Embed Size (px)
Citation preview
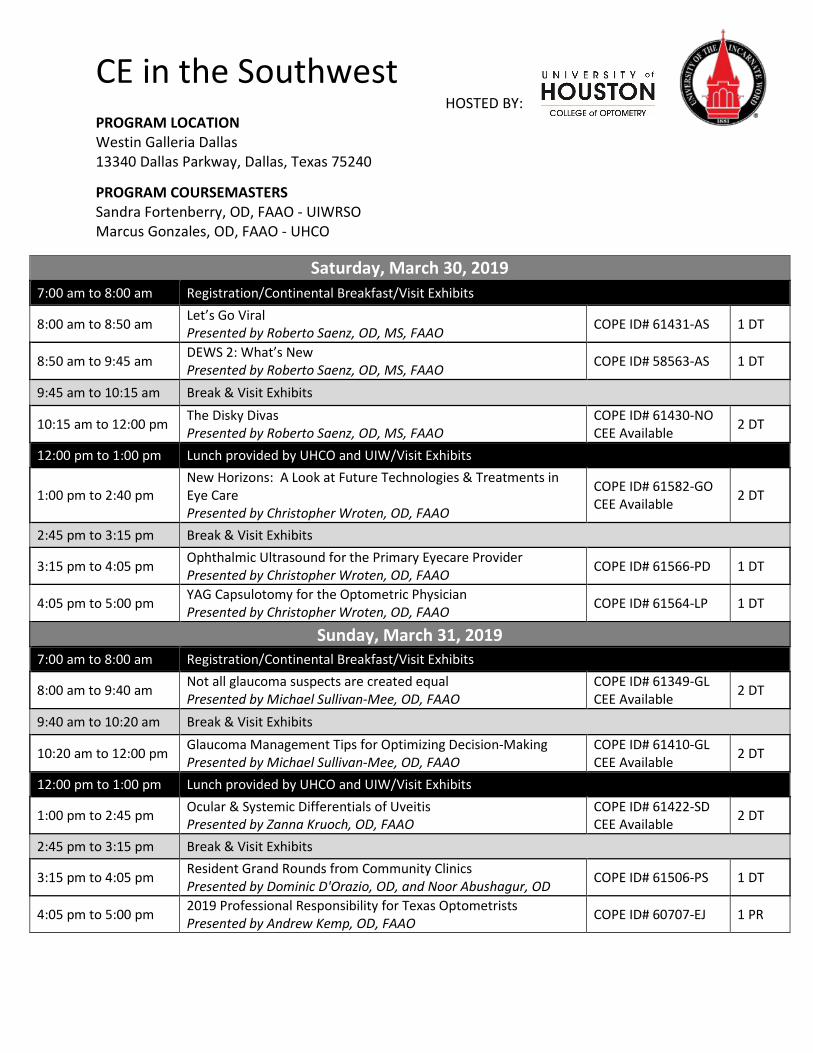
CE in the Southwest
HOSTED BY: PROGRAM LOCATION Westin Galleria Dallas 13340 Dallas Parkway, Dallas, Texas 75240
PROGRAM COURSEMASTERS Sandra Fortenberry, OD, FAAO - UIWRSO Marcus Gonzales, OD, FAAO - UHCO
Saturday, March 30, 2019
7:00 am to 8:00 am Registration/Continental Breakfast/Visit Exhibits
8:00 am to 8:50 am Let’s Go Viral Presented by Roberto Saenz, OD, MS, FAAO COPE ID# 61431-AS 1 DT
8:50 am to 9:45 am DEWS 2: What’s New Presented by Roberto Saenz, OD, MS, FAAO COPE ID# 58563-AS 1 DT
9:45 am to 10:15 am Break & Visit Exhibits
10:15 am to 12:00 pm The Disky Divas Presented by Roberto Saenz, OD, MS, FAAO
COPE ID# 61430-NO CEE Available 2 DT
12:00 pm to 1:00 pm Lunch provided by UHCO and UIW/Visit Exhibits
1:00 pm to 2:40 pm New Horizons: A Look at Future Technologies & Treatments in Eye Care Presented by Christopher Wroten, OD, FAAO
COPE ID# 61582-GO CEE Available 2 DT
2:45 pm to 3:15 pm Break & Visit Exhibits
3:15 pm to 4:05 pm Ophthalmic Ultrasound for the Primary Eyecare Provider Presented by Christopher Wroten, OD, FAAO COPE ID# 61566-PD 1 DT
4:05 pm to 5:00 pm YAG Capsulotomy for the Optometric Physician Presented by Christopher Wroten, OD, FAAO COPE ID# 61564-LP 1 DT
Sunday, March 31, 2019 7:00 am to 8:00 am Registration/Continental Breakfast/Visit Exhibits
8:00 am to 9:40 am Not all glaucoma suspects are created equal Presented by Michael Sullivan-Mee, OD, FAAO
COPE ID# 61349-GL CEE Available 2 DT
9:40 am to 10:20 am Break & Visit Exhibits
10:20 am to 12:00 pm Glaucoma Management Tips for Optimizing Decision-Making Presented by Michael Sullivan-Mee, OD, FAAO
COPE ID# 61410-GL CEE Available 2 DT
12:00 pm to 1:00 pm Lunch provided by UHCO and UIW/Visit Exhibits
1:00 pm to 2:45 pm Ocular & Systemic Differentials of Uveitis Presented by Zanna Kruoch, OD, FAAO
COPE ID# 61422-SD CEE Available 2 DT
2:45 pm to 3:15 pm Break & Visit Exhibits
3:15 pm to 4:05 pm Resident Grand Rounds from Community Clinics Presented by Dominic D'Orazio, OD, and Noor Abushagur, OD COPE ID# 61506-PS 1 DT
4:05 pm to 5:00 pm 2019 Professional Responsibility for Texas Optometrists Presented by Andrew Kemp, OD, FAAO COPE ID# 60707-EJ 1 PR
3/14/2019
1
NOT ALL GLAUCOMA SUSPECTS ARE CREATED ALIKE
Which glaucoma suspects actually have glaucoma ??
Michael Sullivan-Mee, OD, FAAO
AAO Diplomate, Glaucoma
No conflicts of interest to report
And which glaucoma suspects are actually imposters ??
CESW 2019
COURSE FOCUSPrimary Care Optometry
Glaucoma is the second leading cause of blindness,
a disability that is largely preventable if detected in
early stages
1. Maximize visual function2. Identify vision & life-
threatening conditions
GLAUCOMA EPIDEMIOLOGY
Shaikh Y, Yu F, Coleman AL. Burden of undetected and untreated glaucoma in the United States. Am J Ophthalmol 2014.Varma et al. Prevalence of open angle glaucoma and ocular hypertension in Latinos. The Los Angeles Latino Eye Study. Ophthalmology 2004.
1. Access to care2. Diagnostic failure
U.S. estimates: 50% of cases are undiagnosed
Primary Reasons
Under‐diagnosis primarily occurs in young, old, and those with poor access to healthcare
3/14/2019
2
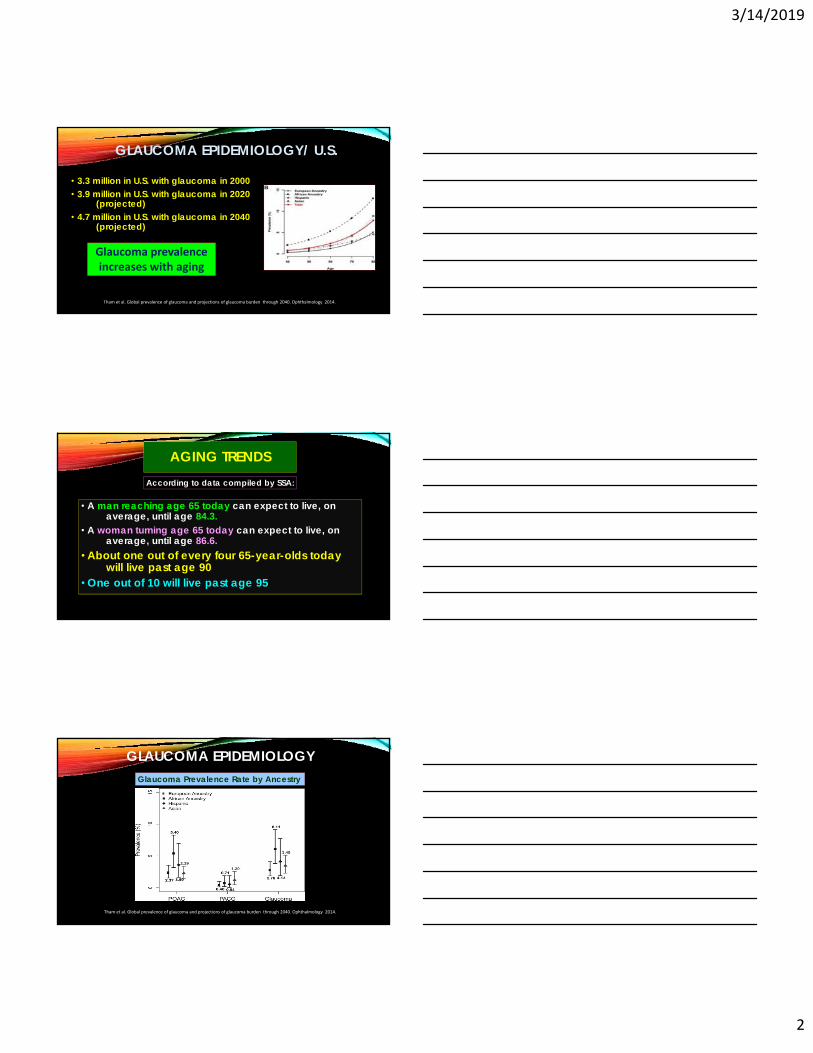
GLAUCOMA EPIDEMIOLOGY/ U.S.
• 3.3 million in U.S. with glaucoma in 2000• 3.9 million in U.S. with glaucoma in 2020
(projected)• 4.7 million in U.S. with glaucoma in 2040
(projected)
Tham et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology 2014.
Glaucoma prevalence increases with aging
AGING TRENDS
• A man reaching age 65 today can expect to live, on average, until age 84.3.
• A woman turning age 65 today can expect to live, on average, until age 86.6.
• About one out of every four 65-year-olds today will live past age 90
• One out of 10 will live past age 95
According to data compiled by SSA:
Tham et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040. Ophthalmology 2014.
Glaucoma Prevalence Rate by Ancestry
GLAUCOMA EPIDEMIOLOGY
3/14/2019
3
Keys to raising our glaucoma suspicion flag
IOP = 29,25
My Mom went blind
from glaucoma
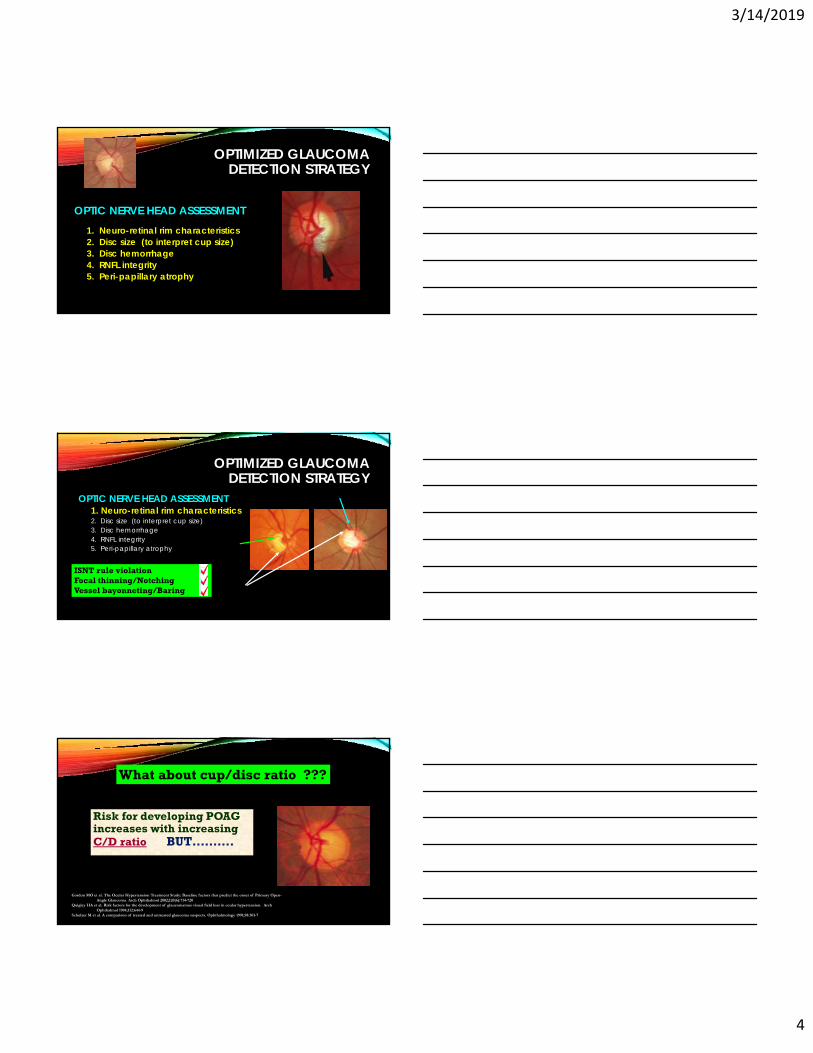
Advanced disease is generally straightforward to diagnose
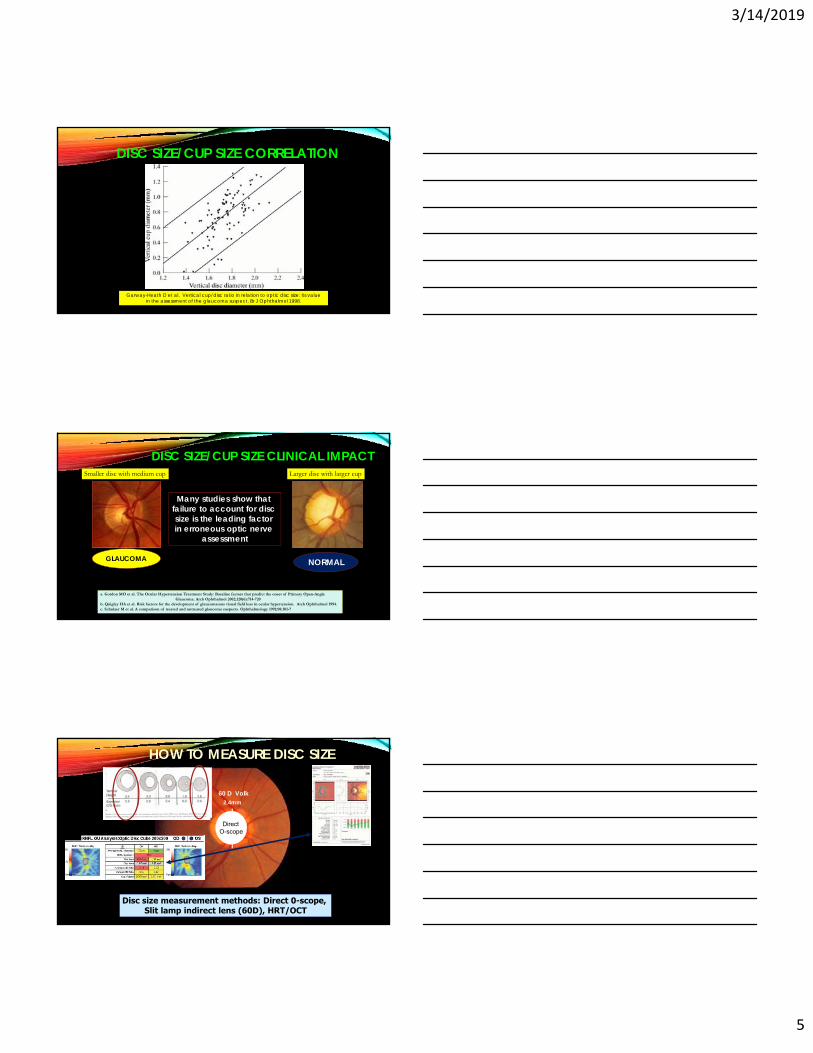
Early glaucoma, however, can be quite challenging to accurately identify
3/14/2019
4
OPTIMIZED GLAUCOMA DETECTION STRATEGY
1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
OPTIC NERVE HEAD ASSESSMENT
OPTIMIZED GLAUCOMA DETECTION STRATEGY
OPTIC NERVE HEAD ASSESSMENT 1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
ISNT rule violation Focal thinning/Notching Vessel bayonneting/Baring
Risk for developing POAG increases with increasing C/D ratio BUT……….
Gordon MO et al. The Ocular Hypertension Treatment Study: Baseline factors that predict the onset of Primary Open-Angle Glaucoma. Arch Ophthalmol 2002;120(6):714-720
Quigley HA et al. Risk factors for the development of glaucomatous visual field loss in ocular hypertension. Arch Ophthalmol 1994;112:644-9
Schulzer M et al. A comparison of treated and untreated glaucoma suspects. Ophthalmology 1991;98:301-7
What about cup/disc ratio ???
3/14/2019
5
DISC SIZE/CUP SIZE CORRELATION
Garway-Heath D et al. Vertical cup/disc ratio in relation to optic disc size: its value in the assessment of the glaucoma suspect. Br J Ophthalmol 1998.
Larger disc with larger cup
GLAUCOMA NORMAL
Smaller disc with medium cup
DISC SIZE/CUP SIZE CLINICAL IMPACT
a. Gordon MO et al. The Ocular Hypertension Treatment Study: Baseline factors that predict the onset of Primary Open-Angle Glaucoma. Arch Ophthalmol 2002;120(6):714-720
b. Quigley HA et al. Risk factors for the development of glaucomatous visual field loss in ocular hypertension. Arch Ophthalmol 1994.c. Schulzer M et al. A comparison of treated and untreated glaucoma suspects. Ophthalmology 1991;98:301-7
Many studies show that failure to account for disc size is the leading factor in erroneous optic nerve
assessment
HOW TO MEASURE DISC SIZE
Disc size measurement methods: Direct 0-scope, Slit lamp indirect lens (60D), HRT/OCT
Direct O-scope
60 D Volk2.4mm
3/14/2019
6
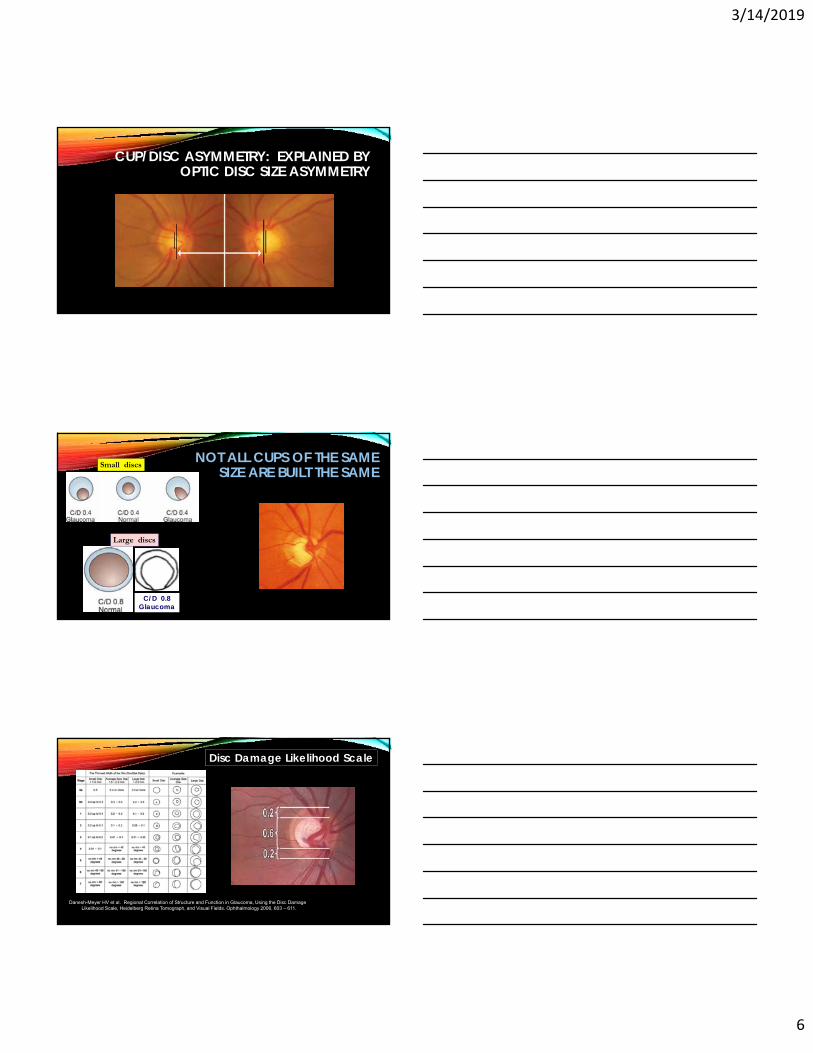
CUP/DISC ASYMMETRY: EXPLAINED BY OPTIC DISC SIZE ASYMMETRY
NOT ALL CUPS OF THE SAME SIZE ARE BUILT THE SAME
C/D 0.8Glaucoma
Small discs
Large discs
..
Danesh-Meyer HV et al. Regional Correlation of Structure and Function in Glaucoma, Using the Disc Damage Likelihood Scale, Heidelberg Retina Tomograph, and Visual Fields. Ophthalmology 2006, 603 – 611.
Disc Damage Likelihood Scale
3/14/2019
7
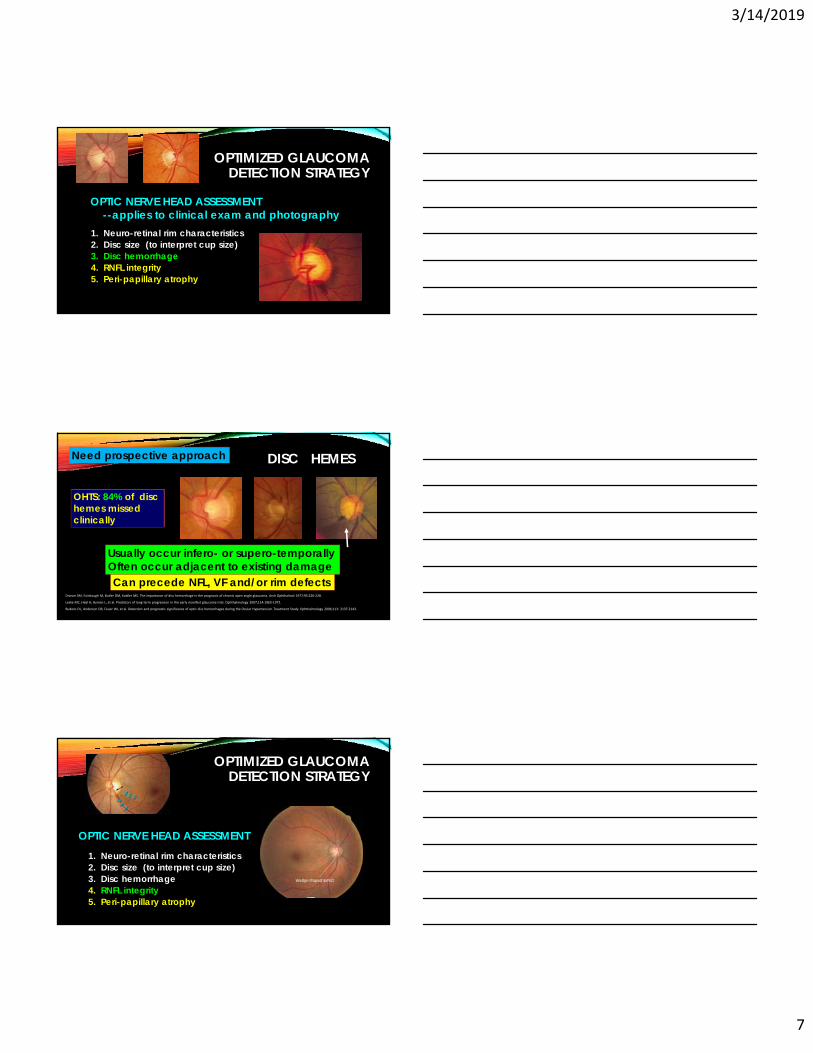
OPTIMIZED GLAUCOMA DETECTION STRATEGY
1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
OPTIC NERVE HEAD ASSESSMENT --applies to clinical exam and photography
Need prospective approach
Can precede NFL, VF and/or rim defects
Usually occur infero- or supero-temporallyOften occur adjacent to existing damage
DISC HEMES
Drance SM, Fairclough M, Butler DM, Kottler MS. The importance of disc hemorrhage in the prognosis of chronic open angle glaucoma. Arch Ophthalmol 1977;95:226‐228.
Leske MC, Heijl A, Hyman L, et al. Predictors of long‐term progression in the early manifest glaucoma trial. Ophthalmology 2007;114:1965‐1972.
Budenz DL, Anderson DR, Feuer WJ, et al. Detection and prognostic significance of optic disc hemorrhages during the Ocular Hypertension Treatment Study. Ophthalmology 2006;113: 2137‐2143.
How many disc hemes clinically missed in OHTS ?
OHTS: 84% of disc hemes missed clinically
OPTIMIZED GLAUCOMA DETECTION STRATEGY
1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
OPTIC NERVE HEAD ASSESSMENT
3/14/2019
8
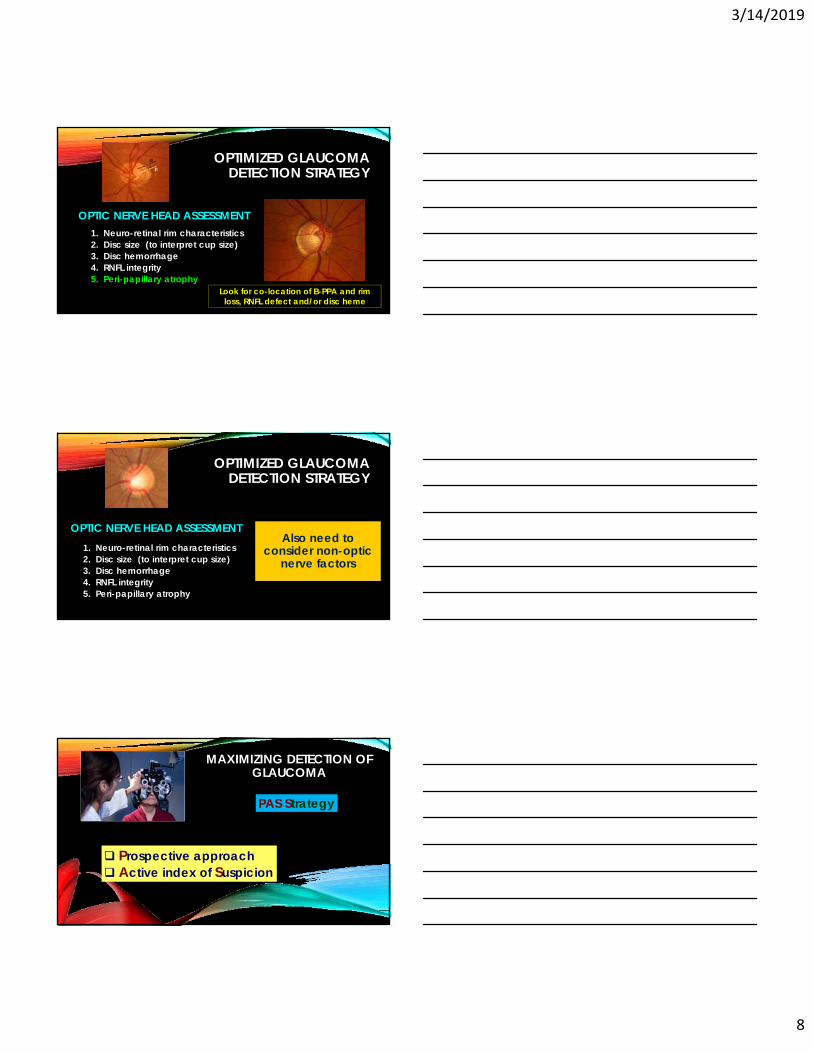
OPTIMIZED GLAUCOMA DETECTION STRATEGY
1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
OPTIC NERVE HEAD ASSESSMENT
Look for co-location of B-PPA and rim loss, RNFL defect and/or disc heme
OPTIMIZED GLAUCOMA DETECTION STRATEGY
1. Neuro-retinal rim characteristics2. Disc size (to interpret cup size)3. Disc hemorrhage4. RNFL integrity 5. Peri-papillary atrophy
OPTIC NERVE HEAD ASSESSMENT Also need to
consider non-optic nerve factors
MAXIMIZING DETECTION OF GLAUCOMA
PAS Strategy
Prospective approach Active index of Suspicion
3/14/2019
9
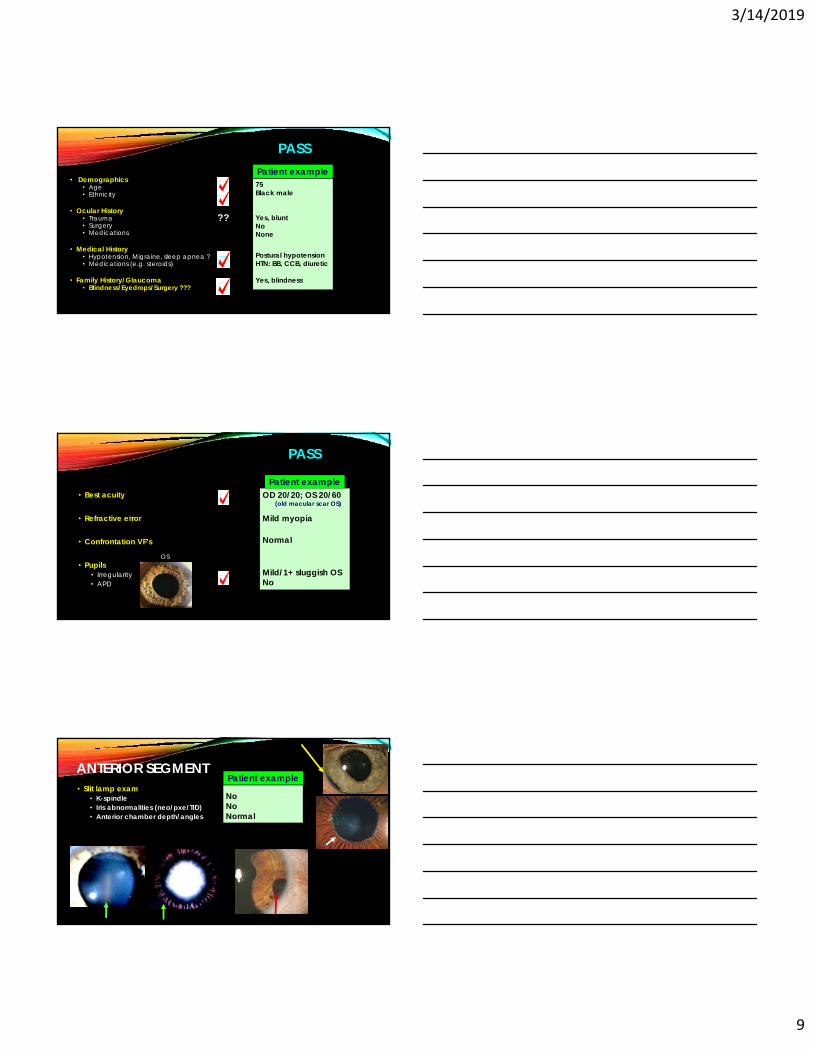
PASS
• Demographics• Age• Ethnicity
• Ocular History• Trauma• Surgery• Medications
• Medical History• Hypotension, Migraine, sleep apnea ?• Medications (e.g. steroids)
• Family History/Glaucoma• Blindness/Eyedrops/Surgery ???
75Black male
Yes, bluntNoNone
Postural hypotensionHTN: BB, CCB, diuretic
Yes, blindness
Patient example
??
• Best acuity
• Refractive error
• Confrontation VF’s
• Pupils• Irregularity• APD
OD 20/20; OS 20/60(old macular scar OS)
Mild myopia
Normal
Mild/1+ sluggish OSNo
Patient example
PASS
OS
ANTERIOR SEGMENT• Slit lamp exam
• K-spindle• Iris abnormalities (neo/pxe/TID)• Anterior chamber depth/angles
Patient example
NoNoNormal
3/14/2019
10
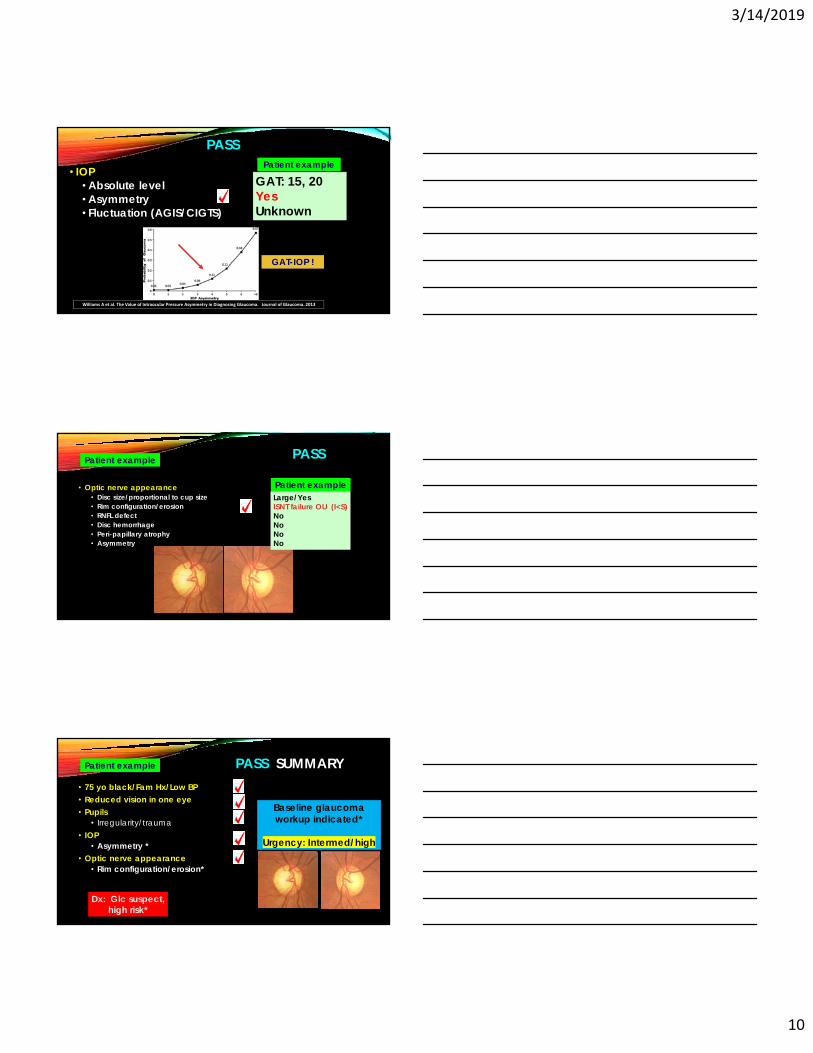
• IOP• Absolute level• Asymmetry• Fluctuation (AGIS/CIGTS)
GAT: 15, 20YesUnknown
Patient example
PASS
Williams A et al. The Value of Intraocular Pressure Asymmetry in Diagnosing Glaucoma. Journal of Glaucoma. 2013
GAT-IOP !
