Embed Size (px)
Citation preview

CCF
Multiple Myeloma: An Overview of the Disease and
It’s Complications
Beth Faiman RN, MSN, CNP, AOCN
Cleveland Clinic Myeloma Program http://www.clevelandclinic.org/myeloma

CCF
Multiple Myeloma: Overview and Objectives
At the end of this presentation, the participant should be able to: Describe the Pathobiology of Multiple
Myeloma, Identify criteria for diagnosis of Multiple
Myeloma, Describe complications of Myeloma and
identify appropriate interventions, Discuss supportive care measures for patients
and families with Myeloma

CCF
Multiple Myeloma: It’s Like a Puzzle.
There are many different factors that go into the diagnosis and management of this disease
Interdisciplinary and aggressive symptom management for our patients is key to their success!

CCF
Integrated Multidisciplinary Clinical Research Group at the Cleveland Clinic Foundation
Phoresis Unit
RadiationOncology
Renal
Neurology
Cardiolology
Radiology &Neuro-Radiology
Orthopedics
Palliative Medicine
Multiple Myeloma

CCF
Did you know?
The first case described in 1844 – Sarah Newbury
Spontaneous fractures of her femurs, rt. humerus
Skeletal evidence of Myeloma obtained from Egyptian Mummies
1850 – Dr. Henry Bence Jones detected heat properties of urinary light chains
Kyle in Malpas (1998), Salmon (1995) and Hussein (1994)

CCF
Plasma Cell Disorders
Multiple Myeloma Other Disorders
Monoclonal gammopathy of undetermined significance (MGUS) Smoldering multiple myeloma (SMM) Solitary Plasmacytoma
Bone Extramedullary
Waldenström’s Macroglobulinemia Primary Amyloidosis (AL) Heavy chain disease POEMS syndrome Type I and II cryoglobulinemia

CCF
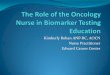
MGUS62% (803)
Myeloma15% (193)
Amyloidosis(AL) 10% (130)Amyloidosis
(AL) 10% (130)
Lymphoproliferative2.5% (31)
Lymphoproliferative2.5% (31)
SMM, 3.5% (44)SMM, 3.5% (44)
Solitary or extramedullary,1.5% (20)
Solitary or extramedullary,1.5% (20)
Macro, 3% (41)Macro, 3% (41)
Other, 2.5% (34)Other, 2.5% (34)
n=1296n=1296
Distribution of Monoclonal Gammopathies
Kyle RA and Rajkumar SV. Cecil Textbook of Medicine, 22nd Edition, 2004

CCF
Pathophysiology: Why do these cells turn malignant? No one Knows!
Chromosomal changes and abnormalities present in 80-90% patients on Fluorescent in Situ Hybridization (FISH) analysis
FISH – molecular cytogenetic technique describes genes, chromosomes and their aberrations
Salmon, S. E., ( Cancer Principals & Practice of Oncology (5th edition). Philadelphia: Lippincott-Raven, pp. 2344-2369.

CCF
Etiology/Risk factors
Radiation – chronic, low level Industrial – farming, herbicide exposure,
Agent Orange First degree relatives- Study by Brown et. al
(1999) provides data consistent with a familial risk, yet did not illustrate race-related differences
Cytogenetic abnormalities Are there more?
Brown, L.M, et. Al. (1999) Multiple myeloma and family history of cancer among blacks and whites in the U. S. Cancer, 85, 2385-2390.

CCF
Pathobiology/Pathogenesis
Cytokines have been implicated in myeloma cell growth, especially Interleukin-6 (IL-6)
In vivo and in vitro studies – a major autocrine and paracrine growth factor – bone marrow stromal cells compose the microenvironment for cells to secrete large amounts of IL-6
Elevated IL-6 levels linked to higher c-reactive protein levels, lower serum albumin levels and a poorer prognosis
Pelliniemi, T.T. (1995). Immunoreactive interleukin-6 and neopterin in patients with multiple myeloma. Blood, 85, 765-771.
Salmon, S. E., (1997). Plasma cell neoplasms. In V.T DeVita, S. Hellman, & S.A Rosenberg, (Eds). Cancer Principals & Practice of Oncology (5th edition). Philadelphia: Lippincott-Raven, pp. 2344-2369.

