Embed Size (px)
Citation preview

Cervical Spine Injuries
in ChildrenArturo S. Gastañaduy M.D.
Associate Professor of PediatricsLouisiana State University Health
Sciences CenterJuly 2010

Objectives
Importance Epidemiology Mechanisms of Injury Differences: Children vs. Adults Clinical Presentation Initial Management
of Cervical Spine Injuries in Children

Christopher Reeve as Superman

Christopher Reeve Paralyzed

Cervical Spine Injuries (CSI) in Children
EpidemiologyKokoska E. Patel J. Martin B.
Data Source NPTR 1994-1999
NPTR 1988-1998
TARN 1989-2000
Age (years) 0 - 20 0 - 20 0 - 15
Injured Children
24,740 75,172 19,538
CSI number (%)
408 (1.6) 1098 (1.5) 662 (3.4)
Males (%) 59 61 58
Cord Injury (%)
35 29 21.9
Mortality (%) 17 17 13

Cervical Spine Injuries in ChildrenMechanism of Injury
Mechanism
Kokoska E.
Patel J. Martin B.
MVA (%) 44 42 49.8
Sports (%) 16 14 7.4
Falls (%) 14 13 37.6
Pedestrian (%)
11 14 -
Bicycle (%)
6 5 -

Cervical Spine Injury in Children
Mechanism of Injury and Age
Mechanism
Young 0 - 10
Old11 - 20
p
MVA(%) 44 43 ns
Falls (%) 17 12 < .01
Pedestrian (%)
18 4 < .001
Bicycle (%) 3 8 < .01
Sports (%) 6 25 < .001

Cervical Spine Injuries in ChildrenType of Injury
Injury Type Kokoska E.%
Patel J.%
Fracture 56 56
Dislocation 25 22
Fracture/Dislocation
- 5
SCIWORASpinal cord injury
without radiological abnormality
19 17

Head and Cervical Spine Differences Children vs.
Adults Characterist
icsChildren Adults
Head/Body Large Small
Fulcrum C2 – C3 C5 – C6
Neck muscles, spine
ligaments
Weak, lax and elastic
Strong, stiff, ↓ elasticity
Vertebral bodies
Anterior wedging
Cartilaginous
No wedgingossified
Articulating facets
More horizontally
oriented
Vertically oriented

Head and Cervical Spine Differences Children vs.
Adults

Cervical Spine Injuries in Children
Age and Level of Injury
AgeYoung0 -10 years
Old11 -20 years
P
HighC1 – C4
85 56 < .01
LowC5 – C7
15 43 < .01

CSI in ChildrenAge and Type of Injury (from
Kokoska)Type Young
0 - 10Old
11 - 20 p
Fractures (%)
42 65 < .01
Dislocations (%)
31 20 < .01
SCIWORA (%)
27 15 < .01

Cervical Spine Injury in Children
Clinical Presentation Varies widely from: A four year old boy without history
of trauma, who was perfectly well before going to bed last night and woke up with pain to the neck and holds his head tilted to the right.
An unconscious 18 year old brought by EMS after a major MVA with history of multiple trauma including the head and neck.
What do we do?

Cervical Spine Injury ManagementFirst Things First
ABCs Protect Cervical Spine. “All children
with head and neck injuries, multiple trauma, neurological deficits have CSI until proven otherwise”
Goals: Stabilize primary injury and prevent secondary injuries.
Remember 3% - 25% of CSI occur during transit or early in the course of management.
Clearing the C-Spine is not an immediate goal.

Cervical Spine Injury ManagementObtain History
Details of events from patient and others
Mechanism of Injury Signs and symptoms Specific neurologic signs or
symptoms Drug ingestion or intoxication PMH: Previous trauma or surgery
Arthritis, syndromes, others

Cervical Spine Injury in ChildrenPhysical Exam
Motor deficit Sensory deficit Altered mental status Neck tenderness Torticollis Limitation of motion Neck muscle spasm Abnormal reflexes Clonus without rigidity
Diaphragmatic breathing without retractions
Spinal shock ↓BP + ↓HR
Priapism Decreased bladder
control Fecal retention Unexplained ileus Labile BP, flushing,
sweating Temperature
instability

Cervical Spine Immobilization
Hard collar + Spine Board Became familiar with the ones used
in your area Tallest collar that not hyperextend
the neck Backboard with occipital recess or
padding under shoulders and body Straps over the forehead, chin,
shoulders, hips, thighs and ankles. Be ready to log roll the patient if
vomit occurs

Cervical Spine Immobilization Assessment
Is the patient appropriately and fully immobilized?
Is the collar the correct size and type? Is the patient neck in neutral
position? Is the patient securely strapped to the
spine board? Has there been a shift in the patient
or the immobilization during transport?
Does immobilization interfere with the assessment and management of the ABCs?

