Embed Size (px)
Citation preview

266
Anesth Pain Med 2011 6 266~269 Case Report
Cerebral hemorrhage presenting as alteration of consciousness during the anesthesia recovery period -A case report-
Department of Anesthesiology and Pain Medicine Ansan Hospital of Korea University Ansan Korea
Doo Jae Min Woon Young Kim Sehwa Lee Yoon Sook Lee Jae Hwan Kim and Young Cheol Park
Received August 25 2010
Revised October 3 2010
Accepted February 11 2011
Corresponding author Woon Young Kim MD Department of
Anesthesiology and Pain Medicine Ansan Hospital of Korea University
516 Gojan-dong Ansan 425-707 Korea Tel 82-31-412-5291 Fax
82-31-412-5294 E-mail ckssiskoreaackr
Catastrophic neurological events can occur rarely in anesthetic
recovery period and they must be quickly diagnosed We report
here on a spontaneous intracerebral hemorrhage (SICH) that
developed during the anesthesia recovery period in a 52-year-old
man who had undergone uneventful orthopedic surgery He had
predisposing factors including 25 year history of heavy alcohol
consumption and smoking The risk of spontaneous intracerebral
hemorrhage following non-cardiovascular and non-neurovascular
surgery is exceedingly small during the anesthesia recovery period
especially for a patient with no history of hypertension and
coagulopathy We also describe the differential diagnosis of an
altered mental status that occurs during anesthetic recovery period
(Anesth Pain Med 2011 6 266sim269)
Key Words Anesthesia recovery period Cerebral hemorrhage
Consciousness Disorder Spontaneous rupture
Adverse events commonly occur in the postanesthesia care
unit and the complication rate may exceed 23 to 30 [12]
Pain (16) and nausea-vomiting (8) are the most common
complications and an altered mental status is seen in 3 to
9 of cases [23] Delayed emergence and emergence delirium
secondary to the anesthetic and analgesic medication that are
administered preoperatively are the principal causes of
postoperative changes of mental status but the differential
diagnosis is rather broad We report here on a case of altered
consciousness in a patient who was in the postanesthetic
recovery unit after undergoing orthopedic surgery The patient
was subsequently diagnosed with cerebral hemorrhage
CASE REPORT
A 52-year-old man weighing 55 kg and with an American
Society of Anesthesiologists (ASA) physical status of grade II
presented to the orthopedic surgery department for open reduc-
tion and internal fixation of his fractures in both forearms He
had no history of hypertension amyloid angiopathy cerebro-
vascular accident diabetes mellitus or a bleeding tendency But
he had a 25 year history of alcohol abuse (3 to 4 times
weekly) and smoking (1 pack daily) The results of the
preoperative liver function tests were mildly elevated The
alanine aminotransferase level was 67 (normal range 0minus45)
Otherwise the other preoperative lab values (complete blood
count urinary analysis electrolytes coagulation profile test
and electrocardiography [ECG]) were in the normal range
Monitors (ECG Blood Pressure [BP] cuff and Pulse Oximetry
[SpO2]) were applied for general anesthesia The BP was
checked in the leg because the patient had both distal radius
fractures of forearms and left ulnar fracture The preoperative
vital signs in the operating room were as follows heart rate
85 beats per minute BP 14673 mmHg and SpO2 98 After
the administration of propofol (120 mg) and rocuronium (40
mg) anesthesia was induced with additional desflurane (up to
5 vol) by a mask in a mixture of oxygen and nitrous oxide
(FiO2 05) Tracheal intubation was performed 2 minutes after
anesthesia was induced Anesthesia was maintained with
desflurane (vol 35minus65) O2 2 Lmin and N2O 2 Lmin
Normally the systolic BP (SBP) in the legs is usually 10 to
20 higher than in the brachial artery pressure [4] The BP
was maintained under 16080 in the leg during the operation
At the end of the operation the patient was fully awakened
and extubated The patient was then transferred to the PACU
Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 267985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
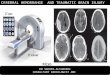
Fig 1 CT scan of the head without contrast material and this was obtained during the recovery time It demonstrated the approximately 75 cm large acute ICH in the left frontotemporal lobe The ICH extended to both lateral ventricles and the 3rd and 4th ventricles through the external capsule
Fig 2 CT scans of the head obtained the next day postoperatively The density and size of the lobar ICH were reduced but localized swelling wasseen in the left frontotemporal lobe with residual IVH in both lateral ventricles
(Postanesthesia Care Unit) At the arrival to the PACU the
postoperative vital signs were as follows heart rate 85 beats
per minute BP 15080 mmHg and SpO2 98 He responded
appropriately to verbal stimuli Throughout the PACU stay the
blood pressure heart rates and oxygen saturation were moni-
tored at 5-minute intervals Two liters oxygen supplementation
was given during the PACU stay by a nasal prong Fifty μg
of fentanyl was intravenously injected for postoperative pain
control and a warm blanket was applied It was noted that the
patient complained of mild headache with an elevated BP
18095 at 50 minutes after the PACU admission Thus 10 mg
of labetalol hydrochloride was intravenously injected and then
the blood pressure fell to the normal range At 2 hours after
the PACU admission the patient showed a slow verbal
response and an altered consciousness Physical and neurologic
exams were immediately performed The patient did not exhibit
spontaneous eye opening but he opened his eyes in response
to a voice He showed a confused mentality minimal
withdrawal to painful stimuli and a positive Babinski sign on
both feet The Glasgow coma scale (GCS) score was 11 The
electrocardiographic findings serum electrolytes and glucose
level were normal Emergency computerized tomography (CT)
scanning without contrast was performed (Fig 1) On the
emergency CT a large acute intracranial hemorrhage (ICH)
was shown in the left basal ganglia both lateral ventricles and
the 3rd and 4th ventricles Emergency decompressive craniec-
tomy and hematoma removal were performed After surgery he
was sent to the intensive care unit (ICU) and the follow-up
CT (Fig 2) was taken two days later He stayed in the ICU
for 24 days and gradually regained consciousness and he was
268 Anesth Pain Med Vol 6 No 3 2011985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
then transferred to a rehabilitation facility
DISCUSSION
The differential diagnosis of altered mental status
during anesthetic recovery period
Delayed emergence from general anesthesia due to the
residual effects of oral intravenous and inhalational sedative
analgesic and anesthetic medications is a most common cause
of an altered mental status for patients in the PACU This
situation may be complicated by preexisting mental dysfunc-
tion postoperative hypothermia or unrecognized preoperative
ingestion of alcohol opioids benzodiazepines and other presc-
ription and illicit drugs that potentiate the effects of anesthe-
sia-related medications
Emergence delirium is a behavioral manifestation of recovery
from general anesthesia and this ranges from mild confusion
and lethargy to extreme excitement and combativeness
Emergence delirium is the second most common cause of an
altered mental status in patients in the PACU Return of the
cognitive function after general anesthesia may be slower in
the elderly population in the immediate postoperative period
whereas agitation and combativeness are more frequently
observed in children and young adults [5] Emergence delirium
may also be produced by the perioperative administration of
ketamine or atropine and by postoperative withdrawal from
alcohol or illicit drugs Moreover it may be amplified by
anxiety and by discomfort such as surgical pain nausea
pruritis and gastric or urinary bladder distention
An abnormal mental status after surgery may be an
