23
Clinical Efficacy of Daratumumab
Monotherapy in Patients With Heavily
Pretreated Relapsed or Refractory
Multiple MyelomaSaad Z. Usmani, MD1; Brendan M. Weiss, MD2; Nizar J. Bahlis, MD3; Andrew Belch, MD4; Sagar Lonial, MD5; Henk M. Lokhorst, MD6; Peter M. Voorhees, MD7; Paul G.
Richardson, MD8; A. Kate Sasser, PhD9; Amy Axel PhD9; Huaibao Feng, PhD10;Clarissa M. Uhlar, PhD9; Jianping Wang, PhD9; Imran Khan, MD10; Tahamtan Ahmadi,
MD9; Hareth Nahi, MD11
1Levine Cancer Institute/Carolinas HealthCare System, Charlotte, NC, USA; 2Division of Hematology-Oncology, Department of Medicine, Abramson Cancer Center and Perelman School of Medicine, University of Pennsylvania,
Philadelphia, PA, USA; 3Tom Baker Cancer Center–University of Calgary, Calgary, AB, Canada; 4Cross Cancer Institute, Edmonton, AB, Canada; 5Department of Hematology and Medical Oncology, Winship Cancer Institute, Emory University, Atlanta, GA, USA; 6Department of Hematology, VU University Medical Center, Amsterdam, The Netherlands;
7Division of Hematology/Oncology, Lineberger Comprehensive Cancer Center, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA; 8Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA, USA; 9Janssen
Research & Development, LLC, Spring House, PA, USA; 10Janssen Research & Development, LLC, Raritan, NJ, USA; 11Karolinska Institute, Department of Medicine, Division of Hematology, Karolinska University Hospital at Huddinge,
Stockholm, Sweden.
43
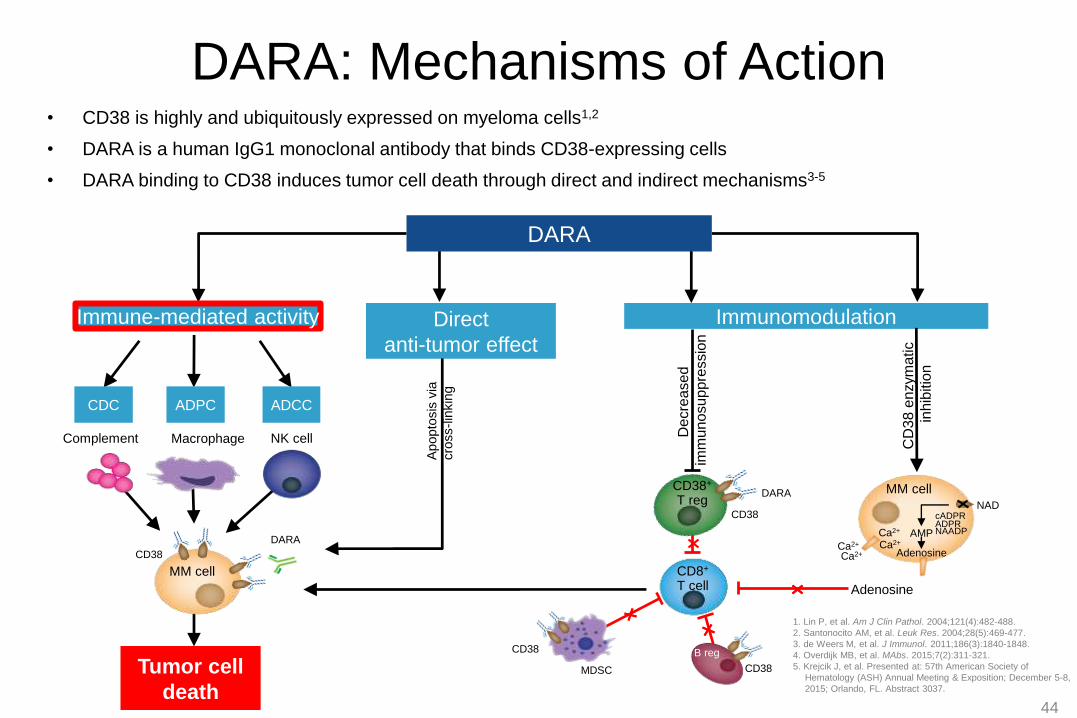
DARA: Mechanisms of Action• CD38 is highly and ubiquitously expressed on myeloma cells1,2
• DARA is a human IgG1 monoclonal antibody that binds CD38-expressing cells
• DARA binding to CD38 induces tumor cell death through direct and indirect mechanisms3-5
Immunomodulation
MM cell
CD38
DARA
NK cellMacrophageComplement
Immune-mediated activity
ADPC ADCCCDC
DARA
Tumor cell
death
1. Lin P, et al. Am J Clin Pathol. 2004;121(4):482-488.
2. Santonocito AM, et al. Leuk Res. 2004;28(5):469-477.
3. de Weers M, et al. J Immunol. 2011;186(3):1840-1848.
4. Overdijk MB, et al. MAbs. 2015;7(2):311-321.
5. Krejcik J, et al. Presented at: 57th American Society of
Hematology (ASH) Annual Meeting & Exposition; December 5-8,
2015; Orlando, FL. Abstract 3037.
44
Adenosine
CD8+
T cell
CD38
CD38
MDSC
B reg
CD38+
T regDARA
CD38
De
cre
ase
d
imm
uno
sup
pre
ssio
n
cADPRADPRNAADP
Ca2+
NAD
MM cell
Adenosine
AMP
Ca2+
Ca2+
Ca2+
CD
38 e
nzym
atic
inhib
itio
n
Direct
anti-tumor effect
Apopto
sis
via
cro
ss-lin
kin
g
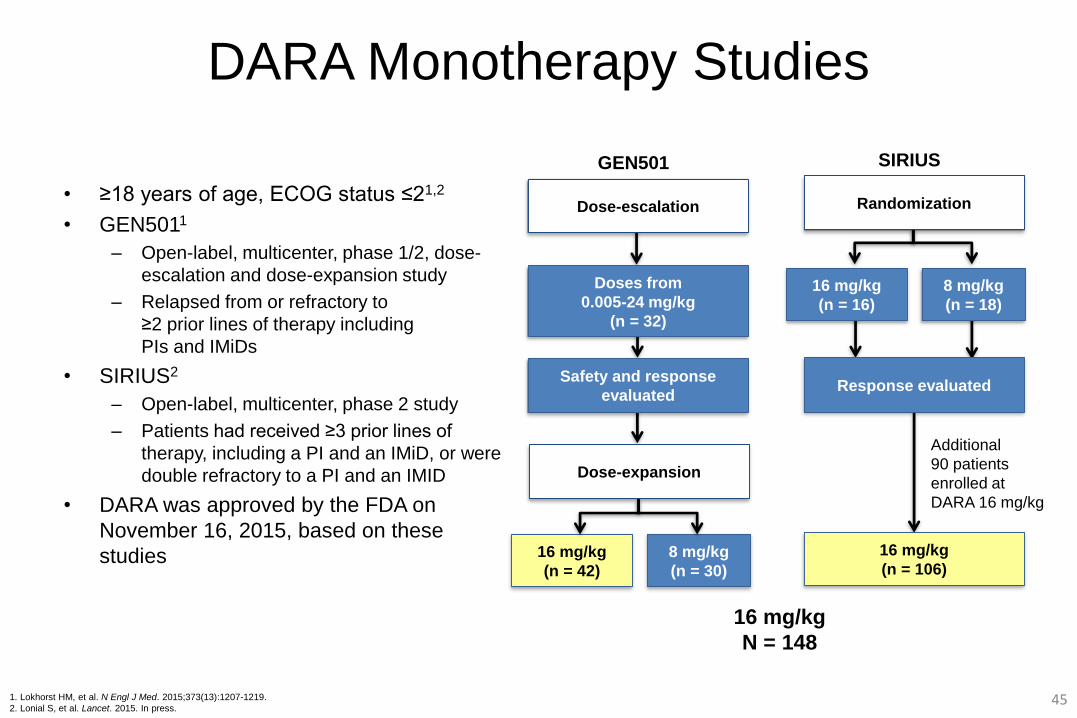
DARA Monotherapy Studies
• ≥18 years of age, ECOG status ≤21,2
• GEN5011
– Open-label, multicenter, phase 1/2, dose-
escalation and dose-expansion study
– Relapsed from or refractory to
≥2 prior lines of therapy including
PIs and IMiDs
• SIRIUS2
– Open-label, multicenter, phase 2 study
– Patients had received ≥3 prior lines of
therapy, including a PI and an IMiD, or were
double refractory to a PI and an IMID
• DARA was approved by the FDA on
November 16, 2015, based on these
studies
16 mg/kg
(n = 16)
8 mg/kg
(n = 18)
16 mg/kg
(n = 106)
Response evaluated
Randomization
Additional
90 patients
enrolled at
DARA 16 mg/kg
SIRIUS
Safety and response
evaluated
Dose-escalation
Doses from
0.005-24 mg/kg
(n = 32)
Dose-expansion
GEN501
16 mg/kg
(n = 42)
8 mg/kg
(n = 30)
