Embed Size (px)
Citation preview
CRITICAL CARE: CARDIOVASCULAR FOCUS 0195-5616/01 $15.00 + .00
CENTRAL VENOUS PRESSURE AND ARTERIAL BLOOD
PRESSURE MEASUREMENTS
Armelle M. de Laforcade, DVM, and Elizabeth A Rozanski, DVM
In critically ill animals, evaluation of central venous pressure (CVP) and arterial blood pressure (BP) provide valuable information to help assess the patient. In particular, CVP may be used to judge the volume status of the pet, and measurement of BP is essential in determining whether perfusion to vital tissues is adequate and in evaluating the risk of negative outcome.
The goals of this article are to review the determinants of CVP and BP, to evaluate different measurement techniques available clinically, and to review clinical guidelines concerning CVP and BP as they apply to the management of critically ill dogs and cats.
CENTRAL VENOUS PRESSURE
Determinants of Central Venous Pressure
CVP is a measure of the hydrostatic pressure within the intrathoracic vena cava.1' 13, 17' 18 As long as no vascular obstruction exists, CVP is reflective of right atrial pressure (RAP). As a measure of RAP, CVP provides information concerning the adequacy of venous blood volume (or preload). CVP is also affected by cardiac output (CO). A low CVP may be indicative of low CO as a result of the effects of hypovolemia, and a high CVP accompanied by low CO suggest heart failure. In
From the Section of Intensive Care, Department of Clinical Sciences, Tufts University School of Veterinary Medicine, North Grafton, Massachusetts
VETERINARY CLINICS OF NORTH AMERICA: SMALL ANlMAL PRACTICE
VOLUME 31 • NUMBER 6 • NOVEMBER 2001 1163
1164 de LAFORCADE & ROZANSKI
addition, CVP measurements provide early evidence of the patient at risk of volume overload, recurrent pericardia! effusion, or right-sided heart failure. CVP may not be considered a substitute for measurement of pulmonary capillary wedge pressure (PCWP), which is considered a reflection of left atrial pressure.6 PCWP measurements are considered more accurate in evaluating a patient for left-sided congestive heart failure, because measurements of greater than 18 mm Hg are indicative of left atrial volume overload. PCWP measurements are technically challenging, expensive, and not commonly performed in animals. Conversely, CVP measurements are technically simple and frequently considered mandatory in critically ill patients where concerns exist with regard to fluid therapy.
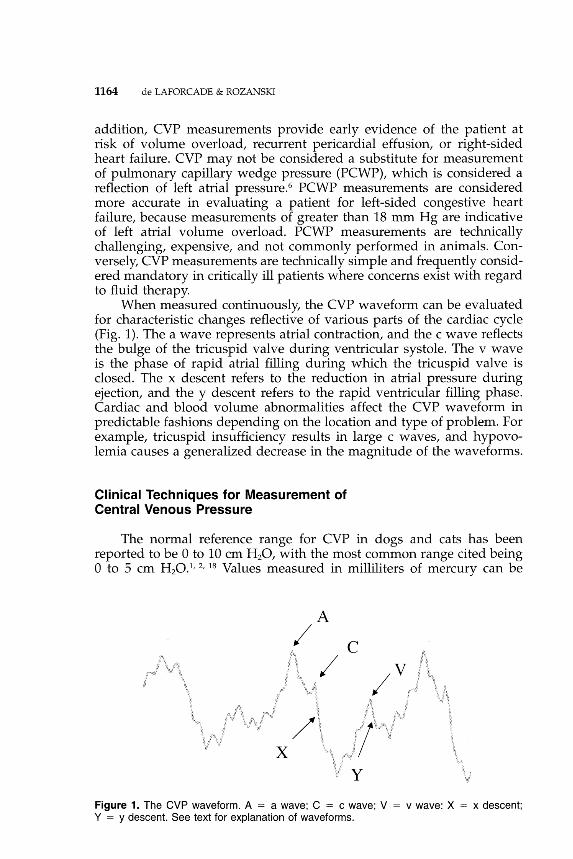
When measured continuously, the CVP waveform can be evaluated for characteristic changes reflective of various parts of the cardiac cycle (Fig. 1). The a wave represents atrial contraction, and the c wave reflects the bulge of the tricuspid valve during ventricular systole. The v wave is the phase of rapid atrial filling during which the tricuspid valve is closed. The x descent refers to the reduction in atrial pressure during ejection, and the y descent refers to the rapid ventricular filling phase. Cardiac and blood volume abnormalities affect the CVP waveform in predictable fashions depending on the location and type of problem. For example, tricuspid insufficiency results in large c waves, and hypovolemia causes a generalized decrease in the magnitude of the waveforms.
