-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
1/16
The assessment of respiratory mechanics begins with
themeasurement of variables whose correlations containinformation
about the mechanical functioning of the respi-ratory system. These
variables are usually pressures and
flows, or volumes, of gas made at appropriate sites. Theamount
of detail that can be gleaned about the mechanicalfunction of the
respiratory system depends on which partic-ular variables are
measured and the conditions under whichthey are measured. Although
the modern history of meas-urement in respiratory mechanics extends
back at least 100years, novel methods and approaches are still
being devel-oped as advances in instrumentation and computer
technol-ogy continue to extend the boundaries of what is
possible.
This review of measurement in respiratory mechanicsbegins with
the general theory of measurement as it appliesto modern electronic
transducers and the acquisition of databy digital computer. It then
proceeds to consider how this
theory is applied to the measurement of respiratory pres-sures,
flows, and volumes. Finally, it is shown how thesemeasurements are
used in combination to collect informa-tion from which respiratory
mechanics are determined.
MEASUREMENT THEORY
The general measurement situation is depicted in Figure
54-1,which shows the steps involved in converting a biologicsignal
into a string of numbers stored on a computer. Ateach step we have
the potential for errors to occur, repre-sented as additive noise.
First we consider the issuesinvolved in transducing the biologic
signal into an electricalsignal. This is performed by a transducer.
We then considerthe process of digitizing the electrical signal so
that it can bemanipulated in digital form on a computer, which is
howany subsequent data analysis is carried out.
TRANSDUCERSA transducer is something that converts energy from
oneform to another, although for the present purposes werestrict
ourselves to the more particular definition of theconversion being
between some biologic quantity we areinterested in and a voltage.
Ideally, we would like the voltageto be a perfect representation of
the biologic quantity, but
this is never the case in practice. It is therefore crucial
tounderstand the imperfections of the transducer to be used inany
particular application and whether or not these imper-fections are
going to limit the amount of information that
can be extracted from the measured signals.
Static Properties of Transducers We first consider thevarious
static properties that characterize a transducers per-formance.
These are properties that do not depend on howrapidly the measured
signal is varying, which is equivalentto saying that the transducer
has no trouble keeping up withthe signal. One such property is
linearity, which refers to theextent to which the voltage v
produced by a transducer canbe represented in terms of the biologic
signal s by an equa-tion of the form
v as b (54-1)
where a and b are constants (solid line in Figure
54-2).Manufacturers of transducers usually specify the linearity
ofa transducer in terms of its full-scale output. A value of 1%is
typical. Although linearity is a desirable trait, with
theavailability of digital computers it is not essential.
Suppose,for example, that v is not a linear function ofs as in
Equation54-1 but is instead a curvilinear function of s that can
beaccurately represented as a polynomial (dashed line inFigure
54-2). If the polynomial coefficients are known (say,from a prior
calibration experiment) it is a simple matter touse a computer to
invert the equation to obtain s as a func-tion ofv, allowing the
recorded voltage to be related back tothe value of the original
biologic signal.
Another important static property of a transducer is
hys-teresis, which refers to the extent to which the voltage
corre-sponding to a biologic signal differs depending on whetherthe
immediately preceding value was below or above thecurrent value
(Figure 54-3). Hysteresis is obviously a badthing and is
unfortunately extremely difficult to correct for,so one should
always try to select a transducer with minimalhysteresis.
In selecting a transducer for a particular application, itis
important to make sure it has the appropriate resolutionand dynamic
range, which determine the smallest andlargest changes in the
biologic signal that can be accurately
CHAPTER 54
MEASUREMENT TECHNIQUES INRESPIRATORY MECHANICS
Jason H. T. Bates
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
2/16
624 Clinical Respiratory Physiology
measured. Related to the issue of resolution is the
signal-to-noise ratio. What the transducer in Figure 54-1
actuallyrecords in response to a biologic signal is a voltage
plusnoise. The latter must be substantially lower than anyimportant
changes that are to be recorded in the biologicsignal (by
preferably at least an order of magnitude).
Dynamic Properties of Transducers We now considerthe somewhat
more complicated issue ofdynamic propertiesof transducers. These
refer to those characteristics thatdetermine how well a transducer
can respond to a changingbiologic signal. Most transducers are
low-pass systemsbecause they can respond faithfully to slowly
varying signals
but have increasing difficulty keeping up as the signalincreases
in frequency. Some transducers are high-pass sys-tems because they
faithfully record high frequencies but donot respond when frequency
is very low. Transducers arecharacterized in general by the way in
which they respondto input signals that vary sinusoidally. Provided
that thetransducers are linear, their voltage outputs to an input
sinewave will also be sinusoidal with the same frequency butwill in
general be altered in amplitude by a factor A andshifted in phase
by an amount . That is, if the input sinewave is sin(2ft), then the
output will be Asin(2 ft )(Figure 54-4). The values ofA and depend
on frequency
and together constitute the frequency response of
thetransducer.
DIGITAL DATAACQUISITIONOnce a transducer has converted a
biologic signal into avoltage, it must be recorded in some
permanent medium forsubsequent analysis and display. In the early
days of physi-ology (ie, until about 20 years ago), physiologic
recordingwas achieved by have a writing instrument move
laterally
over a suitable recording medium as it scrolled by. In theearly
part of the twentieth century, the writing instrumentwas a rigid
pointer and the scrolling medium was a cylindri-cal drum covered in
soot. This was eventually replaced bythe electronic chart recorder,
consisting of one or more ink
pens writing on a roll of paper moving past at constantspeed.
Each experiment produced a (frequently large) stackof paper that
then had to be analyzed manually if calcula-tions were to be made
from the recorded signals.
Since the advent of the modern laboratory digitalcomputer,
however, these earlier analog recording deviceshave been replaced
by digital computers that both recordand analyze experimental data.
The speed and flexibility ofcomputers, together with their
universal availability, haverevolutionized the way that physiologic
research is done.
Everything is thus now done digitally, beginning withthe
recording of the analog voltage signal arriving from
the transducer. Conversion of an analog signal to digitalform is
known as digitization and is accomplished with ananalog-to-digital
(A-D) converter. Figure 54-5 shows what isinvolved. The analog
(continuous) voltage signal is sampledat regularly spaced intervals
by the A-D converter, andthe resulting set of voltage values is
stored in the computeras a set of numbers. These numbers and their
locationsin time then constitute our representation of the
originalsignal.
Resolution and Discretization Error A major considera-tion when
digitizing signals is the resolution of the A-D con-verter, which
defines the smallest difference in voltage level
that it can distinguish in the incoming analog signal. A-D
TransducerAnalog-digitalconverter
Computer
Biologicsignal
Voltage Digitalsignal
Noise Noise
FIGURE 54-1 The general measurement scenario.
Biological signal
Voltage
FIGURE 54-2 Characteristics of a linear (solid line) and
nonlinear(dashed line) transducer.
Biologic signal
Voltage
FIGURE 54-3 Hysteresis. The voltage output by a transducer
inresponse to a particular value of the input biologic signal
dependson whether the value was approached from above or below.
Transducer
Input Output
1.0 A
FIGURE 54-4 If an input to a linear transducer is sin(2ft),
itsoutput in general will beAsin(2ft ), where the values ofA and
characterize the frequency response of the transducer.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
3/16
Measurement Techniques in Respiratory Mechanics 625
converters are set up to receive voltages within a
specifiedrange, such as 10 to 10 volts. This voltage range
isdivided into N equally spaced bins numbered 0 to N1(Figure 54-6).
Nis determined by the number ofbits in theA-D converter. A 12-bit
A-D converter has 212 4,096 bins,a 16-bit converter has 216 65,536
bins, and so on. Thus, for
example, a 12-bit converter with a 10-volt input range
canresolve voltage differences of 20/4,096 0.0049 volts.
The finite resolution of an A-D converter means that caremust be
taken to ensure that it is able to resolve the smallestdifferences
in voltage required by the experimenter. Forexample, suppose one is
measuring flow of gas entering apatients lungs during mechanical
ventilation. If the flowreaches 2,000mL.s1 during both inspiration
and expira-tion, then the range of flows encountered is 4,000mL.s1.
