Embed Size (px)
Citation preview
FACULDADE DE MEDICINA UFPEL
CENTRO DE ENSINO E TREINAMENTO em ANESTESIOLOGIA
INSTRUMENTOS DE AVALIAÇÃO DO ESTRESSE OCUPACIONAL
Prof. Gastão F. Duval Neto, MD , PhD
Stress Performance ScalePerformance
or Eff iciency
Critical Level
Stress or Anxiety
CHANGES IN PHYSICAL AND MENTAL HEALTH OF ANESTHESIOLOGISTS MAY OCCUR
THUS DECREASING IN THE SAFETY OF THE CLINICAL PRACTICE
Anesthesia Patient Safety FoundationNEWSLETTER The Official Journal of the Anesthesia Patient Safety Foundation Volume 20, No. 1, Circulation 75,648
STRESS and FATIGUE IN ANESTHESIOLOGISTS
THIS IS NOT AN UNUSUAL SITUATION NOWADAYS
HOW WILL BE THE SPECIFICALLY PSYCHOLOGICAL BRAIN RESPONSE TO THIS OCCUPATIONAL
STRESSFUL SITUATION
?
Individual Personality
has great importance in the development of
occupational stress
Impaired Resident
Síntese dos Modelos para Estresse Ocupacional
Após o entendimento do conceito de stress tal como dos seus principais modelosteóricos desenvolvidos, podem-se tirar algumas conclusões:
• A percepção de stress é subjetiva, isto é, o mesmo stressor poderá serpercebido de forma diferente e com intensidade diferente por distintosindivíduos;
• O trabalho e as organizações constituem-se como potenciais fontes de pressão;
• O papel individual no ciclo de stress é ativo (características de individualidade);
• O stress ocupacional tem conseqüências psicológicas, fisiológicas ecomportamentais.
.
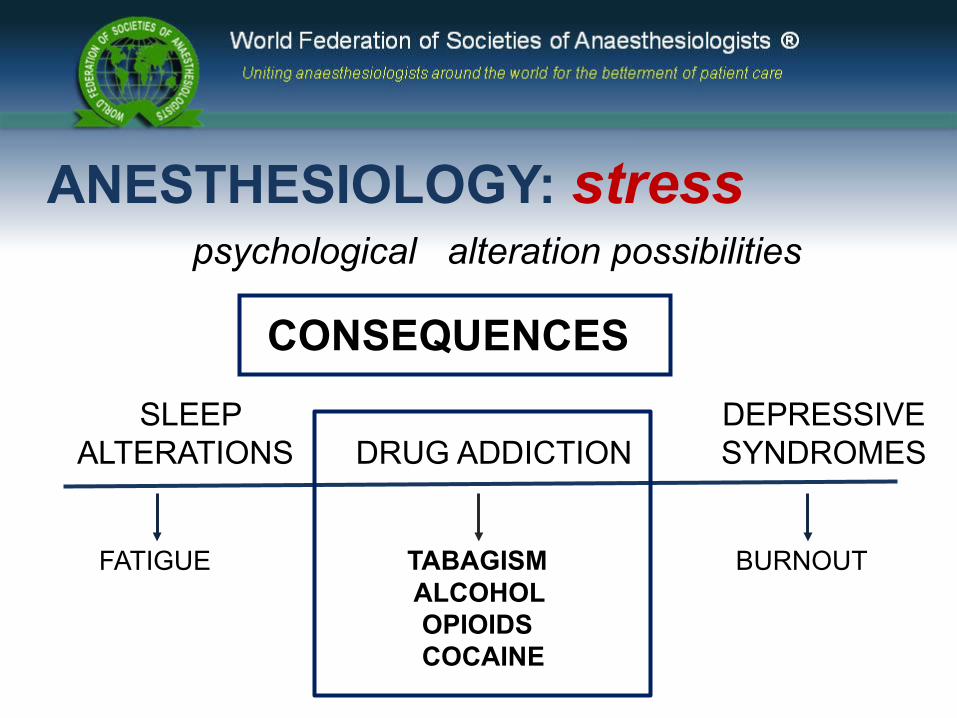
CONSEQUENCES
SLEEP DEPRESSIVE ALTERATIONS DRUG ADDICTION SYNDROMES
FATIGUE TABAGISM ALCOHOL OPIOIDS COCAINE
BURNOUT
ANESTHESIOLOGY: stress psychological alteration possibilities
Editorials
Promoting wellbeing among doctors We should move away from a disease model and focus on positive functioning
Gavin Yamey, deputy editor.
2001;322:252-253 ( 3 February )BMJ
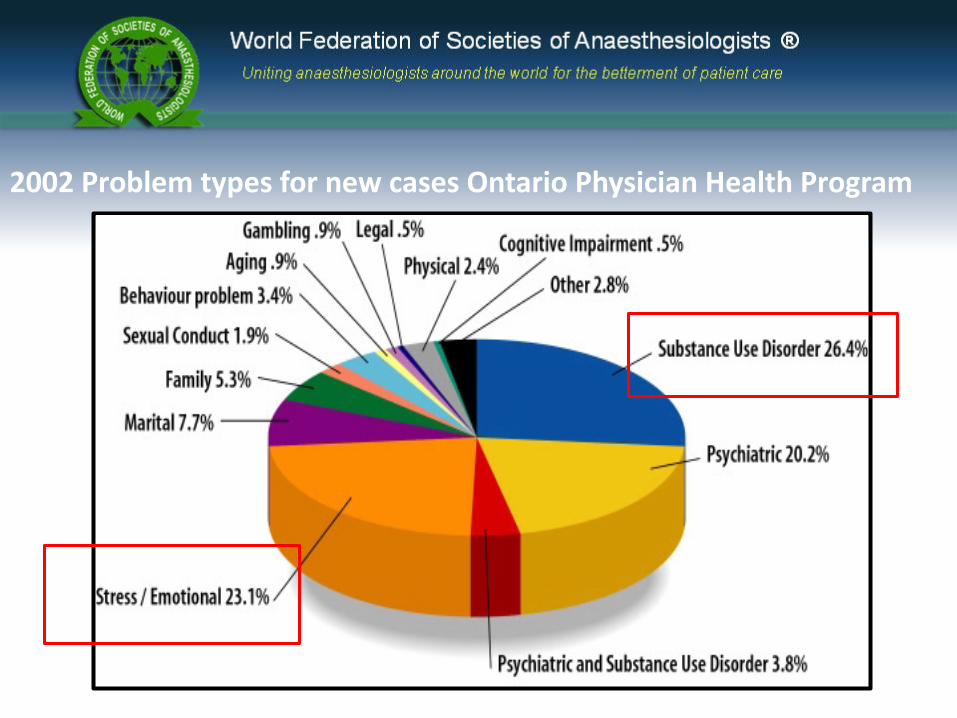
2002 Problem types for new cases Ontario Physician Health Program
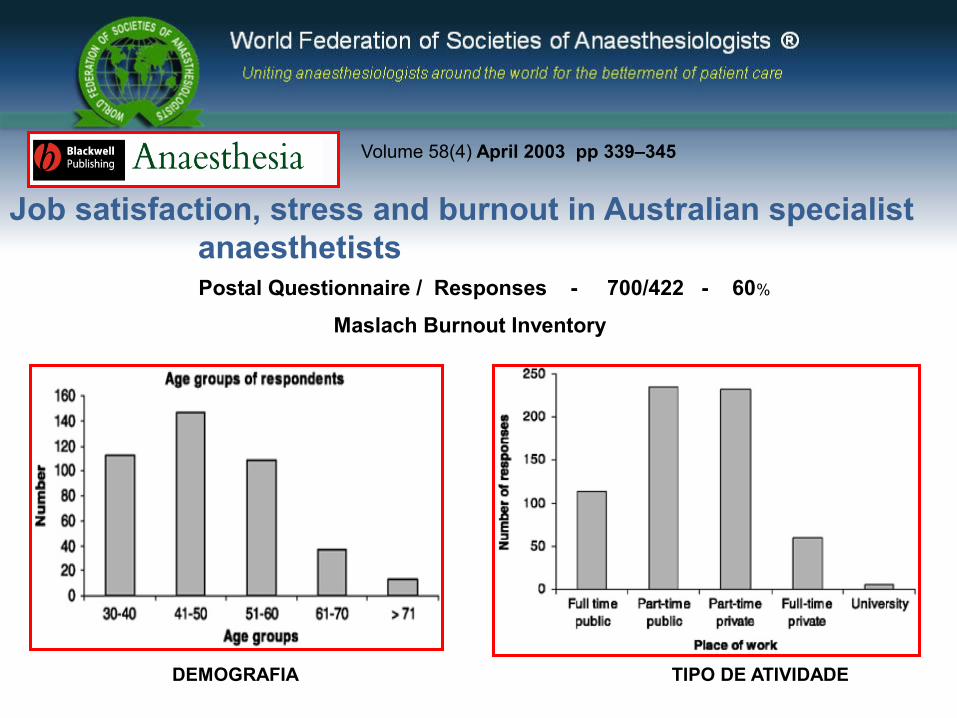
Volume 58(4) April 2003 pp 339–345
Job satisfaction, stress and burnout in Australian specialist anaesthetists
DEMOGRAFIA TIPO DE ATIVIDADE
Postal Questionnaire / Responses - 700/422 - 60%
Maslach Burnout Inventory
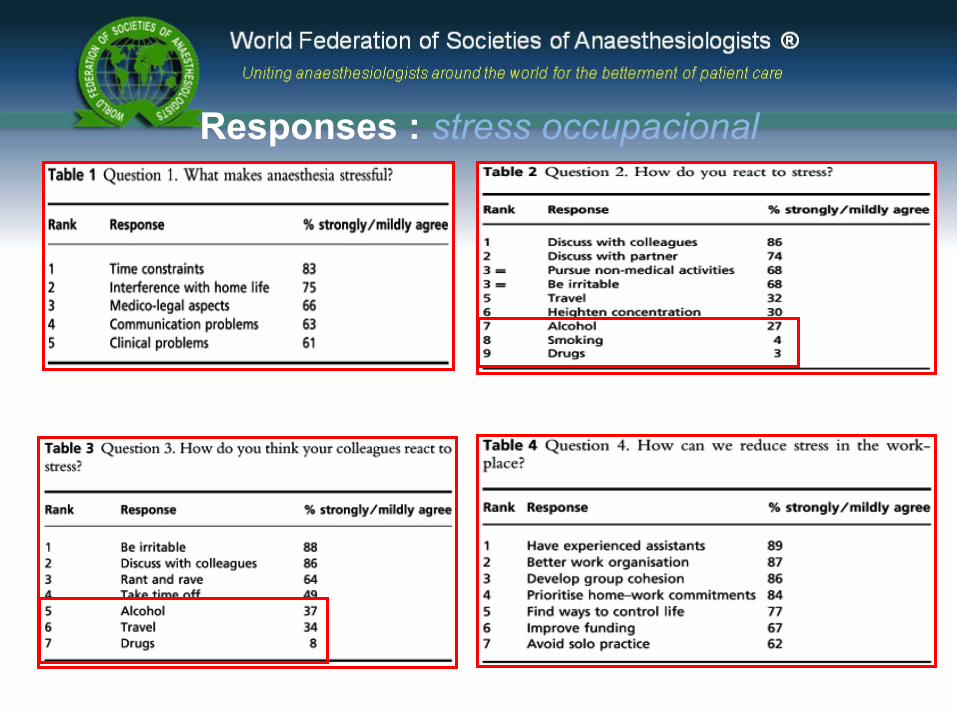
Responses : stress occupacional
Confronting Depression and Suicide in Physicians A Consensus Statement Claudia Center, JD - JAMA - May 14, 2011 -
