Upload
robert-wintermeier
View
226
Download
0
Embed Size (px)
Citation preview
8/6/2019 Cato Simplified Analysis of ObamaCare
1/66
8/6/2019 Cato Simplified Analysis of ObamaCare
2/66
8/6/2019 Cato Simplified Analysis of ObamaCare
3/66
Copyright 2011 by the Cato Institute.
All rights reserved.
Cover design by Jon Meyers.
Printed in the United States of America.
Cato Institute
1000 Massachusetts Ave., N.W.
Washington, D.C., 20001
www.cato.org
8/6/2019 Cato Simplified Analysis of ObamaCare
4/66
Michael Tanner is a senior fellow with the Cato Institute and co-author of Healthy Competition: WhatsHolding Back Health Care and How to Free It.
It has been a year since President Obamashealth care reform bill was signed into law. ThePatient Protection and Affordable Care Act rep-
resents the most significant transformation ofthe American health care system since Medicareand Medicaid. It will fundamentally changenearly every aspect of health care, from insur-ance to the final delivery of care.
The length and complexity of the legislation,combined with a debate that often generatedmore heat than light, has led to massive confu-sion about the laws likely impact. But it is nowpossible to analyze what is and is not in it, whatit likely will and will not do. In particular, wenow know that
While the new law will increase the num-ber of Americans with insurance coverage,it falls significantly short of universal cov-erage. By 2019, roughly 21 million Ameri-cans will still be uninsured.
The legislation will cost far more than ad- vertised, more than $2.7 trillion over 10years of full implementation, and will addmore than $823 billion to the nationaldebt over the programs first 10 years.
Most American workers and businesseswill see little or no change in their sky-rocketing insurance costs, while millions
of others, including younger and health-ier workers and those who buy insuranceon their own through the nongroup mar-ket will actually see their premiums go upfaster as a result of this legislation.
The new law will increase taxes by morethan $569 billion between now and 2019,and the burdens it places on business willsignificantly reduce economic growthand employment.
While the law contains few direct provi-sions for rationing care, it nonetheless
sets the stage for government rationingand interference with how doctors prac-tice medicine.
Millions of Americans who are happywith their current health insurance willnot be able to keep it.
In short, the more we have learned aboutwhat is in this new law, the more it looks likebad news for American taxpayers, businesses,health care providers, and patients.
Executive Summary
8/6/2019 Cato Simplified Analysis of ObamaCare
5/66
8/6/2019 Cato Simplified Analysis of ObamaCare
6/66
Contents
Introduction 1
Part I: The Patient Protection and Affordable Care Act 3
Individual and Employer Mandates 3
Insurance Regulations 6
Subsidies 9
The Exchanges 11
Impact on Consumer-Directed Health Plans 13Medicare Cuts 15
Taxes 19
The CLASS Act 21
Growing the Nanny State 24
Other Provisions 24
Part II: Costs and Consequences 25
Expanded, Not Universal, Coverage 25
Increased Spending, Increased Debt 27
Higher Insurance Premiums 33
Conclusion 34
Appendix I: Timeline 36
Notes 39
8/6/2019 Cato Simplified Analysis of ObamaCare
7/66
8/6/2019 Cato Simplified Analysis of ObamaCare
8/66
The individualmandate isunprecedented iU.S. governance
1
Introduction
On March 21, 2010, in an extraordinarySunday night session, the House of Repre-
sentatives gave final approval to PresidentObamas long-sought health insurance planin a partisan 219212 vote.1 The bill had ear-lier passed the Senate on Christmas Eve 2009.Not a single Republican in either chambervoted for the bill. Four days later, the Senate,using a parliamentary tactic known as rec-onciliation to avoid a Republican filibuster,gave final approval to a package of changesdesigned to fix the bill.2
More than 2,500 pages and 500,000 wordslong,3 the Patient Protection and Affordable
Care Act represents the most significanttransformation of the American health caresystem since Medicare and Medicaid. It willfundamentally change nearly every aspect ofhealth care from insurance to the final deliv-ery of care.
