Embed Size (px)
Citation preview

Pain, 36 (1989) 13-25 Elsevier
13
PAI 01328
Central post-stroke pain - neurological symptoms and pain characteristics
G. Leijon *, J. Boivie * and I. Johansson * *
Departments of * Neurology and * * Radiology University Hospital, S-581 85 Linkcping (Sweden)
(Received 19 July 1988, accepted 25 July 1988)
Sum-7 The intention of the present study was to characterize patients with central post-stroke pain (CPSP) with regard to type and location of the cerebrovascular lesion (CVL), the characteristics of the pain and the neurological symptoms and signs in addition to the pain.
Twenty men and 7 women with a mean age of 67 years and a mean pain duration of 44 months were examined 9-188 (mean 53) months after their stroke. The clinical symptoms and signs and the CT scans indicated that the CVL were located in the lower brain-stem in 8 patients, involved the thalamus in 9 patients and were located lateral and superior to the thalamus in 6 patients. In the remaining 4 patients the location of the CVL could not be determined with certainty. The 3 identified hematomata were all located in the thalamus.
The onset of the pain was immediate in 4 patients, within the first post-stroke months in 10 patients and delayed by l-34 months in the rest.
The pain was on the left side in 18 patients. Twenty patients had hemipain. Most patients experienced more than one type of pain. The most common qualities were burning, aching, pricking and lacerating, with some differences in the frequencies according to the location of the CVL. Burning pain was most common, except among the patients with thalamic CVL, in whom lacerating pain was more common. Aching and pricking pain were also frequent.
All patients considered the pain to be a great burden and most rated the pain intensity as high on a visual analogue scale. The intensity was increased by external stimuli, the most common being joint movements, cold and light touch. Five patients reported aggravation by emotional stimuli.
Besides pain, the only neurological symptom common to all patients was decreased temperature sensibility, as shown by quantitative methods. It is possible that pain sensibility was also abnormal in all. Hypersensitivities to cutaneous stimuli, including evoked dysesthesias were found in 88% of the patients, while the detection thresholds for touch and vibration were abnormal in only 52% and 411, respectively. Similarly, low figures were found for paresis and ataxia, which were present in 48% and 62%. respectively.
It is concluded that only a minority of patients with central pain after stroke have thalamic lesions. The term thalamic pain is therefore inaccurate in most cases of CPSP. The symptoms and signs indicate that the crucial factor for the development of CPSP is a lesion affecting the spino-thalamo-cortical pathway important for temperature and pain sensibility. The level of the lesion along the neuroaxis is not critical for occurrence of the pain, but decides the nature of the associated neurological symptoms and appears to affect the features of the pain.
Key words: Central post-stroke pain; Neurological symptoms; Pain characteristics
Introduction
Correspondence to: Dr. Giiran Leijon, M.D., Department of Cerebrovascular lesions (CVL) are a major Neurology, University Hospital, S-581 85 Linkaping, Sweden. cause of long lasting disability. Pain is one of the
0304-3959/89/$03.50 6 1989 Elsevier Science Publishers B.V. (Biomedical Division)

14
least recognized symptoms following stroke. There are 2 main categories of post-stroke pain: nocicep- tive and neurogenic. The most common nocicep-
tive post-stroke pain is shoulder pain [8] caused by changed dynamics due to paresis. The neurogenic post-stroke pain is caused by the brain lesion itself
and is thus a central neurogenic pain. In the literature the impression is given that
most central post-stroke pain (CPSP) is thalamic
pain, although it is known that extrathalamic CVL, such as lesions in the brain-stem [15,21,22,33,34]
and suprathalamically [1,2,6,8,11,14,19,21,22,33, 34,371 located lesions, can also cause central pain. Thalamic pain was originally described in 1906 by Dejerine and Roussy [17] as one component of the
thalamic syndrome. According to their descrip- tion, the syndrome is characterized by the follow-
ing symptoms: (1) slight hemiplegia; (2) dis- turbance of superficial and deep sensibility; (3) hemiataxia and hemiastereognosia; (4) intolerable
pain; (5) choreoathetoid movements. The cause of the thalamic syndrome is usually a
thalamic infarction or hemorrhage [17,22,33]. The incidence of complete thalamic syndromes is very
low but thalamic pain, i.e., pain caused by a thalamic lesion is less rare [16,34]. In many cases the lesions causing thalamic pain extend consider-
ably lateral to the thalamus. In such patients it is not possible to know the role of the extrathalamic parts of the lesion for the pain.
The clinical features of thalamic pain have been reviewed by several authors [11,22,32,33,34]. Its severity and resistance to all kinds of treatment are well known. The pain is usually described as a
diffuse spontaneous or evoked pain, mainly dis- tributed to the extremities and usually with a burning or aching quality. Its onset is often de-
layed by several months. Somatic, visceral and emotional stimuli increase the pain. Signs of sym-
pathetic dysfunction may also be present [11,29,
331. The literature contains several case reports and
some reviews which indicate that pain due to suprathalamic CVL is similar to thalamic pain [1,2,6,11,13,14,19,22,33,34,37]. Pain following CVL in the brain-stem, most frequently as part of a Wallenberg syndrome, is usually located in the face on the lesion side and the limbs on the
opposite side, but also resembles thalamic pain [15,21,22,33,34]. However, no systematic studies of differences in the clinical features in patients with
CPSP due to brain-stem, thalamic and supraten- torial extrathalamic CVL appear to have been made..
