Embed Size (px)
Citation preview

Brain Injury, October 2008; 22(11): 882–890
Cerebral response to speech in vegetative and minimally conscious
states after traumatic brain injury
DAVINIA FERNANDEZ-ESPEJO1,2, CARME JUNQUE1,2, PERE VENDRELL1,2,MONTSERRAT BERNABEU3,4, TERESA ROIG3, NURIA BARGALLO2,5,& JOSE MARIA MERCADER2,5
1Department of Psychiatry and Clinical Psychobiology, University of Barcelona, Barcelona, Spain, 2Institute of
Biomedical Research August Pi i Sunyer (IDIBAPS), Barcelona, Spain, 3Department of Neuropsychology,4Head Injury Unit, Institut Universitari de Neurorehabilitacio Guttmann, Badalona, Spain, and 5Neuroradiology
Section, Radiology Department, Centre de Diagnostic per la Imatge (CDI), Hospital Clinic, Barcelona, Spain
(Received 8 May 2008; accepted 12 August 2008)
AbstractPrimary objective: To study cerebral response in a functional magnetic resonance imaging (fMRI) task of speech perceptionin a sample of patients in vegetative state (VS) and minimally conscious state (MCS) after traumatic brain injury.Methods: Three patients in VS, four patients in MCS and 19 healthy volunteers were enrolled for the study. All subjectsunderwent an fMRI task of passive listening of narratives played forward and backward, alternated with periods of silence.This study analysed cerebral response to language and to complex sound processing in the healthy subjects’ group and ineach patient, using SPM5.Results: One patient in VS and one in MCS showed cerebral responses to language and to complex sound very similar tothose shown by the healthy volunteers. Two more patients, one in VS and one in MCS, showed significant responsesto complex sound only. Finally, one patient in VS and one patient in MCS failed to show significant activation in responseto either stimulus.Conclusions: Some patients in VS and MCS can preserve cerebral responses to language and auditory stimuli. fMRI may beuseful to identify these responses, which may pass unnoticed in a bedside examination.
Keywords: Functional magnetic resonance imaging, minimally conscious state, traumatic brain injury, vegetative state
Introduction
The vegetative state (VS) is a clinical conditioncharacterized by wakefulness but no signs ofawareness of the self or the environment [1].Patients in VS demonstrate no evidence of sus-tained, reproducible, purposeful or voluntary beha-vioural responses to visual, auditory, tactile ornoxious stimuli and no evidence of languagecomprehension or expression [2, 3]. A sub-groupof patients with reduced consciousness showsintermittent but discernible behavioural evidence
of awareness. These patients are diagnosed asminimally conscious state (MCS) [4].
Clinical differentiation between VS and MCS isbased on the subtle distinction between reflexive andcognitively mediated behaviours. This distinction isnecessarily inferential because it is not possible toassess the consciousness of another person directly.The limitations of the clinical assessment of aware-ness in patients without voluntary motor function areobvious and have frequently been pointed out [5–7].
Functional neuroimaging can be useful to obtaininformation not dependent on the patient’s ability
Correspondence: Carme Junque, Departament de Psiquiatria i Psicobiologia Clınica, Universitat de Barcelona, IDIBAPS, Casanova 143, 08036 Barcelona,Spain. E-mail: [email protected]
ISSN 0269–9052 print/ISSN 1362–301X online � 2008 Informa UK Ltd.DOI: 10.1080/02699050802403573
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

for overt responses and can help in the assessment ofpatients in VS and MCS. Studies using positronemission tomography (PET) in patients in VS andMCS have reported preserved responses to noxious[8] and auditory [9, 10] stimuli. More recently,several functional magnetic resonance imaging(fMRI) studies have also demonstrated that somepatients in VS or MCS may manifest brain activa-tions in response to auditory sentences or narratives[11–13], to their own name vs. other names [14, 15]and to tasks of mental imagery [12].
Demonstrating the preservation of a consistentlanguage-responsive network in a patient with VS orMCS may have important implications for medicaldecisions and treatment and also for legal and ethicalissues. To the authors’ knowledge, there is only onestudy of language comprehension in a sample ofpatients with VS and MCS [13]. This studyevaluated the fMRI responses for speech andcomplex sound in a sample of TBI patients whowere either in PVS or MCS during the first year afterthe injury.