Objective - To encourage treatment of depression and prevention of suicide in physicians by calling for a shift in professional attitudes and institutional policies to support physicians seeking help.
Consensus Process This consensus statement emerged from a plenary session during which each work group presented its recommendations. The consensus statement was circulated to and approved by all participants.
Confronting Depression and Suicide in Physicians A Consensus Statement Claudia Center, JD - JAMA - May 14, 2011 -
The culture of medicine accords low priority to physician mental health despite evidence of untreated mood disorders and an increased burden of suicide.
Barriers to physicians’ seeking help are often punitive, including discrimination in medical licensing, hospital privileges, and professional advancement. This consensus statement recommends transforming professional attitudes and changing institutional policies to encourage physicians to seek help.
As barriers are removed and physicians confront depression and suicidality in their peers, they are more likely to recognize and treat these conditions in patients, including colleagues and medical students.
CONCLUSION
Effect of Brief Behavioral Intervention Program in Managing Stress in Medical Students from Two Southern California Universities Stephanie A. Bughi,BS – Med Edu 11: 17, 2006
General Well Being Scale (GWBS)
Pré teste e Pós teste inicio e final estágio rotatório
a brief behavioral intervention program (BBIP) on stress management
‘
Na psiquiatria, o stress é entendido como um estado de tensão emocional que produz um estado psicológico desagradável caracterizado por irritabilidade, distúrbio de sono e do apetite, dificuldade na concentração e preocupação exagerada com relação a situações triviais. Em geral, há queda no rendimento com diminuição da memória e impotência. Pode ser desencadeado por uma situação súbita ou por situações conflitantes contínuas e seguidas
O stress positivo, chamado de eustresse, assim como o negativo, chamado de distresse, causam reações fisiológicas similares: as extremidades (mãos e pés) tendem a ficar suados e frios, a aceleração cardíaca e pressão arterial tendem a subir, o nível de tensão muscular tende a aumentar, etc.
Na psiquiatria, o stress é entendido como umA situação de tensão emocional que produz um estado psicológico desagradável
caracterizadopor irritabilidade, distúrbio de sono e do apetite, dificuldade na concentração e preocupação exagerada com relação a situações
triviais.