Ifthis flow signal is recorded on a 12-bit A-D converter,
theresulting digitized signal has a maximum resolution
of4,000/4,096 0.98mL.s1. However, it only achieves this
resolution if the entire dynamic range of the A-D converteris
used. This only occurs if the analog signal producedby the flow
transducer is amplified so that a flow of2,000mL.s
1produces the lowest voltage the A-D
converter can receive (eg, 10 volts), and similarly a flow
of 2,000 mL.s1 produces the highest receivable voltage(eg, 10
volts).
This may not be the case. A common error in the labora-tory
occurs when the voltage signal coming in from thetransducer is not
amplified enough to make use of many ofthe discrete bins in the A-D
converter. As an example, sup-pose that the flow signal of 2,000 to
2,000 mL.s1
results in a voltage signal that only occupies the range of
0.1 to 0.1 volts. Now only the middle 1% of the availablebins
(numbers 2,028 to 2,069) of the A-D converter areused, giving a
100-fold reduction in flow resolution. Inextreme examples of this
situation, the discrete levels of theA-D converter will be apparent
in a plot of the resulting volt-age signal (Figure 54-7). The
errors incurred in havinginsufficient vertical resolution in an A-D
converter are calleddiscretization errors.
Sampling Theorem and Aliasing Another major ques-tion that
arises when digitizing analog signals is how fre-quently to sample
the signal. A continuous signal iscomposed of an infinite number of
infinitesimally spaced
points yet must somehow be represented by a finite numberof
digitized values. Obviously, if a signal is changing rapidly,then
sampling its value infrequently will cause the detailbetween the
samples to be lost. On the other hand, samplinga long signal too
rapidly might result in an unmanageablylarge number of data points.
Thus, one might be inclined tothink that the choice of sampling
rate represents a tradeoffbetween capturing detail in the original
signal on the onehand and avoiding being overwhelmed by the volume
ofdata on the other. Fortunately, however, we are saved bysomething
known as the sampling theorem (often associatedwith engineers
Shannon and Nyquist).
To understand the sampling theorem, it is necessary to
first understand what is meant by thefrequency content of
asignal. Any analog signal can be expressed as the sum of aseries
of sine wave functions of appropriate frequency,amplitude, and
phase. Furthermore, this collection of fre-quencies, amplitudes,
and phases is unique to that signal,which means they define it
distinctly from all other possiblesignals. A signal can be
decomposed into its individual sinewave components by the Fourier
transform. A simple exam-ple is given in Figure 54-8, which shows
the four sine wavesmaking up a signal that looks considerably more
complexthan any of its individual components. The frequencycontent
of a signal thus refers to the unique spectrum of
1
0
0.210.430.500.500.420.330.330.370.480.520.590.58..
.t
V(t)
t
FIGURE 54-5 Digitization. An analog voltage signal V(t)
issampled every t seconds to produce a series of numbers that
arestored in a computer for subsequent analysis.
-10 volts
+10 volts
0
4095
Analog signal Digitized signal
FIGURE 54-6 Digitization of the 10 volt analog range by a
12-bitA-D converter. The 20-volt span of possible input signals
isassigned to 4,096 numbers representing successive increments
of4.9 millivolts.
FIGURE 54-7 Discretization error. The left panel shows an
analogsignal faithfully captured by a set of digitized points. The
right
panel shows points occupying discrete levels corresponding
toadjacent bins of the A-D converter.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
4/16
626 Clinical Respiratory Physiology
sinusoidal components from which it is composed. Inparticular,
if the frequency content of a signal is such thatnone of its
sinusoidal components has a frequency greaterthan some maximum
frequency, then the signal is said to beband limited.
The sampling theorem says that it is possible to captureall the
information in a band-limited analog signal by sam-pling the signal
at a rate at least twice the highest frequencyin the signal itself.
Thus, for example, if Fourier analysis ofa signal reveals that it
contains no components with fre-quencies greater thanf0, then we
need not sample the signalany faster than 2f0 (known as the Nyquist
rate). Intuitively,this makes sense because sampling a sine wave at
its Nyquistfrequency means collecting another sample from the
signalevery time it changes direction. If we know we are samplinga
sine wave, then from this set of points we can reconstruct
the intervening continuous signal segments by fitting a sinewave
to the points. Thus, by sampling an analog signal at orabove the
Nyquist rate, we lose no informationthe entireoriginal continuous
signal can be reconstructed from thesampled points alone.
The sampling theorem in principle means we lose noth-ing in
moving from a continuous to a digital environment.However, there is
a practical issuewhat iff0 is so high that
we still end up with an unmanageably large number ofdata points
when we satisfy the sampling theorem?Unfortunately, we cannot drop
the sampling rate below2f0 and hope to merely sacrifice some detail
in the retainedsamples. The high frequencies in the analog signal
do notsimply disappearthey turn up in the digitized data but
atwrong (much lower) frequencies! This is a particularlyinsidious
problem known as aliasing, and experimentersmust always be careful
to avoid it, especially if the powerspectra of the collected data
are of interest. Aliasing canlead to completely erroneous spectral
characterization ofa signal and at the very least degrades the
signal-to-noiseratio of a measurement. Figure 54-9 shows how
aliasing
occurs; a sine wave is sampled at a frequency below theNyquist
rate to yield a set of points that look as if theyrepresent a
different sine wave of a much lower frequency.Obviously, aliasing
can be avoided by sampling at or abovethe Nyquist rate. However, in
practice it is usually necessaryto force the analog signal to be
band limited to somemanageablef0. This is done by passing the
signal through ahigh-quality low-pass electronic filter before it
is digitized.Such filters are known as antialiasing filters. It is
importantto remember that filtering for antialiasing must be
doneprior to digitization of the signal. Once aliasing occurs,no
amount of digital filtering after the fact can fix theproblem.
Fourier transform
FIGURE 54-8 An analog signal can be decomposed (by theFourier
transform) into its component sine waves, each with itsown
frequency, amplitude, and phase.
FIGURE 54-9 A sine wave (solid line) is sampled (dots) below
theNyquist rate, yielding a set of data points defining a different
sinewave (dashed line) at a lower frequency.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
5/16
Measurement Techniques in Respiratory Mechanics 627
MEASUREMENT OF RESPIRATORY SIGNALS
Having established the general considerations for
measuringsignals in the laboratory, we now move on to consider
thosesignals specific to the study of mechanical lung function.
PRESSUREThe measurement of pressure is central to the study of
res-piratory physiology because it is pressure that generates
theflow of gas needed to ventilate the lungs.
Pressure Transducers Pressure transduction is based onthe graded
deformation of some mechanical element whosealtered configuration
is read by some electronic means(Figure 54-10). Until about 15
years ago, the mainstay ofpressure measurement in the respiratory
physiology labora-tory was the variable reluctance transducer in
which a thinmetal disk is placed between the primary and
secondarycoils of a transformer excited by several kHz of
alternatingelectric current. A pressure difference either side of
the diskcauses it to deform in a way that alters the magnetic
flux
linkage between the transformer coils, thereby changing
theinduced voltage in the secondary coil. The change in voltageis
then transformed into a DC voltage proportional to thepressure
difference. These transducers are sensitive andaccurate. They also
typically have a frequency response thatis flat to 20 Hz or more,
depending on the length of the tub-ing connecting its ports to the
sites of pressure measure-ment.1 However, they are somewhat
cumbersome and can bedamaged by over pressurization.