Clinical Techniques for Measurement of Central Venous Pressure
The normal reference range for CVP in dogs and cats has been reported to be 0 to 10 em H 20, with the most common range cited being 0 to 5 em H20.1' z, 18 Values measured in milliliters of mercury can be
A
/
X
Figure 1. The CVP waveform. A = a wave; C = c wave; V = v wave: X = x descent; Y = y descent. See text for explanation of waveforms.
CENTRAL VENOUS AND ARTERIAL BLOOD PRESSURE MEASUREMENTS 1165
converted to centimeters of water by multiplying by a factor of 1.36 (e.g., 4 mm Hg = 5.4 em H20). Values of less than 0 em H20 are indicative of hypovolemia, and values of greater than 12 to 15 em H20 are suggestive of volume overload. Additionally, trends in the CVP over time may provide vital information about an individual patient. For example, for a dog with oliguric renal failure, when CVP values that have been steady at 6 to 7 em H20 for 3 days suddenly decrease to 0 em H 20, the dog may be developing hypovolemia, perhaps secondary to newly developing polyuria. Similarly, a gradual CVP rise to 12 em H20 in a cat receiving intravenous fluids for vomiting and anorexia may be a warning sign of impending volume overload. CVP is lowest at the beginning of inspiration and higher during expiration. Ideally, CVP measurements are made at the end of expiration during the lowest diastolic swing of the waveform.10 Predictably, in animals receiving positive-pressure ventilation, the CVP is highest during the inspiratory phase and lowest at the end of expiration. Additionally, animals receiving positive end-expiratory-pressure ventilation have an increased CVP.12
CVP may be estimated or directly measured. Estimates of CVP may be made through direct visualization of the jugular vein. In a patient with volume overload, pericardia! effusion, or another cause of rightsided heart failure, the jugular vein may seem to be distended and pulsation may be visible. Jugular venous distention is useful as an adjunctive method of assessing CVP, but it does not provide an objective value, and evaluation by different observers or after interventions (e.g., treatment with furosemide) may result in significant differences. Similarly, values for peripheral venous pressure have some correlation with CVP, but variations in venous capacitance and site of measurement make any physiologic correlation clinically irrelevant. Finally, clinicians should recall that peripheral venous distention has no correlation to systemic arterial BP and that animals positioned in lateral recumbency have jugular veins that seem to be distended.
CVP may also be measured using either a water manometer or a pressure transducer. 13 Direct measurements of CVP require the placement of a central venous catheter. The CVP catheter should be placed via either the jugular vein, the femoral vein, or the saphenous vein. The tip of the catheter should be at the level of the junction of the right atrium (for the jugular catheter) or caudal vena cava (when a hind limb vessel is used). 13• 17 Placement of central venous catheters may be technically challenging; thus, familiarity with equipment and techniques is useful. In our hospital, a commercially available through-the-needle catheter (Intracatheter; Becton Dickinson Vascular Access, Sandy, UT} is most commonly used. The jugular vein is most frequently used for central venous catheter placement because it is often the largest and most accessible vein. It is also much less likely to become soiled in the recumbent pet or to be prematurely removed by the patient. In feline patients, the femoral vein is also commonly usedP Potential catheterrelated sources of error include kinking of the catheter either at the site
1166 de LAFORCADE & ROZANSKI
of vein entry or within the lumen, inadvertent catheterization of another vein (e.g., azygous), occlusion by the vessel wall, and formation of venous thrombi surrounding the catheter. All catheters used for CVP determinations should freely "bleed back" and flush easily. Additionally, in any catheter where placement is considered questionable, a thoracic radiograph may be used to document the site of the distal tip.