indication of hypoxemia andor hypercarbia due to the residual
effects of anesthetic agents incomplete reversal of neuromu-
scular blockade airway obstruction pneumothorax or pulmo-
nary aspiration [67] Rarely metabolic derangements such as
hypoglycemia hyperglycemia hypothermia hypercalcemia or
hypermagnesemia may contribute to an abnormal mental status
in patients in the PACU Finally once the reversible causes of
acutely altered sensorium are excluded neurologic events such
as seizure activity and embolic or hemorrhage stroke must be
considered
Therapeutic and diagnostic approach to altered
mental status
A spontaneous intracerebral hemorrhage (SICH) is defined as
a blood clot that arises in the brain parenchyma in the
absence of trauma SICH accounts for 10 to 15 of all
strokes and it is associated with a higher mortality rate than
either ischemic stroke or subarachnoid hemorrhage Arterial
hypertension represents the most common cause of nontrau-
matic ICH in patients between 40 and 70 years of age and
accounts for over 50 of cases [89] Thus it constitutes by
far the most important modifiable risk factor for spontaneous
ICH [1011] Further independent risk factors include moderate
and heavy alcohol abuse old age diabetes mellitus coagulo-
pathy and anticoagulant treatment [12] Excessive use of
alcohol increases the risk of ICH by impairing coagulation and
directly affecting the integrity of cerebral vessels [13]
Cigarette smoking seems to increase the risk for subarachnoid
hemorrhage (SAH) but is less strongly associated with SICH
[11] Diabetes mellitus is more commonly associated with
SICH than with SAH [14]
The classic presentation of SICH is a sudden onset of focal
neurological deficit that progresses over hours with accom-
panying headache nausea vomiting an altered consciousness
and an elevated BP However because inhalational anesthetics
may produce a number of various changes in the mental status
after surgery such as headache emergence excitement and
delirium during the recovery period it is hard to distinguish
between the early signs of SICH and the residual effect of
inhalational anesthetics [15] Emergency Computerized tomo-
graphy (CT) scanning is the initial diagnostic procedure of
choice for acute stroke MRI and cerebral angiography are
being increasingly used in the diagnosis of SICH Yet they are
expensive diagnostic tools to routinely use whenever a patient
complains of headache So conducting neurologic and physical
exams are generally preferred as the first step before
performing CT or magnetic resonance imaging (MRI)
Although delayed emergence from general anesthesia and
emergence delirium are the most common causes of the mental
status changes found in the PACU setting the immediate
evaluation must also include considering the potentially
catastrophic conditions such as hypoxemia incomplete reversal
of neuromuscular blockade and embolic or hemorrhage stroke
SICH is rare during the PACU stay but it must always be
considered in the differential diagnosis of mental status
changes CT scanning is the initial diagnostic procedure of
choice However we recommend to conduct neurologic and
physical exams as the first step before performing CT or
magnetic resonance imaging (MRI)
Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 269985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
REFERENCES
1 Hines R Brash PG Waltrous G OConnor T Complications
occuring in the postanesthesia care unit a survey Anesth Analg
1992 74 503-9
2 Zeler J Wells DG Anesthetic-related recovery room compli-
cations Anaesth Intensive Care 1987 15 168-74
3 Van der Walt JH Webb RK Osborne GA Morgan C Mackay
P The Australian Incident Monitoring Study Recovery room
incidents in the first 2000 incident reports Anaesth Intensive Care
1993 21 650-2
4 Bickley LS Szilagyi PG Bates B Bates guide to physical
examination and history taking 10th ed Philadelphia Wolters
KluwerLippincott Williams amp Wilkins 2009
5 Mecca RS Postoperative recovery In Clinical Anesthesia 3rd ed
Edited by Barash PG Gullen BF Stoeling RK Philadelphia Pa
