Embed Size (px)
Citation preview

CDKN2A/B T2D GWAS risk-SNPs impact locus gene expression and proliferation in
human islets
Yahui Kong1, Rohit B. Sharma
1, Socheata Ly
1, Rachel E. Stamateris
1, William M. Jesdale
2
and Laura C. Alonso1
Diabetes Center of Excellence in the Department of Medicine1, and the Department of
Quantitative Health Sciences2, University of Massachusetts Medical School, Worcester MA
Running title
CDKN2A/B T2D SNPs impact human islet biology
Corresponding author
Laura C. Alonso
774-455-3640 (phone)
508-856-3803 (fax)
AS7-2047, Division of Diabetes
368 Plantation Street, Worcester, MA 01605
Keywords
Aging, ANRIL, beta cell mass, Cdkn2A, Cdkn2B, CDKN2B-AS, insulin secretion, oncogene,
p14, p15, p16, p14ARF
, p15INK4B
, p16INK4A
, pancreatic beta cell, proliferation
Abbreviations
ACTB, beta-actin gene
ANRIL, antisense noncoding RNA in the INK4 locus
ARF, alternate reading frame
CCND2, cyclin D2
CDK, cyclin dependent kinase
CDKN2A, cyclin dependent kinase inhibitor 2, encodes p14ARF
and p16INK4A
CDKN2B, cyclin dependent kinase inhibitor 2, encodes p15INK4B
CDKN2B-AS, cyclin dependent kinase inhibitor 2B antisense
eQTL, expression quantitative trait loci
GAPDH, Glyceraldehyde-3-Phosphate Dehydrogenase
GWAS, genome wide association studies
lncRNA, long non-coding RNA
MTAP, 5-methylthioadenosine phosphorylase
PCNA, proliferating cell nuclear antigen
SNP, single nucleotide polymorphism
Page 1 of 51 Diabetes
Diabetes Publish Ahead of Print, published online February 6, 2018

ABSTRACT
Genome-wide association studies link the CDKN2A/B locus with T2D risk, but mechanisms
increasing risk remain unknown. The CDKN2A/B locus encodes cell cycle inhibitors p14,
p15, and p16, MTAP, and ANRIL, a lncRNA. The goal of this study was to determine
whether CDKN2A/B T2D risk-SNPs impact locus gene expression, insulin secretion, or beta
cell proliferation, in human islets. Islets from non-diabetic donors (n=95) were tested for
SNP genotype (rs10811661, rs2383208, rs564398, rs10757283), gene expression (p14, p15,
p16, MTAP, ANRIL, PCNA, KI67, CCND2), insulin secretion (n=61) and beta cell
proliferation (n=47). Intriguingly, locus genes were co-regulated in islets in two physically
overlapping cassettes: p14-p16-ANRIL, which increased with age, and MTAP-p15, which did
not. Risk-alleles at rs10811661 and rs2383208 were differentially associated with expression
of ANRIL, but not p14, p15, p16 or MTAP, in age-dependent fashion, such that younger
homozygous-risk donors had higher ANRIL expression, equivalent to older donor levels. We
identified several risk-SNP haplotype combinations that may impact locus gene expression,
suggesting possible mechanisms by which SNPs impact locus biology. Risk-allele carriers at
ANRIL coding SNP rs564398 had reduced beta cell proliferation index. In conclusion,
CDKN2A/B locus SNPs may impact T2D risk by modulating islet gene expression and beta
cell proliferation.
Page 2 of 51Diabetes

T2D risk has a strong genetic component. Significant research investment has identified
>100 genomic regions that influence T2D risk in human populations (1–3). Most T2D risk-
SNPs are non-coding, and the mechanism by which they impact local genome biology
remains unclear for most loci (3). Risk alleles may act in multiple ways, interacting with
other genes and polymorphisms in tissue-specific manner. Genome-wide eQTL studies seek
to identify how polymorphisms impact biology at any given locus (1,4–7); however, depth of
information at individual loci is limited in genome-wide studies. Most T2D SNPs influence
risk by impacting islet biology (8), but the cost and inaccessibility of human islets, and poor
utility of non-human models to study the human genome, have slowed progress in clarifying
mechanisms.
SNPs at the CDKN2A/B genomic locus impact risk of T2D, and related diseases such as
gestational diabetes, cystic fibrosis related diabetes and post-transplant diabetes, across
ethnicities and cultures, suggesting a central diabetogenic mechanism (9). Multiple SNPs in
different linkage blocks at the CDKN2A/B locus confer T2D risk (9); mechanisms impacting
risk remain unknown. The CDKN2A/B locus encodes four genes (Figure 1): MTAP,
CDKN2A, CDKN2B and a long-noncoding RNA named ANRIL. CDKN2A and CDKN2B are
well studied, encoding cell cycle inhibitors (p14 and p16 are splice variants of CDKN2A, p15
is encoded at CDKN2B) that impact aging, senescence, and tumorigenesis via regulation of
Rb (retinoblastoma) and p53 (10,11). Three T2D SNPs at this locus, rs10811661, rs2383208
and rs10757283, are non-coding, located downstream of known genes; rs2383208 and
rs10811661 are in one linkage block and rs10757283 is in a separate linkage block
immediately downstream. A fourth SNP, rs564398, about 100,000 bp upstream of these,
falls within exon-2 of ANRIL. These SNPs were identified in large population studies seeking
to identify genomic regions associated with T2D risk (12–14); for more details please see
(9). The three downstream SNPs are mostly associated with T2D risk and not other diseases;
the rs564398 SNP is also associated with coronary heart disease and glaucoma (15). The
absolute magnitude of T2D risk is low with all identified SNPs (at this and other loci); for
example, reported odds ratio for the linkage region containing rs10811661 and rs2383208
ranges from 1.18-1.46 (4,12,14,16,17). Weaker odds ratios were seen for rs564398 1.12-1.26
e.g. (13); intriguingly, multiple studies show that rs564398 is associated with T2D risk in
Page 3 of 51 Diabetes

Caucasian but not Asian populations (18). A risk-risk haplotype of rs10811661/rs2383208
and rs10757283 conferred an odds ratio of 1.24, with stronger association than individual
risk alleles (13). Although each T2D SNP is in linkage disequilibrium with multiple other
SNPs, fine mapping has not identified linked SNPs with greater disease association than
these GWAS-identified SNPs (1,4). The causal SNP in any of these linkage blocks is not yet
known.
In human populations, rs10811661 risk allele is associated with reduced insulin secretory
capacity after oral or IV glucose challenge (16,19–22). Insulin secretory capacity is a
composite endpoint influenced by beta cell mass, insulin production, glucose sensing and
stimulus-secretion coupling (23), factors that cannot currently be effectively separated in
living human subjects. Intriguingly given the aging and senescence roles played by
CDKN2A/B genes, the impact of rs10811661 on T2D risk was influenced by subject age
(18). SNPs at this locus also influence insulin sensitivity and biology of other metabolic
tissues, demonstrating the complexity of even a single genomic locus on T2D biology (9).
Since human studies suggest that CDKN2A/B-locus SNPs impact T2D risk, at least in part,
by reducing insulin secretory capacity, we hypothesized that locus SNPs influence pancreatic
islet biology. Here we present a detailed analysis of CDKN2A/B biology in non-diabetic
human islets. We identified two overlapping co-regulated gene sets: p14-p16-ANRIL, and
p15-MTAP. p14-p16-ANRIL expression, but not p15-MTAP expression, increased with donor
age. Of the four T2D risk-SNPs tested, rs2383208 and rs10811661 risk alleles were
associated with inappropriate high expression of the ANRIL lncRNA in samples from
younger donors. No other SNP-gene interaction was identified, but our data suggest certain
SNP haplotypes that may impact locus gene expression in combinatorial fashion. Finally,
risk-alleles at rs564398 were associated with reduced beta cell proliferation index,
suggesting a functional implication for this SNP, and perhaps the ANRIL lncRNA, in accrual
or maintenance of human beta cell mass.
RESEARCH DESIGN AND METHODS
Human islets
Page 4 of 51Diabetes

Human islets were obtained from the NIH-NIDDK-supported Integrated Islet Distribution
Program at the City of Hope, or from a collaborative group headed at Vanderbilt (24).
Human islet studies were determined by the University of Massachusetts Institutional
Review Board to not qualify for IRB review or exemption because they do not involve the
use of human subjects. De-identified islet samples from 95 non-diabetic subjects were live-
shipped in Prodo islet transport media transport. Donors (Supplemental Table 1) included 42
females, 48 males and 5 without sex reported, age 40 +/- 16 years, ethnicity 1 Asian, 8 Black
or African American, 14 Hispanic/Latino, 66 White, and 6 unknown. Upon receipt, islets
were plated in islet culture medium (RPMI, 10% FBS, 5 mmol/L glucose,
penicillin/streptomycin) and incubated at 37 degrees, 5% CO2 overnight to recover from
isolation and shipment. Following recovery, 800 IEQ were hand-picked, washed in PBS
containing 100 nmol/L Na3VO4, and flash frozen at -80°C in 200 islet equivalent (IEQ)
aliquots for future DNA and RNA analysis. Additional islets from a subset of donors were
cultured as described below for glucose-stimulated proliferation.
Genotyping
DNA and RNA were extracted from flash-frozen 200 IEQ aliquots using the Norgen
RNA/DNA/Protein purification kit (Norgen Biotek Corp., Ontario, Canada) following the
manufacturer's protocol. Genotyping for four CDKN2A/B SNPs: rs564398 (C/T),
rs10811661 (C/T), rs2383208 (G/A) and rs10757283 (C/T) was performed in duplicate using
commercial (C_2618017_10, C_31288917_10, C_15789011_10, C_31288916_10)
TaqMan® SNP genotyping assays (Thermo Fisher Scientific, Waltham, MA, USA) on
Biorad (C1000 Touch Thermal cycler) or Eppendorf (Realplex cycler) real-time PCR
platforms, using 20ng of DNA in a 10µl reaction volume under conditions recommended by
the manufacturer. SNP determination was confirmed by both allelic discrimination and by
manual CT value assessment for all samples and all SNPs. Minor allele frequencies (MAF)
in our cohort were in agreement with expected MAF based on the 1000 genomes project (25)
(Supplemental Table 2), and the observed haplotype frequency of SNP combinations
predicted similar linkage disequilibrium to 1000 genomes-reported values for these SNPs
(Supplemental Table 3)(26).
Page 5 of 51 Diabetes

Gene expression assays
Total RNA was reverse transcribed using SuperScript IV VILO Master Mix kit (Thermo
Fisher Scientific, Waltham, MA, USA). The expression levels of target genes in human islets
were quantitatively assessed in duplicate using Taqman® validated human gene expression
assays (Thermo Fisher Scientific). Primers/probes used were: ANRIL, Hs04259476_m1; p15,
Hs00793225_m1; p14, Hs99999189_m1; p16, Hs02902543_mH; MTAP, Hs00559618_m1;
KI67, Hs01032443_m1; PCNA, Hs00696862_m1; CCND2, Hs00153380_m1; ACTB,
Hs01060665_g1; GAPDH, Hs02758991_g1. ACTB and GAPDH were used as endogenous
reference to normalize gene expression. Reproducibility of duplicate measurements was
high, as assessed by the R2 of the correlation between duplicates and by the absolute value of
the Relative Percentage Difference between the duplicates (Supplemental Figure 1).
Transcript expression levels were presented as log2-transformed expression (∆CT).
Human islet culture experiments
Human islets cultured overnight in islet culture medium were dispersed to single cells using
single-use–apportioned 0.05% trypsin and plated on uncoated glass coverslips (Fisherbrand)
as described (27–29). Dispersed cells were cultured in islet culture medium containing either
5mM or 15mM glucose for 96 hours, with 20 µg/ml bromodeoxyuridine (BrdU) included for
the entire time. After culture, the islet cells were fixed for 10 min in 4% paraformaldehyde
(Sigma). Immunofluorescence staining was performed after unmasking in 1N HCl for 25
minutes at 37°C for insulin, (Abcam, ab7842 or Dako, A056401-2), BrdU (Abcam, ab6326)
and DAPI as described (27–29). β-Cell proliferation, defined as the percent of insulin-
staining cells that were also BrdU-labeled, was quantified on blinded images (30). Data were
expressed as the proliferation index, calculated as the ratio of %BrdU+ β-cells in 15mM
glucose divided by the %BrdU+ β-cells in 5mM glucose.
Statistics
Univariate analyses were performed using GraphPad Prism and expressed as mean ± SD. P
values were determined by two-tailed Student t test when comparing 2 conditions, with F test
to compare variances, one way ANOVA with Tukey post-test for correction for multiple
comparisons when comparing >2 conditions, or by linear regression when assessing the
Page 6 of 51Diabetes