Direct measurement of the CVP may be made with either a water manometer or through the use of an electronic pressure transducer system. Measurement with a water manometer has been widely used in veterinary medicine.13 Supplies needed for this system include a central venous catheter, a water manometer (CVP manometer; Abbott Laboratories, West Chicago, IL), extension tubing, a three-way stopcock, and a syringe filled with 20 to 30 mL of heparinized saline. The patient should be placed in sternal or, ideally, lateral recumbency. The position chosen should be recorded in the patient's medical record. A reference point that correlates with the right atrium should be determined. The right atrium for the patient in lateral recumbency is approximately at the level of the manubrium, and the scapulohumeral joint is the recommended reference point for the patient in sternal recumbency. This "zero" point should be recorded. Clinically, the manometer is often taped to the cage to simplify repeated measurement over time with the patient in the same position. The manometer is connected to the patient, filled with saline, and then allowed to equilibrate. The level of the fluid (at the bottom of the meniscus) on the manometer correlates with the CVP of the patient. The value should be recorded, and measurements should be repeated periodically to follow trends.
An electronic pressure transducer system may also be used to monitor CVP.13 Supplies needed for this system include the central venous catheter, a nondistendible extension set, the pressure transducer, and the electronic measuring system. The pressure transducer is placed at a set point equivalent to RAP (as with the water manometer system) and calibrated. This may be done electronically or with the aid of a mercury manometer depending on the system used. The extension set is connected to the central venous catheter and to the transducer. The electronic display correlates to the CVP. This technique allows CVP waveforms to be observed and recorded. Electronic measurement allows for continuous CVP measurement, and after it is properly set up, this system is much less time-consuming to use.
Clinical Guidelines for the Use of Central Venous Pressure
Measurement of CVP is particularly useful in helping to guide fluid therapy in dogs and cats. In general, the CVP is clinically useful in management of the hypovolemic patient and the patient considered at risk for volume overload. In hypovolemic shock, the CVP is low as a result of reduced effective circulating blood volume. Hypovolemic shock
CENTRAL VENOUS AND ARTERIAL BLOOD PRESSURE MEASUREMENTS 1167
in dogs is commonly caused by trauma, gastric dilatation-volvulus syndrome, and hemorrhage caused by abdominal neoplasia. Hypovolemic shock may be detected clinically by the presence of tachycardia, pale mucous membrane color, weakness, and depression. In these animals, initial therapy should include rapid volume expansion through largebore peripheral catheters. After fluid resuscitation is begun, placement of a central catheter is useful to monitor the CVP throughout resuscitation. The initial CVP is frequently less than 0 em H20. A fluid challenge may be performed in which a bolus of either a crystalloid (20 mL/kg) or a colloid (5 mL/kg) solution is rapidly given over 3 to 5 minutes and its effect on the CVP is recorded. If the bolus does not result in an increase of CVP of at least 2 to 4 em H20, fluid therapy should be continued at a high rate (60-90 mL/kg/hr of crystalloids) until the CVP is increased to at least 5 em H20. If the CVP is being electronically monitored, the fluid bolus may be continued until a rise of 3 to 5 mm Hg is detected and then carefully monitored to maintain fluid infusions up to a point where the CVP is considered optimal (usually 7-10 em HzO)Y
In the patient considered at risk of volume overload, the CVP may also be considered a valuable monitoring tool. Animals con~idered at particular risk of volume overload include dogs and cats with preexisting heart disease that require intravenous fluid therapy for management of another condition and animals undergoing diuresis for renal failure. Any patient (particularly cats) may develop volume overload after being treated with greater than maintenance volumes of intravenous fluids for more than 2 to 3 days. In this group of animals, measurement of the CVP two to four times a day should provide early evidence of impending volume overload.