O stress positivo, chamado de eustresse, assim como o negativo, chamado de distresse, causam reações fisiológicas similares: as extremidades (mãos e pés) tendem a ficar suados e frios, a
aceleração cardíaca e pressão arterial tendem a subir, o nível de tensão
muscular tende a aumentar, etc.
DEFINIÇÕES
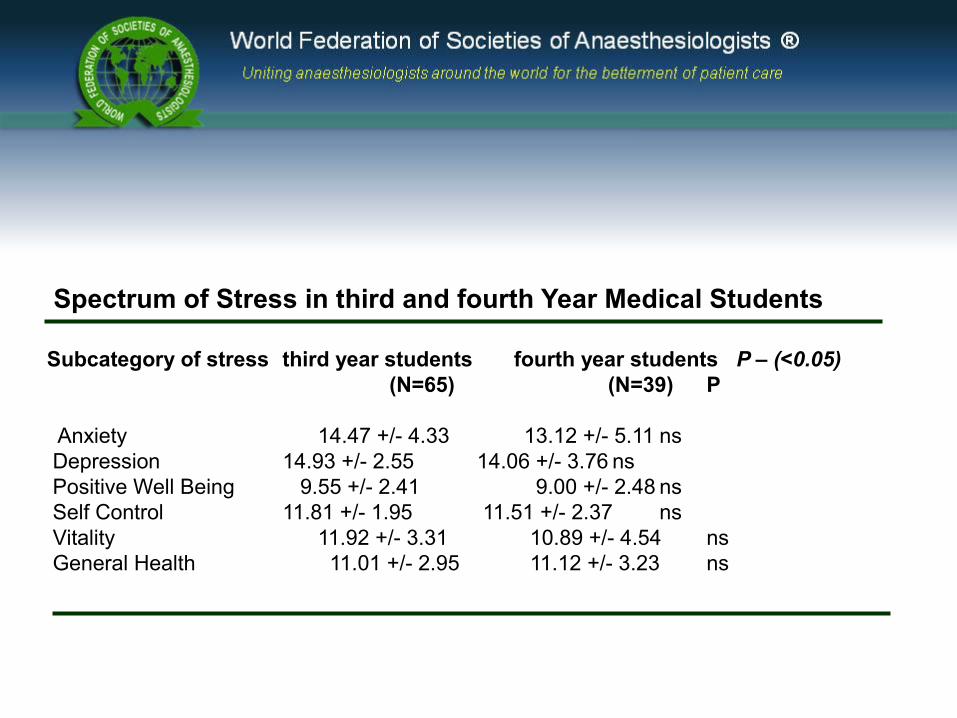
Spectrum of Stress in third and fourth Year Medical Students
Subcategory of stress third year students fourth year students P – (<0.05) (N=65) (N=39) P
Anxiety 14.47 +/- 4.33 13.12 +/- 5.11 ns Depression 14.93 +/- 2.55 14.06 +/- 3.76 ns Positive Well Being 9.55 +/- 2.41 9.00 +/- 2.48 ns Self Control 11.81 +/- 1.95 11.51 +/- 2.37 ns Vitality 11.92 +/- 3.31 10.89 +/- 4.54 ns General Health 11.01 +/- 2.95 11.12 +/- 3.23 ns
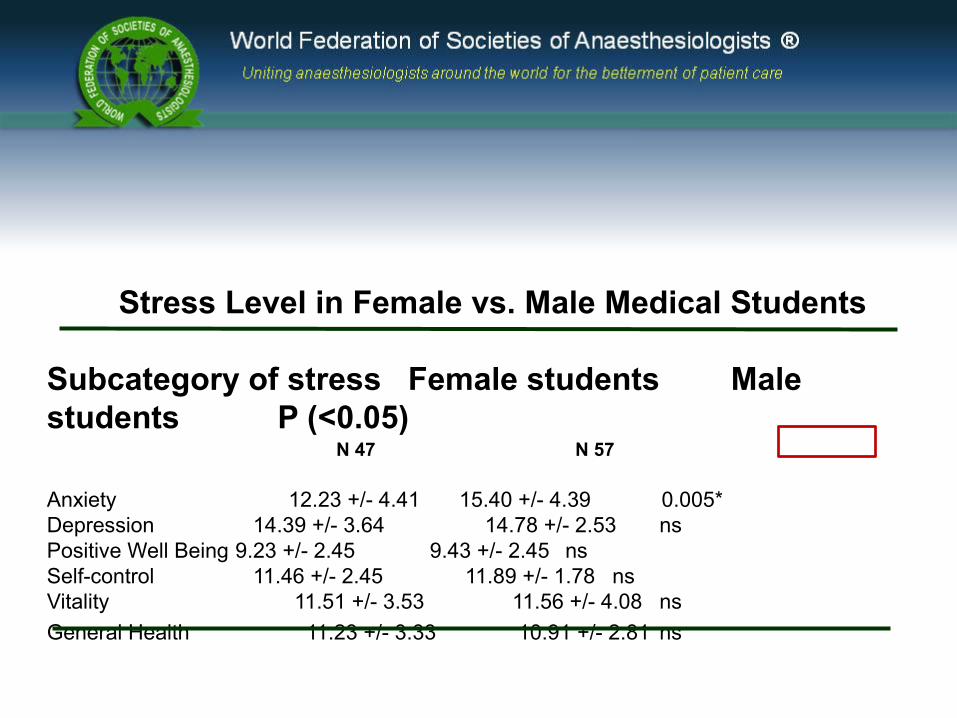
Stress Level in Female vs. Male Medical Students
Subcategory of stress Female students Male students P (<0.05) N 47 N 57
Anxiety 12.23 +/- 4.41 15.40 +/- 4.39 0.005*Depression 14.39 +/- 3.64 14.78 +/- 2.53 nsPositive Well Being 9.23 +/- 2.45 9.43 +/- 2.45 nsSelf-control 11.46 +/- 2.45 11.89 +/- 1.78 nsVitality 11.51 +/- 3.53 11.56 +/- 4.08 nsGeneral Health 11.23 +/- 3.33 10.91 +/- 2.81 ns
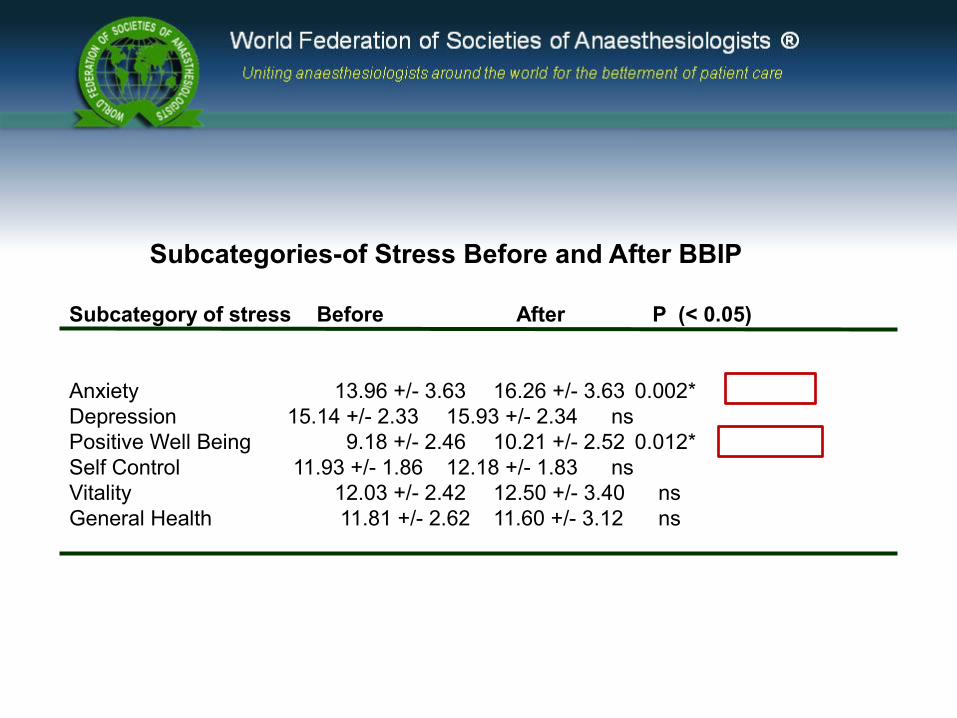
Subcategories-of Stress Before and After BBIP
Subcategory of stress Before After P (< 0.05)
Anxiety 13.96 +/- 3.63 16.26 +/- 3.63 0.002*Depression 15.14 +/- 2.33 15.93 +/- 2.34 nsPositive Well Being 9.18 +/- 2.46 10.21 +/- 2.52 0.012*Self Control 11.93 +/- 1.86 12.18 +/- 1.83 nsVitality 12.03 +/- 2.42 12.50 +/- 3.40 nsGeneral Health 11.81 +/- 2.62 11.60 +/- 3.12 ns
VALOR DA INTERVENÇÃO ATIVA NA SITUAÇÃO DE ESTRESSE OCUPACIONAL EM ÁREA DE FORMAÇÃO MÉDICA
Sources of Stress for Residents and Recommendations for Programs to Assist Them Robert E. Levey, PhD, MPH
SUPPORT STAFF TO THE RESIDENTS can greatly reduce physicians’ anxieties and help them accomplish their educational goals and transition to practice.
A successful residents’ assistance program reduces stress for the resident and his or her family or significant other; facilitates an optimal environment for professional growth and long-term well-being that survives long after residency training is completed; facilitates successful conflict resolution; and assures the protection and safety of patients.
AC AD E M I C ME D I C I N E, vol. 76, FE B , 2 0 0 1
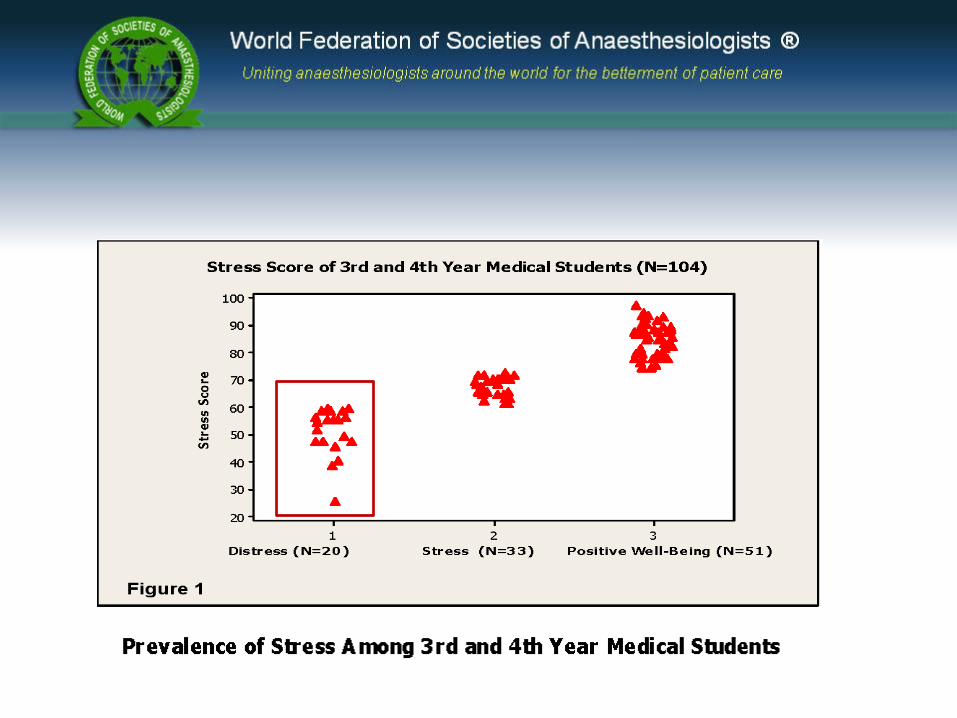
Stress is very prevalent among medical students.