In recent years, respiratory pressure measurement hasbeen taken
over by the piezoresistive transducer,2 inwhich the
pressure-sensitive element changes its electricalresistance as it
deforms. If a constant voltage (or current)
is passed through the piezoresistive element when it
isconfigured to be one of the four arms of a suitably bal-anced
Wheatstone bridge, the voltage across the bridge isthen
proportional to the change in the elements resistance.A medium-gain
amplifier followed by an antialiasingfilter are the only remaining
elements required to producean electrical signal proportional to
pressure that is readyfor digitization. When piezoresistive
pressure transducerswere first used in respiratory physiology in
the 1980s,they tended to suffer from baseline drift, were affected
byorientation and temperature, and were not very sensitive.These
problems have now been essentially overcomeallowing piezoresistive
transducers to be exploited for
their several advantages. These include an
extremelyhigh-frequency response (typically flat to several
hundredHz), robustness (they can be pressurized to many times
theirnominal full-scale range without damage), and the factthat
they can be manufactured using solid-state technologyto be very
small and light. Piezoresistive transducers arealso much cheaper
than their variable reluctance counter-parts and require simpler
electronic signal conditioning
circuitry.
Measuring Pressure at the Airway Opening The assess-ment of
pulmonary function frequently requires that thepressure in a
flowing stream of gas be measured, such as atthe entrance to the
endotracheal tube in a mechanically ven-tilated patient. Gas always
flows down a pressure gradient,so at each point along the stream of
flowing gas there is adriving pressure pushing the gas downstream
of it. The goalis to determine this driving pressure. The easiest
way is toinsert a perpendicular tap into the tube and connect it to
apressure transducer (Figure 54-11). This provides what isknown as
lateral pressure (Plat), and it corresponds to the
pressure exerted perpendicular to the direction of flow asthe
gas moves past the point of measurement. It turns out,however, that
Plat is less than the pressure driving the gasalong the tube
because of a phenomenon known as theBernoulli effect, which occurs
because of the principle ofconservation of energy; the faster gas
is moving along thetube, and consequently the larger its kinetic
energy, the moreit loses in potential energy, manifest as a drop in
Plat. Plat under-estimates true driving pressure, in a tube of
cross-sectional areaA with flow V, by an amount Pb given by the
formula
(54-2)
where is the density of the gas and is a factor determinedby the
flow velocity profile. For example, if the profile is flat(the
linear velocity of the gas molecules is the same at everypoint in
the tube cross section) then 1 and 2 if theprofile is
parabolic.
If the gas in the tube were stationary, then Plat wouldequal
driving pressure, a condition that can always beachieved by
connecting a pressure transducer to a small tube
Pb V
.2
2A2
Pressuresource
Deformableelement
FIGURE 54-10 Pressure transducer. The application of a
pressuredeforms an element whose configuration is converted into an
elec-trical signal proportional to the degree of deformation.
Plat
Pstat
V
.
FIGURE 54-11 Lateral pressure (Plat) measured through a
lateraltap, and static pressure (Pstat) measured with a Pitot
tube.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
6/16
628 Clinical Respiratory Physiology
that enters the flow stream laterally and then bends until
itsopen end faces directly into the oncoming flow (see
Figure54-11). Such a device, called a Pitot tube, measures the
staticpressure (Pstat) in a small parcel of gas that has been
broughtto rest by abutting up against the tube opening. Pb is
thedifference between Pstat and Plat. That is,
Plat Pstat Pb (54-3)
The problem for respiratory pressure measurement causedby the
Bernoulli effect is apparent from Equation 54-2,which shows that Pb
depends on the square of flow dividedby cross-sectional area. When
the area is large enough, Pbis negligible. However, as the area
decreases there comes apoint at which Pb starts to become
important, comparedwith Pstat. Indeed, Equation 54-3 shows that for
small tubeareas Plat may even become negative. Thus, it is
importantin any application in which lateral pressures are measured
tobe sure that the Bernoulli effect is not significantly
affectingthe measurement of the desired quantity, namely
drivingpressure.3 The Bernoulli effect may also be an important
fac-tor influencing the measurement of pressures at the distal
end of an endotracheal tube in an intubated patient.4
Esophageal and Gastric Pressures Two other pressuresof great
practical importance in the study of respiratoryphysiology are
those in the esophagus and stomach.Esophageal pressure (Pes) is a
useful surrogate for pleuralpressure, the esophageal lumen being
separated from thepleural space by only soft tissue. Gastric
pressure (Pga)measures the pressure exerted on the diaphragm by
theabdominal contents, which is important for understandingactive
expiration. The difference between Pes and Pga is thepressure
across the diaphragm, which is important in stud-ies of respiratory
muscle function.5
Both Pes and Pga can be measured using a balloon-tippedcatheter
(Figure 54-12). A thin-walled latex balloon, a fewcentimeters in
length, is sealed over a thin plastic catheter,typically about
100cm long. The balloon is passed into theesophagus, usually via
the nose. Once in place in either theesophagus or stomach, a small
volume of air is injected intothe balloon and a pressure transducer
is connected to theproximal end of the catheter. The volume of air
in the bal-loon must be sufficient to prevent the walls of the
balloonfrom occluding all the multiple holes in the end of the
catheter, but not so much that there is tension in the
balloonwalls. The correct placement of the balloon is gauged
fromthe nature of the recorded pressure signals. When the bal-loon
is in the stomach, spontaneous inspiration produces apositive
deflection in the recorded Pga. As the balloon iswithdrawn and
enters the esophagus, the inspiratory pres-sure swings will
suddenly become negative. At this point,when inspiratory efforts
are made against an occluded air-
way (the so-called occlusion test), the deflections in Pesshould
match those in pressure measured at the airwayopening (Pao). Thus,
a regression of Pes versus Pao shouldyield a slope of unity.6 In
practice, slopes that differ from 1.0by up to 10% are common.
Although the occlusion testrequires that the subject be able to
breathe spontaneously, ithas been shown that the esophageal balloon
also works wellduring paralysis.7 The frequency response of the
esophagealballoon is obviously somewhat compromised by the fact
thatpressure changes in the esophageal lumen must be transmit-ted
through the air inside a long thin catheter to a pressuretransducer
some distance away. However, a reasonably goodresponse to 30Hz has
been observed.8 Pes has also been meas-
ured using catheter-tip piezoresistive transducers, which
havebeen shown to perform well9 and have a much betterfrequency
response than balloon catheter systems. In smallanimals, Pes can be
measured using a water-filled catheter.
10
Alveolar Pressure In experimental animals it is possibleto
measure alveolar pressure directly using a techniqueknown as the
alveolar capsule.11 The chest is opened andretracted to expose the
pleural surface of the lung to whicha small plastic capsule is
fixed (Figure 54-13). The capsulehas a cylindrical chamber leading
down to a small windowon the pleural surface encircled by a flange.
If the pleuralsurface is first swabbed with alcohol and dried, the
flange
can be secured to it with cyanoacrylate glue. Small
punctureholes are then made in the pleural surface within the
capsulewindow. If the holes are made carefully to a depth of 1
to
10 cm
100 cm
Pressuretransducer
Latex balloonPlasticcatheter
FIGURE 54-12 An esophageal balloon catheter. Note the
multipleholes in the walls of the catheter inside the balloon.
Pressuretransducer
Pleural surface
Capsule
Terminalairways
Sub-pleuralalveoli
FIGURE 54-13 The alveolar capsule.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
7/16
Measurement Techniques in Respiratory Mechanics 629
2 mm, preferably with a cautery needle, bleeding is minimaland
the subpleural alveoli are brought into contact with the
capsule chamber. A small piezoresistive pressure transducercan
then be lodged in the chamber to give a direct recordingof
subpleural pressure. In large animals, such as dogs, sev-eral
alveolar capsules can be installed at different sites overthe lung
surface.1214 A single alveolar capsule can even beused in an animal
as small as a mouse.15
FLOWPneumotachographs The mainstay of flow measurementin
respiratory physiology is the pneumotachograph, whichis a
calibrated resistance (R) across which a differential pres-sure is
measured (Figure 54-14). When gas flows throughthe
pneumotachograph, there is a pressure drop (P) from
the upstream side of the resistance to the downstream sidethat
increases as flow (V) increases, thus
P RV (54-4)
IfR is independent ofVover the range of flows of interestthen
the pneumotachograph is said to be linear. Manufac-turers strive
for linearity and always quote the linear rangeof a
pneumotachograph. However, if the device is nonlinear,so that R
depends on V, it is a simple matter to invertEquation 54-4 on a
computer and calculate Vfrom a measure-ment ofP, provided that the
relationship ofR toVis known.