Methods
Subjects
Seven right-handed patients who had sustainedsevere TBI were recruited from the Institut deNeurorehabilitacio Guttmann (Badalona) and theHospital Clınic (Barcelona). Three patients met thediagnostic criteria for VS [2, 3] and four patients metthe diagnostic criteria defining MCS [4]. Patientswere aged 13–48 years (mean¼ 28.8� 13.6) and the
scanning took place within 12 months after theinjury (range¼ 1–11 months). Previous computedtomography (CT) or magnetic resonance imaging(MRI) brain scanning during inpatient hospital stayrevealed different types of brain damage located in avariety of regions across patients (see Table I).Patients with lesion involving the cerebral areas thatshowed significant activations in the control group inthe contrast between forward and backward narra-tives were excluded. Lesions were evaluated in baseof the high-resolution 3D T1-weighted imagesreformatted in the three planes. Malacic andencephalomalacic changes (signal hypointensity)were evaluated in cortical and sub-cortical areas.To determine the clinical characteristics of thepatients, the scores were recored on several beha-vioural consciousness scales adapted to the VS andMCS populations: Disability Rating Scale (DRS)[16] and Rancho Los Amigos Level of CognitiveFunctioning Scale (LCFS) [17, 18]. In one patient(VS2) ratings were obtained retrospectively bymedical record review. Clinical and demographicaldata of patients are summarized in Table I.Nineteen healthy voluntary subjects, eight men and11 women, were recruited as a reference group. Ageranged from 19–49 years (mean¼ 23.9�6.3).
This study was approved by the Ethics Committeeof the Hospital Clinic (Barcelona). Informed writtenconsent was obtained from the families of all patientsand from all healthy volunteers.
Functional MRI task
An fMRI task similar to the one proposedby Dehaene-Lambertz et al. [19] was selected.
Table I. Clinical and demographic characteristics of the patients.
Patient Age/gender Aetiology Lesions on MRI/CTTime since
injury (days) GCS MCS DRS LCFS
MCS1 36/M RTA Right temporal and frontal cortexTAI
198 5/5 1 21 5
MCS2 34/M Hit Diffuse cortical atrophyRight temporal cortexBilateral orbital and pre-frontal cortexTAI
354 3/3 2 18 6
MCS3 18/F RTA Bilateral frontal 235 3/3 4 21 3MCS4 18/M RTA Right temporal cortex and thalamus
Bilateral frontalTAI
82 5/3 1.5 20 5
VS1 44/F Fall Left occipital cortexBilateral prefrontal and parietal cortexTAI
129 4/3 – 25 2
VS2 48/M Fall Right temporal and parietal cortex 33 5/� – 24 2VS3 13/M RTA Bilateral frontal cortex
ThalamusTAI
227 6/3 – 25 2
MCS¼minimally conscious state; VS¼ vegetative state; M¼male; F¼ female; RTA¼ road traffic accident; GCS¼Glasgow Coma Scale(on admission/minimal); MCS¼ time in recovering from the VS to the MCS (months); DRS¼Disability Rating Scale; LCFS¼RanchoLos Amigos Level of cognitive Functioning Scale; TAI¼ traumatic axonal injury.
Cerebral response to speech in vegetative and minimally conscious states after traumatic brain injury 883
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

While in the fMRI scanner, subjects were presenteda passive language auditory processing task compris-ing eight spoken narratives (20 seconds) presentedplayed forward, backward and alternated withperiods of silence with the same length in a three-condition block-design with a total length of 480seconds (see Figure 1). Narratives included everydayevents with neutral emotional content and withoutpersonally meaningful content. They were read by afemale Spanish speaker with vivid intonation andrecorded using the freeware software Audacity 1.3.4(http://audacity.sourceforge.net). Reversed narra-tives (narratives played backward) matched theoriginals in terms of physical complexity andacoustic characteristics such as amplitude andpower of spectrum [11, 20], but violated severalsegmental and suprasegmental phonological proper-ties of human speech [19, 20]. These characteristicsmake reversed speech an ideal control condition forthe non-linguistic aspects of speech. Figure 1 showsa schematic illustration of the fMRI paradigm used.