Lippincott-Raven 1997 pp 1279-303
6 Mathew JP Rosenbaum SH OConnor T Barash PG Emergency
tracheal intubation in the postanesthesia care unit physicain error
or patient disease Anesth Analg 1990 71 691-7
7 Daley MD Norman PH Colmenares ME Sandler AN Hypoxa-
emia in adults in the post-anesthesia care unit Can J Anaesth
1991 38 740-6
8 Gomori JM Grossman RI Hackney DB Goldberg HI Zimmer-
man RA Bilaniuk LT Variable appearances of subacute intra-
cranial hematomas on high-field spin-echo MR AJR Am J Roent-
genol 1988 150 171-8
9 Viswanathan A Chabriat H Cerebral microhemorrhage Stroke
2006 37 550-5
10 Fewel ME Thompson BG Jr Hoff JT Spontaneous intracerebral
hemorrhagea review Neurosurg Focus 2003 15 1-16
11 Thrift AG McNeil JJ Forbes A Donnan GA Risk factors for
cerebral hemorrhage in the era of well-controlled hypertension
Melbourne Risk Factor Study (MERFS) Group Stroke 1996 27
2020-5
12 Ariesen MJ Claus SP Rinkel GJ Algra A Risk factors for
intracerebral 6 hemorrhage in the general population a systematic
review Stroke 2003 34 2060-5
13 Cowan DH Effect of alcoholism on hemostasis Semin Hematol
1980 17 137-47
14 Juvela S Prevalence of risk factors in spontaneous intracerebral
hemorrhage and aneurysmal subarachnoid hemorrhage Arch
Neurol 1996 53 734-40
15 Boucher BA Witt WO Foster TS The postoperative adverse
effects of inhalational anesthetics Heart Lung 1986 15 63-9

Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 267985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
Fig 1 CT scan of the head without contrast material and this was obtained during the recovery time It demonstrated the approximately 75 cm large acute ICH in the left frontotemporal lobe The ICH extended to both lateral ventricles and the 3rd and 4th ventricles through the external capsule
Fig 2 CT scans of the head obtained the next day postoperatively The density and size of the lobar ICH were reduced but localized swelling wasseen in the left frontotemporal lobe with residual IVH in both lateral ventricles
(Postanesthesia Care Unit) At the arrival to the PACU the
postoperative vital signs were as follows heart rate 85 beats
per minute BP 15080 mmHg and SpO2 98 He responded
appropriately to verbal stimuli Throughout the PACU stay the
blood pressure heart rates and oxygen saturation were moni-
tored at 5-minute intervals Two liters oxygen supplementation
was given during the PACU stay by a nasal prong Fifty μg
of fentanyl was intravenously injected for postoperative pain
control and a warm blanket was applied It was noted that the
patient complained of mild headache with an elevated BP
18095 at 50 minutes after the PACU admission Thus 10 mg
of labetalol hydrochloride was intravenously injected and then
the blood pressure fell to the normal range At 2 hours after
the PACU admission the patient showed a slow verbal
response and an altered consciousness Physical and neurologic
exams were immediately performed The patient did not exhibit
spontaneous eye opening but he opened his eyes in response
to a voice He showed a confused mentality minimal
withdrawal to painful stimuli and a positive Babinski sign on
both feet The Glasgow coma scale (GCS) score was 11 The
electrocardiographic findings serum electrolytes and glucose
level were normal Emergency computerized tomography (CT)
scanning without contrast was performed (Fig 1) On the
emergency CT a large acute intracranial hemorrhage (ICH)
was shown in the left basal ganglia both lateral ventricles and
the 3rd and 4th ventricles Emergency decompressive craniec-
tomy and hematoma removal were performed After surgery he
was sent to the intensive care unit (ICU) and the follow-up
CT (Fig 2) was taken two days later He stayed in the ICU
for 24 days and gradually regained consciousness and he was
268 Anesth Pain Med Vol 6 No 3 2011985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
then transferred to a rehabilitation facility
DISCUSSION
The differential diagnosis of altered mental status
during anesthetic recovery period
