Embed Size (px)
Citation preview
Centre for Reviews and Dissemination
Who we are what we do and why it matters
Lesley StewartUniversity of York Council
13th June 2008
CRD
• Established 1994 by NHS R&D
• Part of NIHR
• Academic department of University of York
• 100% research activity
• 53 staff
• 29 research (25 fte)
• National & international relevance & collaboration
What we doCRD Aim
Be an international centre of excellence in evidence synthesis that produces high-quality research evidence and promotes the use of research evidence in health policy and practice
generate knowledge through evaluation of health research transfer of knowledge to policy and practice improve health and health care
Main objectives
• Systematic reviews evaluating important health and public health questions
• Research and develop methods
• Databases of worldwide evidence from SR & economic evaluation
• Guidance, information, advice to DH, NIHR, NHS
Systematic review
• Health decisions should be based on best research evidence
• Systematic reviews provide best evidence by objective assembly, assessment and summary of research findings
• Systematic methodology & transparent process• Locating evidence• Evaluating evidence• Synthesising the evidence • (quantitative meta-analysis)
• Systematic reviews help practitioners and patients make informed choices about healthcare and provide best evidence of effectiveness for developing health policy and clinical guidelines
Why we need systematic reviews
Synthesis
• Reliable summary of otherwise unmanageable amounts of evidence
Totality of evidence
• Evaluation & recommendation should be based on results of all trials
Power and Precision
• Expected benefits of new treatment often moderate
• Trials recruit too few patients to detect such differences reliably
• Combining results of individual trials in meta-analysis may give sufficient numbers (power) for reliable answers
Example
Pre-eclampsia
• Complicates 2-8% of pregnancies, risks for mother & baby
• ~50,000 deaths p.a. (99% of these in low resource settings)