MRI acquisition
Images were acquired on a 3T MRI scanner(Magnetom Trio Tim, Siemens Medical Systems,Germany) at the Centre for Image Diagnosis of theHospital Clınic (CDIC). The MRI protocol includedan fMRI dataset of 240 volumes of 36 axial sliceseach (using a gradient-echo echo-planar imaging[EPI] sequence) and a high-resolution 3D structuraldataset (T1-weighted MP-RAGE [MagnetizationPrepared Rapid Gradient Echo] image) for coregis-tering with the fMRI images. The acquisitionparameters for the fMRI were: TR (repetitiontime)¼ 2000 ms; TE (echo time)¼29 ms; percen-tage phase field of view¼ 100; matrix size¼128�128; slice thickness¼3 mm; interslice gap¼3.75 mm; flip angle¼ 90�. The parameters forthe structural images were: TR¼ 2300 ms,TE¼ 2.98 ms, TI (Inversion Time)¼ 900;
FOV¼ 100�100 cm; matrix size¼ 256� 256; Flipangle¼ 9�; Slice thickness¼1.
The stimuli were presented using the Presentationsoftware (Presentation� v.10.1 NeurobehaviouralSystem) running on a Windows XP PC and aMRI-compatible high-quality digital sound systemincorporating noise-attenuated headphones(VisuaStim Digital. Resonance Technology, Inc.).
fMRI data analysis
The fMRI data was pre-processed and analysedusing SPM5 (Statistical Parametric Mapping,Wellcome Department of Cognitive Neurology,University College London, London, UK, http://www.fil.ion.ucl.ac.uk.spm) running in Matlab 6.5(MathWorks, Natick, MA). Spatial pre-processingincluded the following steps: realignment to correctsubjects’ motion, co-registration between the struc-tural and functional data sets, spatial normalizingand smoothing with an 8 mm Gaussian kernel. Theanalysis was based on the general linear model.Three regressors (one corresponding to each condi-tion) were modelled per subject. Each scan wascoded to belong to one of these conditions.Additional columns included motion parameterscalculated from the realignment step. After modelestimation, t-contrasts were performed for eachsubject. Linguistic processing was assessed by thecontrast between forward and backward narrativeconditions. Auditory processing in response tocomplex sound was assessed by the contrast betweenthe two types of narratives (played forward andbackward) and silence baseline condition (back-ground scanner noise). Special attention was paid tomotion-related artefacts. In each fMRI data-set,scans with levels of motion upper 1.5 mm and0.035 radians were eliminated from the analysis byintroducing them into the subject matrix as specificregressors. The data-sets of one patient were rejectedbecause of high levels of motion in most of the scans.Motion-related artefacts also precluded the statisti-cal analysis of two healthy control data-sets.
The contrast images calculated from each subjectin the control group were then used for a within-group analysis (one-sample t-test) in order to obtainnormal patterns of linguistic processing and auditoryresponses, respectively. The statistical threshold forthese contrasts was set at p< 0.01 corrected usingthe false discovery rate (FDR) procedure.
For the patients, functional activation wasassessed selecting specific regions of interest(ROIs) comprising the areas that showed significantactivation in the same contrast in the referencegroup. For the contrasts calculated from eachpatient, as there was a strong anatomical a priori
hypothesis based on the normal pattern obtained for
Figure 1. The figure illustrates the design of the fMRI task.A block-design was applied, alternating forward narratives,backward narratives and silence.
884 D. Fernandez-Espejo et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

the reference group, the statistical threshold was setat an uncorrected p< 0.005 [21]. ROIs mask werecreated using the MarsBaR toolbox for SPM [22]and applied into the analysis using the WFUPickatlas SPM toolbox (Wake Forest UniversitySchool of Medicine, Winston-Salem, NC) [23]. Theanatomical location of the activated cerebral areaswas determined by the MNI (Montreal NeurologicalInstitute) coordinates and was described followingvisual inspection of the Talairach and Tournauxatlas.
