Embed Size (px)
Citation preview

Retinal Vein Occlusion Studies
Dr. Riyad Banayot

Prevalence Retinal vein occlusions (RVOs) are the 2nd most common retinal vascular diseases after diabetic retinopathy.
The Beaver Dam Study reported a prevalence of 0.1% in patients older than 43 years.
A cross-sectional study from 6 US communities reported that the prevalence of CRVO was 0.2%. (the prevalence was similar across different ethnic and racial groups).
The Blue Mountains Eye Study, the 10-year cumulative incidence of CRVO in a population older than 48 years was 0.4%.
The Singapore Malay Eye Study reported a 0.2% prevalence of CRVO in the Malay population 40 to 80 years old.
The Beijing Eye Study reported that the prevalence of CRVO in a Chinese population of people 40 years and older was 0.1%.(No racial or gender predilection for the disease is apparent).

Associated systemic factors
DiabetesHypertensionHyperlipidaemiaHyperhomocysteinaemia Blood coagulation disorders:
high plasma viscosity such as due to leukaemia, myeloma, Waldenstrom’s macroglobulinaemia, myelofibrosis, changes in protein C pathway, Factor V Leiden.
Systemic inflammatory disorders(Behçets disease, polyarteritis nodosa, sarcoidoisis, Wegener’s
Granulomatosis and Goodpasture’s Syndrome) Glaucoma Shorter axial length Retrobulbar external compression

CRVODisc edemaIncreased dilatation
and tortuosity of all retinal veins
Widespread deep and superficial hemorrhages
Cotton wool spotsRetinal edemaCapillary non-
perfusion in all four quadrants of the retina

HRVO & BRVO

Complications
Classical TreatmentBranch Vein Occlusion Study, 1984, showed
that macular photocoagulation for the treatment of macular edema was superior in improving visual acuity compared with observation.
Central Vein Occlusion Study, 1995, showed that grid laser treatment of macular edema was of no visual benefit despite the elimination of macular edema in treated eyes. Observation for macular edema secondary to CRVO was the standard of care set by this study.

Pharmacologic Rx options for Macular edema
Dexamethasoneintravitreal implant (Ozurdex)
Ranibizumab(Lucentis)
Aflibercept (Eylea)
Bevacizumab (Avastin)
CRVO FDA FDA FDA Off labelBRVO FDA FDA Off label

RVO studiesSCORE-C/B 2009 IV Triamcinolone Vs.
Observe/GridGENEVA-C/B 2010 evaluate IV Dexamethasone
extended to 1 yearSHASTA-C/B 2014 evaluate IV DexamethasoneCRUISE-C 2010 evaluate IV Ranibizumab
extension HORIZONBRAVO-B 2010 evaluate IV Ranibizumab
extension RETAINCOPERNICUS-C 2014 evaluate IV AfliberceptGALILEO-C 2014 evaluate IV AfliberceptVIBRANT-B 2013 evaluate IV Aflibercept

SCORE study 2009
Compared the use of 1-mg, 4-mg intravitreal triamcinolone (Trivaris*) to standard care:
Observation for CRVO Grid laser for BRVO
• unpreserved triamcinolone • Triesence

Results: SCORE-BRVO
Trivaris 1mg Trivaris 4mg Grid LaserYear 1VA gain ≥ 3 lines
26% 27% 29%
Year 2 & 3VA
Sustained Sustained Sustained
Patients who were randomized to grid laser underwent a mean 1.5 treatments in year 1, and those who received IVTA had an average of 2 injections
• The rates of cataract formation and IOP elevation were higher in the steroid groups
• The recommendation was that laser remain the standard of care for BRVO

Results: SCORE-CRVO
Trivaris 1mg Trivaris 4mg ObservationYear 1VA gain ≥ 3 lines
27% 26% 7%
Year 2VA
Sustained Sustained
Patients received an average of 2 injections of IVTA over the course of 1 year