ARTERIAL BLOOD PRESSURE MEASUREMENT
Determinants of Arterial Blood Pressure
Arterial blood pressure (BP) is defined as the force exerted by flowing blood on the vessel walls. 15 Determinants of BP reflect the relation to the cardiovascular system as described by the equation:
BP =CO X PR
where CO is cardiac output and PR is peripheral resistance. CO can be described as the product between heart rate and stroke volume. Stroke volume, or the amount of blood ejected with each ventricular contraction, is influenced by cardiac contractility, preload, and afterload. Although CO plays an important role in BP during exercise, PR is the major determinant at rest. Arterial resistance is controlled by many factors, including sympathetic stimulation, the renin-angiotensin system, and renal regulation of blood volume. BP is tightly controlled in animals, because the cardiovascular system maintains adequate BP at all costs. In
1168 de LAFORCADE & ROZANSKI
situations of decreased BP, compensatory attempts to maintain BP include vasoconstriction and tachycardia. The baroreceptors located in the walls of the carotid sinus and aortic arch send signals to the vasomotor center in the brain stem. A fall in BP leads to increased sympathetic efferent impulses, causing vasoconstriction, increased heart rate, and, ultimately, increased BP. Sympathetic stimulation ("flight or fight" response) results in direct vasoconstriction and subsequent increases in systemic BP.
In addition, hormonal mechanisms are important in long-term (days to weeks) BP control.15 In response to decreased renal perfusion, renin produced by the juxtaglomerular cells in the afferent artery of the renal vasculature catalyzes the transition of angiotensinogen to angiotensin I. Angiotensin-converting enzyme located in the lung then converts angiotensin I to angiotensin II. In addition to its potent vasoconstrictor effects, angiotensin II stimulates the adrenal cortex to release aldosterone, which increases blood volume (and preload) through sodium retention.
Terminology
The information gathered through arterial BP measurement must be correctly interpreted for appropriate decisions to be made.15 Systolic BP is the pressure exerted against the blood vessel walls during systole, or ventricular contraction. Diastolic BP is the pressure exerted during diastole, or the relaxation phase of the cardiac cycle. Because the duration of diastole is longer than that of systole, the mean arterial pressure (MAP), or the average pressure exerted during the cardiac cycle, is calculated as follows:
MAP = (Systolic - Diastolic) I 3 + Diastolic
The systolic pressure minus the diastolic pressure is termed the pulse pressure and is considered the major determinant of palpable pulse strength. The physical examination finding of hyperkinetic (or bounding) pulses is the result of a widening of pulse pressure from either an elevated systolic pressure or a depressed diastolic pressure. Causes include cardiovascular disorders such as patent ductus arteriosus and aortic insufficiency. Other common causes of hyperkinetic pulses include anemia with associated hypovolemia. Palpably weak pulses (hypokinetic) are indicative of reduced pulse pressure. Causes of decreased systolic pressure include volume depletion as well as other causes of reduced CO (e.g., aortic stenosis). Pulses in dogs and cats are best appreciated by palpation of the femoral artery, although a pulse can also be palpated from other arteries, including the dorsal pedal artery, the brachial artery, and, in anesthetized patients, the lingual artery.
CENTRAL VENOUS AND ARTERIAL BLOOD PRESSURE MEASUREMENTS 1169
Clinical Techniques for the Measurement of Blood Pressure
BP may be measured either directly via an indwelling arterial catheter or indirectly through a variety of techniques. The direct measurement of BP is considered the gold standard.