Results
The pattern of cerebral activation obtained from thecontrol group in the contrast between narrativesplayed forward and backward included a highlyrobust and well-circumscribed cluster in the leftsuperior temporal gyrus (STG) and left middletemporal gyrus (MTG). Other significant areas ofactivation were: left inferior frontal gyrus (IFG) andright MTG. In the contrast between the two types ofnarratives and silence baseline this group showedlarge significant bilateral activations in the STG (seeFigure 2 and Table II).
Among the patients, one patient in VS (VS1) andone patient in MCS (MCS3) failed to show anysignificant cerebral activation to forward vs. back-ward narratives or narratives vs. silence baselinewithin the ROIs analysed. Another group of patients,one in VS (VS3) and one in MCS (MCS4), alsofailed to show significant activation in the contrastbetween forward and backward narratives but didshow functional activation in the contrast betweennarratives and baseline similar to that recorded in thecontrol group. Finally, one patient in MCS (MCS1)and, interestingly, one patient in VS (VS2) showedsignificant functional activation in response tolanguage (forward vs. backward narratives) and inresponse to complex sound (narratives vs. silencebaseline) (see Table III and Figure 2). This patientin VS emerged from this state and recoveredconsciousness when assessed at 9 months follow-up.
Discussion
Evidence was found of cerebral changes related toauditory stimuli in four out of six patients. Forwardnarratives elicited significant activation in the lefttemporal lobe in two patients, one in MCS and onein VS. Complex sound, assessed by the sum betweenforward and backward narratives vs. silence baseline,elicited significant activation in temporal lobes infour patients, two in MCS and two in VS. Finally,two patients, one in MCS and one in VS, failed to
show significant activation in response to language orcomplex sound.
The results agree with the findings of Colemanet al. [13] in that a clear relationship was not foundbetween the patients’ fMRI responses and theirdiagnosis of VS or MCS. Similar numbers ofsubjects with both types of diagnosis presentedevidence of simple auditory processing, complexauditory processing or absence of cerebral response.These results indicate that fMRI is a procedure thatprovides useful information to complement theclinical assessment.
Cortical responses to language and complex soundwere seen in two patients in VS. VS2 and VS3fulfilled the diagnostic criteria for VS [2, 3], showingno behavioural evidence of response to auditorystimuli or language comprehension. However, theanalysis of their fMRI data showed robust and well-circumscribed clusters of significant activation in theauditory contrast for VS3 and in both contrastsanalysed for VS2. The fMRI results suggest thatthese patients may preserve functioning of someauditory or language-responsive networks, respec-tively. However, more interestingly, when assessed9 months later, VS2 had recovered consciousnessand was able to communicate. VS2 was scanned ataround 1 month after the injury, just reaching thecriteria for the persistent vegetative state [2].Compared with the other two patients in VS, VS2has different brain lesions that could explain partiallythe results in the fMRI task. VS2 had an extensivebut focalized injury in the right temporoparietalcortex and didn’t suffer from diffuse axonal injury.In any case, his recovery could suggest that fMRIresponses in a task of language processing may havesome prognostic value, especially in the acutephases, when more variability in the outcome couldbe expected.
The results for the activation of secondaryauditory areas in patients in VS seem to contradictthose of previous PET studies. For instance, Bolyet al. [10] reported that cerebral response to auditoryclick stimuli was able to differentiate patients in VSand MCS. In their study patients in MCS activatedprimary and secondary auditory areas (Brodmann’sareas 41, 42 and 22) while patients with vegetativestate did not activate Brodmann’s area 22.Differences in the fMRI paradigm employed or inthe characteristics of the sample (their studyincluded patients with diverse aetiologies) may bein the origin of this discrepancy. Regarding the MCSpatients, these results also disagree with Boly et al.’s[10] results. One of the three patients in MCSanalysed in this study failed to activate neitherprimary nor secondary auditory areas. This patienthad longer time after injury than the other twopatients in MCS showing some response and, more
Cerebral response to speech in vegetative and minimally conscious states after traumatic brain injury 885
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

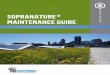
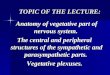
Figure 2. (a) Results from the contrast between narratives and silence in healthy control group (on the top), the healthy subject with theslightest activation (second row) and the patients that showed significant activation within the ROIs analysed (VS2, VS3, MCS1, MCS4).Results are displayed at a FDR-corrected p< 0.01 for the group analysis and a p<0.005 uncorrected for the individual analysis. (b) Resultsfrom the contrast between narratives played forward and backward in healthy control group (on the top), the healthy subject with theslightest activation (second row) and the patients that showed significant activation within de ROIs analysed. Results are displayed at aFDR-corrected p< 0.01 for the group analysis and a p<0.005 uncorrected for the individual analysis.