GENEVA study 2010
Evaluated dexamethasone intravitreal dexamethasone implant (Ozurdex) for the treatment of macular edema 2ry to BRVO or CRVO
Entry criteria:VA: 20/50 to 20/200CMT ≥300 μm
0.7 mg Dexamethasone
0.35 mg Dexamethasone
Sham
Single treatment
Single treatment
Single treatment
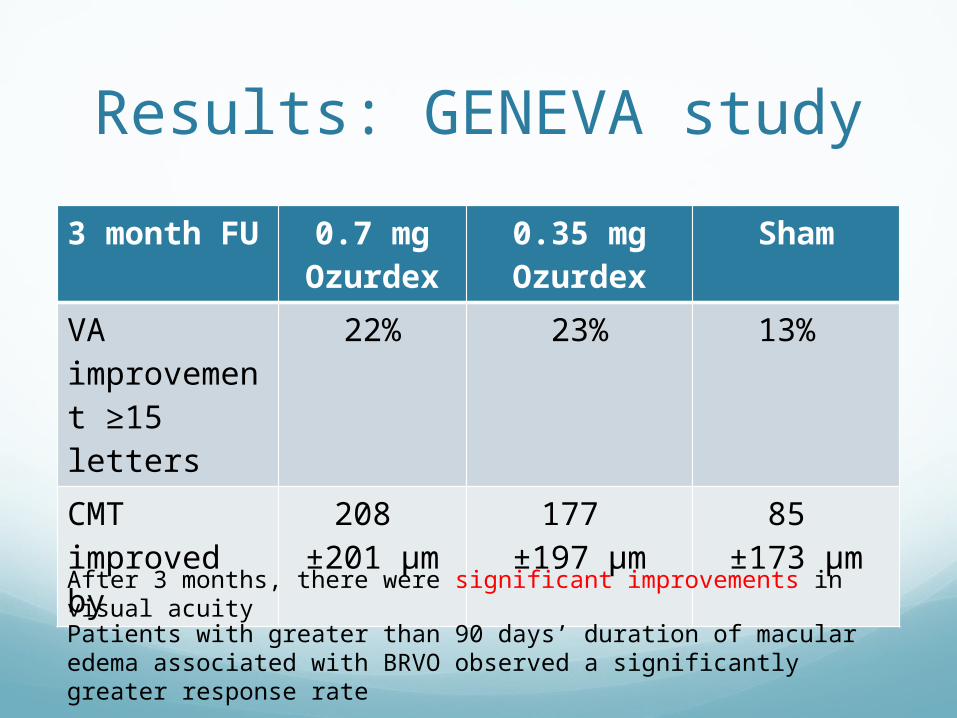
Results: GENEVA study3 month FU
0.7 mg Ozurdex
0.35 mg Ozurdex
Sham
VA improvement ≥15 letters
22% 23% 13%
CMT improved by
208 ±201 μm
177 ±197 μm
85 ±173 μm
After 3 months, there were significant improvements in visual acuityPatients with greater than 90 days’ duration of macular edema associated with BRVO observed a significantly greater response rate

Results: GENEVA study 6 month FU
0.7 mg Ozurdex
0.35 mg Ozurdex
Sham
VA improvement 15 or more letters
22% 19% 18%
CMT improved by
119 ±203 μm
123 ±212 μm
119 ±188 μm
Changes in VA nor CMT for treatment groups were NOT significant when compared with the sham group at the 6-month interval

Extension of GENEVA study
After 6 months, study was extended to 12 monthsPatients received the open-label 0.7 mg
Dexamethasone intravitreal implantCriteria:
VA: <84 ETDRS letters or CMT: >250 um
12 month 0.7 mg Ozurdex
Sham
BCVA improvement 32% 30%

Results: Extension of GENEVA study
12 month 0.7 mg Ozurdex
Sham
BCVA improvement 32% 30% 12 month X2 0.7 mg
OzurdexSham
Cataract 29.8% 5.7% 12 month 0.7 mg OzurdexIOP increase ≥10 mm Hg (1st injection)
12.6%
IOP increase ≥10 mm Hg (2nd injection)
15.4%