relationship between two continuous variables. Multivariable linear models were performed
to examine gene expression (p14, p15, p16, ANRIL, MTAP) simultaneously adjusted for
donor sex, race/ethnicity, age (continuous) and body mass index (continuous); additional
models further adjusted for expression of the other gene products. Missing values were
modeled with a missing indicator, replacing unknown values with sample means for linear
variables. Infrequent or unknown race/ethnicity were grouped in a residual category. RNA
expression associated with SNPs was estimated in linear multivariable models adjusting for
demographics (as above), in two fashions: first, setting the population with no risk alleles as
the common reference group, and second by estimating the linear effect on a per-allele basis
(treating the number of risk alleles as additive). Insulin secretion index was estimated as a
function of demographic variables as described above, and by including each SNP as a
predictor of insulin secretion index. Interpretation of these models can be found in the
Supplemental Materials. P<0.05 was considered significant, although this may be too
generous for the exploratory analyses with multiple comparisons. For the haplotype
hypothesis-generating analyses, the false discovery rate (FDR), calculated by the original
method of Benjamini and Hochberg, was set at 10%, based on our estimation that a
hypothesis with 90% likelihood of being correct warranted experimental follow-up.
RESULTS
CDKN2A/B locus gene expression is coordinately regulated in human islets
To understand the context of how T2D risk-SNPs might impact biology at this locus in
human islets, we first quantified expression of all locus genes (Figure 1A). Validated
Taqman probes were chosen that could independently quantify transcripts including MTAP,
p14 (CDKN2A, ARF), p15 (CDKN2B, INK4B), p16 (CDKN2A, INK4A) and the ANRIL
(CDKN2B-AS1) lncRNA. p14 and p16 are splice variants of CDKN2A, sharing exons 2-3 but
with different first exons; exons 2-3 are in different reading frames and thus p14 and p16
encode entirely different proteins with different functions (31). The ANRIL probe spans
exons 5-6, thus detecting all known isoforms. In this cohort of islet samples from 95 unique
non-diabetic donors (Supplemental Table 1), RNA abundance of p14, p16 and ANRIL were
highly correlated with each other (Figure 1, normalized to ACTB, and Supplemental Figure 2,
Page 7 of 51 Diabetes

normalized to GAPDH). In contrast, abundance of p15, despite being physically located
within the first intron of ANRIL, was poorly (ACTB normalization) or not (GAPDH
normalization) correlated with p14, p16 or ANRIL. On the other hand, p15, but not p14, p16
or ANRIL, was highly correlated with MTAP expression. When the data were examined in
multivariable linear models, integrating donor characteristics such as age into the model,
again p14-ANRIL and p14-p16 were highly correlated, as were p15-MTAP (Supplemental
Table 4). These results suggest two independent but overlapping co-regulatory cassettes at
the CDKN2A/B locus in human islets, with p14-p16-ANRIL in one and p15-MTAP in the
other.
Age-dependent gene expression increase of p14, p16 and ANRIL but not p15 or MTAP
In many tissues, including islets, some CDKN2A/B locus genes increase with advancing age
(9,10,32). In this cohort of human islets, expression of p14, p16 and ANRIL showed a modest
positive correlation with donor age, whereas p15 and MTAP did not (Figure 2A-E). Donor
body mass index (BMI) could potentially confound the impact of age on gene expression;
however, BMI was similar across donor ages (Figure 2F). Furthermore, we observed no
correlation between donor BMI, sex or ethnicity and expression of any CDKN2A/B locus
gene in univariate analysis (Supplemental Figures 3-5). Multivariable linear models
integrating age, sex, race and BMI confirmed a positive correlation between p14, p16 and
ANRIL with donor age, and confirmed a lack of impact of sex, race or BMI on locus gene
expression (Supplemental Table 4). Scatter plots of gene expression versus age showed that
some genes were expressed in very low abundance in islets from juvenile (age < 10 years)
donors, with points falling well below the linear regression curve (Figure 2A, C, D). Focused
analysis of juvenile (<10 years) versus adolescent/adult (>10 years) islets (Figure 2G-K)
revealed that expression of p14, p16 and ANRIL were markedly lower in juvenile islets, but
MTAP and p15 were not, again suggesting altered regulatory characteristics of these two
genes relative to other locus genes. Interestingly, an F test showed that the variances were
reduced in juvenile islets (see standard deviation bars in Figure 2 G-K) for p14 (p<0.0001),
p16 (p<0.001) and ANRIL (p<0.0001) but not for p15 or MTAP (p=ns for both), despite the
much smaller sample size, again suggesting fundamentally different biology of the juvenile
samples. In sum, older age increased expression of p14, p16 and ANRIL, but not p15 or
Page 8 of 51Diabetes

MTAP, and the youth-associated suppression was exaggerated in islets from very young
donors.
T2D risk-SNPs at rs10811661 and rs2383208 increased ANRIL expression in an age-
defined subset of islet samples
We next tested whether T2D-related SNPs at CDKN2A/B impact locus gene expression.
Validated Taqman genotyping procedures ascertained and confirmed the genotype of all
n=95 preps for four T2D SNPs: rs564398 (hg38 chr9:22029548), rs2383208 (hg38
chr9:22132077), rs10811661 (hg38 chr9:22134095) and rs10757283 (hg38 chr9:22134173).
Measured minor allele frequencies (MAF; Supplemental Table 2) were similar to reported
MAFs for ethnicity-matched populations, supporting genotyping accuracy. SNPs rs2383208
and rs10811661 were tightly linked, with only 2 of 95 samples differing in our cohort,
consistent with the linkage disequilibrium reported in LDpair and HaploReg (26,33,34)
(Supplemental Tables 3 and 5). In raw analysis across the entire cohort, no SNP genotype
correlated with abundance of any locus transcript by univariate (Figure 3) or multivariable
(Supplemental Table 6) analysis. Since donor age impacted expression of p14, p16 and
ANRIL, we assessed whether age interfered with the assessment of SNP effect on gene
expression. Mean age was not significantly different between genotypes for any SNP (data
not shown). However, expressing transcript abundance as a function of age revealed that for
ANRIL, but not for p14 or p16, the age-dependent increase was genotype-dependent, evident
only in protective-allele-carrying samples at rs2383208 (Figure 4) and rs10811661
(Supplemental Figure 6). Homozygous-risk samples had high levels of ANRIL across all ages
>10 years (Figure 4B, flat slope of AA regression line even despite the influence of the
juvenile samples). Age-genotype interaction was not observed for any locus gene for
rs10757283 or rs564398 (not shown). When the samples were reanalyzed using a different
methodology, binning by quartiles, it was again evident that samples with protective-allele at
rs2383208 or rs10811661 showed an age-dependent increase in ANRIL, but homozygous-
risk samples did not. In contrast, for p16 the slope of the age-dependent-gene expression
regression lines (Figure 4A) and binning analysis (Figure 4C) were similar across genotypes.
To test whether ANRIL abundance was inappropriately increased by homozygous-risk at
rs2383208 or rs10811661 in samples from young donors, samples between the ages of 10 (to
Page 9 of 51 Diabetes

exclude juveniles, which were all suppressed independent of genotype) and 50 (defined by
the intersection of the linear regression curves in 4B), was stratified by genotype (Figure 4E-
F). ANRIL, but not p16, abundance was significantly increased in younger homozygous-risk
samples compared with protective-allele carriers. Taken together, T2D homozygous-risk
genotype at rs2383208 or rs10811661 prematurely increased ANRIL expression in islets of
younger donors to older-donor levels.
SNPs may interact with each other to combinatorially influence gene expression
This cohort was not powered to perform subgroup analyses to definitively detect gene
expression impact of SNP haplotype combinations. For example, a sample size analysis
using our ANRIL expression mean and standard deviation for rs2383208 genotypes reveals
that we would require n=54 per subgroup to achieve a power of 80% and type 1 error of 0.05.
Given the diminishing number of samples as we partition by haplotype, we do not approach
this sample size for sub-analyses. Instead, we analyzed our dataset using a false discovery
rate (FDR) approach to prioritize hypotheses to test in future studies such as ex vivo
promoter-enhancer experiments. We estimated that a risk tolerance of 90% likelihood that a
hypothesis was correct would support future experimental investment. We then stratified our
gene expression data by all SNP haplotype combinations and analyzed each comparison for
likelihood of difference, defined by a FDR of 10% (Figure 5 and Supplemental Figure 7). By
these criteria, we determined that genotype at rs564398 and rs10757283 may influence the
impact of rs2383208 and/or rs10811661 on gene expression. For rs564398: in homozygous-
protective rs564398, but not risk-allele-containing samples, protective alleles at rs2383208
and rs10811661 may decrease abundance of p16 compared with homozygous-risk carriers.
For rs10757283: in homozygous-risk rs10757283 samples, but not protective-allele samples,
protective-allele at rs2383208 or rs10811661 may decrease abundance of p15. These
observations suggest that individual SNPs may contribute risk by impacting locus biology
only in the presence of other locus SNP genotypes, support investment in future experiments
to test specific combinations, and help narrow which combinations to target.
CDKN2A/B T2D SNPs did not impact glucose-stimulated insulin secretion
Page 10 of 51Diabetes

A subset of islet samples (n=61) were tested for insulin secretion stimulation index at their
respective islet isolation centers. Insulin secretion index was positively correlated with BMI
but showed no relationship with donor age, sex, or islet isolation center by univariate
(Supplemental Figure 8) or multivariable (Supplemental Table 7) analysis. When insulin
secretion index was stratified by SNP genotype, contrary to the hypotheses that CDKN2A/B
T2D risk-SNPs impair glucose sensing, insulin production or stimulus-secretion coupling,
samples with T2D risk-alleles did not show evidence for impairment in ex vivo insulin
secretion in this cohort (Figure 6 and Supplemental Table 8).
Risk alleles at rs564398 reduced glucose-induced beta cell proliferation
Since CDKN2A/B locus genes are best known for inhibiting the cell cycle, we assessed
transcript markers of proliferation (KI67, PCNA and CCND2) in this cohort, as well as the
actual rate of S-phase entry in growth-stimulatory culture conditions, by BrdU labeling, in a
subset of samples. Surprisingly, although PCNA and CCND2 showed a high degree of
correlation with each other, KI67 did not correlate with either PCNA or CCND2 (Figure 7A-
C). No SNP genotype was correlated with abundance of PCNA, CCND2 or KI67 (not
shown). Transcript level is only a surrogate for proliferation, and lacks sensitivity in a tissue
with a very low frequency of proliferation events and a mixture of cell types. To measure
actual cell cycle entry in beta cells we cultured a subset (n=47) of islet preparations in low
(5mM) or high (15mM) glucose and quantified nuclear BrdU incorporation in insulin-
positive cells (Supplemental Figure 9). BrdU incorporation rate in 5mM glucose was
nominally correlated with basal PCNA abundance, but not with KI67 or CCND2
(Supplemental Figure 10). As previously observed (27,28,35), glucose increased human beta
cell proliferation (p<0.0001, not shown). To test whether any T2D SNP genotype impacted
beta cell proliferation, the proliferation index (ratio of BrdU+ beta cells in 15mM compared
to 5mM glucose) was stratified by SNP identity. Genotype at rs2383208, rs10811661 and
rs10757283 did not influence the proliferation index (Figure 7D-E). However, genotype at
rs564398 was strongly associated with the human beta cell proliferation index, with
homozygous-protective alleles showing approximately doubled stimulation of proliferation
by 15mM glucose compared with islet samples harboring risk alleles at this SNP (Figure 7F).
Page 11 of 51 Diabetes