The frequency response of a pneumotachograph dependson the
construction of its resistive element. Some consist ofa honeycomb
arrangement of conduits, whereas others con-sist of a wire screen.
The honeycomb type is less likely tobecome partially blocked by
secretions but has a poorer fre-quency response than the screen
type. Either type should beheated to above body temperature during
prolonged use toavoid breath condensate from settling on the
resistive ele-ment and changing its resistance (and hence altering
the cal-ibration of the device). Pneumotachographs can have a
goodfrequency response above 20 Hz with a resonance occurringat
around 70Hz, provided that the associated differentialtransducer
has a response at least that good and is connectedwith the shortest
possible lengths of tubing.1 The frequency
response of a pneumotachograph degrades rapidly as thetubing
connecting the transducer to the lateral taps eitherside of the
resistance element increases in length. Inad-equate frequency
response can be corrected for to a signifi-cant extent by digital
compensation, giving an effectivelyflat frequency response to more
than 100Hz.16
Another consideration for pneumotachographs concernstheir
dynamic common-mode rejection characteristics. If the
two ports of the pneumotachograph are both subjected to thesame
change in pressure, ideally the device should register aflow of
zero. This is not always the case, however, particu-larly if the
physical dimensions of the two ports are differentand if the input
impedance of the pressure transducer is notvery large compared with
that of the system under investiga-tion when flow oscillates at a
high frequency. Digital compen-sation methods can improve the
situation to a certain extent.17
Poor dynamic common-mode rejection is a significant prob-lem for
pneumotachographs used with very small animals.18
Other Devices for Measuring Flow Although the resis-tive
pneumotachograph is the mainstay for measuring flow
in respiratory applications, other devices have been used.For
example, ultrasonic transducers based on differences
intime-of-flight of sound propagating into the direction flowversus
away from it have an excellent frequency responseand avoid the
problems of a resistive element becomingclogged with secretions.19
Devices based on the rate of cool-ing of a heated wire are also in
use.20
VOLUMEDirect Measurement of Volume The volume of gas enter-ing
the lungs can be measured directly with a spirometerattached to the
mouth or from the pressure or flows emanat-ing from a whole body
plethysmograph when the subject
breathes through a conduit connected to outside the
plethys-mograph. A more convenient but less accurate
plethysmo-graphic method is provided by the changes in trunk
volumeassessed with an inductance plethysmograph.21 Recently, amore
accurate but expensive optical plethymograph has beendeveloped that
allows the detailed measurement of thoracicmovement during
breathing.22 However, for many applica-tions requiring the
assessment of lung function, the easiestway to assess changes in
lung volume is to integrate the flowmeasured at the mouth with a
pneumotachograph.
Integration of Flow Before the advent of the modern lab-oratory
digital computer, integration was typically achievedin real time
using an electronic circuit based on the chargingof a capacitor.
Nowadays, integration is performed digitallyon a computer. The
digitized flow signal consists of a seriesof data points {V1,V2,V3,
} separated by equal time intervalst. A simple formula for
numerical integration is thetrapezoidal rule, which involves
approximating the areaunder a section of a curve by a trapezoid.
This meansapproximating the curve betweenV1 andV2 by a straight
line(Figure 54-15) and calculating the area A under it as
(54-5) AV V
t+ 1 22
V
.
Differential pressuretransducer
Resistive element
FIGURE 54-14 The pneumotachograph.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
8/16
630 Clinical Respiratory Physiology
The areaA under a section of curve is then simply the sumof all
the individual As, thus
(54-6)
There are other more accurate, and more complicated,numerical
integration schemes. However, the key thing isthat t should be
small enough so that the errors involvedin approximating the true
curve between points isnegligible. This can be tested for by
integrating the datausing progressively smaller values for t, until
the results donot change.
MEASUREMENT OF LUNG FUNCTION
Now that a set of respiratory data has been collected andstored
on a computer, as described above, we are faced withthe task of
having to interpret it. How this is done dependsvery much on the
nature of the data collected. In most cases,however, the assessment
of lung function from respiratorydata is based on some model
idealization of the real systemunder study. The model is only
useful if it behaves like thereal system to a satisfactory degree.
It is therefore crucial tounderstand what model is being invoked
whenever lungfunction is being assessed so that the suitability of
the modelcan be evaluated. In most applications, the model
concernedis very simple, typically involving only a single
compart-ment. In some cases, the model may be very complicatedwith
multiple alveolar compartments and airway branchesrepresented.
Regardless of the level of model complexity,however, it is crucial
that any investigation of mechanicallung function begin with an
understanding of the mathe-matical model being invoked.
FORCED EXPIRED FLOWHaving just expounded on the importance of
models in theanalysis of lung function data, it turns out that the
tradi-tional mainstay of clinical pulmonary function testing,
the
A A
VV V V
V
ii
n
nn
+ + + + +
=
1
12 3 12 2
tt
forced expiration, yields quantities that are usually treated
aspurely empirical. The forced vital capacity (FVC) and theforced
expiratory volume in 1 second (FEV1) are widelyused either
individually or as a ratio to diagnose a variety ofcommon lung
pathologies. The great advantage of the forcedexpiration is that it
can be performed easily in an outpatientsetting, requiring nothing
more than a device for measuringflow (or volume) and some
cooperation from the subject.
The measuring device must be able to measure flows ofgreater
than 10 L.s1 with a frequency response that cap-tures the rapid
onset of flow at the start of a maximal forcedexpiration beginning
from total lung capacity. There arecommercially available systems
designed specifically for thistask, either by direct spirometric
measurement of exhaledvolume or by pneumotachograph measurement of
flow.
The clinical utility of forced expired flows arises from
thephenomenon of flow limitation, whereby exhaled flowreaches a
maximum value independent of further increasesin expiratory muscle
activity. Subjects with normal musclefunction can reach this
limiting flow over most of the vitalcapacity range. The limiting
flow is reduced in obstructive
lung disease, and the relationship of flow to exhaled
volumeassumes shapes that are characteristic of various
lungpathologies. Detailed accounts of the flow-volume curve andits
relation to pulmonary disease can be found in standardtexts.23
Unfortunately, the underlying mechanical mecha-nisms in the lung
responsible for producing the flow-volume loop are complex and
nonlinear, so parameters suchas FVC and FEV1 are not easily related
to a model of the res-piratory system. Consequently, making the
link betweenfunction and lung structure from forced expired flows
hasnot been straightforward. In other words, although parame-ters
such FVC and FEV1 are sensitive to both obstructiveand restrictive
lung disease, it is unclear how to deduce the
site or nature of an abnormality from the values of
theseparameters, although some sophisticated computer model-ing
studies have attempted to elucidate the relationshipsbetween the
forced expired flow-volume loop and the phys-ical properties of the
lungs.24 Nevertheless, the convenienceof measuring forced expired
flows and their diagnostic util-ity make this technique the most
clinically important of alllung function measurements.
METHODS BASED ON THE SINGLE-COMPARTMENTMODELThe model of
respiratory or pulmonary mechanics most fre-quently employed as the
basis for lung function measure-ments is that of a single elastic
compartment served by asingle flow-resistive airway (Figure 54-16).
This modelassumes that the lungs are homogeneously ventilated
andthat all alveolar pressures are equal to each other at all
times.
Plethysmography Whole-body plethysmography com-plements the
measurement of forced expired flows as theother major methodology
for measuring lung function incurrent clinical use. Plethysmography
is used to measuretwo important parameters of lung function,
thoracic gas vol-ume (TGV) and airway resistance (Raw), both under
theassumption of the single-compartment linear model. The
V (t)
t2
t3
t1
t
.
A1 A2
FIGURE 54-15 Trapezoidal integration of flow involves
connect-ing each sampled flow value by straight line and summing
the areasunder each trapezoid.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
9/16
FIGURE 54-17 Body plethysmograph used to measure A, TGV and B,
Raw. Pao is airway opening pressure, Pbox is pressure inside
theplethysmograph, and V is mouth flow.
