Embed Size (px)
Citation preview

NEUROSURGICAL ANAESTHESIA AND INTENSIVE CARE
© 2004 The Medicine Publishing Company Ltd322ANAESTHESIA AND INTENSIVE CARE MEDICINE 5:10
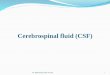
Cerebrospinal fluid (CSF) is a clear, colourless liquid, isotonic with (and similar in composition to) plasma, apart from the fact that it contains only traces of protein. It circulates around and within the CNS, occupying cavities within it and the subarachnoid space around it. The choroid plexuses of the lateral ventricles are largely responsible for its formation, but this is augmented by the smaller choroid plexuses of the third and fourth ventricles and by a seep-age from the surface of the brain. One can describe the CSF as circulating from the lateral ventri-cles through the interventricular foramina into the third ventricle and then by the aqueduct of the midbrain into the fourth ventricle (Figure 1). It leaves the fourth ventricle through its median and lateral apertures to enter the subarachnoid space near the pontine cistern. From this space around the base of the brain, the fluid ebbs and flows around the spinal cord and brain, descending as far as the lumbar cistern and ascending over the cerebellum, through the tentorial notch to the cerebrum and vault of the skull. The fluid is reabsorbed into the venous system largely by the arachnoid villi and granulations, which are most prominent in the superior longitudinal sinus. Some fluid is reabsorbed into perineural blood vessels. Arachnoid villi are microscopic projections that invaginate the walls of the cerebral venous sinuses. During infancy, clusters of these villi (especially those lining the superior longitudinal sinus) increase in size to form cauliflower-like clumps, the arachnoid granulations. These granulations increase in size and number throughout life. The subarachnoid space is narrowest over the cerebral hemi-spheres, but in some areas, where the arachnoid bridges over subdivisions of the brain, wider spaces (cisterns) are formed. The largest of these, the cerebellomedullary cistern (cisterna magna),is between the cerebellum and the medulla. CSF can be obtained by needle puncture.
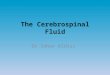
Cisternal punctureThe head must be flexed forwards. The patient is usually sit-ting upright but it is possible to perform the aspiration with the patient lying on one side. The uppermost cervical spine, that of the axis, is palpated with the neck flexed and the aspirating needle is inserted in the midline in the depression just above this point. The needle is directed upwards and forwards, paral-lel to the line joining the external auditory meatus to the nasion
(Figure 2). 4–5 cm below the skin, the needle is felt to pierce the atlanto-occipital ligament and enter the cisterna magna. Though the procedure should not be performed if the relevant CSF samples can be obtained by lumbar puncture, cisternal puncture may be safely performed for the medulla is more than2 cm anterior to the ligament.
Lumbar puncture is described in Anaesthesia and Intensive Care Medicine 5:5: 154.
Cerebrospinal fluid and its circulationJohn Craven
John Craven was formerly Consultant Surgeon at York District Hospital,
York, UK. He trained in Manchester, Uganda and Cardiff. He is past
chairman of the primary examiners of the Royal College of Surgeons of
England.
1
2
Lateral view of ventricles
Arachnoid granulations Subarachnoid space containing CSF
Choroidplexus
4th ventricle
Median aperture
Central canal(of spinal cord)
Cisterna magna
Superior sagittalsinus
Lateral ventricles
3rd ventricle
Cerebral aqueduct
Lateral apertures
Arrows show direction of circulation of CSF
Cisternal puncture
Medulla oblongata
Posterior occipito-atlantoid ligament
Needle
Posterior arch of atlas
Spine of axis Arachnoid and dura
Cisterna magna
Externalauditory meatus
Nasion
Craven.indd 322Craven.indd 322 20/09/2004 10:36:1220/09/2004 10:36:12