The aim of the present study was to char- acterize CPSP patients with regard to the type and location of the CVL, the pain and the neurological
symptoms and signs. Thus, one of the major inten- tions with the study was tb find out whether a symptom entity exists which is typical for CPSP patients in general, and if different clinical entities can be identified in patients with topologically different lesions, i.e., CVL located in the brain- stem, thalamus or above the thalamus. Pre-
liminary results have been reported [26].
Patients and methods
Patients
The results are based on examinations of 20 men and 7 women with a mean age at the time of the investigation of 67 years (range 53-81). For
inclusion in the study the following criteria had to be fulfilled: (1) the patient should have had an
unequivocal stroke episode; (2) the patient should be seeking a remedy for constant or intermittent
pain, which started after the stroke; (3) it should have been excluded that the pain was of nocicep- tive, peripheral neuropathic or psychogenic origin.
Patients with dysphasia severe enough to make an adequate evaluation impossible were excluded. For the same reason, patients with dementia or confusion of other etiology were also excluded.
The 27 patients were selected from a larger
population of patients with pain following stroke at the Department of Neurology. All consecutive patients who fulfilled the criteria for the study during the period February 1985-December 1986 were included.
Table I presents the age at the onset of stroke, the age at examination and the duration of the pain.
Examinations The examinations of the patients were per-
formed 9-188 months (mean 53) after the stroke

15
TABLE I
AGE AT ONSET OF STROKE, AND AT EXAMINATION;
DURATION OF PAIN
Men Women All
(N = 20) (N=7) (N = 27)
Age at onset of stroke (years)
Mean 60 68
Range 47-69 59- 74
Age at time of examination (years)
Mean 66 72
Range 53-78 62- 81
Duration of pain (months)
Mean 33 54
Range 9-75 S-154
62
47- 74
67
53- 81
44
8-154
(for 6 patients the interval was 9-12 months, for 4 patients 13-24 months and for 17 patients it was more than 24 months). The patients were ex- amined according to a project program which included the following procedures:
(1) A systematic history, particularly detailing prior diseases, the stroke episode and sensory abnormalities. The pain history was obtained from a pain questionnaire and from interviews accord- ing to a protocol designed for the study.
(2) A thorough general somatic and neurological
examination.
(3) Computerized tomography (CT) scanning of the brain was performed on a Philips Tomoscan 310 scanner with contiguous 6 mm slices (24 pa- tients), or on an EM1 1010 scanner with contigu- ous 10 mm slices (3 patients). To calculate the sizes of the lesions, the standard measurement devices of the Tomoscan 310 CT scanner (24 patients) and EM1 1010 (1 patient) were used.
(4) Evaluation by an occupational therapist. This examination included tests for auditory, tactile and visual agnosia, constructional and ideomotor apraxia. Visual perception was assessed by using a battery of 16 items [18]. Auditory and tactile agnosia were tested by identifying non-verbal sounds and various objects of different shape and of different material. Ideomotor apraxia was as- sessed using different commands and apraxia for
construction by having the patients copy drawings using cubes and matches.
(5) Evaluation by a social worker. This included data about family relationships, occupation, econ- omy, major traumatic life events, leisure time ac- tivities and possible alcohol or drug abuse.
(6) Analysis of cerebrospinal fluid. (7) Quantitative analysis of sensory abnormali-
ties [7]. (8) Peripheral nerve conduction velocity.
Non-central pain and coexisting diseases
In the diagnostic process particular efforts were made to differentiate nociceptive and peripheral neurogenic pain from central pain. The nerve con- duction velocity in combination with clinical neu- rological examination did not indicate a periph- eral neuropathic condition as the origin of the pain in any case.
Some patients were suspected of having mus- culoskeletal pain. This is common in the age groups dominating the present patient population and among stroke patients due to their paresis. Pa- tients suspected of having such nociceptive pain were referred to an orthopedic specialist for con- sultation.
Nine patients had a history of long lasting pain when they got the CPSP, which was, however, entirely different from their previous pain. The pre-existing pain was a nociceptive pain in 8 pa- tients and a sciatica in the ninth patient. After the stroke 2 of these patients and 2 additional patients had developed a hemiplegic shoulder.
Fourteen patients had a history of ischemic heart disease, 6 had diabetes mellitus, 1 patient a mild rheumatoid arthritis and 1 polymyositis with light pain. None of the patients had a history of major depressive disorder, but two had consulted a general practitioner and received tranquilizers for mild psychiatric symptoms.
Results
Location, type and size of CVL According to the location of the CVL the pa-
tients were divided into 4 groups: BS - brain- stem, CVL located in the medulla oblongata, pons

TABLE II
CT EXAMINATION
Location and volume of CVL in the hemisphere contralateral to the pain.
BS TH SE UI All (N = 8) (N = 9) (N = 6) (N=4) (N = 27)
No lesion 4 0 2 1 7 Cerebellum
Thalamus
Int. caps/basal gangl.
Cortical/subcortical
Volume of CVL (cm’)
Mean
Range
3 0 0 0 3 0 9 0 0 9 1 7 3 1 12 1 5 3 4 13
2.6 18.1 13.2 0.8 32.1 2.0-4.3 0.6-144.4 47.2-99.2 0.5-3.0 0.5-144.4
and midbrain (8 patients); TH - thalamus, CVL affecting the thalamus (9 patients); SE - supra- tentorial, extrathalamic, CVL not affecting thala-
mus (6 patients); UI - unidentified, location of CVL not determined (4 patients).