Measurement Techniques in Respiratory Mechanics 631
calculation of TGV and Raw using a body plethysmograph iscovered
in numerous other articles and books23 and so isdescribed only
briefly here.
TGV is measured first by having the subject make breath-ing
efforts against a closed airway while the change in air-way opening
pressure (Pao) is measured (Figure 54-17A).At the same time, the
pressure in the plethysmograph or theflow leaving it (depending on
whether it is a pressure or flowbox) provides a measure of changes
in total body volume(V). Assuming that the only compressive part of
the bodyis the gas in the lungs, Vis equal to the compression of
thethoracic gas. Applying Boyles law gives
(54-7)
where we have equated 1 atmosphere to 1,000cm H2O inthe
denominator on the left side of Equation 54-7, whichcan be
rearranged to give a measure of TGV.
Next, this measurement of TGV is used to estimate Raw byhaving
the subject pant while completely enclosed inside
P VTGV
ao
1000
the plethysmograph. Flow (V) is measured at the subjectsmouth
with a pneumotachograph while pressure (Pbox)inside the
plethysmograph is measured (Figure 54-17B).Pbox varies because of
two factors. One of these is that gasinspired from the
plethysmograph becomes humidified andheated to body temperature,
thereby increasing in volume.This increases the combined volume of
the remainingplethysmographic gas and the subjects body and so
com-
presses the plethysmographic gas. The other factor is that
anegative pressure in the thorax is required for inspirationand the
converse for expiration. This results in compressivevolume changes
in the thoracic gas that are again manifestas changes in the
combined volume of plethysmographic gasand subject. To the extent
that the first source of changes inPbox can be ignored, the changes
in Pbox can be equated tocompressive changes in thoracic gas
volume, which can thenbe used, again via Boyles law, to infer the
changes inalveolar pressure (Palv). The difference between Palv and
Paodivided byVthen yields a measure ofRaw.
The plethysmographic measurement of TGV and Rawassumes that the
lungs are a homogeneously ventilated (ie,
effectively single-compartment) system. This works well innormal
lungs but may not in severely diseased lungs inwhich obstructed
airways can lead to marked differencesbetween Palv and Pao when
panting against a closed airway.
25
An unrestrained version of plethysmography has beenused in an
attempt to assess lung function in infants26 andsmall animals.27
This technique involves merely measuringvariations in Pao as the
subject breathes while inside the box.Although these pressure
swings arguably give informationabout the pattern of breathing,28
they cannot provide mean-ingful information about respiratory
mechanical function,29
despite recent claims to the contrary.30,31
Resistance and Elastance The single-compartmentmodel of
respiratory mechanics (see Figure 54-16) isdescribed by a simple
and extremely useful mathematicalequation if it is linear. If the
resistive pressure drop betweenone end of the airway and the other
is considered to be pro-portional to the flow of gas (V) through
it, then the constantof proportionality (R) is termed resistance.
Similarly, theelastic recoil pressure inside the compartment is
taken as
FIGURE 54-16 The single-compartment model of the
respiratorysystem. R is resistance and E is elastance (see Equation
54-8).
E
R
Pao
Pao
V
.
A B
Pbox Pbox
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
10/16
632 Clinical Respiratory Physiology
proportional to the volume of the compartment above someelastic
equilibrium volume, with its constant of proportion-ality (E)
termed elastance. Finally, we must account for thepossibility that
the pressure (P) applied across the model(from the entrance to the
airway through to the outside ofthe elastic compartment) has some
finite value P0 when Vand Vare both zero. Simple addition of
pressures shows thatP is the sum of the resistive and elastic
pressures, thus,
P(t) RV(t) EV(t) P0 (54-8)
where we have written the variables P,V, and Vexplicitly
asfunctions of time (t) to remind us that they all vary
duringbreathing.
Equation 54-8 is used in respiratory investigations to esti-mate
R, E, and P0 via multiple linear regression. This pro-vides those
values ofP, V, and Vthat, when used in the rightside of Equation
54-8, provide the closest approximation tothe measured P in the
left side. Closest here means inthe least squares sense, which
means that the sum of thesquared differences between the measured
value ofP and themodel values is minimal. R and E are taken as
measures of
the resistance and elastance of the lung or respiratory sys-tem,
which in a sense they are. Strictly speaking, however, Rand E are
nothing more than the parameters of a simplemodel (see Figure
54-16) that has been forced to match themeasured signals as well as
possible. The usefulness ofR andE as reflections of physiology thus
lies in the degree towhich the single-compartment linear model
accuratelydescribes the behavior of the system under study. In
manycases, this accuracy is acceptable, such as the exampleshown in
Figure 54-18 of a patient with chronic obstructivelung disease
being mechanically ventilated in the intensivecare unit.
When the single-compartment linear model does
describe a set of respiratory data to an acceptable degree
ofaccuracy, one is then faced with the task of assigning a
phys-iologic interpretation to the values ofR and E it provides.
Itmight seem obvious, for example, that R would correspondto the
flow resistance of the airway tree. However, this turnsout not to
be the case, at least not entirely. Studies with thealveolar
capsule in dogs and other animals have allowedtotal lung resistance
(ie, R) to be partitioned into airwayresistance and tissue
resistance.11,32 The latter has beenshown to depend greatly on the
frequency at which thelungs are oscillated and, at normal breathing
frequencies,may constitute the great majority ofR.13 It is not
until fre-quency gets well above the range of normal breathing
(aboveabout 2Hz) that the tissue component ofR decreases to
thepoint where R is a good reflection of airway
resistancealone.3335 In the intact animal, R also contains a
significantcontribution from the chest wall.36
Nonlinear Single-Compartment Models There are situ-ations in
which the single-compartment linear model doesnot describe a set of
respiratory data with acceptable accu-racy. The model must then be
replaced by a more realistic(and invariably more complex) model. An
example typicallyoccurs when the volume excursions of the lungs
becomelarge or when the stiffness of the lung tissue increases
in
certain diseases. In this case, one often finds that thedynamic
elastic behavior of the tissues is significantly betterdescribed by
a curvilinear function of volume rather than astraight line, as in
the linear model. For example, it has beenshown in both humans37
and animals38 that a nonlinearmodel with the equation
P(t) RV(t) E1V(t) E2V2(t) P0 (54-9)
sometimes fits the data significantly better than the
linearmodel above (see Equation 54-8). The nonlinear model
isstructurally the same as the linear model in that it still
hasonly a single compartment being ventilated through a
singleairway. The difference is that the elastic properties of the
tis-sues surrounding the compartment are nonlinear. Similarly,the
linear resistance term in Equation 54-8 can be replacedby two terms
representing a flow-dependent resistance asoriginally proposed by
Rohrer.38 Which of these modelsshould be used to describe a given
set of respiratory data canbe decided using, for example, the
F-ratio test applied to themean squared differences between
measured P and P pre-dicted by the various models.38
Another use of the single-compartment model ofrespiratory
mechanics arises when the stiffness of the lungor respiratory
system is assessed from the quasistatic pressure-volume (P-V)
curve. The P-V curve is obtained by inflating
0 1 2
0
10
20
30
data
model fit
Time (s)
Pressure
(cmH2O)
0.0
0.5
1.0
Volume(l)
-2
0
2
Flow
(l/s)
FIGURE 54-18 Example of pressure, flow, and volume data over
asingle breath from a mechanical ventilated patient in the
intensivecare unit. The lower panel also shows the fit to pressure
producedby Equation 54-8.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
11/16
Measurement Techniques in Respiratory Mechanics 633
and deflating the lungs, either continuously or in steps,slowly
enough that the resistive pressure drop across theairways can be
neglected. The result is a relationship thatembodies the elastic
properties of the pulmonary or respira-tory tissues, viewed as a
single compartment. The modelinvoked to account for the P-V curve
is thus again a single-compartment model, but now it is nonlinear
because theelastic recoil pressure inside the compartment increases
dis-
proportionately as volume approaches total lung capacity.