Increased awareness of stress and early intervention may prevent burnout and improve health care delivery.
In our group of students, a brief stress management intervention during the third and 4 th year of medical training had salutary effects.
Addressing the effect of stress on doctors, particularly young doctors in training, becomes paramount since high stress and its associated consequences can result in either losing doctors from the medical
profession or putting both doctors and patients at risk.
Medical schools are called upon to identify and help medical students to manage stress, since learning to cope with stress early in the medical training will prepare them to better deal with the undoubtedly high
stress they will be exposed to in the medical practice.
By doing so, students will be empowered to find solutions to their academic, social, and medical career difficulties and help them to better adjust to the complex life of a practicing physician in the 21st century
Conclusion
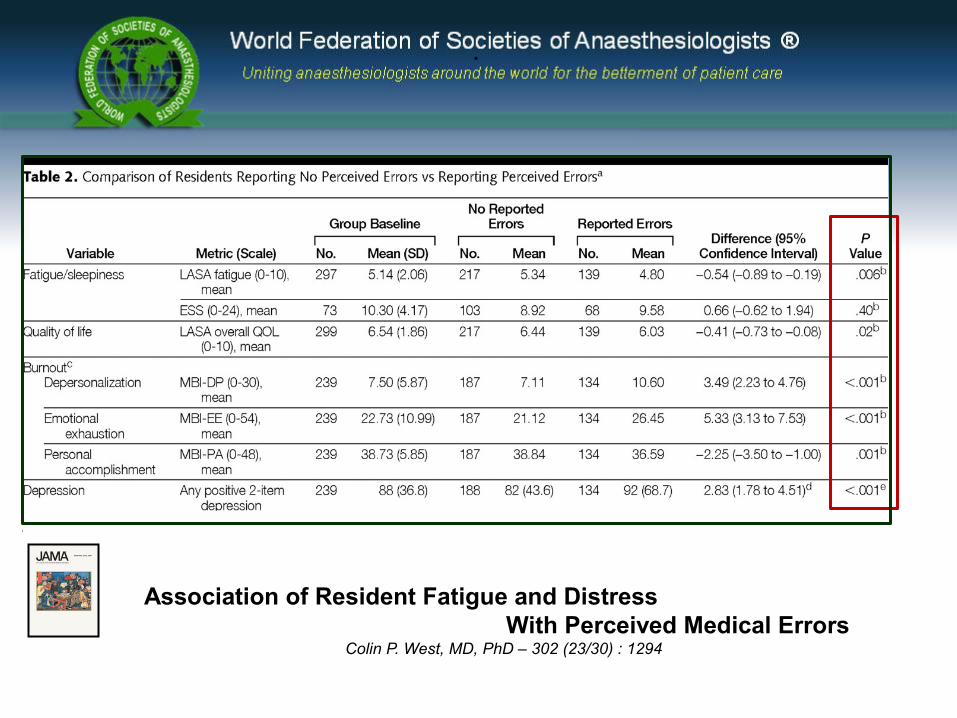
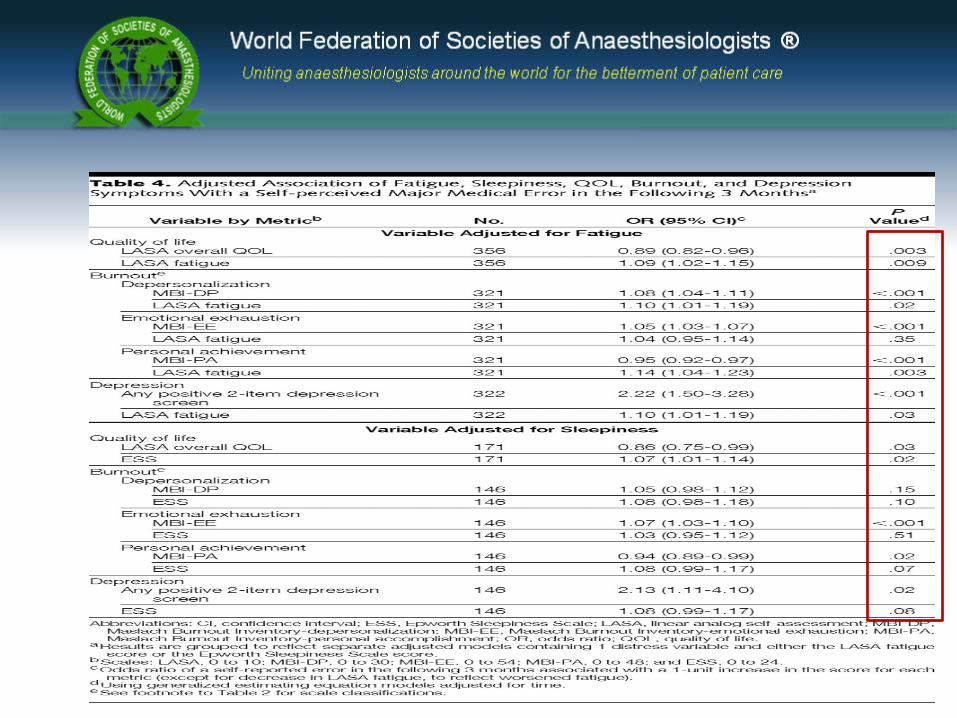
Association of Resident Fatigue and Distress With Perceived Medical Errors Colin P. West, MD, PhD – 302 (23/30) : 1294 - 2011
This study suggests that fatigue, sleepiness, burnout, depression, and reduced QOL are independently associated with an increased risk of future self-perceived major medical errors.
In addition to the national efforts to reduce fatigue and sleepiness, well-designed interventions to prevent, identify, and treat distress among physicians are needed.
Additional research is necessary to determine the most effective strategies for accomplishing these goals. Changes to the process of physician training should address both resident fatigue and distress in an effort to improve resident and patient safety.
.
West, C. P. et al. JAMA 2009;302:1294-1300
Copyright restrictions may apply.
Association of Resident Fatigue and Distress With Perceived Medical Errors Colin P. West, MD, PhD – 302 (23/30) : 1294

Working hours, occupational stress and depression among physicians K Tomioka 61 (3): 163-170 ; 2011
Aims - To investigate the cross-sectional association between working hours, OS and depression among physicians.
Results The questionnaire was returned by 795 alumni (response rate, 42%), and 706 respondents (534 men and 172 women) were suitable for analysis.
(>70 h/week) x (<54 h/week)
The adjuste odds ratio (Ors) of depression stratified according to working hours and ERR tended to be higher in the groups with a higher level of occupational stress.
Conclusions
This study indicates that the management of OS is needed as a countermeasure against depression among physicians.
Depression in Medical Trainees
Prospective medical students and residents are extremely unlikely to report a history of depression during highly competitive selection interviews.
The prevalence of depression in these populations and in medical student and postgraduate trainees is unknown, but it is estimated to range from 15-30%.