886 D. Fernandez-Espejo et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

interestingly, she was the patient who remained inVS longer before recovering to an MCS (4 months).In the same way, the VS patient who failed to showcortical activation in this task (VS1) had also morethan 4 months of evolution, whereas VS2, asexplained above, had only 1 month of evolution.
A recent longitudinal study in patients in very-longterm persistent vegetative state has demonstrated adecrease in brain activation in several fMRI para-digms in the follow-up assessment regarding thebaseline [24]. These results suggest that the time ofevolution could also have an important role, even in
Table II. Patterns of activation obtained from the control group.
Coordinate
Contrast Brain structure BA K Side x y z z-value
1 Superior and middle temporal gyrus 21, 22 452 L �60 �15 �6 5.59Inferior frontal gyrus 47 72 L �39 33 �12 4.86Middle temporal gyrus 21 37 R 60 3 �15 4.73
2 Superior temporal gyrus 42, 22 821 R 68 �20 9 6.71Superior temporal gyrus 22, 41 907 L �60 �12 0 5.89
The last four columns (coordinates and z-value) refer to the main peak of activation into the cluster; Coordinates refers to MontrealNeurological Institute. Results thresholded at p< 0.01 FDR-corrected; BA¼Brodmann areas; K¼ cluster size; L¼ left hemisphere;R¼ right hemisphere. Contrast 1¼ contrast between forward and backward narratives; contrast 2¼ contrast between narratives and silencebaseline.
Figure 2. Continued.
Cerebral response to speech in vegetative and minimally conscious states after traumatic brain injury 887
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

the first year after injury. The results from VS3 seemto contradict this trend. However, this is the young-est patient in the sample. The Multi-Society Taskforce on Persistent Vegetative State (MSTF) foundthat the prognosis for recovery of consciousness aftera traumatic injury was slightly better in children thanin adults [25]. Conversely, a recent work in childrenand young adults in VS or MCS did not find acontribution of age to the level of consciousness atdischarge after an intensive neurorehabilitationprogramme [26]. This study did not explore theeffect of age, but it is suggested that this variablecould also have some effect in the outcome and inthe cortical responsiveness after a severe injury.
Cortical activation does not necessarily implylanguage comprehension. From the fMRI studyone cannot infer successful comprehension or con-sciousness. For example, using the same paradigm,Dehaene-Lambertz et al. [20] observed corticalactivation in 3-month-old infants both awake andasleep. In that study, both awake and sleepingsubjects activated left-lateralized brain regions inthe contrast between forward and backward narra-tives. Moreover, deeply sedated normal subjects alsoactivated temporal lobe regions in response tosentences [27]. So a parsimonious conclusion inVS subjects is that the cortical network involved inlanguage processing is spared in some subjects and
Table III. Functional activation for the fMRI task in each patient.