Cervical Spine Clearing in Pediatric Trauma Patients
Slack SE, Clancy MJ: Comprehensive literature search of the studies on the subject (2004)
241 papers, 71 relevant No “Gold Standard” to identify all
CSI Many papers did not include clinical
follow up Only the National Emergency X-
Radiography Utilization Study NEXUS was considered valid for its purpose.

Clinical Clearing of the Cervical Spine
The NEXUS Study Prospective Observational Study:
34,000 pts. Radiographs were ordered at the
discretion of examining physician Mix of participating institutions Imaged patients received at least
cross-table lateral, AP and open mouth odontoid views.
Treating physicians completed data forms with demographics and the presence or absence of 5 low risk criteria.

Clinical Clearing the Cervical Spine
NEXUS Low-Risk Criteria
No midline cervical tenderness
No evidence of intoxication
No altered level of alertness
No focal neurological deficit
No distracting painful injury

Clinical Clearing the Cervical Spine
Results of NEXUS Study
< 18 years
≥ 18 years
Total
Number of cases
3,065905 < 9 years
31,004 34,069
CSI Patients 30 (0.98%)
4 < 9 years
788 (2.54%)
818 (2.4%)
Low-risk patients
603 (19.7%)
3706 (12.0%)
4309 (12.6%)
Low-risk patients with
CSI
0 8 8

Clinical Clearing the Cervical Spine
Results of NEXUS Study (cont.)Pediatric Group
Overall
Sensitivity 95% CI
100 %87.8 - 100
99. 2 %98.0 – 99.6
NPV 95% CI
100 %99.2 - 100
99.8 %99.6 - 100
Specificity95% CI
19.9 %18.5 – 21.3
12.93 %
PPV95% CI
1.2 %0.8 – 1.8
2.72 %

Clinical Clearing the Cervical Spine
NEXUS Study Conclusions No CSI was identified in the
pediatric group without at least one NEXUS risk factor
About 20% less radiographs would have been performed
However there were few pediatric patients with CSI. Lower end of CI: 87.8
Only 4 injured patients were younger than 9 yrs.
NEXUS criteria can be used with caution in pediatric patients ≥ 8 years.

If cervical spine can not be cleared clinically
Cervical Spine Radiographs
Maintain Cervical Spine Immobilization
C1-C7 Cross-table lateral: 80% of bony
lesions AP: lateral mass fractures Odontoid views in ≥ 9 yr. Waters
< 9yr Tree views: Dx 90% of CS
fractures

The ABCS of Radiographic Cervical Spine Evaluation
A. Alignment: Lordotic curves, malalignment, subluxation, distraction.
B. Bones: Fractures, anterior and posterior cervical columns, ossification centers
C. Cartilage: Intervertebral disk spaces, ossification centers
S. Soft Tissues: Prevertebral, predental spaces.

Clearing Cervical Spine by X Rays

Cervical Spine Flexion Injury
Flexion teardrop fracture Flexion of spine +
vertical axis compression
Anterior-inferior fracture of vertebral body
Anterior displacement of the fragment
Significant posterior ligament disruption
Extremely unstable

Cervical Spine Flexion Injury
Clay Shoveler Fracture Avulsion fracture
of the spinous process
Abrupt neck flexion in muscular individuals
Usually lower vertebrae
Fragment easily seen in lateral view
Stable

Cervical Spine Flexion Injury
Anterior subluxation Posterior ligament
complex rupture Anterior
longitudinal ligament preserved
No bony injury Widening of
interspinous processes distance
Anterior column intact
Stable in extension unstable in flexion