1. Lokhorst HM, et al. N Engl J Med. 2015;373(13):1207-1219.
2. Lonial S, et al. Lancet. 2015. In press.
16 mg/kg
N = 148
45
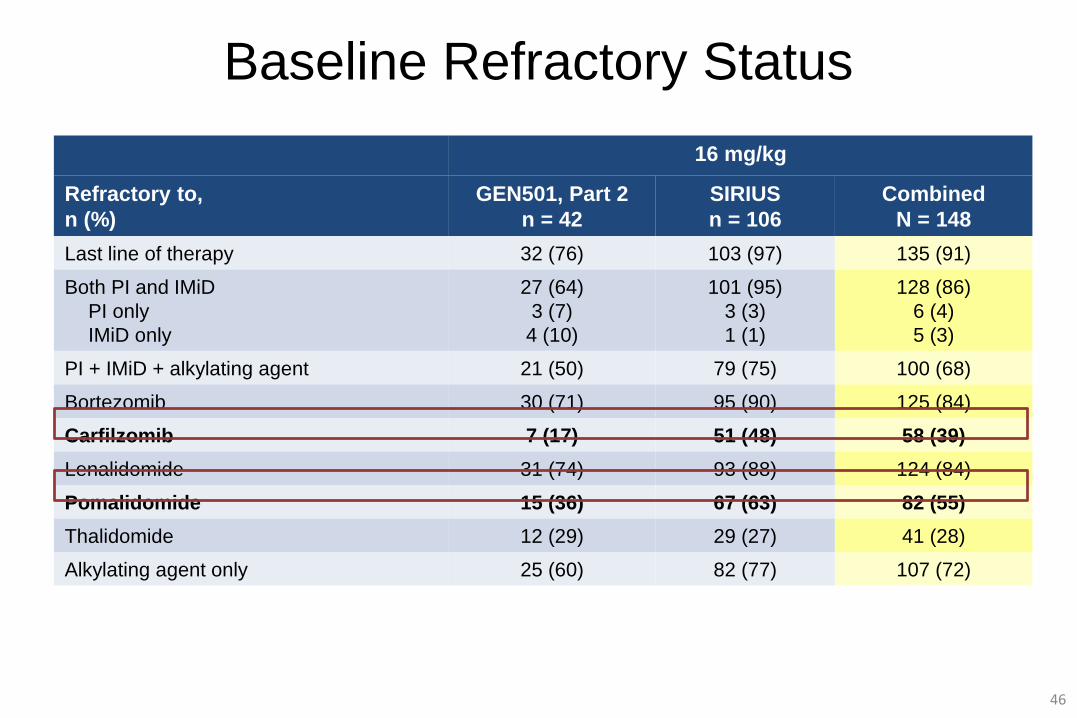
Baseline Refractory Status
16 mg/kg
Refractory to,
n (%)
GEN501, Part 2
n = 42
SIRIUS
n = 106
Combined
N = 148
Last line of therapy 32 (76) 103 (97) 135 (91)
Both PI and IMiD
PI only
IMiD only
27 (64)
3 (7)
4 (10)
101 (95)
3 (3)
1 (1)
128 (86)
6 (4)
5 (3)
PI + IMiD + alkylating agent 21 (50) 79 (75) 100 (68)
Bortezomib 30 (71) 95 (90) 125 (84)
Carfilzomib 7 (17) 51 (48) 58 (39)
Lenalidomide 31 (74) 93 (88) 124 (84)
Pomalidomide 15 (36) 67 (63) 82 (55)
Thalidomide 12 (29) 29 (27) 41 (28)
Alkylating agent only 25 (60) 82 (77) 107 (72)
46
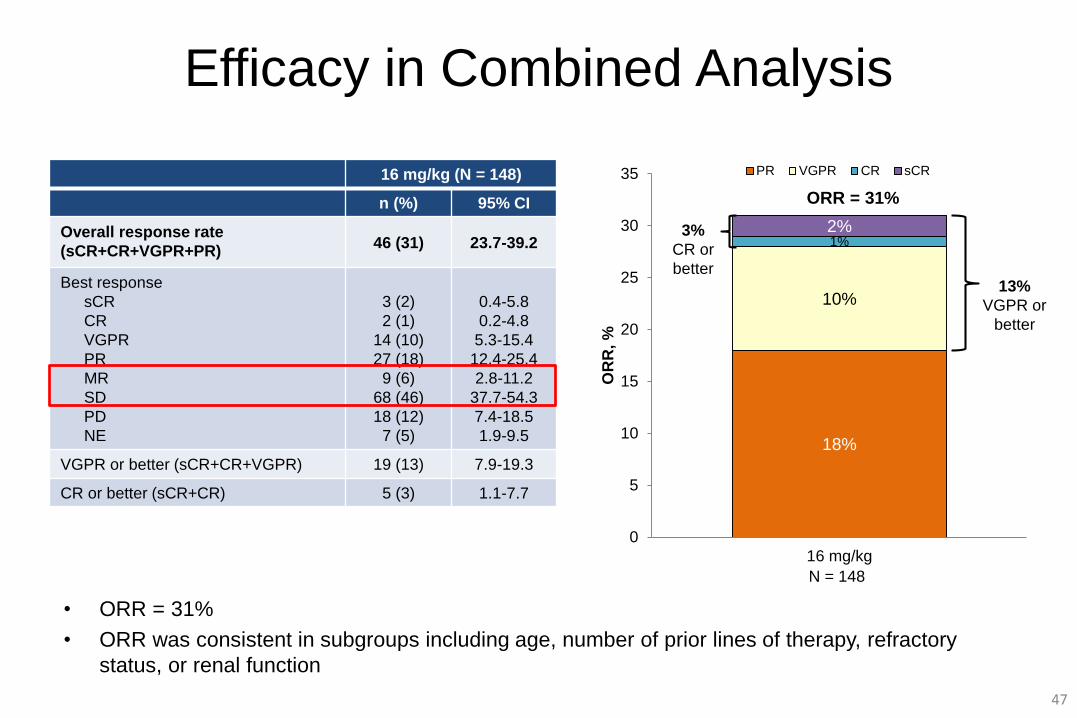
Efficacy in Combined Analysis
18%
10%
1%2%
0
5
10
15
20
25
30
35
16 mg/kg
OR
R, %
PR VGPR CR sCR
ORR = 31%
16 mg/kg (N = 148)
n (%) 95% CI
Overall response rate
(sCR+CR+VGPR+PR)46 (31) 23.7-39.2
Best response
sCR
CR
VGPR
PR
MR
SD
PD
NE
3 (2)
2 (1)
14 (10)
27 (18)
9 (6)
68 (46)
18 (12)
7 (5)
0.4-5.8
0.2-4.8
5.3-15.4
12.4-25.4
2.8-11.2
37.7-54.3
7.4-18.5
1.9-9.5
VGPR or better (sCR+CR+VGPR) 19 (13) 7.9-19.3
CR or better (sCR+CR) 5 (3) 1.1-7.7
• ORR = 31%
• ORR was consistent in subgroups including age, number of prior lines of therapy, refractory