• Optic nerve appearance• Disc size/proportional to cup size• Rim configuration/erosion• RNFL defect• Disc hemorrhage• Peri-papillary atrophy• Asymmetry
Patient exampleLarge/YesISNT failure OU (I<S)NoNoNoNo
PASSPatient example
PASS SUMMARY• 75 yo black/Fam Hx/Low BP • Reduced vision in one eye• Pupils
• Irregularity/trauma• IOP
• Asymmetry *• Optic nerve appearance
• Rim configuration/erosion*
Patient example
Baseline glaucoma workup indicated*
Urgency: Intermed/high
Dx: Glc suspect, high risk*
3/14/2019
11
• Elevated or asymmetric IOP• Slit lam finding
• Shallow anterior chamber/angle• K-spindle/Iris transillumination defect• Pseudoexfoliation material• Irisneovascularization/mass
• ANYAngleclosureconcern
• Any optic nerve clinical suspicion*
NOT ALL GLAUCOMA SUSPECTS ARE CREATED ALIKE
Summary: Who needs baseline GLAUCOMA workup ?
ANY CRITICAL FINDING CUMULATIVE HAZARD• Combination of minor risk factors
BASELINE GLAUCOMA SUSPECT WORKUP
• GAT-IOP• GONIOSCOPY (4-mirror; compression)• Pachymetry• VF test (24-2 vs FDT-matrix vs HEP vs Octopus)• Optic nerve photography (preferably stereo)• OCT
• RNFL• Disc*• Macula*
BASELINE GLAUCOMA SUSPECT WORKUP
• GAT-IOP
Sullivan-Mee M1, Gerhardt G, Halverson KD, Qualls C. Repeatability and reproducibility for intraocular pressure measurement by dynamic contour, ocular response analyzer, and goldmann applanation tonometry. J Glaucoma. 2009 Dec;18(9):666-73
World Glaucoma Association consensus statements:1. Goldmann applanation tonometry is more precise (lowest measurement variability),
compared to other methods.2. Intraobserver variability: 2.5 mmHg (two readings by the same observer
will be within this figure for 95% of subjects)Interobserver variability: ± 4 mmHg (95% confidence limits either
side of mean difference between observers)(In clinical practice these figures may be considerably higher )
3/14/2019
12
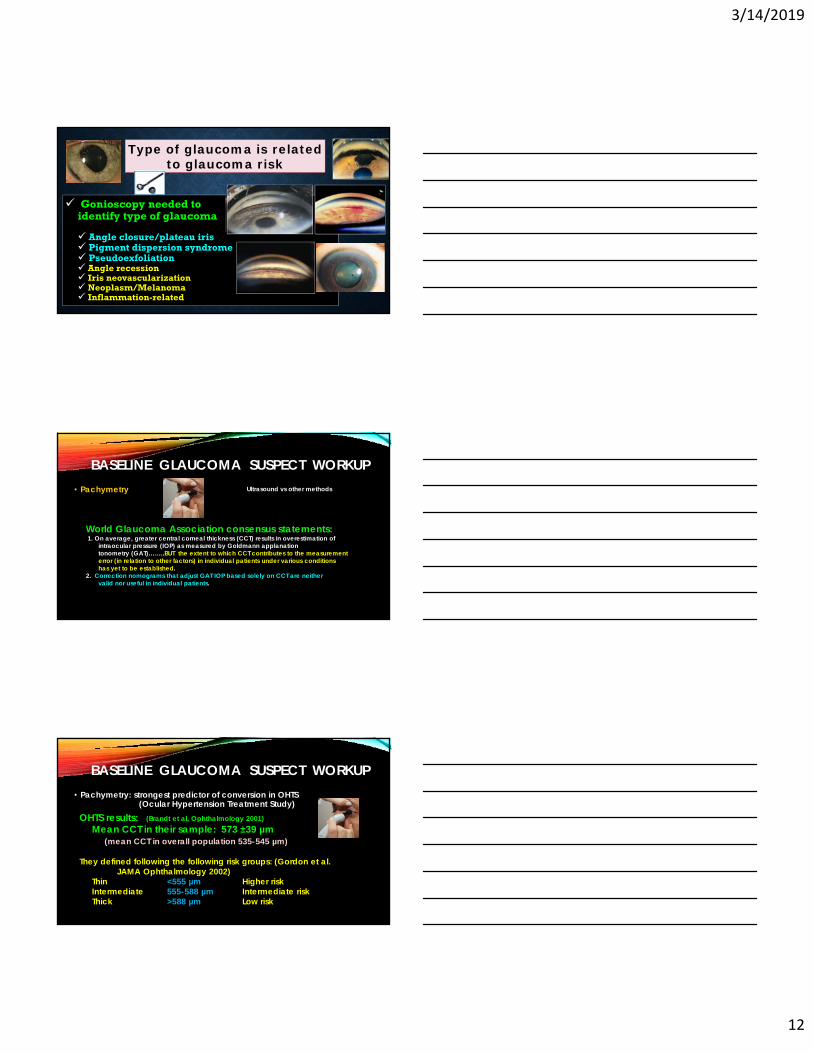
Type of glaucoma is related to glaucoma risk
Gonioscopy needed to identify type of glaucoma
Angle closure/plateau iris Pigment dispersion syndrome Pseudoexfoliation Angle recession Iris neovascularization Neoplasm/Melanoma Inflammation-related
BASELINE GLAUCOMA SUSPECT WORKUP• Pachymetry
World Glaucoma Association consensus statements:1. On average, greater central corneal thickness (CCT) results in overestimation of
intraocular pressure (IOP) as measured by Goldmann applanationtonometry (GAT)……..BUT the extent to which CCT contributes to the measurement error (in relation to other factors) in individual patients under various conditionshas yet to be established.
2. Correction nomograms that adjust GAT IOP based solely on CCT are neithervalid nor useful in individual patients.
Ultrasound vs other methods
BASELINE GLAUCOMA SUSPECT WORKUP• Pachymetry: strongest predictor of conversion in OHTS
OHTS results: (Brandt et al, Ophthalmology 2001)Mean CCT in their sample: 573 ±39 µm
(mean CCT in overall population 535-545 µm)
They defined following the following risk groups: (Gordon et al. JAMA Ophthalmology 2002)
Thin <555 µm Higher riskIntermediate 555-588 µm Intermediate riskThick >588 µm Low risk
(Ocular Hypertension Treatment Study)
3/14/2019
13
BASELINE GLAUCOMA SUSPECT WORKUP
• VF test (24-2 vs FDT-matrix vs HEP vs Octopus)• Optic nerve photography (preferably stereo)
• OCT• RNFL• Disc*• Macula*
Optical coherence tomography• Fast• Objective• Quantitative• Repeatable
Anatomic structures of interest• RNFL• Macula• Neuro-retinal rim
OPTIMIZED GLAUCOMA DETECTION STRATEGY
• Diagnostic accuracy: expert-level performance• Vessani RM et al. Comparison of quantitative imaging devices and subjective optic nerve
head assessment by general ophthalmologists to differentiate normal from glaucomatous eyes. J Glaucoma 2009.
• Azuara-Blanco A et al. Clinical agreement among glaucoma experts in the detection of glaucomatous changes of the optic disk using simultaneous stereoscopic photographs. Am J Ophthalmol 2003.
• Improves consistency in optic nerve assessment• Almazroa A et al. Agreement among ophthalmologists in marking the optic disc and optic
cup in fundus images. Int Ophthalmol 2016.• Abrams LS, Scott IU, Spaeth GL, Quigley HA, Varma R Agreement among optometrists,
ophthalmologists, and residents in evaluating the optic disc for glaucoma. Ophthalmology 1994 Oct;101(10):1662-7.
WHAT DOES SD-OCT DO FOR US ?
3/14/2019
14
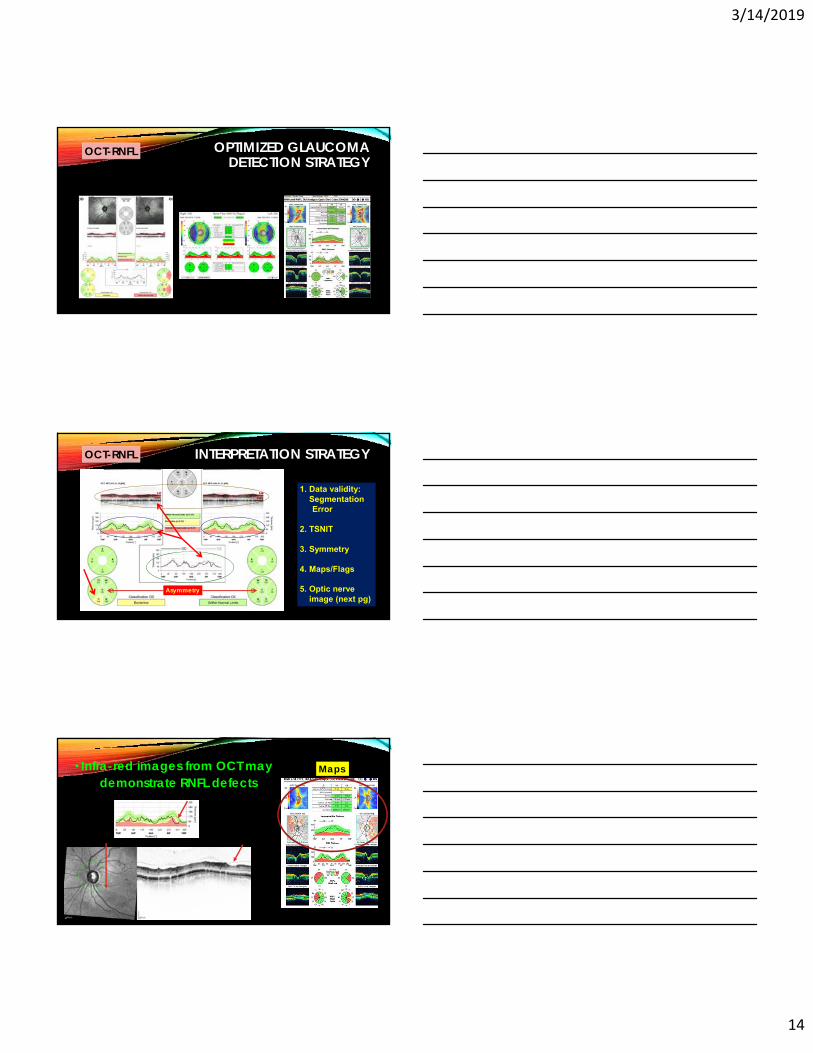
OCT-RNFL OPTIMIZED GLAUCOMA DETECTION STRATEGY
INTERPRETATION STRATEGY
Asymmetry
1. Data validity: Segmentation Error
2. TSNIT
3. Symmetry
4. Maps/Flags
5. Optic nerve image (next pg)
OCT-RNFL
• Infra-red images from OCT may demonstrate RNFL defects
Maps
3/14/2019
15
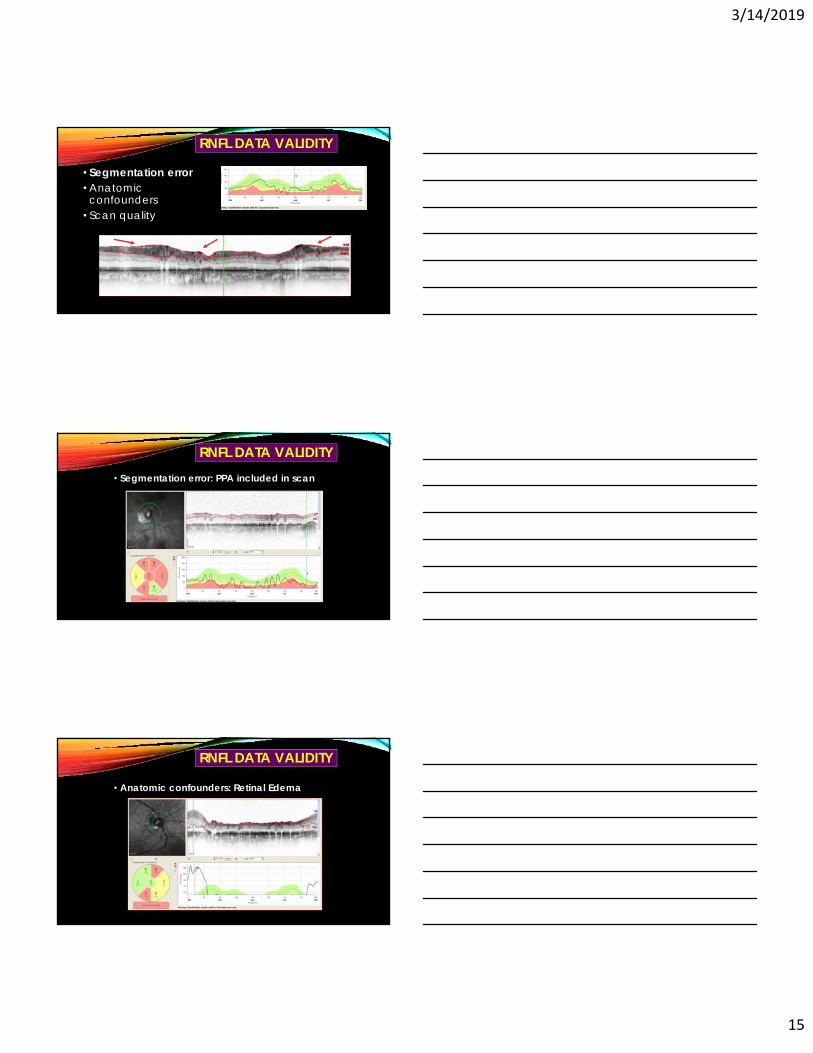
RNFL DATA VALIDITY
• Segmentation error• Anatomic
confounders• Scan quality
• Segmentation error: PPA included in scan
RNFL DATA VALIDITY
• Anatomic confounders: Retinal Edema
RNFL DATA VALIDITY
3/14/2019
16
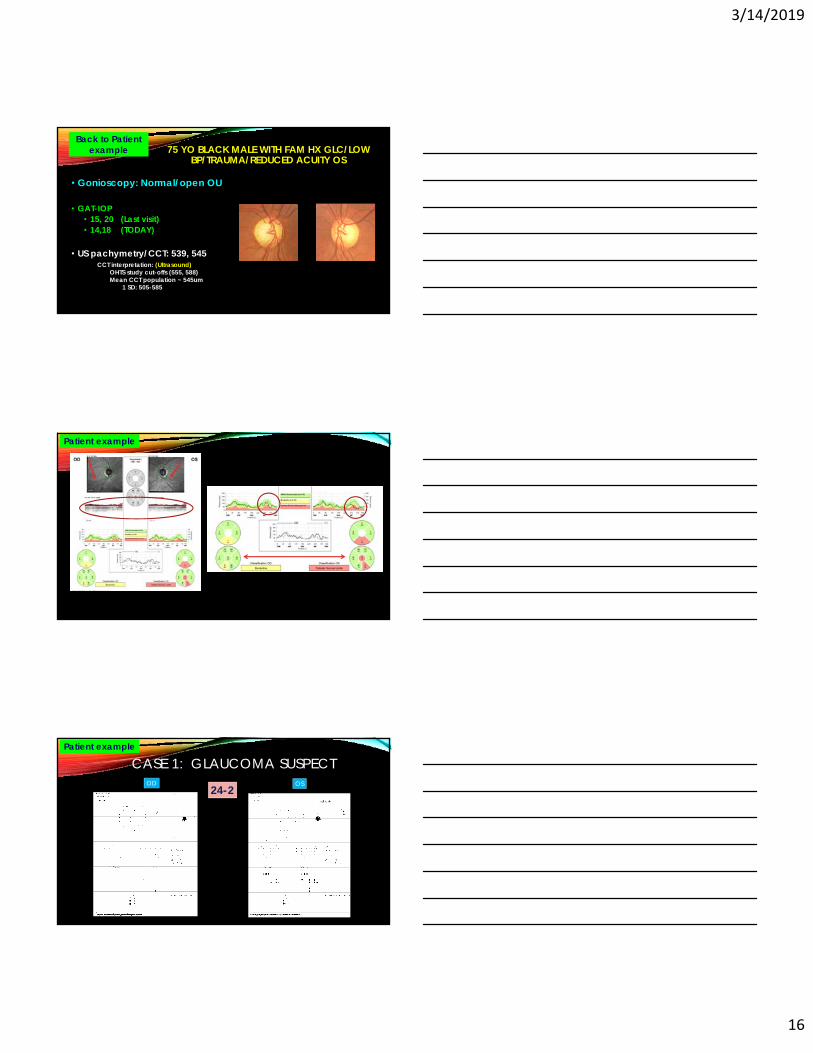
75 YO BLACK MALE WITH FAM HX GLC/LOW BP/TRAUMA/REDUCED ACUITY OS
• Gonioscopy: Normal/open OU
• GAT-IOP• 15, 20 (Last visit)• 14,18 (TODAY)
• US pachymetry/CCT: 539, 545
Back to Patient example
CCT interpretation: (Ultrasound)OHTS study cut-offs (555, 588)Mean CCT population ~ 545um
1 SD: 505-585
Patient example
OD OS24-2
CASE 1: GLAUCOMA SUSPECTPatient example
3/14/2019
17
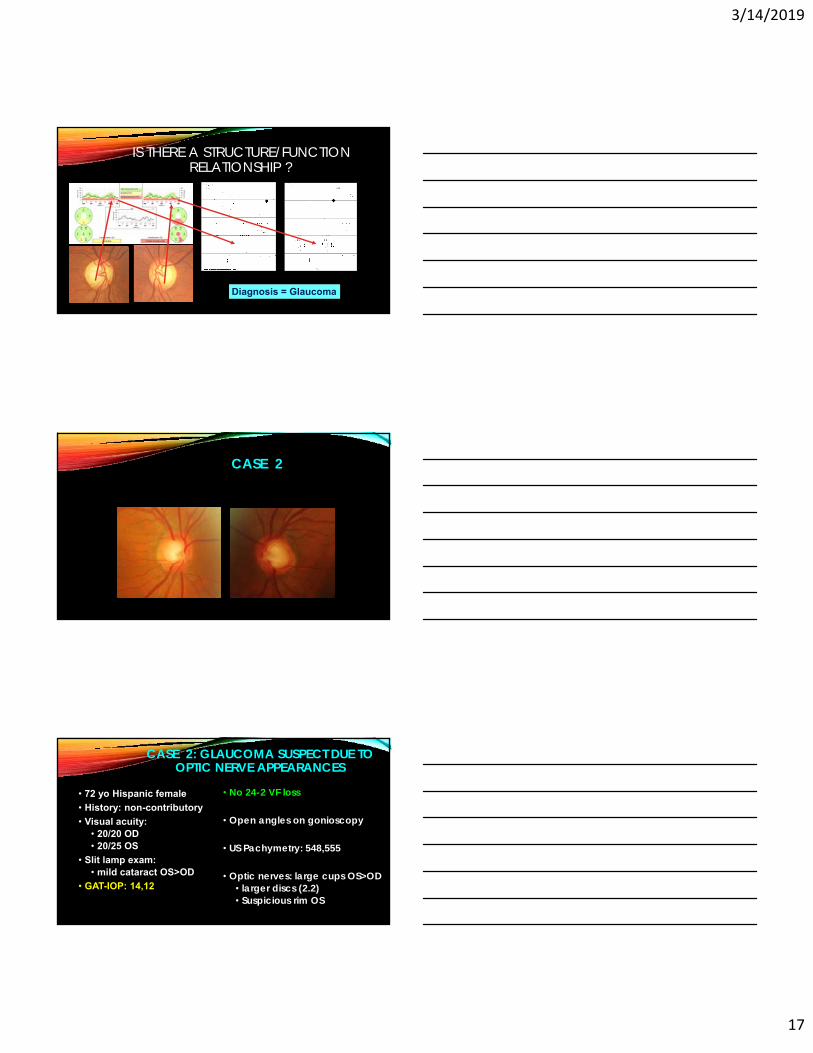
IS THERE A STRUCTURE/FUNCTION RELATIONSHIP ?
Diagnosis = Glaucoma
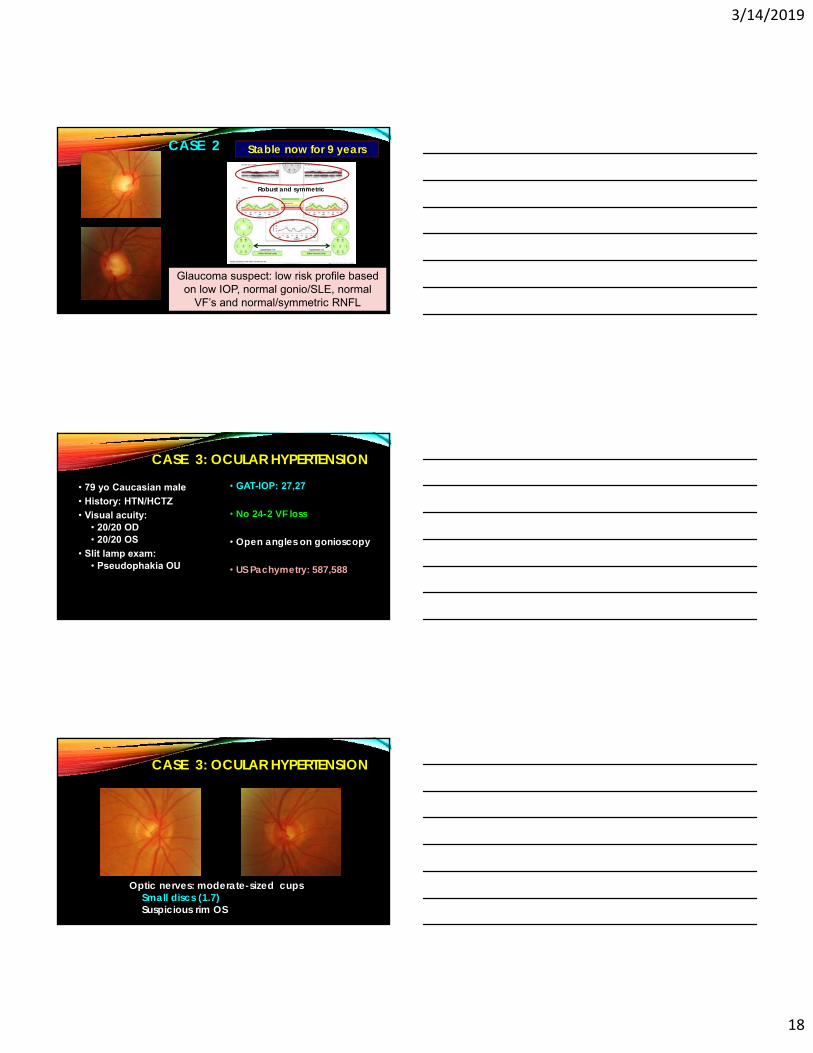
CASE 2
CASE 2: GLAUCOMA SUSPECT DUE TO OPTIC NERVE APPEARANCES
• 72 yo Hispanic female
• History: non-contributory
• Visual acuity: • 20/20 OD• 20/25 OS
• Slit lamp exam: • mild cataract OS>OD
• GAT-IOP: 14,12
• No 24-2 VF loss
• Open angles on gonioscopy
• US Pachymetry: 548,555
• Optic nerves: large cups OS>OD• larger discs (2.2)• Suspicious rim OS
3/14/2019
18
CASE 2
rnfl
Glaucoma suspect: low risk profile based on low IOP, normal gonio/SLE, normal
VF’s and normal/symmetric RNFL
Robust and symmetric
Stable now for 9 years
• 79 yo Caucasian male
• History: HTN/HCTZ
• Visual acuity: • 20/20 OD• 20/20 OS
• Slit lamp exam: • Pseudophakia OU
• GAT-IOP: 27,27
• No 24-2 VF loss
• Open angles on gonioscopy
• US Pachymetry: 587,588
CASE 3: OCULAR HYPERTENSION
CASE 3: OCULAR HYPERTENSION
Optic nerves: moderate-sized cupsSmall discs (1.7)Suspicious rim OS
3/14/2019
19
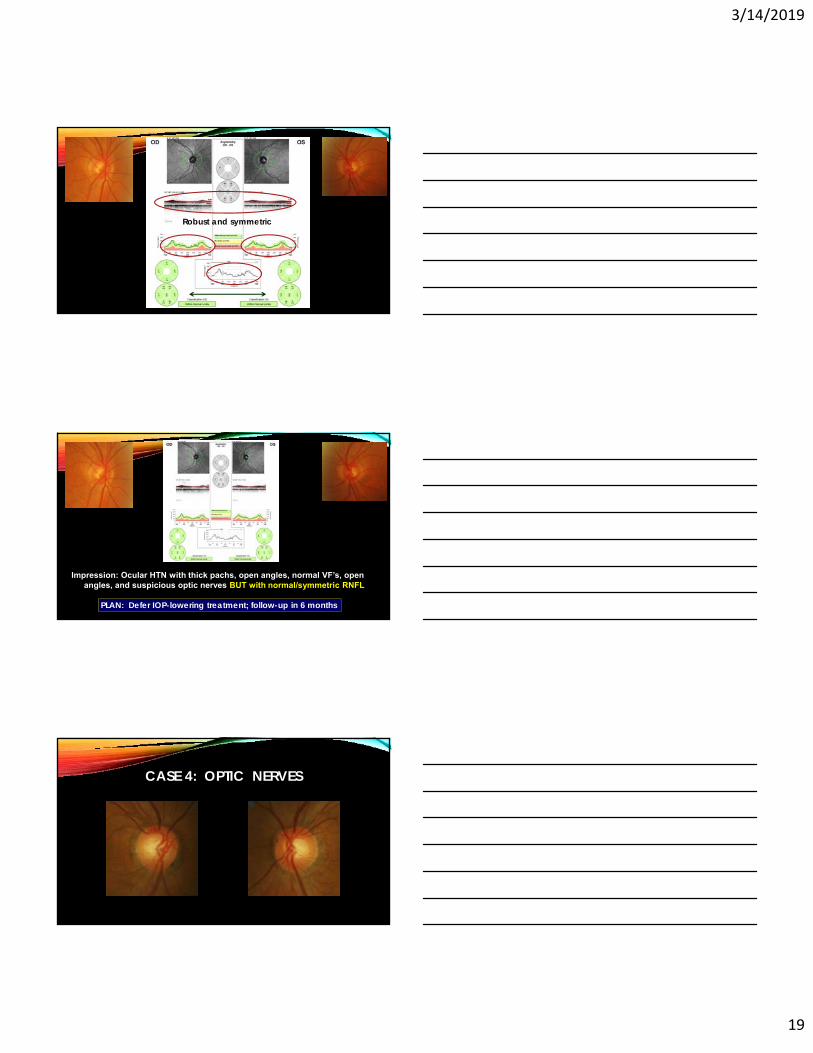
CASE 3
Put in oct-rnflRobust and symmetric
CASE 3
Put in oct-rnfl
Impression: Ocular HTN with thick pachs, open angles, normal VF’s, open angles, and suspicious optic nerves BUT with normal/symmetric RNFL
PLAN: Defer IOP-lowering treatment; follow-up in 6 months
CASE 4: OPTIC NERVES
3/14/2019
20
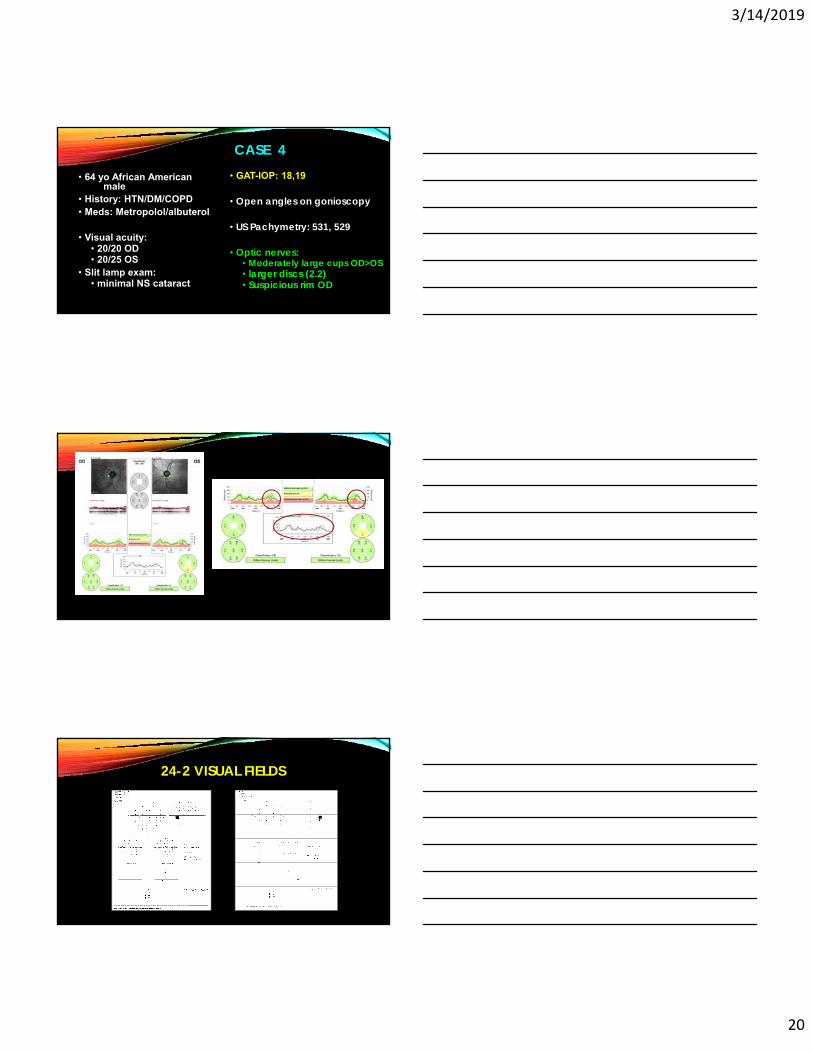
CASE 4
• 64 yo African American male
• History: HTN/DM/COPD• Meds: Metropolol/albuterol
• Visual acuity: • 20/20 OD• 20/25 OS
• Slit lamp exam: • minimal NS cataract
• GAT-IOP: 18,19
• Open angles on gonioscopy
• US Pachymetry: 531, 529
• Optic nerves: • Moderately large cups OD>OS• larger discs (2.2)• Suspicious rim OD
24-2 VISUAL FIELDS
3/14/2019
21
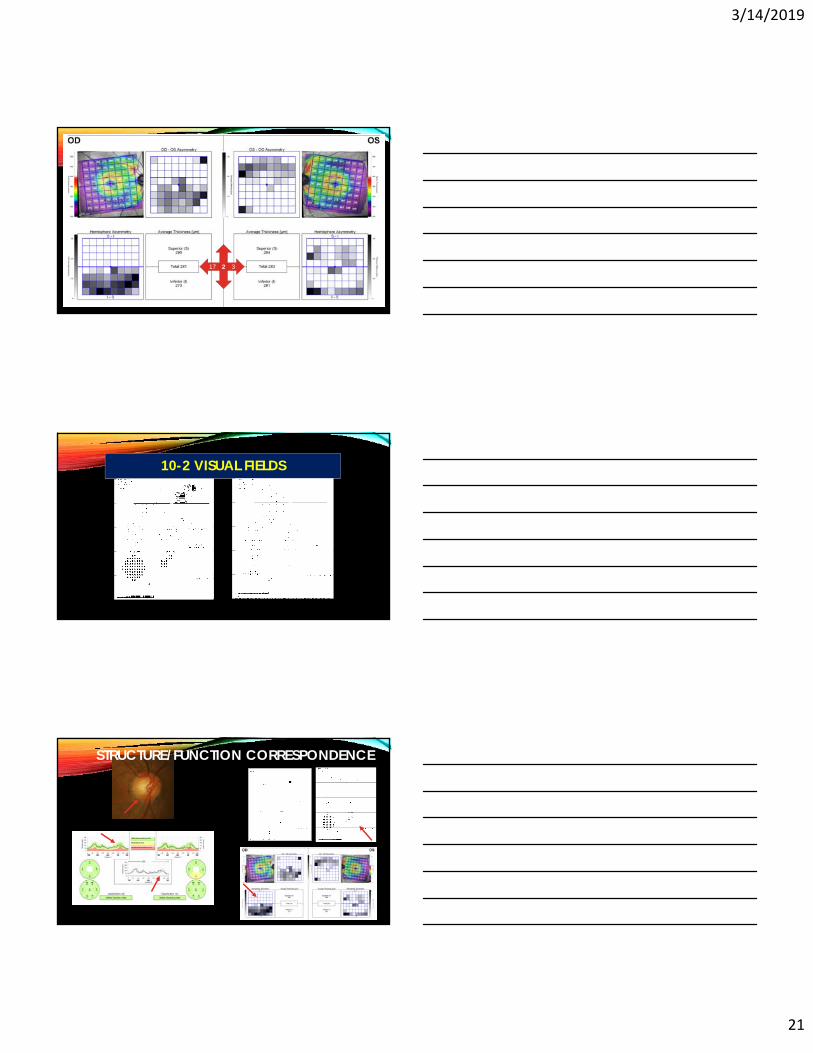
17 32
10-2 VISUAL FIELDS
STRUCTURE/FUNCTION CORRESPONDENCE
3/14/2019
22
OPTIMIZED GLAUCOMA DETECTION STRATEGY MACULA-OCT
OD
OS
94 8
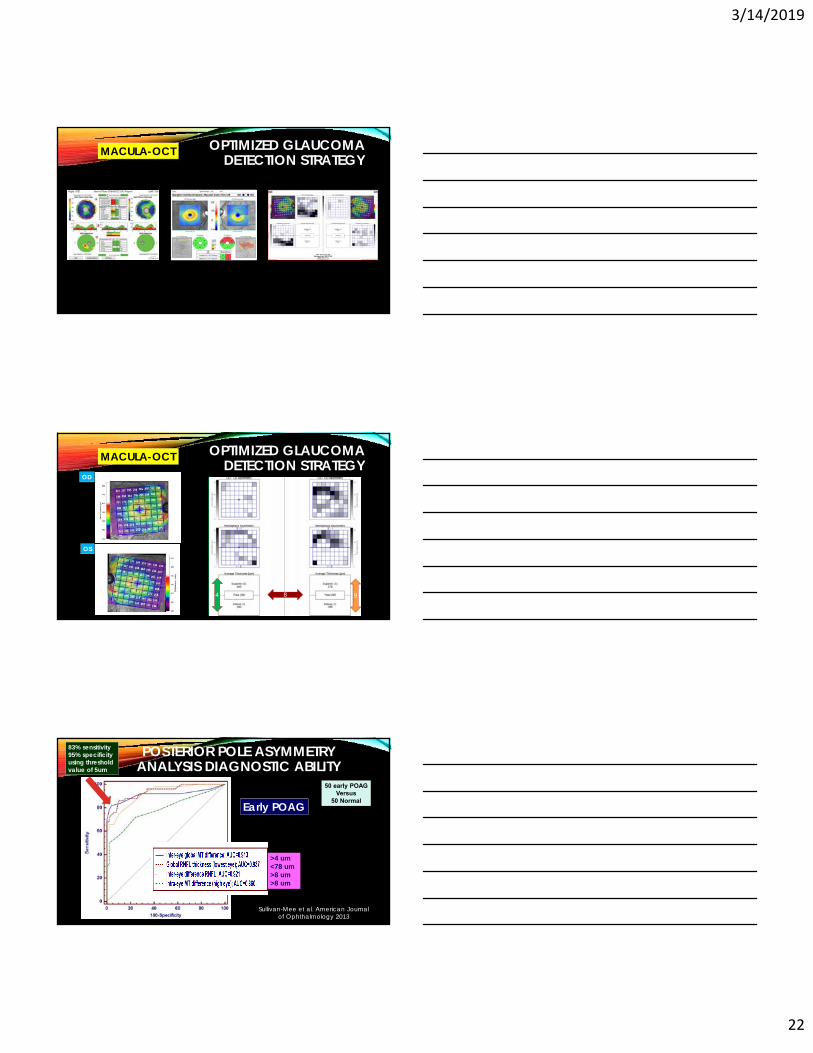
OPTIMIZED GLAUCOMA DETECTION STRATEGY MACULA-OCT
POSTERIOR POLE ASYMMETRY ANALYSIS DIAGNOSTIC ABILITY
50 early POAGVersus
50 Normal
83% sensitivity95% specificityusing threshold value of 5um
Sullivan-Mee et al. American Journalof Ophthalmology 2013
Early POAG
>4 um<78 um>8 um>8 um
3/14/2019
23