The final legislation was in some ways,an improvement over earlier versions. It wasnot the single-payer system sought by manyliberals. Nor did it include the interim stepof a so-called public option that wouldlikely have led to a single-payer system in
the long run.4 The employer mandate is farless onerous than the 8 percent payroll taxonce championed by the House.5 And a pro-posed income tax surtax on the wealthy wasdropped.6 But that does not mean that thisis, as the president has claimed, a moder-ate bill.
It mandates that every American purchasea government-designed insurance package,while fundamentally reordering the insur-ance market and turning insurers into some-thing resembling public utilities, privately
owned while their operations are substan-tially regulated and circumscribed by Wash-ington. Insurance coverage will be extendedto millions more Americans as governmentsubsidies are expanded deep into the middleclass. Costs will be shifted between groups,though ultimately not reduced. And a newentitlement will be created, with the threat
of higher taxes and new debt for future gen-erations. In many ways, it has rewritten therelationship between the government andthe people, moving this country closer toEuropean-style social democracy.
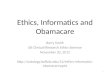
The legislation remains deeply unpopu-lar. Recent polls show substantial majoritiessupport repealing it. For example, a Rasmus-sen poll in late January of this year showed58 percent of likely voters supported repeal,with just 38 percent opposed. Similarly, amid-January Fox News poll showed regis-tered voters favoring repeal by 17 percent. Infact, with the exception of aNew York Times/CBS News poll of all Americans, recentpolling has consistently shown that mostvoters support repeal (Figure 1).
Republicans ran on a platform of repealor repeal and replace during the 2010 mid-term elections, and surveys suggest that op-position to the health care law was an impor-tant reason that they recaptured the Houseand gained six Senate seats. On health care,exit polls showed that at least half of voterswanted to repeal Obamacare. This repre-sented an almost unprecedented level of op-position for a major entitlement expansion.Given that exit polls have a history of over-sampling Democratic voters, an even better
measure might be an election-night Rasmus-sen telephone poll that found 59 percent ofvoters in favor of repeal.7 A Kaiser Founda-tion survey of voters found similar results: 56percent of midterm voters said they wantedto see some or all of the law repealed. 8An-other post-election survey found that 45 per-cent saw their vote as a specific message ofopposition to the health care bill.9
The new Republican majority in theHouse has already begun efforts to undothe health care law. On January 18, 2011, the
House voted 245 to 189 to repeal it.10 Whilerepeal is all but impossible in the short term,given Democratic control of the Senateand a presidential veto, Republicans plan acontinued assault on the law, ranging fromattempts to repeal some of the most un-popular provisions to plans for de-fundingimplementation.11
8/6/2019 Cato Simplified Analysis of ObamaCare
9/66
2
Meanwhile, outside of Washington, op-position remains active. Seven statesArizo-na, Idaho, Louisiana, Missouri, Oklahoma,Utah, and Virginiahave passed variationsof the Health Care Freedom Act prohibit-ing mandatory health insurance.12 Similarlegislation has been introduced in nearly allremaining states. State governments havealso been slow to cooperate with federal ef-
forts to implement the law. For example 23states refused to set up a high-risk pool inresponse to the law, and several states areconsidering a refusal to establish exchanges.
Numerous court challenges have alsobeen filed, raising questions about the con-stitutionality of various aspects of the leg-islation, especially its individual mandate.13
Plaintiffs include 28 states, as well as indi- viduals, business groups, and others.14 Todate, the outcome of those suits has beenmixed. In two minor lawsuits in Michiganand Virginia, courts have upheld the man-date.15 However, in the two most closelywatchedand extensively arguedcases, fed-eral judges struck down the mandate, andwhile the judge in the Virginia case allowed
other portions of the law to go forward, thejudge in Florida ruled that the lack of a sever-ability clause made the entire law unconsti-tutional.16 All the cases will be appealed andthe final decision will be made by the U.SSupreme Court.