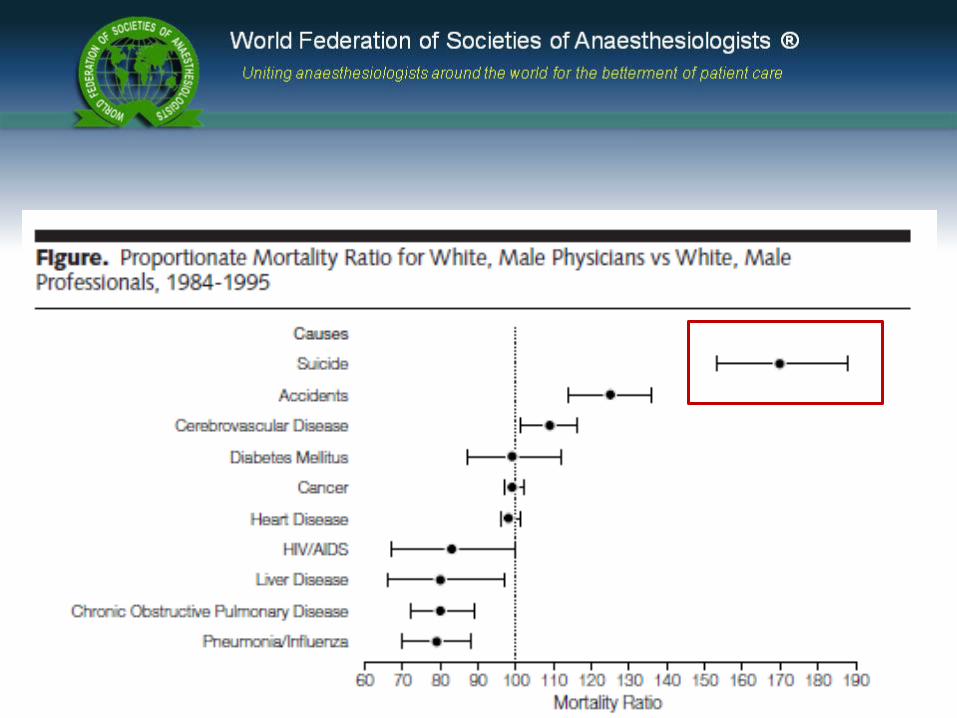
After accidents, suicide is the most common cause of death among medical students.
Shaw DL, Wedding D, Zeldow PB. Suicide among medical students and physicians, special problems of medical students. In: Wedding D, ed. Behavior and Medicine. 3rd ed. Hogrefe and Huber: 2001:78-9 (chap 6).
Rates of medication errors among depressed and burnout residents: prospective cohort study
Amy M Fahrenkopf – 336 : 488, 2008
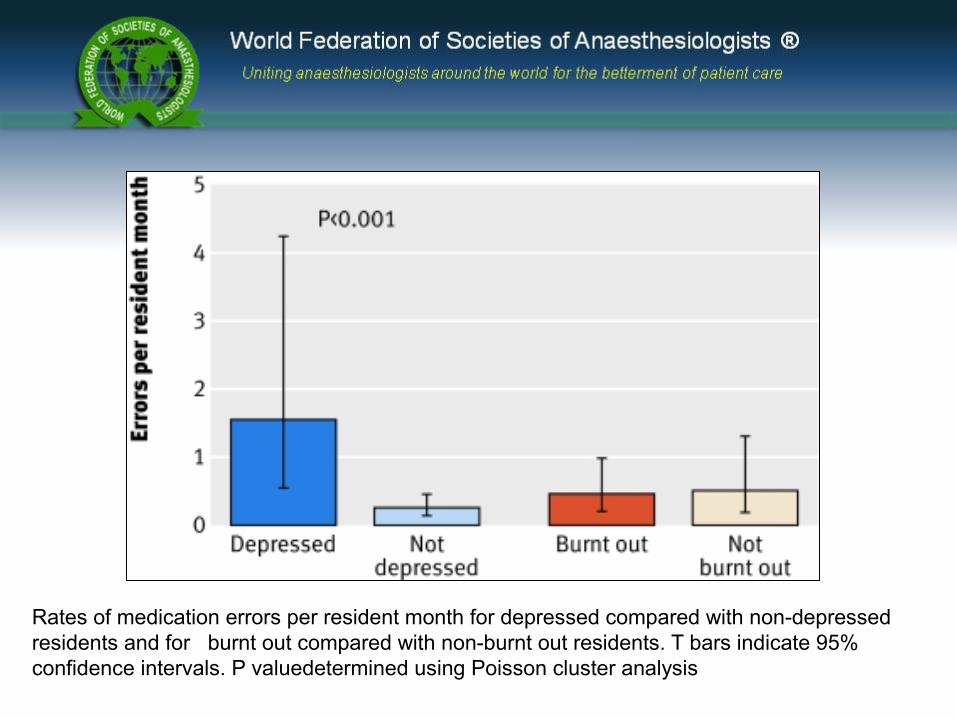
Rates of medication errors per resident month for depressed compared with non-depressed residents and for burnt out compared with non-burnt out residents. T bars indicate 95% confidence intervals. P valuedetermined using Poisson cluster analysis
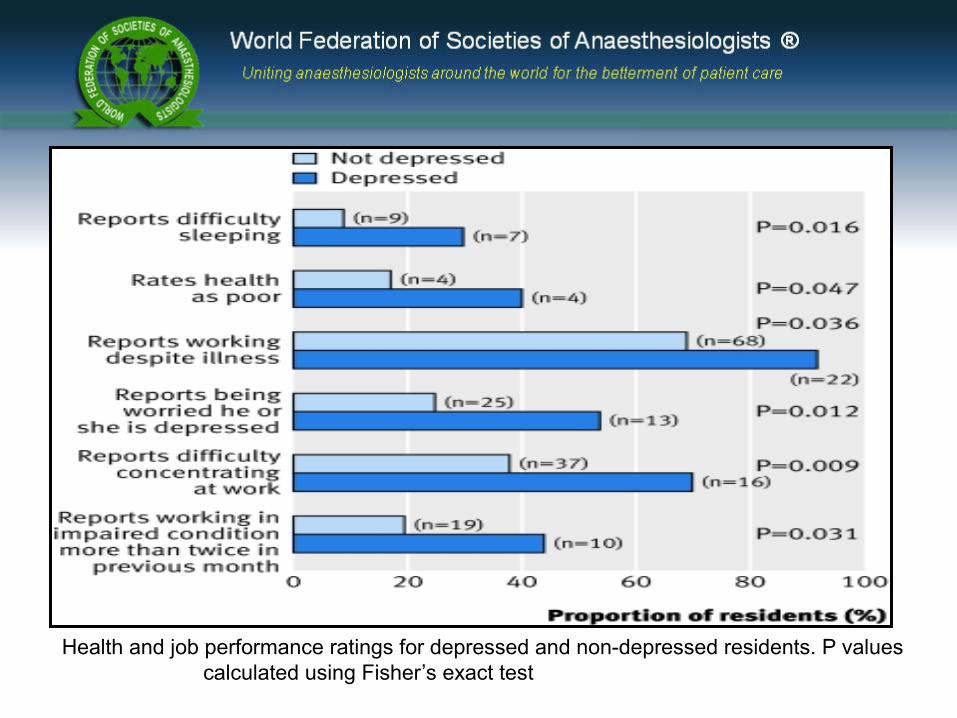
Health and job performance ratings for depressed and non-depressed residents. P values calculated using Fisher’s exact test
Development of four self-report measures of job stressors and strain:
Interpersonal Conflict at Work Scale, Organizational Constraints Scale, Quantitative Workload Inventory, and Physical Symptoms Inventory.
Despite the widespread use of self-report measures of both job-related stressors and strains, relatively few carefully developed scales for which validity data exist are available.
In this article, we discuss 3 job stressor scales (Interpersonal Conflict at Work Scale, Organizational Constraints Scale, and Quantitative Workload Inventory) and 1 job strain scale (Physical Symptoms Inventory). Using meta-analysis, we combined the results of 18 studies to provide estimates of relations between our scales and other variables. Data showed moderate convergent validity for the 3 job stressor scales, suggesting some objectively to these self-reports
Occupational Stress Inventory - Revised Edition™ (OSI-R™)
ANÁLISE INTEGRADA
Gastão F. Duval Neto, MD PhD Professor of Anesthesiology of Anesthesia Department of UFPel, BrazilPresident of Occupational Health Committee of Brazilian Society of Anesthesiology
Isabelle Hansez, PhD Professor Department of Work Psychology, University of Liège, Belgium
STUDY of RELATIONSHIP AMONG OCCUPATIONAL STRESS LEVEL and THE WORK CONDITIONS: IN ANESTHESIOLOGY TRAINING PROGRAMS IN BRAZIL
STUDY of RELATIONSHIP AMONG OCCUPATIONAL STRESS LEVEL and THE WORK CONDITIONS: IN ANESTHESIOLOGY TRAINING PROGRAMS IN BRAZIL
Main Objective evaluation of the relationship among the occupational stress level and the work conditions : differences among the R1 , R2, R3 years of training and instructors.