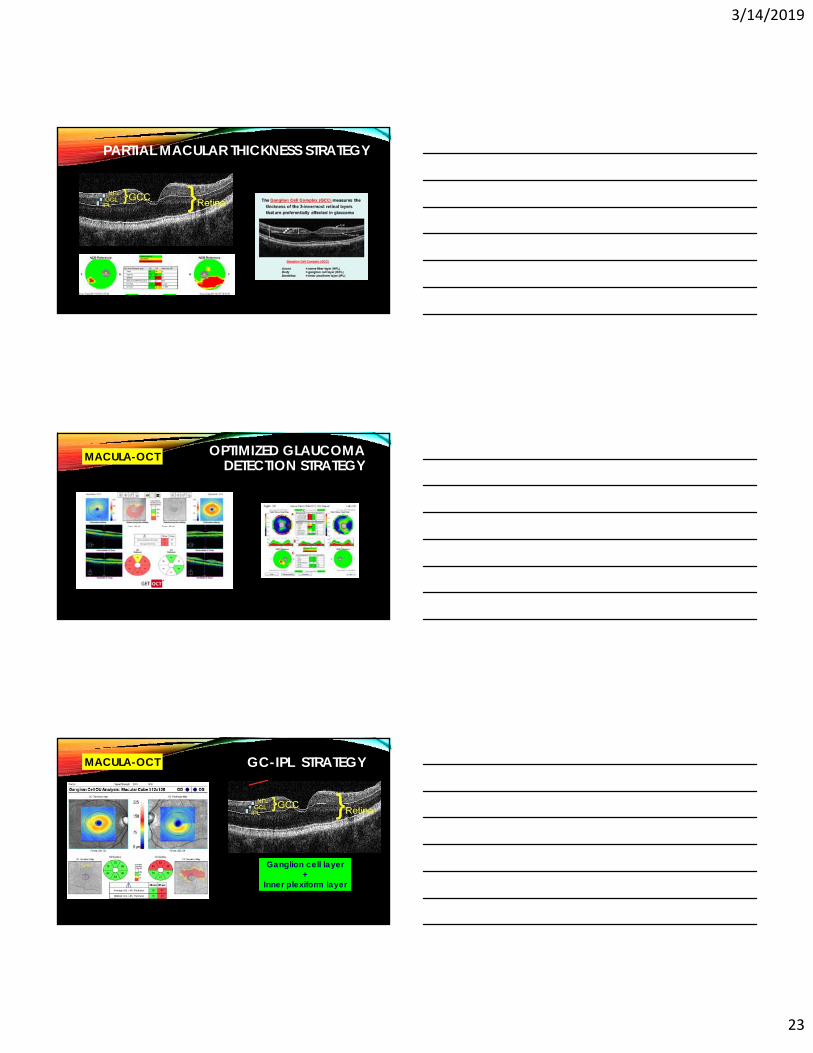
PARTIAL MACULAR THICKNESS STRATEGY
OPTIMIZED GLAUCOMA DETECTION STRATEGY MACULA-OCT
MACULA-OCT
Ganglion cell layer +
Inner plexiform layer
GC-IPL STRATEGY
3/14/2019
24
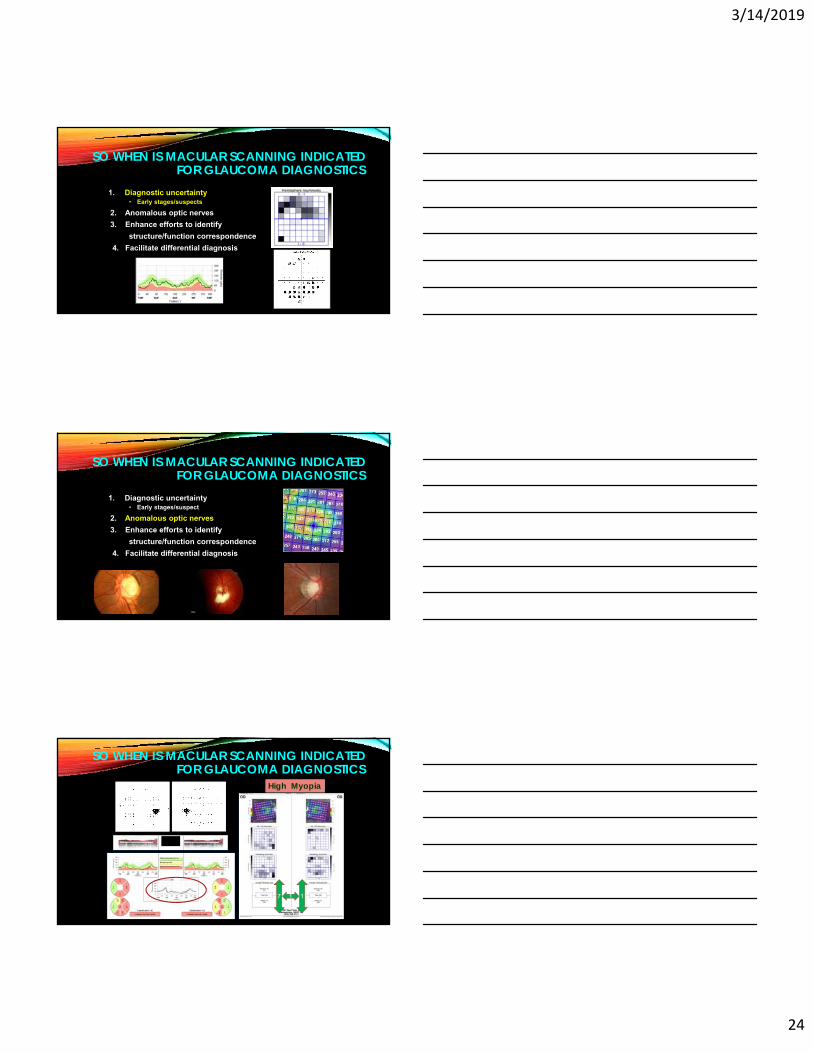
1. Diagnostic uncertainty• Early stages/suspects
2. Anomalous optic nerves
3. Enhance efforts to identify
structure/function correspondence
4. Facilitate differential diagnosis
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
1. Diagnostic uncertainty• Early stages/suspect
2. Anomalous optic nerves
3. Enhance efforts to identify
structure/function correspondence
4. Facilitate differential diagnosis
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
High Myopia
xxxx
7 11
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
3/14/2019
25
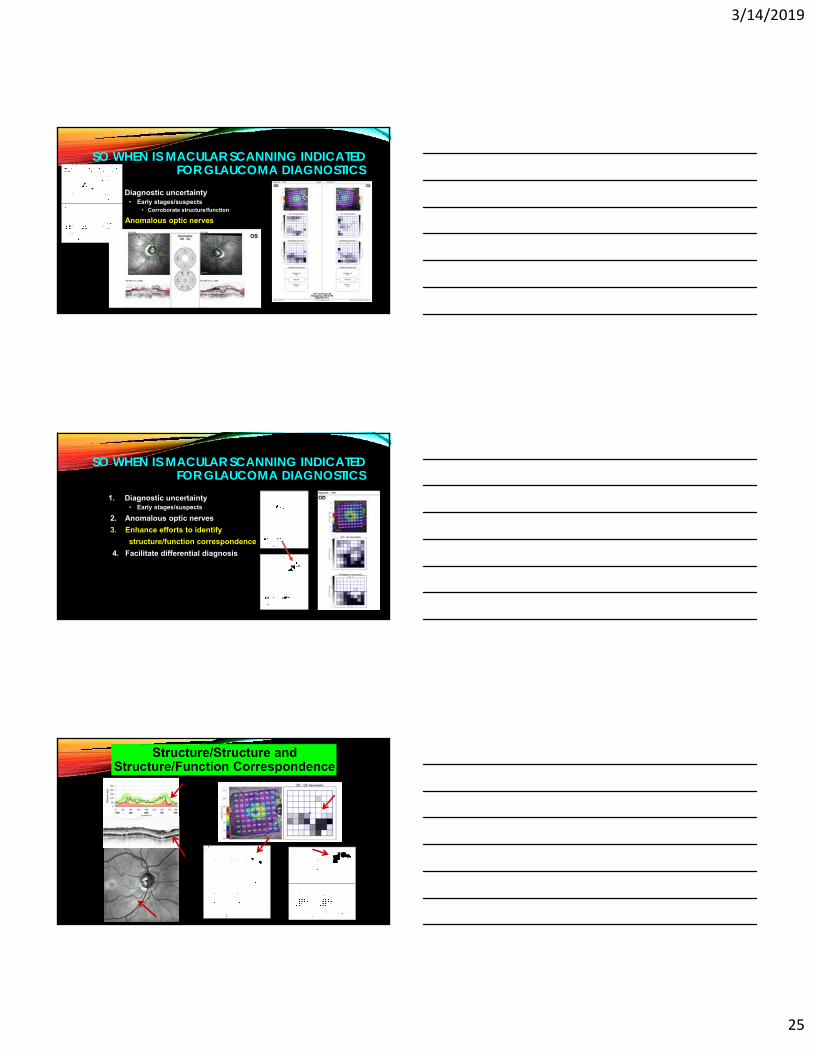
1. Diagnostic uncertainty• Early stages/suspects
• Corroborate structure/function
2. Anomalous optic nerves
3. Enhance efforts to identify
structure/function correspondence
4. Facilitate differential diagnosis
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
1. Diagnostic uncertainty• Early stages/suspects
2. Anomalous optic nerves
3. Enhance efforts to identify
structure/function correspondence
4. Facilitate differential diagnosis
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
3/14/2019
26
1. Diagnostic uncertainty• Early stages/suspects
2. Anomalous optic nerves
3. Enhance efforts to identify
structure/function correspondence
4. Facilitate differential diagnosis
SO WHEN IS MACULAR SCANNING INDICATED FOR GLAUCOMA DIAGNOSTICS
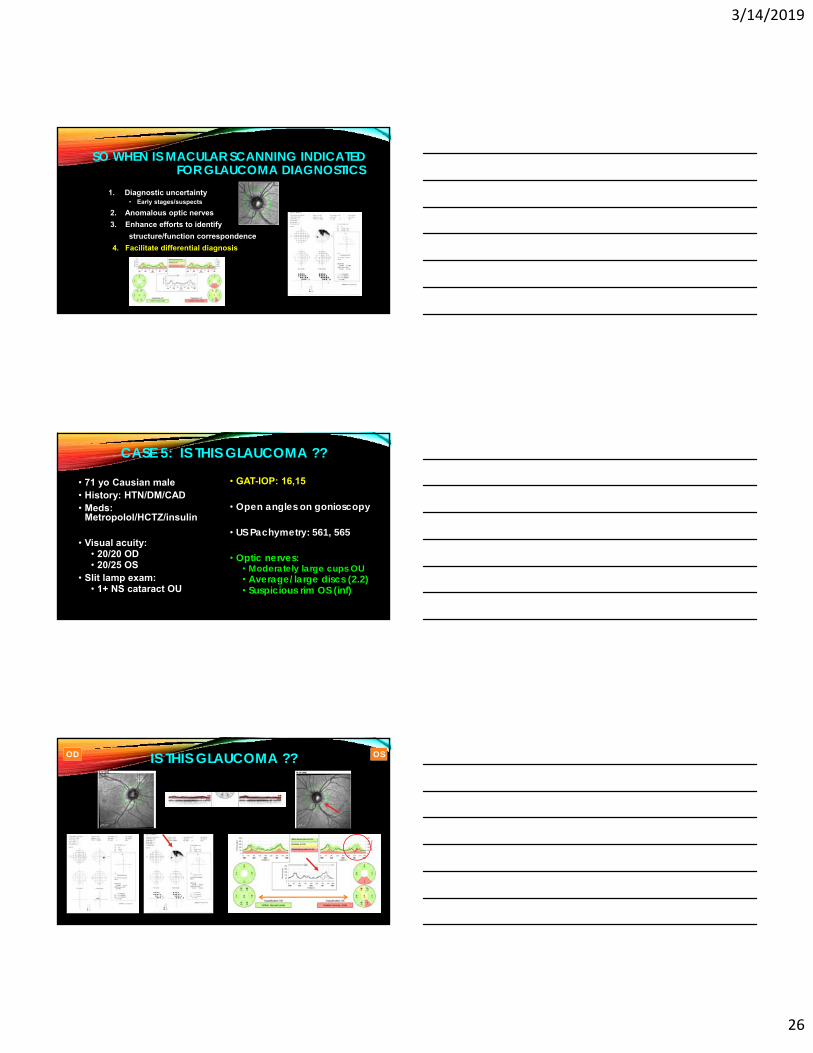
• 71 yo Causian male• History: HTN/DM/CAD• Meds:
Metropolol/HCTZ/insulin
• Visual acuity: • 20/20 OD• 20/25 OS
• Slit lamp exam: • 1+ NS cataract OU
• GAT-IOP: 16,15
• Open angles on gonioscopy
• US Pachymetry: 561, 565
• Optic nerves: • Moderately large cups OU• Average/large discs (2.2)• Suspicious rim OS (inf)
CASE 5: IS THIS GLAUCOMA ??
IS THIS GLAUCOMA ??OD OS
3/14/2019
27
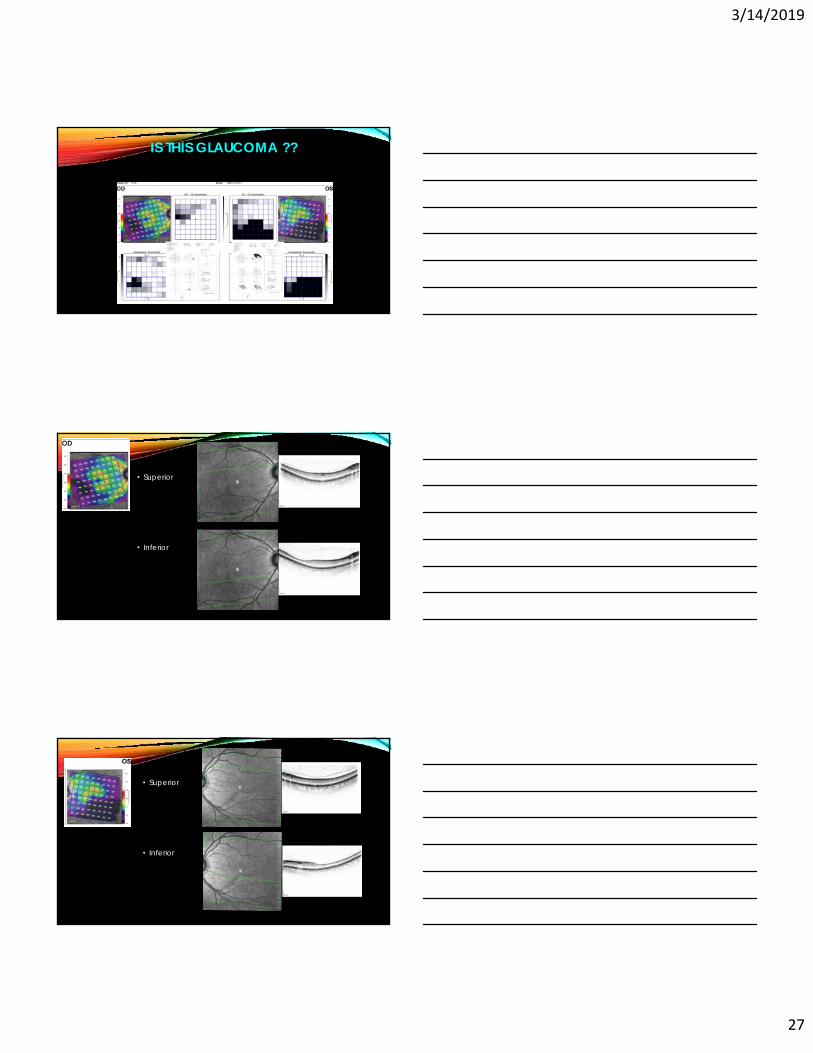
IS THIS GLAUCOMA ??
• Superior
• Inferior
• Superior
• Inferior
3/14/2019
28
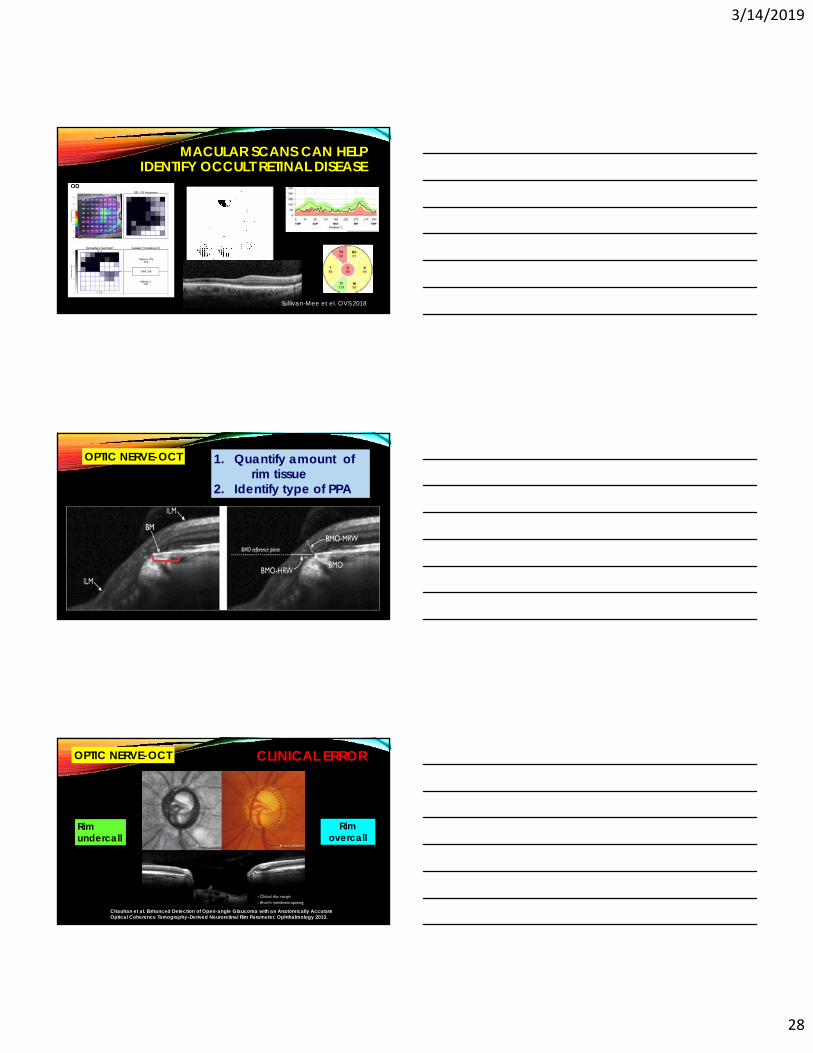
MACULAR SCANS CAN HELP IDENTIFY OCCULT RETINAL DISEASE
Sullivan-Mee et el. OVS 2018
1. Quantify amount of rim tissue
2. Identify type of PPA
OPTIC NERVE-OCT
Rim undercall
Rim overcall
Chauhan et al. Enhanced Detection of Open-angle Glaucoma with an Anatomically Accurate Optical Coherence Tomography–Derived Neuroretinal Rim Parameter. Ophthalmology 2013.
CLINICAL ERROROPTIC NERVE-OCT
3/14/2019
29
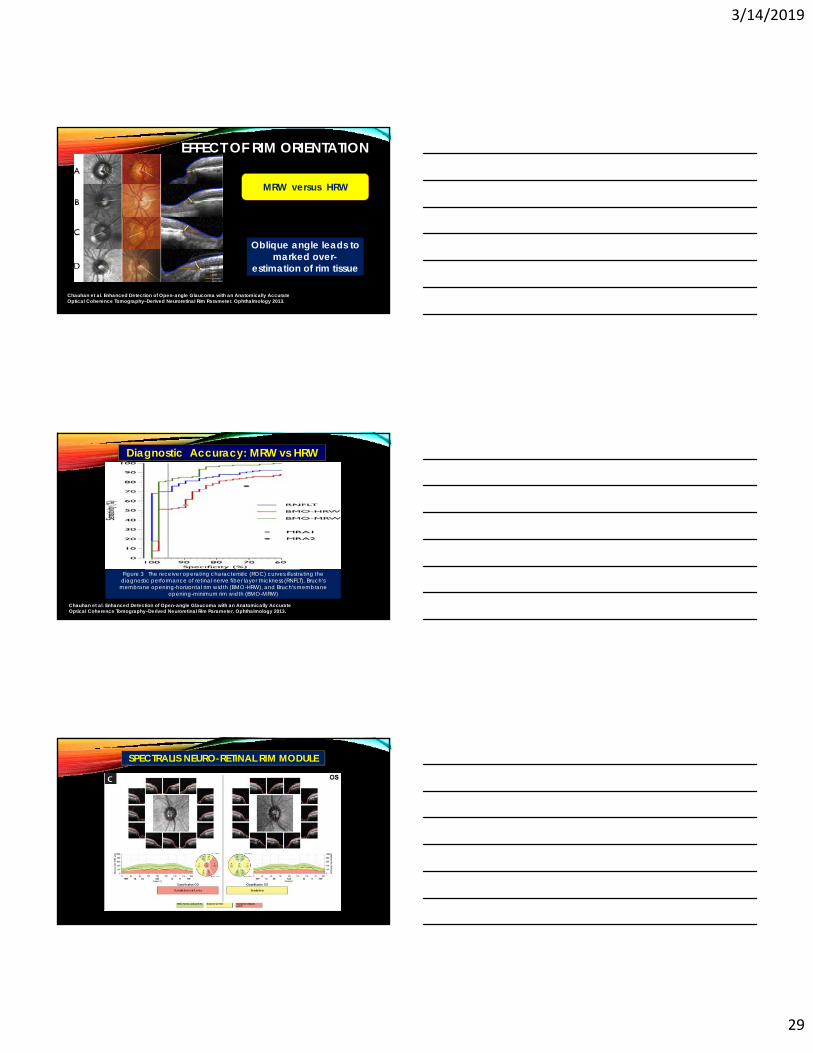
EFFECT OF RIM ORIENTATION
Chauhan et al. Enhanced Detection of Open-angle Glaucoma with an Anatomically Accurate Optical Coherence Tomography–Derived Neuroretinal Rim Parameter. Ophthalmology 2013.
MRW versus HRW
Oblique angle leads to marked over-
estimation of rim tissue
Chauhan et al. Enhanced Detection of Open-angle Glaucoma with an Anatomically Accurate Optical Coherence Tomography–Derived Neuroretinal Rim Parameter. Ophthalmology 2013.
Diagnostic Accuracy: MRW vs HRW
Figure 3 The receiver operating characteristic (ROC) curves illustrating the diagnostic performance of retinal nerve fiber layer thickness (RNFLT), Bruch's
membrane opening-horizontal rim width (BMO-HRW), and Bruch's membrane opening-minimum rim width (BMO-MRW)
SPECTRALIS NEURO-RETINAL RIM MODULE
os
3/14/2019
30
Differentiation of Parapapillary Atrophy
JONAS JB ET AL. MICROSTRUCTURE OF PARAPAPILLARY ATROPHY: BETA ZONE AND GAMMA ZONE. IOVS 2013
Alpha: agingBeta: glaucomaGamma: myopia
PPA zones are associated with:
1. Quantitative evaluation of optic nerve healtha) Can reliably identify healthy impostersb) Can reliably identify optic nerve damage
OPTIMIZED GLAUCOMA DETECTION STRATEGY Value of OCT
CONFIDENCE !!!
2. Permits corroboration of structure/structure and structure/function abnormality
Wants updated spectacle Rx No other ocular/visual complaints
Last eye exam 3 years ago in California No history of eye injury/surgery/disease/trauma Med Hx: borderline DM/HTN; no meds Fam Hx: no glaucoma/blindness
Last case: 60 year old black male reports for routine eye exam
3/14/2019
31
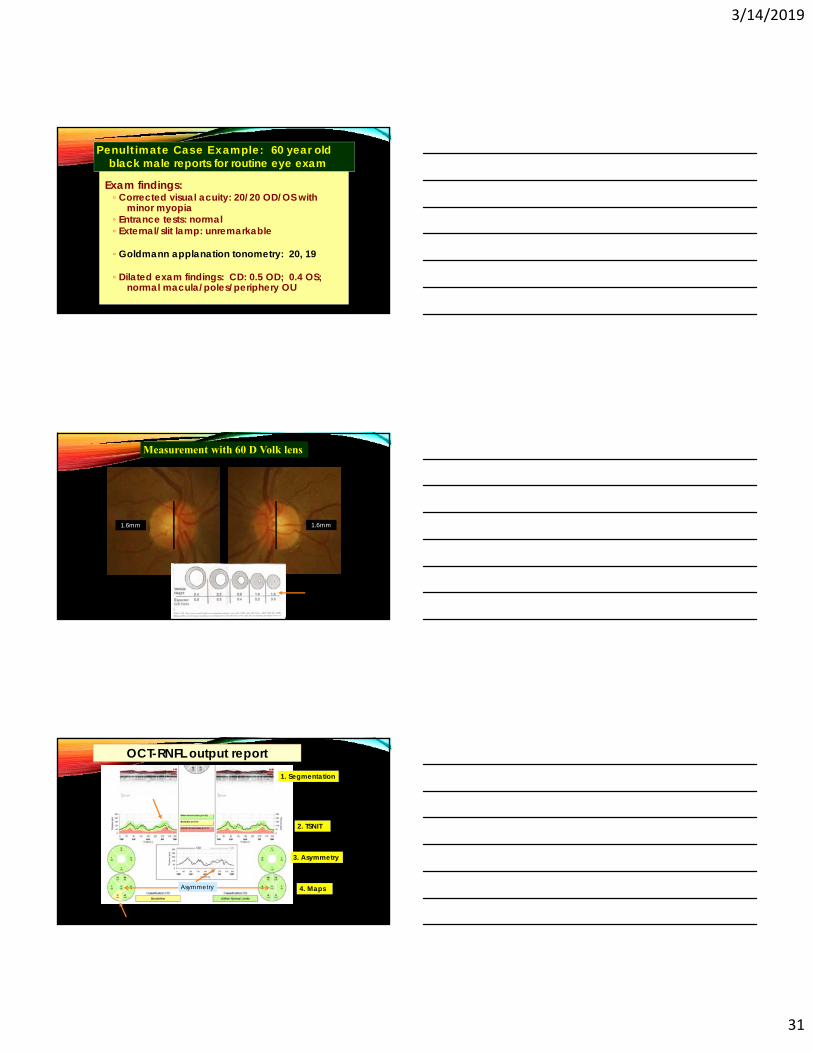
Exam findings: ◦ Corrected visual acuity: 20/20 OD/OS with
minor myopia◦ Entrance tests: normal◦ External/slit lamp: unremarkable
◦ Goldmann applanation tonometry: 20, 19
◦ Dilated exam findings: CD: 0.5 OD; 0.4 OS; normal macula/poles/periphery OU
Penultimate Case Example: 60 year old black male reports for routine eye exam
1.6mm 1.6mm
Measurement with 60 D Volk lens
OCT-RNFL output report
Asymmetry
1. Segmentation
2. TSNIT
3. Asymmetry
4. Maps
3/14/2019
32
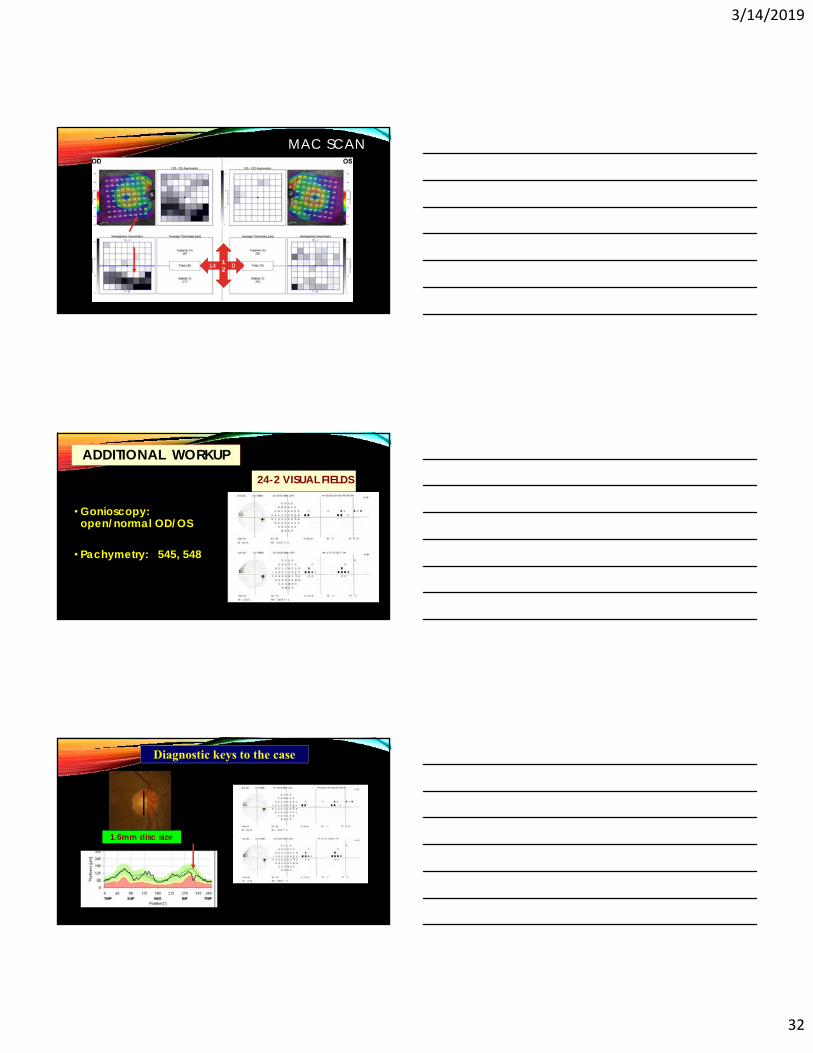
MAC SCAN
14 012
• Gonioscopy: open/normal OD/OS
• Pachymetry: 545, 548
ADDITIONAL WORKUP24-2 VISUAL FIELDS
1.6mm disc size
Diagnostic keys to the case
3/14/2019
33
CONCLUSION
Accurate identification of undiagnosed glaucoma requires a prospective, structured approach that incorporates a graduated index of suspicion
OCT is useful not just for aiding glaucoma diagnosis but ALSO for calling out the GS imposters
Optometrists are well-positioned and crucial for reducing glaucoma burden in the coming decades
3/14/2019
1
GLAUCOMA MANAGEMENT: OPTIMIZING DECISION-MAKING
TIPS FROM THE TRENCHES
Michael Sullivan-Mee, OD, FAAO
AAO Diplomate, Glaucoma
Albuquerque VA Medical Center
CESW 2019No conflicts of interest to report
Many factors must be considered for good quality, consistent decision-making
Mission Glaucoma
CLINICAL SUCCESS IN GLAUCOMA MANAGEMENT
PATIENT THAT IS STABLE
No apparent structural deterioration No progressive loss of rim No progressive loss of RNFL or new RNFL defects No new disc hemorrhages
No progressive visual field loss
Acceptable level of IOP (treated or untreated)
3/14/2019
2
BUT WHAT IS FAILURE IN GLAUCOMA MANAGEMENT ?
PATIENT THAT IS NOT STABLE
(+) structural deterioration progressive loss of rim tissue
progressive loss of RNFL (exceeding age-related rate)
new clinically evident RNFL defects
new disc hemorrhages
(+) progressive visual field loss
UN-Acceptable level of IOP
According to George Spaeth, MD:1) Prevent disability in our patients.2) If disability already exists, repair the
disability or prevent further disability.
SO WHAT ARE THE GOALS FOR GLAUCOMA CARE ?
All about “Quality of life”
• Maintain visual abilities• Ability to perform and enjoy
household, work, and personal tasks
• Reduction of risk for MVA
• Reduction of risk for falling
Quality of life factors impacting treatment decisions
• Maintain ability to live independently
• Maintain ability to remain physically active and mobile
• Reduce Psychological stress
• Fear of falling• Fear of blindness
• Negative effects of treatment/care• Burden of glaucoma
meds/follow-up visits/disease costs
• Glaucoma medicine side effects
3/14/2019
3
1. Preventsymptomaticvisionloss2. Limitfurthervisionlossifvisionloss
alreadyexists3.Preventblindness
Glaucoma Goal Summary
Foundation of care is to:
1. SEVERITY OF DISEASE
4. Life expectancy !
2. Rate of disease
progression
To achieve these goals clinically:
3. Level/cause/risk associated with IOP and the methods to treat it
The Essential Factors In Glaucoma
Decision-Making
IOP and type of glaucoma
Rate of progression
Lifeexpectancy
Severity of disease
3/14/2019
4
LIFE EXPECTANCY DIFFERENCES (RACE/GENDER)
EFFECT OF AGING ON LIFE EXPECTANCY
EFFECT OF AGING ON LIFE EXPECTANCY
• A man reaching age 65 today can expect to live, on average, until age 84.3.
• A woman turning age 65 today can expect to live, on average, until age 86.6.