The diagnosis of the brain-stem lesions rested
mainly on acknowledged clinical criteria [12] in- cluding combinations of cranial nerve symptoms, sensory abnormalities with alternate laterality and
ataxia. In 7 patients the clinical picture was that
of a complete or partial Wallenberg syndrome and the remaining patient had other signs of a bulbo- pontine lesion. CT did not reveal signs of a vascu- lar lesion in the brain-stem in any of the BS patients but 3 of them had signs of cerebellar infarctions, which none of the other 19 patients
had (Table II). Only patients with CT-verified lesions affecting
the thalamus were classified as TH patients. For inclusion in the TH group it was also required that there were no neurological symptoms indicating an infratentorial lesion. Only 2 of the 9 TH pa- tients had CVL restricted to the thalamus (Fig. 1E and I). These lesions affected the posterior part of the lateral half of the thalamus. It appeared likely that these lesions, as well as the other 7 CVL which extended into the thalamus, engaged the ventroposterior thalamic region, i.e, including the large somatosensory relay nuclei in that region. This could not be determined with certainty, how- ever. Most of the CVL not restricted to the thalamus were large (4 of them > 50 cm3) and extended laterally into the internal capsule, basal
ganglia and other structures (Table II and Fig. lA-I).
Four of the 6 SE patients had CT verified lesions (Table II and Fig. lJ-M). All had symp-
toms and signs indicating a supratentorial CVL. These symptoms were either disturbances of higher cortical functions like aphasia, agnosia and apraxia
and hemianopia or hemipareses with ipsilateral facial paresis of the central type. Two of the lesions were located close to the thalamus and
involved the anterior limb of the internal capsule, but none extended into its posterior limb. The patient with the lesion closest to the thalamus was examined twice with CT, at the occurrence of the stroke and 10 months after the stroke (Fig. 1J). Both times the CVL was well demarcated and
included parts of the anterior limb of the internal capsule as well as parts of the basal ganglia, but did not extend into the thalamus. In the 2 SE patients in which no lesions were found on CT the clinical symptoms indicated supratentorial CVL (one patient had hemiparesis and tactile agnosia and the other hemiparesis with ipsilateral facial
paresis). In the 4 patients classified as UI patients it was
not possible to localize the relevant CVL with CT or clinical criteria. All 4 UI patients had unilateral hemihypesthesia. One had a slight extremity pare- sis, two slight gait disturbances and one a mild ataxia. All symptoms except the sensory abnor- malities and the ataxia were of short duration. All 4 UI patients had bilateral supratentorial lesions on CT.

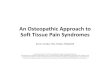
TH PATIENTS 17
SE PATIENTS
~~~~
Fig. 1. CT findings in 9 patients with thalamic CVL (A-I) and 4 patients with supratentorial, extrathahmic CVL (J-M). Black areas indicate extension of CVL.

18
Only 3 of the 27 patients had identified hemor- rhages, all affecting the thalamus. However, it is possible that there were additional hemorrhages,
since no CT examination was performed during the first weeks after the occurrence of the stroke in
9 of the TH, SE and UI patients.
Supratentorial lesions in the hemisphere ipsi- lateral to the pain were found in 1 BS and 1 SE
patient. Central atrophy was found on CT in 3 BS patients, 5 TH patients, 2 SE patients and 1 UI
patient. As expected, there was a higher incidence of central atrophy in patients with supratentorial than infratentorial lesions. Such atrophies add to other reasons for the difficulty in calculating the
initial size of the CVL.
Pain characteristics
Duration and onset. At the time of the examina- tion the patients had experienced pain for an average of 44 months (Table I). The time from the
stroke to the onset of pain varied. Four of the 27 patients experienced the pain already on the first
post-stroke day. In 10 patients the pain started during the first post-stroke month. In the rest the intervals between the stroke and the onset of pain
were: 1-3 months in 7 patients; 5-12 months in 3 patients; 24-34 months in 3 patients.
Twenty of the patients experienced a gradual onset of the pain. Some of these reported that the onset of the pain coincided with improvement of perceived sensory loss and onset of dysesthesias. There were no major differences in the delay or
TABLE III
LATERALIZATION AND DISTRIBUTION OF PAIN
the type of the onset of pain hetween the 4 patient groups.
Twenty-three patients had constant pain. but the 4 patients with intermittent pain experienced
pain every day and the pain-free intervals lasted a few hours at the most.
Location. All patients considered it easy to de- scribe the location of the pain, which was superfi-
cial in 8, deep in 8 and both superficial and deep in 11 patients. The pain was left-sided in two-thirds
of the patients (the 2 BS patients with alternate laterality face/extremities were classified accord- ing to side of extremity pain; Table III). Among
the patients with identified supratentorial CVL (TH and SE groups), the proportions of left and right-sided pain were 73% and 27%.
Fifty-two percent of the patients experienced pain in the entire right or left side of the body, with the exception of the face. Thirty-three per-
cent had pain in the face as well in other parts of the body.
Quality. The pain drawings and interviews showed that most patients had more than one kind of pain. The mean number of pain qualities was 2.0 (range l-4). The most common pain char-
acteristics are listed in Table IV, which shows that there was no dominating pain characteristic com- mon to all CPSP patients. The most frequently
reported were burning, aching, pricking and lacerating pain.