comparison among levels of job control (5 dimensions) in Brazilian and Belgian anesthetists.
evaluation of relationship among the demographic characteristics ( like age, sex, conjugal situation) and level of stress during training programs in Brazil
Methodology
Two questionnaires were applied :
PNOS - POSITIVE and NEGATIVE OCCUPATIONAL STRESS INVENTORY (HANSEZ 2004)
WOCCQ - MULTI-DIMENSIONAL SCALE TO MEASURE THE CONTROL THAT HAS IN HIS/HER WORK SITUATION (HANSEZ 2001)
STUDY of RELATIONSHIP AMONG OCCUPATIONAL STRESS LEVEL and THE WORK CONDITIONS: IN ANESTHESIOLOGY TRAINING PROGRAMS IN BRAZIL
STUDY of RELATIONSHIP AMONG OCCUPATIONAL STRESS LEVEL and THE WORK CONDITIONS: IN ANESTHESIOLOGY TRAINING PROGRAMS IN BRAZIL
EVALUATION OF THE RELIABILITY COEFFICIENT OF THE ANSWERS OF THE QUESTIONNAIRES
CRONBACH’s COEFFICIENT ALPHA 0,78 for job engagement 0,85 for job strain
STUDY of RELATIONSHIP AMONG OCCUPATIONAL STRESS LEVEL and THE WORK CONDITIONS: IN ANESTHESIOLOGY TRAINING PROGRAMS IN BRAZIL
SAMPLE DESCRIPTION
1225 questionnaires were applied
776 questionnaires were returned
69 %
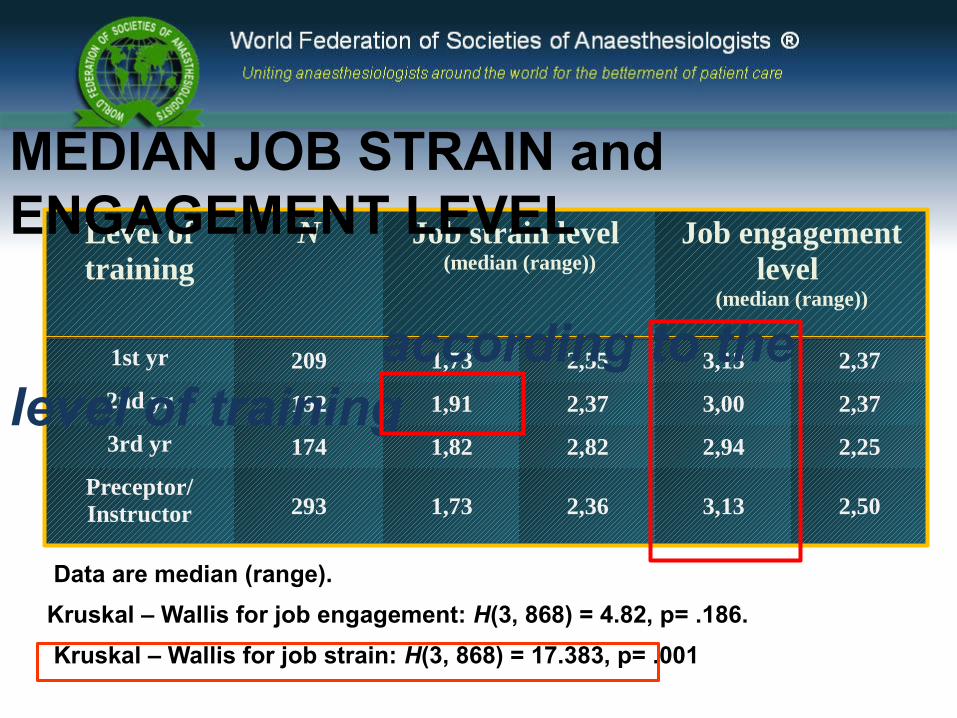
Level of training
N Job strain level (median (range))
Job engagement level
(median (range))
1st yr 209 1,73 2,55 3,13 2,37
2nd yr 192 1,91 2,37 3,00 2,37
3rd yr 174 1,82 2,82 2,94 2,25
Preceptor/Instructor 293 1,73 2,36 3,13 2,50
Data are median (range). Kruskal – Wallis for job engagement: H(3, 868) = 4.82, p= .186. Kruskal – Wallis for job strain: H(3, 868) = 17.383, p= .001
MEDIAN JOB STRAIN and ENGAGEMENT LEVEL according to the level of training
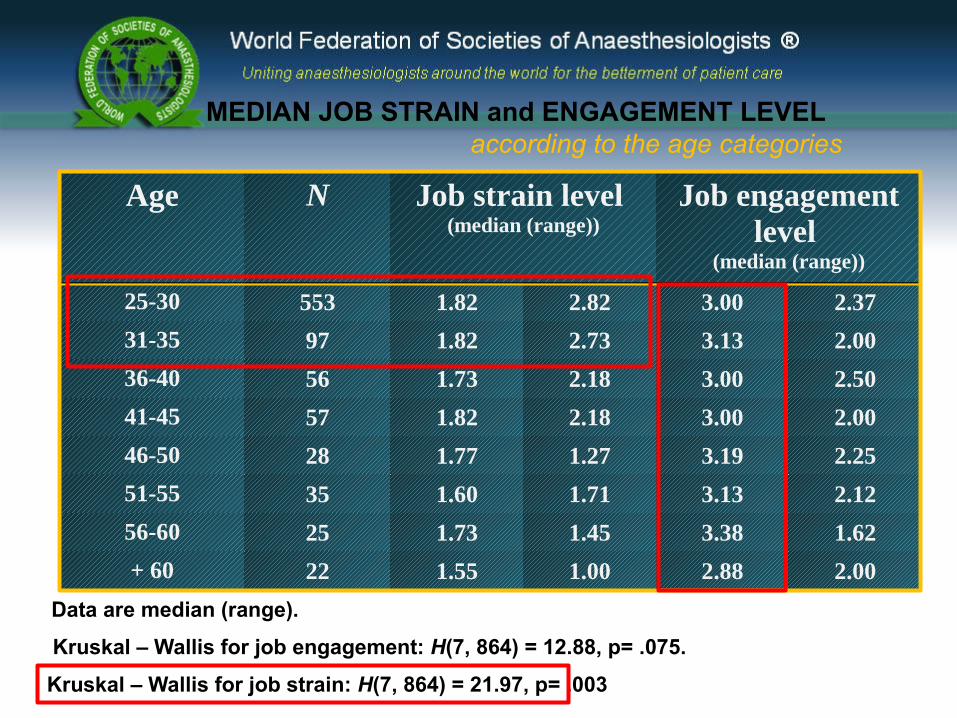
Age N Job strain level (median (range))
Job engagementlevel
(median (range))
25-30 553 1.82 2.82 3.00 2.37
31-35 97 1.82 2.73 3.13 2.00
36-40 56 1.73 2.18 3.00 2.50
41-45 57 1.82 2.18 3.00 2.00
46-50 28 1.77 1.27 3.19 2.25
51-55 35 1.60 1.71 3.13 2.12
56-60 25 1.73 1.45 3.38 1.62
+ 60 22 1.55 1.00 2.88 2.00
Data are median (range).
Kruskal – Wallis for job engagement: H(7, 864) = 12.88, p= .075.