Direct Blood Pressure Measurement
Direct arterial pressure is measured by placing a catheter directly into an artery and connecting the catheter to an electronic pressure transducer. Direct arterial pressure monitoring allows for continuous BP measurement and provides easy access to arterial blood samples for blood gas analysis.
Arterial catheter placement is most commonly achieved using the dorsal pedal artery or, in small dogs and cats, the femoral artery (Fig. 2). Any palpable peripheral artery can be used, however. A 20- to 24-gauge over-the-needle catheter can be used depending on the size of the artery. A sterile preparation is performed over the site of catheterization. The catheter is placed using a technique similar to that used when placing a venous catheter. Most operators find the initial placement of an arterial catheter to be more challenging than that of a venous catheter. With experience, arterial catheter placement becomes routine. Many clinicians have found placement initially easier in large-breed anesthetized dogs. The catheter is then flushed with heparinized saline and capped. Once the catheter is in place, it can be connected using extension tubing to a transducer, which displays the pressure waveform. Although some monitors estimate and display systolic, diastolic, and mean pressures, others provide a scale next to the waveform from which the systolic and diastolic pressures can be estimated.
Disadvantages include the need for specific technical skill, invasive nature of the procedure, cost of equipment, and need for maintenance of the catheter with frequent heparinization. Arterial catheterization also carries the risk of thrombosis and infection.9 In the patient with lifethreatening hypotension or hypertension, however, direct BP determination is considered mandatory.
Indirect Blood Pressure Measurement
Several methods of indirect BP measurement are available.H, 7' 10, n, 19
All indirect BP measurement techniques are based on detection of blood flow beneath an inflated cuff. In general, indirect measurement techniques are noninvasive and require less technical expertise. Disadvantages of these techniques involve less accurate measurements during hypotensive states or severe vasoconstriction.
Doppler Ultrasonography. The Doppler flow method involves a small ultrasound probe placed on a peripheral artery (generally the dorsal pedal) (Fig. 3). The ultrasound probe contains a piezoelectric
1170 de LAFORCADE & ROZANSKI
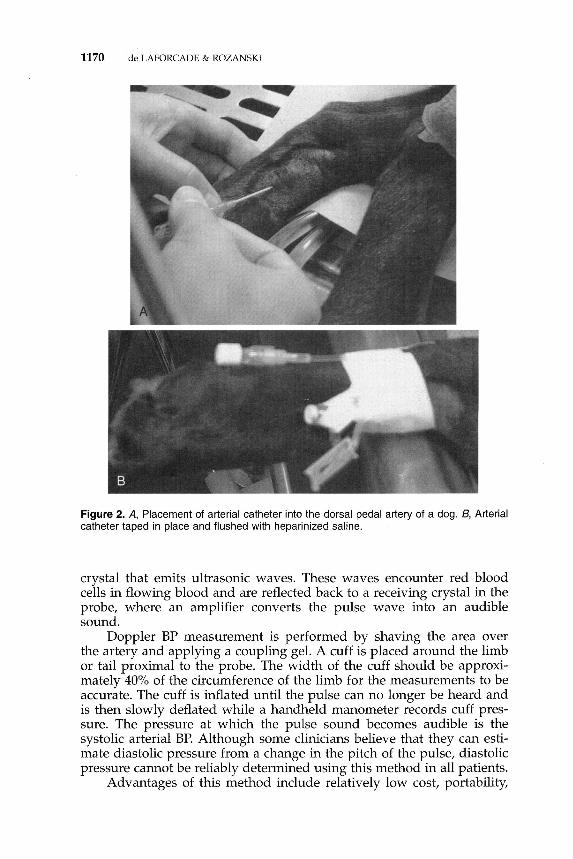
Figure 2. A, Placement of arterial catheter into the dorsal pedal artery of a dog. 8 , Arterial catheter taped in place and flushed with heparinized saline.
crystal that emits ultrasonic waves. These waves encounter red blood cells in flowing blood and are reflected back to a receiving crystal in the probe, where an amplifier converts the pulse wave into an audible sound.