Delayed emergence from general anesthesia due to the
residual effects of oral intravenous and inhalational sedative
analgesic and anesthetic medications is a most common cause
of an altered mental status for patients in the PACU This
situation may be complicated by preexisting mental dysfunc-
tion postoperative hypothermia or unrecognized preoperative
ingestion of alcohol opioids benzodiazepines and other presc-
ription and illicit drugs that potentiate the effects of anesthe-
sia-related medications
Emergence delirium is a behavioral manifestation of recovery
from general anesthesia and this ranges from mild confusion
and lethargy to extreme excitement and combativeness
Emergence delirium is the second most common cause of an
altered mental status in patients in the PACU Return of the
cognitive function after general anesthesia may be slower in
the elderly population in the immediate postoperative period
whereas agitation and combativeness are more frequently
observed in children and young adults [5] Emergence delirium
may also be produced by the perioperative administration of
ketamine or atropine and by postoperative withdrawal from
alcohol or illicit drugs Moreover it may be amplified by
anxiety and by discomfort such as surgical pain nausea
pruritis and gastric or urinary bladder distention
An abnormal mental status after surgery may be an
indication of hypoxemia andor hypercarbia due to the residual
effects of anesthetic agents incomplete reversal of neuromu-
scular blockade airway obstruction pneumothorax or pulmo-
nary aspiration [67] Rarely metabolic derangements such as
hypoglycemia hyperglycemia hypothermia hypercalcemia or
hypermagnesemia may contribute to an abnormal mental status
in patients in the PACU Finally once the reversible causes of
acutely altered sensorium are excluded neurologic events such
as seizure activity and embolic or hemorrhage stroke must be
considered
Therapeutic and diagnostic approach to altered
mental status
A spontaneous intracerebral hemorrhage (SICH) is defined as
a blood clot that arises in the brain parenchyma in the
absence of trauma SICH accounts for 10 to 15 of all
strokes and it is associated with a higher mortality rate than
either ischemic stroke or subarachnoid hemorrhage Arterial
hypertension represents the most common cause of nontrau-
matic ICH in patients between 40 and 70 years of age and
accounts for over 50 of cases [89] Thus it constitutes by
far the most important modifiable risk factor for spontaneous
ICH [1011] Further independent risk factors include moderate
and heavy alcohol abuse old age diabetes mellitus coagulo-
pathy and anticoagulant treatment [12] Excessive use of
alcohol increases the risk of ICH by impairing coagulation and
directly affecting the integrity of cerebral vessels [13]
Cigarette smoking seems to increase the risk for subarachnoid
hemorrhage (SAH) but is less strongly associated with SICH
[11] Diabetes mellitus is more commonly associated with
SICH than with SAH [14]
The classic presentation of SICH is a sudden onset of focal
neurological deficit that progresses over hours with accom-
panying headache nausea vomiting an altered consciousness
and an elevated BP However because inhalational anesthetics
may produce a number of various changes in the mental status
after surgery such as headache emergence excitement and
delirium during the recovery period it is hard to distinguish
between the early signs of SICH and the residual effect of
inhalational anesthetics [15] Emergency Computerized tomo-
graphy (CT) scanning is the initial diagnostic procedure of
choice for acute stroke MRI and cerebral angiography are
being increasingly used in the diagnosis of SICH Yet they are
expensive diagnostic tools to routinely use whenever a patient
complains of headache So conducting neurologic and physical
exams are generally preferred as the first step before
performing CT or magnetic resonance imaging (MRI)
Although delayed emergence from general anesthesia and
emergence delirium are the most common causes of the mental