Kruskal – Wallis for job strain: H(7, 864) = 21.97, p= .003
MEDIAN JOB STRAIN and ENGAGEMENT LEVEL according to the age categories
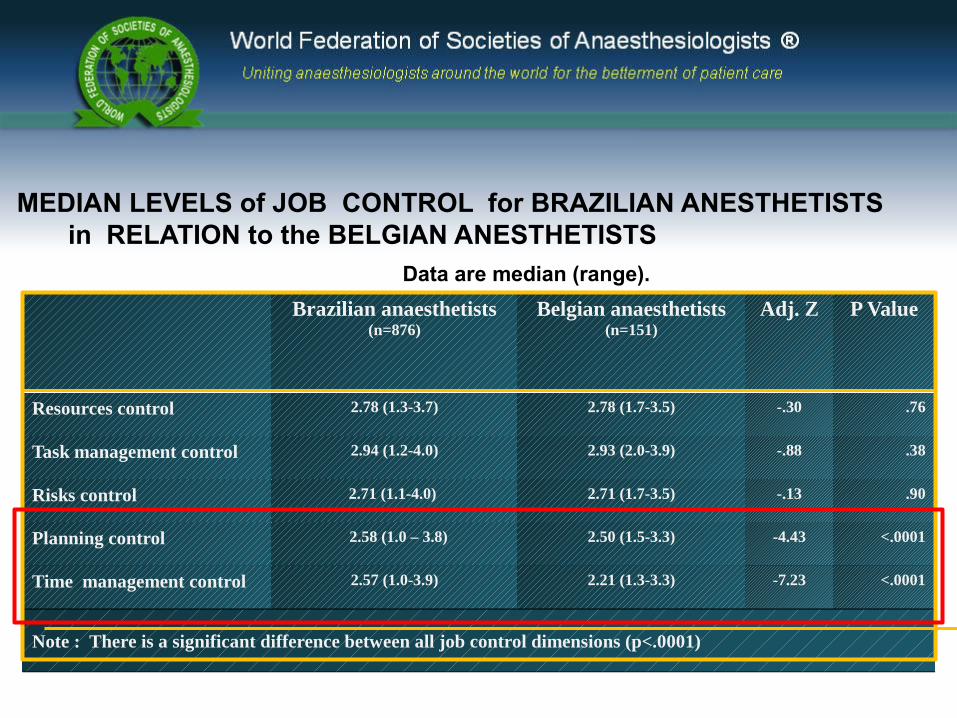
Brazilian anaesthetists(n=876)
Belgian anaesthetists(n=151)
Adj. Z P Value
Resources control 2.78 (1.3-3.7) 2.78 (1.7-3.5) -.30 .76
Task management control 2.94 (1.2-4.0) 2.93 (2.0-3.9) -.88 .38
Risks control 2.71 (1.1-4.0) 2.71 (1.7-3.5) -.13 .90
Planning control 2.58 (1.0 – 3.8) 2.50 (1.5-3.3) -4.43 <.0001
Time management control 2.57 (1.0-3.9) 2.21 (1.3-3.3) -7.23 <.0001
Note : There is a significant difference between all job control dimensions (p<.0001)
MEDIAN LEVELS of JOB CONTROL for BRAZILIAN ANESTHETISTS in RELATION to the BELGIAN ANESTHETISTS Data are median (range).
AGRADEÇO PELA SUA ATENÇÃO !
Stressors – são acontecimentos ou características dos acontecimentos (estímulos) que induzem stress nas pessoas que os enfrentam (exemplo: sobrecarga de trabalho, conflitos com as excessivas exigências dos casos clínicos , demandas jurídicas, competitividade, etc. ).
Strain – é constituído pelas respostas psicológicas, físicas ou comportamentais dos indivíduos aos stressors.
Definições
O stress ocupacional é “a interação das condições de trabalho com as características do trabalhador, de tal modo que as exigências que lhe são criadas ultrapassam a sua capacidade em lidar com elas” (Ross e Atmaier, 1994), ou seja, esgota as estratégias para lidar com o stress, estratégias essas que são designadas por coping.
Os potenciais resultados de longo prazo do stress ocupacional e a necessidade de criar programas com vista à sua gestão e redução, levaram muitos investigadores a desenvolver modelos teóricos de stress ocupacional.
?
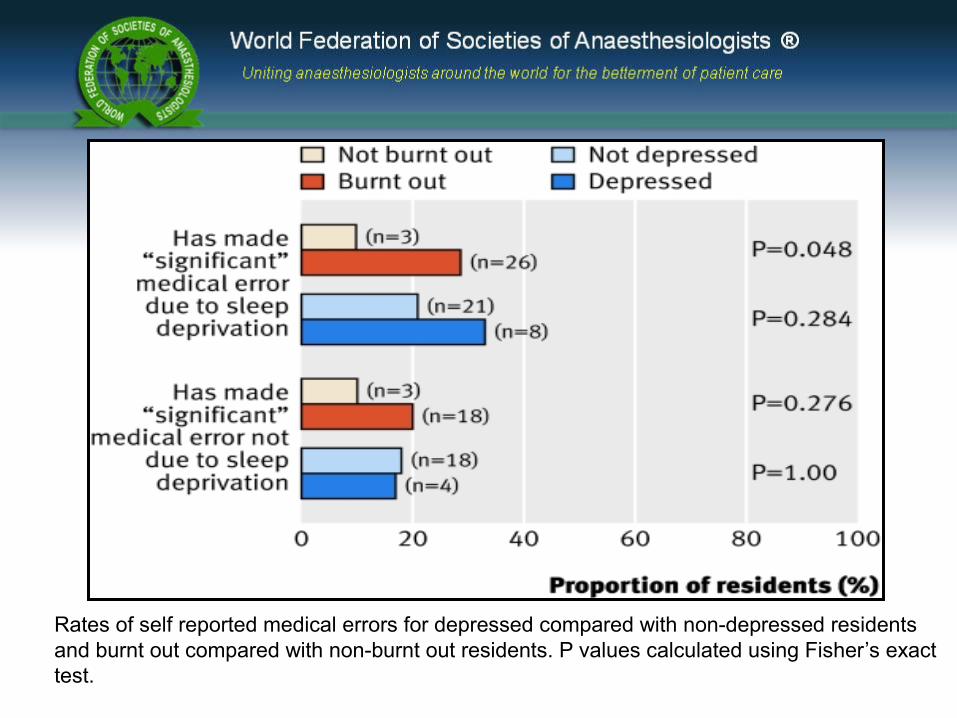
Rates of self reported medical errors for depressed compared with non-depressed residents and burnt out compared with non-burnt out residents. P values calculated using Fisher’s exact test.