CCF
Pathophysiology: The Pluripotent Stem Cell
Myeloid stem cell
Lymphoid stem cell – the earliest cell – can self-replicate or differentiate into: T- Lymphocytes regulate immune
response, cell mediated immunity B- Lymphocytes – mature into plasma
cells, responsible for humoral immunity
Sheridan, C.A and Serrano, M. (2000). Multiple myelomaCancer nursing principles and practice (5th edition). Boston: Jones and Bartlett, pp. 1354-1370.

CCF
Pathophysiology: Remember the Immunoglobulins?
Five classes: IgG, IgA, IgM, IgD, IgE
Comprised of 4 polypeptide chains, 2 heavy and 2 light
Heavy: Take their name from their class: IgG = gamma, IgA = alpha, IgM = Mu.
Light: Kappa (κ) and Lambda (λ)
Sheridan, C.A and Serrano, M. (2000). Multiple myeloma.. Cancer nursing principles and practice (5th edition).
Boston: Jones and Bartlett, pp. 1354-1370.

CCF
Pathophysiology: So what happens?
Abnormal, overproduction of one immunoglobulin, it makes a “clone” of itself;
Referred to as the “M” protein (monoclonal), or “M- Spike”, normal plasma cells turn malignant
This “M” Protein is present in 80-90% patients These excess amounts of abnormal proteins
interfere with humoral immunity

CCF
Case Presentation
Mr. Peterson is a 62-year-old gentleman with a past medical history of hypertension, hyperlipidemia and osteoarthritis, who presented first to his Primary Care Physician (PCP) after experiencing severe 8/10 back pain while working in his yard. He had complained of intermittent lower back pain for “many years”, and a prior CT scan 8 months ago of the lumbar spine showed arthritic changes. He had also been complaining of some fatigue, and had noticed some new right hip pain, however this was attributed to increasing his work schedule, and “old age”.

CCF
Case Presentation
Where do you go from here?
What do you suspect to be part of the diagnosis?
What tests can you anticipate that the Practitioner would perform?

CCF
Laboratory Evaluation
General
Specific

CCF
Diagnostic Tests Blood and Urine Tests
Generic blood analysis Complete blood cell counts (CBC) Calcium, uric acid and creatinine Albumin, Beta-2-microglobulin, C-reactive protein, LDH
M proteins Blood—Serum protein electrophoresis and Immunofixation Urine protein electrophoresis and immunofixation Quantitative Immunoglobulins, serum free light chain assay
Radiological Skeletal survey; MRI/computerized tomography (CT)
scanning if needed Bone Marrow
Aspirate and biopsy with karyotyping and plasma cell labeling index

CCF
MULTIPLE MYELOMACBC
CBC Anemia (60%)
Cytokine mediated, or from Crowded Bone Marrow Blunted Erythropoeisis and shortened red cell survival Increased blood volume Chronic Renal Disease Macrocytic anemia
B12 and Folate levels Neuropathy Count recovery Quality of life
MDS Leukopenia Thrombocytopenia
Beckmann MJ et al Low Serum Vitamin B12 in Patients with Plasma Cell Myeloma Is Associated with True Functional Cobalamin Deficiency. American Journal of Clinical Pathology, 1995, 104:350
Baz R et al The Prevalence of Vitamin B-12 Deficiency in Plasma Cell Dyscrasias: A Retrospective Analysis. Blood 2002, 2368 a

CCF
B-12 deficiency in plasma cell dyscrasia: Monoclonal proteins like Vitamin B-12!
B-12 deficiency•B-12 < 200 pg/ml•B-12 >200<300pg/ml& Elevated MMA
Probable B-12 deficiency
•B-12 >200<300pg/ml& normal MMA•B-12 > 300pg/ml& elevated MMA
Baz et al; Cancer 101 (4):790-795, 2004.

CCF
B-12 deficiency in plasma cell dyscrasia
Myeloma Amyloid MGUS
B-12 Deficiency
14.2% 3.6% 5.8%
Probable B-12 deficiency
10.7% 7.1% 4.1%
Total 24.9% 10.7% 9.9%
N= 664 patients
Baz et al; Cancer 101 (4):790-795, 2004.