Coordinate
Patient Contrast Brain structure BA K Side x y z z-value
MCS1 1 Middle temporal gyrus 21 6 L �57 6 �15 3.27Middle temporal gyrus 21 5 L �54 �27 �9 3.08
2 Superior temporal gyrus 21, 41, 42 492 L �63 �6 �3 InfMiddle temporal gyrusPost-central gyrusTransverse temporal gyrus
40, 42, 21 124 R 54 �24 18 4.97
MCS3 1 – – – – – – – –2 – – – – – – – –
MCS4 1 – – – – – – – –2 Middle temporal gyrus 21 34 L �54 �30 6 3.84
Superior temporal gyrus 21 6 R 45 �39 15 3.67Superior temporal gyrus 42 11 R 66 �33 15 3.58Superior temporal gyrus 41 9 R 45 �33 0 3.33Middle temporal gyrusSuperior temporal gyrus
21 21 R 63 0 �9 3.8
Insula 13 3 L �39 �42 15 2.87Superior temporal gyrus 22 7 R 54 �15 �6 2.77Inferior parietal lobule 40 2 L �60 �33 21 2.73
VS1 1 – – – – – – – –2 – – – – – – – –
VS2 1 Superior temporal gyrusMiddle temporal gyrus
22, 21 32 L �57 �51 9 3.58
Middle temporal gyrus 21 5 L �60 �6 �6 3.14Superior temporal gyrus 22 2 L �51 �18 �3 2.79Middle temporal gyrus 21 2 L �57 9 �15 2.70
2 Transverse temporal gyrusSuperior temporal gyrus
41, 42, 22 121 L �57 �18 9 4.81
Parietal postcentral gyrusSuperior temporal gyrus
43, 22 26 R 54 �18 15 4.45
Middle temporal gyrus 21 3 R 69 �36 �3 2.79Middle temporal gyrus 21 3 L �60 �27 �9 2.65
VS3 1 – – – – – – – –2 Superior temporal gyrus
Transverse temporal gyrus22, 42 395 R 57 �9 6 7.56
Middle temporal gyrus 21 3 R 69 �18 �9 3.68Middle temporal gyrusSuperior temporal gyrus
21, 42 121 L �66 �18 �9 3.62
Middle temporal gyrus 22 2 R 69 �42 3 3.10Middle temporal gyrus 21 5 L �66 �36 �3 2.93
The last four columns (coordinates and z-value) refer to the main peak of activation into the cluster; Coordinates refers to MontrealNeurological Institute. Results thresholded at p< 0.005 uncorrected; BA¼Brodmann areas; K¼ cluster size; L¼ left hemisphere; R¼ righthemisphere. Contrast 1¼ contrast between natural and reversed speech; contrast 2¼ contrast between sound and baseline.
888 D. Fernandez-Espejo et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

impaired in others. The identification of preservedcortical networks could also have implications indecisions about the inclusion of patients in neuror-ehabilitation programmes addressed to stimulatecognitive functions such as language.
Longitudinal studies using fMRI are needed toinvestigate the evolution of patients with somedegree of cortical activation concomitant to stimula-tion. Functional magnetic resonance imaging, inspite of its high sensitivity to motion artefacts,performs better than PET scan studies, because ofits lower degree of invasiveness [28]. In a 2-yearfollow-up study of four cases in persistent vegetativestate, Rousseau et al. [24] found only one case ofcerebral activation for passive motor stimulation andauditory and visual primary stimuli in the baselineassessment; the patient did not recover conscious-ness and moreover significant deterioration of herfunctional excitability of primary cortices wasobserved during the follow-up, possibly due to thelength of the period since the brain injury (3 years).In addition the stimuli used in that study onlyactivated the primary cortical areas and to achieveconsciousness complex cortical circuitry must berestored [9, 29]. In normal subjects, Boly et al. [30]tested four paradigms that can be used to testvolitional brain activity in non-communicative braininjured patients and found motor imagery andspatial navigation to be the most robust mentalimagery tasks.
The pattern of cerebral activation related tospeech perception in these patients coincided withthat seen in normal controls regarding the lefttemporal lobe, but none of the patients activatedthe frontal lobe. This may be due to the large-scaleimpairment of the cortico-cortical connectivity or tothe decreased frontal metabolism [31]. Frontal lobefunctions are more dependent on white matterintegrity than other neocortical regions and thelongitudinal superior and inferior fascicles areimpaired in severe TBI [32]. The lack of activationof the frontal lobe in the patients cannot be due tothe presence of frontal lesions. Only one patient(MCS4) had a lesion in the left inferior frontal gyrus.This lesion affected a region localized more dorsallythan the area showing significant activations in thecontrol group, but one can not discard that it couldbe affecting the linguistic network. However thispatient also failed to show temporal activations tospeech, that unlikely may be due to this frontallesion.