• PARIS international collaborative project initiated to • Assess whether antiplatelet agents reduce PE• Explore which women benefit more
• Data from 31 RCTs, 32,217 women
Lancet 2007 369: 1791 – 1798
DOI: 10.1016/S0140-6736(07)60712-0
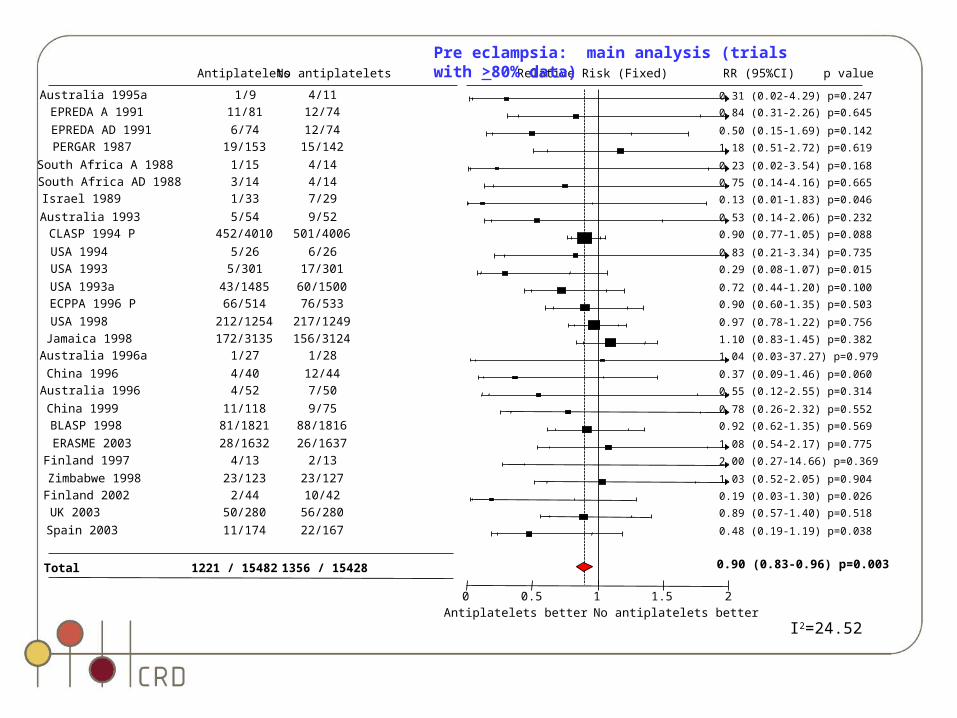
Australia 1995a 1/9 4/11
EPREDA A 1991 11/81 12/74
EPREDA AD 1991 6/74 12/74
PERGAR 1987 19/153 15/142
South Africa A 1988 1/15 4/14
South Africa AD 1988 3/14 4/14
Israel 1989 1/33 7/29
Australia 1993 5/54 9/52
CLASP 1994 P 452/4010 501/4006
USA 1994 5/26 6/26
USA 1993 5/301 17/301
USA 1993a 43/1485 60/1500
ECPPA 1996 P 66/514 76/533
USA 1998 212/1254 217/1249
Jamaica 1998 172/3135 156/3124
Australia 1996a 1/27 1/28
China 1996 4/40 12/44
Australia 1996 4/52 7/50
China 1999 11/118 9/75
BLASP 1998 81/1821 88/1816
ERASME 2003 28/1632 26/1637
Finland 1997 4/13 2/13
Zimbabwe 1998 23/123 23/127
Finland 2002 2/44 10/42
UK 2003 50/280 56/280
Spain 2003 11/174 22/167
Total 1221 / 15482 1356 / 15428
Antiplatelets No antiplatelets Relative Risk (Fixed) RR (95%CI) p value
Antiplatelets better No antiplatelets better0 1 20.5 1.5
0.31 (0.02-4.29) p=0.247
0.84 (0.31-2.26) p=0.645
0.50 (0.15-1.69) p=0.142
1.18 (0.51-2.72) p=0.619
0.23 (0.02-3.54) p=0.168
0.75 (0.14-4.16) p=0.665
0.13 (0.01-1.83) p=0.046
0.53 (0.14-2.06) p=0.232
0.90 (0.77-1.05) p=0.088
0.83 (0.21-3.34) p=0.735
0.29 (0.08-1.07) p=0.015
0.72 (0.44-1.20) p=0.100
0.90 (0.60-1.35) p=0.503
0.97 (0.78-1.22) p=0.756
1.10 (0.83-1.45) p=0.382
1.04 (0.03-37.27) p=0.979
0.37 (0.09-1.46) p=0.060
0.55 (0.12-2.55) p=0.314
0.78 (0.26-2.32) p=0.552
0.92 (0.62-1.35) p=0.569
1.08 (0.54-2.17) p=0.775
2.00 (0.27-14.66) p=0.369
1.03 (0.52-2.05) p=0.904
0.19 (0.03-1.30) p=0.026
0.89 (0.57-1.40) p=0.518
0.48 (0.19-1.19) p=0.038
0.90 (0.83-0.96) p=0.003
Pre eclampsia: main analysis (trials with >80% data)
I2=24.52
CRD systematic reviews• Wide range of topics on important health and public health issues spanning
therapy, diagnosis, prognosis