CCF
B-12 deficiency in plasma cell dyscrasia
15% of MM are B-12 deficient B-12 deficiency appears more prevalent in
IgA subtype 80% of B12 deficient patients have normal
MCV 35% of MM are B-12 or folate deficient B-12 influences
BM activity Neuropathy Endothelial health
Baz et al; Cancer 101 (4):790-795, 2004

CCF
Diagnostic Tests: Metabolic Panel
Hypercalcemia in 25% of the patients Hyperuricemia and Renal failure in 25-40%
Renal insufficiency – present in 20-25% patients at diagnosis – does not necessarily mean poor prognosis – present at one time or another in 50% Usually caused by Kappa or Lambda Light chains -
Some may have myeloma kidney or amyloidosis Albumin, Beta-2-microglobulin is now known to be an
EXCELLENT indicator of prognosis
Malpas, J. S. Et al. (1998). Myeloma Biology and Management: Second edition. New York: Oxford university press.
** Br.J.Haematol. 122 (3):441-450, 2003

CCF
New SWOG staging system **
Beta 2 M
Beta 2M< 5.5
Beta 2M> 5.5
Stage 1
Beta 2M<2.5
Beta 2M>2.5 < 5.5
Stage 2
Albumin> 3.0
Albumin< 3.0
Stage 3 Stage 4
** Br.J.Haematol. 122 (3):441-450, 2003

CCF
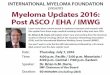
0%
20%
40%
60%
80%
100%
0 5 10 15 20Years After Registration
Stage IStage IIStage IIIStage IV
N197614447152
Deaths158563421149
Medianin Months
53402416
P < .0001
Southwest Oncology Group (SWOG)Stage (All Patients)
Overall Survival

CCF
Diagnostic Tests Blood and Urine Tests
Generic blood analysis Complete blood cell counts (CBC) Calcium, uric acid and creatinine Albumin, Beta-2-microglobulin, C-reactive protein, LDH
Monoclonal proteins Blood—Serum protein electrophoresis and Immunofixation Urine protein electrophoresis and immunofixation Quantitative Immunoglobulins, serum free light chain assay
Radiological Skeletal survey; MRI/computerized tomography (CT) scanning
if needed Bone Marrow
Aspirate and biopsy with karyotyping and plasma cell labeling index

CCF
MULTIPLE MYELOMADiagnosis SPEP/UPEP Immunofixation of the serum and the urine- This is
where heavy and light chains are determined Serum protein electrophoresis – presence of M-
protein - could miss 15% of the patients with MGUS Immunofixation- investigates abnormal bands Not performing a urine evaluation could miss 10% of
the patients with hypogammaglobulinemia where the M-Spike is ‘hiding’ under the gamma region and is undetected.
Malpas, J. S. Et al. (1998). Myeloma Biology and Management: Second edition. New York: Oxford university press.

CCF
Multiple Myeloma:Serum Protein Electrophoresis

CCF
Multiple Myeloma:Serum Protein Electrophoresis

CCF
Diagnostic Tests Blood and Urine Tests
Generic blood analysis Complete blood cell counts (CBC) Calcium, uric acid and creatinine Albumin, Beta-2-microglobulin, C-reactive protein, LDH
M proteins Blood—Serum protein electrophoresis and Immunofixation Urine protein electrophoresis and immunofixation Quantitative Immunoglobulins, serum free light chain assay
Radiological Skeletal survey; MRI/computerized tomography (CT)
scanning if needed Bone Marrow
Aspirate and biopsy with karyotyping and plasma cell labeling index

CCF
Multiple Myeloma, spine

CCF
Diagnostic Tests Blood and Urine Tests
Generic blood analysis Complete blood cell counts (CBC) Albumin, Beta-2-microglobulin, C-reactive protein, LDH Calcium, uric acid and creatinine
M proteins Blood—Serum protein electrophoresis and Immunofixation Urine protein electrophoresis and immunofixation Quantitative Immunoglobulins, serum free light chain assay
Radiological Skeletal survey; MRI/computerized tomography (CT)
scanning if needed Bone Marrow
Aspirate and biopsy with karyotyping and plasma cell labeling index
Kyle (2005). Overview of Multiple Myeloma. On-Line. Available: www.uptodateonline.com

CCF
MULTIPLE MYELOMA: Diagnosis
Bone marrow (BM) aspirate and biopsy Suggested at baseline, end of therapy Cytogenetics and plasma cell labeling index
are helpful with prognosis; especially at baseline, but aren’t essential
As Myeloma disease may be assessed with serum and urine testing, BM does not need to be repeated unless clinically indicated
Vescio, R. A & Berenson, J.R. (2000). Myeloma, macroglobulinemia and heavy chain disease. In C.M Haskell (Ed). Cancer Treatment, 5th edition. Philadelphia: Saunders, pp. 1503-1539.