Although this sample was homogeneous in termsof aetiology, it is small and heterogeneous regardingevolution time since injury. To determine thepredictive power of fMRI for the restoration ofcognitive functions, multi-centre studies are neededto allow the isolation of the critical variables involved
in recovery after TBI. The functional connectivityapproach in fMRI studies combined with DTI datacould provide valuable data for solving the enigmasof the individual differences in the patterns ofactivation and functional recovery.
Conclusion
These results provide further evidence that func-tional neuroimaging may have an important role inthe identification of residual cognitive function inpatients with disorders of consciousness which maybe neglected in a bedside examination.
Acknowledgements
This study was supported by grant SAF2007-66077and fellowship AP2006-00862, from the SpanishMinistry of Education and Science. Part of thisresearch work was presented at the Seventh WorldCongress on Brain Injury (Lisbon, 2008).
Declaration of interest: The authors report noconflicts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
1. Jennett B, Plum F. Persistent vegetative state after braindamage. A syndrome in search of a name. Lancet 1972;1:734–737.
2. The Multi-Society Task Force on PVS. Medical aspects of thepersistent vegetative state (1). New England Journal ofMedicine 1994;330:1499–1508.
3. Royal College of Physicians. The permanent vegetative state[Report of a working party]. Journal of the Royal College ofPhysicians of London 1996;30:119–121.
4. Giacino JT, Ashwal S, Childs N, Cranford R, Jennett B,Katz DI, Kelly JP, Rosenberg JH, Whyte J, Zafonte RD, et al.The minimally conscious state: Definition and diagnosticcriteria. Neurology 2002;58:349–353.
5. Bernat JL, Rottenberg DA. Conscious awareness in PVS andMCS: The borderlands of neurology. Neurology 2007;68:885–886.
6. Andrews K, Murphy L, Munday R, Littlewood C.Misdiagnosis of the vegetative state: Retrospective study in arehabilitation unit. BMJ (Clinical Research Ed.) 1996;313:13–16.
7. Shiel A, Gelling L, Wilson B, Coleman M, Pickard JD.Difficulties in diagnosing the vegetative state. British Journal ofNeurosurgery 2004;18:5–7.
8. Laureys S, Faymonville ME, Peigneux P, Damas P,Lambermont B, Del Fiore G, Degueldre C, Aerts J,Luxen A, Franck G, et al. Cortical processing of noxioussomatosensory stimuli in the persistent vegetative state.NeuroImage 2002;17:732–741.
9. Laureys S, Faymonville ME, Degueldre C, Fiore GD,Damas P, Lambermont B, Janssens N, Aerts J, Franck G,Luxen A, et al. Auditory processing in the vegetative state.Brain 2000;123:1589–1601.
Cerebral response to speech in vegetative and minimally conscious states after traumatic brain injury 889
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.

10. Boly M, Faymonville ME, Peigneux P, Lambermont B,Damas P, Del Fiore G, Degueldre C, Franck G, Luxen A,Lamy M, et al. Auditory processing in severely brain injuredpatients: Differences between the minimally conscious stateand the persistent vegetative state. Archives of Neurology2004;61:233–238.
11. Schiff ND, Rodriguez-Moreno D, Kamal A, Kim KH,Giacino JT, Plum F, Hirsch J. fMRI reveals large-scalenetwork activation in minimally conscious patients.Neurology 2005;64:514–523.
12. Owen AM, Coleman MR, Boly M, Davis MH, Laureys S,Pickard JD. Detecting awareness in the vegetative state.Science 2006;313:1402.
13. Coleman MR, Rodd JM, Davis MH, Johnsrude IS,Menon DK, Pickard JD, Owen AM. Do vegetative patientsretain aspects of language comprehension? Evidence fromfMRI. Brain 2007;130:2494–2507.
14. Staffen W, Kronbichler M, Aichhorn M, Mair A,Ladurner G. Selective brain activity in response to one’sown name in the persistent vegetative state. Journal ofNeurology, Neurosurgery and Psychiatry 2006;77:1383–1384.
15. Di HB, Yu SM, Weng XC, Laureys S, Yu D, Li JQ, Qin PM,Zhu YH, Zhang SZ, Chen YZ. Cerebral response to patient’sown name in the vegetative and minimally conscious state.Neurology 2007;68:895–899.