status changes found in the PACU setting the immediate
evaluation must also include considering the potentially
catastrophic conditions such as hypoxemia incomplete reversal
of neuromuscular blockade and embolic or hemorrhage stroke
SICH is rare during the PACU stay but it must always be
considered in the differential diagnosis of mental status
changes CT scanning is the initial diagnostic procedure of
choice However we recommend to conduct neurologic and
physical exams as the first step before performing CT or
magnetic resonance imaging (MRI)
Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 269985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
REFERENCES
1 Hines R Brash PG Waltrous G OConnor T Complications
occuring in the postanesthesia care unit a survey Anesth Analg
1992 74 503-9
2 Zeler J Wells DG Anesthetic-related recovery room compli-
cations Anaesth Intensive Care 1987 15 168-74
3 Van der Walt JH Webb RK Osborne GA Morgan C Mackay
P The Australian Incident Monitoring Study Recovery room
incidents in the first 2000 incident reports Anaesth Intensive Care
1993 21 650-2
4 Bickley LS Szilagyi PG Bates B Bates guide to physical
examination and history taking 10th ed Philadelphia Wolters
KluwerLippincott Williams amp Wilkins 2009
5 Mecca RS Postoperative recovery In Clinical Anesthesia 3rd ed
Edited by Barash PG Gullen BF Stoeling RK Philadelphia Pa
Lippincott-Raven 1997 pp 1279-303
6 Mathew JP Rosenbaum SH OConnor T Barash PG Emergency
tracheal intubation in the postanesthesia care unit physicain error
or patient disease Anesth Analg 1990 71 691-7
7 Daley MD Norman PH Colmenares ME Sandler AN Hypoxa-
emia in adults in the post-anesthesia care unit Can J Anaesth
1991 38 740-6
8 Gomori JM Grossman RI Hackney DB Goldberg HI Zimmer-
man RA Bilaniuk LT Variable appearances of subacute intra-
cranial hematomas on high-field spin-echo MR AJR Am J Roent-
genol 1988 150 171-8
9 Viswanathan A Chabriat H Cerebral microhemorrhage Stroke
2006 37 550-5
10 Fewel ME Thompson BG Jr Hoff JT Spontaneous intracerebral
hemorrhagea review Neurosurg Focus 2003 15 1-16
11 Thrift AG McNeil JJ Forbes A Donnan GA Risk factors for
cerebral hemorrhage in the era of well-controlled hypertension
Melbourne Risk Factor Study (MERFS) Group Stroke 1996 27
2020-5
12 Ariesen MJ Claus SP Rinkel GJ Algra A Risk factors for
intracerebral 6 hemorrhage in the general population a systematic
review Stroke 2003 34 2060-5
13 Cowan DH Effect of alcoholism on hemostasis Semin Hematol
1980 17 137-47
14 Juvela S Prevalence of risk factors in spontaneous intracerebral
hemorrhage and aneurysmal subarachnoid hemorrhage Arch
Neurol 1996 53 734-40
15 Boucher BA Witt WO Foster TS The postoperative adverse
effects of inhalational anesthetics Heart Lung 1986 15 63-9

268 Anesth Pain Med Vol 6 No 3 2011985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
then transferred to a rehabilitation facility
DISCUSSION
The differential diagnosis of altered mental status
during anesthetic recovery period
Delayed emergence from general anesthesia due to the
residual effects of oral intravenous and inhalational sedative
analgesic and anesthetic medications is a most common cause
of an altered mental status for patients in the PACU This
situation may be complicated by preexisting mental dysfunc-
tion postoperative hypothermia or unrecognized preoperative
ingestion of alcohol opioids benzodiazepines and other presc-
ription and illicit drugs that potentiate the effects of anesthe-
sia-related medications
Emergence delirium is a behavioral manifestation of recovery
from general anesthesia and this ranges from mild confusion
and lethargy to extreme excitement and combativeness
Emergence delirium is the second most common cause of an
altered mental status in patients in the PACU Return of the
cognitive function after general anesthesia may be slower in
the elderly population in the immediate postoperative period
whereas agitation and combativeness are more frequently
observed in children and young adults [5] Emergence delirium