Acommonly used equation for describing the descending limbof the
P-V curve is the exponential expression39
VA BeKP (54-10)
where A, B, and K are constants chosen to make the rightside of
the equation match the left side as closely aspossible.
The ascending limb of the P-V curve lies to the right ofthe
descending limb (Figure 54-19), reflecting a phenome-non known as
hysteresis. The amount of hysteresis dependson the volume range
over which Vis cycled and is caused bya number of factors. One of
the most important is recruit-
ment of closed airspaces during inspiration that remainopen
during expiration. Hysteresis may become markedlyenhanced in
pathologies such as acute lung injury.40
METHODS BASED ON MULTICOMPARTMENT MODELSThe single-compartment
linear model (see above) generallydescribes respiratory
pressure-flow data well when volumeexcursions are modest and the
volume oscillations are con-centrated around a single frequency,
such as pertains, forexample, during normal breathing or mechanical
ventilation.However, the values ofR and E obtained using this
modelvary with frequency. In particular, R decreases markedly
asfrequency is increased over the range of normal breathing,
whereas E correspondingly increases. The main reason forthis
frequency dependence ofR and E in normal lungs is thefact that the
respiratory tissues are viscoelastic, that is, theyexert a recoil
pressure that is a function not only of volumebut also of volume
history.41 In diseased lungs, additionalvariation of R and E with
frequency may be caused byregional variations in mechanical
function throughout thelung, leading to transient redistribution of
gas as the lungsare dynamically inflated and deflated.42,43 In any
case, thesingle-compartment linear model no longer suffices as
adescription of pulmonary or respiratory mechanics whenmultiple
frequencies are involved. Instead, we need toinvoke models
featuring two or more compartments toaccount for regional
differences in mechanical functionthroughout the lung.44
Interrupter Technique A technique for assessing lungfunction
that was first introduced nearly a century agoinvolves the rapid
interruption of airflow at the airway open-ing, while pressure just
behind the point of interruption ismeasured. Initially, it was
thought that this maneuver wouldsimply obliterate any resistive
pressure drop across the air-ways, so that the observed sudden
change in pressure wouldreflect Raw. However, work over the past
two decades hasshown that the sudden change in pressure occurring
with
0 5 10 15
-10
0
10
20
30
40
Time (s)
Pressure
(cmH2O)
0.0
0.2
0.4
0.6
0.8
1.0
Volume(ml)
0 10 20 30
0.0
0.2
0.4
0.6
0.8
Volume(l)
Pressure (cmH2O)
A
B
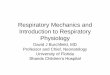
FIGURE 54-19 A, Pressure and volume data obtained from a
mouseduring stepwise inflation and deflation of the lungs. B,
Ascendingand descending limbs of the quasistatic pressure-volume
(P-V)curve derived from the plateaus of the data in Figure
54-19A.
interruption of flow is accompanied by some rapid
dampedoscillations and a subsequent further transient change
inpressure to a stable plateau (Figure 54-20). The oscillationsare
mainly owing to ringing of the gas in the central air-ways,45
whereas the secondary slow pressure change is due
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
12/16
634 Clinical Respiratory Physiology
to the viscoelastic properties of the respiratory tissues
whenthe lung is normal12 and may be accentuated by gas
redistri-bution in pathologic situations.46 Interpreting the
initialrapid and secondary slower pressure changes has been doneon
the basis of two-compartment models of
respiratorymechanics.44,47,48
The interrupter technique is currently gaining interestamong
pediatricians,49 who face a particular challenge intrying to assess
lung function in young children and infantsunable to perform the
voluntary maneuvers necessary togenerate forced expired flows.
However, the interruption offlow is merely a specialized kind of
flow perturbation.Understanding the information obtained by
applying gen-eral flow perturbations to the lungs is best done in
the con-text of the forced oscillation technique and impedance.
Input Impedance The frequency dependence ofR and Ehas led
respiratory researchers to move to a more global assess-ment of
mechanics based on a quantity known as input imped-ance (Zin). Zin
can be determined over a range of frequenciesby subjecting the
lungs to an oscillatoryVsignal that containsmultiple frequencies.
Zin is then determined by taking the ratioof the Fourier transform
ofP to the Fourier transform ofV.This yields a complex function of
frequency
Zin(f) R(f) iX(f) (54-11)
with a real part R(f) and an imaginary part X(f), where. The
value ofR at each value off is equal to the
resistance of an equivalent single-compartment linearmodel, so
the R(f) is called the resistance. X(f) is called thereactance and
at each f is related to the elastance of theequivalent
single-compartment model by
(54-12)X fE f
f( )
( )=
2
i = 1
Zin is thus nothing more than a description of how R and Evary
over a range of frequencies. Zin still requires that thesystem
under study be linear. This assumes that whatevervalues ofR and E
are obtained at a particular frequency, theirvalues do not depend
on the amplitudes of the P, V, and Vsignals used to measure them
(which, of course, is neverprecisely the case in practice).
Forced Oscillation Technique The measurement ofZin isachieved by
the so-called forced oscillation technique in whicha flow generator
(such as a loudspeaker or piston pump) isused to drive an
oscillatory flow into the lungs via the airwayopening.50 The
frequency range over which the signal oscil-lates determines the
kind of information that will be obtainedabout respiratory
mechanical function. At frequencies belowabout 2Hz, much ofZin is
determined by the rheologic prop-erties of the tissues, as well as
regional mechanical hetero-geneities throughout the lung should
they exist. Regionalheterogeneities can affect the shape of Zin
above 2Hz aswell.42,43 At frequencies of hundreds of Hz one obtains
infor-mation about the acoustic characteristics of the
airways.51
Whatever the frequency range, the interpretation ofZin in
physiologic terms requires some kind of model of thesystem under
investigation. For example, normal respiratoryor pulmonary Zin is
described very accurately below about20 Hz by a model consisting of
a uniformly ventilatedcompartment surrounded by viscoelastic
tissue. The com-partment is served by a single airway having a
newtonianresistance RN, whereas the viscoelastic tissue has
animpedance with real and imaginary parts that both
decreasehyperbolically withf. The equation for the impedance of
thisconstruct, which is frequently referred to as the
constant-phase model, is35
(54-13)
where the parameter is related to the two tissue parame-ters via
the relation
(54-14)
Gti characterizes the viscous dissipation of energy in the
tis-sues and so is related (but not equivalent to) tissue
resist-ance. Hti characterizes the storage of elastic energy in
thetissues and is closely related to E. Iis an inertance
reflectingthe mass of the gas in the central airways. The four
parame-ters RN, I, Gti, and Hti together account for the entire
fre-quency spectrum of Zin below 20Hz in a convenient andcompact
way. They also allow Zin to be partitioned into acomponent
pertaining to the airways (ie, RN and I) and acomponent pertaining
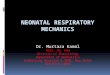
to the lung periphery (ie, Gti and Hti).Figure 54-21 shows an
example of the fit to Zin provided byEquation 54-13.
Other Respiratory Impedances The calculation ofrespiratory
impedance is not limited to Zin obtained from Pand V at the airway
opening. Any relevant pressure andflow signals will do, although
the impedance obtained will
= 2 1
tanH
Gti
ti
Z f R i fI G iHf
in ti tiN( )( )= + +
22
0.0 0.5 1.0
Pressure(arbitraryuntis)
Time (s)
Initial rapid pressure change
Secondary slowerpressure change
Damped high-frequencyoscillations
Point of flowinterruption
FIGURE 54-20 Schematic representation of airway opening
pres-sure recorded during interruption of expiratory flow. An
initialalmost instantaneous jump in pressure is accompanied by
rapid
damped oscillations, which are followed by a slower further
pres-sure change.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
13/16
Measurement Techniques in Respiratory Mechanics 635
be different in each case. For example, if pressure is
oscil-lated around the body surface while flow is measured atthe
mouth, the impedance obtained is known as transferimpedance (Ztr).