16. Rappaport M, Hall KM, Hopkins K, Belleza T, Cope DN.Disability rating scale for severe head trauma: Coma tocommunity. Archives of Physical Medicine andRehabilitation 1982;63:118–123.
17. Hagen C, Malkmus D, Durham P. Levels of cognitivefunctioning. In: Rehabilitation of the head injured adultcomprehensive physical management. Downey, CA:Professional Staff Association of Rancho of Los AmigosHospital; 1979. pp 87–89.
18. Hagen C. Language disorders in head trauma. In: Holland A,editor. Language disorders in adults: Recent advances. SanDiego, CA: College-Hill Press; 1984. pp 247–281.
19. Dehaene-Lambertz G, Dehaene S, Hertz-Pannier L.Functional neuroimaging of speech perception in infants.Science 2002;298:2013–2015.
20. Binder JR, Frost JA, Hammeke TA, Bellgowan PS,Springer JA, Kaufman JN, Possing ET. Human temporallobe activation by speech and nonspeech sounds. CerebralCortex 2000;10:512–528.
21. Friston KJ, Holmes A, Poline JB, Price CJ, Frith CD.Detecting activations in PET and fMRI: Levels of inferenceand power. NeuroImage 1996;4:223–235.
22. Brett M, Anton JL, Valabregue R, Poline JB. Region ofinterest analysis using an SPM toolbox [abstract]. Presentedat the 8th International Conference on Functional Mappingof the Human Brain; 2–6 June 2002; Sendai, Japan (Availableon CD-ROM in NeuroImage, Vol 16, No 2, Abstract497;2002).
23. Maldjian JA, Laurienti PJ, Kraft RA, Burdette JH. Anautomated method for neuroanatomic and cytoarchitectonicatlas-based interrogation of fMRI data sets. NeuroImage2003;19:1233–1239.
24. Rousseau MC, Confort-Gouny S, Catala A, Graperon J,Blaya J, Soulier E, Viout P, Galanaud D, Le Fur Y,Cozzone PJ, et al. A MRS-MRI-fMRI exploration of thebrain. Impact of long-lasting persistent vegetative state. BrainInjury 2008;22:123–134.
25. The Multi-Society Task Force on PVS. Medical aspects ofthe persistent vegetative state (2). New England Journal ofMedicine 1994;330:1572–1579.
26. Eilander HJ, Wijnen VS, Scheirs JG, de Kort PL, Prevo AJ.Children and young adults in a prolonged unconscious statedue to severe brain injury: Outcome after an early intensiveneurorehabilitation programme. Brain Injury 2005;19:425–436.
27. Davis MH, Coleman MR, Absalom AR, Rodd JM,Johnsrude IS, Matta BF, Owen AM, Menon DK.Dissociating speech perception and comprehension atreduced levels of awareness. Proceedings of the NationalAcademy of Sciences (USA) 2007;9:16032–16037.
28. Laureys S, Owen AM, Schiff ND. Brain function in coma,vegetative state, and related disorders. Lancet Neurology2004;3:537–546.
29. Laureys S, Boly M, Maquet P. Tracking the recovery ofconsciousness from coma. The Journal of ClinicalInvestigation 2006;116:1823–1825.
30. Boly M, Coleman MR, Davis MH, Hampshire A, Bor D,Moonen G, Maquet PA, Pickard JD, Laureys S, Owen AM.When thoughts become action: An fMRI paradigm to studyvolitional brain activity in non-communicative brain injuredpatients. NeuroImage 2007;36:979–992.
31. Nakayama N, Okumura A, Shinoda J, Nakashima T,Iwama T. Relationship between regional cerebral metabolismand consciousness disturbance in traumatic diffuse braininjury without large focal lesions: An FDG-PET study withstatistical parametric mapping analysis. Journal of Neurology,Neurosurgery and Psychiatry 2006;77:856–862.
32. Kraus MF, Susmaras T, Caughlin BP, Walker CJ,Sweeney JA, Little DM. White matter integrity and cognitionin chronic traumatic brain injury: A diffusion tensor imagingstudy. Brain 2007;130:2508–2519.
890 D. Fernandez-Espejo et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Wes
tern
Ont
ario
on
03/2
9/11
For
pers
onal
use
onl
y.