SHASTA Study 2014
The effects of multiple dexamethasone implants for macular edema secondary to CRVO or BRVO
Patients received a mean 3.2 dexamethasone implants with mean injection interval between implants was 5.6 months
After 6 implants BRVO CRVOBCVA gain ≥2 lines 59.7% 66.7%CMT significant
reductionsignificant reduction
IOP increase ≥10 mm Hg
32.6%Medical treatment for high IOP
29.1%
Surgical treatment for high IOP 1.7%Laser treatment for high IOP 1.4%

CRUISE study 2010
12-month clinical trialEvaluated the efficacy and safety of anti-VEGF
injections in the treatment of macular edema secondary to CRVO
Criteria:visual acuity of 20/40 to 20/320CMT≥ 250 μm
Injections0.3 mg ranibizumab
0.5 mg ranibizumab
Observation
Monthly for 6 M Monthly for 6 M Monthly for 6 M“as needed” basis from months 6-12
“as needed” basis from months 6-12
0.5 mg ranibizumab, followed by “as needed” basis

Results: CRUISE study initial effects of ranibizumab therapy within 7days after the first
injections
6 month FU
0.3 mg ranibizum
ab
0.5 mg ranibizum
ab
Observation
VA improvement ≥3 lines
46.2% 47.7% 16.9%
Letters from baseline BCVA
12.7 14.9 0.8
CMT improved by
433.7 ±51.2 μm
452.3 ±44.7 μm
167.7 ±53.7 μm
These improvements were maintained in both treated groups at 12 months

HORIZON studyextension of CRUISE study
HORIZON extension trial, patients continue to receive 0.5mg ranibizumab on a PRN basis
FU on a mandatory quarterly basis for the next year A total of 151 patients with CRVO received ranibizumab
therapy and the mean number of injections was 3.9 (range 0 – 12).
Ranibizumab 0.5mg
SHAM
VA improvement from CRUISE baseline
- 4.1
Letters gained from CRUISE baseline
12 7.6

BRAVO study 2010
12-month clinical trialEvaluated the efficacy and safety of anti-VEGF
injections in the treatment of macular edema secondary to BRVO
Injections0.3 mg ranibizumab
0.5 mg ranibizumab
Sham
Monthly for 6 M Monthly for 6 M Monthly for 6 M“as needed” basis from months 6-12
“as needed” basis from months 6-12
0.5 mg ranibizumab, followed by “as needed” basis
subjects were eligible to receive rescue laser treatment during the clinical trial

Results: BRAVO study6 month FU
0.3 mg ranibizum
ab
0.5 mg ranibizum
ab
Sham
VA improvement ≥3 lines
55.2% 61.1% 28.8%
Letters from baseline BCVA
16.6 18.3 7.3
CMT improved by
337.3 ±38.3 μm
345.2 ±41.2 μm
157.7 ±38.6 μmEffects were not permanent and the patients might require several
re-injections

RETAIN studyextension of CRUISE study
The RETAIN study was an extension study for patients who completed the HORIZON study.
Only 34 patients from the BRAVO study were enrolled in the RETAIN study. On average, patients had a follow-up of 4 years.
Patients were followed monthly during the first year of the study and at least every 3 months during the second year of the study.
Reinjections were performed if intraretinal fluid was identified. Results demonstrate the excellent long-term outcomes of eyes
with macular edema secondary to BRVO.
RanibizumabResolution of macular edema
44%
VA improvement ≥3 lines 53%BCVA of 6/12 or better 80%

COPERNICUS study 2014
Evaluating the efficacy of aflibercept in CRVOEntry criteria:
VA: 20/40 to 20/320 CMT >250 μm
2 mg aflibercept ShamMonthly for 6 M Monthly for 6 M“as needed” basis from months 6-12
Allowed to receive afliberceptafter week 24

Results: COPERNICUS study
6 month FU 2 mg aflibercept ShamVA improvement ≥15 letters
57.9% 12.3%
CMT improved by
457.2 μm 144.8 μm
Benefits were maintained at 52 weeks