It seems almost certain, therefore, thatthe debate over health care reform will be
Figure 1
Repeal of Health Care Law
Source: Real Clear Politics.
8/6/2019 Cato Simplified Analysis of ObamaCare
10/66
3
Simply havinginsurance is notnecessarilyenough to satisfthe mandate.
with us for some time to come.In the meantime, the legislation has
spawned enormous confusion. Insurancecompanies report people calling and asking,Where do we get the free Obamacare, and
how do I sign up for that?
17
But for goodor ill, those expecting immediate change arelikely to be disappointed. Most of the ma- jor provisions of the legislation are phasedin quite slowly. The most heavily debatedaspects, mandates, subsidies, and even mostof the insurance reforms dont begin until2014 or later.
Former House Speaker Nancy Pelosionce famously told us: We have to passthe bill so you can find out whats in it.18A year after passage, we are indeed discover-
ing what is in it. And what we are finding in-creasingly looks like it will leave Americansless healthy, less prosperous, and less free.
Part I:The Patient Protection and
Affordable Care Act
Individual andEmployer Mandates
Perhaps the single most important as-pect of the law is its individual mandate, alegal requirement that every American ob-tain health insurance coverage that meetsthe governments definition of minimumessential coverage. Those who dont receivesuch coverage through government pro-grams, their employer, or some other groupwould be required to purchase individualcoverage on their own.19
This individual mandate is unprecedent-
ed in U.S. governance. Back in 1993, whenthe Clinton health care plan was under con-sideration, the Congressional Budget Officenoted: A mandate requiring all individualsto purchase health insurance would be anunprecedented federal action. The govern-ment has never required people to buy anygood or service as a condition of lawful resi-
dence in the United States.20 Moreover, theindividual mandate raises serious constitu-tional questions.21 Even the CongressionalResearch Service was not able to conclude itwas constitutional!22
Under the law, beginning in 2014, thosewho failed to obtain insurance would besubject to a tax penalty. That penalty wouldbe quite mild at first, either $95 or one per-cent of annual income in 2014, whichever isgreater.23 But it ramps up quickly after that,the greater of $325 or 2 percent of annualincome in 2015, and the greater of $695 or2.5 percent of annual income after that. Incalculating the total penalty for an unin-sured family, children count as half an adult,which means that in 2016 an uninsured
family of four would face a minimum penal-ty of $2,085 ($695+$695+$347.50+$347.50),pro-rated on the basis of the number ofmonths that the person was uninsured overthe course of the year.24 Individuals will beexempt from the penalties if they earn lessthan an income threshold to be determinedby the secretary of Health and Human Ser-vices (but presumed to be roughly the pov-erty level), or if they are unable to obtaininsurance that costs less than 8 percent oftheir gross incomes.25
According to the CBO, roughly four mil-lion Americans will be hit by penalties in2016, with the penalties averaging slightlymore than $1,000.26 In fact, the federal gov-ernment expects to raise $17 billion frompenalties by 2019.27
Simply having insurance, however, is notnecessarily enough to satisfy the mandate.To qualify, insurance would have to meetcertain government-defined standards forminimum essential coverage. For example,in order to qualify, plans would be required
to cover ambulatory patient services, emer-gency services, hospitalization; maternityand newborn care, mental health and sub-stance abuse treatment; prescription drugs;rehabilitative and habitative services; labo-ratory services; preventative services; well-ness services; chronic disease management;pediatric services; and dental and vision care
8/6/2019 Cato Simplified Analysis of ObamaCare
11/66
4
More thantwo-thirds of
companies couldbe forced tochange their
current coverage.
for children.28 The secretary of HHS is giventhe authority to define the meaning of thoseterms and ultimately to set the minimumbenefits package.29 That process is ongoing,as an Institute of Medicine committee con-
siders whether to mandate the inclusion ofbenefits such as autism treatment or in vitrofertilization.30
In addition, plans must meet the new in-surance regulatory requirements below.