• About one out of every four 65-year-olds today will live past age 90
• One out of 10 will live past age 95
According to data compiled by SSA:
3/14/2019
5
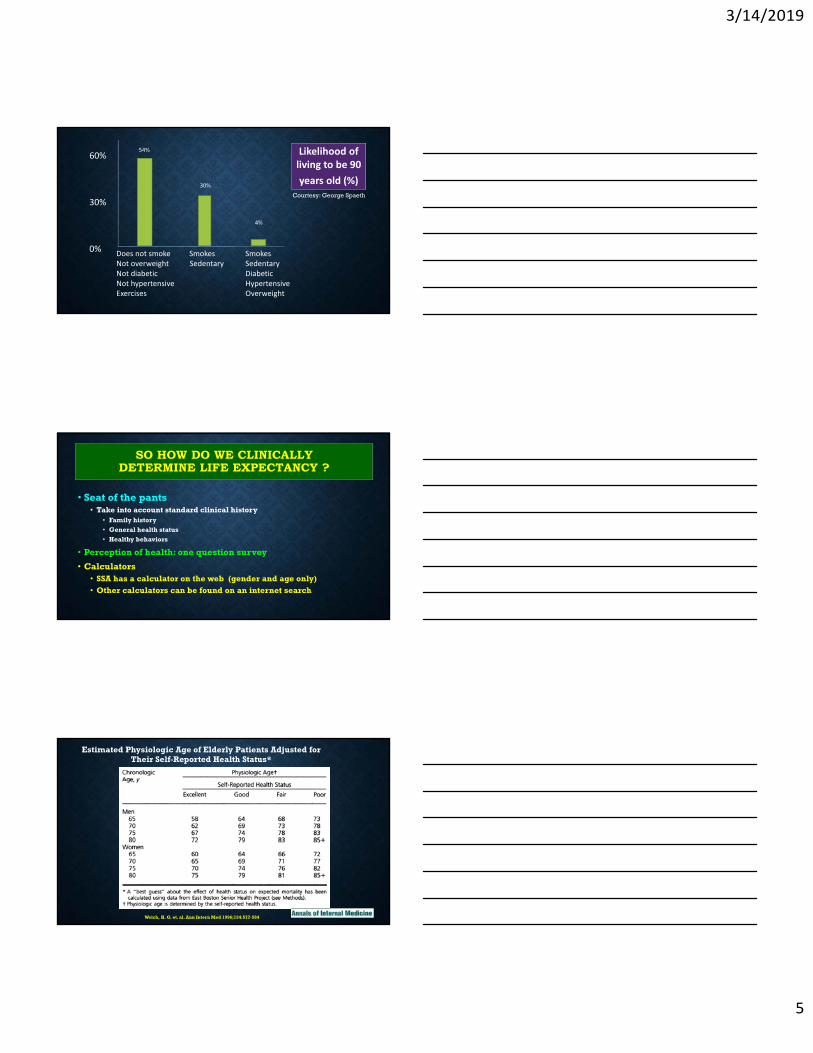
Likelihood of living to be 90
years old (%)
60%
30%
0%Does not smoke Smokes SmokesNot overweight Sedentary SedentaryNot diabetic DiabeticNot hypertensive HypertensiveExercises Overweight
54%
30%
4%
Courtesy: George Spaeth
• Seat of the pants• Take into account standard clinical history
• Family history
• General health status
• Healthy behaviors
• Perception of health: one question survey
• Calculators• SSA has a calculator on the web (gender and age only)• Other calculators can be found on an internet search
SO HOW DO WE CLINICALLY DETERMINE LIFE EXPECTANCY ?
Estimated Physiologic Age of Elderly Patients Adjusted for Their Self-Reported Health Status*
Welch, H. G. et. al. Ann Intern Med 1996;124:577-584
3/14/2019
6
HTTPS://WWW.MYABARIS.COM/TOOLS/LIFE-EXPECTANCY-CALCULATOR-HOW-
LONG-WILL-I-LIVE/
LIFE EXPECTANCY CALCULATOR
• The ABARIS life expectancy calculator is based on a
statistical regression of more than 400,000 data samples. The data was collected by the National Institute of Health and AARP.
https://www.myabaris.com/tools/life-expectancy-calculator-how-long-will-i-live/
AgeGenderRaceHeightWeight
EducationMarital statusRetired ?Annual Income
Exercise habitsGeneral healthDM statusAlcohol habitsSmoking habits
Email required
LIFE EXPECTANCY
Ultimately, every case needs an assessment of life expectancy
All personal health information, health behaviors and family history/family
member longevity should be considered in this effort so that treatment/management
decisions can be optimally titrated
3/14/2019
7
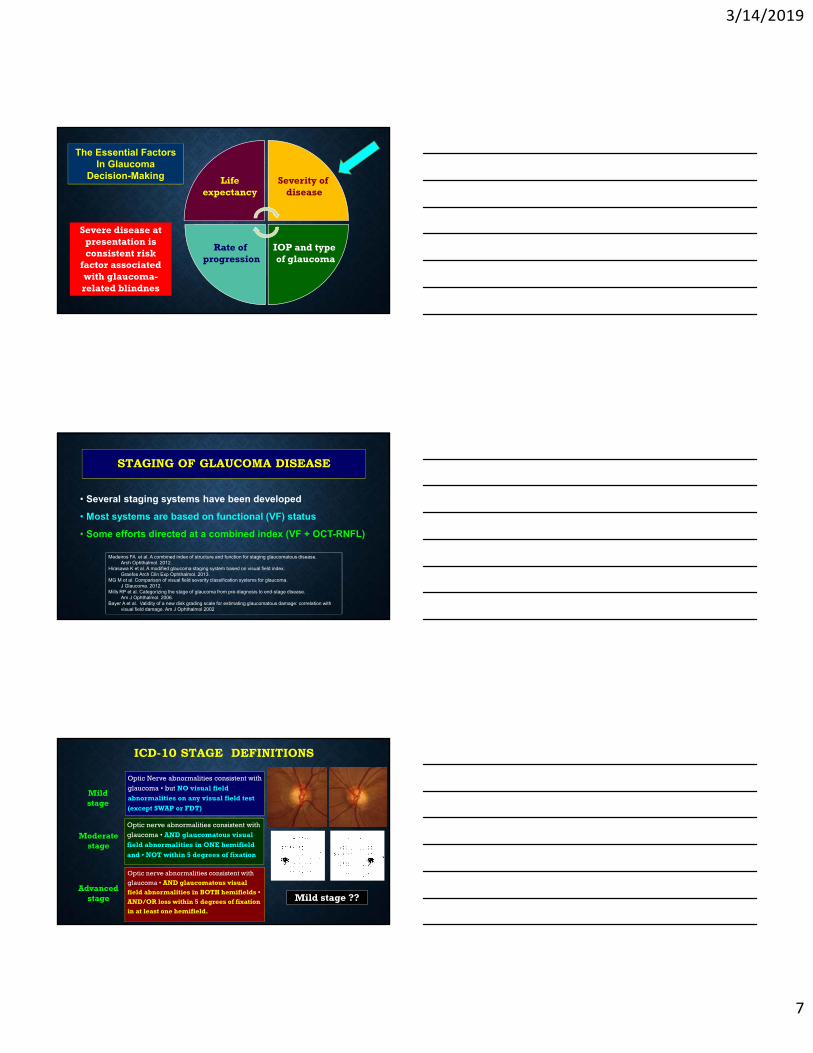
The Essential Factors In Glaucoma
Decision-Making
IOP and type of glaucoma
Rate of progression
Lifeexpectancy
Severity of disease
Severe disease at presentation isconsistent risk
factor associatedwith glaucoma-related blindnes
STAGING OF GLAUCOMA DISEASE
• Several staging systems have been developed
• Most systems are based on functional (VF) status
• Some efforts directed at a combined index (VF + OCT-RNFL)
Medeiros FA et al. A combined index of structure and function for staging glaucomatous disease. Arch Ophthalmol. 2012.
Hirasawa K et al. A modified glaucoma staging system based on visual field index. Graefes Arch Clin Exp Ophthalmol. 2013.
MG M et al. Comparison of visual field severity classification systems for glaucoma.J Glaucoma. 2012.
Mills RP et al. Categorizing the stage of glaucoma from pre-diagnosis to end-stage disease. Am J Ophthalmol. 2006.
Bayer A et al. Validity of a new disk grading scale for estimating glaucomatous damage: correlation with visual field damage. Am J Ophthalmol 2002
ICD-10 STAGE DEFINITIONS
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in BOTH hemifields • AND/OR loss within 5 degrees of fixation in at least one hemifield.
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in ONE hemifield
and • NOT within 5 degrees of fixation
Optic Nerve abnormalities consistent with
glaucoma • but NO visual field abnormalities on any visual field test
(except SWAP or FDT)
Mild stage
Moderate stage
Advanced stage Mild stage ??
3/14/2019
8
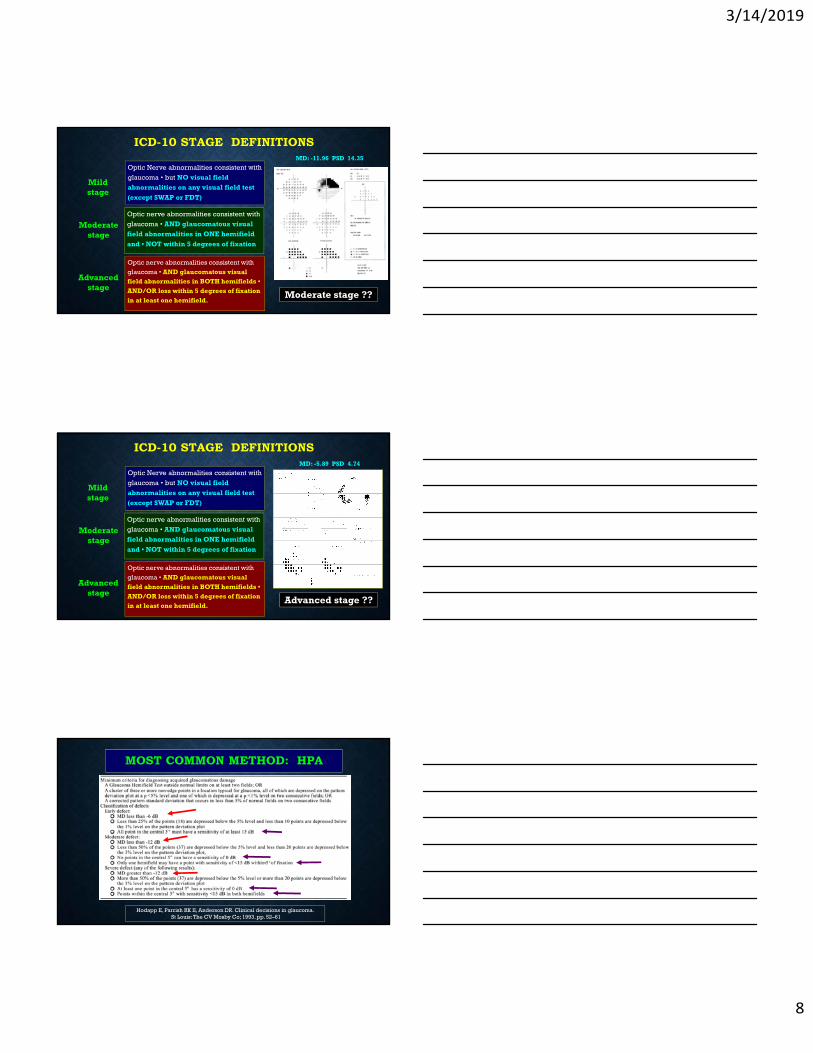
ICD-10 STAGE DEFINITIONS
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in BOTH hemifields • AND/OR loss within 5 degrees of fixation in at least one hemifield.
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in ONE hemifield
and • NOT within 5 degrees of fixation
Optic Nerve abnormalities consistent with
glaucoma • but NO visual field abnormalities on any visual field test
(except SWAP or FDT)
Mild stage
Moderate stage
Advanced stage
Moderate stage ??
MD: -11.96 PSD 14.35
Put severe arc that spares fxnhere
ICD-10 STAGE DEFINITIONS
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in BOTH hemifields • AND/OR loss within 5 degrees of fixation in at least one hemifield.
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in ONE hemifield
and • NOT within 5 degrees of fixation
Optic Nerve abnormalities consistent with
glaucoma • but NO visual field abnormalities on any visual field test
(except SWAP or FDT)
Mild stage
Moderate stage
Advanced stage
Advanced stage ??
MD: -5.89 PSD 4.74
MOST COMMON METHOD: HPA
Hodapp E, Parrish RK II, Anderson DR. Clinical decisions in glaucoma.St Louis: The CV Mosby Co; 1993. pp. 52–61
3/14/2019
9
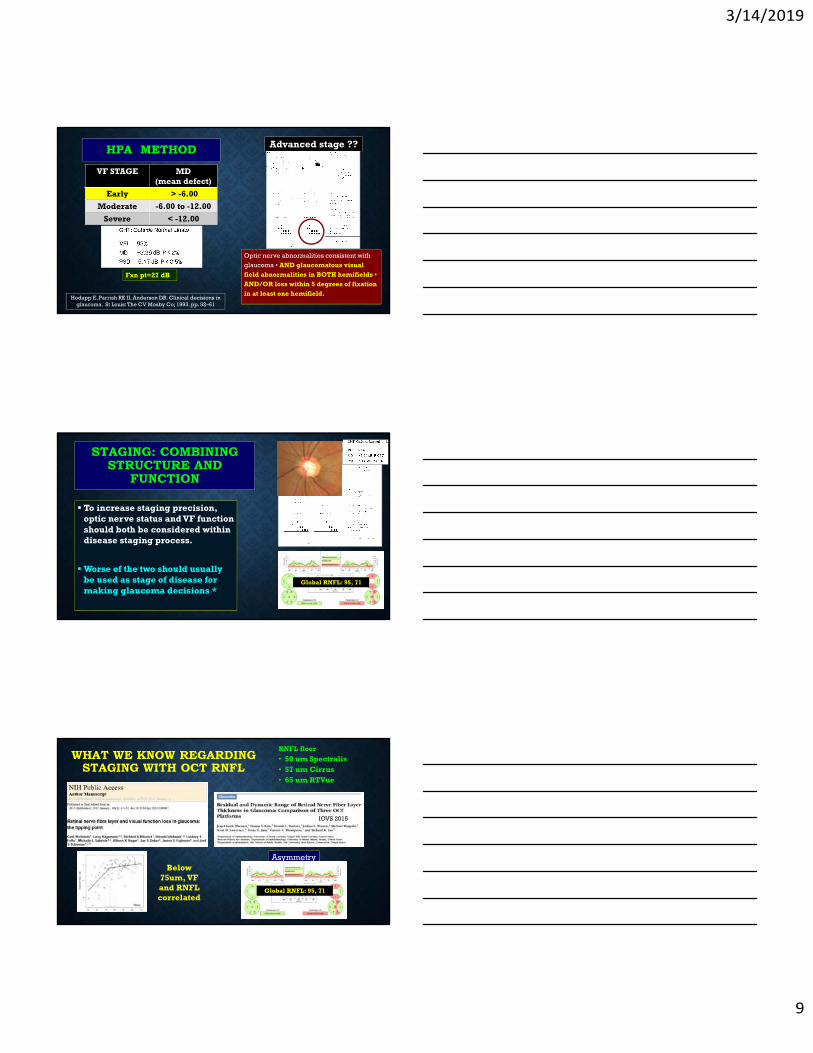
HPA METHOD
Hodapp E, Parrish RK II, Anderson DR. Clinical decisions in glaucoma. St Louis: The CV Mosby Co; 1993. pp. 52–61
VF STAGE MD(mean defect)
Early > -6.00
Moderate -6.00 to -12.00
Severe < -12.00
Optic nerve abnormalities consistent with
glaucoma • AND glaucomatous visual field abnormalities in BOTH hemifields • AND/OR loss within 5 degrees of fixation in at least one hemifield.
Advanced stage ??
Fxn pt=27 dB
STAGING: COMBINING STRUCTURE AND
FUNCTION
To increase staging precision, optic nerve status and VF function should both be considered within disease staging process.
Worse of the two should usually be used as stage of disease for making glaucoma decisions *
Global RNFL: 95, 71
WHAT WE KNOW REGARDING STAGING WITH OCT RNFL
RNFL floor
• 50 um Spectralis• 57 um Cirrus• 65 um RTVue
Below 75um, VF and RNFL correlated
IOVS 2015
Asymmetry
Global RNFL: 95, 71
3/14/2019
10
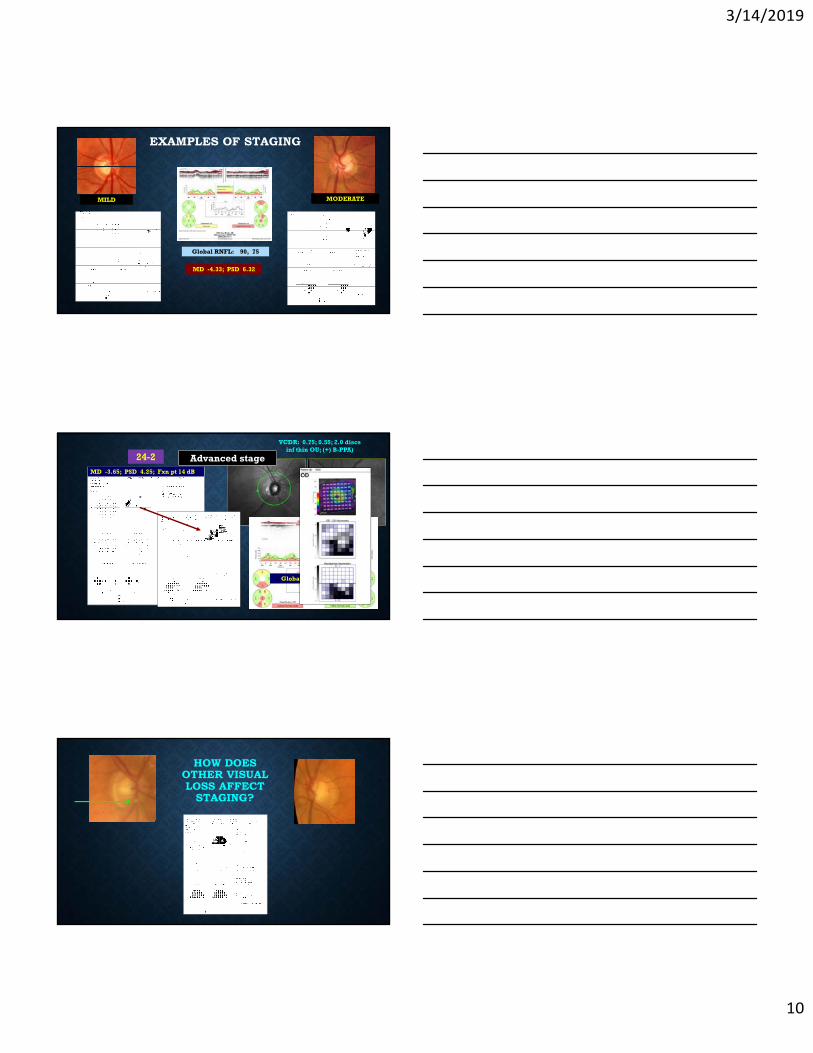
MD -4.33; PSD 6.32
EXAMPLES OF STAGING
Global RNFL: 90, 75
MODERATEMILD
MD -3.65; PSD 4.25; Fxn pt 14 dB
VCDR: 0.75; 0.55; 2.0 discsinf thin OU; (+) B-PPA)
24-2
Global RNFL: 67, 80
Moderate stage ??Advanced stage
HOW DOES OTHER VISUAL LOSS AFFECT
STAGING?
3/14/2019
11
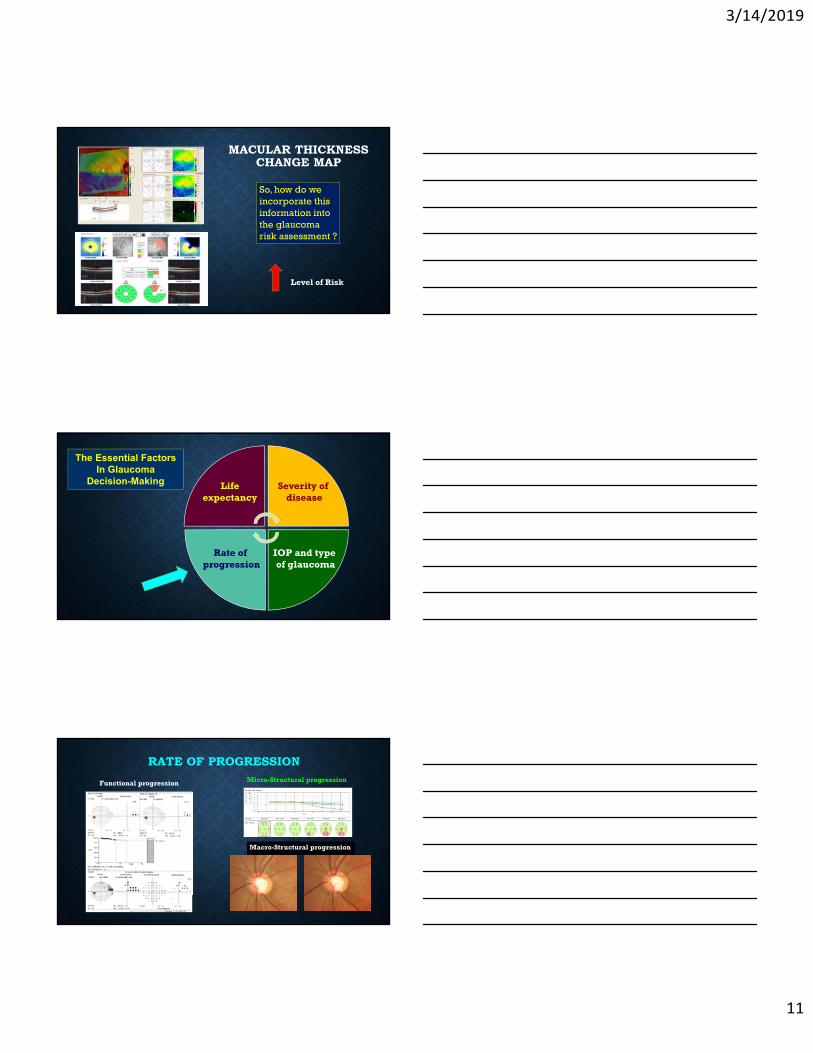
MACULAR THICKNESS CHANGE MAP
So, how do we incorporate this information into the glaucoma risk assessment ?
Level of Risk
The Essential Factors In Glaucoma
Decision-Making
IOP and type of glaucoma
Rate of progression
Lifeexpectancy
Severity of disease
RATE OF PROGRESSION
Functional progression Micro-Structural progression
Macro-Structural progression
3/14/2019
12
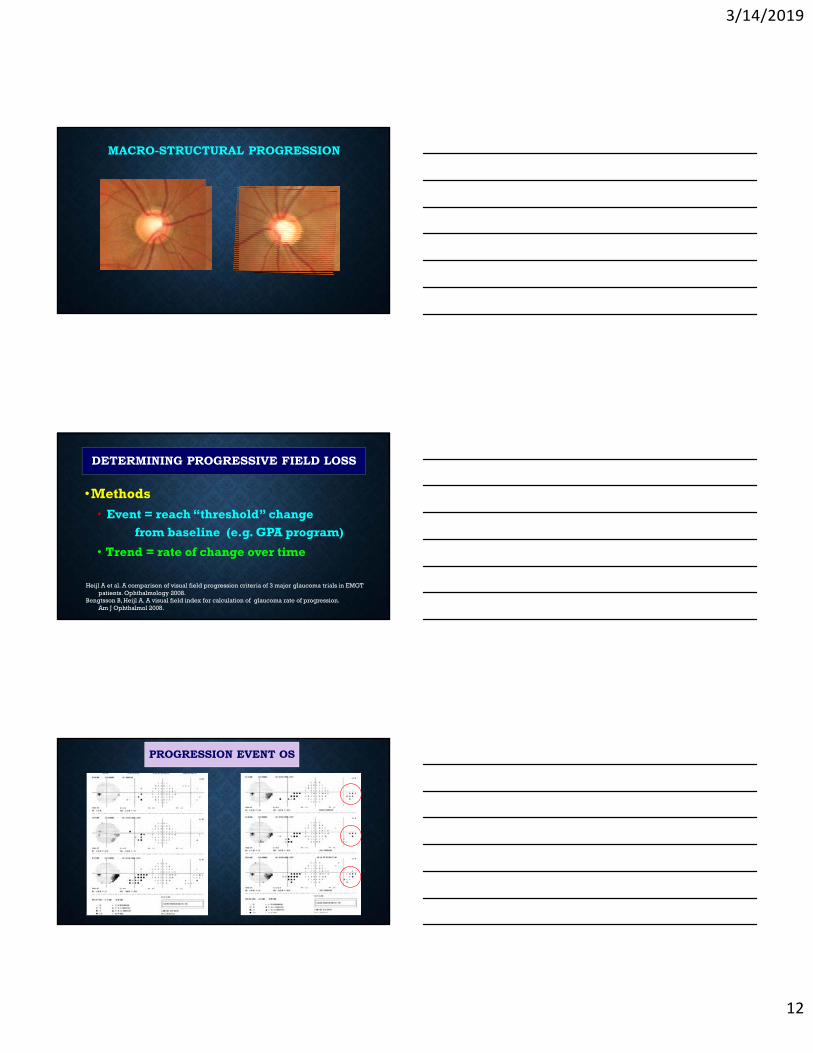
MACRO-STRUCTURAL PROGRESSION
DETERMINING PROGRESSIVE FIELD LOSS
Heijl A et al. A comparison of visual field progression criteria of 3 major glaucoma trials in EMGT patients. Ophthalmology 2008.
Bengtsson B, Heijl A. A visual field index for calculation of glaucoma rate of progression. Am J Ophthalmol 2008.
•Methods
• Event = reach “threshold” change
from baseline (e.g. GPA program)
• Trend = rate of change over time
PROGRESSION EVENT OS
3/14/2019
13
MODE OF VISUAL FIELD TESTING
HVF 24-2 offers best option for monitoring
established glaucoma
• SAP (standard automated perimetry)
• Sita, 24-2 pattern, achromatic
Sample PA et al. Identifying glaucomatous vision loss with visual-function-specific perimetry in the diagnostic
innovations in glaucoma study. IOVS 2006.
3/14/2019
14
• Timely determination of rate of change
• Numbers of tests to detect change event
• Effect of poor reliability
Frequency of Visual field testing
Pertinent factors
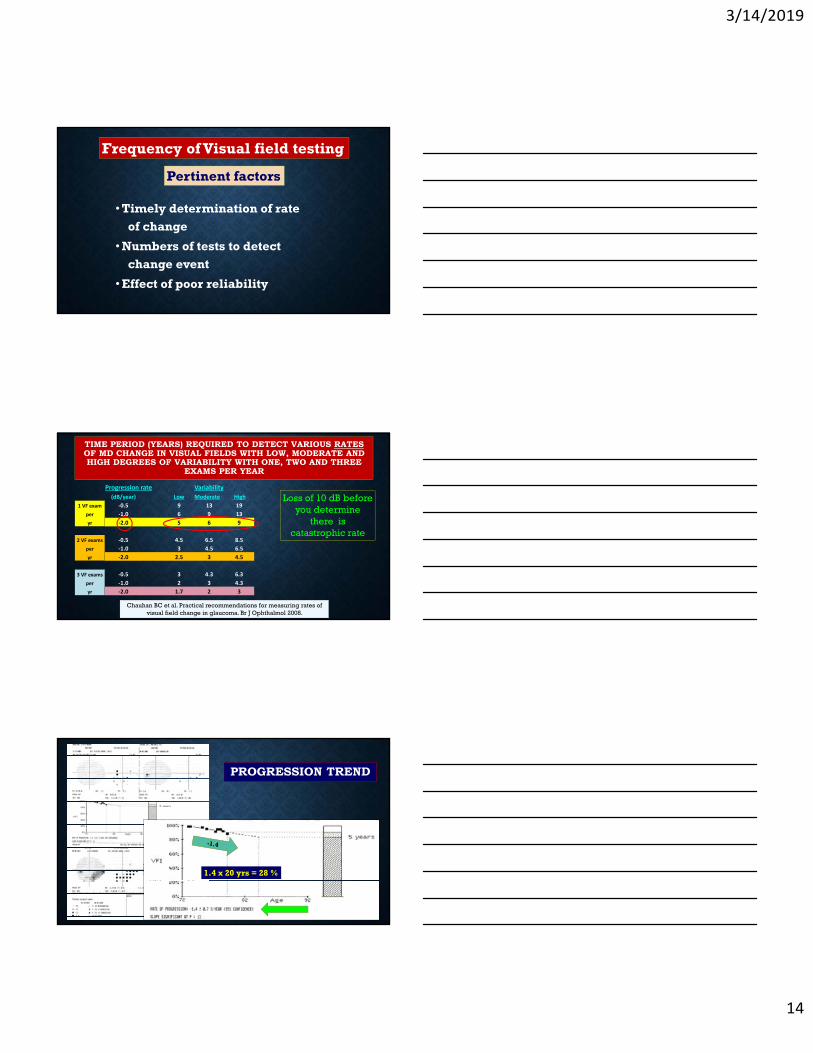
TIME PERIOD (YEARS) REQUIRED TO DETECT VARIOUS RATESOF MD CHANGE IN VISUAL FIELDS WITH LOW, MODERATE AND HIGH DEGREES OF VARIABILITY WITH ONE, TWO AND THREE
EXAMS PER YEAR
Chauhan BC et al. Practical recommendations for measuring rates of visual field change in glaucoma. Br J Ophthalmol 2008.
Progression rate Variability
(dB/year) Low Moderate High
1 VF exam ‐0.5 9 13 19
per ‐1.0 6 9 13
yr ‐2.0 5 6 9
2 VF exams ‐0.5 4.5 6.5 8.5
per ‐1.0 3 4.5 6.5
yr ‐2.0 2.5 3 4.5
3 VF exams ‐0.5 3 4.3 6.3
per ‐1.0 2 3 4.3
yr ‐2.0 1.7 2 3
Loss of 10 dB before you determine
there is catastrophic rate
PROGRESSION TREND
1.4 x 20 yrs = 28 %
3/14/2019
15
CONSIDERATIONS WITH RATE OF PROGRESSION IN ADVANCED DISEASE
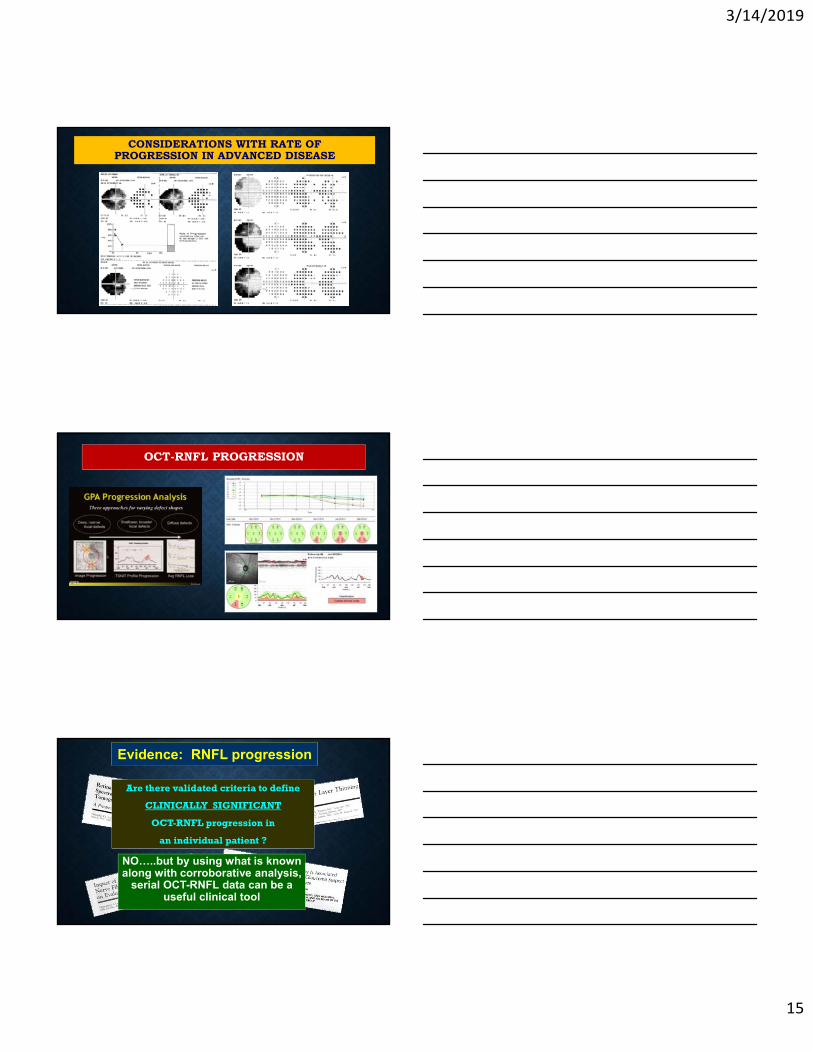
OCT-RNFL PROGRESSION
Evidence: RNFL progression
Are there validated criteria to define
CLINICALLY SIGNIFICANT
OCT-RNFL progression in
an individual patient ?
NO…..but by using what is known along with corroborative analysis,
serial OCT-RNFL data can be a useful clinical tool
3/14/2019
16
STABLE RNFL OVER TIME
OCT RNFL and Guided Progression Analysis (GPA)
CONSIDERATIONS FOR IDENTIFYING TRUE PROGRESSION
• Data validity
• Scan quality
• Segmentation
• Centration
• Anatomical variation including pathology
• Age-related RNFL decline
• Baseline thickness effect
• Floor effect
• Axial length/magnification effects
• Frequency of testing
• Statistical vs. clinical significance
3/14/2019
17
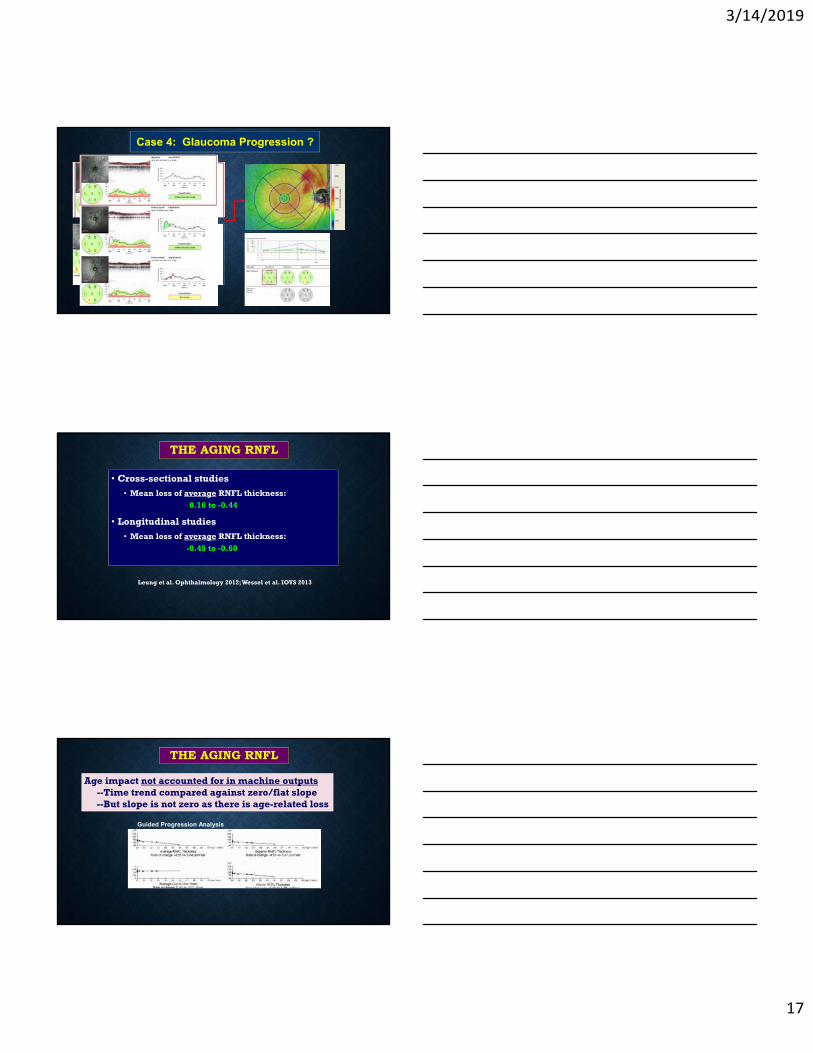
Case 4: Glaucoma Progression ?