Doppler BP measurement is performed by shaving the area over the artery and applying a coupling gel. A cuff is placed around the limb or tail proximal to the probe. The width of the cuff should be approximately 40% of the circumference of the limb for the measurements to be accurate. The cuff is inflated until the pulse can no longer be heard and is then slowly deflated while a handheld manometer records cuff pressure. The pressure at which the pulse sound becomes audible is the systolic arterial BP. Although some clinicians believe that they can estimate diastolic pressure from a change in the pitch of the pulse, diastolic pressure cannot be reliably determined using this method in all patients.
Advantages of this method include relatively low cost, portability,
CENTRAL VENOUS AND ARTERIAL BLOOD PRESSURE MEASUREMENTS 1171
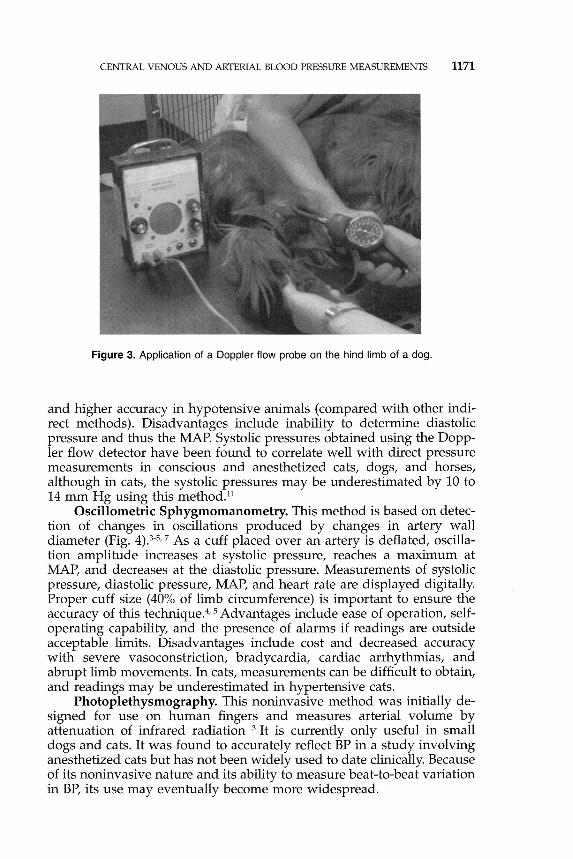
Figure 3. Application of a Doppler flow probe on the hind limb of a dog.
and higher accuracy in hypotensive animals (compared with other indirect methods). Disadvantages include inability to determine diastolic pressure and thus the MAP. Systolic pressures obtained using the Doppler flow detector have been found to correlate well with direct pressure measurements in conscious and anesthetized cats, dogs, and horses, although in cats, the systolic pressures may be underestimated by 10 to 14 mm Hg using this method.l1
Oscillometric Sphygmomanometry. This method is based on detection of changes in oscillations produced by changes in artery wall diameter (Fig. 4).3-5• 7 As a cuff placed over an artery is deflated, oscillation amplitude increases at systolic pressure, reaches a maximum at MAP, and decreases at the diastolic pressure. Measurements of systolic pressure, diastolic pressure, MAP, and heart rate are displayed digitally. Proper cuff size (40% of limb circumference) is important to ensure the accuracy of this technique.4• 5 Advantages include ease of operation, selfoperating capability, and the presence of alarms if readings are outside acceptable limits. Disadvantages include cost and decreased accuracy with severe vasoconstriction, bradycardia, cardiac arrhythmias, and abrupt limb movements. In cats, measurements can be difficult to obtain, and readings may be underestimated in hypertensive cats.