Unlike previous versions of the bill, how-ever, individuals who currently have insur-ance are grandfathered in, meaning they willnot have to change their current insuranceto meet the new minimum benefit.31 Theywill even be able add a spouse or childrento the plan without changing. While clearly
an improvement over earlier versions, thisdoes not necessarily mean that people willbe able to keep their current plan. In partic-ular, making changes to their current planwill end the plans grandfathered status, andwould require that individuals bring theirplan into compliance with the full range offederal mandates and requirements, even ifthose additional mandates make the newplan more expensive or include benefits thatthe individual does not want. What changesmeet the threshold to end grandfathered
status will be determined by the secretary ofHHS.32
Regardless of what federal regulatorseventually decide, the grandfathering ofcurrent plans may be short-lived. That is be-cause, aside from spouses and children, in-surers will not be able to continue enrollingnew customers in the noncomplying plans.As a result, insurers may stop offering theseplans. Over time, the vast majority of non-complying plans will simply fade away.
There has been some dispute over the
governments ability to enforce the man-date. While the law imposes penalties forfailure to comply and authorizes the IRSto collect those penalties (indeed, the IRSis expected to hire as many as 11,800 ad-ditional agents, auditors, and examinersfor enforcement)33 it does not contain anycriminal penalties for failing to comply, and
it forbids the use of liens or levies to collectthe penalties. However, the IRS is nothing ifnot resourceful. Already, IRS deputy com-missioner Steven Miller has said that theIRS may withhold tax refunds to individu-
als who fail to comply with the mandate.
34
And, because money is fungible, the IRcould simply apply part of your regular taxpayments toward the mandate penalty, andthen penalize you for failing to pay thoseregular taxes in full.
Interestingly, the law may have createdthe worst of both worlds, a mandate thatis costly and violates individual liberty, butone that is still weak enough that it may becheaper for many individuals to pay the pen-alty than to purchase insurance. As a result
it may fall far short of its proponents goalof bringing young and healthy individuals,who today frequently forego insurance, intothe insurance pool. The Congressional Bud-get Office, in fact, estimates that the penal-ties from individuals failing to comply withthe mandate will generate $17 billion be-tween 2014 and 2019.35 And according to aRAND Corporation study, those remaininguninsured after implementation are likelyto be younger and healthier as a group thantodays uninsured.36 Massachusettss expe-
rience with an individual mandate yielded just such a result. Slightly more than 35percent of that states remaining uninsuredare between the ages of 18 and 25, and morethan 60 percent are under the age of 35.37
Before the mandate, those between the agesof 18 and 25 made up roughly 30 percentof the uninsured, suggesting that the young(and presumably healthier) are less likely tocomply with the mandate.38
Indeed, evidence suggests that Massa-chusetts residents are increasingly gaming
the system: purchasing insurance when theyknow they are going to use health care ser-vices, then dropping it when they no longerneed it. In 2009 alone, 936 people signedup for coverage with Blue Cross and BlueShield of Massachusetts for three months orless and ran up claims of more than $1,000per month while in the plan. Their medical
8/6/2019 Cato Simplified Analysis of ObamaCare
12/66
5
Some of theregulatorychanges arelikely to have
unintendedconsequences.