may also be produced by the perioperative administration of
ketamine or atropine and by postoperative withdrawal from
alcohol or illicit drugs Moreover it may be amplified by
anxiety and by discomfort such as surgical pain nausea
pruritis and gastric or urinary bladder distention
An abnormal mental status after surgery may be an
indication of hypoxemia andor hypercarbia due to the residual
effects of anesthetic agents incomplete reversal of neuromu-
scular blockade airway obstruction pneumothorax or pulmo-
nary aspiration [67] Rarely metabolic derangements such as
hypoglycemia hyperglycemia hypothermia hypercalcemia or
hypermagnesemia may contribute to an abnormal mental status
in patients in the PACU Finally once the reversible causes of
acutely altered sensorium are excluded neurologic events such
as seizure activity and embolic or hemorrhage stroke must be
considered
Therapeutic and diagnostic approach to altered
mental status
A spontaneous intracerebral hemorrhage (SICH) is defined as
a blood clot that arises in the brain parenchyma in the
absence of trauma SICH accounts for 10 to 15 of all
strokes and it is associated with a higher mortality rate than
either ischemic stroke or subarachnoid hemorrhage Arterial
hypertension represents the most common cause of nontrau-
matic ICH in patients between 40 and 70 years of age and
accounts for over 50 of cases [89] Thus it constitutes by
far the most important modifiable risk factor for spontaneous
ICH [1011] Further independent risk factors include moderate
and heavy alcohol abuse old age diabetes mellitus coagulo-
pathy and anticoagulant treatment [12] Excessive use of
alcohol increases the risk of ICH by impairing coagulation and
directly affecting the integrity of cerebral vessels [13]
Cigarette smoking seems to increase the risk for subarachnoid
hemorrhage (SAH) but is less strongly associated with SICH
[11] Diabetes mellitus is more commonly associated with
SICH than with SAH [14]
The classic presentation of SICH is a sudden onset of focal
neurological deficit that progresses over hours with accom-
panying headache nausea vomiting an altered consciousness
and an elevated BP However because inhalational anesthetics
may produce a number of various changes in the mental status
after surgery such as headache emergence excitement and
delirium during the recovery period it is hard to distinguish
between the early signs of SICH and the residual effect of
inhalational anesthetics [15] Emergency Computerized tomo-
graphy (CT) scanning is the initial diagnostic procedure of
choice for acute stroke MRI and cerebral angiography are
being increasingly used in the diagnosis of SICH Yet they are
expensive diagnostic tools to routinely use whenever a patient
complains of headache So conducting neurologic and physical
exams are generally preferred as the first step before
performing CT or magnetic resonance imaging (MRI)
Although delayed emergence from general anesthesia and
emergence delirium are the most common causes of the mental
status changes found in the PACU setting the immediate
evaluation must also include considering the potentially
catastrophic conditions such as hypoxemia incomplete reversal
of neuromuscular blockade and embolic or hemorrhage stroke
SICH is rare during the PACU stay but it must always be
considered in the differential diagnosis of mental status
changes CT scanning is the initial diagnostic procedure of
choice However we recommend to conduct neurologic and
physical exams as the first step before performing CT or
magnetic resonance imaging (MRI)
Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 269985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
REFERENCES
1 Hines R Brash PG Waltrous G OConnor T Complications
occuring in the postanesthesia care unit a survey Anesth Analg
1992 74 503-9
2 Zeler J Wells DG Anesthetic-related recovery room compli-
cations Anaesth Intensive Care 1987 15 168-74
3 Van der Walt JH Webb RK Osborne GA Morgan C Mackay