Photoplethysmography. This noninvasive method was initially designed for use on human fingers and measures arterial volume by attenuation of infrared radiation 3 It is currently only useful in small dogs and cats. It was found to accurately reflect BP in a study involving anesthetized cats but has not been widely used to date clinically. Because of its noninvasive nature and its ability to measure beat-to-beat variation in BP, its use may eventually become more widespread.

1172 de LAFORCADE & ROZANSKI
Figure 4. Application of an oscillometric blood pressure monitor on the hind limb of a dog.
Clinical Guidelines for Blood Pressure Monitoring
Hypotension
Hypotension can be defined as a MAP less than 60 mm H g, which is the minimum pressure required to maintain adequate perfusion to the brain and kidneys.21 Causes of hypotension include hypovolemia secondary to dehydration or blood loss, sepsis, bradycardia or other arrhythmias, or cardiovascular depression caused by anesthetic medications. The first step in the treatment of hypotension is to remove the underlying cause if one can be identified. Additionally, volume support with crystalloids, colloids, or blood products may be used. Adequacy of volume replacement may be monitored with CVP measurements. Finally, if adequate intravascular volume is present but hypotension persists, therapy with a vasopressor or positive inotrope may be considered (e.g., dopamine, dobutamine). If untreated, hypotension results in death.
Hypertension
Hypertension has been defined by various authors as a MAP greater than 145 mm Hg.16• 20 Hypertension may be triggered by hyperthyroidism, renal disease, or neoplasia as well as by a variety of other causes.
CENTRAL VENOUS AND ARTERIAL BLOOD PRESSURE MEASUREMENTS 1173
Primary essential hypertension is rare in dogs and cats. Hypertension may also be caused by the "white coat" effect, where normal animals may have dramatic increases in their BP when brought inside the veterinary hospital.14 Treatment of hypertension involves removal of the underlying cause if possible. Long-term sequelae of untreated hypertension may include retinal detachment, left ventricular hypertrophy, kidney failure, and cerebral vascular accidents.16• 20 Several drugs are used to control hypertension in cats and dogs. These include amlodipine, enalapril, hydralazine, and, in acute situations, nitroprusside.8• 20 Amlodipine is a calcium channel antagonist with good vascular effects. It has been widely used in cats with hypertension.20 Enalapril is an angiotensinconverting enzyme inhibitor that prevents the formation of angiotensin II (a potent vasoconstrictor). Enalapril causes decreases in PR and MAP. Other effects such as reduced RAP, PCWP, and CO make it useful for the treatment of heart failure in addition to the treatment of hypertension. Hydralazine is a phthalazine derivative that acts directly on vascular smooth muscle to reduce PR and BP by interfering with calcium movement and preventing vascular contraction. Hydralazine has a greater effect on arteries than on veins and is used for the treatment of congestive heart failure and occasionally for systemic hypertension. Sodium nitroprusside is a balanced vasodilator that is used in the setting of an acute hypertensive crisis. Nitroprusside rapidly decreases BP and PR through the effects of nitric oxide. Nitroprusside use is restricted to hospitals with 24-hour monitoring and experience with vasoactive substances.
CONCLUSIONS
The routine use of CVP monitoring in the critically ill animal can provide the clinician with a better knowledge base about intravascular volume status, which can improve ability to tailor fluid . therapy to an individual patient. Measurement of the BP can help to ensure that hypotension is addressed early and that the long-term complications of hypertension are avoided or minimized.