DISCUSSION
We have performed a comprehensive analysis of how one T2D GWAS locus associated with
insulin secretory capacity in human populations influences human islet biology. In n=95 islet
samples we quantified locus gene expression, SNP genotype, donor characteristics, beta cell
function (insulin secretion) and beta cell proliferation. We have made several important
observations. First, the locus contains two distinct gene cassettes that are physically
overlapping but have different regulatory characteristics, one age-dependent and the other
not. Juvenile islets have markedly suppressed expression of p14-p16-ANRIL but not p15-
MTAP. Second, individual T2D SNPs at the locus do not substantially alter expression of
locus genes, but subtle age-dependent influences are detected, which, contrary to
expectations, impact the ANRIL lncRNA rather than the most prominent locus product, p16.
SNPs may interact with each other to influence gene expression, increasing the complexity of
genotype interpretation and raising intriguing mechanistic hypotheses. Third, genotype did
not impact insulin secretion index. Finally, risk-allele at rs564398, which is located within a
transcribed exon of ANRIL, decreased the beta cell proliferation index. This work improves
understanding of how CDKN2A/B T2D SNPs impact human islet biology, and suggests the
influence of the locus on human insulin secretory capacity may be effected via beta cell mass
rather than function.
How SNPs influence T2D risk is an important question in genetics today (3). Although the
CDKN2A/B locus is associated with a number of different disease syndromes (36), the SNPs
we selected to study are most strongly related to T2D risk, with the exception of rs564398,
which is also associated with coronary disease and glaucoma (15). CDKN2A/B SNPs are
associated with a range of diabetes-related syndromes beyond T2D, such as gestational
diabetes and transplant-related diabetes (9). Since this locus is active in many different cell
types, and the coronary disease risk region is mostly non-overlapping with the T2D risk
region (36), it is likely that CDKN2A/B impact on diseases other than T2D is mediated by
effects outside the islet. Given the association of rs10811661/rs2383208 with impaired
insulin production capacity, to identify possible T2D risk mechanisms we performed our
study in islets. Our data highlight the complexity of genetic inputs to human metabolism.
Even starting with a genomic locus repeatedly associated with disease risk across ethnicities
Page 12 of 51Diabetes

and T2D-related syndromes (9), with in vivo evidence that the islet is the risk-mediating
tissue (16,19–21), abundant preclinical locus knowledge in model systems (9,32), and a
fairly large sample size of the relevant tissue, the impact of risk-SNPs is subtle. As with
many studies in human islets, our data illustrate the marked variability from one donor to the
next, which reflects the variability of outbred human populations. We incorporated donor
parameters such as age and BMI in our analyses, but could not measure many potential other
confounding pre-mortem influences such as insulin sensitivity (liver, muscle, brain, fat),
coexisting diseases and medications, environmental effects (diet, stresses, toxins), exercise
history, prenatal events, and others. Islet stress related to donor demise, isolation, shipping
and culture may also introduce variability (37). In this context, subtle effects observed in this
challenging system may reflect large effects in certain sub-populations, or small effects
present uniformly across variable conditions.
The presence of two gene expression cassettes at the locus, only one of which is age-
dependent, suggests interesting biology. p16 is well known to increase with age in many
tissues and organisms (10). Our observation that p15 abundance did not increase with age in
human islets conflicts with published results in other tissues (38,39). The relationship
between MTAP and CDKN2A/B locus genes has not been extensively studied, but these are
contained in the same Hi-C defined topologically associating domain in the human genome
(Supplemental Figure 11) (40,41). Whether co-regulation of p15 and MTAP has functional
importance in the islet remains unknown.
rs2383208/rs10811661 impacted ANRIL abundance in age-dependent fashion. Islets
containing homozygous-risk alleles showed a “premature aging” phenotype, with young risk-
allele islets having ANRIL levels similar to older protective-allele islets. The low MAF for
these SNPs precluded comparison between homozygous-protective and homozygous-risk,
which might have revealed a larger effect size. We do not currently know whether one of
these, or another SNP in linkage with them, is causative. Fine mapping of this region has not
revealed SNPs with greater impact on T2D risk (1,4), but islet ANRIL abundance was not the
endpoint in those studies. These SNPs fall near a known regulatory region downstream of the
3’ end of ANRIL which may regulate ANRIL transcription. Mechanistically, how higher
Page 13 of 51 Diabetes

ANRIL abundance in islets might increase T2D risk is unknown. In other cell types, ANRIL is
pro-proliferative (42), an effect mediated by ANRIL-dependent suppression of locus cell
cycle inhibitors p14, p15 and p16 (43). Our RNA analyses did not detect any hint of negative
correlation between ANRIL and p14/p16 in islets; in fact, the strong positive correlation
between these transcripts calls into question whether ANRIL negatively regulates other locus
genes in human islets.
Beyond SNP regulation of ANRIL abundance, a second observation also points to a role for
ANRIL in human islets: rs564398, which influences the beta cell proliferation index, is a
transcribed polymorphism in this long-noncoding RNA. Although the causative SNP remains
unknown, it is possible that rs564983 itself impacts lncRNA activity. ANRIL is a
complicated gene, with 20 exons and at least 14 reported isoforms (42). Some ANRIL
variants are circular (44). Exon-2 is not contained in all isoforms, but is generally associated
with linear variants (44). Whether rs564398 identity impacts ANRIL isoform production,
splicing, stability, or interaction with other cellular DNA, RNA or protein, to regulate human
beta cell proliferation, remains unknown. Genotype at rs564398 did not correlate with
expression of cell cycle genes, or BrdU incorporation, under basal conditions; rs564398 may
be a marker for beta cell responsiveness to proliferation-inducing conditions rather than
increased proliferation in unstimulated conditions. Importantly, there are many SNPs in
linkage with rs564398, and any of these, or a combination of these, could be influencing
biology instead of rs564398 itself. Also important, while rs564398 has been repeatedly
confirmed to be associated with T2D in Caucasian populations, it has little to no relationship
to T2D risk in Asian populations (45–47). Taken together with the ‘premature aging’
influence of rs10811661/rs2383208 on ANRIL expression, CDKN2A/B SNPs may impact
T2D risk by adversely impacting accrual of beta cell mass during early adulthood.
Combinatorial SNP regulation of gene expression increases the complexity of how genomic
variation may impact cellular function. Whole-genome studies restricting locus analyses to
single ‘lead’ SNPs cannot detect biology related to two or more local SNPs interacting with
each other. The mechanism by which SNPs interact to regulate CDKN2A/B locus gene
expression in human islets is unknown. Interaction between rs10757283 and rs2383208 or
Page 14 of 51Diabetes

rs10811661 linked SNPs to regulate p15 abundance could be via modulation of transcription
factor occupancy or epigenetic regulation of the enhancer region in which they are located
(48). Intriguingly, our observed interaction between these SNPs is supported by a
complementary LD-block analysis which revealed that a haplotype consisting of
rs2383208/rs10811661 and rs10757283 was associated with T2D risk (13). There are
multiple SNPs in linkage disequilibrium with rs10811661 and also with rs10757283; actual
causal polymorphisms are unknown. A physical or functional interaction between the ANRIL
lncRNA and this enhancer may mediate cooperation between rs564398 and rs2383208,
rs10811661 or linked SNPs to regulate p16 expression. Our study cannot distinguish
between in-cis and in-trans interaction. Focused, cell-type-specific studies are needed to
determine how SNP combinations influence locus gene expression.
This study adds to the body of knowledge debating the relative influence of beta cell mass
versus function on T2D risk. Our study found that CDKN2A/B SNPs did not influence
glucose-stimulated insulin secretion, both in univariate analysis and in multivariable models
incorporating donor age, sex, race and BMI, and islet isolation center. This is perhaps
surprising given the in vivo data linking risk allele at rs10811661 with impaired insulin
secretion (16,22). Since in vivo insulin secretion is a composite outcome of both mass and
function, CDKN2A/B SNPs may impact beta cell mass but not beta cell function. This
concept is in agreement with the widespread assumption that CDKN2A/B SNPs influence
beta cell proliferation because of the known cell cycle inhibitory effects of locus genes p14,
p15 and p16 (49). Our rs564398 data are the first demonstration, to our knowledge, of a
CDKN2A/B locus SNP impacting beta cell proliferation.
Our study has caveats. Multiple cell types are found in human islets. Other than the
proliferation measurements, which were assessed in insulin-positive cells, all other studies
were performed on whole islets. We did not assess the relative proportion of islet cells that
were beta cells, and to the extent that gene expression may be cell type specific, variable
cellular makeup may have influenced results. In addition, there is considerable heterogeneity
even among beta cells (50,51). Repeating our current analyses on sorted beta cells, or on
single cells, exceeds our current resources. The insulin secretion data have caveats; using the
Page 15 of 51 Diabetes

IIDP-reported insulin secretion index introduces technical variability, although benefits from
freshly isolated, pre-shipment tissue. Our confirmation that insulin secretion correlated with
BMI, but not with isolation center, are reassuring in this regard.
In sum, this work provides new information about how CDKN2A/B T2D SNPs impact islet
biology, suggests the ANRIL lncRNA may play a role in human islets, and uncovers a link
between a T2D SNP and beta cell proliferation. Further studies into the CDKN2A/B locus to
develop a mechanistic understanding of how these SNPs impact islet biology to influence
T2D risk could one day open the door for using personalized genomic information to inform
T2D sub-type definitions and therapeutic choice.
ACKNOWLEDGMENTS
LCA devised and planned the experiments. YK performed the majority of the experiments;
SL, RBS and RES also performed experiments. YK and LCA analyzed the data. WMJ
performed the multivariable linear modeling. LCA, the guarantor of this work, wrote the
manuscript; all authors viewed and had the opportunity to edit and approve of the
manuscript. The authors have no conflicts of interest with the work contained in this
manuscript. Human pancreatic islets were provided by the NIDDK-funded Integrated Islet
Distribution Program (IIDP) at City of Hope, as well as Sambra Redick and David Harlan
from the UMass Medical School, and Alvin C. Powers from Vanderbilt University. We are
grateful to Ahmet Rasim Barutcu, from the Broad Institute and Harvard University, for
helpful guidance with the TAD analysis. We would like to thank the Beta Cell Biology
Group at the University of Massachusetts Medical School for many helpful discussions. This
work was supported by NIH/NIDDK: R01-DK095140 (LCA), DK104211 (ACP),
DK106755 (ACP), 2UC4DK098085 (IIDP) and by the American Diabetes Association grant
#1-15-BS-003 (LCA) in collaboration with the Order of the Amaranth.
Page 16 of 51Diabetes

REFERENCES 1. Morris AP. Fine Mapping of Type 2 Diabetes Susceptibility Loci. Curr Diab Rep
[Internet]. 2014 [cited 2015 Dec 30];14(11). Available from:
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4169615/
2. Morris AP, Voight BF, Teslovich TM, Ferreira T, Segrè AV, Steinthorsdottir V, et al.
Large-scale association analysis provides insights into the genetic architecture and
pathophysiology of type 2 diabetes. Nat Genet. 2012 Sep;44(9):981–90.
3. Fuchsberger C, Flannick J, Teslovich TM, Mahajan A, Agarwala V, Gaulton KJ, et al.
The genetic architecture of type 2 diabetes. Nature. 2016 Aug 4;536(7614):41–7.
4. Gaulton KJ, Ferreira T, Lee Y, Raimondo A, Mägi R, Reschen ME, et al. Genetic fine
mapping and genomic annotation defines causal mechanisms at type 2 diabetes
susceptibility loci. Nat Genet. 2015 Dec;47(12):1415–25.
5. van de Bunt M, Manning Fox JE, Dai X, Barrett A, Grey C, Li L, et al. Transcript
Expression Data from Human Islets Links Regulatory Signals from Genome-Wide
Association Studies for Type 2 Diabetes and Glycemic Traits to Their Downstream
Effectors. PLoS Genet. 2015 Dec;11(12):e1005694.
6. Fadista J, Vikman P, Laakso EO, Mollet IG, Esguerra JL, Taneera J, et al. Global
genomic and transcriptomic analysis of human pancreatic islets reveals novel genes
influencing glucose metabolism. Proc Natl Acad Sci. 2014 Sep 23;111(38):13924–9.
7. Varshney A, Scott LJ, Welch RP, Erdos MR, Chines PS, Narisu N, et al. Genetic
regulatory signatures underlying islet gene expression and type 2 diabetes. Proc Natl
Acad Sci U S A. 2017 Feb 28;114(9):2301–6.
8. Gaulton KJ. Mechanisms of Type 2 Diabetes Risk Loci. Curr Diab Rep. 2017
Sep;17(9):72.
9. Kong Y, Sharma RB, Nwosu BU, Alonso LC. Islet biology, the CDKN2A/B locus and
type 2 diabetes risk. Diabetologia. 2016 Aug;59(8):1579–93.
10. Kim WY, Sharpless NE. The regulation of INK4/ARF in cancer and aging. Cell. 2006
Oct 20;127(2):265–75.
11. Sharpless NE, Sherr CJ. Forging a signature of in vivo senescence. Nat Rev Cancer.
2015 Jul;15(7):397–408.
12. Scott LJ, Mohlke KL, Bonnycastle LL, Willer CJ, Li Y, Duren WL, et al. A genome-
wide association study of type 2 diabetes in Finns detects multiple susceptibility variants.
Science. 2007 Jun 1;316(5829):1341–5.
Page 17 of 51 Diabetes