spending while insured was more than fourtimes the average for consumers who buycoverage on their own and retain it in a nor-mal fashion.39 Given that the penalties un-der the Massachusetts mandate are actually
stronger than those under the Patient Pro-tection and Affordable Care Act, this doesnot bode well for the national plan.40
The law also contains an employer man-date. Beginning in 2014, if a company with50 or more full-time employees (or theequivalent41) does not provide health insur-ance to its workers, and as a result even asingle worker qualifies for a subsidy to helppurchase insurance through the exchange(see below), the company must pay a taxpenalty of $2,000 for every person they em-
ploy full time (minus 30 workers). Thus acompany employing 100 workers would beassessed a penalty of $2,000 x 70 workers.42CBO estimates that those penalties will costbusinesses $52 billion from 2014 to 2019.43
Even more than the individual mandate,the employer mandate may affect peoplewho already have health insurance coverage.In part, this would be because far more peo-ple receive their insurance through work.But, in addition, HHS has released rules sug-gesting that if companies make any signifi-
cant changes to their current coverage theywill no longer be grandfathered under theemployer mandate, meaning that they willhave to bring their plan into full compli-ance with all the new federal requirements.Among the changes that would end grand-fathered protection would be a change ininsurance carrier, changes in or the elimi-nation of any currently covered benefit, de-creases in the employers contribution rate,increases in annual payment limits, and in-creases in employee cost-sharing, including
any increase in deductibles or copayments.44 An internal study by HHS estimates thatmore than two-thirds of companies couldbe forced to change their current coverage.For small businesses, the total could reach80 percent.45
Even offering the correct benefits will notnecessarily exempt companies from penal-
ties. Companies that offer coverage, butwhich have employees who still qualify for asubsidy because the employees contributionis deemed unaffordable (that is, it exceeds 8percent of an employees income), will still
have to pay a penalty of the lesser of $3,000per employee receiving a subsidy or $2,000per worker whether they are receiving sub-sidy or not. A survey by the employer ben-efits firm, Mercer, suggests that as many asone-third of employers could face penaltiesfor failing to meet the affordable insurancerequirement.46
Such a mandate is simply a disguised taxon employment. As Princeton Universityprofessor Uwe Reinhardt, the dean of healthcare economists, points out, [Just because]
the fiscal flows triggered by the mandatewould not flow directly through the publicbudgets does not detract from the measuresstatus of abona fide tax.47
And while it might be politically appeal-ing to claim that business will bear the newtax burden, nearly all economists see it quitedifferently. The amount of compensationa worker receives is a function of his or herproductivity. The employer is generally in-different to the composition of that com-pensation. It can be in the form of wages,
benefits, or taxes. What really matters is thetotal cost of hiring that worker. Mandatingan increase in the cost of hiring a worker byadding a new payroll tax does nothing to in-crease that workers productivity. Employerswill therefore seek ways to offset the addedcost by raising prices (the least likely solu-tion in a competitive market), lowering wag-es, reducing future wage increases, reducingother benefits (such as pensions), cuttingback on hiring, laying off current workers,shifting workers from full-time to part-time,
or outsourcing.48 In fact, a survey by TowersWatson shows that employers are preparingto take exactly those steps.49
And, as with the individual mandate, thepenalty may be low enough that many busi-nesses may find it less costly to pay than toplay.50 As an internal document preparedfor Verizon explains Even though the pro-
8/6/2019 Cato Simplified Analysis of ObamaCare
13/66
6
Such a rigid capmay create a
number ofunintended
consequences.