THE AGING RNFL
• Cross-sectional studies
• Mean loss of average RNFL thickness: -0.16 to -0.44
• Longitudinal studies
• Mean loss of average RNFL thickness:
-0.45 to -0.60• 95% CI ~ 3µm per year
Leung et al. Ophthalmology 2012; Wessel et al. IOVS 2013
Age impact not accounted for in machine outputs--Time trend compared against zero/flat slope--But slope is not zero as there is age-related loss
Guided Progression Analysis
THE AGING RNFL
3/14/2019
18
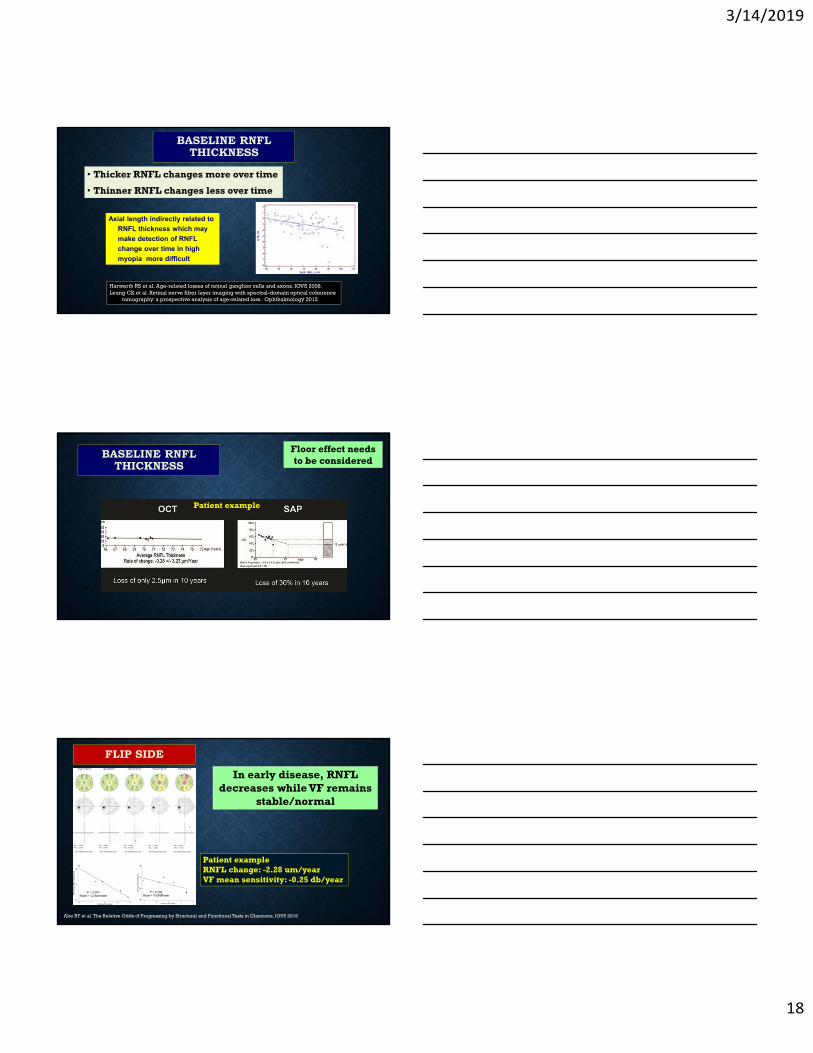
BASELINE RNFL THICKNESS
• Thicker RNFL changes more over time
• Thinner RNFL changes less over time
Harwerth RS et al. Age-related losses of retinal ganglion cells and axons. IOVS 2008.Leung CK et al. Retinal nerve fiber layer imaging with spectral-domain optical coherence
tomography: a prospective analysis of age-related loss. Ophthalmology 2012
Axial length indirectly related to
RNFL thickness which may
make detection of RNFL
change over time in high
myopia more difficult
Floor effect needs to be considered
BASELINE RNFL THICKNESS
Patient example
In early disease, RNFL decreases while VF remains
stable/normal
FLIP SIDE
Abe RY et al. The Relative Odds of Progressing by Structural and Functional Tests in Glaucoma. IOVS 2016
Patient exampleRNFL change: -2.28 um/yearVF mean sensitivity: -0.25 db/year
3/14/2019
19
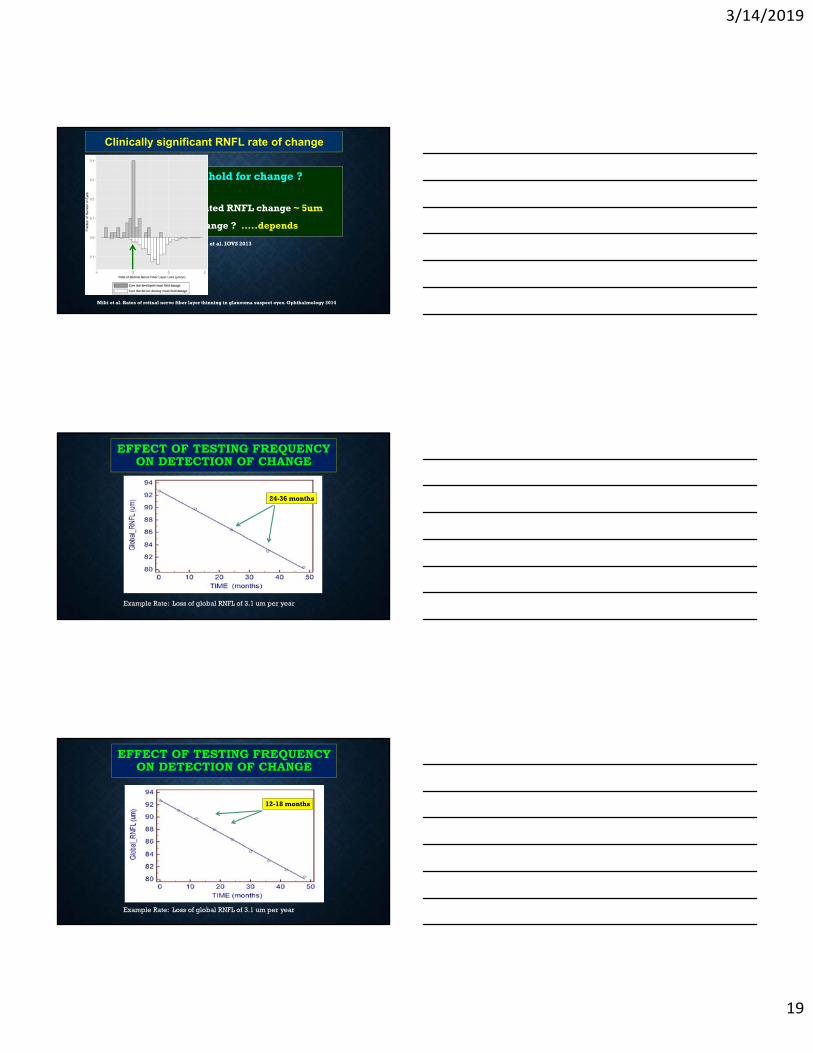
What is clinical threshold for change ?
1. Significant event-related RNFL change ~ 5um
2. Significant rate of change ? …..depends
Clinically significant RNFL rate of change
Leung et al. Ophthalmology 2012; Wessel et al. IOVS 2013
Miki et al. Rates of retinal nerve fiber layer thinning in glaucoma suspect eyes. Ophthalmology 2014
EFFECT OF TESTING FREQUENCY ON DETECTION OF CHANGE
24-36 months
Example Rate: Loss of global RNFL of 3.1 um per year
Example Rate: Loss of global RNFL of 3.1 um per year
12-18 months
EFFECT OF TESTING FREQUENCY ON DETECTION OF CHANGE
3/14/2019
20
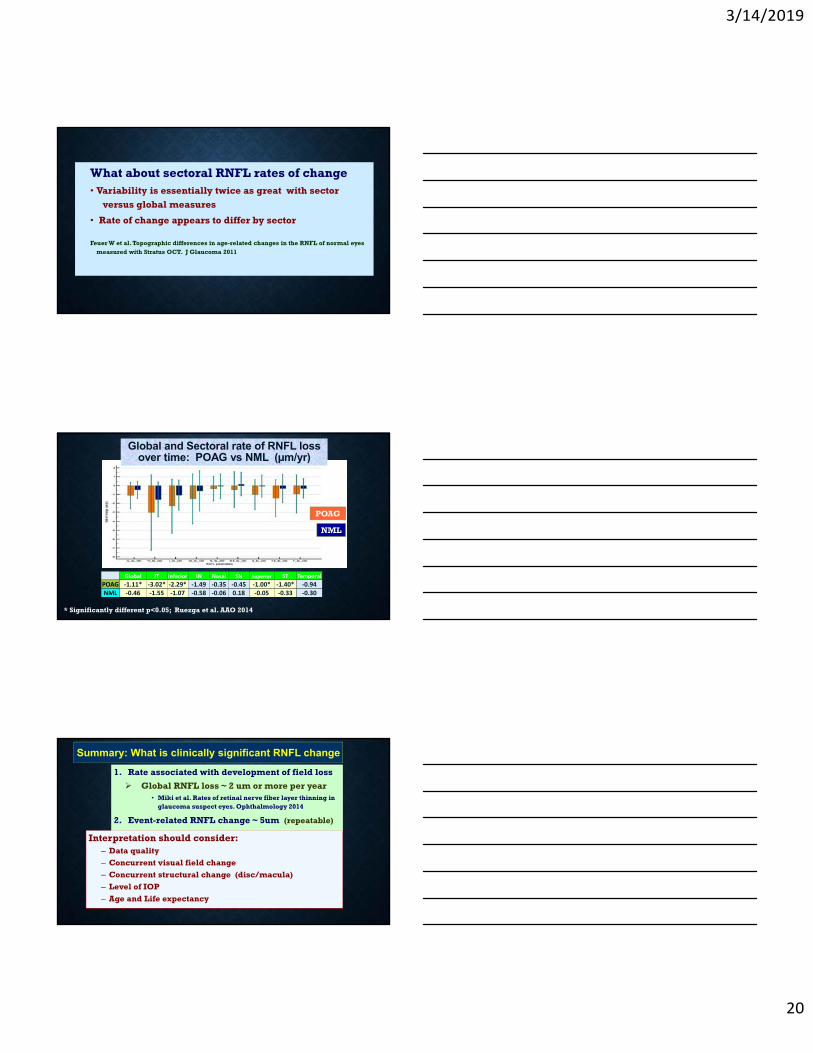
What about sectoral RNFL rates of change• Variability is essentially twice as great with sector
versus global measures
• Rate of change appears to differ by sector
Feuer W et al. Topographic differences in age-related changes in the RNFL of normal eyes measured with Stratus OCT. J Glaucoma 2011
Global IT Inferior IN Nasal SN Superior ST Temporal
POAG ‐1.11* ‐3.02* ‐2.29* ‐1.49 ‐0.35 ‐0.45 ‐1.00* ‐1.40* ‐0.94NML ‐0.46 ‐1.55 ‐1.07 ‐0.58 ‐0.06 0.18 ‐0.05 ‐0.33 ‐0.30
* Significantly different p<0.05; Ruezga et al. AAO 2014
POAG
NML
Global and Sectoral rate of RNFL loss over time: POAG vs NML (µm/yr)
1. Rate associated with development of field loss
Global RNFL loss ~ 2 um or more per year• Miki et al. Rates of retinal nerve fiber layer thinning in
glaucoma suspect eyes. Ophthalmology 2014
2. Event-related RNFL change ~ 5um (repeatable)
Summary: What is clinically significant RNFL change
Interpretation should consider:– Data quality
– Concurrent visual field change
– Concurrent structural change (disc/macula)
– Level of IOP
– Age and Life expectancy

3/14/2019
21
What about Macular Thickness Progression ?
Zhang et al. Comparison of Glaucoma Progression Detection by Optical Coherence Tomography and Visual Field. Am J Ophthalmol 2017;184:63-74.
The Essential Factors In Glaucoma
Decision-Making
IOP and type of glaucoma
Rate of progression
Lifeexpectancy
Severity of disease
Level/cause/risk associated with IOP and the methods to treat it
Case Example
Age: 45Occupation: Engineer
s/p LASIK at age 35--moderate myopia
1. “Vision seems off”2. Trouble serving a
volleyball (loses it during serve)
3. No discomfort/pain
Wants enhancement !
1422
OD
Diagnosis: Advanced primary angle closure glaucoma
(with missed opportunity)
OS OS
3/14/2019
22
Current factors of case decision making
Age: 45Good health
Current visual status VA normal OD/OS VF: severe loss OS
Treatment goals Maintain current
visual status Keep IOP low Healthy 45 year old/monocular/high risk !
OD OS
Disease progression rate To be determined
So is PACG something to worry about ?
PACG blinds disproportionately vs. OAG: 3-10x more people blind from PACG vs. OAG
IOP tends to be relatively high in angle closure
PACG is usually asymptomatic (up to 85% or more of cases )
Asymptomatic presentations often lead to late diagnosis and treatment
So is PACG something to worry about ?
PACG blinds disproportionately vs. OAG: 3-10x more people blind from PACG vs. OAG
IOP tends to be relatively high in angle closure
PACG is usually asymptomatic (up to 85% or more of cases )
Asymptomatic presentations often lead to late diagnosis and treatment
3/14/2019
23
Type of glaucoma is related to glaucoma risk
SLE/gonio needed to identify 2’ glaucoma
Angle closure/plateau iris Pigment dispersion syndrome Pseudoexfoliation Angle recession Iris neovascularization Neoplasm/Melanoma Inflammation-related
HOW IS IOP RISK ASSESSED/CONSIDERED ?
• Level/elevation of IOP*• IOP symmetry*• Type of Glaucoma/
cause of IOP elevation*• Fluctuation ?
* Requires thorough & timely SLE/GONIO
Williams AL et al. The value of intraocular pressure asymmetry in diagnosting glaucoma. J Glaucoma 2013
WHAT IS AN ACCEPTABLE LEVEL OF IOP ?
• This estimate based on : • Untreated high IOP• Estimated IOP volatility• Disease severity
• Other visual morbidity• Progression rate• Life expectancy
Level of IOP that does not permit the development of symptomatic vision loss
3/14/2019
24
INITIAL TARGET GUIDANCE FROM CIGTS VS EMGT
Both trials examined treatment in early glaucoma
EMGT used fixed tx regimen (betaxolol and ALT) Average IOP reduction with tx = 22%
CIGTS medical treatment group had strict IOP targets, based on a formula that involved untxIOP and visual field status;
Average medical IOP reduction with tx = 35% Surgery group reduction =46%
In EMGT, 45% of treated subjects had VF progressionIn CIGTS, 0% had visual field progression
BEYOND TARGET IOP, ACHIEVING AN ACCEPTABLE LEVEL OF IOP REQUIRES ADHERENCE TO THE
TREATMENT REGIMEN
• Factors to consider with regard to medical adherence: • Tolerance to topical agents/ocular surface health• Instillation techniques• Regimen complexity• Medicine Costs• Comprehension of disease• Medical co-morbidity
Both under-treatment and lack of adherence have been consistently identified as risks
for glaucoma-related blindness
WHAT IF IOP IS ACCEPTABLE BUT THE DISEASE CONTINUES TO
PROGRESS ?
• Expected IOP fluctuation• Measurement confounders
• Steroid treatments • BP meds (b-blocker)• Dehydratrion
• Nocturnal IOP/BP pressure changes• Sleep posture issue• Harmful activities (eye rubbing/ valsalva/ yoga ?• Irregular med adherence and/or instillation
technique• Inaccurate IOP measurements• Progression rate/life expectancy/disease stage
These factors should be considered
3/14/2019
25
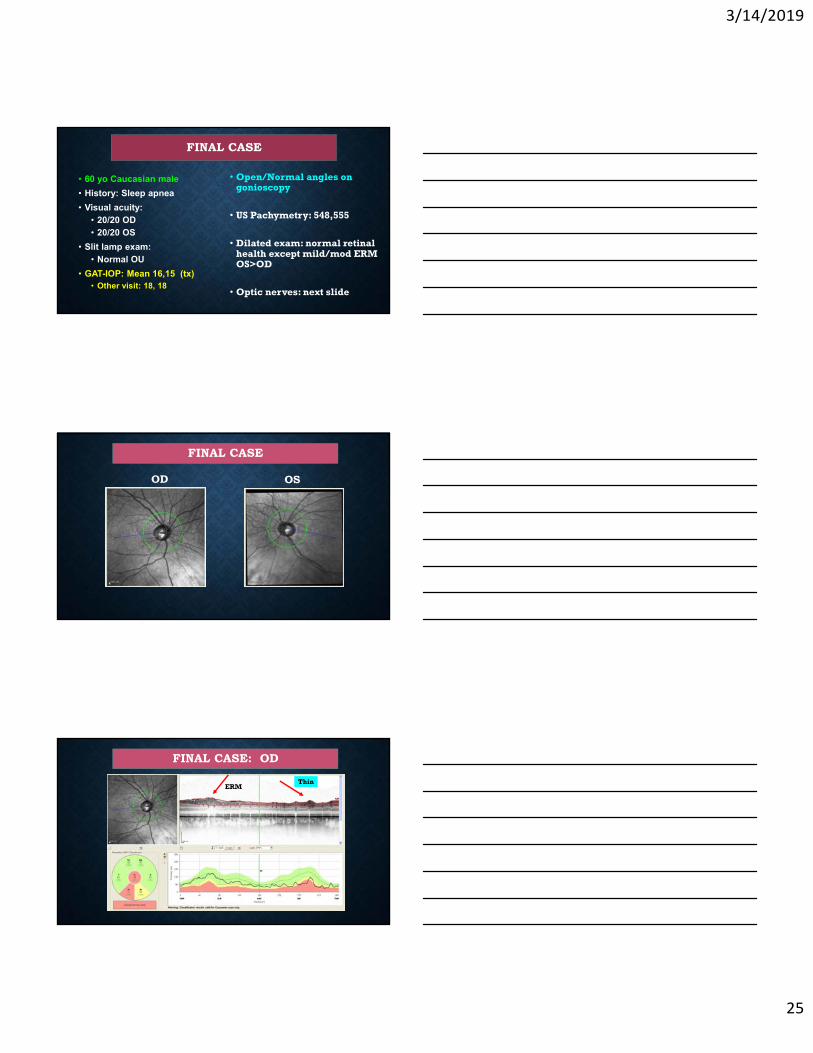
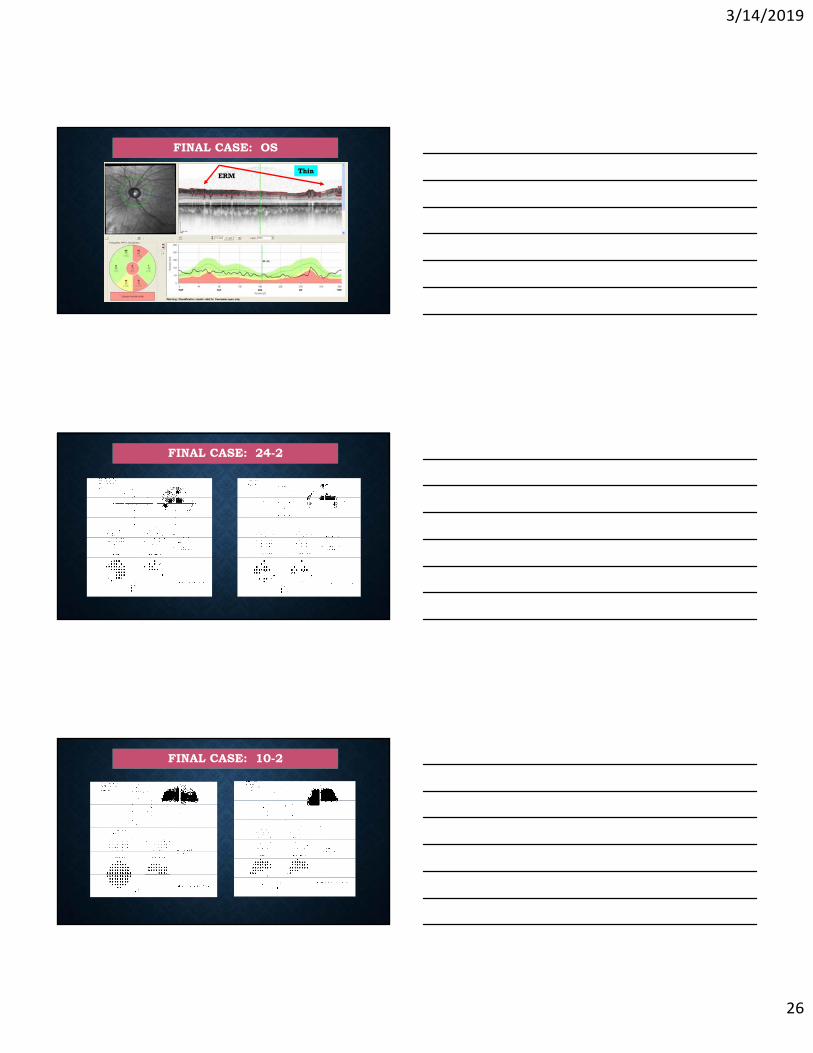
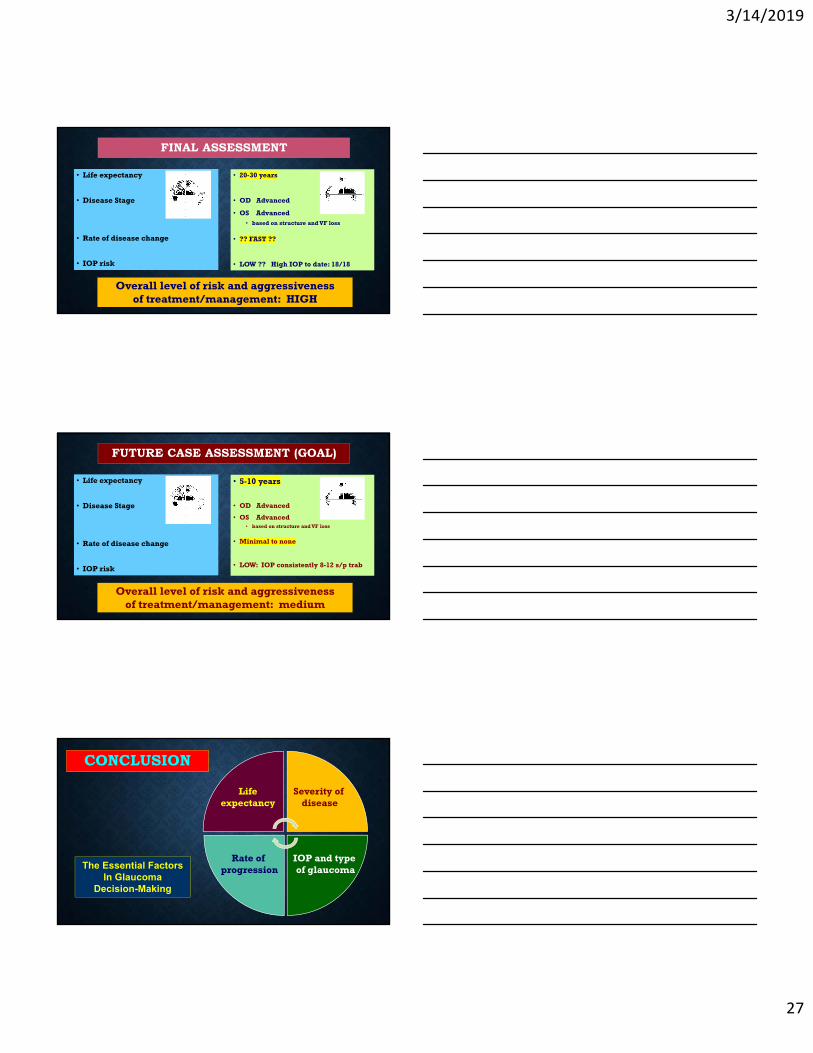
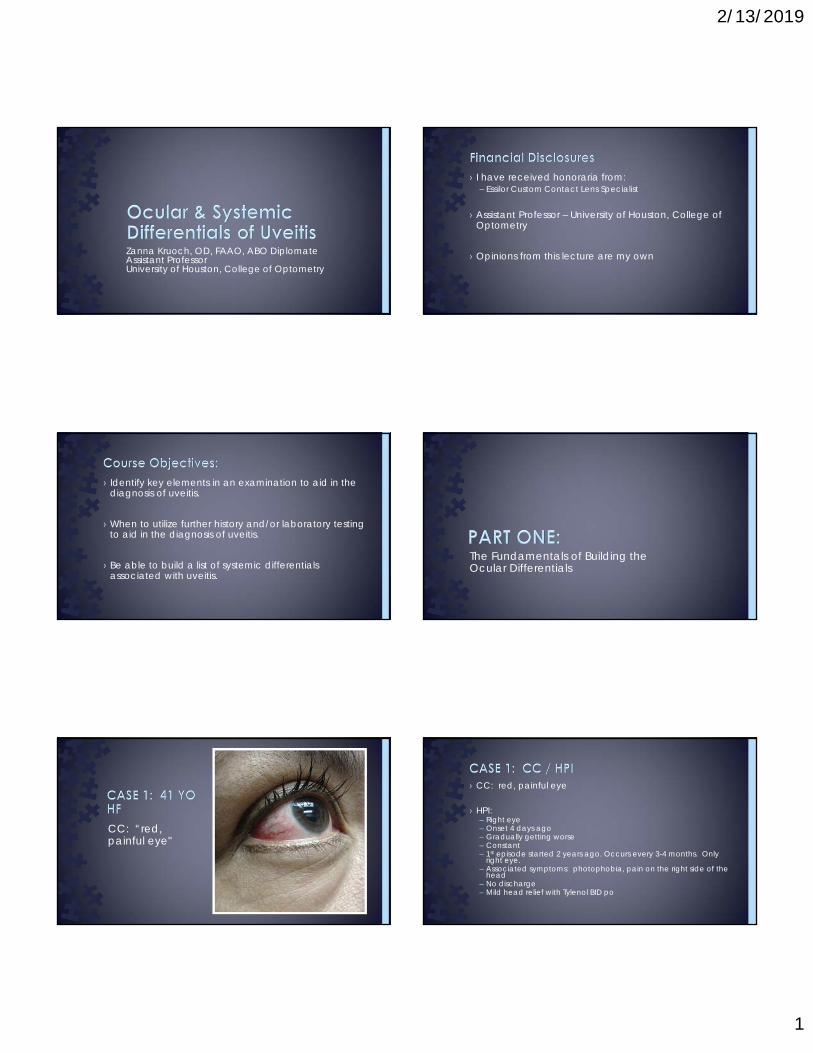
• 60 yo Caucasian male
• History: Sleep apnea
• Visual acuity: • 20/20 OD• 20/20 OS
• Slit lamp exam: • Normal OU
• GAT-IOP: Mean 16,15 (tx)• Other visit: 18, 18
• Open/Normal angles on gonioscopy
• US Pachymetry: 548,555
• Dilated exam: normal retinal health except mild/mod ERM OS>OD
• Optic nerves: next slide
FINAL CASE
OD
FINAL CASE
OS
FINAL CASE: OD
ERMThin
3/14/2019
26
FINAL CASE: OS
ERMThin
FINAL CASE: 24-2
FINAL CASE: 10-2
3/14/2019
27
• Life expectancy
• Disease Stage
• Rate of disease change
• IOP risk
FINAL ASSESSMENT
Overall level of risk and aggressiveness of treatment/management: HIGH
• 20-30 years
• OD Advanced
• OS Advanced • based on structure and VF loss
• ?? FAST ??
• LOW ?? High IOP to date: 18/18
• Life expectancy
• Disease Stage
• Rate of disease change
• IOP risk
FUTURE CASE ASSESSMENT (GOAL)
• 5-10 years
• OD Advanced
• OS Advanced • based on structure and VF loss
• Minimal to none
• LOW: IOP consistently 8-12 s/p trab
Overall level of risk and aggressiveness of treatment/management: medium
The Essential Factors In Glaucoma
Decision-Making
IOP and type of glaucoma
Rate of progression
Lifeexpectancy
Severity of disease
CONCLUSION
2/13/2019
1
Zanna Kruoch, OD, FAAO, ABO DiplomateAssistant ProfessorUniversity of Houston, College of Optometry
› I have received honoraria from:– Essilor Custom Contact Lens Specialist
› Assistant Professor – University of Houston, College of Optometry
› Opinions from this lecture are my own
› Identify key elements in an examination to aid in the diagnosis of uveitis.
› When to utilize further history and/or laboratory testing to aid in the diagnosis of uveitis.
› Be able to build a list of systemic differentials associated with uveitis.
The Fundamentals of Building the Ocular Differentials
CC: “red, painful eye"
› CC: red, painful eye
› HPI: – Right eye– Onset 4 days ago– Gradually getting worse– Constant– 1st episode started 2 years ago. Occurs every 3-4 months. Only
right eye.– Associated symptoms: photophobia, pain on the right side of the
head– No discharge– Mild head relief with Tylenol BID po
2/13/2019
2
› POH:– Unremarkable
› PMH:– Hypothyroidism, primary
› Systemic Medications:– Levothyroxine
› ALL:– Penicillin
› Intraocular Pressures – OD 38 mmHg– OS 14 mmHg– Time: 8:39 am
› VA (sc)– OD 20/20– OS 20/25, PH 20/20
› EOMs– Unrestricted OD, OS
› CF– FTFC OD, OS
› PERRL (-) APD– Marked photophobia
Determining the ocular differentials
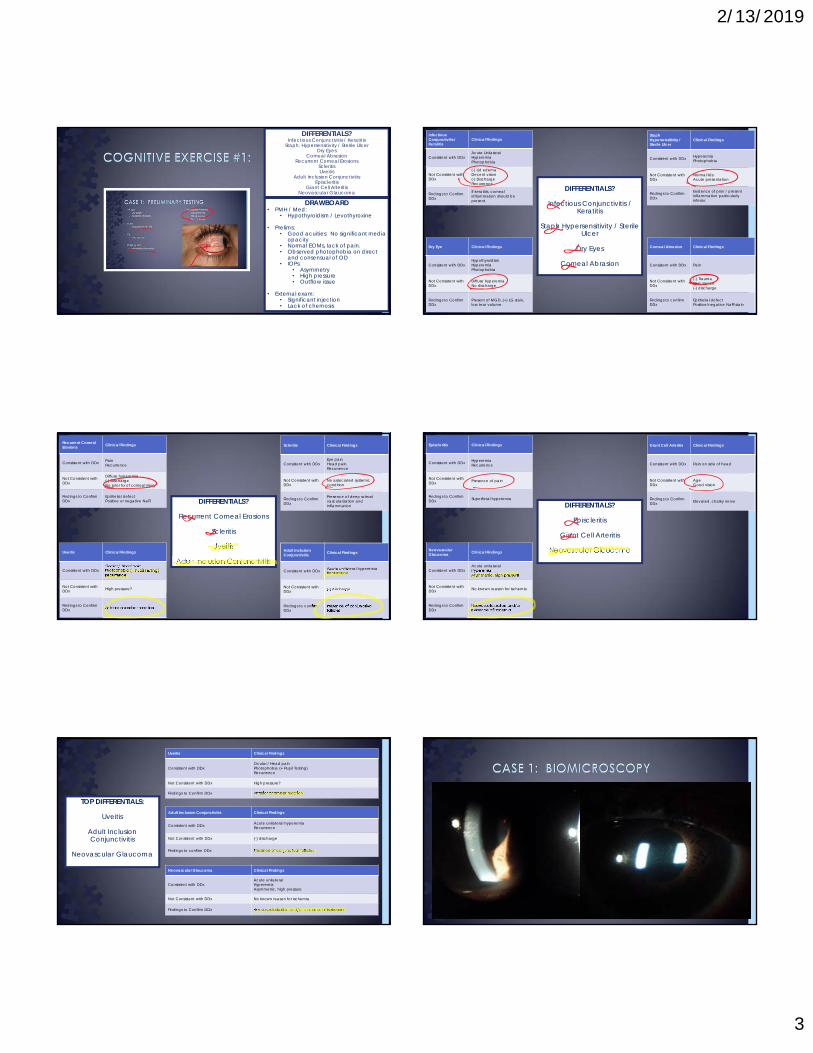
DIFFERENTIALS?
Infectious Conjunctivitis / Keratitis
Staph. Hypersensitivity / Sterile Ulcer
Dry Eyes
Corneal Abrasion
Recurrent Corneal Erosions
Scleritis
Uveitis
DRAWBOARD• Age/Race/Gender:
• 41 yro:• Collagen-vascular auto-
immune?• MS?
• Hispanic:• Secondary inflammation from
DM?• Female
• Adnexa / External:• No lid lesions evident• No lid edema• Hyperemia, no evident discharge• No heavy flaking or madarosis
DIFFERENTIALS?
Infectious Conjunctivitis / KeratitisStaph. Hypersensitivity / Sterile Ulcer
Dry EyesCorneal Abrasion
Recurrent Corneal ErosionsScleritisUveitis
DRAWBOARD• CC: red and painful
• Inflammation• Corneal pain receptors
• HPI:• Acute unilateral red eye:
• Infectious i.e. viral or bacterial?• Hx of recurrence:
• Chlamydia? Episcleritis or iritis? • Photophobia:
• CB spasm• Corneal defect causing spasms?
• Head pain:• GCA?• Scleritis?