13. Zeggini E, Weedon MN, Lindgren CM, Frayling TM, Elliott KS, Lango H, et al.
Replication of Genome-Wide Association Signals in UK Samples Reveals Risk Loci for
Type 2 Diabetes. Science. 2007 Jun 1;316(5829):1336–41.
14. Saxena R, Voight BF, Lyssenko V, Burtt NP, de Bakker PIW, Chen H, et al. Genome-
wide association analysis identifies loci for type 2 diabetes and triglyceride levels.
Science. 2007 Jun 1;316(5829):1331–6.
15. Cunnington MS, Santibanez Koref M, Mayosi BM, Burn J, Keavney B. Chromosome
9p21 SNPs Associated with Multiple Disease Phenotypes Correlate with ANRIL
Expression. PLoS Genet. 2010 Apr;6(4):e1000899.
16. Grarup N, Rose CS, Andersson EA, Andersen G, Nielsen AL, Albrechtsen A, et al.
Studies of association of variants near the HHEX, CDKN2A/B, and IGF2BP2 genes with
type 2 diabetes and impaired insulin release in 10,705 Danish subjects: validation and
extension of genome-wide association studies. Diabetes. 2007 Dec;56(12):3105–11.
17. Xu M, Bi Y, Xu Y, Yu B, Huang Y, Gu L, et al. Combined effects of 19 common
variations on type 2 diabetes in Chinese: results from two community-based studies. PloS
One. 2010;5(11):e14022.
18. Peng F, Hu D, Gu C, Li X, Li Y, Jia N, et al. The relationship between five widely-
evaluated variants in CDKN2A/B and CDKAL1 genes and the risk of type 2 diabetes: a
meta-analysis. Gene. 2013 Dec 1;531(2):435–43.
19. Hribal ML, Presta I, Procopio T, Marini MA, Stančáková A, Kuusisto J, et al. Glucose
tolerance, insulin sensitivity and insulin release in European non-diabetic carriers of a
polymorphism upstream of CDKN2A and CDKN2B. Diabetologia. 2011 Apr;54(4):795–
802.
20. Hart LM ‘t, Simonis-Bik AM, Nijpels G, Haeften TW van, Schäfer SA, Houwing-
Duistermaat JJ, et al. Combined Risk Allele Score of Eight Type 2 Diabetes Genes Is
Associated With Reduced First-Phase Glucose-Stimulated Insulin Secretion During
Hyperglycemic Clamps. Diabetes. 2010 Jan 1;59(1):287–92.
21. Dimas AS, Lagou V, Barker A, Knowles JW, Mägi R, Hivert M-F, et al. Impact of
Type 2 Diabetes Susceptibility Variants on Quantitative Glycemic Traits Reveals
Mechanistic Heterogeneity. Diabetes. 2014 Jun 1;63(6):2158–71.
22. Jonsson A, Ladenvall C, Ahluwalia TS, Kravic J, Krus U, Taneera J, et al. Effects of
Common Genetic Variants Associated With Type 2 Diabetes and Glycemic Traits on α-
and β-Cell Function and Insulin Action in Humans. Diabetes. 2013 Aug 1;62(8):2978–
83.
23. Brereton MF, Rohm M, Ashcroft FM. β-Cell dysfunction in diabetes: a crisis of
identity? Diabetes Obes Metab. 2016 Sep;18 Suppl 1:102–9.
Page 18 of 51Diabetes

24. Dai C, Hant Y, Shostak A, Poffenberger G, Hart N, Prasad N, et al. Age-dependent
human β-cell proliferation induced by GLP-1 and calcineurin signaling. J Clin Invest. in
press.
25. 1000 Genomes Project Consortium, Auton A, Brooks LD, Durbin RM, Garrison EP,
Kang HM, et al. A global reference for human genetic variation. Nature. 2015 Oct
1;526(7571):68–74.
26. Machiela MJ, Chanock SJ. LDlink: a web-based application for exploring population-
specific haplotype structure and linking correlated alleles of possible functional variants.
Bioinformatics. 2015 Nov 1;31(21):3555–7.
27. Sharma RB, O’Donnell AC, Stamateris RE, Ha B, McCloskey KM, Reynolds PR, et al.
Insulin demand regulates β cell number via the unfolded protein response. J Clin Invest.
2015 Oct 1;125(10):3831–46.
28. Stamateris RE, Sharma RB, Kong Y, Ebrahimpour P, Panday D, Ranganath P, et al.
Glucose induces mouse beta cell proliferation via IRS2, mTOR and cyclin D2 but not the
insulin receptor. Diabetes. (in press, 2016).
29. Pascoe J, Hollern D, Stamateris R, Abbasi M, Romano LC, Zou B, et al. Free fatty acids
block glucose-induced β-cell proliferation in mice by inducing cell cycle inhibitors p16
and p18. Diabetes. 2012 Mar;61(3):632–41.
30. Alonso LC, Yokoe T, Zhang P, Scott DK, Kim SK, O’Donnell CP, et al. Glucose
infusion in mice: a new model to induce beta-cell replication. Diabetes. 2007
Jul;56(7):1792–801.
31. Robertson KD, Jones PA. Tissue-specific alternative splicing in the human INK4a/ARF
cell cycle regulatory locus. Oncogene. 1999 Jul 1;18(26):3810–20.
32. Krishnamurthy J, Ramsey MR, Ligon KL, Torrice C, Koh A, Bonner-Weir S, et al.
p16INK4a induces an age-dependent decline in islet regenerative potential. Nature. 2006
Sep 28;443(7110):453–7.
33. Ward LD, Kellis M. HaploReg: a resource for exploring chromatin states, conservation,
and regulatory motif alterations within sets of genetically linked variants. Nucleic Acids
Res. 2012 Jan;40(Database issue):D930–4.
34. Gaunt TR, Rodríguez S, Day IN. Cubic exact solutions for the estimation of pairwise
haplotype frequencies: implications for linkage disequilibrium analyses and a web tool
“CubeX.” BMC Bioinformatics. 2007 Nov 2;8:428.
35. Levitt HE, Cyphert TJ, Pascoe JL, Hollern DA, Abraham N, Lundell RJ, et al. Glucose
stimulates human beta cell replication in vivo in islets transplanted into NOD-severe
combined immunodeficiency (SCID) mice. Diabetologia. 2011 Mar;54(3):572–82.
Page 19 of 51 Diabetes

36. Jeck WR, Siebold AP, Sharpless NE. Review: a meta-analysis of GWAS and age-
associated diseases. Aging Cell. 2012 Oct;11(5):727–31.
37. Stiegler P, Stadlbauer V, Hackl F, Schaffellner S, Iberer F, Greilberger J, et al.
Prevention of oxidative stress in porcine islet isolation. J Artif Organs Off J Jpn Soc Artif
Organs. 2010 Apr;13(1):38–47.
38. Menthena A, Koehler CI, Sandhu JS, Yovchev MI, Hurston E, Shafritz DA, et al.
Activin A, p15INK4b Signaling, and Cell Competition Promote Stem/Progenitor Cell
Repopulation of Livers in Aging Rats. Gastroenterology. 2011 Mar;140(3):1009–20.
39. Wang F, Zhang L. p15INK4b regulates cell cycle signaling in hippocampal astrocytes
of aged rats. Aging Clin Exp Res. 2016 Oct 1;28(5):813–21.
40. Zhou X, Maricque B, Xie M, Li D, Sundaram V, Martin EA, et al. The Human
Epigenome Browser at Washington University. Nat Methods. 2011 Nov 29;8(12):989–
90.
41. Wang Y, Zhang B, Zhang L, An L, Xu J, Li D, et al. The 3D Genome Browser: a web-
based browser for visualizing 3D genome organization and long-range chromatin
interactions | bioRxiv. BioRxiv [Internet]. 2017 [cited 2017 Dec 15]; Available from:
https://www.biorxiv.org/content/early/2017/02/27/112268
42. Congrains A, Kamide K, Ohishi M, Rakugi H. ANRIL: molecular mechanisms and
implications in human health. Int J Mol Sci. 2013;14(1):1278–92.
43. Aguilo F, Zhou M-M, Walsh MJ. Long noncoding RNA, polycomb, and the ghosts
haunting INK4b-ARF-INK4a expression. Cancer Res. 2011 Aug 15;71(16):5365–9.
44. Burd CE, Jeck WR, Liu Y, Sanoff HK, Wang Z, Sharpless NE. Expression of linear
and novel circular forms of an INK4/ARF-associated non-coding RNA correlates with
atherosclerosis risk. PLoS Genet. 2010;6(12):e1001233.
45. Wu Y, Li H, Loos RJF, Yu Z, Ye X, Chen L, et al. Common variants in CDKAL1,
CDKN2A/B, IGF2BP2, SLC30A8, and HHEX/IDE genes are associated with type 2
diabetes and impaired fasting glucose in a Chinese Han population. Diabetes. 2008
Oct;57(10):2834–42.
46. Ng MCY, Park KS, Oh B, Tam CHT, Cho YM, Shin HD, et al. Implication of genetic
variants near TCF7L2, SLC30A8, HHEX, CDKAL1, CDKN2A/B, IGF2BP2, and FTO
in type 2 diabetes and obesity in 6,719 Asians. Diabetes. 2008 Aug;57(8):2226–33.
47. Horikawa Y, Miyake K, Yasuda K, Enya M, Hirota Y, Yamagata K, et al.
Replication of genome-wide association studies of type 2 diabetes susceptibility in Japan.
J Clin Endocrinol Metab. 2008 Aug;93(8):3136–41.
Page 20 of 51Diabetes

48. Pasquali L, Gaulton KJ, Rodríguez-Seguí SA, Mularoni L, Miguel-Escalada I, Akerman
I, et al. Pancreatic islet enhancer clusters enriched in type 2 diabetes risk-associated
variants. Nat Genet. 2014 Feb;46(2):136–43.
49. Hannou SA, Wouters K, Paumelle R, Staels B. Functional genomics of the CDKN2A/B
locus in cardiovascular and metabolic disease: what have we learned from GWASs?
Trends Endocrinol Metab. 2015 Apr;26(4):176–84.
50. Gutierrez GD, Gromada J, Sussel L. Heterogeneity of the Pancreatic Beta Cell. Front
Genet. 2017;8:22.
51. Roscioni SS, Migliorini A, Gegg M, Lickert H. Impact of islet architecture on β-cell
heterogeneity, plasticity and function. Nat Rev Endocrinol. 2016 Dec;12(12):695–709.
Page 21 of 51 Diabetes