status, or renal function
47
3%
CR or
better13%
VGPR or
better
N = 148
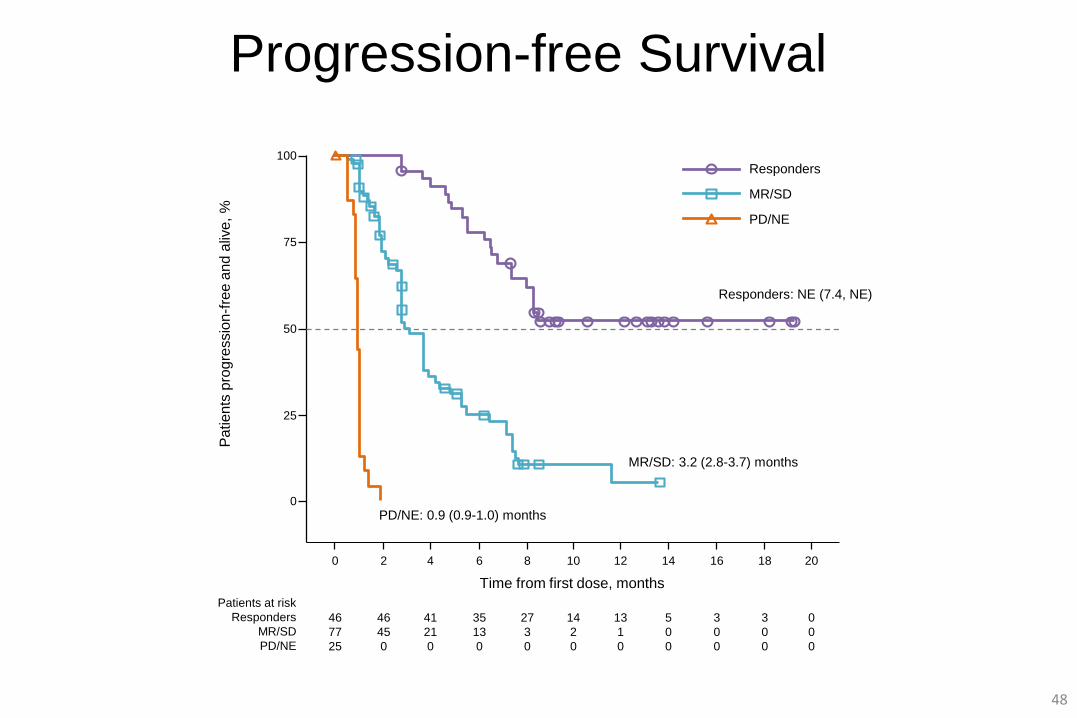
Progression-free Survival
Responders: NE (7.4, NE)
MR/SD: 3.2 (2.8-3.7) months
PD/NE: 0.9 (0.9-1.0) months
48
0
Pa
tien
ts p
rog
ressio
n-f
ree a
nd
aliv
e,
%
2 6 8 12 14 18 20
Time from first dose, months
Patients at risk
Responders
MR/SD
PD/NE
0
25
50
75
100
4 10 16
Responders
MR/SD
PD/NE
46
77
25
46
45
0
35
13
0
27
3
0
13
1
0
5
0
0
3
0
0
0
0
0
41
21
0
14
2
0
3
0
0
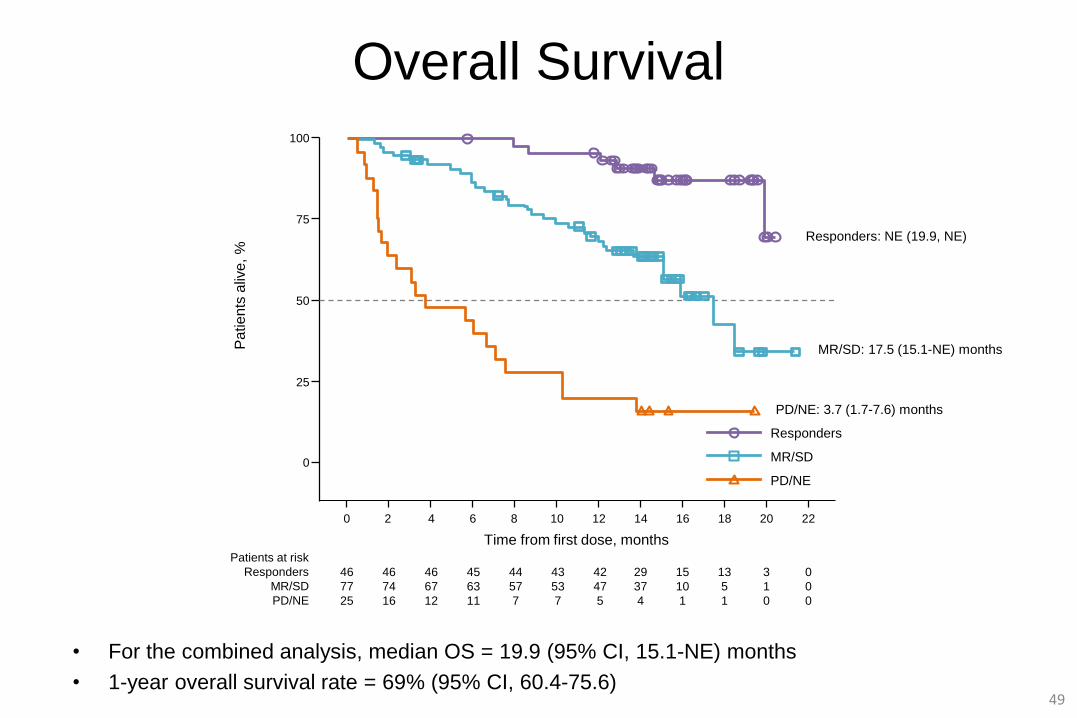
Overall Survival
• For the combined analysis, median OS = 19.9 (95% CI, 15.1-NE) months
• 1-year overall survival rate = 69% (95% CI, 60.4-75.6)49
0
Pa
tien
ts a
live
, %
2 6 8 12 14 18 22
Time from first dose, monthsPatients at risk
Responders
MR/SD
PD/NE
Responders
0
25
50
75
100
4 10 16
MR/SD
PD/NE
46
77
25
46
74
16
45
63
11
44
57
7
42
47
5
29
37
4
3
1
0
0
0
0
46
67
12
43
53
7
15
10
1
20
13
5
1
Responders: NE (19.9, NE)
MR/SD: 17.5 (15.1-NE) months
PD/NE: 3.7 (1.7-7.6) months
Fresh biopsy
Fresh biopsy
Patient encounter
Genomic
profiling
Data interpretation
Management decision
Clinical response?
Drug resistance?
Salvage or new therapy?
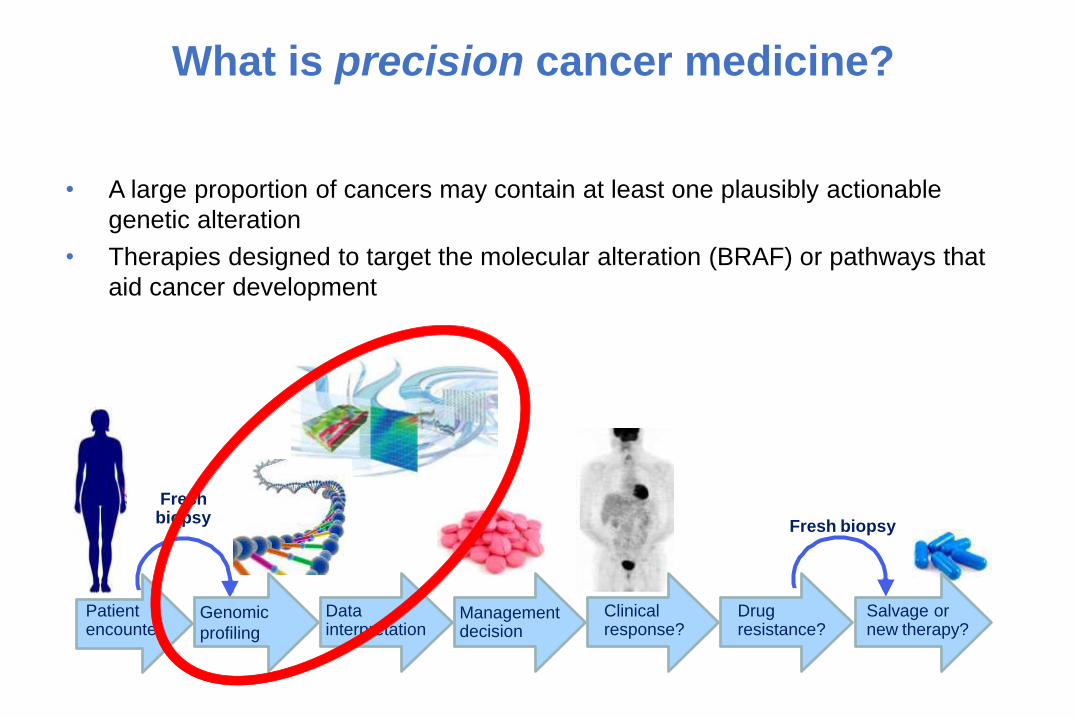
What is precision cancer medicine?
