Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1980, 64, 918-922
Central retinal artery occlusion followingcosmetic blepharoplastyPHILLIP W. KELLY' AND DONALD R. MAY2From the 'Ophthalmology Service, Wilford Hall USAF Medical Center, Lackland Air Force Base,San Antonio, Texas, and the 2Department of Ophthalmology, School of Medicine,University of California, Davis, California 95616, USA
SUMMARY A case is presented of a 70-year-old white male who underwent a bilateral cosmeticlower lid blepharoplasty with fat removal. He subsequently developed a right orbital haemorrhagewhich resulted in the occlusion of the central retinal artery. The patient had no light perceptionwith his right eye for approximately 1 hour, but vision was eventually restored to 20120 after emer-gency therapeutic measures. There are many possible causes of visual loss following blepharoplasty,with orbital haemorrhage being the most common. Visual loss secondary to blepharoplasty can beprevented in the preoperative, intraoperative, and postoperative phases of surgery. Blindness as acomplication of cosmetic blepharoplasty can be reversible if recognised early and treated appro-priately. These facts must be kept in mind by all surgeons who perform blepharoplasties.
Blindness following cosmetic blepharoplasty is rare.According to DeMere's survey of 3000 physiciansperforming blepharoplasties' the occurrence was0 04% or 1 case per 2500 operations. In 1969 Smith2reported that visual loss following blepharoplastywas rarely encountered as a complication of blepha-roplasty. Castanares3 reported that he had seen onlyI case of blindness following blepharoplasty, buthad seen at least 40 cases of unilateral partialblindness during his 25 years of practice. Jafek4reported one case of unilateral blindness attributedto an intraorbital haemorrhage following blepharo-plasty with fat excision. His review of the medicalliterature revealed no case reports for such anoccurrence over the previous 5 years. Putterman5reported the case of a patient who suffered completeunilateral blindness following blepharoplasty withfat excision. With therapeutic intervention theaffected eye of this patient was returned to its pre-operative visual acuity with no apparent sequelae.Hueston and Heinze6 discussed the early diagnosis
and surgical reversal of a case of blindness followingblepharoplasty. They later reported a similar case ofblindness reversed by wound decompression.7 Theyconcluded that outpatient blepharoplasty procedureswere 'intrinsically unsafe' and recommended closeinpatient supervision postoperatively.
Correspondence to Major Phillip W. Kelly, USAF MC,Ophthalmology Service/SGHSE, USAF Regional Hospital,Sheppard (ATC), Sheppard Air Force Base, Texas 76311,USA.
Blindness following orbital surgery other thanblepharoplasty was reported by Long and Ellis8 in1971. Eight cases were described which followedorbital exposure by Berke-Kronlein technique.Blindness has also been described following reduc-tion of fractured zygoma,9 the repair of orbital floorfractures,10 retinal detachment procedures,1' andneurosurgical procedures.12The most recent literature review and discussion
of blindness following blepharoplasty was byWaller.13 He concluded that blindness is a rare butreal complication of blepharoplasty which must beconsidered by the physician performing this opera-tion.
Case report
A 70-year-old white male underwent bilateralcosmetic upper lid blepharoplasties with fat removal.Six weeks later he was scheduled to undergo cosme-tic bilateral lower lid blepharoplasties, also with fatexcision. His preoperative examination included avisual acuity of 20/20 in both eyes and was otherwisecompletely normal except for dermatochalasis ofboth lower lids. He had no history of hypertensionor any other medical problem and was receiving nomedication.The procedure performed was a standard bilateral
lower lid blepharoplasty under local anaesthesia asdescribed in the AAOO manual on ophthalmicplastic surgery.'4 Fat excision was performed without
918
copyright. on F
ebruary 16, 2021 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.12.918 on 1 Decem
ber 1980. Dow
nloaded from

Central retinal artery occlusion following cosmetic blepharoplasty
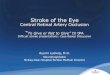
Fig. 1 Four hours followingbilateral lower lid blepharo-plasties with fat excision. Therehas been a right orbitalhaemorrhage with proptosis,subconjunctival haemorrhage,chemosis, and periorbitaloedema. Vision is no lightperception with the right eyeand 20/20 with the left.