• Lack of discharge:• Less likely to be infectious
DIFFERENTIALS?Infectious Conjunctivitis / Keratitis
Staph. Hypersensitivity / Sterile UlcerDry Eyes
Corneal AbrasionRecurrent Corneal Erosions
ScleritisUveitis
Adult Inclusion ConjunctivitisEpiscleritis
Giant Cell Arteritis
2/13/2019
3
DIFFERENTIALS?Infectious Conjunctivitis / Keratitis
Staph. Hypersensitivity / Sterile UlcerDry Eyes
Corneal AbrasionRecurrent Corneal Erosions
ScleritisUveitis
Adult Inclusion ConjunctivitisEpiscleritis
Giant Cell ArteritisNeovascular Glaucoma
DRAWBOARD• PMH / Med:
• Hypothyroidism / Levothyroxine
• Prelims:• Good acuities: No significant media
opacity• Normal EOMs, lack of pain. • Observed photophobia on direct
and consensual of OD• IOPs:
• Asymmetry• High pressure• Outflow issue
• External exam:• Significant injection• Lack of chemosis
DIFFERENTIALS?
Infectious Conjunctivitis / Keratitis
Staph Hypersensitivity / Sterile Ulcer
Dry Eyes
Corneal Abrasion
InfectiousConjunctivitis / Keratitis
Clinical Findings
Consistent with DDxAcute UnilateralHyperemiaPhotophobia
Not Consistent with DDx
(-) Lid edemaDecent vision(-) DischargeRecurrence
Findings to Confirm DDx
If keratitis, corneal inflammation should be present.
Staph Hypersensitivity / Sterile Ulcer
Clinical Findings
Consistent with DDx HyperemiaPhotophobia
Not Consistent with DDx
Normal lidsAcute presentation
Findings to Confirm DDx
Evidence of prior / present inflammation particularly inferior.
Dry Eye Clinical Findings
Consistent with DDxHypothyroidismHyperemiaPhotophobia
Not Consistent with DDx
Diffuse hyperemiaNo discharge
Findings to Confirm DDx
Present of MGD, (+) LG stain, low tear volume.
Corneal Abrasion Clinical Findings
Consistent with DDx Pain
Not Consistent with DDx
(-) TraumaRecurrence(-) discharge
Findings to confirm DDx
Epithelial defectPositive/negative NaFl stain
DIFFERENTIALS?
Recurrent Corneal Erosions
Scleritis
Uveitis
Adult Inclusion Conjunctivitis
Recurrent Corneal Erosions Clinical Findings
Consistent with DDx PainRecurrence
Not Consistent with DDx
Diffuse hyperemia(-) DischargeNo prior hx of corneal injury
Findings to Confirm DDx
Epithelial defectPositive or negative NaFl
Scleritis Clinical Findings
Consistent with DDxEye painHead painRecurrence
Not Consistent with DDx
No associated systemiccondition
Findings to Confirm DDx
Presence of deep scleral vascularization and inflammation
Uveitis Clinical Findings
Consistent with DDxOcular / Head painPhotophobia (+ Pupil Testing)Recurrence
Not Consistent with DDx High pressure?
Findings to Confirm DDx Anterior chamber reaction
Adult Inclusion Conjunctivitis Clinical Findings
Consistent with DDx Acute unilateral hyperemiaRecurrence
Not Consistent with DDx (-) discharge
Findings to confirm DDx
Presence of conjunctival follicles
Adult Inclusion Conjunctivitis Clinical Findings
Consistent with DDx Acute unilateral hyperemiaRecurrence
Not Consistent with DDx (-) discharge
Findings to confirm DDx
Presence of conjunctival follicles
Episcleritis Clinical Findings
Consistent with DDx HyperemiaRecurrence
Not Consistent with DDx Presence of pain
Findings to Confirm DDx Superficial hyperemia
Giant Cell Arteritis Clinical Findings
Consistent with DDx Pain on side of head
Not Consistent with DDx
AgeGood vision
Findings to Confirm DDx Elevated, chalky nerve
NeovascularGlaucoma Clinical Findings
Consistent with DDxAcute unilateralHyperemiaAsymmetric, high pressure
Not Consistent with DDx No known reason for ischemia
Findings to Confirm DDx
Neovascularization and/or evidence of ischemia
DIFFERENTIALS?
Episcleritis
Giant Cell Arteritis
Neovascular Glaucoma
TOP DIFFERENTIALS:
Uveitis
Adult Inclusion Conjunctivitis
Neovascular Glaucoma
Uveitis Clinical Findings
Consistent with DDxOcular / Head painPhotophobia (+ Pupil Testing)Recurrence
Not Consistent with DDx High pressure?
Findings to Confirm DDx Anterior chamber reaction
Adult Inclusion Conjunctivitis Clinical Findings
Consistent with DDx Acute unilateral hyperemiaRecurrence
Not Consistent with DDx (-) discharge
Findings to confirm DDx Presence of conjunctival follicles
Neovascular Glaucoma Clinical Findings
Consistent with DDxAcute unilateralHyperemiaAsymmetric, high pressure
Not Consistent with DDx No known reason for ischemia
Findings to Confirm DDx Neovascularization and/or evidence of ischemia

2/13/2019
4
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
3+ injection temporally, 2+ diffuse injection elsewhere,
(-) folliclesCONJUNCTIVA white and quiet
4-5 scattered fine KPs diffusely, 1 pigmented fine
KPCORNEA clear, (-) KPs
3+ cells, 1+ flare A/C (-) C/F
flat, brown, (-) nodules, (-) NVI IRIS flat, brown, (-) nodules
clear LENS clear
clear, (-) cells VITREOUS clear, (-) cells
› Assessment:1. Non-granulomatous anterior uveitis OD.
› History of recurrence.
› Plan:1. In-office instillation of 1 gtt Scopolamine 0.25% and 1 gtt
Pred Forte OD. Start Pred Forte 1% q2h OD during waking hours. RTC 2 days for f/u, IOP ck, and DFE.
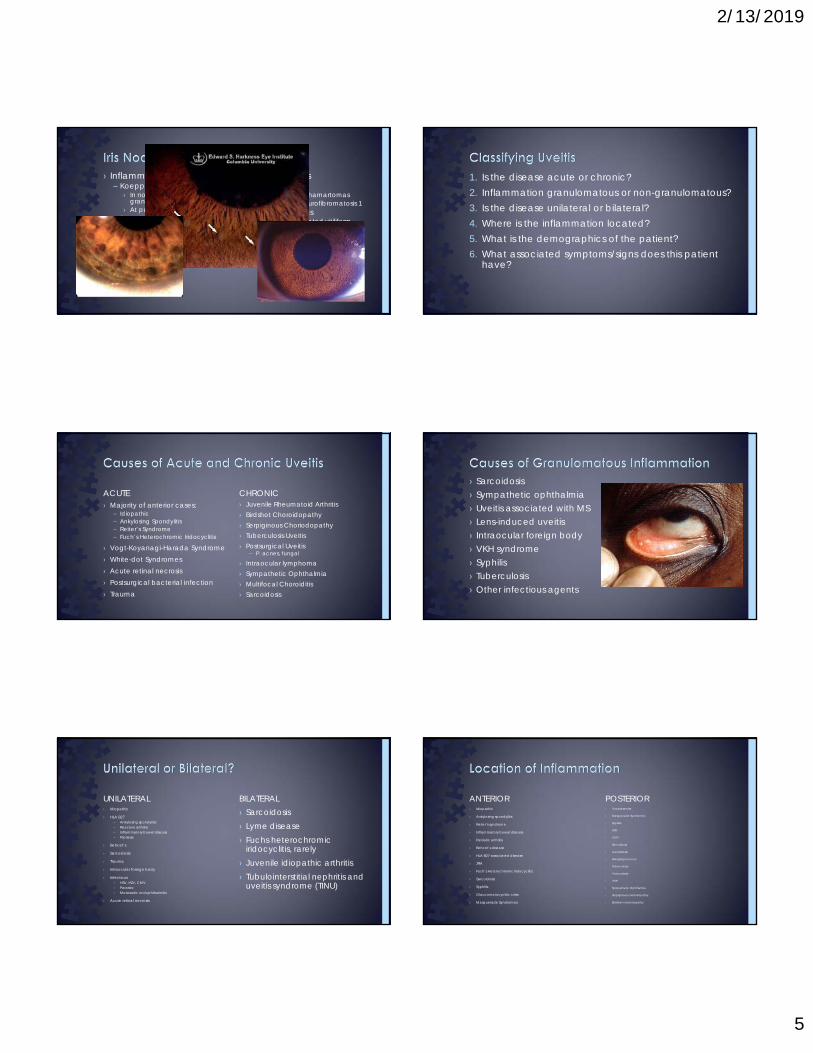
› Inflammation of the uveal tissue – iris, ciliary body, choroid
› Symptoms include pain, photophobia, decreased vision.
› Two broad types:– Nongranulomatous
› Fine KPs› Koeppe nodules
– Granulomatous› Mutton fat keratic precipitates› Busacca nodules
› Anterior chamber flare, resulting from extra protein in the aqueous, is usually present.
– 0 = None– 1+ = Faint– 2+ = Moderate (iris and lens detail clear)– 3+ = Marked (iris and lens detail hazy)– 4+ = Intense (fibrin or plastic aqueous)
› Cells, the hallmark of iritis, are present in the aqueous. They should be graded by severity under high-magnification slit lamp examination in a 1 X 3-mm field of light
– 0 < 1– 0.5 = 1-5 cells– 1+ = 6-15 cells– 2+ = 16-25 cells– 3+ = 26-50 cells– 4+ = More than 50 cells
› WBCs that collects on the back of the endothelium– Fresh KPs – round, white, regular in shape– Old KPs- irregular in shape, pigmented
› Sign of chronic inflammation
› Types:– Fine KPs – typically non-granulomatous– Mutton fat KPs – typically granulomatous– Stellate KPs – part of Fuch’s Heterochromic
Iridocyclitis
2/13/2019
5
› Nevus Nodules– Lisch
› melanocytic hamartomas› present in Neurofibromatosis 1
– Mammallations › Regular, elevated vitiliform
nodules regularly spaced on hyperpigmented iris
› Unilateral› Seen in association with ocular
melanocytosis– 1 in 400 with ocular
melanocytosis will develop uveal melanoma
› Can be associated with high IOP
› Inflammatory Nodules– Koeppe
› In nongranulomatous and granulomatous
› At pupillary margin– Busacca
› Almost always granulomatous› At mid-periphery
1. Is the disease acute or chronic?2. Inflammation granulomatous or non-granulomatous?3. Is the disease unilateral or bilateral?4. Where is the inflammation located?5. What is the demographics of the patient?6. What associated symptoms/signs does this patient
have?
› Juvenile Rheumatoid Arthritis› Birdshot Choroidopathy› Serpiginous Choriodopathy› Tuberculosis Uveitis› Postsurgical Uveitis
– P. acnes, fungal
› Intraocular lymphoma› Sympathetic Ophthalmia› Multifocal Choroiditis› Sarcoidosis
CHRONIC› Majority of anterior cases:
– Idiopathic– Ankylosing Spondylitis– Reiter’s Syndrome– Fuch’s Heterochromic Iridocyclitis
› Vogt-Koyanagi-Harada Syndrome› White-dot Syndromes› Acute retinal necrosis› Postsurgical bacterial infection› Trauma
ACUTE› Sarcoidosis› Sympathetic ophthalmia› Uveitis associated with MS› Lens-induced uveitis› Intraocular foreign body› VKH syndrome› Syphilis› Tuberculosis› Other infectious agents
› Sarcoidosis› Lyme disease› Fuchs heterochromic
iridocyclitis, rarely› Juvenile idiopathic arthritis› Tubulointerstitial nephritis and
uveitis syndrome (TINU)
BILATERAL› Idiopathic
› HLA B27– Ankylosing spondylitis– Reactive arthritis– Inflammatory bowel disease– Psoriasis
› Behcet’s
› Sarcoidosis
› Trauma
› Intraocular foreign body
› Infectious– HSV, HZV, CMV– Parasitic– Metastatic endophthalmitis
› Acute retinal necrosis
UNILATERAL› Toxoplasmosis
› Masquerade Syndromes
› Syphilis
› HSV
› CMV
› Sarcoidosis
› Candidiasis
› Mengingococcus
› Tuberculosis
› Toxocariasis
› VKH
› Sympathetic Ophthalmia
› Serpiginous choriodopathy
› Birdshot choriodopathy
POSTERIOR› Idiopathic
› Ankylosing spondylitis
› Reiter’s syndrome
› Inflammatory bowel disease
› Psoriatic arthritis
› Behcet’s disease
› HLA-B27-associated disease
› JRA
› Fuch’s Heterochromic Iridocyclitis
› Sarcoidosis
› Syphilis
› Glaucomatocyclitic crisis
› Masquerade Syndromes
ANTERIOR
2/13/2019
6
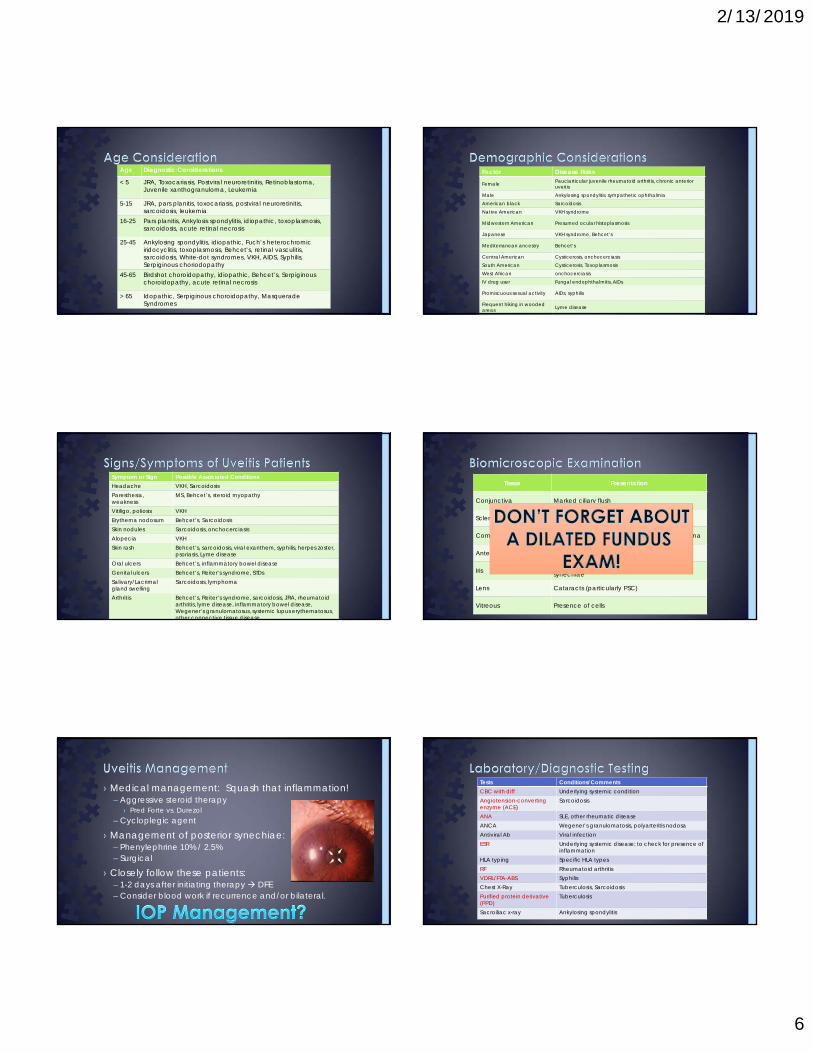
Age Diagnostic Considerations
< 5 JRA, Toxocariasis, Postviral neuroretinitis, Retinoblastoma, Juvenile xanthogranuloma, Leukemia
5-15 JRA, pars planitis, toxocariasis, postviral neuroretinitis, sarcoidosis, leukemia
16-25 Pars planitis, Ankylosis spondylitis, idiopathic, toxoplasmosis, sarcoidosis, acute retinal necrosis
25-45 Ankylosing spondylitis, idiopathic, Fuch’s heterochromiciridocyclitis, toxoplasmosis, Behcet’s, retinal vasculitis, sarcoidosis, White-dot syndromes, VKH, AIDS, Syphilis, Serpiginous choriodopathy
45-65 Birdshot choroidopathy, idiopathic, Behcet’s, Serpiginouschoroidopathy, acute retinal necrosis
> 65 Idopathic, Serpiginous choroidopathy, Masquerade Syndromes
Factor Disease Risks
Female Pauciarticular juvenile rheumatoid arthritis, chronic anterior uveitis
Male Ankylosing spondylitis, sympathetic ophthalmiaAmerican black Sarcoidosis
Native American VKH syndrome
Midwestern American Presumed ocular histoplasmosis
Japanese VKH syndrome, Behcet’s
Mediterranean ancestry Behcet’s
Central American Cysticerosis, onchocerciasisSouth American Cysticerosis, Toxoplasmosis
West African onchocerciasisIV drug user Fungal endophthalmitis, AIDs
Promiscuous sexual activity AIDs, syphilis
Frequent hiking in wooded areas Lyme disease
Symptom or Sign Possible Associated ConditionsHeadache VKH, SarcoidosisParesthesia,weakness
MS, Behcet’s, steroid myopathy
Vitiligo, poliosis VKHErythema nodosum Behcet’s, SarcoidosisSkin nodules Sarcoidosis, onchocerciasisAlopecia VKHSkin rash Behcet’s, sarcoidosis, viral exanthem, syphilis, herpes zoster,
psoriasis, Lyme diseaseOral ulcers Behcet’s, inflammatory bowel diseaseGenital ulcers Behcet’s, Reiter’s syndrome, STDsSalivary/Lacrimal gland swelling
Sarcoidosis, lymphoma
Arthritis Behcet’s, Reiter’s syndrome, sarcoidosis, JRA, rheumatoid arthritis, lyme disease, inflammatory bowel disease, Wegener’s granulomatosus, systemic lupus erythematosus, other connective tissue disease
Tissue Presentation
Conjunctiva Marked ciliary flush
Sclera Scleritis
Cornea Presence of keratic precipitates, corneal edema
Anterior chamber Cells, flare, or hypopyon
Iris Atrophy of iris, heterochromia, posterior synechiae
Lens Cataracts (particularly PSC)
Vitreous Presence of cells
› Medical management: Squash that inflammation!– Aggressive steroid therapy
› Pred Forte vs. Durezol– Cycloplegic agent
› Management of posterior synechiae:– Phenylephrine 10% / 2.5%– Surgical
› Closely follow these patients:– 1-2 days after initiating therapy DFE– Consider blood work if recurrence and/or bilateral.
Tests Conditions/CommentsCBC with diff Underlying systemic conditionAngiotension-converting enzyme (ACE)
Sarcoidosis
ANA SLE, other rheumatic diseaseANCA Wegener’s granulomatosis, polyarteritis nodosaAntiviral Ab Viral infectionESR Underlying systemic disease; to check for presence of
inflammationHLA typing Specific HLA typesRF Rheumatoid arthritisVDRL/FTA-ABS SyphilisChest X-Ray Tuberculosis, SarcoidosisPurified protein derivative (PPD)
Tuberculosis
Sacroiliac x-ray Ankylosing spondylitis
2/13/2019
7
The Exercise of Building the Systemic Differentials for Uveitis
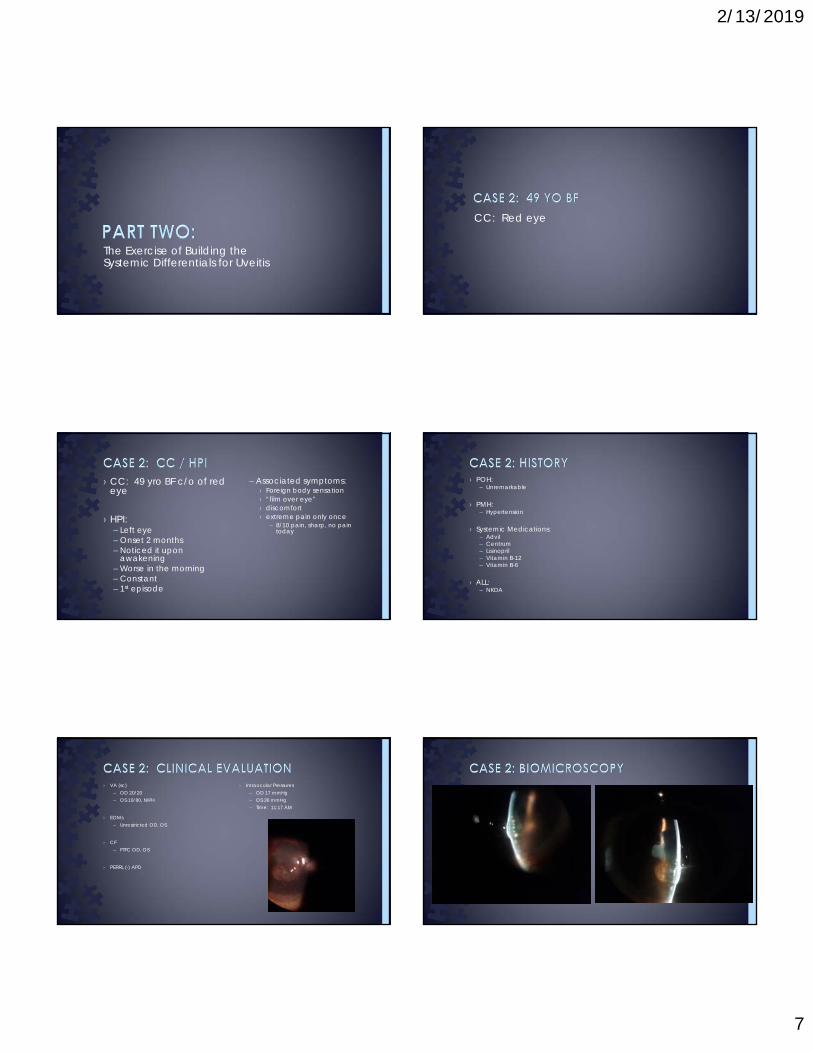
CC: Red eye
– Associated symptoms: › Foreign body sensation› “film over eye”› discomfort› extreme pain only once
– 8/10 pain, sharp, no pain today
› CC: 49 yro BF c/o of red eye
› HPI: – Left eye– Onset 2 months – Noticed it upon
awakening– Worse in the morning– Constant– 1st episode
› POH:– Unremarkable
› PMH:– Hypertension
› Systemic Medications:– Advil– Centrum– Lisinopril– Vitamin B-12– Vitamin B-6
› ALL:– NKDA
› Intraocular Pressures – OD 17 mmHg– OS 36 mmHg– Time: 11:17 AM
› VA (sc)– OD 20/20– OS 10/80, NIPH
› EOMs– Unrestricted OD, OS
› CF– FTFC OD, OS
› PERRL (-) APD
2/13/2019
8
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
white and quiet CONJUNCTIVA 1+ injection
Clear, (-) KPs CORNEA
Intraepithelial bullae, localized cornea edema, (+) MF KPs inferior, (+) fine
KPs centrally
(-) C/F A/C(+) C/F – however difficult
to visualize due to presence of k-edema
flat, brown, (-) nodules IRIS (+) posterior synechiae @ 10, 11, and 1 o’clock
clear LENS clear
clear, (-) cells VITREOUS clear, (-) cells
OD OS
Clear, (-) cells VITREOUS
0.35 R C/D
distinct DISC
pink, healthy RIM
(+) FR, flat MACULA
2/3 VESSELS
RED REFLEXHAZY VIEWS
› Assessment:1. Granulomatous anterior uveitis OS.
› 1st episode
› Plan:1. In-office instillation of 1 gtt Homatropine 5%, 1 gtt Durezol,
and 1 gtt Azopt OS. Start Durezol QID OS, HomatropineBID, and Azopt BID OS. Return 3 days for follow-up and fundus evaluation. Uveitis survey given to patient to complete.
› Series of questions to help identify systemic cause of uveitis
› When to administer survey:– Nonresponsive to treatment– Granulomatous anterior uveitis– Recurrence of uveitis– Posterior uveitis
2/13/2019
9
› Pros:– Detailed and easy to understand for patients– Inclusive– Useful in deciding what bloodwork to order
› Cost effective
› Cons:– Symptoms that may be late in the course of the disease; not
very useful– May need to repeat
› Several online available› Uveitis.org offers an example:
– http://www.uveitis.org/uveitis-questionnaire
› Email me for our clinic’s uveitis survey– [email protected]
› Prior illnesses:– Night sweats– Headaches– Sinus problems– White patches of hair or skin– Loss of hair
› Social Hx:– Own a dog– Cigarette use– BCP use
› Prior conditions:– HTN– Herpes (cold sores)– Chickenpox– Measles– Mumps– Allergies
Utilizing the uveitis survey to extract differential diagnoses.
DIFFERENTIALS:Toxocariasis
HSVSarcoidosis
VKH Breaking down the case to extract differentials.
2/13/2019
10
DIFFERENTIALS:Toxocariasis
HSVVKH
SarcoidosisBehcet’s Disease
Acute Retinal NecrosisBirdshot Chorioretinitis
Serpiginous Retinopathy
DIFFERENTIALS:Toxocariasis
HSVVKH
SarcoidosisBehcet’s Disease
Acute Retinal NecrosisBirdshot Chorioretinitis
Serpiginous Retinopathy
DIFFERENTIALS:Toxocariasis
HSVVKH
SarcoidosisBehcet’s Disease
Acute Retinal NecrosisBirdshot Chorioretinitis
Serpiginous Retinopathy
› Lyme Disease› Coccidiodomycosis› Leprosy› Toxoplasmosis› Brucellosis› Post surgical
inflammation› Necrotizing
herpetic retinopathies– Acute retinal
necrosis (ARN)– Progressive Outer
Retinal Necrosis (PORN)
› Sarcoidosis› Sympathetic
ophthalmia› Uveitis associated
with MS› Intraocular foreign
body› Vogt-Koyanagi-
Harada syndrome› Syphilis› Tuberculosis› HSV, VZV, CMV, EBV› Toxocara canis
DIFFERENTIALS:Toxocariasis
HSVVKH
SarcoidosisBehcet’s Disease
Acute Retinal NecrosisBirdshot Chorioretinitis
Serpiginous Retinopathy
DIFFERENTIALS:Toxocariasis
HSVVKH
SarcoidosisBehcet’s Disease
Acute Retinal NecrosisBirdshot Chorioretintis
Serpiginous Retinopathy
› Subtypes:– HSV-1: infection in or around mouth– HSV-2: infection of genital or anal area
› HSV-1:– More likely to cause ocular complications than HSV-2– Highly contagious– Commonly acquired during childhood and remains latent and
asymptomatic– Symptoms:
› Mildly painful mouth sores› In immunocompromised patients, severe symptoms can occur with
frequent recurrence

2/13/2019
11
› Most common manifestation: HSV Keratitis– Granulomatous inflammation from Descemets to Bowmans in
stromal disease– T-cell mediated immune response with HSV antigens located in
deep stroma and endothelium– Can affect all layers of the cornea
› HSV Epithelial Keratitis is the most common herpetic infection› HSV Stromal Keratitis is the most common recurrent herpetic infection
› HSV-associated Uveitis:– Typically unilateral– Associated with acute ocular hypertension– Can be nongranulomatous or granulomatous inflammation– Residual damage can lead to iris atrophy
› Chronic granulomatous inflammation that can affect several organs
› Gold standard of diagnosis is the presence of non-caseating granulomata on tissue biopsy– Ancillary testing can be obtained if biopsy is not possible
› Ocular involvement can occur before systemic disease in up to 30% of cases
› Bimodal age distribution of ocular sarcoidosis– 20 to 30 yro– 50 to 60 yro
› African Americans are more likely to develop ocular involvement than Caucasians
› Females more likely than males to develop ocular involvement
› Most common:– Uveitis– Dry Eye– Conjunctival Nodules
› Less common:– Multifocal choroiditis– Retinal vasculitis:
› “Candle-wax drippings” exudates› Perivascular sheathing
https://openi.nlm.nih.gov/imgs/512/140/2855661/PMC2855661_MEAJO-16-202-g028.pnghttp://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/pulmonary/sarcoidosis/#figure9
› Ocular involvement:– Decrease vision or visual field defect– Visual hallucinations– Papilledema– EOM defects– Pupillary defects
› Other neurological involvement:– Cranial neuropathy: optic and facial most commonly affected– Encephalopathy– Vasculopathy– Peripheral neuropathy– Meningitis– Hydrocephalus
› Ocular Sarcoidosis can affect any structure of the eye and its adnexa.
› Uveitis is one of the most common findings.
› Race, age, chronic history
› HSV typically presents with corneal inflammation
› Uveitis can occur in HSV but not as likely
› Lack of iris atrophy
2/13/2019
12
Tests Conditions/CommentsCBC with diff Underlying systemic condition
Angiotension-converting enzyme (ACE) Sarcoidosis
ANA SLE, other rheumatic diseaseANCA Wegener’s granulomatosis, polyarteritis nodosaAntiviral Ab Viral infectionESR Underlying systemic disease; to check for presence of
inflammationHLA typing Specific HLA typesRF Rheumatoid arthritisVDRL/FTA-ABS SyphilisChest X-Ray Tuberculosis, SarcoidosisPurified protein derivative (PPD) Tuberculosis
Sacroiliac x-ray Ankylosing spondylitis
Lysozome Sarcoidosis
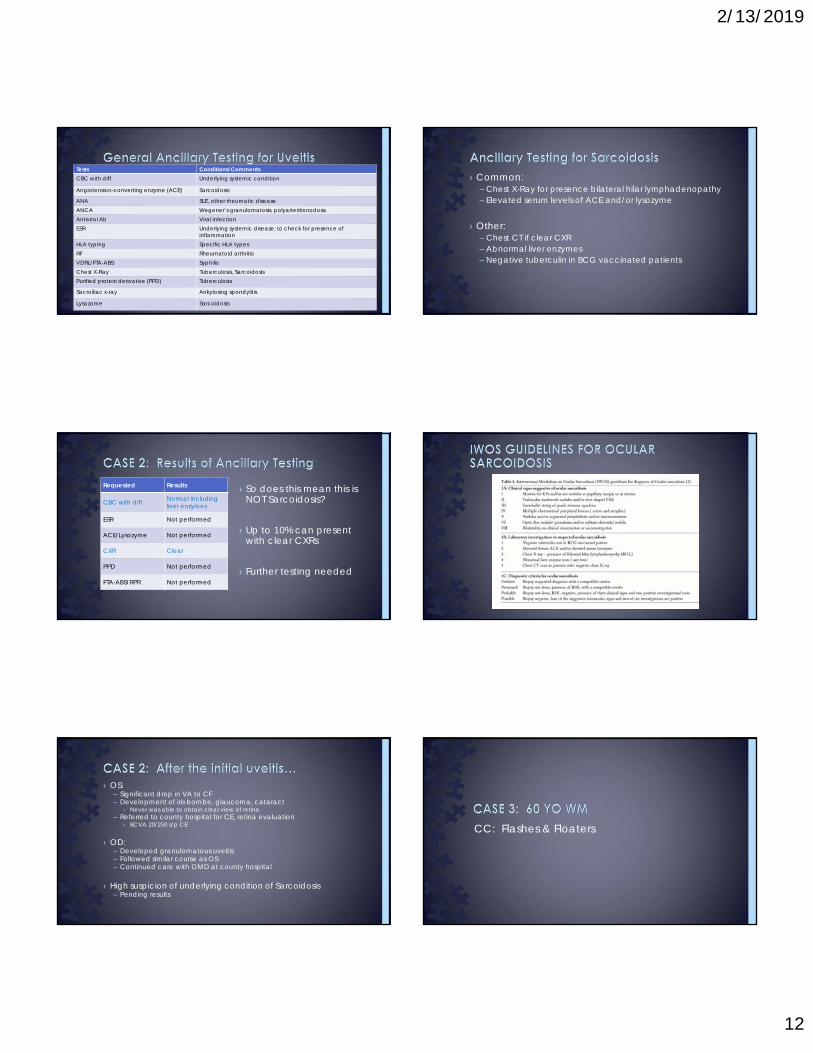
› Common:– Chest X-Ray for presence bilateral hilar lymphadenopathy– Elevated serum levels of ACE and/or lysozyme
› Other:– Chest CT if clear CXR– Abnormal liver enzymes– Negative tuberculin in BCG vaccinated patients
› So does this mean this is NOT Sarcoidosis?