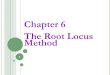
FIGURE LEGENDS Figure 1. CDKN2A/B locus genes were expressed coordinately in human islets. (A) Diagram
of the CDKN2A/B locus at 9p21, adapted from the UCSC genome browser GRCh38/hg38
assembly. Vertical arrows show the locations of T2D SNPs tested in this study, by linkage block:
green (rs564398; left-most), blue (rs2383208 and rs10811661; middle two) and red
(rs10757283; right-most). (B-D) Abundance of p14, p16 and ANRIL were highly correlated in
human islet samples. (E-G) p15 abundance did not correlate with p16, and only marginally
correlated with p14 and ANRIL. MTAP expression was marginally correlated with p14, p16 and
ANRIL (H and not shown), but (I) highly correlated with p15 expression. mRNA abundance is
expressed as delta-Ct, normalized to ACTB. Line, p values and R-squared values were calculated
by linear regression; n=95 for all panels. Red lines highlight correlations with higher R-squared
values.
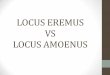
Figure 2. Abundance of p14, p16 and ANRIL, but not p15 or MTAP, was correlated with
donor age and strongly reduced in juvenile islets. (A-E) Consistent with prior observations,
p16 mRNA abundance was positively correlated with donor age (in years). p14 and ANRIL were
also correlated with age, but p15 and MTAP were not. Age accounted for only a small proportion
of the variance in gene expression, even for p16. (F) BMI partitioned equally across donor age in
this cohort (dotted lines demarcate BMI 18-25 (normal weight), 25-30 (overweight) and >30
(obese). (G-K) Islets from juvenile donors (age <10 years) contained markedly less p14, p16 and
ANRIL, but not p15 or MTAP, than older islets. mRNA abundance is expressed as delta-Ct,
normalized to ACTB. Mean +/- SD; p values and R-squared values were calculated by linear
regression (A-F) or by Student’s T-test (G-K). All panels n=92; missing values are due to lack of
donor information for age and BMI (3 samples).
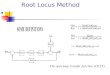
Figure 3. In crude analysis, individual SNP identity did not impact expression of locus
genes in human islets. Risk allele for each SNP, the right-most genotype in each case, is in red.
All comparisons were non-significant by ANOVA with correction for multiple comparisons.
ANRIL showed a trend towards higher abundance in islets with homozygous-risk for rs10811661
(p=0.08) and rs2383208 (p=0.07) compared with protective-allele-carrying samples.
Page 22 of 51Diabetes

rs108=rs10811661; rs238=rs2383208; rs107=rs10757283; rs564=rs564398. mRNA
abundance is expressed as delta-Ct, normalized to ACTB. Mean +/- SD; n=95 for all sub-panels.
Figure 4. Age interacted with genotype at rs2383208 to determine ANRIL abundance;
young donors with protective alleles had lower ANRIL expression. (A-B) Expressing p16 (A)
or ANRIL (B) abundance as a function of donor age, stratified by genotype, showed that unlike
p16, age-dependence of ANRIL was driven by samples of rs2383208-GG+GA genotype and was
absent in samples with AA (homozygous risk) genotype. (C-D) Binning analysis of the cohort
(non-juvenile samples separated by quartiles) illustrated the age-dependent ANRIL increase in
GG+GA samples but not in homozygous-risk AA samples. Juveniles <10 years of age showed
markedly lower abundance, independent of genotype. (E-F) In younger donors (ages 10-50;
lower threshold defined by juvenile cutoff and upper threshold defined by the intersection of the
regression curves in (B), which is 50.8) homozygous-risk increased ANRIL abundance. mRNA
abundance is expressed as delta-Ct, normalized to ACTB. Statistics by linear regression (A-B),
ANOVA (D-F) with overall ANOVA significance in upper left corner and significant pairwise
comparisons after correction for multiple comparisons labeled. Sample size: (A-D) n=92 (3
samples missing age) and (E-F) n=57 samples between the ages of 10-50.
Figure 5. SNP combinatorial haplotypes may influence locus gene expression. (A)
Schematic showing approximate locations of the T2D SNPs analyzed in this study, relative to
the ANRIL gene. SNP colors, as in Figure 1A, indicate linkage disequilibrium. (B-C): Protective
alleles of rs10811661 (shown) and rs2383208 (Supplemental Fig 4) may decrease expression of
p16 in homozygous-protective rs564398-CC samples. The same comparison for p14 did not
meet FDR<10% (q-value 17%); for ANRIL, FDR>20% (not shown). (D-E): Homozygous risk
alleles at both neighboring SNPs rs10757283 and rs10811661 may collaboratively increase p15
expression. The same comparison for MTAP showed FDR>20%. * indicates FDR<10%, our pre-
determined risk tolerance for future experiments exploring haplotype hypotheses. mRNA
abundance is expressed as delta-Ct, normalized to ACTB. n=95 for all panels. All other inter-
SNP comparisons, both shown and not shown (aside from those in Supplemental Figure 4),
resulted FDR>10% or had insufficient data points to evaluate (defined as n=2 or fewer). FDR,
false discovery rate.
Page 23 of 51 Diabetes

Figure 6. Insulin secretion was similar across SNP genotypes. 61 of the islet preparations
were tested for glucose-stimulated insulin release “stimulation index” at islet isolation centers;
the IIDP-derived insulin secretion index is plotted against donor genotype. No relationship is
evident between T2D SNP genotype and IIDP-reported insulin secretory index.
rs108=rs10811661; rs238=rs2383208; rs107=rs10757283; rs564= rs564398. n=61 for all
SNPs.
Figure 7. Risk allele at rs564398 suppressed glucose induction of beta cell proliferation. (A-
C) RNA abundance of proliferation-related genes PCNA, CCND2 and KI67 in flash-frozen islets
showed a strong correlation between PCNA and CCND2 (A) but not with KI67 (B-C). (D-F)
rs564398, but not rs2383208, rs10811661 or rs10757283 was associated with beta cell
proliferation. Islets containing 1 or 2 T2D risk alleles at rs564398 had lower proliferation index
than islets containing homozygous-protective alleles at rs564398. Dispersed islets were cultured
on glass coverslips for 96 hours in either 5mM glucose (unstimulated) or 15mM glucose
(stimulated) with BrdU present for the whole 96 hours. Cultures were fixed, immunostained,
imaged, blinded and the percent insulin(+) cells that were also BrdU(+) quantified by manual
counting. Plotted is the proliferation index, which is the ratio of 15mM to 5mM. n=95 (A-C) and
n=43 (D-F; 47 preps tested, but 4 preps had 0% BrdU+ in 5mM glucose and thus could not
calculate an index). mRNA abundance is expressed as delta-Ct, normalized to ACTB. Mean +/-
SD; p values are by linear regression (A-C) and ANOVA with correction for multiple
comparisons (D-F).
Page 24 of 51Diabetes

Figure 1. CDKN2A/B locus genes were expressed coordinately in human islets. (A) Diagram of the CDKN2A/B locus at 9p21, adapted from the UCSC genome browser GRCh38/hg38 assembly. Vertical arrows
show the locations of T2D SNPs tested in this study, by linkage block: green (rs564398; left-most), blue
(rs2383208 and rs10811661; middle two) and red (rs10757283; right-most). (B-D) Abundance of p14, p16 and ANRIL were highly correlated in human islet samples. (E-G) p15 abundance did not correlate with p16, and only marginally correlated with p14 and ANRIL. MTAP expression was marginally correlated with p14,
p16 and ANRIL (H and not shown), but (I) highly correlated with p15 expression. mRNA abundance is expressed as delta-Ct, normalized to ACTB. Line, p values and R-squared values were calculated by linear
regression; n=95 for all panels. Red lines highlight correlations with higher R-squared values.
172x163mm (300 x 300 DPI)
Page 25 of 51 Diabetes

Figure 2. Abundance of p14, p16 and ANRIL, but not p15 or MTAP, was correlated with donor age and strongly reduced in juvenile islets. (A-E) Consistent with prior observations, p16 mRNA abundance was positively correlated with donor age (in years). p14 and ANRIL were also correlated with age, but p15 and
MTAP were not. Age accounted for only a small proportion of the variance in gene expression, even for p16. (F) BMI partitioned equally across donor age in this cohort (dotted lines demarcate BMI 18-25 (normal
weight), 25-30 (overweight) and >30 (obese). (G-K) Islets from juvenile donors (age <10 years) contained markedly less p14, p16 and ANRIL, but not p15 or MTAP, than older islets. mRNA abundance is expressed as delta-Ct, normalized to ACTB. Mean +/- SD; p values and R-squared values were calculated by linear regression (A-F) or by Student’s T-test (G-K). All panels n=92; missing values are due to lack of donor
information for age and BMI (3 samples).
172x163mm (300 x 300 DPI)
Page 26 of 51Diabetes

Figure 3. In crude analysis, individual SNP identity did not impact expression of locus genes in human islets. Risk allele for each SNP, the right-most genotype in each case, is in red. All comparisons were non-significant by ANOVA with correction for multiple comparisons. ANRIL showed a trend towards higher
abundance in islets with homozygous-risk for rs10811661 (p=0.08) and rs2383208 (p=0.07) compared with protective-allele-carrying samples. rs108=rs10811661; rs238=rs2383208; rs107=rs10757283;
rs564=rs564398. mRNA abundance is expressed as delta-Ct, normalized to ACTB. Mean +/- SD; n=95 for all sub-panels.
172x163mm (300 x 300 DPI)
Page 27 of 51 Diabetes

Figure 4. Age interacted with genotype at rs2383208 to determine ANRIL abundance; young donors with protective alleles had lower ANRIL expression. (A-B) Expressing p16 (A) or ANRIL (B) abundance as a
function of donor age, stratified by genotype, showed that unlike p16, age-dependence of ANRIL was driven
by samples of rs2383208-GG+GA genotype and was absent in samples with AA (homozygous risk) genotype. (C-D) Binning analysis of the cohort (non-juvenile samples separated by quartiles) illustrated the age-dependent ANRIL increase in GG+GA samples but not in homozygous-risk AA samples. Juveniles <10 years of age showed markedly lower abundance, independent of genotype. (E-F) In younger donors (ages 10-50; lower threshold defined by juvenile cutoff and upper threshold defined by the intersection of the
regression curves in (B), which is 50.8) homozygous-risk increased ANRIL abundance. mRNA abundance is expressed as delta-Ct, normalized to ACTB. Statistics by linear regression (A-B), ANOVA (D-F) with overall ANOVA significance in upper left corner and significant pairwise comparisons after correction for multiple comparisons labeled. Sample size: (A-D) n=92 (3 samples missing age) and (E-F) n=57 samples between
the ages of 10-50.
172x163mm (300 x 300 DPI)
Page 28 of 51Diabetes

Figure 5. SNP combinatorial haplotypes may influence locus gene expression. (A) Schematic showing approximate locations of the T2D SNPs analyzed in this study, relative to the ANRIL gene. SNP colors, as in Figure 1A, indicate linkage disequilibrium. (B-C): Protective alleles of rs10811661 (shown) and rs2383208
(Supplemental Fig 4) may decrease expression of p16 in homozygous-protective rs564398-CC samples. The same comparison for p14 did not meet FDR<10% (q-value 17%); for ANRIL, FDR>20% (not shown). (D-E): Homozygous risk alleles at both neighboring SNPs rs10757283 and rs10811661 may collaboratively increase
p15 expression. The same comparison for MTAP showed FDR>20%. * indicates FDR<10%, our pre-determined risk tolerance for future experiments exploring haplotype hypotheses. mRNA abundance is expressed as delta-Ct, normalized to ACTB. n=95 for all panels. All other inter-SNP comparisons, both
shown and not shown (aside from those in Supplemental Figure 4), resulted FDR>10% or had insufficient data points to evaluate (defined as n=2 or fewer). FDR, false discovery rate.
172x163mm (300 x 300 DPI)
Page 29 of 51 Diabetes

Figure 6. Insulin secretion was similar across SNP genotypes. 61 of the islet preparations were tested for glucose-stimulated insulin release “stimulation index” at islet isolation centers; the IIDP-derived insulin
secretion index is plotted against donor genotype. No relationship is evident between T2D SNP genotype and
IIDP-reported insulin secretory index. rs108=rs10811661; rs238=rs2383208; rs107=rs10757283; rs564= rs564398. n=61 for all SNPs.
172x163mm (300 x 300 DPI)
Page 30 of 51Diabetes

Figure 7. Risk allele at rs564398 suppressed glucose induction of beta cell proliferation. (A-C) RNA abundance of proliferation-related genes PCNA, CCND2 and KI67 in flash-frozen islets showed a strong correlation between PCNA and CCND2 (A) but not with KI67 (B-C). (D-F) rs564398, but not rs2383208,
rs10811661 or rs10757283 was associated with beta cell proliferation. Islets containing 1 or 2 T2D risk alleles at rs564398 had lower proliferation index than islets containing homozygous-protective alleles at
rs564398. Dispersed islets were cultured on glass coverslips for 96 hours in either 5mM glucose (unstimulated) or 15mM glucose (stimulated) with BrdU present for the whole 96 hours. Cultures were fixed,
immunostained, imaged, blinded and the percent insulin(+) cells that were also BrdU(+) quantified by manual counting. Plotted is the proliferation index, which is the ratio of 15mM to 5mM. n=95 (A-C) and n=43 (D-F; 47 preps tested, but 4 preps had 0% BrdU+ in 5mM glucose and thus could not calculate an
index). mRNA abundance is expressed as delta-Ct, normalized to ACTB. Mean +/- SD; p values are by linear regression (A-C) and ANOVA with correction for multiple comparisons (D-F).
172x163mm (300 x 300 DPI)
Page 31 of 51 Diabetes