• drug interventions: cancer, coronary syndromes, ADHD• surgical interventions: haemorrhoids, aortic aneurysms• diagnostic interventions: UTI, neuro- imaging, FOB screening• behavioural interventions: CSF/ME, people bereaved by suicide • delivery and organisation of care: self care support networks• policy interventions: tobacco control, organ donation (57 completed since 2003)
• Many have direct link to policy e.g NICE , DH Policy Research Programme, National Cancer Guidance, NHS Cancer Screening Programmes
• Disseminated widely
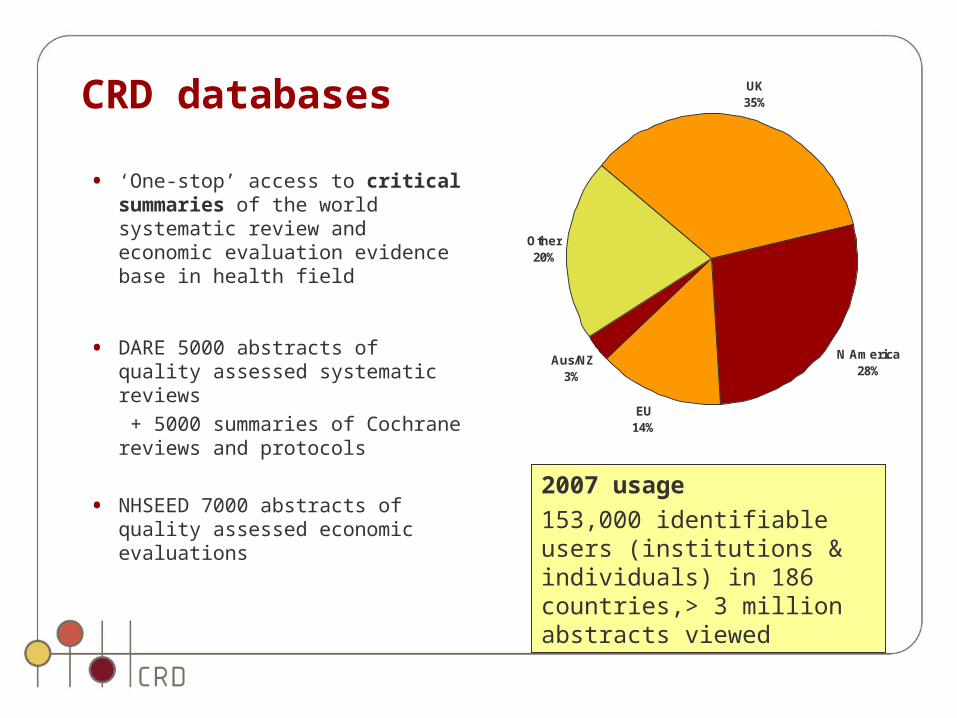
CRD databases
• ‘One-stop’ access to critical summaries of the world systematic review and economic evaluation evidence base in health field
• DARE 5000 abstracts of quality assessed systematic reviews
+ 5000 summaries of Cochrane reviews and protocols
• NHSEED 7000 abstracts of quality assessed economic evaluations
UK35%
N America28%
EU14%
Aus/NZ3%
Other20%
2007 usage
153,000 identifiable users (institutions & individuals) in 186 countries,> 3 million abstracts viewed
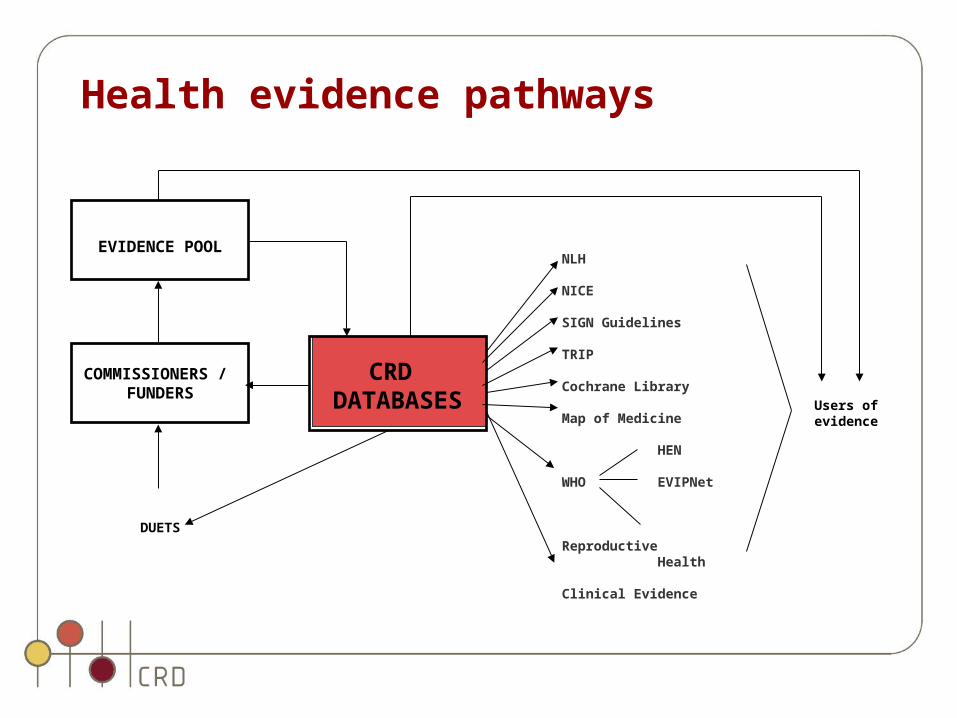
EVIDENCE POOL
COMMISSIONERS / FUNDERS
DUETS
CRD DATABASES
NLH NICE SIGN Guidelines TRIP Cochrane Library Map of Medicine
HEN WHO EVIPNet Reproductive Health Clinical Evidence
Users of evidence
Health evidence pathways
Methods development• R&D of methods important part of CRD role
• information retrieval• synthesis• dissemination
• E.g. avoidance of bias, methods for review of diagnostic test accuracy studies, public health, narrative synthesis
• PhD fellowships• Information retrieval of adverse events• ? IPD prognostic models
• CRD publish internationally recommended guidance on undertaking systematic reviews (30,000 downloads annually) 3rd edition publication date September 2008
CRD research
• informs real health decisions, impacts on policy and practice, improves health
Best Research for Best Health
• CRD named as a ‘key plank’ of the new national health research strategy
Lancet Editorial July 2006
• NHS R&D’s most important contribution to the UK science base is building systematic review capacity
Further information: http://www.york.ac.uk/inst/crd/