• A large proportion of cancers may contain at least one plausibly actionable
genetic alteration
• Therapies designed to target the molecular alteration (BRAF) or pathways that
aid cancer development
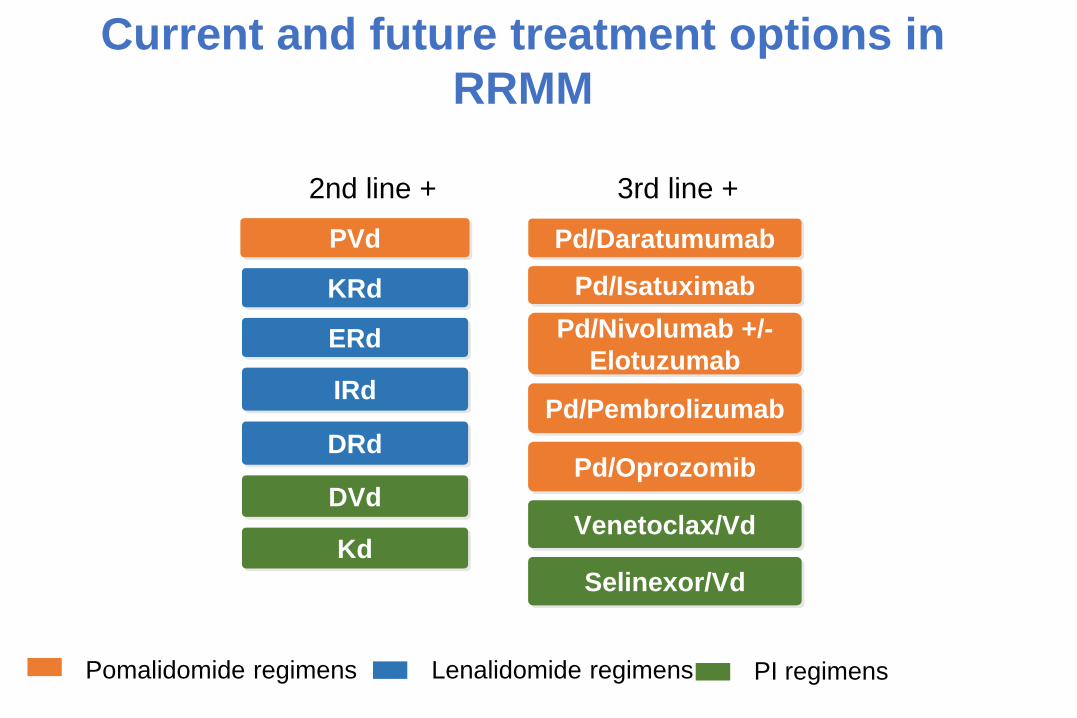
Current and future treatment options in
RRMM
Pd/Nivolumab +/-
Elotuzumab
Pomalidomide regimens
PVd
Pd/Isatuximab
Pd/Pembrolizumab
Pd/Daratumumab
KRd
ERd
IRd
DRd
DVd
Lenalidomide regimens PI regimens
Venetoclax/Vd
Selinexor/Vd
Kd
Pd/Oprozomib
3rd line +2nd line +
Immunotherapy
- Naïve
Tested for long, always failed
Anti CD138, Il6R, IgF1R…
Most recent anti CS1/SLAMF7/Elotuzumab
Succes = AntiCD38
- Conjugated = failure
Vedotin/MMAE
Maybe IFN
- Vaccination = failure
- Armed
Car T cells
BiTEs
…
Phase 1b Study of Daratumumab Plus Pomalidomide and Dexamethasone in Relapsed and/or Refractory Multiple
Myeloma (RRMM) With ≥2 Prior Lines of Therapy
Ajai Chari,1 Attaya Suvannasankha,2 Joseph W. Fay,3 Bertrand Arnulf,4 Jonathan Kaufman,5 Jainulabdeen J. Ifthikharuddin,6 Brendan Weiss,7 Amrita Krishnan,8
Suzanne Lentzsch,9 Raymond Comenzo,10 Jianping Wang,11 Tara Masterson,12
Kerri Nottage,11 Jordan Schecter,11 Christopher Chiu,12 Nushmia Khokhar,12
Tahamtan Ahmadi,12 Sagar Lonial5
ClinicalTrials.gov Identifier:
NCT01998971
1Tisch Cancer Institute, Mount Sinai School of Medicine, New York, NY, USA; 2Indiana University School of Medicine and Simon Cancer Center,
Richard L. Roudebush VAMC, Indianapolis, IN, USA; 3Baylor Institute for Immunology Research, Dallas, TX, USA; 4Hôpital Saint Louis, Paris,
France; 5Department of Hematology and Medical Oncology,
Winship Cancer Institute, Emory University, Atlanta, GA, USA; 6James P. Wilmot Cancer Center, University of Rochester Strong Memorial Hospital,
Rochester, NY, USA; 7Abramson Cancer Center and Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA; 8The Judy and Bernard Briskin
Myeloma Center, City of Hope,
Duarte, CA, USA; 9Columbia University Medical Center, New York, NY, USA; 10Division of Hematology-Oncology, Tufts Medical Center, Boston, MA,
USA; 11Janssen Research & Development, Raritan, NJ, USA; 12Janssen Research & Development, Spring House, PA, USA.
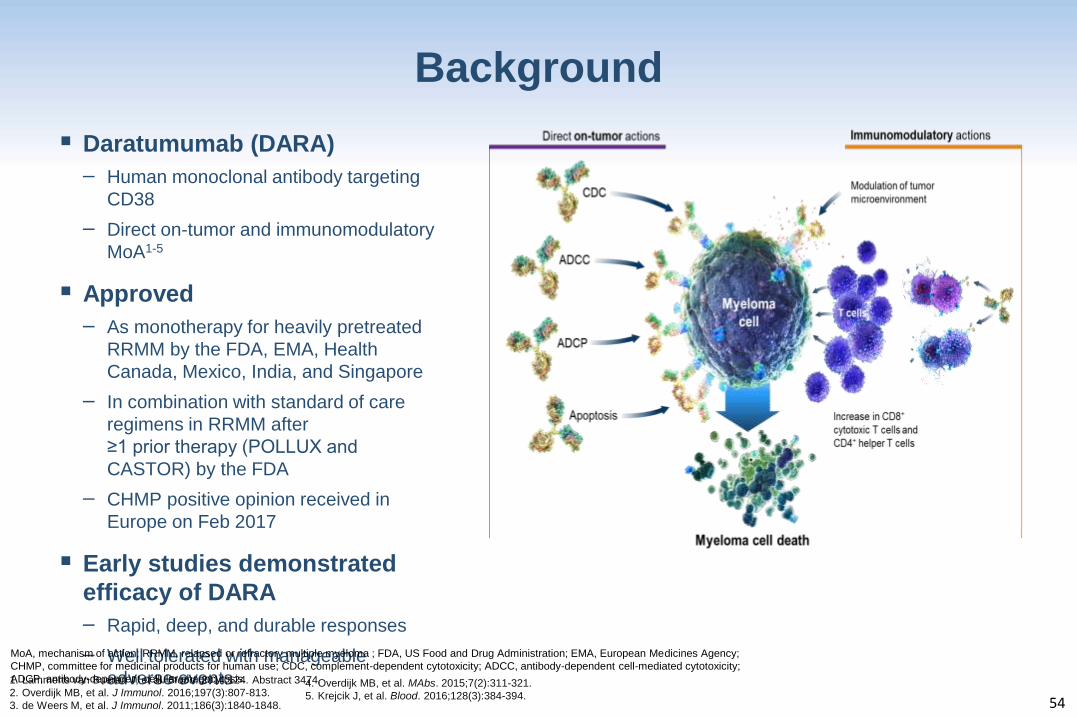
Background
▪ Daratumumab (DARA)
– Human monoclonal antibody targeting
CD38
– Direct on-tumor and immunomodulatory
MoA1-5
▪ Approved
– As monotherapy for heavily pretreated
RRMM by the FDA, EMA, Health
Canada, Mexico, India, and Singapore
– In combination with standard of care
regimens in RRMM after
≥1 prior therapy (POLLUX and
CASTOR) by the FDA
– CHMP positive opinion received in
Europe on Feb 2017
▪ Early studies demonstrated
efficacy of DARA
– Rapid, deep, and durable responses
– Well tolerated with manageable
adverse events
54
1. Lammerts van Bueren J, et al. Blood. 2014;124. Abstract 3474.
2. Overdijk MB, et al. J Immunol. 2016;197(3):807-813.
3. de Weers M, et al. J Immunol. 2011;186(3):1840-1848.