posed assessments [on companies that donot provide health care] are material, theyare modest when compared to the averagecost of health care.51 In fact, CBO estimatesthat at least 10 to 12 million workers could
lose their current employer-provided healthinsurance.52 Approximately 8 to 9 millioncould end up on Medicaid, with the restpurchasing subsidized coverage through theexchanges (see below).53 But this may vastlyunderestimate the actual number of work-ers who could be dumped from their currentcoverage, as several large U.S. corporationshave indicated that they may drop their cur-rent coverage.54
Insurance RegulationsSince the advent of the McCarran-
Fergusson Act in 1945, health insurance hasbeen primarily regulated at the state level.55The Patient Protection and Affordable CareAct imposes a host of new federal insuranceregulations that will significantly changethe way the health insurance industry doesbusiness. Some of these regulatory changesare likely to be among the laws most initial-ly popular provisions. But many are likely to
have unintended consequences.Perhaps the most frequently discussed
regulatory measure is the ban on insurersdenying coverage because of preexisting con-ditions. Throughout the health care debate,proponents of reform highlighted stories ofpeople with terrible illnesses who were un-able to get insurance coverage.56
Under the Patient Protection and Afford-able Care Act insurers would be prohibitedfrom making any underwriting decisionsbased on health status, mental or physical
medical conditions, claims experience, med-ical history, genetic information, disability,other evidence of insurability, or other fac-tors to be determined later by the secretaryof HHS.57
Specifically, the law would require insur-ers to accept every employer and individual. . . that applies for such coverage.58 Insur-
ers are also forbidden to cancel insurance ifa policyholder becomes sick.59 Finally, therewill be limits on the ability of insurers to vary premiums on the basis of an individuals health. That is, insurers must charge
the same premium for someone who is sickas for someone who is in perfect health.60
Insurers may consider age in setting premi-ums, but those premiums cannot be morethan three times higher for their oldest thantheir youngest customers.61 Smokers mayalso be charged up to 50 percent more thannonsmokers.62 The only other factors thatinsurers may consider in setting premiumsare geographic location and whether thepolicy is for an individual or a family.63
It is also worth noting that, while a ban
on preexisting conditions for children start-ed last year, the rules will not apply to adultsuntil 2014.64 Until then, adults with preex-isting conditions will be eligible to partici-pate in federally sponsored high-risk pools.65
The high-risk pools will contract with pri-vate, nonprofit insurers for plans that mustcover at least 65 percent of the costs of par-ticipants care. Out-of-pocket costs would becapped at $5,950 a year for an individual or$11,900 for a family. The risk pools were sup-posed to be in place no later than the end of
June 2010, but there have been numerous de-lays.66 As many as 23 states have declined toestablish the pools, forcing the federal gov-ernment to set them up in those states.
So far, very few people have enrolled inthe risk polls. In fact, by the end of 2010,only 8,011 people had signed up nation-wide.67 One reason may be that premiumswithin the pools are relatively high. For ex-ample, the premium for a non-smoking 4554 year old ranges from $330 per month inHawaii to $729 per month in North Caroli-
na.68 However, a bigger problem may be thestructure of the program, which is incom-patible with existing state high-risk pools.69
Individuals currently insured through theirstate risk pool must drop out of that pool,remain uninsured for six months, then jointhe federal pool. Its not surprising that thathas not been a popular option.
8/6/2019 Cato Simplified Analysis of ObamaCare
14/66
7
While the ban on medical underwritingmay make health insurance more availableand affordable for those with preexistingconditions and reduce premiums for olderand sicker individuals, it will increase premi-ums for younger and healthier individuals.The RAND Corporation recently conducteda study for the Associated Press concluding
that premiums for the young would riseabout 17 percent, roughly $500 per year, asa result of the new law.70 Other studies sug-gest that the increase could be much higher.For example, a study by the independent ac-tuarial firm Millman, Inc., concluded thatpremiums for young men could increase by10 to as much as 30 percent.71 The Council
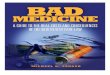
for Affordable Health Insurance suggeststhat premiums for some individuals couldincrease by 75 to 95 percent in states thatdo not now have guaranteed issue or com-munity rating requirements (see Figure 2).72
Moreover, the ban may not be as effectiveas proponents hope in making insuranceavailable to those with preexisting condi-
tions. Insurance companies have a variety ofmechanisms for evading such restrictions. Asimple example is for insurers to focus theiradvertising on young healthy people, orthey can locate their offices on the top floorof a building with no elevator or providefree health club memberships while failingto include any oncologists in their network.
Figure 2
Possible Premium Increases for Young Workers Under PPACA
Source: RAND and Millman studies cited in Carla Johnson, Health Premiums Could Rise 17 Percent for Young Adults, Associated Press, March 2
2010; and Brian McManus, Universal Coverage + Guaranteed Issue + Modified Community Rating = 95% Rate Increase, Council for Affordable HeaInsurance, August 2009.
8/6/2019 Cato Simplified Analysis of ObamaCare
15/66
8
Tennesseesexperience with
Tenncareprovides a
cautionary tale.