A comparison between the 3 groups with iden- tified CVL indicates some differences in the pain
L.ateralisation
Right Left
Distribution
Hemipain except face Hemipain Abdomen-lower limb
Thorax-upper limb Face-thorax-upper limb Alternate
BS TH SE UI All
(N = 8) (N = 9) (N = 6) (N = 4) (N = 27)
3 2 2 2 9 (33%)
5 7 4 2 18 (67%)
2 5 5 2 14 (52%)
1 3 1 1 6 (22%)
2 0 0 1 3 (11%)
1 0 0 0 1 (4%)
0 1 0 0 1 (4%)
2 0 0 0 2 (7%)

19
TABLE IV
QUALITY OF PAIN EXPRESSED AS PERCENTAGES FOR THE RESPECTIVE GROUPS
N.B., Most patients perceived more than one quality of pain.
(“N”= 8) TNH_9)
SE All
(N =6) (uNI=4) (N = 27)
Burning 75 22 83 75 59
Aching 38 22 33 25 30
Pricking 25 22 33 50 30
Lacerating 0 44 33 25 26
Shooting 13 22 0 0 11
Squeezing 13 22 0 0 11
Throbbing 0 22 17 0 11
Other 13 22 17 25 19
qualities. The most striking differences were those between the thalamic and extrathalamic groups. While 75% of the BS and 83% of the SE patients experienced burning pain, only 22% of the TH patients did so. In the TH group lacerating pain was the most common quality, a type of pain which none of the BS patients experienced. The TH group also differed from the other groups by having a larger diversity of pain qualities.
Intensity and factors affecting the pain. The pain intensity was estimated by asking the patients to indicate the experienced average pain intensity during ordinary conditions on a visual analogue
TABLE V
FACTORS INCREASING AND DECREASING THE PAIN
;:=S) ;f=9) ;:=6) ;=4) ;=27)
Increasing ( W)
Movements 38
Cold 63
Warmth 20
Touch 63
Emotion 25
Other 38
Decreasing (5%)
Movement 38
Cold 0
Warmth 25
Rest 13
Other 0
89 83 75 70
33 33 75 48
11 33 25 22
44 17 50 44
33 0 0 19
0 17 0 15
13 17 0 19
0 22 0 7
33 50 0 30
56 17 75 37
0 0 0 0
scale (VAS; 100 mm). The mean VAS values for the 4 groups were (ranges in parentheses): BS 61 (39-94); TH 79 (68-98); SE 50 (30-91); UI 25 (12-39). Even in patients who did not rate the intensity particularly high on VAS, it became evi- dent from the interviews that the pain was a great burden to them.
The pain intensity fluctuated considerably dur- ing the days in all patients. These fluctuations were partly spontaneous, partly due to external or emotional factors. Table V shows various factors affecting the pain. Joint movements, including walking and change in posture, were the most common factors increasing the pain, with cold and light touch second and third in this respect. Emo- tions like sudden fear, joy, loud noises and bright light increased the pain in 19% of the patients. No patient spontaneously reported increased pain on visceral activity like micturition.
The same kind of stimuli that increased the pain in some patients had the opposite effect in others. However, it was less common that the pain was decreased by stimuli and this effect was also less powerful (Table V).
Non-opiate analgesics were regularly used by 5 CPSP patients due to nociceptive pain. None of the 27 patients reported having had any effect of non-opiate analgesics on their CPSP. No patient used opiate analgesics.
Non-sensory neurological signs The examination of the patients with regard to
paresis, ataxia, agnosia, apraxia, choreoathetosis,

20
TABLE VI
NON-SENSORY NEUROLOGICAL SIGNS AT THE TIME OF EXAMINATION
Paresis
Ataxia
Choreo-athetosis Agnosia
Apraxia
Dysphasia (light) Hemianopia
None
Moderate
Severe None
Moderate
Severe
Auditory
Tactile
Visual
Constructional
Ideomotor
BS
TNH_ 9)
SE UI All (N = 8) (N = 6) (N=4) (N = 27)
7 2 1 4 14 (52%)
1 4 5 0 10 (37%)
0 3 0 0 3 (11%) 5 O/6 1 3 9 (38%)
3 5/6 5 1 14 (58%)
0 l/6 0 0 1 (4%)
0 0 1 0 1 (4%) 0 O/8 O/4 O/3 0 (0%) 0 3/6 l/4 O/3 4 (19%)
0 3/8 l/4 O/3 4 (17%)
0 2/8 O/4 O/3 2 (9%)
0 O/8 O/4 O/3 0 (0%)
0 1 1 0 2 (7%) 0 4 2 0 6 (22%)
dysphasia and visual field defects showed that there were no non-sensory neurological signs com-
mon to all CPSP patients (Table VI). The most common signs were paresis and ataxia. However, even these signs were moderately to slightly devel-
oped when present, except in a few patients. At the time of the examination 52% of the CPSP patients had no paresis. Thirty-seven percent had moderate and only 11% had severe paresis (Table VI). All 3 patients with severe paresis had a large
lesion including parts of the internal capsule and the thalamus. At the onset of the stroke the corre-
sponding figures were 37% and 19% for moderate and severe paresis, respectively. Thus 44% of the patients had no paresis at all during the course of
the disease. We found moderate limb ataxia in 58% of the
24 patients in whom it could be examined (Table VI). Only 1 patient had severe ataxia. Probably the major reason why only 3 of the 8 BS patients had ataxia was the delay from the onset of the stroke to the examination, which allowed much of the ataxia to disappear.