difficulty. The fat presented easily and haemostasiswas achieved by cauterising the cut end of fat beforereleasing the haemostat. The orbital septum wasnot sutured. Haemostasis appeared adequate at theend of the procedure. A small pressure patch wasplaced over both infraorbital rims, leaving the eyesuncovered. The patient was instructed to remove thepatches on arriving home and to apply ice packsintermittently over both lower lids.The patient began to notice right orbital pain and
significant swelling of the right lower lid 2 hoursafter surgery. He returned to the ophthalmologyclinic about 4 hours after surgery. He stated thathe had been unable to see light with his right eye formore than 1 hour before returning to the clinic. Hehad also experienced severe pain of his right eyeduring that time.The initial evaluation revealed marked proptosis
of the right eye with extensive subconjunctivalhaemorrhage, chemosis, limited motility, and peri-orbital oedema (Fig. 1). The right eye was hard tofinger palpation, and the intraocular pressure wasover 60 mmHg measured with a Schi0tz tonometerwith a 15 g weight. The right eye had no lightperception. The right pupil was not reactive to lightbut was reactive consensually to light to the left eyeand to a near stimulus. Direct and indirect ophthal-moscopic examination of the right eye revealed noperfusion of blood through the central retinal arteryor its branches and stagnation of blood in thevenous system.Immediate therapeutic measures were instituted.
Initially a right lateral canthotomy was performed.The right lower lid suture line was then opened andapproximately 10 ml of blood under pressure was
released. A 3 ml retrobulbar injection was givenconsisting of equal parts of lidocaine HCI 2%,hyaluronidase, and aminophylline. An additional2 ml of hyaluronidase was injected into the swollenright lower lid. Intermittent digital massage wasapplied to the right eye. An intravenous drip wasstarted and 500 mg of acetazolamide was givenrapidly followed by 25 g of mannitol over 3minutes. No additional mannitol was given. Anadditional 250 mg of acetazolamide was givenintravenously every 6 hours for the next 24 hours.Bag rebreathing was started with the patient in thesupine position until carbogen (5% C02, 95% 02)became available. Carbogen was administered withcontinuous monitoring of the patient's pulse, respira-tions, and blood pressure for 10 minutes every hourfor 12 hours.
After these measures were performed 15 minuteshad passed and the intraocular pressure was 38mmHg with a Schi0tz tonometer with a 10 g weight.Ophthalmoscopy revealed perfusion of the entireretina at that time without apparent occlusion ofany portion of the retinal artery system. Within 30minutes the temporal half of the patient's rightvisual field returned increasing to a full visual fieldto confrontation within I hour after treatment wasbegun. At that time the patient's vision with hisright eye was 20/200 with a near card.
Gentamicin 80 mg intramuscularly every 8 hoursand methicillin sodium 2 mg intravenously every 6hours were started and continued for 72 hours.After drainage from the lower lid wound ceased at48 hours, a retroauricular skin graft was used toclose the wound.The visual acuity in the right eye improved to
919
copyright. on F
ebruary 16, 2021 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.12.918 on 1 Decem
ber 1980. Dow
nloaded from

Phillip W. Kelly and Doniald R. May
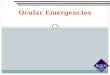
Fig. 2 Ten months after thecentral retinal artery occlusion.A satisfactory cosmetic resulthas been achieved. Vision is20/20 with both eyes.
20/60 by 48 hours and to 20/20 within 72 hours oftreatment. Visual field perimetry in the right eyeshowed slight constriction of the central isoptre at24 hours, but reverted to normal within 48 hours.The patient's vision was 20/20 in the right eye with afull visual field 10 months after the central retinalartery occlusion. A good cosmetic result was alsoachieved on his right lower lid (Fig. 2).
Discussion
Various mechanisms have been proposed as thecause of visual loss following blepharoplasty. Mostauthors feel that increased intraorbital pressure is amajor factor, whether it is a result of orbital hae-morrhage or oedema as a result of operative mani-pulation. Hepler et al.15 felt that sudden or completeloss of vision following blepharoplasty was causedby (1) orbital haemorrhage causing increased orbitalpressure which compromised the vascular circula-tion within the eye; (2) acute angle-closure glaucomain susceptible individuals; or (3) optic nerve ischae-mia, possibly due to orbital manipulation and/orpressure or secondary systemic hypotension frompreoperative medications. Also all the cases ofvisual loss following blepharoplasty which he andothers13 reported have been associated with fatremoval at the time of surgery.