Even the ban on excluding preexistingconditions for children has already had un-intended consequences. Several large insur-ers have stopped offering child only insur-ance plans, thereby depriving thousands of
parents of a low-cost insurance option.
73
In a similar vein, the law also bans re-scissions, or the practice of insurers drop-ping coverage for individuals who becomesick.74 Under existing practices, insurerssometimes retroactively review an individu-als initial insurance application and cancelthe policy if the application is found to beinaccurate.75 Because insurers would under-take such a review only when individualssubmitted large claims (and were thereforesick) and the grounds for rescission often
appeared to be very minor discrepancies, thepractice was widely condemned by the billsproponents. Under the legislation, insurerscould cancel coverage only in cases of fraudor intentional misrepresentation of mate-rial fact. While likely to be very popular, thisprovision may have little practical impact. According to a congressional report, thereare actually fewer than 5,000 rescissions peryear, and at least some of those were cases ofactual fraud where cancellations would stillbe allowed under this legislation.76
A second new insurance regulation wouldprohibit insurers from imposing lifetimelimits on benefit payouts.77 Although pop-ular, this provision is also likely to have lessimpact than most people believe. Roughly40 percent of insured Americans already hadpolicies with no lifetime caps. For those pol-icies that did have a cap on lifetime benefits,that cap was usually somewhere between$2.5 and 5 million, with many running ashigh as $8 million, amounts that very fewpeople ever reached.78 Still, some individu-
als with chronic or catastrophic conditionswill undoubtedly benefit from this provi-sion, although there are no solid estimateson how many. Removing lifetime caps willmost likely increase the cost of reinsuringpolicies, leading ultimately to higher premi-ums, but most insurers predict the increasewill be modest.79
This regulation, however, may have amuch bigger impact on more than onemillion part-time, seasonal, and low-wageworkers who currently take advantage oflow-cost, limited benefit plans. Those plans,
known in the industry as mini-med plans,have inexpensive premiums because theycan, among other things, restrict the num-ber of covered doctor visits or impose amaximum on insurance payouts in a yearThey are particularly popular with low-wageworkers in the restaurant and retail indus-tries. The prohibition on lifetime caps couldall but eliminate these plans, meaning thatas many as a million workers could losethe coverage they have now. Some could beforced into Medicaid, while others would be
forced to purchase much more expensive in-surance than they have today.80
In fact, the administration has alreadybeen forced to issue more than 728 waiversas of February 2011, allowing some employ-ers to continue offering mini-med plans.81
These include large employers such as Mc-Donalds, which had threatened to dropcoverage for most of its workforce in theabsence of an exemption.82 Several unionsincluding at least three locals of the ServiceEmployees International union, 17 Team-
sters chapters, 28 affiliates of the UnitedFood and Commercial Workers Union, sev-eral locals of the Communications Workersof America, and chapters of the AmericanFederation of Teachers have received waiv-ers as well.83 However, at least 50 companieshave had their requests for waivers denied(The administration will not divulge thenames of those companies.)84
The law also places limits on deductiblesEmployer plans may not have an annual de-ductible higher than $2,000. Family policies
are limited to deductibles of $4,000 or less.85
There is an exception, however, for individu-als under the age of 30, who will be allowedto purchase a catastrophic policy with a de-ductible of $4,000 for an individual, $8,000for a family.86
In addition, the law requires insurers tomaintain a medical loss-ration (that is the
8/6/2019 Cato Simplified Analysis of ObamaCare
16/66
9
The phase-out othese benefitscreates a highmarginal tax
penalty.