4. Overdijk MB, et al. MAbs. 2015;7(2):311-321.
5. Krejcik J, et al. Blood. 2016;128(3):384-394.
MoA, mechanism of action; RRMM, relapsed or refractory multiple myeloma ; FDA, US Food and Drug Administration; EMA, European Medicines Agency;
CHMP, committee for medicinal products for human use; CDC, complement-dependent cytotoxicity; ADCC, antibody-dependent cell-mediated cytotoxicity;
ADCP, antibody-dependent cellular phagocytosis.
18
25
9
8
0
10
20
30
40
50
60
70
DARA + POM-D (N =103)
OR
R, %
PR VGPR
CR sCR
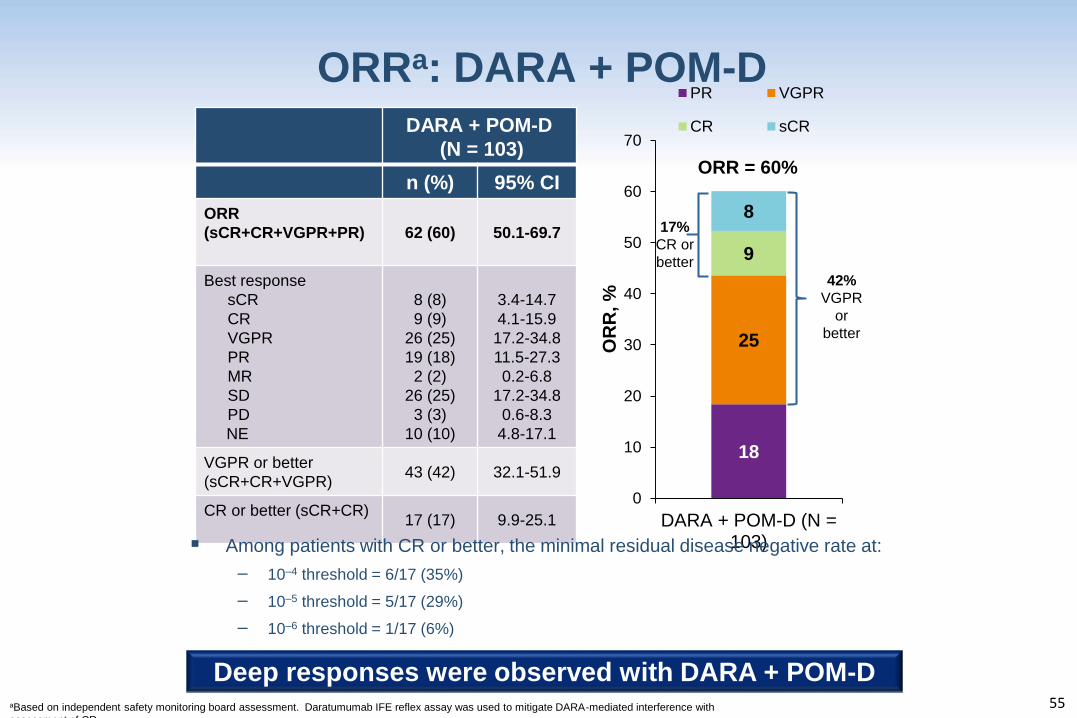
ORRa: DARA + POM-D
55
DARA + POM-D
(N = 103)
n (%) 95% CI
ORR
(sCR+CR+VGPR+PR) 62 (60) 50.1-69.7
Best response
sCR
CR
VGPR
PR
MR
SD
PD
NE
8 (8)
9 (9)
26 (25)
19 (18)
2 (2)
26 (25)
3 (3)
10 (10)
3.4-14.7
4.1-15.9
17.2-34.8
11.5-27.3
0.2-6.8
17.2-34.8
0.6-8.3
4.8-17.1
VGPR or better
(sCR+CR+VGPR)43 (42) 32.1-51.9
CR or better (sCR+CR)17 (17) 9.9-25.1
ORR = 60%
42%
VGPR
or
better
17%
CR or
better
aBased on independent safety monitoring board assessment. Daratumumab IFE reflex assay was used to mitigate DARA-mediated interference with
assessment of CR.
▪ Among patients with CR or better, the minimal residual disease negative rate at:
– 10–4 threshold = 6/17 (35%)
– 10–5 threshold = 5/17 (29%)
– 10–6 threshold = 1/17 (6%)
Deep responses were observed with DARA + POM-D
Isatuximab
CD38
ISATUXIMAB TCD14079
A Phase Ib Study of Isatuximab plus
Pomalidomide and Dexamethasone in
Relapsed/Refractory Multiple Myeloma
(RRMM)
Joseph Mikhael,1 Paul Richardson,2 Saad Usmani,3
Noopur Raje,4 William Bensinger,5 Dheepak Kanagavel,6
Lei Gao,7 Samira Ziti-Ljajic,6 Kenneth Anderson2
1Mayo Clinic, Phoenix, AZ, USA; 2Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA,
USA; 3Levine Cancer Institute/Carolinas Healthcare System, Charlotte, NC, USA; 4Massachusetts
General Hospital, Boston, MA, USA; 5Swedish Cancer Institute, Seattle, WA, USA; 6Sanofi R&D, Vitry-
Alfortville, France; 7Sanofi Oncology, Cambridge, MA, USA
ISATUXIMAB TCD14079
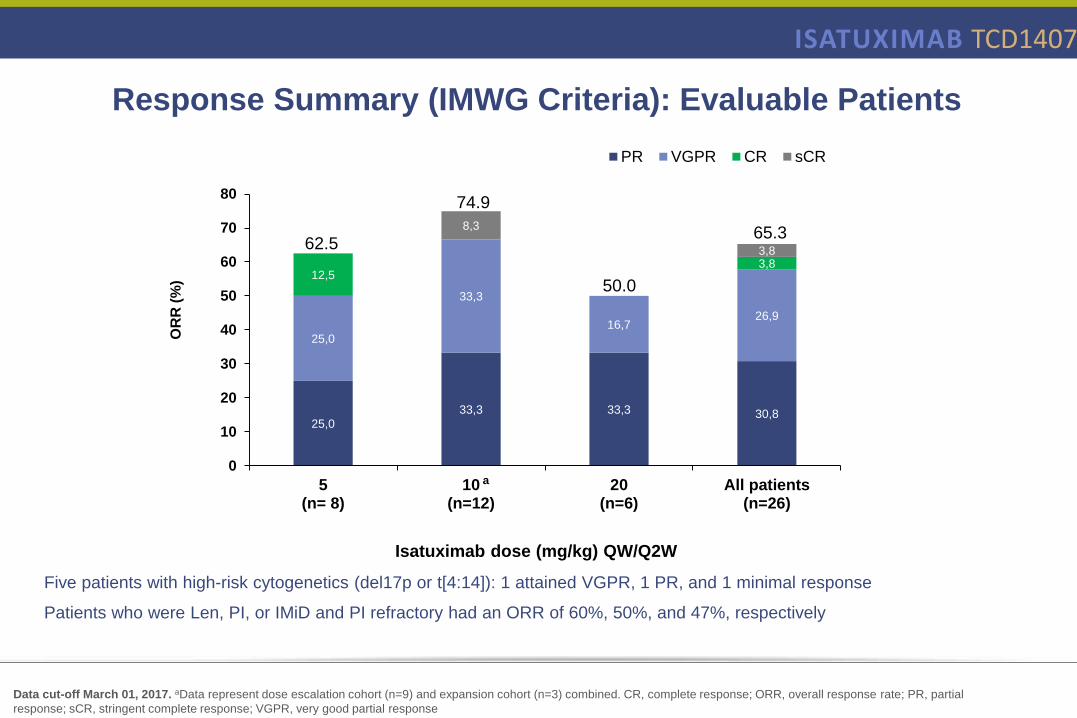
25,0
33,3 33,3 30,8
25,0
33,3
16,726,9
12,53,8
8,3
3,8
0
10
20
30
40
50
60
70
80
5(n= 8)
10(n=12)
20(n=6)
All patients(n=26)
OR
R (
%)
PR VGPR CR sCR
a
Isatuximab dose (mg/kg) QW/Q2W
62.5
74.9
50.0
65.3
Data cut-off March 01, 2017. aData represent dose escalation cohort (n=9) and expansion cohort (n=3) combined. CR, complete response; ORR, overall response rate; PR, partial
response; sCR, stringent complete response; VGPR, very good partial response
Five patients with high-risk cytogenetics (del17p or t[4:14]): 1 attained VGPR, 1 PR, and 1 minimal response