CCF
Chromosomal Alterations in Myeloma Chromosome anomalies: incidence
Conventional G-banding: 30-50% of patients Interphase FISH: > 90% of cases SKY: ? ~ 100%
Specific chromosome changes IgH translocations (14q32): 60% of cases
11q13 (cyclin D1 locus, 15-20%) 4p16 (FGFR3, MMSET, 12%) 6p21 (cyclin D3) 16q23 (c-maf, 1%) 20q11 (mafB)
Others: 13 deletion (10-20% of patients using conventional cytogenetics and 50% using FISH), c-myc translocations, 17p-, hypodiploidy, Ras mutations
Kuehl WM. Nat Rev Cancer 2002;3:17,Tricot G. Brit J Hematol 2002;116:211,Facon T. Blood. 2001;97:1566Fonseca R. Blood. 2002;4:1417, Bergsagel L. Proc Natl Acad Sci USA. 1996;93:13931 Fonseca R. Cancer Res. 2004;64:1546

CCF
Plasma Cells Differentiated

CCF
Plasmablastic Morphology

CCF
Plasma Cells are Immune Cells
Plasma cells are “immune Cells”, and meant to survive.
While most regimens for treatment of Myeloma include Dexamethasone or Prednisone as the basis of therapy, the goal with treatment is to attack the bone marrow microenvironment in different ways.
Steroids interfere with IL-6, and induce apoptosis of the plasma cell

CCF
MM cells
Bone Marrow Stromal Cells
PBMC
IL-6
TNF
IL-1
IL-2
IFN
CD8+ T Cells
Bone Marrow Vessels
ICAM-1
VEGF
bFGF
NK Cells
Role of Bone Marrow Microenvironment
Hideshima et al. Blood 96: 2943, 2000Davies et al. Blood 98: 210, 2001Gupta et al. Leukemia 15: 1950, 2001
Mitsiades et al. Blood 99: 4525, 2002Lentzsch et al Cancer Res 62: 2300, 2002

CCF
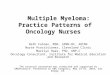
Angiogenesis in Myeloma
Normal Marrow Myeloma Marrow
CD 34 staining
Rajkumar SV 2004

CCF
Case Presentation I
Review of systems is positive for mild constipation, increased fatigue over the last few weeks, and shortness of breath on exertion. Pain is currently controlled with Tylenol #3 every 6 hrs as needed, prescribed by his PCP.
Physical Examination is normal, except he appears to be pale. The Musculoskeletal exam reveals point-tenderness to Thoracic spine, and bilateral hip joints.

CCF
Clinical Presentation
Subjective: Not all inclusive - everyone is different. General:
Back/bony pains- #1 presenting symptom Generalized weakness and fatigue Flu-like symptoms, nausea and vomiting
(electrolytes) Easy bruisability, recurrent infections (low plts) Neuro: Headaches, blurred vision, ataxia, vertigo 20% of patients will be diagnosed based on
routine laboratory examination, and are asymptomatic!

CCF
Clinical Presentation
Objective: Pallor Tenderness over affected bony areas Altered mental status Incontinence, loss of sphincter tone, lower
extremity weakness with pain may signify an Oncologic emergency – Spinal cord compression must be ruled out
Tachycardia/ arrhythmias due to electrolyte imbalance and associated renal impairment

CCF
Multiple Myeloma: Diagnosis According to Durie/Salmon Staging
Does Not: Take into account prognostic variables such as:
Inherent biology, cytogenetics, or proliferative rate of tumor
Chemosensitivity
Does provide us with a standardized tool for diagnosing and classifying Myeloma

CCF
Multiple Myeloma: Diagnosis According to Durie/Salmon Staging
* all of the following: *one or more of following:
Stage I Stage III Hgb >10g/dl <8.5 g/dl Serum Ca <12 mg/dl >12 g/dl Bone survey nml, solitary Lytic lesions
plasmacytoma Low M component High M component
A= Creat < 2.0 B = Creat > 2.0

CCF
Multiple Myeloma: International Staging System (ISS) for Prognosis
• B2M = Serum Beta-2 microglobulin• ALB = Serum Albumin in g/dL
Good and Poor risk groups: Age is the only significant risk
factor that impacts outcome Survival >5 years is
associated w/ age < 60 yrs Survival <2 yrs is correlated w/
age >60, plts <130,000 mm3, elevated LDH
Cytogenetics do influence outcome, however chromosome 13 deletion and presence of complex chromosome abnormalities do not add to the impact of age, B2M and ALB.
Stage 1 B2M < 3.5
ALB > 3.5
Stage 2 B2M < 3.5 ALB < 3.5
Stage 3 B2M > 5.5
Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol 2003; 121:749.