16 18 20 22 24
1618
2022
24
Ct value 2
Ct v
alue
1
ACTNp<0.0001R2=0.85
RPD1.13%
Supplemental Figure 1. Taqman gene expression duplicates show high reproducibility. For each CDKN2A/B locus gene, Taqman Ct values of replicate 1 (Ct value 1) and replicate 2 (Ct value 2) are plotted. The RPD values, the absolute value of the Relative Percentage Di�erence, were calculated from the equa-tion RPD=(D1-D2)/(D1+D2)/2X100. RPDs for all genes were well within established goals for biological replicate variability of 10%. Line, p values and R-squared values were calculated by linear regression; n=95 for all panels.
A B GAPDHp<0.0001R2=0.94
RPD0.81%
16 18 20 22 2416
1820
2224
Ct value 2
Ct v
alue
1
C
RPD0.65%
p14p<0.0001R2=0.95
26 28 30 32 34 36
2628
3032
3436
Ct value 2
Ct v
alue
1
RPD1.05%
p15p<0.0001R2=0.92
22 24 26 28 30 32 34
2224
2628
3032
34
Ct value 2
Ct v
alue
1
D
E F G H
I J K
RPD1.05%
p15p<0.0001R2=0.92
22 24 26 28 30 32 34
2224
2628
3032
34
Ct value 2
Ct v
alue
1
RPD0.56%
p16p<0.0001R2=0.97
24 26 28 30 32 34
2426
2830
3234
Ct value 2
Ct v
alue
1
RPD1.30%
ANRILp<0.0001R2=0.87
25 30 35 40
2530
3540
Ct value 2
Ct v
alue
1RPD0.60%
MTAPp<0.0001R2=0.94
22 24 26 28 30 32
2224
2628
3032
Ct value 2
Ct v
alue
1
20 25 30 35 40
2025
3035
40
Ct value 2
Ct v
alue
1
RPD0.60%
KI67p<0.0001R2=0.99
24 26 28 30 32 34
2426
2830
3234
Ct value 2
Ct v
alue
1
RPD0.64%
PCNAp<0.0001R2=0.88
20 22 24 26 28 30
2022
2426
2830
Ct value 2
Ct v
alue
1
RPD0.67%
CCND2p<0.0001R2=0.96
Page 32 of 51Diabetes

0.0000 0.0005 0.0010
0.00
20.
004
ANRIL
p14
0.000 0.002 0.004
0.01
0.02
p14
p16
0.00 0.01 0.02
0.00
050.
0010
p16
ANR
IL
0.00 0.01 0.02
0.02
0.04
p16
p15
p<0.0001R2=0.42
p<0.0001R2=0.83
p<0.0001R2=0.37
p<0.0001R2=0.52
Supplemental Figure 2. CDKN2A/B locus gene expression in human islets normalized to GAPDH. As observed when normalized to ACTIN, CDKN2A/B locus genes when normalized to islet GAPDH abundance revealed a high degree of correlation between p14-p16-ANRIL (A-C). p15 and MTAP showed little or no correlation with p14, p16 or ANRIL (D-G). However, p15 and MTAP expression correlated with each other. mRNA abundance is expressed as delta-Ct, normalized to GAPDH. Line, p values and R-squared values were calculated by linear regression; n=95 for all panels. Red lines high-light correlations with higher R-squared values.
A B C D
HE F G p<0.01R2=0.08
p=ns
p=ns p=ns
0.00 0.02 0.04
0.02
0.04
p15
MTA
P
0.0000 0.0005 0.0010
0.02
0.04
ANRIL
MTA
P
0.0000 0.0005 0.0010
0.02
0.04
ANRIL
p15
0.000 0.002 0.004
0.02
0.04
p14
p15
Page 33 of 51 Diabetes

A B C
D E
Supplemental Figure 3. Donor BMI did not correlate with locus gene expression. (A-E) Reported donor BMI was compared with islet gene expression by univariate linear regression analysis. No locus gene mRNA abundance was correlated with BMI. mRNA abundance is expressed as delta-Ct, normalized to actin. Statistical analysis was calculated by linear regres-sion; n=92 for all panels. Missing values include the 3 islet samples for which donor BMI was not available.
0 20 40 60
0.00
20.
004
BMI
p14
0 20 40 60
0.02
0.04
BMI
p15
0 20 40 60
0.01
0.02
BMI
p16
0 20 40 60
0.00
050.
0010
BMI
ANR
IL
0 20 40 60
0.02
0.04
BMI
MTA
P
Page 34 of 51Diabetes

A B C
D E F
Supplemental Figure 4. Locus gene expression did not vary by donor sex. (A-E) No relationship was observed between locus gene expression and donor sex. F: female; M: male. (F) The mean age of male donors was signi�cantly lower than that of females, owing to an unfortunately high number of teenage and young-adult male donors. After age-matching the male and female cohorts (by removing all samples from both sexes with age < 27 years), reanalysis con�rmed that no locus gene expression correlated with donor sex (data not shown). mRNA abundance is expressed as delta-Ct, normalized to actin. Statistical analy-sis was calculated by Student’s t-test; n=42 females and 48 males for all panels. Missing values include the 5 islet samples for which donor sex was not available.
p<0.05
0.00
050.
0010
ANR
IL0.
002
0.00
4
p14
0.01
0.02
0.03
p15
0.01
0.02
p16
0.02
0.04
MTA
P
020
4060
80
Don
or A
ge
F M F M F M
F M F M F M
Page 35 of 51 Diabetes

A B C
D E F
Supplemental Figure 5. Locus gene expression did not di�er by donor ethnici-ty. (A-E) No relationship was observed between locus genes and donor ethnicity. (F) Mean donor age was not di�erent in the ethnicity categories. mRNA abundance is expressed as delta-Ct, normalized to actin. Statistical analysis was calculated by ANOVA; p=ns for all comparisons. Sample sizes are n=1 (Asian), n=8 (black), n=14 (hispanic) and n=66 (white). Missing values include the 6 islet samples for which donor ethnicity was not available.
0.00
000.
0005
0.00
10
ANR
IL0.
000
0.00
20.
004
p14
0.01
0.02
0.03
p15
0.00
0.01
0.02
p16
0.01
0.02
0.03
MTA
P
0
20
40
60
80
Don
or A
ge
Asi
anB
lack
His
pani
cW
hite
Asi
anB
lack
His
pani
cW
hite
Asi
anB
lack
His
pani
cW
hite
Asi
anB
lack
His
pani
cW
hite
Asi
anB
lack
His
pani
cW
hite
Asi
anB
lack
His
pani
cW
hite
Page 36 of 51Diabetes

p=0.03, R2=0.20p=0.001, R2=0.16
p=0.0002, R2=0.46p=ns
CC+CTAll panels: rs10811661 TT C=protective, T=risk
Supplemental Figure 6. Age interacts with genotype at rs10811661 to determine ANRIL abundance; young donors with protective alleles had lower ANRIL expression. Similar analysis to Figure 4 for rs2383208. (A-B) Expressing p16 (A) or ANRIL (B) abundance as a function of donor age, strati�ed by geno-type, showed that unlike p16, age-dependence of ANRIL was driven by samples of rs10811661-CC+CT geno-type and was absent in samples with TT genotype. (C-D) Binning analysis of the cohort (non-juvenile sam-ples separated by quartiles) illustrated an age-dependent ANRIL increase in CC+CT samples but not in homozygous-risk TT samples. Juveniles <10 years of age showed markedly di�erent biology, independent of genotype. (E-F) In younger donors (ages 10-50; lower threshold de�ned by juvenile cuto� and upper thresh-old de�ned by the intersection of the regression curves in (B), which is 50.8) homozygous-risk increased ANRIL abundance. mRNA abundance is expressed as delta-Ct, normalized to actin. Statistics by linear regres-sion (A-B), ANOVA (D-F) with overall ANOVA signi�cance in upper left corner and signi�cant pairwise com-parisons after correction for multiple comparisons labeled. Sample size: (A-D) n=92 (3 samples missing age) and (E-F) n=57 samples between the ages of 10-50.
<10
15-3
132
-44
45-5
152
-68
<10
15-3
132
-44
45-5
152
-68
p<0.05p<0.05
p<0.01
p=nsp<0.01
<10
15-3
132
-44
45-5
152
-68
<10
15-3
132
-44
45-5
152
-68
p=0.05 p<0.05A C E
B D F p<0.05
p=ns
CC CT TT
CC CT TT
0 20 40 60 800.000
0.005
0.010
0.015
0.020
0.025
Donor age
p16
0 20 40 60 800.0000
0.0005
0.0010
0.0015
Donor age
ANR
IL
0.00
0.01
0.02
p16
0.00
000.
0005
0.00
10
ANR
IL
0.00
0.01
0.02
p16
0.00
000.
0004
0.00
08
ANR
IL
Page 37 of 51 Diabetes

Supplemental Figure 7. Haplotype analysis showing rs2383208 comparisons. Related to the analysis in Figure 5 for rs10811661. (A-B): For p16, in homozygous-protective rs564398-CC samples, homozy-gous-risk rs2383208 increased expression. The same comparison for p14 did not meet FDR<10% (q-value 17%); for ANRIL, FDR>20% (not shown). (C-D): rs10757283 and rs2383208 may collaboratively regulate p15 expression; for MTAP for the same comparison, FDR>20%. * indicates FDR<10%, our pre-determined risk tolerance for future experiments exploring haplotype hypotheses. mRNA abundance is expressed as delta-Ct, normalized to actin. n=95 for all panels. All other inter-SNP comparisons, both shown and not shown, resulted FDR >10% or had insu�cient data points to evaluate (de�ned as n=2 or fewer). FDR, False Discovery Rate.
C D
A B
0.00
0.01
0.02
0.03
p16
rs564398 CC CT TT
*
0.000
0.001
0.002
0.003
0.004
0.005
p14
rs564398 CC CT TT
All panels: rs2383208 GG+GA rs2383208 AA
0.00
0.01
0.02
0.03
0.04
0.05
p15
*
rs10757283 CC CT TT0.00
0.01
0.02
0.03
0.04
MTA
P
rs10757283 CC CT TT
Page 38 of 51Diabetes

Supplemental Figure 8. Insulin secretion index correlated with donor BMI but was not related to age, sex or isolation center. (A) Insulin secretion index positively correlated with donor BMI. Vertical dotted lines represent demarkations between normal weight (18-25), overweight (25-30) and obese (>30). (B-D) Insulin secretion index was not related to donor age (B), donor sex (C), or isolation center (D). Numerals I-VI refer to the six di�erent islet isolation centers where the IIDP islet samples originated; we do not have insulin secretion data from any non-IIDP samples used in this study. (A-B): n=61; line, p values and R-squared values were calculated by linear regression. (C): n=31 (F), n=30 (M); mean +/- SD, p value by Student’s t-test. (D): n=61 samples from all isolation centers combined; mean +/- SD, ANOVA with Bonfer-roni correction for multiple comparisons.
A B
C D
p<0.01R2=0.13
p=ns
p=nsp=ns
0 20 40 60 800
5
10
15
Donor age
Insu
lin s
ecre
tion
inde
x
10 20 30 40 50 600
5
10
15
Donor BMI
Insu
lin s
ecre
tion
inde
x
F M0
5
10
Insu
lin s
ecre
tion
inde
x
I II IIIIslet isolation center
IV V VI02468
10
Insu
lin s
ecre
tion
inde
x
Page 39 of 51 Diabetes

F F
F
F
5 mM glucose
Insulin BrdU Dapi
15 mM glucose
F
Supplemental Figure 9. Images of dispersed human islet cells cultured for BrdU analysis. Human islets were rested overnight, dispersed using trypsin, and cultured on coverslips for 96 hours in 5mM or 15mM glucose with BrdU included for the entire 96 hours. Coverslips were �xed in paraformaldehyde, immunostained for insulin and BrdU, mounted in Dapi-containing media, and imaged using �uorescent microscopy. Images were blinded and manually counted for total insulin(+) cells and % of insulin(+) BrdU(+) cells to generate the data shown in Figure 7. F, BrdU-staining �broblast. Arrows denote BrdU(+) Insulin(+) cells.
Page 40 of 51Diabetes

0.0 0.5 1.0 1.5 2.00.00
0.05
0.10
0.15
BrdU 5mM
CC
ND
2
0.0 0.5 1.0 1.5 2.00.00
00.
005
0.01
00.
015
0.02
0
BrdU 5mM
KI67
0.0 0.5 1.0 1.5 2.00.00
00.
002
0.00
40.
006
BrdU 5mM
PCN
A
Supplemental Figure 10. Cell cycle gene expression (on whole islets under basal (5mM) glucose culture conditions, same samples as all previous gene expression data), shown in relation to dispersed islet cell BrdU incorporation in basal (5mM) glucose conditions. PCNA was marginally correlated with BrdU%; KI67 and CCND2 were not. mRNA abundance is expressed as delta-Ct, normalized to actin. BrdU 5mM: % of insulin(+) cells that were also BrdU(+) cells, in 5mM glucose cultures. Statistical analysis was calculated by linear regression; n=46 all panels.
p<0.05R2=0.10 p=ns p=ns
Page 41 of 51 Diabetes