› Up to 10% can present with clear CXRs
› Further testing needed
Requested Results
CBC with diff Normal including liver enzymes
ESR Not performed
ACE/Lysozyme Not performed
CXR Clear
PPD Not performed
FTA-ABS/RPR Not performed
› OS:– Significant drop in VA to CF– Development of iris bombe, glaucoma, cataract
› Never was able to obtain clear view of retina– Referred to county hospital for CE, retina evaluation
› BCVA 20/250 s/p CE
› OD:– Developed granulomatous uveitis– Followed similar course as OS– Continued care with OMD at county hospital
› High suspicion of underlying condition of Sarcoidosis– Pending results
CC: Flashes & Floaters
2/13/2019
13
› CC: flashes and floaters
› HPI: – OS > OD– Persistent flashes OS started 2 months ago, OD has occurred
“every now and then”– Associated symptoms:
› Constant “cloudy vision OS” which started before flashes› Experiencing vertigo with flashes and cloudy vision
› POH:– Retinal tear s/p laser OS – 2 years prior
› PMH:– Adult Rheumatoid Arthritis– HIV: per pt “well controlled” although unknown CD4 and viral load
› Systemic Medications:– Aleve– Meloxicam– Stribild– Tylenol
› ALL:– NKDA
› Intraocular Pressures – OD 17 mmHg– OS 11 mmHg– Time 1:10 pm
› VA (sc)– OD 20/20– OS 20/30, NIPH
› EOMs– Unrestricted OD, OS
› CF– FTFC OD, OS
› PERRL (-) APD
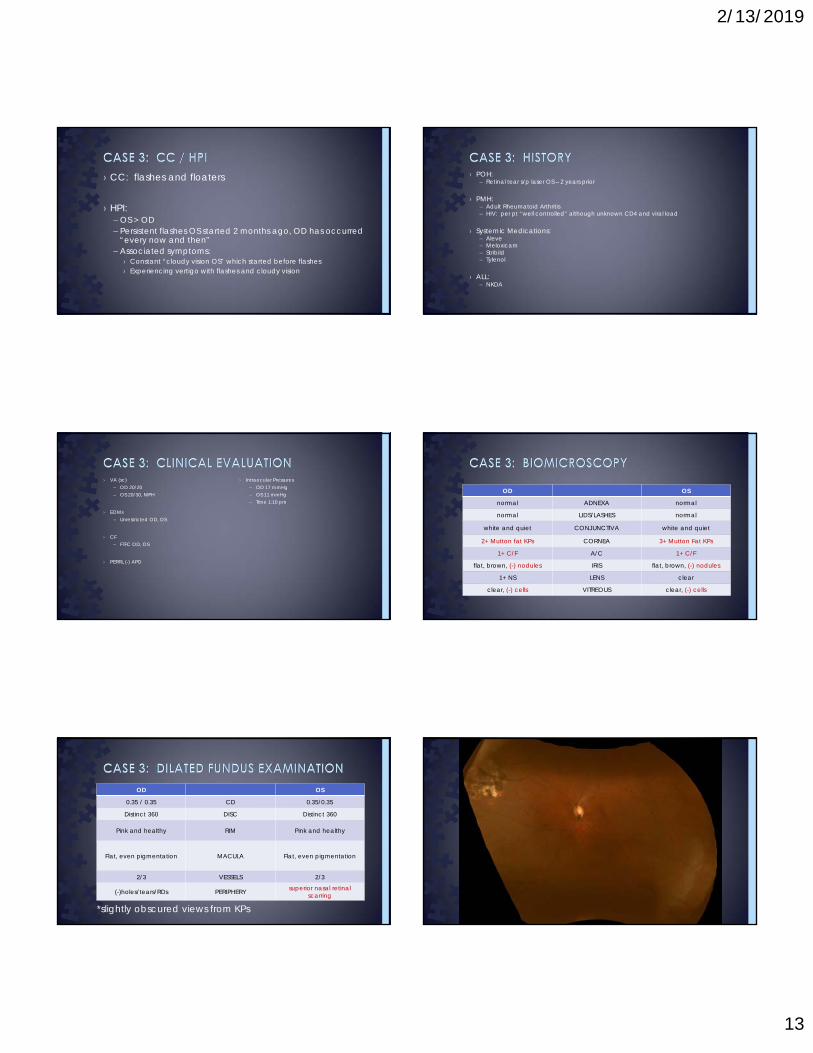
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
white and quiet CONJUNCTIVA white and quiet
2+ Mutton fat KPs CORNEA 3+ Mutton Fat KPs
1+ C/F A/C 1+ C/F
flat, brown, (-) nodules IRIS flat, brown, (-) nodules
1+ NS LENS clear
clear, (-) cells VITREOUS clear, (-) cells
OD OS
0.35 / 0.35 CD 0.35/0.35
Distinct 360 DISC Distinct 360
Pink and healthy RIM Pink and healthy
Flat, even pigmentation MACULA Flat, even pigmentation
2/3 VESSELS 2/3
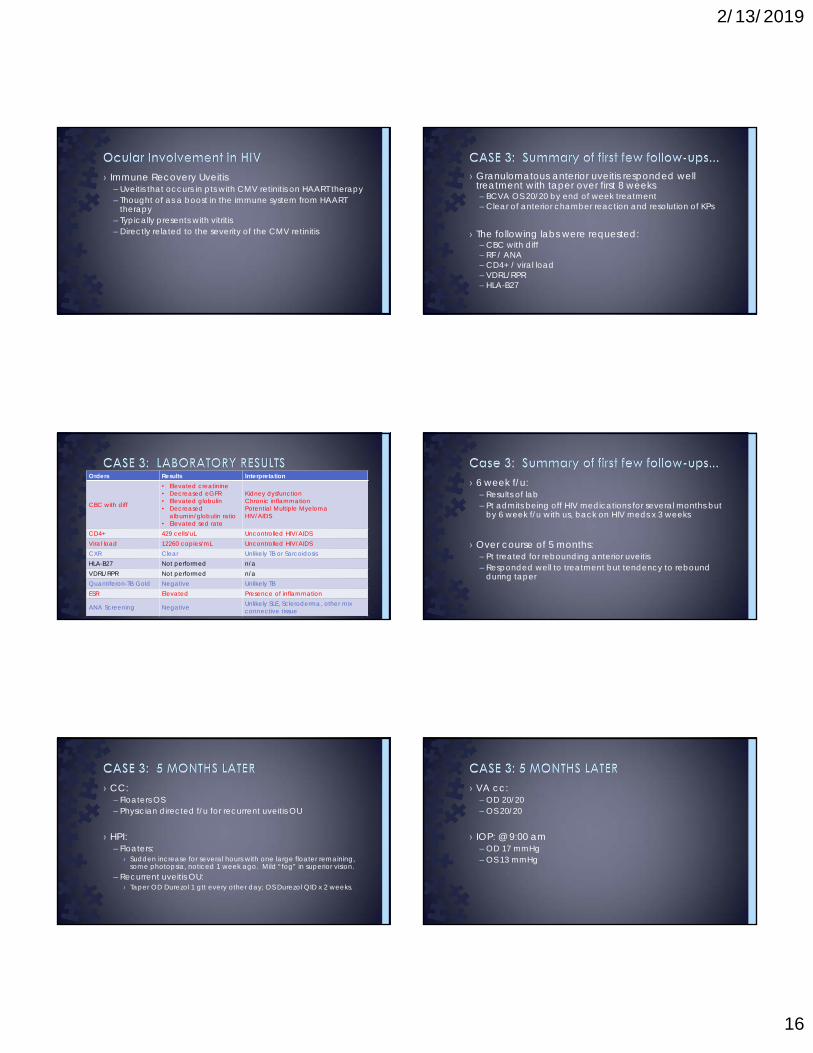
(-)holes/tears/RDs PERIPHERY superior nasal retinal scarring
*slightly obscured views from KPs

2/13/2019
14
› Assessment:– Bilateral anterior granulomatous uveitis
› Plan:– Start Omnipred 8x/day, Cyclopentolate QID OU.– Uveitis survey given.– RTC 1 week. Building the systemic differentials list.
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
VKH
› Current/Prior Conditions:– Anemia– Hepatitis– HTN– Pneumonia– Herpes– Chickenpox– Shingles– Measles– AIDS/HIV– Rheumatoid Arthritis
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
VKHAIDS/HIV
Rheumatoid Arthritis
› Prior symptoms:– Night sweats– Fatigue– Poor appetite– Tingling/numbness of ears– Hearing/ringing of ears– Painfully cold fingers– Sore in the
throat/sneezing/sinus problems
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
VKHAIDS/HIV
Rheumatoid Arthritis
› Symptoms:– Stiff joints– Stiff lower back– Back pain while sleeping
› Social Hx:– Owned dogs– Bisexual/homosexual relations
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
VKHAIDS/HIV
Rheumatoid ArthritisAnkylosing Spondylitis
Toxocariasis

2/13/2019
15
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
VKHAIDS/HIV
Rheumatoid ArthritisAnkylosing Spondylitis
Toxocariasis
› Inflammatory polyarthritis characterized by inflammation of the joint, leading to synovial joint destruction– Extremities– Cervical spine
› Females > Males
› Can start at any age but most common ages of 40-60
› 25% of RA patients will have ocular involvement
› Greater tendency to affect anterior vs. posterior segment– Most common:
› Dry eyes› Episcleritis / Scleritis:
– May extend to uvea causing uveitis› Peripheral ulcerative keratitis
– Less common:› Choroiditis› Retinal vasculitis (sub-type of uveitis)› Macular edema› Retinal detachments
› Scleritis: – Uncommon inflammation of sclera usually resulting in extreme pain– Scleritis prevalence of 4-10% in RA patients– RA-related scleritis makes up 1/3 of all scleritis cases– Anterior scleritis is much more common than posterior (90% vs 10%)
› Classified base on:– Distribution:
› Diffuse affecting one or more quadrants› Nodular with tenderness and scleral thickening
– Destruction: › Necrotizing › Non-necrotizing
› Uveitis:– Not typically associated with adult RA– Present concurrently with scleritis
http://emedsa.org.au/EDHandbook/eyes/redeye/Scleritis2.jpg
› Retrovirus largely affecting helper CD4+ T cells resulting in severe immunosuppression
› Initially homosexual/bisexual activity accounted for most transmission until early 1990s; now heterosexual activity is the major route of transmission– IV drug abuse– Perinatal transmission– Needle stick injury
› Can affect almost every tissue of the eye– Most common:
› Dry eye› Retinal microvasculopathy› CMV retinitis
– CD4+ count drops below 200 ocular involvement› CMV retinitis likely when CD4+ count below 50 - 100
› CMV Retinitis most frequent ocular infection in HIV – If uveitis present typically mild non-granulomatous uveitis – Clinical presentation:
› Slowly progression of retinal whitening spreading along the vasculature with hemorrhages
› Necrosis leads to thin atrophic retina leading to higher risk of RDs› Optic nerve may be involved› Low grade vitritis
2/13/2019
16
› Immune Recovery Uveitis– Uveitis that occurs in pts with CMV retinitis on HAART therapy– Thought of as a boost in the immune system from HAART
therapy – Typically presents with vitritis– Directly related to the severity of the CMV retinitis
› Granulomatous anterior uveitis responded well treatment with taper over first 8 weeks– BCVA OS 20/20 by end of week treatment– Clear of anterior chamber reaction and resolution of KPs
› The following labs were requested:– CBC with diff– RF / ANA– CD4+ / viral load – VDRL/RPR– HLA-B27
Orders Results Interpretation
CBC with diff
• Elevated creatinine• Decreased eGFR• Elevated globulin• Decreased
albumin/globulin ratio• Elevated sed rate
Kidney dysfunctionChronic inflammationPotential Multiple MyelomaHIV/AIDS
CD4+ 429 cells/uL Uncontrolled HIV/AIDSViral load 12260 copies/mL Uncontrolled HIV/AIDSCXR Clear Unlikely TB or SarcoidosisHLA-B27 Not performed n/aVDRL/RPR Not performed n/aQuantiferon-TB Gold Negative Unlikely TBESR Elevated Presence of inflammation
ANA Screening Negative Unlikely SLE, Scleroderma, other mix connective tissue
› 6 week f/u:– Results of lab– Pt admits being off HIV medications for several months but
by 6 week f/u with us, back on HIV meds x 3 weeks
› Over course of 5 months:– Pt treated for rebounding anterior uveitis– Responded well to treatment but tendency to rebound
during taper
› CC: – Floaters OS– Physician directed f/u for recurrent uveitis OU
› HPI: – Floaters:
› Sudden increase for several hours with one large floater remaining, some photopsia, noticed 1 week ago. Mild “fog” in superior vision.
– Recurrent uveitis OU:› Taper OD Durezol 1 gtt every other day; OS Durezol QID x 2 weeks.
› VA cc: – OD 20/20– OS 20/20
› IOP: @ 9:00 am– OD 17 mmHg– OS 13 mmHg
2/13/2019
17
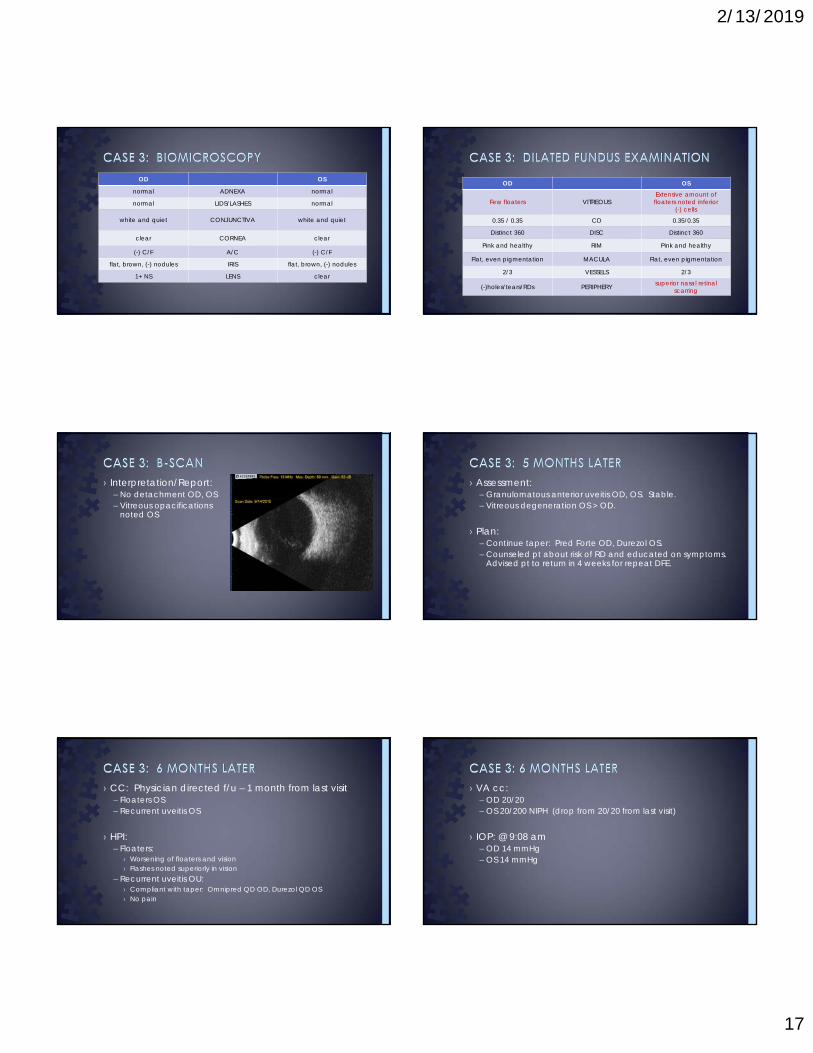
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
white and quiet CONJUNCTIVA white and quiet
clear CORNEA clear
(-) C/F A/C (-) C/F
flat, brown, (-) nodules IRIS flat, brown, (-) nodules
1+ NS LENS clear
OD OS
Few floaters VITREOUSExtensive amount of floaters noted inferior
(-) cells
0.35 / 0.35 CD 0.35/0.35
Distinct 360 DISC Distinct 360
Pink and healthy RIM Pink and healthy
Flat, even pigmentation MACULA Flat, even pigmentation
2/3 VESSELS 2/3
(-)holes/tears/RDs PERIPHERY superior nasal retinal scarring
› Interpretation/Report:– No detachment OD, OS– Vitreous opacifications
noted OS
› Assessment:– Granulomatous anterior uveitis OD, OS. Stable.– Vitreous degeneration OS > OD.
› Plan:– Continue taper: Pred Forte OD, Durezol OS.– Counseled pt about risk of RD and educated on symptoms.
Advised pt to return in 4 weeks for repeat DFE.
› CC: Physician directed f/u – 1 month from last visit– Floaters OS– Recurrent uveitis OS
› HPI: – Floaters:
› Worsening of floaters and vision› Flashes noted superiorly in vision
– Recurrent uveitis OU:› Compliant with taper: Omnipred QD OD, Durezol QD OS› No pain
› VA cc: – OD 20/20– OS 20/200 NIPH (drop from 20/20 from last visit)
› IOP: @ 9:08 am– OD 14 mmHg– OS 14 mmHg
2/13/2019
18
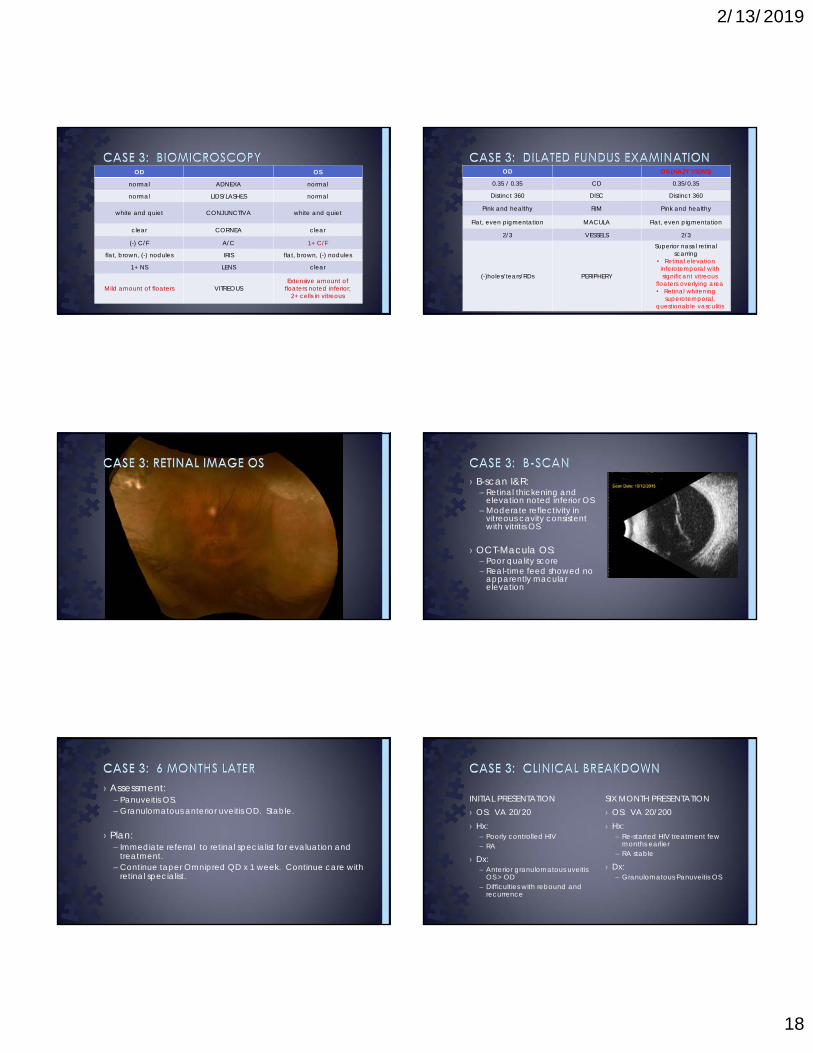
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
white and quiet CONJUNCTIVA white and quiet
clear CORNEA clear
(-) C/F A/C 1+ C/F
flat, brown, (-) nodules IRIS flat, brown, (-) nodules
1+ NS LENS clear
Mild amount of floaters VITREOUSExtensive amount of
floaters noted inferior;2+ cells in vitreous
OD OS (HAZY VIEWS)
0.35 / 0.35 CD 0.35/0.35
Distinct 360 DISC Distinct 360
Pink and healthy RIM Pink and healthy
Flat, even pigmentation MACULA Flat, even pigmentation
2/3 VESSELS 2/3
(-)holes/tears/RDs PERIPHERY
Superior nasal retinal scarring
• Retinal elevation inferotemporal with significant vitreous
floaters overlying area• Retinal whitening
superotemporal, questionable vasculitis
› B-scan I&R:– Retinal thickening and
elevation noted inferior OS– Moderate reflectivity in
vitreous cavity consistent with vitritis OS
› OCT-Macula OS:– Poor quality score– Real-time feed showed no
apparently macular elevation
› Assessment:– Panuveitis OS.– Granulomatous anterior uveitis OD. Stable.
› Plan:– Immediate referral to retinal specialist for evaluation and
treatment.– Continue taper Omnipred QD x 1 week. Continue care with
retinal specialist.
› OS: VA 20/200› Hx:
– Re-started HIV treatment few months earlier
– RA stable
› Dx:– Granulomatous Panuveitis OS
SIX MONTH PRESENTATIONINITIAL PRESENTATION› OS: VA 20/20› Hx:
– Poorly controlled HIV – RA
› Dx: – Anterior granulomatous uveitis
OS > OD– Difficulties with rebound and
recurrence
2/13/2019
19
› Adult RA:– If uveitis present, typically presents with associated scleritis.
› HIV:– Are retinal findings consistent with CMV retinitis?
› No:– CD4+ count of our patient at 429– Whereas CMV retinitis tends to occur when CD4+ count falls below 50
› CMV retinitis presents with hemorrhages or granular appearance along with uveitis
– Typically non-granulomatous anterior uveitis
DIFFERENTIALS:TuberculosisSarcoidosis
SyphilisHSV/VZV/CMV/EBV
Necrotizing herpetic retinopathies: Acute retinal necrosis (ARN) Progressive Outer Retinal Necrosis (PORN)
VKHAIDS/HIV
Rheumatoid ArthritisAnkylosing Spondylitis
Toxocariasis
› Auto-immune disease characterized by bilateral uveitis– HLA-DR4– Viral triggers
› Higher incidence in Asians, native Americans, Hispanics, Middle Easterners
› Associated with meningeal, auditory, integumentary manifestations– Neurological and auditory occurs prior to uveitis– Integumentary tends to occur after uveitis
› Prodromal:– 1-2 weeks with flu-like symptoms
› Acute:– Acute bilateral posterior uveitis– Non-granulomatous nature first two weeks– Dec VA
› Chronic: – Signs of depigmentation of uveal tissue
› “Sunset glow fundus” depigmentation of the choroid is the most common sign› Nummular chorioretinal scarring
– Signs of depigmentation of integumentary:› Poliosis, alopecia, vitiligo
› Chronic recurrent:– Mild panuveitis with recurrent episodes of anterior uveitis– Recurrence of uveitis changes from nongranulomatous to granulomatous
› Herpetic etiology– VZV most common– HSV second most common
› Generally in immune-competent individuals
› Clinical Presentation:– One or more areas of retinal necrosis
with distinct borders in peripheral retina
› Circumferential spread– Inflammatory reaction of anterior or
vitreous chamber– Rapid progression of disease in
absence of treatment– Occlusive vasculopathy
http://imagebank.asrs.org/Content/imagebank/Image18-ARN-Lecture.jpg/image-full;max$643,0.ImageHandler
2/13/2019
20
› Etiology:– Typically VZV– Other herpetic etiologies have been reported
(CMV, HSV)
› Immunocompromised individuals– HIV patients with CD4+ count of < 50 cells/ul
› Clinical Presentation:– Minimal to no inflammation of aqueous or vitreous
humors– Absence of vascular inflammation– Multifocal or confluent areas of retinal
opacification in peripheral retina– Necrosis creates atrophic, thin areas in the retina
leading to retinal detachments
› Poor prognosis due to difficulties responding to antiviral therapy
http://www.medscape.com/viewarticle/777098_4
› For:– Immunocompromised individual– Areas of retinal whitening
› Against:– Significant aqueous and vitreous
humor inflammation– Suspicious of retinal vasculitis
PORN› For:
– Presence of vitritis– Areas of retinal whitening
› Against:– Pt is immunocompromised
ARN
› Initial reports:– Assessment: Highly suspicious for PORN due to HIV status– Plan:
› Vitrectomy with biopsy› Tx of intravitreal Foscarnet, oral Valtrex› Laboratory titers for Toxoplasmosis, Syphilis
› Later reports:– Positive for Syphilis– Assessment: Syphilitic Retinitis
› Refer for LP› Initiate treatment for Syphilis
› Originally known as luetic disease
› Veneral disease caused by spirochete Treponema pallidum
› Can be acquired or congenital
› High rate of co-infection of HIV and syphilis
› Tertiary:– Affects cardiovascular
system and CNS months to years later
– Categories:› Gummatous syphilis:
– Granulomatous lesions usually at liver, bone, and testes
– Ulcerate then fibrotic› Cardiovascular syphilis:
– 10 years after initial infection– Aneurysm formation
› Neurosyphilis:– Various parts of CNS affected– Argyll-Robertson pupil
› Primary: – Painless chancre at site of
transmission– Highly contagious
› Secondary: – Fever and malaise– Generalized rash especially
at palms and soles
› Latent:– Clinically undetectable– Some will go into tertiary
syphilis while others remain asymptomatic
› Can occur at any stage of syphilis
› All ocular structures can be affected
› Ocular complications include:– Conjunctivitis– Episcleritis / scleritis– Interstitial keratitis– Uveitis (most common finding)– Iris roseolae (dilated iris vessels)– Elevated IOP– Chorioretinitis / retinitis
https://www.reviewofophthalmology.com/article/how-to-recognize-ocular-syphilishttps://www.aao.org/eyenet/article/be-on-lookout-ocular-syphilis
2/13/2019
21
› Anterior Uveitis: – Granulomatous– Isolated anterior uveitis is uncommon
› One study suggested granulomatous anterior uveitis tends to occur in HIV positive patients who are also affected by Syphilis
› Posterior Uveitis:– Most common ocular manifestation– Posterior involvement usually includes:
› Chorioretinitis› Retinitis› Vasculitis› Vitritis› Panuveitis
› Posterior Placoid Chorioretinitis:– Infection of RPE in macular or
peripapillary region– Characterized by ill-defined yellow
placoid confluent lesion – Vitritis, vasculitis, papillitis and serous
detachment may be present
› Retinitis / Chorioretinitis:– “Ground glass” retinitis with vasculitis– Patchy earlier on then progressed to
confluent– Choroidal involvement typically
multifocal, punctate lesions – Responds well to penicillin treatment
unlike ARN or PORN
http://imagebank.asrs.org/Content/imagebank/Sifilis-Caso01Color01.jpg/image-full;max$643,0.ImageHandlerhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC2694006/
https://link.springer.com/chapter/10.1007/978-3-319-23416-8_4#citeass
› 1st Dx: Granulomatous anterior uveitis– R/O RA:
› Lack of scleritis– R/O uncontrolled HIV:
› Anterior uveitis rare› If present, non-granulomatous
› 2nd Dx: Panuveitis– Consider HIV again?
› Vitreous and retina involvement now– R/O ARN:
› Typically in immunocompetent patient– R/O PORN:
› Tends to occur when CD4+ falls below 50› Presence of significant anterior/vitreous
inflammation not consistent with PORN› Choroid affected› Retinal vasculitis present
http://www.retinalphysician.com/archive/2013/October/images/OMD_Oct_A09_Fig01.jpg
› 3rd Dx: Syphilitic Chorioretinitis– Areas of retinal whitening
indicating necrosis– “Ground glass”
appearance with small area of multifocal punctate lesion
– GRANULOMATOUS anterior inflammation
– Posterior inflammation
CC: Pain and redness
2/13/2019
22
› CC: Pain and redness
› HPI: – OD– Started 1 week prior– Upon awakening– Saw an optometrist and was told he had a viral infection.
He was sick 2 weeks before symptoms began.
› POH: unremarkable
› PMH: unremarkable
› Medication: none
› ALL: NKDA
› Intraocular Pressures – OD 29 mmHg– OS 22 mmHg– Time 1:10 pm
› VA (sc)– OD 20/20– OS 20/20
› EOMs– Unrestricted OD, OS
› CF– FTFC OD, OS
› PERRL (-) APD
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal
4+ Diffuse InjectionMild chemosis
FolliclesCONJUNCTIVA Follicles
clear CORNEA clear
3+ cells / 1+ flare A/C (-) C/F
flat, brown, (-) nodules IRIS flat, brown, (-) nodules
clear LENS clear
clear, (-) cells VITREOUS clear, (-) cells
OD OS
0.25/0.25 CD 0.25/0.25
Distinct 360 DISC Distinct 360
Pink and healthy RIM Pink and healthy
Flat, even pigmentation MACULA Flat, even pigmentation
2/3 VESSELS 2/3
(-)holes/tears/RDs PERIPHERY superior nasal retinal scarring
› Viral Conjunctivitis:– Symptoms x 1 week OD– Hx of URI– Diffuse injection– (+) Follicles
› Uveitis:– Symptoms– Diffuse injection– Presence of cells & flare
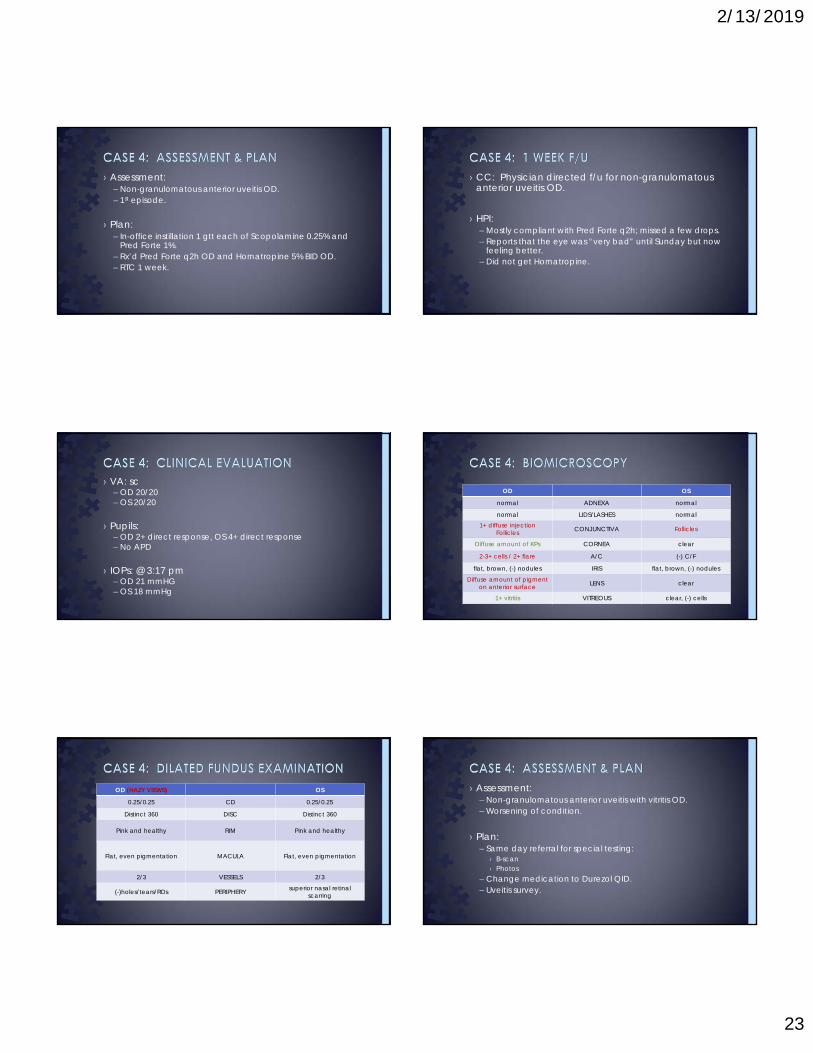
2/13/2019
23
› Assessment:– Non-granulomatous anterior uveitis OD. – 1st episode.
› Plan:– In-office instillation 1 gtt each of Scopolamine 0.25% and
Pred Forte 1%. – Rx’d Pred Forte q2h OD and Homatropine 5% BID OD. – RTC 1 week.
› CC: Physician directed f/u for non-granulomatous anterior uveitis OD.
› HPI:– Mostly compliant with Pred Forte q2h; missed a few drops.– Reports that the eye was “very bad” until Sunday but now
feeling better. – Did not get Homatropine.
› VA: sc– OD 20/20– OS 20/20
› Pupils:– OD 2+ direct response, OS 4+ direct response– No APD
› IOPs: @ 3:17 pm– OD 21 mmHG– OS 18 mmHg
OD OS
normal ADNEXA normal
normal LIDS/LASHES normal1+ diffuse injection
Follicles CONJUNCTIVA Follicles
Diffuse amount of KPs CORNEA clear
2-3+ cells / 2+ flare A/C (-) C/F
flat, brown, (-) nodules IRIS flat, brown, (-) nodules
Diffuse amount of pigment on anterior surface LENS clear
1+ vitritis VITREOUS clear, (-) cells
OD (HAZY VIEWS) OS
0.25/0.25 CD 0.25/0.25
Distinct 360 DISC Distinct 360
Pink and healthy RIM Pink and healthy
Flat, even pigmentation MACULA Flat, even pigmentation
2/3 VESSELS 2/3
(-)holes/tears/RDs PERIPHERY superior nasal retinal scarring
› Assessment:– Non-granulomatous anterior uveitis with vitritis OD. – Worsening of condition.
› Plan:– Same day referral for special testing:
› B-scan› Photos
– Change medication to Durezol QID.– Uveitis survey.
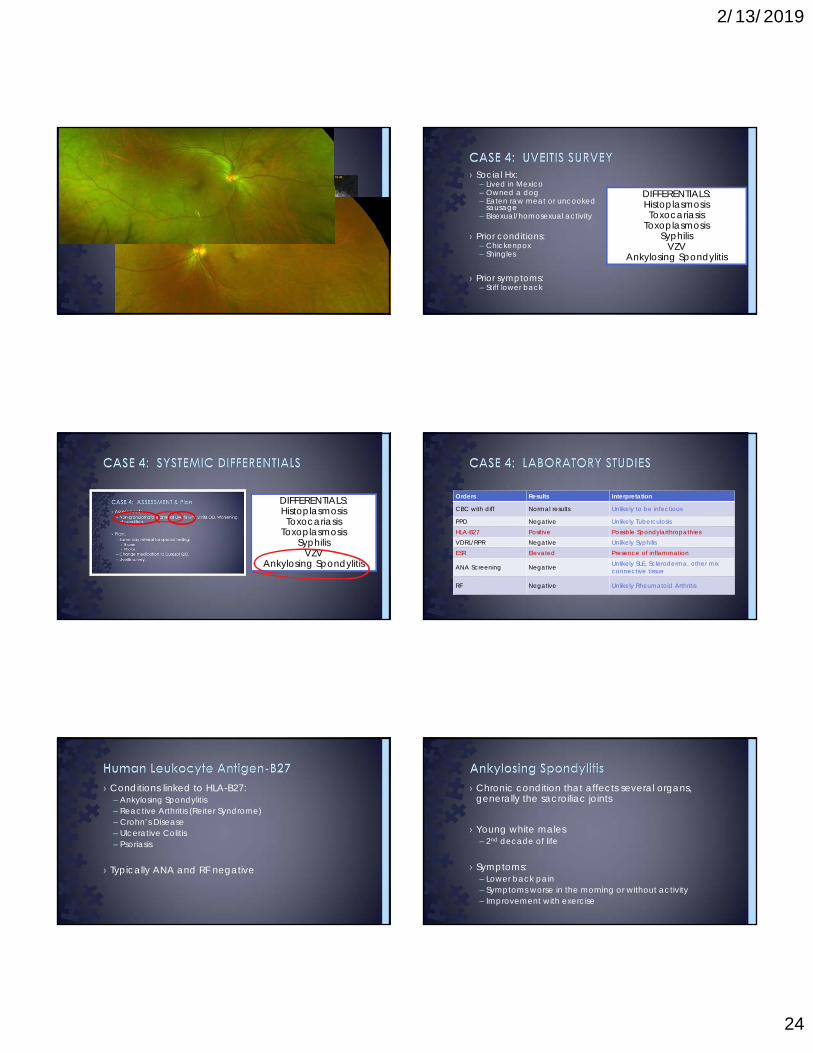
2/13/2019
24
› B-Scan:– Unremarkable
› Photos:– Unremarkable
› Social Hx:– Lived in Mexico– Owned a dog– Eaten raw meat or uncooked
sausage– Bisexual/homosexual activity
› Prior conditions:– Chickenpox– Shingles
› Prior symptoms:– Stiff lower back
DIFFERENTIALS:HistoplasmosisToxocariasis
ToxoplasmosisSyphilis
VZVAnkylosing Spondylitis
DIFFERENTIALS:HistoplasmosisToxocariasis
ToxoplasmosisSyphilis
VZVAnkylosing Spondylitis
Orders Results Interpretation
CBC with diff Normal results Unlikely to be infectious
PPD Negative Unlikely TuberculosisHLA-B27 Positive Possible SpondylarthropathiesVDRL/RPR Negative Unlikely SyphilisESR Elevated Presence of inflammation
ANA Screening Negative Unlikely SLE, Scleroderma, other mix connective tissue
RF Negative Unlikely Rheumatoid Arthritis
› Conditions linked to HLA-B27:– Ankylosing Spondylitis– Reactive Arthritis (Reiter Syndrome)– Crohn’s Disease– Ulcerative Colitis– Psoriasis
› Typically ANA and RF negative
› Chronic condition that affects several organs, generally the sacroiliac joints
› Young white males– 2nd decade of life
› Symptoms:– Lower back pain– Symptoms worse in the morning or without activity– Improvement with exercise
2/13/2019
25
› Greater anterior segment involvement vs. posterior segment
› Presents most commonly as uveitis:– Anterior, non-granulomatous– Greater tendency to have more inflammation with ocular
surgeries– Greater severity relative to idiopathic uveitis
› Treatment:– More resistant to traditional therapies– Require more aggressive steroids – Consult with PCP for medical management
› Understanding the key elements to make a diagnosis of uveitis– CC & History– Clinical signs
› Hallmark› Other subtle signs
› Utilize additional tests to aid in the systemic cause of uveitis– Survey– Laboratory testing
› Create the systemic differentials– Utilize the history and clinical signs– Pull from the uveitis survey– Use laboratory testing (and repeat testing) to confirm your
suspicion.