Patients who were Len, PI, or IMiD and PI refractory had an ORR of 60%, 50%, and 47%, respectively
Response Summary (IMWG Criteria): Evaluable Patients
Etude Isatuximab TED14154 : Etude d’escalade de dose, en ouvert et multicentrique, évaluant la tolérance, la pharmacocinétique et l’efficacité du SAR650984 (isatuximab) chez des patients atteints
d’un myélome multiple en rechute et réfractaire
Pr Xavier Leleu
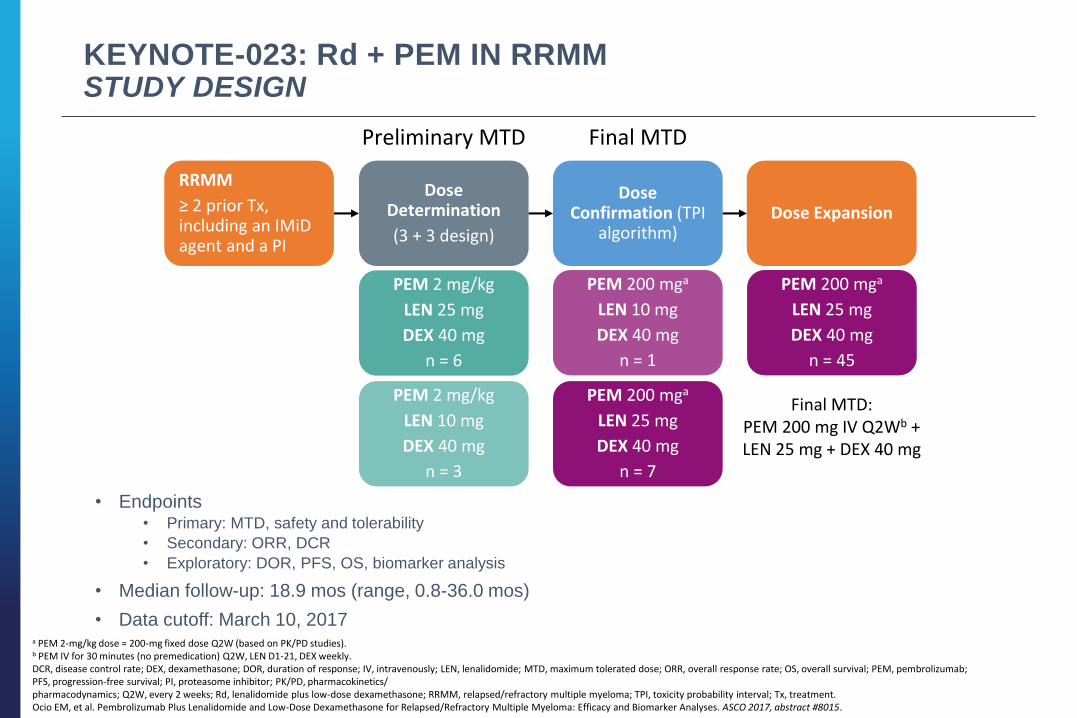
KEYNOTE-023: Rd + PEM IN RRMMSTUDY DESIGN
• Endpoints• Primary: MTD, safety and tolerability
• Secondary: ORR, DCR
• Exploratory: DOR, PFS, OS, biomarker analysis
• Median follow-up: 18.9 mos (range, 0.8-36.0 mos)
• Data cutoff: March 10, 2017
RRMM
≥ 2 prior Tx, including an IMiD agent and a PI
Dose Determination
(3 + 3 design)
Dose Confirmation (TPI
algorithm)Dose Expansion
a PEM 2-mg/kg dose ≈ 200-mg fixed dose Q2W (based on PK/PD studies). b PEM IV for 30 minutes (no premedication) Q2W, LEN D1-21, DEX weekly.DCR, disease control rate; DEX, dexamethasone; DOR, duration of response; IV, intravenously; LEN, lenalidomide; MTD, maximum tolerated dose; ORR, overall response rate; OS, overall survival; PEM, pembrolizumab; PFS, progression-free survival; PI, proteasome inhibitor; PK/PD, pharmacokinetics/pharmacodynamics; Q2W, every 2 weeks; Rd, lenalidomide plus low-dose dexamethasone; RRMM, relapsed/refractory multiple myeloma; TPI, toxicity probability interval; Tx, treatment.Ocio EM, et al. Pembrolizumab Plus Lenalidomide and Low-Dose Dexamethasone for Relapsed/Refractory Multiple Myeloma: Efficacy and Biomarker Analyses. ASCO 2017, abstract #8015.
Preliminary MTD Final MTD
PEM 2 mg/kg
LEN 25 mg
DEX 40 mg
n = 6
PEM 2 mg/kg
LEN 10 mg
DEX 40 mg
n = 3
PEM 200 mga
LEN 10 mg
DEX 40 mg
n = 1
PEM 200 mga
LEN 25 mg
DEX 40 mg
n = 7
PEM 200 mga
LEN 25 mg
DEX 40 mg
n = 45
Final MTD:PEM 200 mg IV Q2Wb +LEN 25 mg + DEX 40 mg
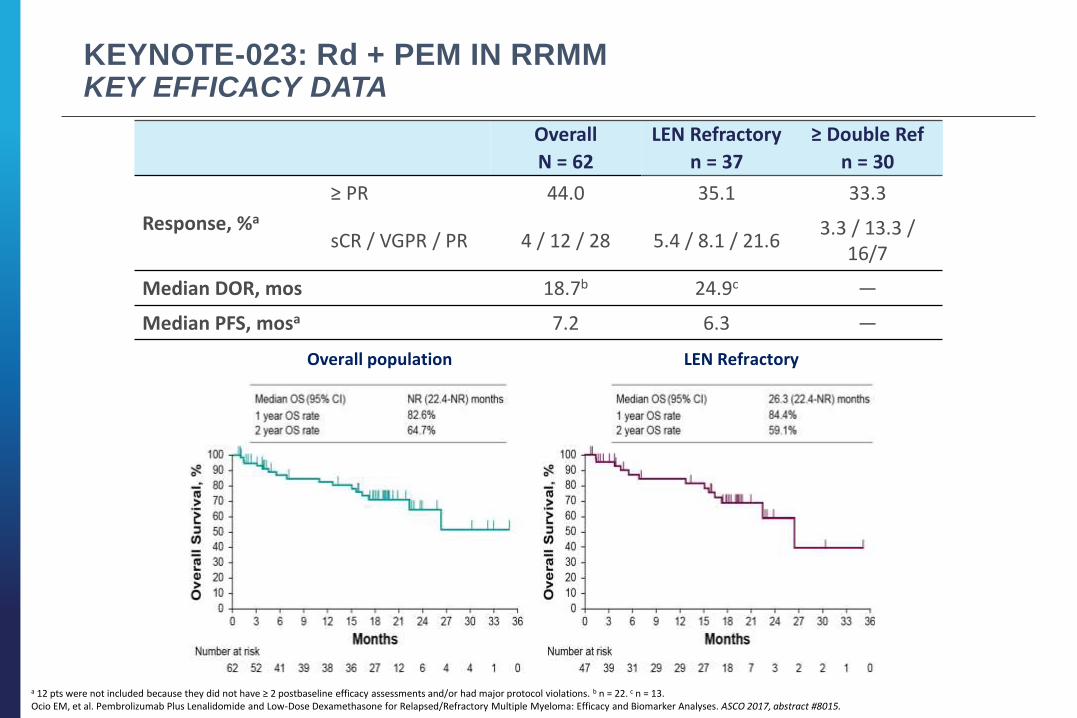
KEYNOTE-023: Rd + PEM IN RRMMKEY EFFICACY DATA
Overall
N = 62
LEN Refractory
n = 37
≥ Double Ref
n = 30
Response, %a
≥ PR 44.0 35.1 33.3
sCR / VGPR / PR 4 / 12 / 28 5.4 / 8.1 / 21.63.3 / 13.3 /
16/7
Median DOR, mos 18.7b 24.9c —
Median PFS, mosa 7.2 6.3 —
a 12 pts were not included because they did not have ≥ 2 postbaseline efficacy assessments and/or had major protocol violations. b n = 22. c n = 13. Ocio EM, et al. Pembrolizumab Plus Lenalidomide and Low-Dose Dexamethasone for Relapsed/Refractory Multiple Myeloma: Efficacy and Biomarker Analyses. ASCO 2017, abstract #8015.