Putterman5 proposed additional causes for orbitalhaemorrhages: (1) eyelid neovascularisation secon-dary to retinal detachment repairs; and (2) reboundvasodilatation from epinephrine-constricted vesselsescaping cautery during surgery. Another commonlyreported cause of orbital haemorrhage is excessivetugging on orbital fat during excision. Inadequatehaemostasis of excised fat by failure to adequately
cauterise the cut ends can also lead to orbital hae-morrhage. Other contributing causes to orbitalhaemorrhage are bleeding diatheses or severearteriosclerosis.The usual mechanism of visual loss is increased
intraorbital pressure producing a central retinalartery and/or vein occlusion, or causing directpressure on the optic nerve with subsegment occlu-sion of its vascular supply. Total vascular insuffi-ciency for 60- 120 minutes produces permanent lossof vision.7 A lesser duration of occlusion leads tovariable visual recovery. Clinically the signs andsymptoms of orbital haemorrhage are an acuteonset of orbital pain with an increased intraorbitalpressure manifested by proptosis, lid ecchymosis,increased intraocular pressure, limited extraocularmuscle movement, and a dilated, unresponsivepupil. Visual acuity is usually reduced but can rangefrom 20/20 to no light perception. The clinicianshould be familiar with these signs and symptomsso that he may act quickly and definitively shouldthey appear.The treatment of orbital haemorrhage as shown
by the above signs and symptoms varies accordingto the author. If no visual loss has occurred andvision does not appear threatened, close observationof visual acuity, intraocular pressure, and fundusvessel perfusion may be all that is required. However,when evidence of acute or impending decreasedretinal perfusion occurs, immediate therapy mustbe initiated. If the surgeon caring for the patient isnot an ophthalmologist, immediate assistance froma qualified ophthalmologist should be obtainedwhile emergency measures are being instituted.A lateral canthotomy can be performed easily to
decrease intraorbital pressure. The surgical wound
920
copyright. on F
ebruary 16, 2021 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.12.918 on 1 Decem
ber 1980. Dow
nloaded from

Central retinal artery occlusion following cosmetic blepharoplasty
should also be opened and the haematoma evacua-ted. A search for the bleeding site should be per-formed.An intravenous drip should be started and 20%
mannitol solution should be given as a bolus of12-5 g (62 5 ml) over an initial 3-5 minute interval,followed by a slower administration of additionalmannitol solution to achieve a total dose of 1 g/kgof body weight over the next 30 minutes.16 Intra-venous acetazolamide (500 mg) is given as an intra-venous push bolus with an additional 250 mg givenintravenously every 6 hours for at least the first 24hours. Digital ocular massage may be helpful todecrease intraocular pressure while awaiting actionof the intravenous osmotic agent. The patientshould be placed horizontally and made to rebreathein a small paper bag (a classic lunch bag size is best)until a mixture of 95% 02/5% CO2 (carbogen) canbe obtained for intermittent breathing. Carbogen isavailable from most pulmonary therapy laboratories.The injection of retrobulbar xylocaine and amino-phylline can be performed to promote dilation ofthe central retinal artery. The efficacy of this treat-ment has not been definitively proved and is notuniversally recommended. Hyaluronidase is addedto promote diffusion of the xylocaine and amino-phylline through the orbital tissues. The hyaluroni-dase also greatly enhances the reabsorption offluid from the orbital tissues."7
Paracentesis of the anterior chamber has beenadvocated to reduce intraocular pressure,'6 but thisis a hazardous procedure and should be performedonly by an ophthalmologist experienced in thetechnique."8 Intraocular haemorrhage, cataract for-mation, and iris prolapse are only 3 of the possiblecomplications which can result from a paracentesis.