One of the patients in the SE group had choreoathetotic movements in the hand and 1 patient in the TH group had a transient hemibal- lism.
Somatosensory symptoms and signs Quantitative and conventional clinical methods
were used to examine sensibility. The side con-
tralateral to the pain was used as a control side. In the quantitative tests the thresholds had to be at least twice as high on the affected side to be classified as raised. The sensory symptoms and signs have been reported in detail elsewhere [7; Boivie et al., in prep.], and so only a summary will be given here.
All patients had some kind of sensory
abnormality on the affected side. Its components varied, but one feature was common to all pa- tients, namely a decreased sensibility to innoxious temperatures. In 80% of the patients the defect was severe and 70% actually did not perceive temperatures at all in the 0-50°C range. Twenty- five of the 27 patients also had decreased sensibil- ity for noxious cold and heat. In the clinical examination 96% and 93%, respectively, had abnormal pin-prick and cold sensibility. There were some, but not major differences between the patient groups regarding abnormalities in temper- ature and pin-prick.
Fifty-two percent had raised thresholds to touch, but in the clinical examination with cotton wool 85% reported abnormal touch sensibility.

This figure includes 37% with hypersensitivity to the stimulus. The sensibility for touch was more severely affected in the TH patients than in the other groups. No BS patient had raised touch thresholds in the hand and foot, but two of them had raised thresholds on the cheek.
Vibrametry showed that 41% had raised thresholds. Seven of the 11 patients with de- creased vibration sensibility were TH patients. Similar relationships were found for 2-point dis- crimination and kinesthesia.
All but 3 patients reported spontaneous or evoked paresthesias and/or dysesthesias. Sponta- neous dysesthesias were most common, occurring in 85% of the patients. In 23 of the 25 patients adequately tested with regard to hypersensitivity to external somatic stimuli, some kind of hyper- sensitivity could be demonstrated. Hypersensitiv- ity to cold and pin-prick were more common than to cotton wool. Among other abnormal features found in the CPSP patients radiation of perceived stimuli (in 50%) and after-sensations (in 38%) can be mentioned.
Social relationships
At the time of the examination, 4 patients were working in their previous occupation, 10 had re- tired due to old age and 13 had retired early with a pension due to the stroke and/or other diseases. All patients regarded their economy as satisfac- tory. Twenty-one patients were married, 5 were widowed and 1 patient was single. There were considerable differences between the groups re- garding how they spent their leisure time. All BS patients were active during that time, while only 2 of 9 TH patients and 2 of 6 SE patients were active during leisure time. None of the patients was addicted to alcohol or drugs. Only 1 patient reported a major traumatic life event (in the family) during the year preceding the onset of pain.
Laboratory tests Routine cerebrospinal fluid examination (21
patients) was essentially normal.
Discussion
The present study clearly shows that central post-stroke pain can be caused not only by cerebrovascular lesions affecting the thalamus, but by CVL located suprathalamically and in the lower parts of the brain-stem, as well. The results thereby confirm and extend previously published material [11,22,32-341 and in fact indicate that only a minority of CPSP patients have CVL that affect the thalamus. Thus, the term ‘thalamic pain’ has often been used inappropriately. Furthermore, our results show that regarding the onset, character and intensity of the pain there are no uniform signs indicating that the pain originates in the brain-stem, thalamus or suprathalamus. The only sign, common to all CPSP patients besides the pain, is a disturbance of sensibility for tempera- ture and possibly for pain.
Characteristics of the CVL causing CPSP
The question whether the location of the CVL was correctly assessed is important for the conclu- sions of the present study. The localization was based on a combination of information from CT and clinical symptoms and signs. It was consid- ered important to include clinical criteria even if the CT examination showed a CVL, because pre- viously acquired CVL are sometimes found when CT examinations are made because of suspected acute strokes [35]. The present results support this view, because 6 patients had old, clinically silent CVL in the cerebral hemisphere ipsilateral to the pain.
The occurrence of bilateral CVL among the CPSP patients in the present study agrees with a literature report [35] and is not surprising, since many of them were old and had widespread atherosclerosis. The fact that 52% of the CPSP patients had a history of ischemic heart disease is an indicator of this. In deciding which hemisphere was clinically relevant, symptoms and signs other than the pain were used.
Regarding the largest subgroup, the TH group, there is no doubt that all of them had a lesion in the thalamus as revealed by CT. The topical diag- noses of the BS patients was based on clinical criteria. The fact that the ischemic CVL in the

22
brain-stem could not be demonstrated in the CT examinations is in agreement with general experi-
ence, because such CVL are usually not seen with conventional CT [lo]. Three of the patients had CVL in the cerebellum, which is common in pa-
tients with Wallenberg and other brain-stem syn-
dromes caused by ischemic stroke [12]. In the UI group the location of the CVL could
not be determined with reasonable certainty due to absence of CT verification and lack of unequiv-
ocal clinical criteria for a supra- or infratentorial lesion. Probably three of them belonged to the SE
group, but because of some uncertainty it was decided not to include them in that group.