CCF
Classification Characteristics Management
Monoclonal gammopathy of undetermined significance (MGUS)
Serum M protein <3 g/dL
Bone marrow plasma cells <10% if done
Absence of anemia, renal failure, hypercalcemia, and lytic bone lesions
Observation, with treatment beginning at disease progression
Smoldering multiple myeloma (SMM)
Serum M protein <3 g/dLand/or
Bone marrow plasma cells <10% if done
Absence of anemia, renal failure, hypercalcemia, and lytic bone lesions
Observation, with treatment beginning at disease progression
Indolent multiple myeloma (IMM) Presence of serum/urine M protein
Bone marrow plasmacytosis
Mild anemia or few small lytic bone lesions
Absence of symptoms
Monitoring every 3 months, with treatment beginning at disease progression
Multiple myeloma (MM) Presence of serum/urine M protein
Bone marrow plasmacytosis
Anemia, renal failure, hypercalcemia, or lytic bone lesions
Patients with primary systematic amyloidosis and bone marrow plasma cells ≥30% are considered to have both MM and amyloidosis
Immediate treatment
Differential Diagnosis
Rajkumar SV. Leukemia 2001;15:1274
Br.J.Haematol. 121 (5):749-757, 2003

CCF
Kyle RA and Rajkumar SV. Immunol Rev. 2003;194:112-139
MGUS: Risk of Progression Based on Initial M-spike

CCF
Multiple Myeloma: Diagnosis
Plasmacytosis –Bone Marrow Biopsy Serum and urine electrophoresis Beta 2 Microglobulin Lytic lesions With or without renal failure – ANY SIGN OF
ORGAN DYSFUNCTION Especially if patient is symptomatic Treat ASAP

CCF
Smoldering (Asymptomatic) MM: Do we need to Treat?
Treatment Options
Observation Clinical Trial
Kyle & Greipp. N Engl J Med 1980; 302:1347-1349Hjorth et al. Eur J Haematol 1993; 50:95-102Witzig. Br J Haematol 1994; 87:266-72

CCF
Complications of Myeloma
Complications of Myeloma- Altered Bone Marrow Environment Infections RenalMetabolicNeurologic (Peripheral Neuropathy)Hyperviscosity SyndromeSkeletal

CCF
Newly diagnosed and relapsed patient with MM. What are our goals?
Administer antineoplastic therapy and management of complications Chemosensitive; response – 50-75%; survival 24-40
mos. Vs. no treatment, survival 12 months Address concerns at diagnosis
hair loss, loss of appetite, nausea and GI side effects and provide appropriate interventions. reassurance
Negotiate short term and long term goals important to maintaining an optimal level of functioning, optimal health, assist patients in achieving them

CCF
Complications of Myeloma- Altered Bone Marrow Environment
Bone marrow involvement – normocytic, normochromic anemia manifested by weakness is present 60% at diagnosis Iron, B12 and folate Vitamin Deficiencies
Concerns at diagnosis and through chemotherapy: Neutropenia/Granulocytopenia Thrombocytopenia

CCF
Complications of Myeloma- Altered Bone Marrow Environment
Educate regarding: Fatigue –Erythropoeitin/Darbopoeitin
Blood transfusions, negotiate activities, treatment
Safety precautions - thrombocytopenia Infections – Avoid people with colds, report to
practitioner if patient notes signs and symptoms of illness

CCF
Complications of Myeloma- Infections
Infections: The main cause of death for patients with hematologic malignancies.
Patients with MM have serious abnormalities of humoral immunity, consisting of impaired antibody formation after antigenic stimulation and depressed polyclonal immunoglobulin levels in serum
*Flu vaccine not always effective
Paradisi, F., et. Al. (2001). Infections in multiple myeloma. Infectious Disease Clinics of North America, 15(2).