Systemic antibiotics should be started after open-ing of a surgical wound for the evacuation of a
haemorrhage. The wound should be closed againonly after drainage has ceased.During the acute treatment phase the patient
should be carefully monitored with visual acuities,pupillary response, funduscopy, and confrontationvisual fields to assess the response to therapy.After the immediate therapy has ceased the visualacuity and visual fields should be examined andrecorded.The prevention of orbital haemorrhage with
subsequent visual loss can be grouped into 3 cate-gories: preoperative, intraoperative, and post-operative.'9
(1) PREOPERATIVEMoser et al.20 reported nonsurgically related post-operative blindness following blepharoplasty sur-
gery. They emphasised the need for preoperative
examination and recording of visual acuity andother unassociated ocular pathology. DeMere et al.1found that adequate eye examinations were per-formed in only 50% of patients undergoing eyelidsurgery. This ranged from a high of 90% in ophthal-mologists to 15% for plastic surgeons. Amblyopiais present in about 2% of our population, andcoexistent eye disease in patients undergoing eyelidsurgery is a distinct possibility which must be ruledout, for example, cataract, glaucoma, old trauma orscar, or retinal detachment. Patients often do notrealise that one eye is blind until the opposite eye isclosed or covered. Discovering this immediatelyafter surgery, even though it was pre-existent,causes the patient to relate the decreased visualacuity to the surgery itself.A good drug history should be obtained with
particular emphasis on vasodilators, aspirin, war-farin sodium, and other blood coagulation alteringagents. An evaluation for arteriosclerosis and hyper-tension should also be performed. Any eye abnor-malities should be noted and recorded if possiblewith photographs. One should rule out thyroid orrenal disease as causes for lid abnormalities.19 Asurgeon should be hesitant to perform blepharo-plasty with fat removal in a one-eyed patient unlessit is definitely indicated. A history of a true allergyto local anaesthetics obviates their use duringblepharoplasty and general anaesthesia is indicatedinstead.
(2) INTRAOPERATIVEDuring the operative procedure care must be givento meticulous dissection, atraumatic tissue handling,and complete haemostasis. Undue traction on theorbital contents, especially during fat removal, canlead to orbital haemorrhage. Fat removal must belimited to that fat which presents itself through theorbital septum with only light pressure on the globe.The orbital septum should not be excessively openedto obtain orbital fat. When excising orbital fat, aclamp should be placed on the fat, the fat excisedwith scissors (to leave a larger stump on the clampfor cauterisation), and cauterisation carried out witha hot wire or bipolar cautery. Cautery should beused with care anterior to the orbital septum andnever intraorbitally. Electrocoagulation by dia-thermy is not thought to be adequate for haemo-stasis. When the fat has been cauterised, the clampshould then be opened and the distal stump of fatexamined for bleeding with additional cautery asnecessary. Before closing the wound a dry field isessential to avoid complications. If epinephrine isused with the local anaesthetic, care must be exer-cised that postoperative rebound vascular dilatationdoes not occur in a previously dry field.
921
copyright. on F
ebruary 16, 2021 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.12.918 on 1 Decem
ber 1980. Dow
nloaded from

Phillip W. Kelly and Donald R. May
Avoidance of inadvertent excessive pressure onthe globe should be practised. Hollenhorst et al.12reported that central retinal artery occlusions canoccur during cervical neurosurgical procedures as aresult of the head rest causing inadvertent ocularpressure. If an eye is covered during any surgicalprocedure, a protective metal shield must beproperly placed over the eye to prevent inadvertentpressure.
(3) POSTOPERATIVEPostoperative pressure dressings are mentioned onlyto be condemned. Pressure increases as reported byJarrett and Brockhurst'1 do occur with elasticbandages over the eyes and can contribute to vascu-lar compromise. Pressure dressings obscure obser-vation needed to detect decreasing visual acuity,increasing intraocular pressure, and signs of orbitalhaemorrhage or other increases in orbital pressure.If an orbital haemorrhage occurs, pressure dressingsraise the intraorbital pressure to much higher levelsthan if no patch were present. Many authors feelthat blepharoplasty with fat removal should not bedone unless careful postoperative observation ispossible, meaning hospital admission in most cases.During the first 2 hours postoperatively visual
acuity assessments and observation for pain orproptosis should be performed every 10 minutes.The intervals can be lengthened to every 4 hours from2 to 24 hours after surgery. The examination mustbe performed by qualified medical observers. Agauze pad soaked in iced or chilled saline can beloosely applied over the eyes for the first 24 hours todecrease swelling.