The CT examination does not allow exact lo- calization of CVL with regard to individual path- ways and nuclei. The rough examination that could
be made showed that only the thalamic lesions correlated with known somatosensory structures. They appeared to involve the ventro-posterior
thalamic region (VP), which is the most important
relay for the ascending somatosensory pathways to the cerebral cortex. The thalamo-cortical pro- jections from VP are thought to pass in the pos- terior half of the posterior limb of the internal capsule [31]. Some of the lateral extensions of the
CVL in the TH patients reached this zone, but it was not affected by any of the suprathalamic CVL in the SE patients. However, the sensory abnor-
malities in the SE patients indicated that somato- sensory thalamo-cortical pathways or cortical centers were injured by the CVL. The sensory abnormalities in the BS patients indicated lesions
of the somatosensory pathways in those patients, too.
It cannot be excluded that the proportion of hemorrhages is somewhat underestimated in the
present study. Nevertheless the results show that CPSP is more often caused by infarctions then by hemorrhages, just as stroke is in general more frequently ischemic than hemorrhagic [40].
Features of the CPSP It is important to recognize the fact that CPSP
can start long after the onset of the stroke. The longest delay among the present patients was about 3 years, but in 78% it had started within 3 months. These delays agree with previously published stud-
ies on CPSP and other central pain conditions [22,33]. Some reports indicate that CPSP can precede other symptoms [2,21]. This was not the case in any of the present patients.
The results of the present study show that no pain features are pathognomonic for or univer-
sally present in central post-stroke pain. It is commonly a well located, severe, constant pain with fluctuations in intensity due to various exter- nal and internal stimuli. It can have many differ- ent qualities and often the patient experiences
more than one type of pain. The most common pain quality is burning, except in patients with thalamic involvement. In most patients CPSP af-
fects almost the entire side of the body, but it may be concentrated in the upper or the lower quadrant, too. The pain distribution illustrates one of the major differences between central pain and pe- ripheral neuropathic pain. It is equally common for the pain to be superficial or deep.
The most intense pain was reported by the
thalamic patients, who were also the most disabled and least active during their leisure time. The
brain-stem patients also experienced severe pain, but most of them could enjoy a full social life in spite of the pain.
Thus, for CPSP in general there are no ubiquitous pain characteristics, but some features are more common than others. Similar rela-
tionships are found, for the subgroups of CPSP patients, i.e., for the patients with lower brain-stem or supratentorial lesions with or without thalamic involvement. The lack of pathognomonic features for the respective group does not mean that their pain is identical. The results show that there are differences in the incidences of the pain qualities, the factors affecting the pain and the intensity of the pain. Our results concerning the pain in the present study agree well with previous reports
[11,13,23,32-341. The observation that none of our CPSP pa-
tients reported relief from analgesics is in agree- ment with clinical experiences of patients with
neurogenic pain [4,38,39]. In the present study there was a dominance of
men (74%) left-sided pain (67%) and a relatively low age at onset. The present patients were younger at the onset of the stroke (mean 62 year) than the

23
general stroke population. None of these dif- ferences have been mentioned in the previous literature on CPSP with the exception of the rela- tively low age found by Agnew et al. [l]. The male dominance cannot be explained by a difference in the incidence of stroke between men and women, because this is higher in women (with a mean age of 68 years) than men (with a mean age of 60 years) in Sweden [40].
One of the aims of the present study was to investigate whether any particular neurological symptoms and signs are typical for patients with CPSP. The results indicate that there is only one type of symptom common to all CPSP patients, besides pain, namely a disturbance in somatic sensibility. The non-sensory neurological symp- toms and signs in our CPSP patients agree well with the literature. Head and Holmes [25] noticed as early as 1911 that patients with thalamic pain have no or only minor motor symptoms, a notion extended to CPSP patients with suprathalamic and brain-stem lesions by Riddoch [34] and by Cassinari and Pagni [13].
The disturbance in somatic sensibility common to all the CPSP patients was not uniform across subm~~ities. The feature common to all of them was an abnormality in temperature sensibility, while about half of the patients had normal thresholds for touch and vibration [7]. Hypersensi- tivity to mechanical and/or thermal stimuli was seen in 88% of the patients. Thus the present results contradict the statement by Head and Holmes that the only constant finding of the thalamic syndrome is an excessive reaction to stimuli [25].
Based on the results from the analysis of the sensory abnormalities it was concluded that the crucial factor for the development of CPSP is a lesion of the pathways that are most important for temperature and pain sensibility [7]. In accordance with Cassinari and Pagni [13] and based on the present results, it is proposed that this pathway is the spino-th~~o-cortical pathway. Furthermore, it appears, as also mentioned by Cassinari and Pagni [13], that the level of the lesion is not crucial for the development of CPSP. Thus lesions at any
level along the passage in the lower brain-stem, the thalamus and superior to the thalamus can cause CPSP. The importance of lesions of the spino-thalamic pathways for dysesthetic central pain due to spinal cord injury was recently pointed out by BeriC et al. [5]. However, more evidence, including anatomical data, is needed before the hypothesis about the lesion responsible for CPSP can be considered to be proven. It has for instance not been possible to show anatomically which thalamo-cortical pathways or exactly which thalamic nuclei were involved in the present pa- tients.
Possible mechanisms The pathophysiolo~cal mechanisms behind
CPSP are still more difficult to determine than the anatomy of the lesions causing it. Several authors have proposed that thalamic pain and other CPSP is the result of disintegration and disinhibition in the somatosensory systems [2,13,20,21,24,25,29, 32,33,36]. Most of the investigators have favored the idea that it is caused by a removal of inhibi- tory influences via the lemniscal pathways that normally act on neurons which are crucial for pain [32,36]. The results of the present study do not contradict the notion of disinhibition, but they do not fit the idea that this disi~bition is caused by a lesion of the ‘lemniscal’ pathways (or of ‘epi- critic’ sensibility as has also been argued). On the contrary, the results show that many CPSP pa- tients have normal ‘letiscal’ sensibility, while all have abnormal temperature sensibility.