Ztr has been used in numerous studies inboth animals52 and
humans.5355 Although in principle Ztrshould give similar
information about lung function to Zin,its measurement may be
associated with some practicaladvantages. First, when the distal
airways of the lungbecome significantly constricted, the flow
oscillationsapplied at the mouth to measure Zin may become
shuntedto a large degree into the central airways that have a
finitecompliance.43 If the amount of flow reaching the lungsbecomes
small to the point that it approaches the noise level
of flow measurements at the mouth, then one effectivelyloses the
ability to probe the lung periphery. In contrast,when pressure
oscillations are applied at the body surface,flow is driven from
the lung periphery toward the trachea,and shunting into the central
airway compartment isminimized. This means that all flow measured
at the mouthcomes from the lung periphery, giving Ztr a
signal-to-noiseadvantage over Zin for the investigation of
severelyconstricted lungs.
Another recently developed variant of respiratory imped-ance
uses the heart as the oscillatory source, producing whathas been
termed output impedance.56 When a subjectrelaxes with an open
glottis, the beating heart perturbsthe lungs sufficiently to
generate a small flow that can bemeasured at the mouth. When the
airway opening isoccluded, corresponding pressure oscillations are
measuredjust behind the point of occlusion. The impedance
deter-mined from these two signals was found to have anessentially
zero imaginary part and a real part that corre-sponded closely to
the resistance of the conducting airways,as measured by Zin.
56
Yet a further type of respiratory impedance has beenobtained by
applying forced oscillations in flow to thelungs of dogs through an
alveolar capsule.57 The resultingalveolar input impedance (ZA)
between 26 and 200Hz
was found to be well described by a simple model consistingof a
subpleural alveolar compartment connecting to therest of the lungs
by a terminal airway compartment. Themagnitude ofZA was found, on
the basis of an anatomicallyaccurate computer model of the dog
lung,58 to correspondto that expected of a single lung acinus. When
ZA wasfollowed during the development of bronchoconstriction,the
response of the lung periphery was demonstrated to be
extremely heterogeneous both spatially and temporally.59,60
The information obtained about lung mechanical functionthus
depends on the site at which flow perturbations areapplied and
where pressures and flows are measured. It alsodepends to a great
extent on the nature of the flowperturbations themselves. Measuring
lung mechanics duringnormal breathing in a conscious subject using
an esophagealballoon has the advantage of allowing the subject to
remainin a reasonably natural state. However, it suffers from the
dis-advantage that the subject is free to choose the breathing
pat-tern, which may change with an intervention. This itself
willaffect the measurement of mechanics regardless of any
truechanges in the intrinsic mechanical properties of the
airways
or tissues. Thus, one faces a trade-off between minimizingthe
interventional nature of the measurement and controllingfor
confounding variables. This situation has been likened tothe
uncertainty principle of quantum mechanics.61
SUMMARY
The quantitative study of respiratory mechanics
involvesmeasurement at two levels, namely the measurement of theraw
signals that carry the mechanical information and themeasurement of
key physiologic parameters that embody thisinformation. Measurement
of signals requires the use of trans-ducers for recording pressure,
flow, and volume and comput-
ers for capturing and storing the data. Measurement
ofphysiologic parameters involves matching the measured sig-nals to
a suitable mathematical model of respiratory mechan-ics. There are
many decisions to be made in achieving theseends, such as which
type of transducer to use, how fast tosample the signals, what
resolution of analog-to-digital con-verter is required, what kind
of perturbation should beapplied to the respiratory system, and
what mathematicalmodel should be invoked to interpret the data.
There is nouniversally correct decision for any of these issues
because theappropriate action to be taken depends on the
physiologicquestions being addressed. These questions, whatever
theyare, will determine what mathematical model of
respiratorymechanics should be invoked, what frequency response
char-acteristics are required of the transducers, what data
samplingrate is needed, and so on. It is therefore important for
the res-piratory scientist to understand the basics of
measurementtheory as it applies to both the collection of
physiologicsignals and their interpretation through mathematical
models.Such an understanding minimizes the risk, for example,
ofbeing misled by measurement artifact from a transducer thatis not
up to the task required of it or of being confused by theapparently
bizarre behavior of a calculated parameterobtained using a model
that does not apply to the situation athand.
0 5 10 15 20
-14
-12
-10
-8
-6
-4
-2
0
2
Real part
Imaginary part
Model fit
Impedan
ce(cmH2O.s/m)
Frequency (Hz)
FIGURE 54-21 Fit of constant-phase model (Equation 54-13) toZin
data from a mouse.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
14/16
636 Clinical Respiratory Physiology
REFERENCES
1. Jackson AC, Vinegar A. A technique for measuring
frequency
response of pressure, volume, and flow transducers. J Appl
Physiol 1979;47:4627.
2. Duvivier C, Rotger M, Felicio da Silva J, et al. Static
and
dynamic performances of variable reluctance and piezore-
sistive pressure transducers for forced oscillation measure-
ments. Eur Respir J 1991;1:14650.
3. Bates JHT, Sly PD, Sato J, et al. Correcting for the
Bernoulli
effect in lateral pressure measurements. Pediatr Pulmonol
1992;12:2516.
4. Navalesi P, Hernandez P, Laporta D, et al. Influence of site
of tra-
cheal pressure measurement on in situ estimation of endo-
tracheal tube resistance. J Appl Physiol 1994;77:2899906.
5. Couture JG, Chartrand D, Gagner M, Bellemare F.
Diaphragmatic and abdominal muscle activity after endo-
scopic cholecystectomy. Anesth Analg 1994;78:7339.
6. Baydur A, Behrakis PK, Zin WA, et al. A simple method for
assessing the validity of the esophageal balloon technique.
Am Rev Respir Dis 1982;126:78891.
7. Dechman G, Sato J, Bates JHT. Factors affecting the accuracy
of
esophageal balloon measurement of pleural pressure in
dogs. J Appl Physiol 1992;72:3838.
8. Peslin R, Navajas D, Rotger M, Farre R. Validity of
theesophageal balloon technique at high frequencies. J Appl
Physiol 1993;74:103944.
9. Panizza JA. Comparison of balloon and transducer catheters
for
estimating lung elasticity. J Appl Physiol 1992;72:2315.
10. Wang CG, DiMaria G, Bates JH, et al. Methacholine-induced
air-
way reactivity of inbred rats. J Appl Physiol 1986;61:21805.
11. Fredberg JJ, Keefe DH, Glass GM, et al. Alveolar
pressure
nonhomogeneity during small-amplitude high-frequency
oscillation. J Appl Physiol 1984;57:788800.
12. Bates JH, Ludwig MS, Sly PD, et al. Interrupter
resistance
elucidated by alveolar pressure measurement in open-
chest normal dogs. J Appl Physiol 1988;65:40814.
13. Ludwig MS, Dreshaj I, Solway J, et al. Partitioning of
pulmonary
resistance during constriction in the dog: effects of volume
history. J Appl Physiol 1987;62:80715.
14. Ludwig MS, Romero PV, Bates JH. A comparison of the
dose-
response behavior of canine airways and parenchyma. J
Appl Physiol 1989;67:12205.
15. Tomioka S, Bates JH, Irvin CG. Airway and tissue mechanics
in
a murine model of asthma: alveolar capsule vs. forced
oscillations. J Appl Physiol 2002;93:26370.
16. Renzi PE, Giurdanella CA, Jackson AC. Improved frequency
response of pneumotachometers by digital compensation.
J Appl Physiol 1990;68:3826.
17. Farre R, Peslin R, Navajas D, et al. Analysis of the
dynamic
characteristics of pressure transducers for studying
respira-
tory mechanics at high frequencies. Med Biol Eng Comput
1989;27:5316.
18. Schuessler TF, Maksym GN, Bates JHT. Estimating tracheal
flowin small animals. Proceedings of the 15th Annual
International Meeting of the I.E.E.E. Engineering in
Medicine and Biology Society; 1993 October 2831; San
Diego, California. p. 5601.
19. Schibler A, Hall GL, Businger F, et al. Measurement of lung
vol-
ume and ventilation distribution with an ultrasonic flow
meter in healthy infants. Eur Respir J 2002;20:9128.