› Be flexible!– The course of the condition may change.– Your differentials may change.
1. Generali E, Cantarini L, Selmi C. Ocular involvement in systemic autoimmune diseases. Clinic Rev Allerg Immunol (2015)49:263-270.
2. Emmett T. Cunningham Jr MD, PhD, MPH, Robert W. Wong MD, Ako Takakura MD, Kenneth M. Downes MD & Manfred Zierhut MD (2014) Necrotizing Herpetic Retinitis, Ocular Immunology and Inflammation, 22:3, 167-169.
3. Wensing B, de Groot-Mijnes, JDF, Rothova A. Necrotizing and nonnecrotizing variants of herpetic uveitis with posterior segment involvement. Arch Ophthalmol (2011)129:403-409.
4. Robinson MR, Ross ML, Whitcup SM. Ocular manifestations of HIV infection. Curr Opin Ophthalmol 1999,10:431-437.
5. Liu D, Birnbaum AD. Update on sarcoidosis. Curr Opin Ophthalmol 2015,26:512-516.
6. Alejandra de-la-Torre MD, PhD, Juanita Valdes-Camacho MD & C. Stephen Foster MD (2016): Bilateral Herpes Simplex Uveitis: Review of the Literature and Own Reports , Ocular Immunology and Inflammation.
7. Mambretti J. Chest x-ray stages of sarcoidosis. J Insur Med 2004;36:91-92.
8. Pasadhika S, Rosenbaum JT. Ocular sarcoidosis. Clin Chest Med 2015 December;36(4):669-683.
9. Agrawal R, Gonzales-Lopez JJ, Meier F et al. Ocular and systemic features of sarcoidosis and correlation with the international workshop for ocular sarcoidosis diagnostic crtieria. Sarcoidosis Vasc Diffuse Lung Dis 2015;32:237-245.
10. Sakata VM, Theodoro da Silva F, Hirata CE. Diagnosis and classification of Vogt-Koyanagi-Harada disease. Autoimmunity Reviews 2014;13:550-555.
11. Du L, Kijlstra A, Yang P. Vogt-Koyanagi-Harada disease: Novel insights into pathophysiology, diagnosis and treatment. Progress in Retinal and Eye Research 2016;52:84-111.
12. Murray PI, Rauz S. The eye and inflammatory rheumatic diseases: The eye and rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis. Best Practice & Research Clinical Rheumatology 30 (2016): 802-825.
13. Hughes EH, Guzowsky M, Simunovic MP et al. Syphilitic retinitis and uveitis in HIV-positive adults. Clinical and Experimental Ophthalmology 2010; 38: 851-856.
14. Ittner EA, Bhakhri R, Newman T. Necrotizing herpetic retinopathies: a review and progressive outer retinal necrosis case report. Clin ExpOptom 2016; 99:24-29.
15. Nussenblat RB, Lane HC. Human immunodeficiency virus disease: changing patterns of intraocular inflammation. Am J Ophthalmol. 1998 Mar;125(3):374-82.
16. Whitcup SM1, Fortin E, Lindblad AS et al. Discontinuation of anticytomegalovirus therapy in patients with HIV infection and cytomegalovirus retinitis. JAMA. 1999 Nov 3;282(17):1633-7.
17. Bansal R, Gupta V, Gupta A. Current approach in the diagnosis and management of panuveitis. Indian J. Ophthalmol. 2010 Jan-Feb; 58(1):45-54.
18. Verma S, Hughes JD, Mabey D et al. Symptomatic anterior uveitis in HIV-positive patients. International Journal of STD & AIDS. 1999;10:2680274.
19. Amaratunge BC, Camuglia JE, Hall AJ. Syphilitic uveitis: A review of clinical manifestations and treatment outcomes of syphilitic uveitis in human immunodeficiency virus-positive and negative patients. Clinical and Experimental Ophthalmology 2010; 38: 68-74.
20. Androudi S, Dastiridou A, Symeonidis C et al. Retinal vasculitis in rheumatic disease: an unseen burden. Clin Rheumatol (2013)32:7-13.
21. Chen J, Lee L. Posterior placoid chorioretinitis: an unusual ocular manifestations of syphilis. Clinical Opthalmology 2008:2(3)669-673.
22. Liping D, Aize K, c, Peizeng Y. Vogt-Koyanagi-Harada disease: Novel insights into pathophysiology, diagnosis and treatment. Progress in Retinal and Eye Research 52 (2016) 84-111.
23. Haug S.J., Cunningham E.T. (2017) Syphilitic Uveitis. In: Chee SP., Khairallah M. (eds) Emerging Infectious Uveitis. Springer, Cham

2/1/2019
1
Resident Grand Rounds from Community Clinics
Dominic D’Orazio, OD Noor Abushagur, OD
Ocular Disease Residents of DFW
BENIGN OR MALIGNANT? THAT IS THE QUESTIONDominic D’Orazio ODOcular Disease Resident at Cedar Springs Eye Clinic, Dallas, TX
Case:
46 y/o African American female
Hx of DMII
Presents for annual comprehensive and evaluation for possible ocular complications from DMII
Pertinent Findings
VA(sc): 20/20 OD and OS
Confrontation fields: FTFC
Pupils: PERRLA (-) APD
Elevated melanocytic nevus on right central brow (reported as longstanding)
Pertinent Findings: Posterior
Gray/black growth on superior optic nerve OS
Approximately 1 disc diameter in size
No other significant posterior findings
Diagnosed as an ONH Melanocytoma
Photodocumentation as baseline
Scheduled for 6 month follow up
Pertinent Findings: Posterior
October 2011
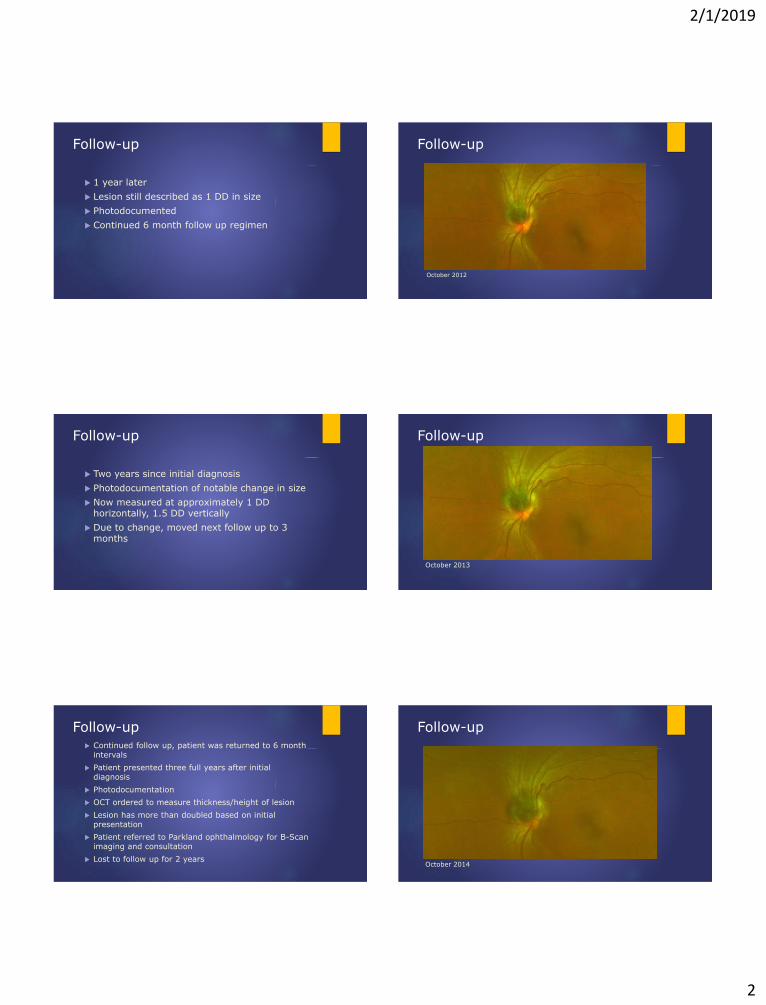
2/1/2019
2
Follow-up
1 year later
Lesion still described as 1 DD in size
Photodocumented
Continued 6 month follow up regimen
Follow-up
October 2012
Follow-up
Two years since initial diagnosis
Photodocumentation of notable change in size
Now measured at approximately 1 DD horizontally, 1.5 DD vertically
Due to change, moved next follow up to 3 months
Follow-up
October 2013
Follow-up Continued follow up, patient was returned to 6 month
intervals
Patient presented three full years after initial diagnosis
Photodocumentation
OCT ordered to measure thickness/height of lesion
Lesion has more than doubled based on initial presentation
Patient referred to Parkland ophthalmology for B-Scan imaging and consultation
Lost to follow up for 2 years
Follow-up
October 2014
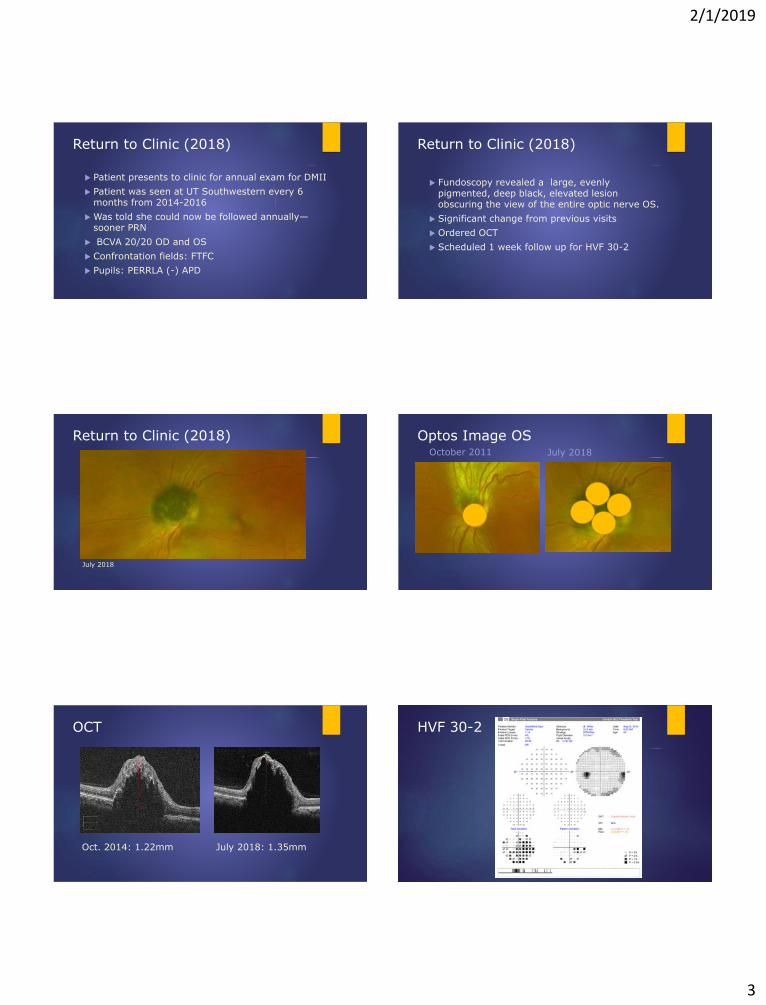
2/1/2019
3
Return to Clinic (2018)
Patient presents to clinic for annual exam for DMII
Patient was seen at UT Southwestern every 6 months from 2014-2016
Was told she could now be followed annually—sooner PRN
BCVA 20/20 OD and OS
Confrontation fields: FTFC
Pupils: PERRLA (-) APD
Return to Clinic (2018)
Fundoscopy revealed a large, evenly pigmented, deep black, elevated lesion obscuring the view of the entire optic nerve OS.
Significant change from previous visits
Ordered OCT
Scheduled 1 week follow up for HVF 30-2
Return to Clinic (2018)
July 2018
Optos Image OSOctober 2011 July 2018
OCT
Oct. 2014: 1.22mm July 2018: 1.35mm
HVF 30-2
2/1/2019
4
OCT Angiography
An alternative to IV indocyanine green angiography and fluorescein angiography
“Uses laser light reflectance of the surface of moving red blood cells to accurately depict vessels through different segmented areas of the eye”
May eliminate the need in certain cases for these intravascular dyes
OCT Disc Angiography: July 2018
Is this dangerous? What is an Optic Nerve Melanocytoma?
Optic Nerve Melanocytoma
“Melanocytoma” coined in 1965 lecture by Dr. Zimmerman
Determined lesion was benign
Challenged by Cogan
proposed “magnocellular nevus of optic nerve”
According to Shields, “hyperpigmented magnocellular nevus of the optic nerve (HMOD)” is more accurate
Optic Nerve Melanocytoma
Now defined as a variant of the melanocytic nevus
Dark brown/deep black color
Mean age of diagnosis – 52
No racial predilection (different from choroidal melanoma)
Slightly more common in females (62% of 115 cases from Wills Eye Hospital series)
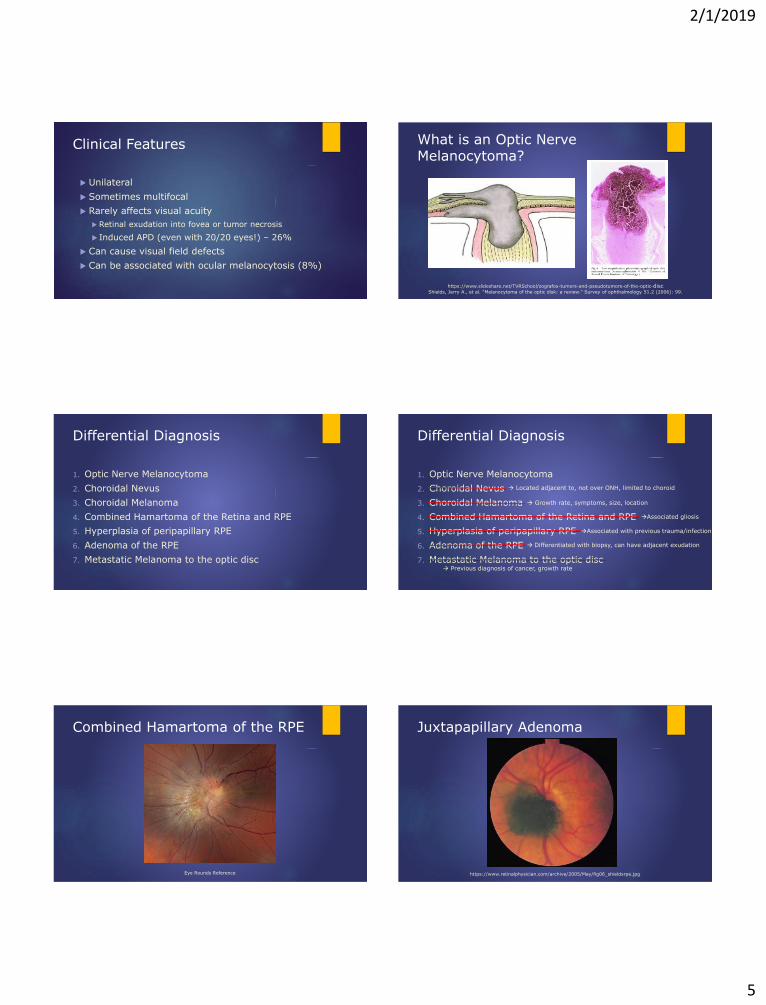
2/1/2019
5
Clinical Features
Unilateral
Sometimes multifocal
Rarely affects visual acuity
Retinal exudation into fovea or tumor necrosis
Induced APD (even with 20/20 eyes!) – 26%
Can cause visual field defects
Can be associated with ocular melanocytosis (8%)
What is an Optic Nerve Melanocytoma?
Shields, Jerry A., et al. "Melanocytoma of the optic disk: a review." Survey of ophthalmology 51.2 (2006): 99.
https://www.slideshare.net/TVRSchool/zografos-tumors-and-pseudotumors-of-the-optic-disc
Differential Diagnosis
1. Optic Nerve Melanocytoma
2. Choroidal Nevus
3. Choroidal Melanoma
4. Combined Hamartoma of the Retina and RPE
5. Hyperplasia of peripapillary RPE
6. Adenoma of the RPE
7. Metastatic Melanoma to the optic disc
Differential Diagnosis
1. Optic Nerve Melanocytoma
2. Choroidal Nevus
3. Choroidal Melanoma
4. Combined Hamartoma of the Retina and RPE
5. Hyperplasia of peripapillary RPE
6. Adenoma of the RPE
7. Metastatic Melanoma to the optic disc
Associated gliosis
Associated with previous trauma/infection
Differentiated with biopsy, can have adjacent exudation
Located adjacent to, not over ONH, limited to choroid
Growth rate, symptoms, size, location
Previous diagnosis of cancer, growth rate
Combined Hamartoma of the RPE
Eye Rounds Reference
Juxtapapillary Adenoma
https://www.retinalphysician.com/archive/2005/May/fig06_shieldsrpe.jpg
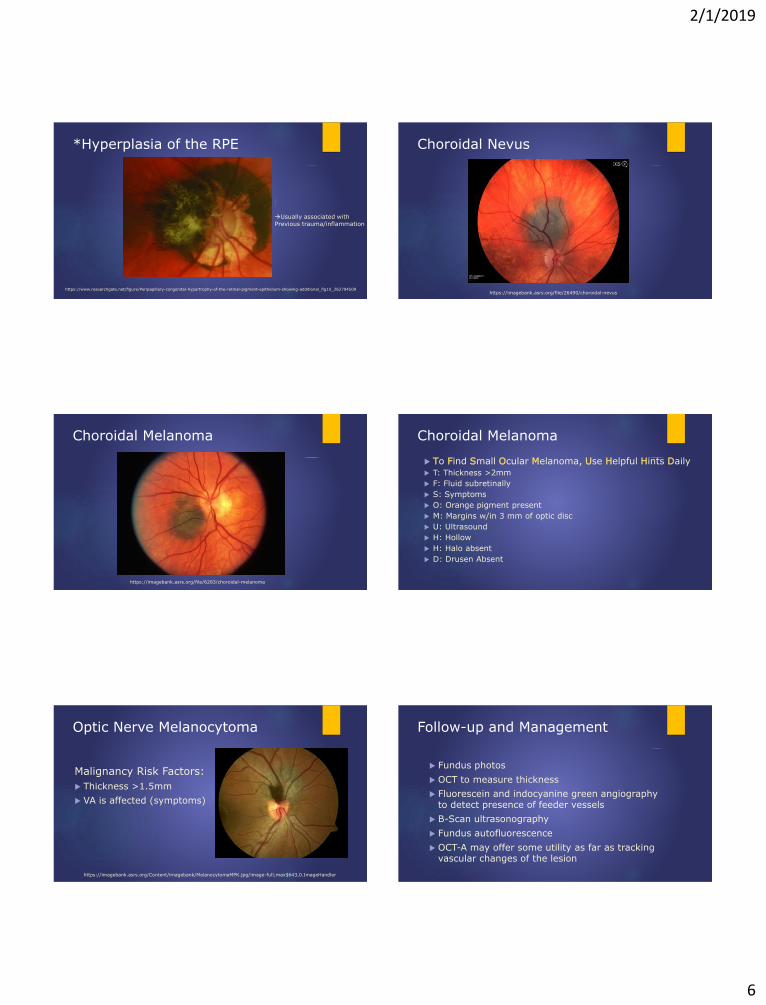
2/1/2019
6
*Hyperplasia of the RPE
Usually associated with
Previous trauma/inflammation
https://www.researchgate.net/figure/Peripapillary-congenital-hypertrophy-of-the-retinal-pigment-epithelium-showing-additional_fig10_262794509
Choroidal Nevus
https://imagebank.asrs.org/file/26490/choroidal-nevus
Choroidal Melanoma
https://imagebank.asrs.org/file/6283/choroidal-melanoma
Choroidal Melanoma
To Find Small Ocular Melanoma, Use Helpful Hints Daily T: Thickness >2mm
F: Fluid subretinally
S: Symptoms
O: Orange pigment present
M: Margins w/in 3 mm of optic disc
U: Ultrasound
H: Hollow
H: Halo absent
D: Drusen Absent
Optic Nerve Melanocytoma
Malignancy Risk Factors:
Thickness >1.5mm
VA is affected (symptoms)
https://imagebank.asrs.org/Content/imagebank/MelanocytomaMPK.jpg/image-full;max$643,0.ImageHandler
Follow-up and Management
Fundus photos
OCT to measure thickness
Fluorescein and indocyanine green angiography to detect presence of feeder vessels
B-Scan ultrasonography
Fundus autofluorescence
OCT-A may offer some utility as far as tracking vascular changes of the lesion
2/1/2019
7
Follow-up and Management
Risk for malignant transformation – 1-2% (Shields) VA affected?
Thickness?
Risk for malignant transformation of choroidal melanoma – below 1% (Singh et al.) Yet we often scrutinize these…
Gene Expression Profiling (GEP) BAP1 gene
SF3B1 and EIF1AX genes
Follow-up and Management
Change has been documented as late as 33 years after initial diagnosis (Shukla et al.)
Monitor every 12 months (sooner PRN)
Fundus photos
OCT
VA
Consider referral again if considerable change
References
1.) Shields, Jerry A., et al. “Melanocytoma of the Optic Disk: A Review.” Survey of Ophthalmology, vol. 51, no. 2, Mar. 2006, pp. 93–104.
2.) Reidy, James J., et al. “Melanocytoma: Nomenclature, Pathogenesis, Natural History and Treatment.” Survey of Ophthalmology, vol. 29, no. 5, 1985, pp. 319–327.
3.) Friedman, Neil J., et al. The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology. (475-476, 503) Elsevier, 2009.
4.)Singh, Arun D., et al. “Estimating the Risk of Malignant Transformation of a Choroidal Nevus.” Ophthalmology, vol. 112, no. 10, 24 June 2005, pp. 1784–1789.
5.) “Clinical Ophthalmology: a Systematic Approach.” Clinical Ophthalmology: a Systematic Approach, by Jack J. Kanski and Brad Bowling, Elsevier, 2012, pp. 496–506.
6.) Shields, Carol L., et al. “Clinical Factors in the Identification of Small Choroidal Melanoma.” Canadian Journal of Ophthalmology / Journal Canadien D'Ophtalmologie, vol. 39, no. 4, 2004, pp. 351–357.
7.)Shields, Carol L., et al. “Melanoma of the Eye: Revealing Hidden Secrets, One at a Time.” Clinics in Dermatology, vol. 33, no. 2, 2015, pp. 183–196.
8.) Shields, Jerry A.., et al. “Total Blindness From Presumed Optic Nerve Melanocytoma.” American Journal of Ophthalmology, vol. 139, no. 6, 19 Nov. 2004, pp. 1113–1114.
9.) Shukla, Shripaad Y., et al. “Transformation of Optic Disc Melanocytoma Into Melanoma Over 33 Years.” Archives of Ophthalmology, vol. 130, no. 10, 1 Oct. 2012, pp. 1344–1347.
10.) Meyer, David, et al. “Malignant Transformation of an Optic Disk Melanocytoma.” American Journal of Ophthalmology, vol. 127, no. 6, 5 Feb. 1999, pp. 710–714.
11.) Apinyawasisuk, Supanut, et al. “Clinical and Spectral-Domain Optical Coherence Tomography Appearance of Optic Disc Melanocytoma: A New Classification and Differentiation from Pigmented Choroidal Lesions.” Ocular Oncology and Pathology, vol. 3, no. 2, 2016, pp. 142–148.
Questions?
It’s Not Rare if it’s in Your Chair - Plaquenil
Noor Abushagur, OD
Ocular Disease Resident at Community Eye Clinic Fort Worth
A little about me…

2/1/2019
8
Case #1
59 year old Hispanic female
CC: diabetic exam
Medical Hx: DM, RA, HTN
Medications: unknown arthritis med unknown HTN medication, unknown DM medication
History of Chloroquine use 250mg/day from 2008-2013
BCVA: 20/25 OD/OS
Lens: Moderate combined cataract OU
Macula: bulls eye appearance OU
CASE #1 – Photos
CASE #1 – Macula OCT9/11/2018 Community Eye Center
OSODMacula Thickness OU: Macular Cube 512x128
Signal Strength:
Exam Time:
Exam Date:
Technician:
Gender:
DOB:
ID:
Name:
6/10
12:13 PM
9/11/2018
czmadmin,
Female
2/8/1959
20516
Corrales, Lucia
12:15 PM
7/10
OD OS
Serial Number: 5000-2740 5000-2740
OS ILM-RPE ThicknessOD ILM-RPE Thickness
Fovea: 264, 59 Fovea: 256, 62
OD OCT Fundus
OS ILM-RPE Thickness MapOD ILM-RPE Thickness Map
OD Horizontal B-Scan OS Horizontal B-Scan
OS OCT Fundus
BScan: 59 62BScan:
Doctor's Signature ExamRoom3SW Ver: 7.0.1.290Copyright 2013Carl Zeiss Meditec, IncAll Rights Reserved
Page 1 of 1
Comments
CASE #1 – Visual Field
Case #1 – Assessment & Plan
1. Type II DM without complications, OU
2. Chloroquine Toxicity, OU
3. Combined cataract, OU
4. Hyperopia, presbyopia, OU
Case #2
63 year old African female
CC: reports blurred vision at distance and near (referred from CAN for cataract eval)
Medical Hx: HTN, arthritis, malaria
Medications: amlodipine, iron supplement, Tylenol
Hx of Chloroquine use for malaria x many years
BCVA:
OD: 20/60++
OS: 20/250
Lens: severe combined cataract OS>>OD
Macula: bulls eye appearance
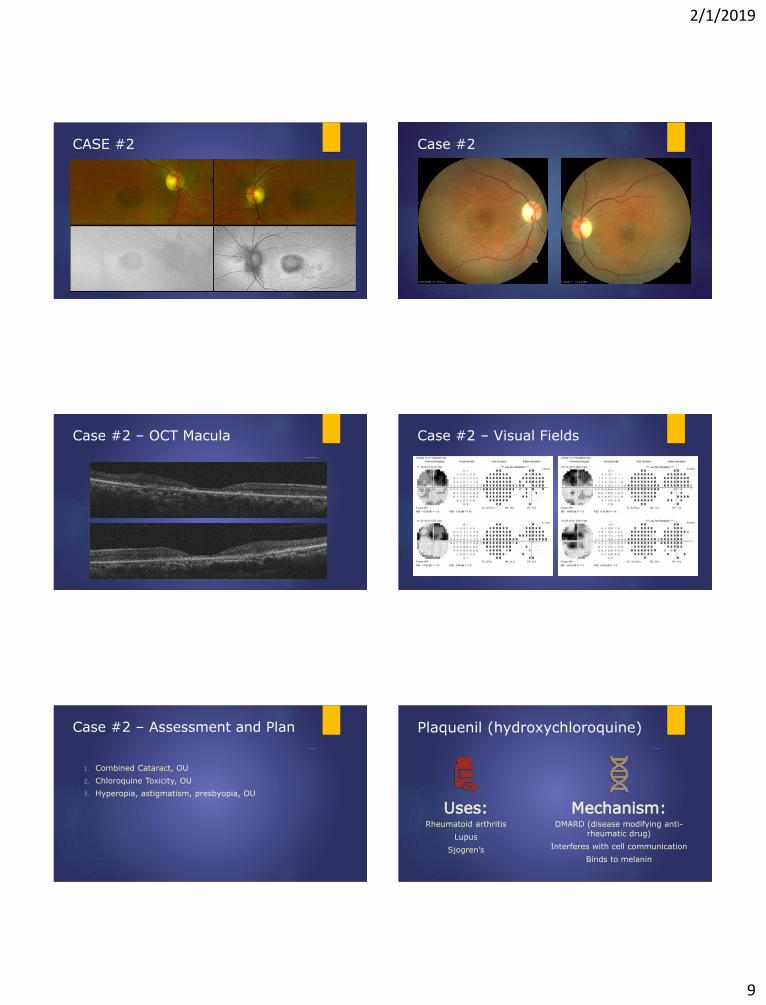
2/1/2019
9
CASE #2 Case #2
Case #2 – OCT Macula Case #2 – Visual Fields
Case #2 – Assessment and Plan
1. Combined Cataract, OU
2. Chloroquine Toxicity, OU
3. Hyperopia, astigmatism, presbyopia, OU
Plaquenil (hydroxychloroquine)
Uses:Rheumatoid arthritis
Lupus
Sjogren’s
Mechanism: DMARD (disease modifying anti-
rheumatic drug)
Interferes with cell communication
Binds to melanin

2/1/2019
10
Advantages
Cost
Minimal side effects: nausea and diarrhea
Visual changes are seen rarely
Effects on cholesterol
Hydroxychloroquine (HCQ) may lower LDL levels!!
May also reduce total cholesterol levels
Prescribing Guidelines
Old daily dosage (based on ideal weight)
New recommendation – Use real weight
Very thin patients in particular are at increased risk when dose is calculated by ideal weight (as previously recommended)1
Toxicity based on cumulative dose is no longer a thing!
Toxicity Mechanism is not well understood
Binding to melanin in the RPE may serve to concentrate the agents and contribute to, or prolong their toxic effects1
The primary damage is to the photoreceptors, and as the ONL degenerates, there is secondary disruption of the RPE.1
The macular localization of the disease suggests that light absorption or possibly cone metabolism may play a role, but that is speculation.1
Toxicity Signs
VA usually not affected
CME may develop
Retinopathy can progress after drug is discontinued
Chloroquine (and sometimes HCQ) can cause corneal verticillata
Reversible
No association with retinopathy
Toxicity Stats
Overall statistical risk for retinal toxicity is 7.5%
This varies greatly, depending on daily dose / duration of use
In patients taking <5mg/kg/day HCQ:
Less than 1% risk in first 5 years
Less than 2% risk in first 10 years
20% chance after 20 years!
Who’s At Risk1. Daily dose and duration of use
Dosage >5mg/kg
2. Renal diseaseCQ and HCQ are cleared through kidneys
3. Concurrent Tamoxifen use5x increased risk
4. Retinal and macular disease Adding a retinal toxin to an already diseased retina
Interferes with accuracy of testing for maculopathy
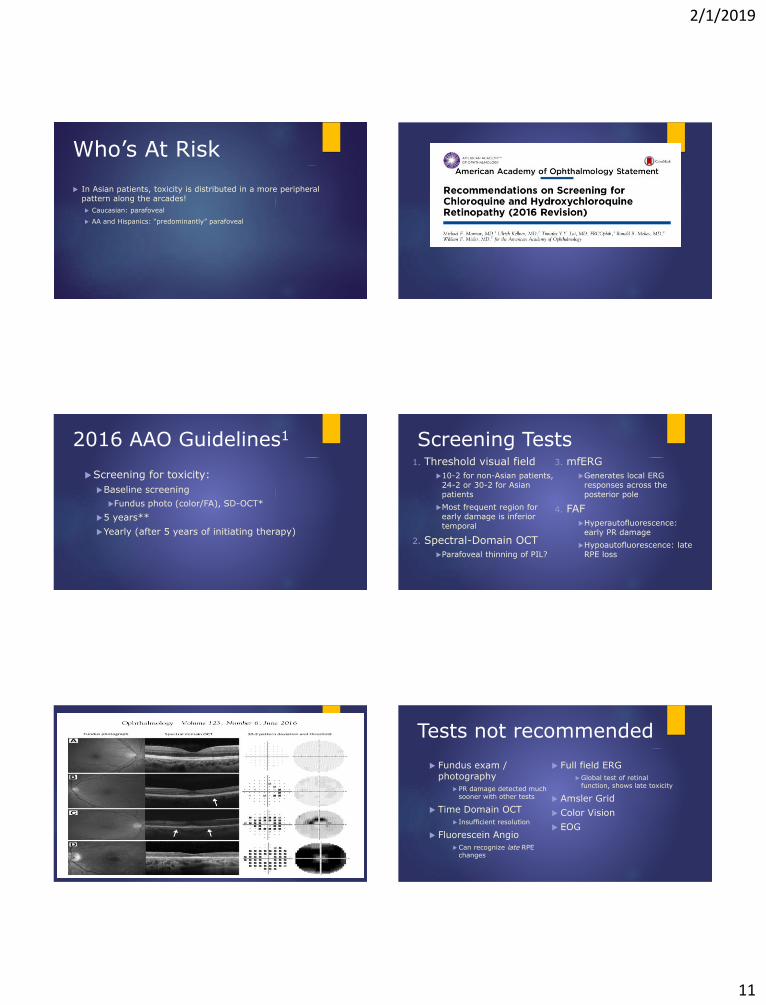
2/1/2019
11
Who’s At Risk
In Asian patients, toxicity is distributed in a more peripheral pattern along the arcades!
Caucasian: parafoveal
AA and Hispanics: “predominantly” parafoveal
2016 AAO Guidelines1
Screening for toxicity:
Baseline screening
Fundus photo (color/FA), SD-OCT*
5 years**
Yearly (after 5 years of initiating therapy)
Screening Tests 1. Threshold visual field
10-2 for non-Asian patients, 24-2 or 30-2 for Asian patients
Most frequent region for early damage is inferior temporal
2. Spectral-Domain OCT
Parafoveal thinning of PIL?
3. mfERG
Generates local ERG responses across the posterior pole
4. FAF
Hyperautofluorescence: early PR damage
Hypoautofluorescence: late RPE loss
Tests not recommended
Fundus exam / photography
PR damage detected much sooner with other tests
Time Domain OCT
Insufficient resolution
Fluorescein Angio
Can recognize late RPE changes
Full field ERG
Global test of retinal function, shows late toxicity
Amsler Grid
Color Vision
EOG
2/1/2019
12
References
1. Marmor, M. F. (2016). Recommendations on Screening for Chloroquine and Hydroxychloroquine Retinopathy - 2016. Retrieved from https://www.aao.org/clinical-statement/revised-recommendations-on-screening-chloroquine-h.Academy ppt
2. Harrison, W. (n.d.). Update on Plaquenil Testing: 2016 Guidelines and Beyond. Lecture.
3. Bowling, B. (2016). Kanski’s Clinical Ophthalmology: A systematic approach. Saunders. Questions?