Supplemental Figure 11. Topologically Associated Domain analysis of the human CDKN2A/B locus by Hi-C of lymphoblastoid cell line GM12878. Assmebly: hg19. (A) 25 kb resolution, and (B) 10 kb reso-lution. Data are from Rao et al, Cell 159(7):1665-1680 (2014), and analysis is by the Yue lab website http://promoter.bx.psu.edu/hi-c/view.php and "The 3D Genome Browser: a web-based browser for visual-izing 3D genome organization and long-range chromatin interactions." http://biorxiv.org/content/ear-ly/2017/02/27/112268, Biorxiv, 2017.
A. resolution 25 kb
B. resolution 10 kb
Page 42 of 51Diabetes

Supplemental Table 1: Donor characteristics and data obtained for each islet preparation
Sex Age BMI Ethinicity Cause of DeathSNP
genotype and RNA
Insulin secretion
Beta cell proliferation
M 42 22.76 Black Anoxia x x xM 40 38.91 White Unknown x x xF 54 22.6 White Cerebrovascular/stroke x xF 51 35.6 White Anoxia x x xF 38 33.1 White Anoxia x x xM 22 32.1 Hispanic Head trauma x xF 47 34.5 Hispanic Cerebrovascular/stroke x xF 39 45.2 White Anoxia x x xM 40 35.4 White Unknown x xM 46 29.3 Unknown Cerebrovasular/stroke x xM 22 40.2 White Head trauma x xM 1.8 18.7 White anoxia xF 0.2 20.8 Hispanic Anoxia xM 48 31.2 White Cerebrovascular/stroke x x
Unknown Unknown Unknown Unknown Unknown xM 57 29.8 White Head Trauma x xF 45 27.4 White Cerebrovascular/stroke x x xF 51 28.7 White Cerebrovascular/stroke x x xM 25 33.8 Hispanic Head Trauma x x xF 50 41.3 Hispanic Cerebrovascular/stroke x xF 49 36.9 White Cerebrovascular/stroke x x xF 52 35.2 White Cerebrovascular/stroke x xF 47 29.9 Black Cerebrovascular/stroke x xF 61 31 Black Cerebrovascular/stroke x xF 32 39.4 White Unknown x x xF 8 16.1 White Cerebrovascular/stroke xF 29 21 White Head trauma x x xM 7 26.6 White Anoxia xM 52 29 White Anoxia x xF 52 31.4 White Cerebrovascular/stroke x x xM 28 32.8 White Cerebrovascular/stroke x x xM 15 23 White Head trauma x x xM 63 38.6 White Anoxia x x xM 35 32 Hispanic Cerebrovascular/stroke x x xM 24 29.4 White Head trauma x xF 36 42.7 White Anoxia x x xM 18 27.9 White Cerebrovascular/stroke x x xM 55 33.4 White Cerebrovascular/stroke x xF 45 32.9 White Cerebrovascular/stroke x x xF 39 22.8 White Cerebrovascular/stroke x xF 56 21.43 White Chronic back pain/stroke xM 19 34.1 Hispanic Head trauma x x xM 25 26 White Cerebrovascular/stroke x x xM 32 27.8 Black Head trauma x x xF 49 31.6 White Cerebrovascular/stroke x xF 58 19.2 White Anoxia x x xM 21 24.8 White Head trauma x x xF 45 26.6 White Cerebrovascular/stroke x x xF 56 33.4 Black Cerebrovascular/stroke x x xM 35 28.5 Asian Head trauma x x xM 30 56.8 White Anoxia x xM 63 21.9 White Cerebrovascular/stroke x x x
Page 43 of 51 Diabetes

F 54 30.1 White Cerebrovascular/stroke x x xM 20 19.8 White Anoxia x x xF 52 26.8 Black Cerebrovascular/stroke x x xM 37 30.5 White Head trauma x x xF 53 31.9 White Cerebrovascular/stroke x x xF 59 28.2 Hispanic Cerebrovascular/stroke x x xF 33 34.2 Black Cerebrovascular/stroke x x xF 40 23 Hispanic Cerebrovascular/stroke x x xM 47 31 White Anoxia x x xM 1.3 22 White Head trauma/Blunt Injury xF 44 34.5 White Cerebrovascular/stroke x x xF 47 36.4 Black Anoxia x x xM 15 24.6 Hispanic Head trauma x xM 49 26.47 White Head trauma/Blunt Injury x xF 59 22 White Cerebrovascular/stroke x x xM 59 26.8 White Anoxia x x xM 68 29.7 White Cerebrovascular/stroke x x xM 60 31.3 White Head trauma x x xM 60 37.9 White Anoxia x x xF 37 25.07 Hispanic Anoxia x
Unknown Unknown Unknown Unknown Unknown xUnknown 29 42.2 Unknown Unknown x
F 40 27.8 White Cerebrovascular/stroke xM 28 32 Hispanic Cerebrovascular/stroke xF 27 26.9 White Cerebrovascular/stroke xM 51 30.2 White Cerebrovascular/stroke xM 52 33.7 White Cerebrovascular/stroke xF 51 23.9 White Unknown xM 30 26.5 Hispanic Unknown xM 30 26.9 White Head trauma xF 63 36.6 White Cerebrovascular/stroke x
Unknown Unknown Unknown Unknown Unknown xM 45 25.49 White Head trauma xM 54 39.2 White Blunt Head Trauma MVA xM 17 32.5 White Unknown xM 51 28.1 Hispanic Unknown x
Unknown 56 26.7 Unknown Unknown xF 35 37 White Cerebrovascular/stroke xM 36 51.9 White Cerebrovascular/stroke xF 40 28.4 White Unknown xF 33 22.3 White Cerebrovascular/stroke xM 35 46.1 White Unknown xM 48 29 White Cerebrovascular/stroke x
Page 44 of 51Diabetes

Supplemental Table 2: Minor Allele Frequenciesrs2383208 rs10757283 rs10811661 rs564398
G/G C/C C/C C/CG/A C/T C/T C/TA/A T/T T/T T/TG T C CA T T T
All (n=95) 16.3% 46.8% 15.3% 36.8%
Black (n=8) 6.3% 37.5% 0.0% 6.3%
Hispanic (n=13) 10.7% 42.9% 10.7% 28.6%
Caucasian (n=62) 18.9% 50.0% 18.2% 42.4%
Observed minor allele frequency in 1000
GenomesEUR 17.3% 43.9% 16.8% 41.4%
Supplemental Table 2. For each SNP the minor allele, risk allele (in red) and observed minor allele frequency (MAF) in this human islet cohort are described. These MAFs are similar to those reported in the large populations tested in the 1000 genomes project (data are shown for EUR, since we have too few samples in non-white categories for accurate comparison).
Observed minor allele frequency in this
human islet cohort
CDKN2A/B LocusT2D SNPs tested
Minor alleleRisk allele
Page 45 of 51 Diabetes

Supplemental Table 3: Linkage Disequilibrium
Expected LD (R2) (from EUR population)rs564398 rs2383208 rs10811661 rs10757283
rs564398 0.006 0.007 0.016rs2383208 0.006 0.952 0.256rs10811661 0.007 0.952 0.258rs10757283 0.016 0.256 0.258
Observed LD (R2) in our samplesrs564398 rs2383208 rs10811661 rs10757283
rs564398 0.040 0.046 0.001rs2383208 0.040 0.924 0.221rs10811661 0.046 0.924 0.204rs10757283 0.001 0.221 0.204O
bserved in our
samples (n
=95)
Expe
cted
(EUR
popu
latio
n) by
LDpair
Supplemental Table 3. Expected LD (R2) (top chart) were calculated using the LDpair function on the NIH-‐supported LDlink website. The EUR population was selected since the majority of
our samples were Caucasian. The observed LD (R2) in our samples (bottom chart) were calculated using the cubeX web tool at http://www.oege.org/software/cubex/.
Page 46 of 51Diabetes

Supplemental Table 4: Multivariable linear models testing relationships between donor characteristics and gene expression
Sex Point SE p Point SE p Point SE p Point SE p Point SE pFemale v. Male 0.0869 0.1578 0.5819 0.9949 1.0280 0.3331 0.8965 0.8675 0.3014 0.0410 0.0426 0.3362 0.6714 1.0426 0.5196
Race/ethnicityBlack v. White -0.2308 0.2706 0.3937 -2.7309 11.7634 0.1215 -0.6622 1.4880 0.6563 0.0145 0.0731 0.8428 -2.8995 1.7884 0.1050Other v. White -0.0723 0.2016 0.7198 1.2057 1.3136 0.3587 0.0125 1.1084 0.9910 -0.0177 0.0545 0.7454 -0.0933 1.3322 0.4836
Age, per year 0.0186 0.0051 0.0003 -0.0641 0.0332 0.0535 0.1099 0.0280 <0.0001 0.0030 0.0014 0.0304 -0.0178 0.0337 0.5961
BMI, per kg/m2 -0.0085 0.0107 0.4281 0.0383 0.0697 0.5829 0.0212 0.0588 0.7181 -0.0003 0.0029 0.9063 -0.0108 0.0707 0.8788
Above model, integrating mRNA expression of other locus genesp14 - - - 2.8584 1.1627 0.0140 4.8178 0.3939 <0.0001 0.1584 0.0424 0.0002 -0.0666 1.2224 0.9566p15 0.0209 0.0085 0.0140 - - - -0.0892 0.0533 0.0944 0.0000 0.0039 0.9992 0.5201 0.0900 <0.0001p16 0.1269 0.0104 <0.0001 -0.3209 0.1918 0.0944 - - - 0.0033 0.0074 0.6577 0.1248 0.1980 0.5285
ANRIL 0.8076 0.2164 0.0002 0.0028 2.7079 0.9992 0.6317 1.4258 0.6577 - - - 3.8463 2.7320 0.1592MTAP -0.0005 0.0086 0.9566 0.5005 0.0866 <0.0001 0.0334 0.0529 0.5285 0.0053 0.0038 0.1592 - - -
Supplemental Table 4. Exploratory multivariable model testing for impact of donor characteristics (sex, race, age, BMI) on gene expression confirmed a positive relationship between donor age and islet abundance of p14, p15 (marginal association; inverse relationship), p16 and ANRIL. This model did not uncover an impact of sex, race or BMI on expression of these genes. Integrating expression of other locus genes into the model (lower rows) confirmed a significant positive correlation between p14-ANRIL, p14-p16 and p15-MTAP, as well as p14-p15 (weaker correlation). Point estimate is the difference in gene expression conferred by comparator condition to control condition, or the incremental increase in gene expression conferred by higher amount for linear input variables such as age, BMI and gene expression. SE, standard error of the point estimate. Other: combined all samples of non-white race, since sample size was too small to analyze for those other than black or white. BMI, body mass index.
p14 p15 p16 ANRIL MTAP
Page 47 of 51 Diabetes