Overall population LEN Refractory
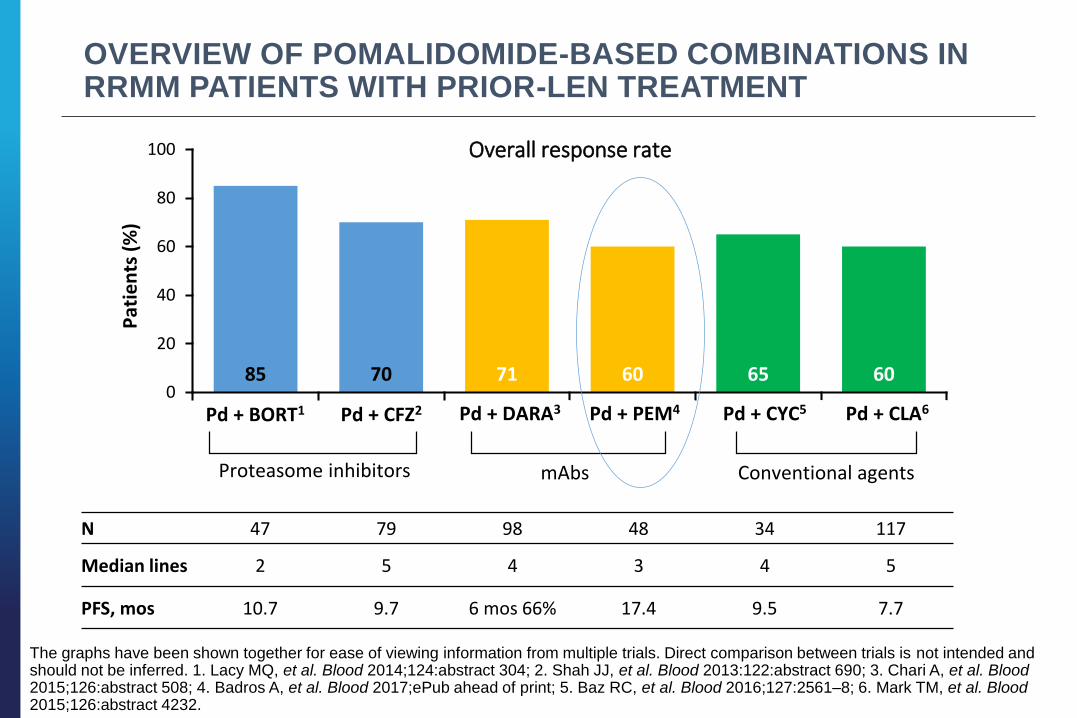
OVERVIEW OF POMALIDOMIDE-BASED COMBINATIONS IN RRMM PATIENTS WITH PRIOR-LEN TREATMENT
The graphs have been shown together for ease of viewing information from multiple trials. Direct comparison between trials is not intended and should not be inferred. 1. Lacy MQ, et al. Blood 2014;124:abstract 304; 2. Shah JJ, et al. Blood 2013:122:abstract 690; 3. Chari A, et al. Blood 2015;126:abstract 508; 4. Badros A, et al. Blood 2017;ePub ahead of print; 5. Baz RC, et al. Blood 2016;127:2561–8; 6. Mark TM, et al. Blood 2015;126:abstract 4232.
N 47 79 98 48 34 117
Median lines 2 5 4 3 4 5
PFS, mos 10.7 9.7 6 mos 66% 17.4 9.5 7.7
Proteasome inhibitors Conventional agentsmAbs
85 70 71 60 65 600
20
40
60
80
100 Overall response rateP
atie
nts
(%
)
Pd + BORT1 Pd + CFZ2 Pd + DARA3 Pd + PEM4 Pd + CYC5 Pd + CLA6
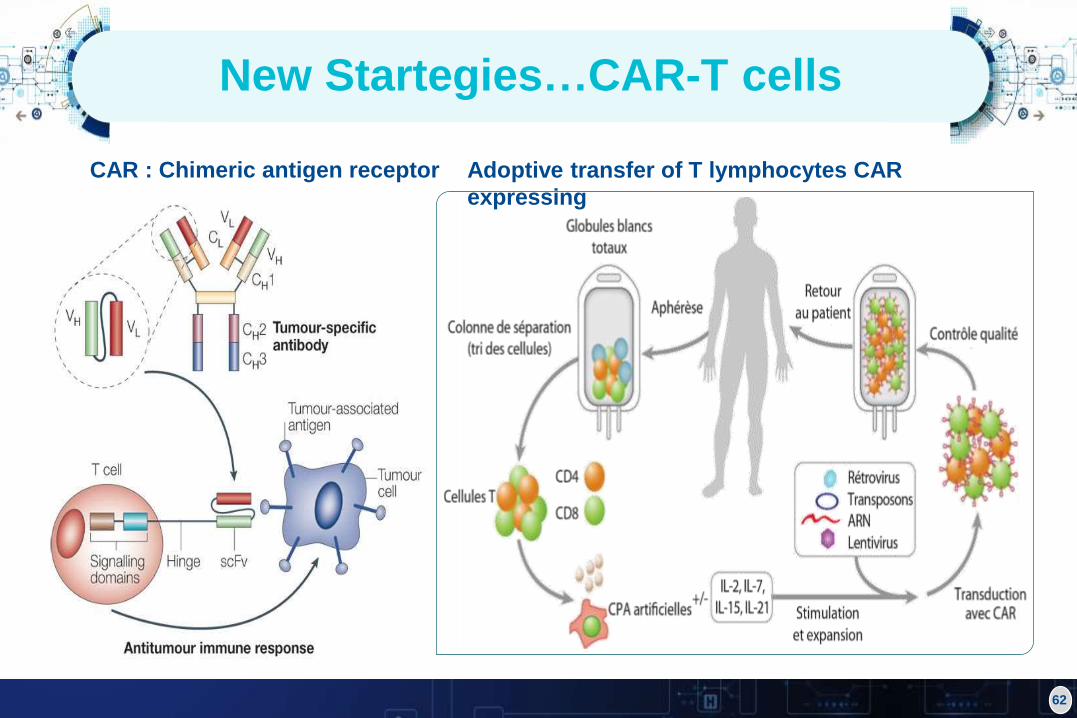
New Startegies…CAR-T cells
62
CAR : Chimeric antigen receptor Adoptive transfer of T lymphocytes CAR
expressing
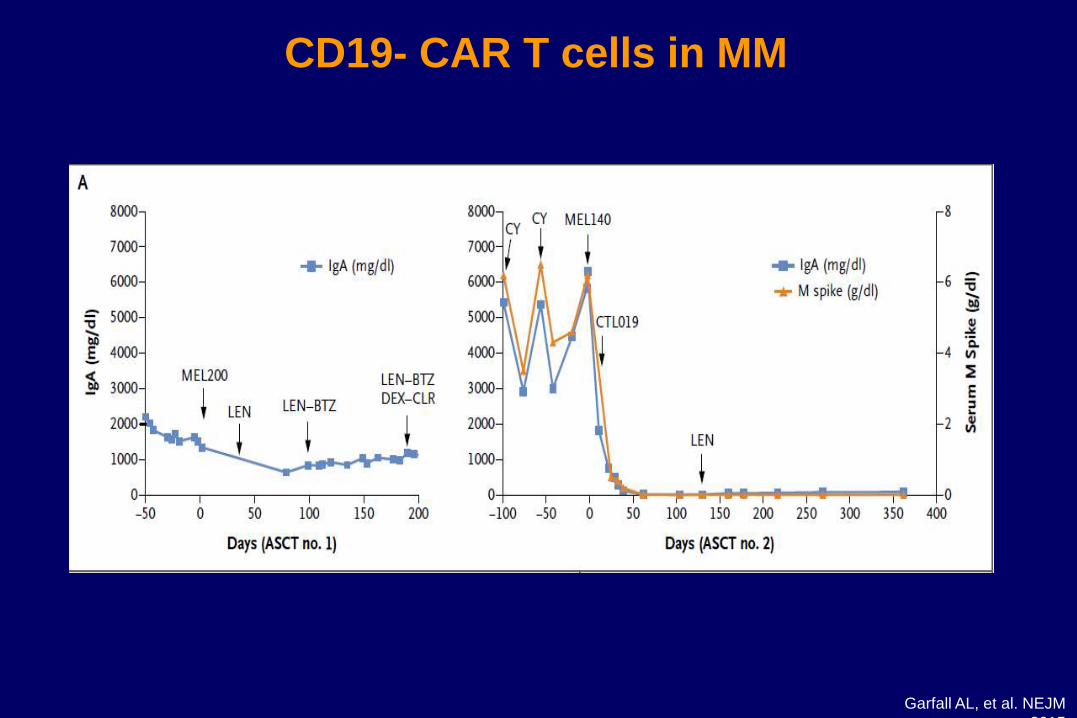
CD19- CAR T cells in MM
Garfall AL, et al. NEJM
2015
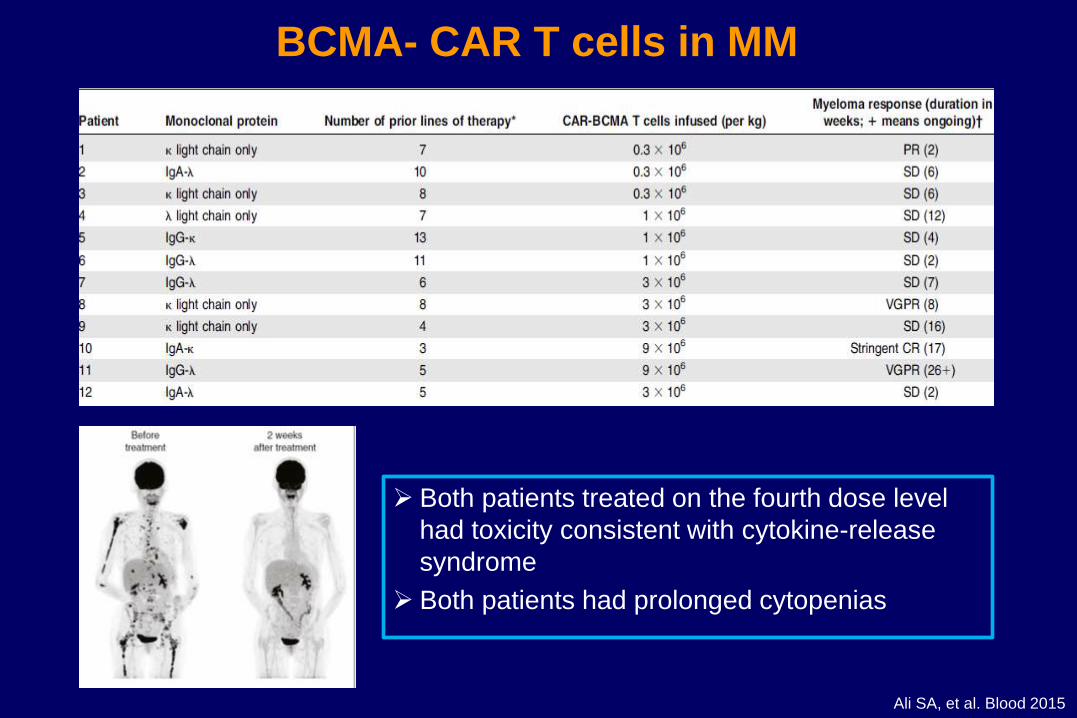
BCMA- CAR T cells in MM
➢ Both patients treated on the fourth dose level
had toxicity consistent with cytokine-release
syndrome
➢ Both patients had prolonged cytopenias
Ali SA, et al. Blood 2015
ABSTRACT S103
Phase I, Open-Label Trial of Anti-BCMA Chimeric Antigen Receptor T cells in
Patients With Relapsed / Refractory Multiple Myeloma