CCF
Complications of Myeloma- Infections
Most infections are in urinary/respiratory tracts, with Streptococcus pneumoniae and Gram negative bacilli (GNB) the most likely causitive organisms.
These can occur at any time during therapy – whether in a plateau phase or during treatment
23-Valent Pneumococcal Vaccine is indicated
Paradisi, F., et. Al. (2001). Infections in multiple myeloma. Infectious Disease Clinics of North America, 15(2).

CCF
Complications of Myeloma- Infections
What can nurses do? Provide non-pharmacologic and
pharmacologic interventions related to related to disease prevention
Non-pharmacologic: Target to UTI/Respiratory, or if at Nadir, must be individualized to each patient- education is the key!
Pharmacologic: IVIG, antibiotic prophylaxis, vaccines, growth factors
Malpas, J. S. (1998). Myeloma Biology and Management: Second edition. New York: Oxford university press. Gautier, M. (1994). Multiple myeloma in the elderly. American Geriatric Society, 42, 653-664.

CCF
Complications of Myeloma- Renal
Renal insufficiency –present at one time or another in 50%
Cause: Dehydration or medications such as NSAIDs May be implicated, but more likely due to Kappa or Lambda Light chains
Some may have “myeloma kidney” as the kidney has trouble filtering the light chains and through the glomerulus and proximal tubule
Malpas, J. S. (1998). Myeloma Biology and Management: Second edition. New York: Oxford university press.

CCF
Complications of Myeloma- Renal
Nursing: Avoid nephrotoxic agents (IV dyes, non-steroidals (NSAIDS), aminoglycosides especially), monitor electrolytes, serum creatinine.
Educate patients on ways to maintain hydration, assess fluid status, urine character
Renal failure may be corrected if damaging cause is corrected (I.e hypercalcemia, hyperuricemia, dehydration, disease)
PLASMAPHERESIS
Malpas, J. S. (1998). Myeloma Biology and Management: Second edition. New York: Oxford university press.

CCF
Complications of Myeloma: Metabolic
Metabolic Syndromes:
hypercalcemia
hyperuricemia
Treat the suspected, underlying cause

CCF
Complications of Myeloma: Hyperviscosity Serum
Hyperviscosity syndrome – increased vascular sludging can occur in individuals with IgM, IgG, or IgA myeloma.
Uncommon, found in less than 5% patients Symptoms of easy fatigability, blurred vision,
drowsiness, headaches, confusion Treated with Plasmapheresis Nursing: Rare; but be aware!

CCF
Complications of Myeloma: Neurologic (Peripheral Neuropathy)
Due to Myeloma disease or Drug Induced Often Heavy chain IgM or related to amyloid if no
diabetes, heart disease or if never treated with chemotherapy
If previously treated with Vincristine, Thalidomide, or Bortezomib
Adjunct medicines (Neurontin, check for vitamin deficiency, LGlutamine) - Neurology referral
Nursing: emotional support, comfortable shoes, ongoing research

CCF
Complications of Myeloma- Skeletal
Bone Involvement = Pain!
70% an up to 100% in some series
Plasmacytoma with significant bone
destruction could be elicited clinically and
radiologically (MRI, PET scanning)
Analgesia- pain assessment, BTCP,
persistent and incident pain – discuss barriers
to good pain control Body JJ, et al. J Clin Oncol. 1998.

CCF
Complications of Myeloma- Skeletal
Radiology
Plain-film radiography- sensitivity is low, some use to screen - Bone survey more reliable
Magnetic resonance imaging – highly sensitive to bone metastases, spinal mets, soft tissue tumors
Computed tomography scan – confirm suspicious findings raised on bone survey
More to be addressed later!

CCF
Complications of Myeloma: Skeletal
Chemotherapy for disease progression, bisphosphonates
Analgesia - Avoid NSAID’s, but be liberal, closely obtaining pain scores and altering the dosages if necessary
Radiotherapy Only for identified lesions – relieves pain from local tumor in 60-80 % patients

CCF
Management of Myeloma: Supportive Care is Key! Multiple Myeloma is a complex disease! Although it comprises only a small
percentage of the population, it remains imperative that Nurses be aware of the disease, and management of symptoms
Be aware of local and national support groups for patients and their families to participate – provide education materials, handouts according to learning needs