GALILEO study 2014
Evaluating the efficacy of aflibercept in CRVOEntry criteria:
VA: 20/40 to 20/320 CMT >250 μm
2 mg aflibercept ShamMonthly for 6 M Monthly for 6 M“as needed” basis from months 6-12
“as needed” basis from months 6-12

Results: GALILEO study
6 month FU 2 mg aflibercept ShamVA improvement ≥15 letters
60% 22%
CMT improved by
448.6 μm 169.3 μm
Benefits were maintained at 52 weeks
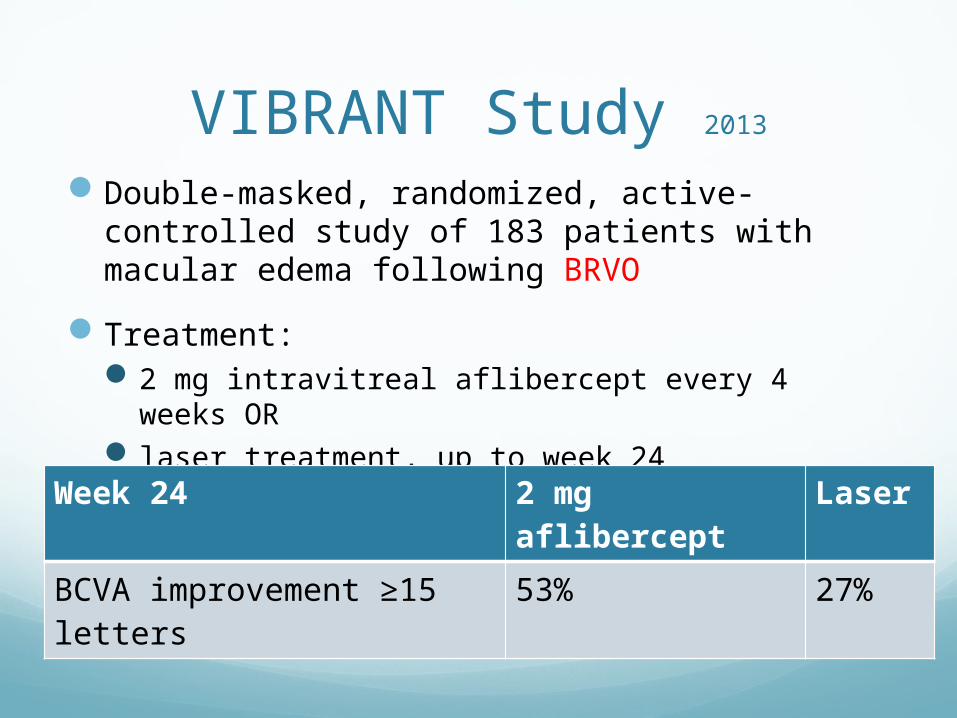
VIBRANT Study 2013
Double-masked, randomized, active-controlled study of 183 patients with macular edema following BRVO
Treatment:2 mg intravitreal aflibercept every 4 weeks OR laser treatment, up to week 24
Week 24 2 mg aflibercept
Laser
BCVA improvement ≥15 letters
53% 27%

RVO studies Recommendation
SCORE-C/B IV Triamcinolone Vs. Grid/Observation
Laser remain the standard of care for BRVO
IV Beneficial for CRVOGENEVA-C/B evaluate IV
Dexamethasone3M: Changes significant6M: Changes NOT significant
extension 12M: Changes NOT significantCataract 30%, IOP 15%
SHASTA-C/B evaluate IV Dexamethasone
Changes significantIOP 33%
CRUISE-C evaluate IV Ranibizumab VA, letters, CMT improvement
HORIZON Changes NOT significantBRAVO-B evaluate IV
Ranibizumabimprovement NOT permanent need re-inject
RETAIN improved CMT & VACOPERNICUS-C evaluate IV Aflibercept improvement maintainedGALLILEO-C evaluate IV Aflibercept improvement maintainedVIBRANS-B evaluate IV Aflibercept improvement better with IV vs.
laser
Summary