Evidently all CPSP patients have some kind of central deafferentation, which in many is partial. Therefore, there are many possibilities for creating zones with neurons that are hyperexcitable and/or spontaneously active. Conceivably, such zones could account for the kind of pain and hypersensi- tivity found in CPSP patients. Physiological stud- ies have shown that hyperactive zones are indeed present in somatosensory centers including the cortex, after peripheral and central deafferenta- tion [3,27,28].
Conclusions Most patients who suffer from central pain
caused by a stroke have extrathalamic lesions.

24
Thus the term thalamic pain is in many cases inappropriate and it is proposed that this pain condition is called central post-stroke pain.
Most patients have hypersensitivity to cuta- neous stimuli and dysesthesias. The only patho- gnomonic symptom in CPSP appears to be a sensory abnormality affecting temperature (and possible pain) sensibility. It is proposed that this kind of sensory disturbance is included as a di- agnostic criterion for CPSP in clinical practice. The sensory symptoms form the bases for a hy- pothesis that the crucial factor for the occurrence of CPSP is a lesion affecting the spino-thalamo- cortical system.
There are no ubiquitous pain characteristics among CPSP patients. Instead there is a large variation in the expression of the pain.
CPSP should be included among the diagnostic alternatives in patients who suffer pain after a stroke. The pain distribution, frequent over-reac- tions to somatic stimuli and dysesthesias support the diagnosis. It should be recognized that the pain may begin long after the stroke and that there may be no non-sensory neurological symp- toms.
Acknowledgements
The authors wish to express their thanks to Mrs. Elisabeth 6mholmer for examination of per- ceptual dysfunctions and apraxia, Mrs. Eva Blomqvist and Mrs. Gunilla Lakomaa for collec- tion of data regarding social conditions, Mrs. Gunnel Rosen for excellent technical assistance and Professor Ulf Lindblom for constructive com- ments on the manuscript.
The study was supported by grants from the County Council of Gstergotland, the Swedish As- sociation of the Neurologically Disabled and the Swedish Society for Medical Research.
References
I Agnew, D.S., Shetter, A.G., Segall, H.D. and Flom, R.A., Thalamic pain. In: J.J. Bonica, U. LindbIom and A. Iggo
(Eds.), Advances in Pain Research and Therapy, Vol. 5, Raven Press, New York, 1983, pp. 941-946.
2 Ajuraguerra, J. de, La Douleur dans les Affections du
Systeme Nerveux Central, Doin, Paris, 1937.
3 Albe-Fessard, D. and Lombard M.C., Use of an animal
model to evaluate the origin of and protection against
deafferentation pain. In: J.J. Bonica, U. Lindblom and A.
Iggo (Eds.), Advances in Pain Research and Therapy, Vol.
5, Raven Press, New York, 1983, pp. 691-700.
4 Am&r, S. and Meyerson, B.A., Lack of analgesic effect of
opioids on neuropathic and idiopathic forms of pain, Pain.
33 (1988) 11-23.
5 BeriC, A., DimitrijeviC, M.A. and Lindblom, U., Central
dysesthesia syndrome in spinal cord injury patients, Pain.
34 (1988) 109-116.
6 Biemond, A., The conduction of pain above the level of the
thalamus opticus, Arch. Neurol. Psychiat.. 75 (1956)
231-244.
7 Boivie, J.. Leijon, G. and Johansson, J., Abnormalities in
sensibility accompanying central post-stroke pain. Pain.
Suppl. 4 (1987) S405.
8 Bowsher, D., Lahuerta. J. and Brock, L., Twelve cases of
central pain, only three with thalamic lesion, Pain. Suppl. 2
(1984) S83.
9 Bruton, J.D., Shoulder pain in stroke patients with hemi-
plegia or hemiparesis following a cerebrovascular accident,
Physiotherapy, 71 (1985) 2-4.
10 Buanno, F.S., Fossel, E.T. and Kistler, J.P., Nuclear mag-
netic resonance in stroke. In: H.J.M. Bamett, J.P. Mohr.
B.J. Stein and F.M. Yatsu (Eds.), Stroke. Pathophysiology,
Diagnosis and Management, Vol. 1, Churchill Livingstone,
New York, 1986, pp. 170-180.
11 Cambier, J., Le syndrome de Dejerine-Roussy. Rev. Neu-
rol., 138 (1982) 979-988.
12 Caplan, L.R., Vertebrovascular occlusive disease. In: H.J.M.
Barnett, J.P. Mohr, B.J. Stein and F.M. Yatsu (Eds.),
Stroke. Pathophysiology, Diagnosis and Management, Vol.
1, Churchill Livingstone, New York, 1986, pp. 570-619.
13 Cassinari, V. and Pagni, C.A., Central Pain, a Neurosurgi-
cal Survey, Harvard University Press, Cambridge. MA..
1969.
14 Cesaro, P., Thalamic pain. In: J.M. Besson, G. Guilbaud
and M. Peschanski (Eds.), Thalamus and Pain. Elsevier,
Amsterdam, 1987, pp. 259-270.