References
1. Aldrich J, Haskins S: Monitoring the critically ill patient. In Bonagura JD, Kirk RW (eds): Current Veterinary Therapy, vol XII. Philadelphia, WB Saunders, 1995, pp 98-105
2. Bell FW, Osborne CA: Maintenance fluid therapy. In Kirk RW, Bonagura JD (eds): Current Veterinary Therapy, vol X. Philadelphia, WB Saunders, 1989, pp 37-43
3. Binns SH, Sisson DD, Buoscio DA, et a!: Doppler ultrasonographic, oscillometric sphygmomanometric, and photoplethysmographic techniques for non-invasive blood pressure measurement in anesthetized cats. J Vet Intern Med 9:405-414, 1995
4. Bodey AR, Young LE, Bartram DH, et al: A comparison of direct and indirect (oscillometric) measurements of arterial blood pressure in anaesthetised dogs using tail and limb cuffs. Res Vet Sci 57:265-269, 1994
1174 de LAFORCADE & ROZANSKI
5. Bodey AR, Michell AR, Bovee KC, et al: Comparison of direct and indirect (oscillometric) measurements of arterial blood pressure in conscious dogs. Res Vet Sci 61:17-21, 1996
6. Bolte AC, Decker GA, van Eyck J, et al: Lack of agreement between central venous pressure and pulmonary capillary wedge pressure in preeclampsia. Hypertension and Pregnancy 19:261-271, 2000
7. Branson KR, Wagner-Mann CC, Mann FA: Evaluation of an oscillometric blood pressure monitor on anesthetized cats and the effect of cuff placement and fur on accuracy. Vet Surg 26:347-353, 1997
8. Brown SA, Henik RA: Diagnosis and treatment of systemic hypertension. Vet Clin North Am Small Anim Pract 28:1481-1494, 1998
9. Burrows CF: Techniques and complications of intravenous and intraarterial catheterization in dogs and cats. JAm Anim Hosp Assoc 163:1357-1363, 1973
10. Clayton DG: Inaccuracies in manometric central venous pressure measurement. Resuscitation 16:221-230, 1988
11. Grandy JL, Dunlop CI, Hodgson DS, et al: Evaluation of the Doppler ultrasonic method of measuring systolic arterial blood pressure in cats. Am J Vet Res 53:1166-1169, 1992
12. Halck SW, Walther-Larsen S, Sanchez R: Measurement of central venous pressure after open heart surgery and effect of positive end expiratory pressure. Dan Med Bull 38:181-182, 1991
13. Hansen BD: Technical aspects of fluid therapy. Catheters and monitoring of fluid therapy. In DiBartola SP (ed): Fluid Therapy in Small Animal Practice. Philadelphia, WB Saunders, 1992, pp 341-370
14. Kallet AJ, Cowgill LD, Kass PH: Comparison of blood pressure measurements obtained in dogs by the use of indirect oscillometry in a veterinary clinic versus at home. JAVMA 210:651-654, 1997
15. Kittleson MD, Olivier NB: Measurement of systemic arterial blood pressure. Vet Clin North Am Small Anim Pract 13:321-336, 1983
16. Littman MP: Spontaneous systemic hypertension in 24 cats. J Vet Intern Med 8:79-86, 1994
17. Machon RG, Raffe MR, Robinson EP: Central venous pressure measurements in the caudal vena cava of sedated cats. J Vet Emerg Crit Care 5:121-129, 1995
18. Oakley RE, Olivier B, Eyster GE, et al: Experimental evaluation of central venous pressure monitoring in the dog. J Am Anim Hosp Assoc 33:77-82, 1997
19. Sawyer DC, Brown M, Striler EL, et al: Comparison of direct and indirect blood pressure measurement in anesthetized dogs. Lab Anim Sci 41:134-138, 1991
20. Synder PS: Amlodipine: A randomized, blinded clinical trial in 9 cats with systemic hypertension. J Vet Intern Med 12:157-162, 1998
21. Wagner AE, Brodbelt DC: Arterial blood pressure monitoring in anesthetized animals. JAVMA 210:1279-1285, 1997
Address reprint requests to
Armelle M. de Laforcade, DVM Section of Intensive Care
Department of Clinical Sciences Tufts University School of Veterinary Medicine
200 Westboro Road North Grafton, MA 01536
e-mail: [email protected]