P The Australian Incident Monitoring Study Recovery room
incidents in the first 2000 incident reports Anaesth Intensive Care
1993 21 650-2
4 Bickley LS Szilagyi PG Bates B Bates guide to physical
examination and history taking 10th ed Philadelphia Wolters
KluwerLippincott Williams amp Wilkins 2009
5 Mecca RS Postoperative recovery In Clinical Anesthesia 3rd ed
Edited by Barash PG Gullen BF Stoeling RK Philadelphia Pa
Lippincott-Raven 1997 pp 1279-303
6 Mathew JP Rosenbaum SH OConnor T Barash PG Emergency
tracheal intubation in the postanesthesia care unit physicain error
or patient disease Anesth Analg 1990 71 691-7
7 Daley MD Norman PH Colmenares ME Sandler AN Hypoxa-
emia in adults in the post-anesthesia care unit Can J Anaesth
1991 38 740-6
8 Gomori JM Grossman RI Hackney DB Goldberg HI Zimmer-
man RA Bilaniuk LT Variable appearances of subacute intra-
cranial hematomas on high-field spin-echo MR AJR Am J Roent-
genol 1988 150 171-8
9 Viswanathan A Chabriat H Cerebral microhemorrhage Stroke
2006 37 550-5
10 Fewel ME Thompson BG Jr Hoff JT Spontaneous intracerebral
hemorrhagea review Neurosurg Focus 2003 15 1-16
11 Thrift AG McNeil JJ Forbes A Donnan GA Risk factors for
cerebral hemorrhage in the era of well-controlled hypertension
Melbourne Risk Factor Study (MERFS) Group Stroke 1996 27
2020-5
12 Ariesen MJ Claus SP Rinkel GJ Algra A Risk factors for
intracerebral 6 hemorrhage in the general population a systematic
review Stroke 2003 34 2060-5
13 Cowan DH Effect of alcoholism on hemostasis Semin Hematol
1980 17 137-47
14 Juvela S Prevalence of risk factors in spontaneous intracerebral
hemorrhage and aneurysmal subarachnoid hemorrhage Arch
Neurol 1996 53 734-40
15 Boucher BA Witt WO Foster TS The postoperative adverse
effects of inhalational anesthetics Heart Lung 1986 15 63-9

Doo Jae Min et alCerebral hemorrhage during the anesthesia recovery period 269985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103985103
REFERENCES
1 Hines R Brash PG Waltrous G OConnor T Complications
occuring in the postanesthesia care unit a survey Anesth Analg
1992 74 503-9
2 Zeler J Wells DG Anesthetic-related recovery room compli-
cations Anaesth Intensive Care 1987 15 168-74
3 Van der Walt JH Webb RK Osborne GA Morgan C Mackay
P The Australian Incident Monitoring Study Recovery room
incidents in the first 2000 incident reports Anaesth Intensive Care
1993 21 650-2
4 Bickley LS Szilagyi PG Bates B Bates guide to physical
examination and history taking 10th ed Philadelphia Wolters
KluwerLippincott Williams amp Wilkins 2009
5 Mecca RS Postoperative recovery In Clinical Anesthesia 3rd ed
Edited by Barash PG Gullen BF Stoeling RK Philadelphia Pa
Lippincott-Raven 1997 pp 1279-303
6 Mathew JP Rosenbaum SH OConnor T Barash PG Emergency
tracheal intubation in the postanesthesia care unit physicain error
or patient disease Anesth Analg 1990 71 691-7
7 Daley MD Norman PH Colmenares ME Sandler AN Hypoxa-
emia in adults in the post-anesthesia care unit Can J Anaesth
1991 38 740-6
8 Gomori JM Grossman RI Hackney DB Goldberg HI Zimmer-
man RA Bilaniuk LT Variable appearances of subacute intra-
cranial hematomas on high-field spin-echo MR AJR Am J Roent-
genol 1988 150 171-8
9 Viswanathan A Chabriat H Cerebral microhemorrhage Stroke
2006 37 550-5
10 Fewel ME Thompson BG Jr Hoff JT Spontaneous intracerebral
hemorrhagea review Neurosurg Focus 2003 15 1-16
11 Thrift AG McNeil JJ Forbes A Donnan GA Risk factors for
cerebral hemorrhage in the era of well-controlled hypertension
Melbourne Risk Factor Study (MERFS) Group Stroke 1996 27
2020-5
12 Ariesen MJ Claus SP Rinkel GJ Algra A Risk factors for
intracerebral 6 hemorrhage in the general population a systematic
review Stroke 2003 34 2060-5
13 Cowan DH Effect of alcoholism on hemostasis Semin Hematol
1980 17 137-47
14 Juvela S Prevalence of risk factors in spontaneous intracerebral
hemorrhage and aneurysmal subarachnoid hemorrhage Arch
Neurol 1996 53 734-40
15 Boucher BA Witt WO Foster TS The postoperative adverse
effects of inhalational anesthetics Heart Lung 1986 15 63-9