15 Currier, R.D., Giies, CL. and DeJong, R.N., Some com-
ments on Wallenberg’s lateral medullary syndrome, Neu-
rology, 10 (1960) 778-791.
16 Davis, R.A. and Stokes, J.W., Neurosurgical attempts to
relieve thalamic pain, Surg. Gynecol. Obstet., 123 (1966)
371-384.
17 Dejerine, J. et Roussy, G., La syndrome thalamique. Rev.
Neurol., 14 (1906) 521-532.
18 Eriksson, S., Bemspang, B. and Fugl-Meyer, A.R., Percep- tual and motor impairment within two weeks after stroke.
A multifacto~~ statistical approach, Occup. Ther. J. Res..
7 (1987) l-25. 19 Fields, H.L. and Adams, J.E., Pain after cortical injury
relieved by electrical stimulation of the internal capsule,
Brain, 97 (1974) 169-178.

25
20 Foerster, O., Die Leitungsbahnen des Schmerzgefuhls und
die Chirurgische Behandlung der Schmerzzustande, Urban
and Schwarzenberg, Berlin, 1927.
21 Gamin, R., La douleur dam les affections organiques du
systeme nerveux central, Rev. Neurol., 68 (1937) 105-153.
22 Garcin, R., Thalamic syndrome and pain of central origin.
In: .A. Soulairac, J. Cahn and J. Charpentier (Eds.), Pain,
Academic Press, London, 1968, pp. 521-541.
23 Hamby, W..B., Reversible central pain, Arch. Neurol., 5
(1961) 528-532.
24 Hassler, R., Die zentrale Systeme des Schmerzes, Acta
Neurochir., 8 (1960) 353-423.
25 Head, H. and Holmes, G., Sensory disturbances from
cerebral lesions, Brain, 34 (1911) 102-254.
26 Leijon, G., Boivie, J. and Johansson, I., A clinical investiga-
tion of central post-stroke pain, Pain, Suppl. 4 (1987) S404.
27 Lenz, F.A., Tasker, R.R., Dostrovsky, J.O., Kwan, H.C.,
Gore&i, J., Hiruyama, T. and Murphy, J.T., Abnormal
single-unit activity recorded in the somatosensory thalamus
of a quadriplegic patient with central pain, Pain, 31 (1987)
225-236.
28 Lenz, A.F., Tasker, R.R., Dostrovsky, J.O., Kwan, H.C.,
Gore&i, J., Hiruyama, T. and Murphy, J.T., Abnormal
single-unit activity and response to stimulation in the pre-
sumed ventrocaudal nucleus of patients with central pain.
In: G. Dubner, G.F. Gebhart and M.R. Bond (Eds.), Pain
Research and Clinical Management, Vol. 3, Elsevier,
Amsterdam, 1988, 157-164.
29 Lhermitte, J., Physiologie des ganglions centraux. Les corps
stries. La couche optique. Les formations sous-thalamiques.
In: G.H. Roger and L. Binet (I%.), Trait6 de Physiologic
Normale et Pathologique, Masson, Paris, 1933, pp. 357-402.
30 Martin, J.J., Thalamic syndromes. In: P.J. Vinken and
G.W. Bruyn (Eds.), Handbook of Clinical Neurology, Vol.
2, North-Holland Publ., Amsterdam, 1969, pp. 469-496.
31 Namba, S., Wani, T., Shimizu, Y., Fujiwara, N., Namba,
Y., Nakamua, S. and Nishimoto, A., Sensory and motor
responses to deep brain stimulation. Correlation with
anatomical structures, J. Neurosurg., 63 (1985) 224-234.
32 Noordenbos, W., Pain, Elsevier, Amsterdam, 1959, pp.
43-48.
33 Pagni, C.A., Central pain due to spinal cord and brain stem
damage. In: P.D. Wall and R. Melzack (Eds.), Textbook of
Pain, Churchill Livingstone, London, 1984, pp. 481-495.
34 Riddoch, G., The clinical features of central pain, Lancet,
234 (1938) 1093-1098, 1150-1156,1205-1209.
35 Savoiardo, M., CT scanning. In: H.J.M. Bamett, J.P. Mohr,
B.J. Stein and F.M. Yatsu (Eds.), Stroke. Pathophysiology,
Diagnosis and Management, Vol. 1, Churchill Livingstone,
New York, 1986, pp. 189-219.
36 Schott, B., Laurent, B. et Mauguitre, F., Les douleurs
thalamiques: etude critique de 43 cas, Rev. Neurol., 142
(1986) 308-315.
37 Schuster, P., Beitrage zur Pathologie des Thalamus, I-III,
Arch. Psychiat. Nerve&r., 105 (1936) 358-432, 550-622,
and 106 (1937) 13-53.
38 Tasker, R., Deafferentation and nociceptive pain. In: F.
Sicuteri et al. (Eds.), Trends in Cluster Headache, Elsevier,
Amsterdam, 1987, pp. 41-48.
39 Tasker, R.R., The problem of deafferentation pain in the
management of the patient with cancer, J. Palliative Care, 2
(1987) 8-12.
40 Terent, A., A prospective epidemiological survey of
cerebrovascular disease in a Swedish community, Uppsala
J. Med. Sci., 84 (1979) 235-246.
41 Walker, A.E., The anatomical basis of the thalamic syn-
drome, J. Belg. Neurol. Psychiat., 38 (1938) 69-95.