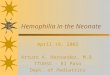
Posterior Cervical Line (PCL) of Swischuk
PCL connects the anterior aspect of the spinous processes of C1 and C3
If subluxation of C2 on C3, draw PCL
(A) No subluxation. PCL cannot be applied
(B) Subluxation: Anterior aspect of C2 spinous process misses PCL >2 mm (hangman’s fracture)
(C) Pseudosubluxation: Anterior aspect of C2 spinous process <2 mm or touches PCL

Cervical Spine Flexion Injury
Bilateral Facet Dislocation Involves annulus
and anterior & posterior ligaments
Upper vertebra inferior facets pass above and anterior to lower facets
Body displacement > half anterior-posterior diameter
Extremely unstable, disk herniation during reduction

Odontoid Fractures
Better seen in open mouth views.
Type I: fracture at the tip of the odontoid.
Type II: Fracture at the base of the odontoid.
Type III: Fracture extends to the body of the odontoid

Odontoid Process (Dens) Fracture
Fracture through base of dens. Dens and C1 posterior to C2

Indications forFlexion and Extension Views
To diagnose ligament injuries Alert patients No neurologic deficits Normal Cervical Spine (3 views) Neck pain or muscle spasm Patient able to actively flex and
extend neck

CT/MRI Indications
Altered mental status, risk factors C-spine incompletely visualized on plain films Abnormal or suspicious C-spine films Suspicion of injuries despite normal
radiographs CT Sensitivity and Specificity ≥ 98% MRI: better than CT for soft tissues:
SCIWORA

Cervical Spine Extension Injury
C1 Posterior arch fracture Neck
hyperextension C1 posterior arch
compressed by occiput and C2 spinous process
Lateral view: fracture line through posterior arch
No widening of pre-dental space

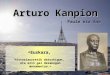
Two year old boy after major MVASpine CT

Same patient MRIDiagnosis: SCIWORA

Limitations for the routine use of the CT and MRI in the
evaluation of cervical spine in children
Cervical spine injuries are rare in children
CT radiation dose is 10 times > plain films
CT is more costly MRI availability is limited MRI difficult for critically ill child

C-spine injury Treatment
Stabilize primary injury and prevent secondary injuries
No Treatment Guidelines Neurosurgery ASAP Closed reduction + Halo
immobilization Surgery for ligament injuries Steroids: Controversial, no data for
children

Management Pitfalls for CSI
(from Haizlip JA; Scherrer PD) “I didn’t think she needed a cervical
collar, she was walking around at the scene of the accident”
“They secured him on an adult board without anything under him, since he is already secured we’ll just leave him like that”
She is 5 years old, said her neck didn’t hurt, so I thought it was OK to take her out of the collar”

Management Pitfalls for CSI
continued… “I am pretty sure that line on the x-
ray is just a growth plate. He looks fine and CS fractures in children are rare anyway”
“The x-ray tech can’t get this little girl to hold still and open her mouth for the odontoid view”
“The boy you sent for flexion-extension films says his neck hurts to bend. What shall we do?

Management Pitfalls for CSI
continued… “To be in the safe side, I get a CT in
every child with neck trauma”
“All her films were clear and she seems fine, I told the parents they have nothing to worry about”
“She is unconscious, however her x-rays and CT are normal thus I am going to take the collar off”

Selected References
Kokoska ER, Keller MS, Rallo MC, Weber TR. Characteristics of Pediatric Cervical Spine Injuries. J Pediatr Surg 2001; 36: 100-106
Patel JC, Tepas JJ, Mollit DL, Pieper P: Pediatric Cervical Spine Injuries: Defining the Disease. J Pediatr Surg 2001; 36: 373-376
Martin BW, Dykes E, Lecky FE: Patterns and risks in spinal trauma.Arch Dis Child 2004; 89: 860-865

Selected References
Viccellio P, Simon H, Pressman B, et al: A Prospective Multicenter Study of Cervical Spine Injury in Children. Pediatrics 2001; 108: 20-26
Slack SE, Clancy MJ: Clearing the Cervical Spine of Paediatric Trauma Patients. Emerg Med J. 2004; 21:189-193
Hadley MN: Management of Pediatric Cervical Spine and Spinal Cord Injuries. Neurosurgery 2002; 50 (3) S85-S99

Selected References
Haizlip JA, Scherrer PD: Emergency Evaluation of the Pediatric Cervical Spine. Pediatric Emergency Medicine Practice 2008; 5 (7) 1-24