Supplemental Table 5: List of SNPs in linkage disequilibrium with SNPs tested in this study
chr pos (hg38) LD(r²) LD(D') variant Ref Alt AFR freq AMR freq ASN freq EUR freq9 22133285 0.93 0.98 rs10965250 G A 0.05 0.14 0.44 0.169 22134069 0.93 0.98 rs10811660 G A 0.05 0.14 0.44 0.169 22134095 0.93 0.98 rs10811661 T C 0.05 0.14 0.44 0.169 22134254 0.93 0.97 rs10811662 G A 0.1 0.15 0.43 0.179 22132730 0.95 0.99 rs10965247 A G 0.05 0.14 0.44 0.169 22132879 0.96 0.98 rs10965248 T C 0.07 0.14 0.44 0.179 22132699 0.97 0.99 rs10965246 T C 0.07 0.14 0.44 0.179 22132077 1 1 rs2383208 A G 0.17 0.14 0.4 0.17
chr pos (hg38) LD(r²) LD(D') variant Ref Alt AFR freq AMR freq ASN freq EUR freq9 22136490 0.82 0.99 rs1333051 A T 0.08 0.09 0.15 0.149 22132077 0.93 0.98 rs2383208 A G 0.17 0.14 0.4 0.179 22132730 0.94 0.97 rs10965247 A G 0.05 0.14 0.44 0.169 22132699 0.96 0.99 rs10965246 T C 0.07 0.14 0.44 0.179 22132879 0.97 1 rs10965248 T C 0.07 0.14 0.44 0.179 22134254 0.99 1 rs10811662 G A 0.1 0.15 0.43 0.179 22133285 1 1 rs10965250 G A 0.05 0.14 0.44 0.169 22134069 1 1 rs10811660 G A 0.05 0.14 0.44 0.169 22134095 1 1 rs10811661 T C 0.05 0.14 0.44 0.16
chr pos (hg38) LD(r²) LD(D') variant Ref Alt AFR freq AMR freq ASN freq EUR freq9 22134303 0.91 0.99 rs7019437 C G 0.23 0.45 0.63 0.419 22134652 0.98 0.99 rs7019778 A C 0.23 0.46 0.64 0.439 22133646 0.99 1 rs10217762 T C 0.2 0.45 0.63 0.439 22133985 0.99 1 rs10757282 T C 0.23 0.45 0.64 0.439 22134173 1 1 rs10757283 C T 0.45 0.47 0.64 0.43
chr pos (hg38) LD(r²) LD(D') variant Ref Alt AFR freq AMR freq ASN freq EUR freq9 22015998 0.81 0.91 rs1101329 C T 0.01 0.21 0.1 0.419 22043613 0.81 0.99 rs1412830 C T 0.01 0.19 0.1 0.379 22021173 0.82 0.91 rs597816 T C 0.01 0.21 0.1 0.419 22007358 0.84 -‐0.99 rs3217977 CA C 0.96 0.75 0.9 0.559 22056360 0.84 -‐0.93 rs7866783 A G 0.98 0.79 0.9 0.599 22011643 0.85 0.98 rs573687 G A 0.01 0.19 0.1 0.389 21999329 0.86 0.95 rs2811713 G A 0.01 0.19 0.18 0.399 22009699 0.86 -‐1 rs2069418 G C 0.98 0.77 0.9 0.559 22049480 0.88 -‐0.94 rs200059580 A ACT 0.99 0.8 0.9 0.599 22015466 0.89 0.98 rs1101330 C A 0.02 0.19 0.1 0.399 22051671 0.89 -‐0.95 rs944801 G C 0.99 0.79 0.9 0.599 22052735 0.89 -‐0.95 rs6475604 T C 0.99 0.8 0.9 0.599 22054041 0.89 -‐0.95 rs7030641 C T 0.99 0.79 0.9 0.599 22003368 0.9 -‐0.99 rs1063192 G A 0.99 0.79 0.82 0.579 22019130 0.9 1 rs523096 A G 0.01 0.23 0.1 0.439 22019674 0.9 1 rs518394 G C 0.01 0.23 0.1 0.439 22022377 0.9 0.99 rs581876 C T 0.01 0.19 0.32 0.399 22026078 0.9 1 rs615552 T C 0.01 0.22 0.1 0.439 22045318 0.9 -‐0.96 rs1360589 C T 0.99 0.79 0.9 0.589 22040766 0.94 -‐0.98 rs1333037 C T 0.99 0.79 0.9 0.589 22036113 0.95 -‐0.99 rs1008878 G T 0.97 0.79 0.9 0.589 22036368 0.95 -‐0.99 rs1556515 C T 0.97 0.79 0.9 0.589 22031006 0.96 -‐1 rs7865618 G A 0.99 0.8 0.9 0.589 22033367 0.96 -‐1 rs2157719 C T 0.99 0.8 0.9 0.589 22028213 0.98 1 rs142048183 CAT C 0.01 0.2 0.1 0.419 22043927 0.98 0.99 rs1412829 A G 0.01 0.21 0.1 0.419 22026595 0.99 1 rs613312 G A 0.01 0.2 0.1 0.419 22026640 0.99 1 rs543830 A T 0.01 0.2 0.1 0.419 22027403 0.99 1 rs599452 G A 0.01 0.2 0.1 0.419 22029081 0.99 1 rs679038 G A 0.02 0.2 0.1 0.419 22032153 0.99 1 rs634537 T G 0.02 0.21 0.1 0.419 22029548 1 1 rs564398 T C 0.01 0.2 0.1 0.41
rs2383208
rs10811661
rs10757283
rs564398
Supplemental Table 5. Multiple SNPs are in linkage disequilibrium with the T2D-‐associated CDKN2A/B SNPs genotyped in this
study. Data in this table include all SNPs in HaploReg with LD(r2) > 0.80, from the EUR population data (chosen because the majority of our samples were Caucasian). T2D SNPs genotyped for this study are in red font. Allele frequencies in AFR, AMR, ASN, EUR are included for reference. Pos, position. Ref, reference allele. Alt, alternate allele.
Page 48 of 51Diabetes

Supplemental Table 6: Multivariable linear models testing for SNP impact on gene expression
point SE p point SE p point SE p point SE p point SE prs2383208
A/A v. G/A 0.1151 0.1679 0.4931 2.0529 1.7650 0.0565 0.4085 0.9206 0.6572 0.0635 0.0450 0.1585 -0.4870 1.1066 0.6599A/A v. G/G 0.2909 0.5227 0.5779 2.3846 3.3504 0.4766 3.1359 2.8652 0.2738 0.0817 0.1401 0.5598 -3.7195 -3.4444 0.2802
number of risk alleles 0.1234 0.1467 0.4003 1.8169 0.9414 0.0536 0.7264 0.8064 0.3677 0.0573 0.0394 0.1455 -0.8634 0.9693 0.3731
rs10811661T/T v. C/T 0.0473 0.1742 0.7862 2.1538 1.1138 0.0531 0.0192 0.9540 0.9839 0.0566 0.0467 0.2259 -0.5684 1.1453 0.6197T/T v. C/C 0.2730 0.5242 0.6025 2.4398 3.3510 0.4666 3.0297 2.8701 0.2911 0.0806 0.1406 0.5667 -3.7490 3.4458 0.2766
number of risk alleles 0.0729 0.1513 0.6297 1.8850 0.9679 0.0515 0.4498 0.8316 0.5886 0.0519 0.0406 0.2008 -0.9444 0.9963 0.3432
rs10757283T/T v. C/T -0.0318 0.2011 0.8742 1.9756 1.2644 0.1182 0.5558 1.1087 0.6162 -0.0274 0.0548 0.6178 2.5824 1.3227 0.0509T/T v. C/C -0.3073 0.2179 0.1586 -1.5806 1.3704 0.2488 -0.9627 1.2017 0.4231 -0.0600 0.0594 0.3127 1.8335 1.4336 0.2009
number of risk alleles -0.1637 0.1085 0.1316 -1.0181 0.7081 0.1505 -0.5668 0.6011 0.3458 -0.0302 0.0295 0.3058 0.7796 0.7215 0.2799
rs564398T/T v. C/T 0.0252 0.1692 0.8814 0.4790 1.0970 0.6624 0.1187 0.9339 0.8988 -0.0102 0.0459 0.8236 -0.1792 1.1199 0.8729T/T v. C/C 0.2564 0.2379 0.2810 2.2636 1.5427 0.1423 0.8902 1.3133 0.4979 -0.0336 0.0646 0.6032 1.2535 1.5749 0.4261
number of risk alleles 0.1049 0.1133 0.3547 0.9840 0.7350 0.1806 0.3712 0.6248 0.5525 -0.0153 0.0307 0.6183 0.4443 0.7510 0.5541
p14 p15 p16 ANRIL MTAP
Supplemental Table 6. Exploratory multivariable model testing for impact of CDKN2A/B locus T2D SNP genotype, incorporating donor characteristics (sex, race, age, BMI from Supplemental Table 2) on gene expression failed to reveal a significant impact of any genotype on any gene expression. Point estimate is the difference in gene expression relative to protective genotype (individual comparisons) or incremental gene expression for each additional risk allele at that SNP (number of risk alleles). SE, standard error of the point estimate. Risk allele is depicted in red for each SNP.
Page 49 of 51 Diabetes

Supplemental Table 7: Multivariable models testing determinants of insulin secretion indexmean difference in
insulin secretion index p-‐value
Female v. Male -‐0.25 ( -‐1.03 -‐ 0.53 ) 0.5318
age (per year) 0.00 ( -‐0.03 -‐ 0.03 ) 0.8951
African-‐American v. White 0.02 ( -‐1.09 -‐ 1.13 ) 0.974
BMI (per kg/m2) 0.08 ( 0.03 -‐ 0.14 ) 0.0029
Female v. Male -‐0.32 ( -‐1.05 -‐ 0.41 ) 0.3873
age (per year) 0.00 ( -‐0.03 -‐ 0.03 ) 0.9665
African-‐American v. White -‐0.10 ( -‐1.14 -‐ 0.95 ) 0.8588
BMI (per kg/m2) 0.10 ( 0.02 -‐ 0.17 ) 0.0171
Supplemental Table 7. Multivariable model testing for impact of donor characteristics (sex, age, race, BMI) on insulin secretion index confirmed a positive relationship between donor BMI and insulin secretion, but did not uncover an impact of sex, race or age. Integrating islet isolation center into the model using a generalized estimating equation (GEE) approach to adjust for potential clustering of insulin secretion measurements within islet isolation centers (lower rows) confirmed a significant positive correlation between BMI and insulin secretion index (0.10 units of insulin secretion index per BMI unit, p=0.0171). In a multivariable linear model adjusted for sex, age, ethnicity and BMI, mean insulin secretion values from center IV (see Supplemental figure 8) were higher than the mean values from the other centers, but after Bonferroni adjustment none of the between-center mean comparisons were statistically significant (not shown). BMI, body mass index.
95% confidence interval
Isolation center not
includ
ed in m
odel
Isolation center
includ
ed in m
odel
Page 50 of 51Diabetes

Supplemental Table 8: Multivariable models testing for impact of SNP genotype on insulin secretion index
mean difference in insulin secretion p-‐value
mean difference in insulin secretion p-‐value
mean difference in insulin secretion p-‐value
mean difference in insulin secretion p-‐value
-‐0.32 ( -‐1.16 -‐ 0.52 ) 0.4583 -‐0.25 ( -‐1.03 -‐ 0.53 ) 0.5316 -‐0.25 ( -‐1.03 -‐ 0.53 ) 0.5264 -‐0.24 ( -‐1.04 -‐ 0.55 ) 0.55030.00 ( -‐0.03 -‐ 0.03 ) 0.7976 0.00 ( -‐0.03 -‐ 0.03 ) 0.8704 0.00 ( -‐0.03 -‐ 0.03 ) 0.8717 0.00 ( -‐0.03 -‐ 0.03 ) 0.96850.05 ( -‐1.07 -‐ 1.17 ) 0.9330 0.07 ( -‐1.07 -‐ 1.21 ) 0.9031 0.04 ( -‐1.07 -‐ 1.16 ) 0.9387 0.19 ( -‐1.04 -‐ 1.43 ) 0.75730.08 ( 0.03 -‐ 0.14 ) 0.0030 0.08 ( 0.03 -‐ 0.14 ) 0.0041 0.08 ( 0.03 -‐ 0.14 ) 0.0039 0.09 ( 0.03 -‐ 0.14 ) 0.0021
no risk alleles v. two -‐0.03 ( -‐1.16 -‐ 1.11 ) 0.9655one risk allele v. two 0.17 ( -‐0.93 -‐ 1.27 ) 0.7661
one risk allele v. two 0.20 ( -‐0.74 -‐ 1.13 ) 0.6773
one risk allele v. two 0.18 ( -‐0.71 -‐ 1.07 ) 0.6961
no risk alleles v. two 0.02 ( -‐1.15 -‐ 1.19 ) 0.9692one risk allele v. two 0.45 ( -‐0.42 -‐ 1.32 ) 0.3123
Supplemental Table 8. In multivariable linear models adjusted for sex, age, race and BMI, and for potential clustering of insulin secretion index produced by different islet isolation centers (using a GEE approach), none of the four CDKN2A/B SNP genotypes had any significant association with insulin secretion index. These models confirmed the positive relationship between donor BMI and insulin secretion. BMI, body mass index.
rs10757283
rs10811661
rs2383208
rs564398
Female v. MaleAge (per year)African-‐American v. WhiteBMI (per kg/m2)
rs10757283 rs10811661 rs2383208 rs564398
95% confidence interval
95% confidence interval
95% confidence interval
95% confidence interval
Page 51 of 51 Diabetes