Should signs or symptoms of an orbital haemorr-hage occur, the surgeon should be contacted imme-diately. If decreasing visual acuity is found secondaryto the suspected orbital haemorrhage, emergencytreatment measures should be immediately institutedas outlined above. If visual loss is reversed, carefulmonitoring of the patient's visual status is necessaryincluding visual acuity, pupillary reaction, fundusexamination, and visual fields until the patient'scondition is entirely stable.
Dr John W. Shore and Dr Hal C. Hudson, Captain MarshaYeager Sherry, and Lieut. Nancy Wylie provided invaluableassistance during the emergency care of this patient.
References
I DeMere M, Wood T, Austin W. Eye complications withblepharoplasty or other eyelid surgery. A nationalsurvey. Plast Reconstr Surg 1974; 53: 634-7.
2 Smith B. Postsurgical complications of cosmetic blepharo-plasty. Trans Am Acad Ophthalmol Otolaryngol 1969;73: 1162-4.
3 Castanares S. Eyelid Plasty. In: Goldwyn RM, ed. TheUnfavorable Result in Plastic Surgery: Avoidance andTreatment. Boston: Little, Brown, 1972: 267.
4 Jafek BW, Kreiger AE, Morledge D. Proceedings:Blindness following blepharoplasty. Arch Otolaryngol1973; 98: 366-9.
5 Putterman AM. Temporary blindness after cosmeticblepharoplasty. Am J Ophthalmol 1975; 80: 1081-3.
6 Hueston JT, Heinze JB. Successful early relief of blind-ness occurring after blepharoplasty. Case report. PlastReconstr Surg 1974; 53: 588-92.
7 Hueston JT, Heinze JB. A second case of relief of blind-ness following blepharoplasty: Case Report. PlastReconstr Surg 1977; 59: 430-1.
8 Long JC, Ellis PP. Total unilateral visual loss followingorbital surgery. Am J Ophthalmol 1971; 71: 218-20.
9 Varley EWB, Holt-Wilson AD, Watson PG. Acuteretinal arterial occlusion following reduction of a frac-tured zygoma and its successful treatment. Br J OralSurg 1968; 6: 31-6.
10 Nicholson DH, Guzak SV Jr. Visual loss complicatingrepair of orbital floor fractures. Arch Ophthalmol 1971;86: 369-75.
11 Jarrett WH, Brockhurst RJ. Unexplained blindness andoptic atrophy following retinal detachment surgery.Arch Ophthalmol 1965; 73: 782-91.
12 Hollenhorst RW, Svien HJ, Benoit CF. Unilateralblindness occurring during anesthesia for neurosurgicaloperations. Arch Ophthalmol 1954; 52: 819-30.
13 Waller RR. Is blindness a realistic complication inblepharoplasty procedures? Ophthalmology 1978; 85:730-5.
14 Silver B. Ophthalmic Plastic Surgery. 3rd ed. Rochester:American Academy of Ophthalmology and Otolaryn-gology, 1977.
15 Hepler RS, Sugimura GI, Straatsma BR. On the occur-rence of blindness in association with blepharoplasty.Plast Reconstr Surg 1976; 57: 233-5.
16 Hartley JM Jr, Lester JC, Schatten WE. Acute retrobul-bar haemorrhage during elective blepharoplasty: itspathophysiology and management. Plast Reconstr Surg1973; 52: 8-12.
17 May DR. Hyaluronidase in the treatment of orbitalhaemorrhage. In preparation.
18 Lemoine AN Jr, Rees TD, Newell FW. Discussion.Plast Reconstr Surg 1973; 52: 12-5.
19 Wiggs EO. Blepharoplasty complications. Trans AmAcad Ophthalmol Otolaryngol 1976; 81: OP603-6.
20 Moser MH, DiPirro E, McCoy FJ. Sudden blindnessfollowing blepharoplasty: report of seven cases. PlastReconstr Surg 1973; 51: 364-70.
922
copyright. on F
ebruary 16, 2021 by guest. Protected by
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.64.12.918 on 1 Decem
ber 1980. Dow
nloaded from