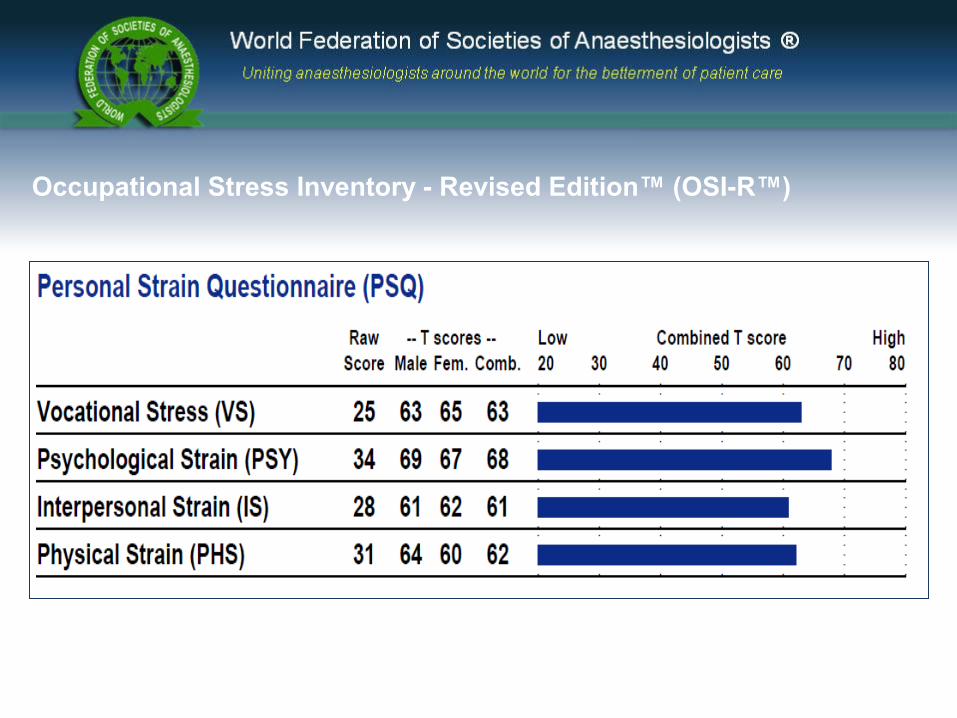
Occupational Stress Inventory - Revised Edition™ (OSI-R™)
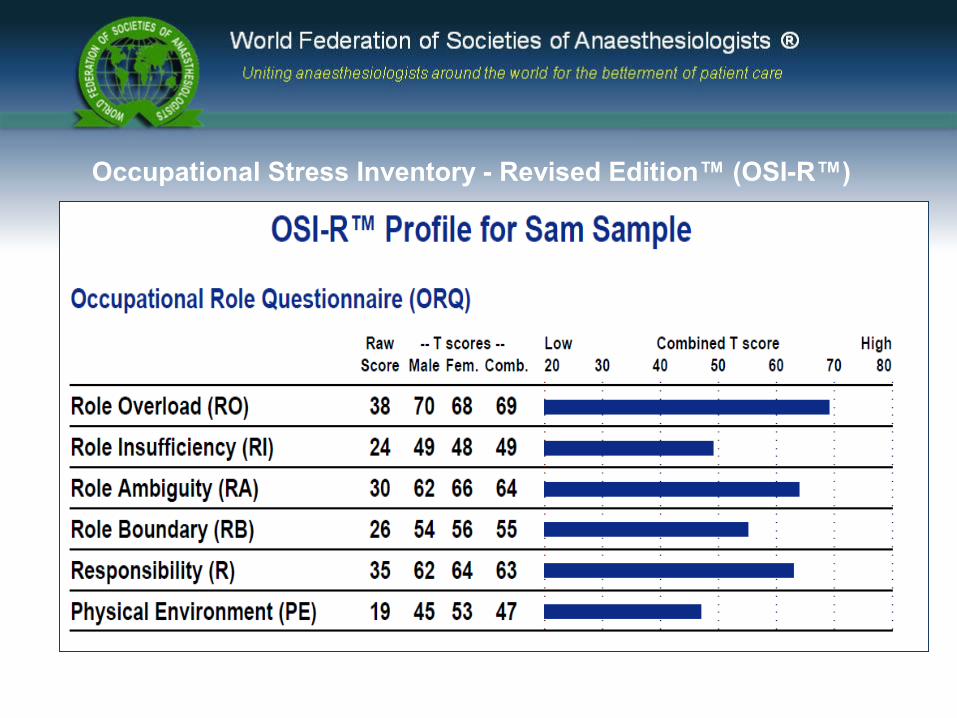
Occupational Stress Inventory - Revised Edition™ (OSI-R™)
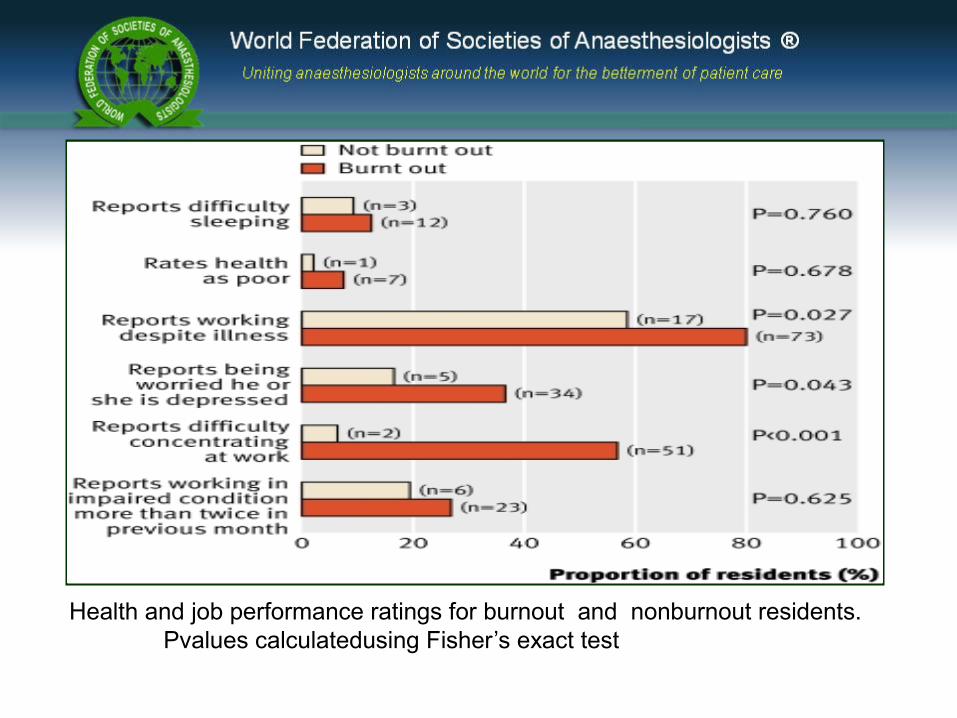
Health and job performance ratings for burnout and nonburnout residents.Pvalues calculatedusing Fisher’s exact test
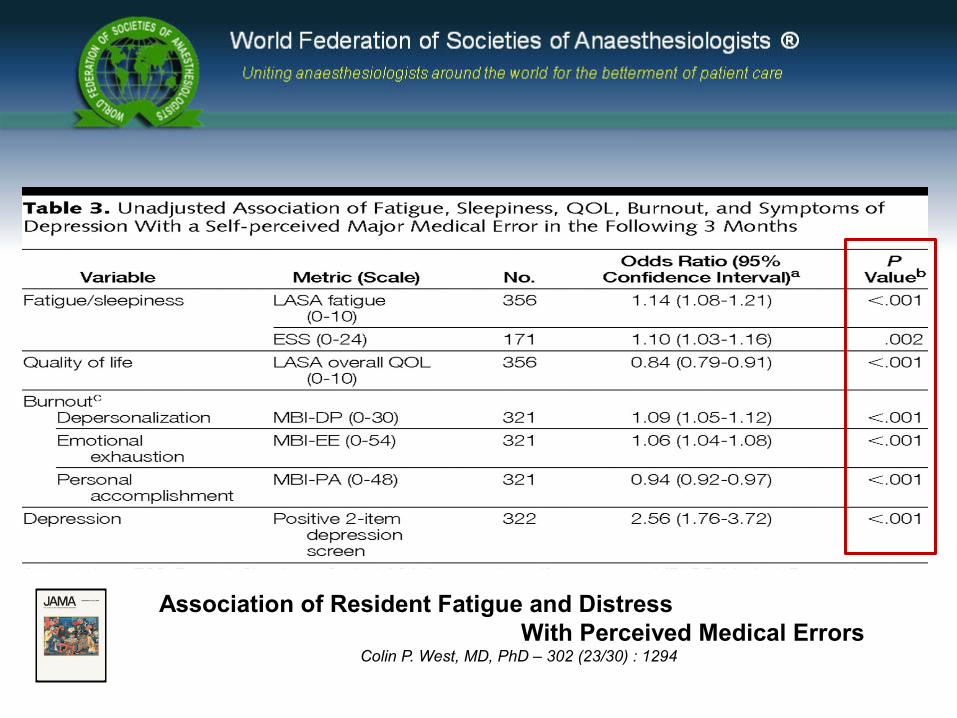
Association of Resident Fatigue and Distress With Perceived Medical Errors Colin P. West, MD, PhD – 302 (23/30) : 1294
FIRST OF ALL :
“ is necessary to understanding the problem with great profundity ”
Conceito de “ESTRESSE”
" é
É complexo com múltiplos aspectos.
Os primeiros estudos foram especificamente baseados em dados fisiológicos
NÃO VALORIZAVAM O ESTRESSE PSICOGÊNICO
WHAT IS ALREADY KNOWN ON THIS TOPIC
Depression and burnout are highly prevalent in doctors in training.
Burnout is associated with a higher rate of self reported errors among residents.
WHAT THIS STUDY ADDS
Depressed residents in paediatrics were more than six timesas likely to make errors in medication as their rnon-depressed colleagues
Burnout did not seem to be associated with higher rates of medication errors














![VFD-F Series - MEP USER MANUAL.pdf · [11.81] 330.0 [12.99] 688.3 [27.10] 275.0 [10.83] 370.0 [14.57] 715.8 [28.18] 300.0 [11.81] 420.0 [12.54] Unit: mm [inch] 02 - Comparison of](https://img.pdfslide.us/doc/110x75/604d47655cd63b31d17dbfdf/vfd-f-series-mep-user-1181-3300-1299-6883-2710-2750-1083-3700.jpg)











![14.46 [367.30mm] 34.92 [887.01mm] 26.77 [680.00mm] 5.91 ... · Roll ±3° ilt +15 / -5 MAX:27.56" [700.00mm] MIN:11.81"[300.00MM] MAX:31.50" [800.00mm] MIN:15.75"[400.00MM] 26.48"](https://img.pdfslide.us/doc/110x75/60830f4b5c9f19005830f437/1446-36730mm-3492-88701mm-2677-68000mm-591-roll-3-ilt-15-.jpg)