Wanggang Zhang, Wanhong Zhao, Jie Liu, Aili He, Yinxia Chen, Xingmei Cao, Nan Yang, Baiyan Wang, Pengyu Zhang, Yilin Zhang, Fangxia Wang, Bo Lei, Liufang Gu, Yun Yang, Ju Bai, Ruili Zhang, Xugeng Wang, Xiaorong Ma, Jianli Wang, Jin Wang,
Lili Wei, Juanli Zhang, Xinzhao Zang, Qiuchuan Zhuang, Frank (Xiaohu) Fan
Oral Presentation at the 22nd Congress of the European Hematology Association
June 22–25, 2017
Friday, June 23, 2017; 12:15–12:30
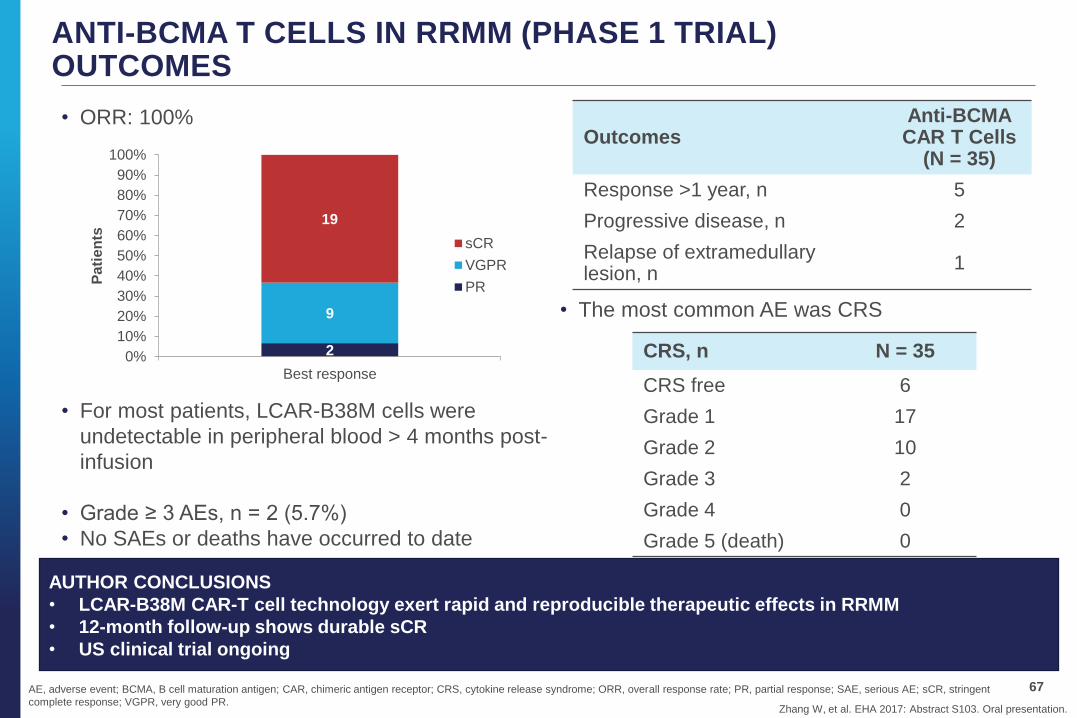
ANTI-BCMA T CELLS IN RRMM (PHASE 1 TRIAL)OUTCOMES
• For most patients, LCAR-B38M cells were
undetectable in peripheral blood > 4 months post-
infusion
• Grade ≥ 3 AEs, n = 2 (5.7%)
• No SAEs or deaths have occurred to date
67
Zhang W, et al. EHA 2017: Abstract S103. Oral presentation.
OutcomesAnti-BCMA CAR T Cells
(N = 35)
Response >1 year, n 5
Progressive disease, n 2
Relapse of extramedullary lesion, n
1
AE, adverse event; BCMA, B cell maturation antigen; CAR, chimeric antigen receptor; CRS, cytokine release syndrome; ORR, overall response rate; PR, partial response; SAE, serious AE; sCR, stringent
complete response; VGPR, very good PR.
AUTHOR CONCLUSIONS
• LCAR-B38M CAR-T cell technology exert rapid and reproducible therapeutic effects in RRMM
• 12-month follow-up shows durable sCR
• US clinical trial ongoing
CRS, n N = 35
CRS free 6
Grade 1 17
Grade 2 10
Grade 3 2
Grade 4 0
Grade 5 (death) 0
2
9
19
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Best response
Pa
tie
nts
sCR
VGPR
PR
• ORR: 100%
• The most common AE was CRS
Never give up!
Thank you for your attention