20. Clary AL, Fouke JM. Fast-responding automated airway
tem-
perature probe. Med Biol Eng Comput 1991;29:5014.
21. Cohen KP, Ladd WM, Beams DM, et al. Comparison of imped-
ance and inductance ventilation sensors on adults during
breathing, motion, and simulated airway obstruction. IEEE
Trans Biomed Eng 1997;44:55566.
22. Aliverti A, Dellaca R, Pelosi P, et al. Compartmental
analysis
of breathing in the supine and prone positions by opto-
electronic plethysmography. Ann Biomed Eng 2001;
29:6070.
23. Gold WM. Pulmonary function testing. In: Murray JF, Nadel
JA,
editors. Textbook of respiratory medicine. Philadelphia
(PA): W.B. Saunders; 2000. p. 781882.
24. Lambert RK, Wilson TA, Hyatt RE, Rodarte JR. A
computational
model for expiratory flow. J Appl Physiol 1982;52:4456.
25. Shore S, Milic-Emili J, Martin JG. Reassessment of body
plethys-
mographic technique for the measurement of thoracic gas
volume in asthmatics. Am Rev Respir Dis 1982;126:51520.
26. Drorbaugh J, Fenn W. A barometric method for measuring
ventilation in newborn infants. Pediatrics 1955;16:817.
27. Hamelmann E, Schwarze J, Takeda K, et al. Noninvasive
meas-
urement of airway responsiveness in allergic mice using
barometric plethysmography. Am J Respir Crit Care Med
1997;156:76675.
28. Epstein RA, Epstein MA, Haddad GG, Mellins RB. Practical
implementation of the barometric method for measure-
ment of tidal volume. J Appl Physiol 1980;49:110715.
29. Lundblad LK, Irvin CG, Adler A, Bates JH. A reevaluation of
the
validity of unrestrained plethysmography in mice. J Appl
Physiol 2002;93:1198207.
30. Finotto S, Neurath MF, Glickman JN, et al. Development
ofspontaneous airway changes consistent with human
asthma in mice lacking T-bet. Science 2002;295:3368.
31. Chong BT, Agrawal DK, Romero FA, Townley RG. Measurement
of bronchoconstriction using whole-body plethysmograph:
comparison of freely moving versus restrained guinea pigs.
J Pharmacol Toxicol Methods 1998;39:1638.
32. Fredberg JJ, Ingram RH Jr, Castile RG, et al. Nonhomogeneity
of
lung response to inhaled histamine assessed with alveolar
capsules. J Appl Physiol 1985;58:191422.
33. Sato J, Davey BL, Shardonofsky F, Bates JH.
Low-frequency
respiratory system resistance in the normal dog during
mechanical ventilation. J Appl Physiol 1991;70:153643.
34. Hantos Z, Daroczy B, Suki B, Nagy S. Low-frequency
respira-
tory mechanical impedance in the rat. J Appl Physiol 1987;
63:3643.35. Hantos Z, Daroczy B, Suki B, et al. Input impedance
and
peripheral inhomogeneity of dog lungs. J Appl Physiol
1992;72:16878.
36. Bates JH, Abe T, Romero PV, Sato J. Measurement of
alveolar
pressure in closed-chest dogs during flow interruption.
J Appl Physiol 1989;67:48892.
37. Bersten AD. Measurement of overinflation by multiple
linear
regression analysis in patients with acute lung injury. Eur
Respir J 1998;12:52632.
38. Wagers S, Lundblad L, Moriya HT, et al CG. Nonlinearity
of
respiratory mechanics during bronchoconstriction in mice
with airway inflammation. J Appl Physiol 2002;92:18027.
39. Salazar E, Knowles JH. An analysis of pressure-volume
charac-
teristics of the lungs. J Appl Physiol 1964;19:97104.40.
Hickling KG. The pressure-volume curve is greatly modified
by recruitment. A mathematical model of ARDS lungs. Am J
Respir Crit Care Med 1998;158:194202.
41. Bates JH, Brown KA, Kochi T. Respiratory mechanics in the
nor-
mal dog determined by expiratory flow interruption. J Appl
Physiol 1989;67:227685.
42. Kaczka DW, Ingenito EP, Israel E, Lutchen KR. Airway and
lung
tissue mechanics in asthma. Effects of albuterol. Am J
Respir Crit Care Med 1999;159:16978.
43. Lutchen KR, Greenstein JL, Suki B. How inhomogeneities
and
airway walls affect frequency dependence and separation
of airway and tissue properties. J Appl Physiol 1996;80:
1696707.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
15/16
Measurement Techniques in Respiratory Mechanics 637
44. Similowski T, Bates JHT. Two compartment modelling of
respiratory system mechanics at low frequencies: gas
redistribution or tissue rheology? Eur Respir J 1991;4:3538.
45. Romero PV, Sato J, Shardonofsky F, Bates JH.
High-frequency
characteristics of respiratory mechanics determined by
flow interruption. J Appl Physiol 1990;69:16828.
46. Ludwig MS, Romero PV, Sly PD, et al. Interpretation of
interrupter resistance after histamine-induced constriction
in the dog. J Appl Physiol 1990;68:16516.
47. Bates JH, Baconnier P, Milic-Emili J. A theoretical analysis
of
interrupter technique for measuring respiratory mechanics.
J Appl Physiol 1988;64:220414.
48. Bates JH, Rossi A, Milic-Emili J. Analysis of the behavior
of the
respiratory system with constant inspiratory flow. J Appl
Physiol 1985;58:18408.
49. Frey U, Silverman M, Kraemer R, Jackson AC.
High-frequency
respiratory input impedance measurements in infants
assessed by the high speed interrupter technique. Eur
Respir J 1998;12:14858.
50. MacLeod D, Birch M. Respiratory input impedance measure-
ment: forced oscillation methods. Med Biol Eng Comput
2001;39:50516.
51. Dorkin HL, Lutchen KR, Jackson AC. Human respiratory
input
impedance from 4 to 200Hz: physiological and modeling
considerations. J Appl Physiol 1988;64:82331.52. Sobh JF, Lilly
CM, Drazen JM, Jackson AC. Respiratory transfer
impedance between 8 and 384Hz in guinea pigs before and
after bronchial challenge. J Appl Physiol 1997;82:17281.
53. Marchal F, Bouaziz N, Baeyert C, et al. Separation of airway
and
tissue properties by transfer respiratory impedance and
thoracic gas volume in reversible airway obstruction. Eur
Respir J 1996;9:25361.
54. Peslin R, Gallina C, Duvivier C. Respiratory transfer
imped-
ances with pressure input at the mouth and chest. J Appl
Physiol 1986;61:816.
55. Peslin R, Gallina C, Teculescu D, Pham QT. Respiratory
input
and transfer impedances in children 9-13 years old. Bull
Eur Physiopathol Respir 1987;23:10712.
56. Bijaoui E, Baconnier PF, Bates JH. Mechanical output
imped-
ance of the lung determined from cardiogenic oscillations.
J Appl Physiol 2001;91:85965.
57. Davey BL, Bates JH. Regional lung impedance from forced
oscillations through alveolar capsules. Respir Physiol 1993;
91:16582.
58. Mishima M, Balassy Z, Bates JH. Assessment of local lung
impedance by the alveolar capsule oscillator in dogs: a
model analysis. J Appl Physiol 1996;80:116572.
59. Balassy Z, Mishima M, Bates JH. Changes in regional lung
impedance after intravenous histamine bolus in dogs:
effects of lung volume. J Appl Physiol 1995;78:87580.
60. Mishima M, Balassy Z, Bates JH. Acute pulmonary response
to
intravenous histamine using forced oscillations through
alveolar capsules in dogs. J Appl Physiol 1994;77:21408.61.
Bates JH, Irvin CG. Measuring lung function in mice: the
phenotyping uncertainty principle. J Appl Physiol 2003;
94:1297306.
-
7/27/2019 ch54MEASUREMENT TECHNIQUES IN RESPIRATORY
MECHANICS
16/16