ratio of benefits paid to premiums collect-ed) of at least 85 percent for large groupsand 80 percent for small groups and indi-viduals.87 Insurance companies that pay outbenefits less than the required proportion of
the premium, must rebate the difference topolicy holders on an annual basis beginningin 2011.88 This requirement is intended toforce insurers to become more efficient byreducing the amount of premiums that canbe used for administrative expenses (andinsurer profits).89 However, while there isundoubtedly waste in insurance overhead,such a rigid cap may create a number of un-intended consequences. Insurance overheadincludes many useful services and programs.These include efforts to monitor patient
care to ensure that those with chronic medi-cal conditions are getting appropriate care,exactly the type of program that PresidentObama says he wants to encourage, and ef-forts to combat fraud and abuse. Those pro-grams can actually reduce overall costs andresult in lower insurance premiums. Forc-ing insurers to abandon those efforts couldhave the perverse effect of increasing coststo consumers.90
Finally, the legislation would also allowparents to keep their dependent children
on their policies until the child reaches age27. This too is generally considered a popu-lar aspect of the new law, but it does comewith a price tag. HHS estimates that everydependent added to a policy will increasepremiums by $3,380 per year.91 And employ-ers have indicated that they are reluctant toadd dependent children to the coverage theyprovide, even if insurers offer it, meaningparents will have to pay most or all of theadditional cost.92
The new insurance regulations may re-
sult in many insurers withdrawing fromtheir less profitable markets, leaving manyconsumers with few insurance choices. Al-ready, Principal Financial has stopped sell-ing health insurance, which has resulted incoverage being dropped for some 840,000people.93 And Aetna has announced that itis pulling out of the individual market in
Colorado.94 Perversely, the Patient Protec-tion and Affordable Care Act could reducecompetition in the insurance market.
Overall, most of the laws insurance re-forms have been among the more politically
popular aspects of the new law, but they arelikely to have only a minor impact and may,indeed, have a number of unintended con-sequences.
Subsidies
The number one reason that people givefor not purchasing insurance is that theycannot afford it.95 Therefore, the legislationsprincipal mechanism for expanding cover-
age (aside from the individual and employermandates) is to pay for it, either throughgovernment-run programs such as Medicaidand the State Childrens Health InsuranceProgram (SCHIP) or through subsidizingthe purchase of private health insurance.
Starting this year, states are required toexpand their Medicaid programs to coverall U.S. citizens with incomes below 133 per-cent of the poverty level ($14,404 for an indi-vidual; $29,327 for a family of four; higher inAlaska, Hawaii, and the District of Colum-
bia).96 Previously, only pregnant women andchildren under age six were covered to 133percent of the poverty level. Children 618were required to be covered up to 100 per-cent of the poverty level, though 18 statescovered children from families with higherincomes. In fact a few states covered preg-nant women and children under age 1 up to185 percent of the poverty level.97 Most otherlow-income children were covered throughSCHIP (up to 250 percent of poverty).
Thus, the primary result of the laws Med-
icaid expansion would be to extend coverageto the parents in low-income families and tochildless adults. In particular, single, child-less men will now be eligible for Medicaid.This raises potentially serious concerns. Low-income, childless, adult men in particularare a high-risk, high-cost health care popula-tion. That means costs may run higher than
8/6/2019 Cato Simplified Analysis of ObamaCare
17/66
10
All together thelaw represents amassive increase
in the welfarestate.
expected, a problem that may be exacerbatedby adverse selection within that population.
Tennessees experience with TennCareprovides a cautionary tale. In 1994, Tennes-see expanded Medicaid eligibility to unin-
sured citizens who werent able to get healthinsurance through their employers or exist-ing government programs and to citizenswho were uninsurable because of pre-existingconditions. Over the next 10 years, Medicaidcosts in the other 49 states rose by 71 per-cent. In Tennessee they increased by an over-whelming 149 percent.98 Despite this mas-sive increase in spending, health outcomesdid not improve. Even the states Democraticgovernor Phil Bredesen called the program adisaster.99 Similar problems with the Patient
Protection and Affordable Care Acts Med-icaid expansion could dramatically drive upcosts for both the federal and state govern-ments.
Initially, the federal government will pay100 percent of the cost for new enrollees.However, beginning in 2017, states will berequired to pick up a portion of the cost. Theimpact on state budgets would very dramat-ically. Those states like California, whoseeligibility standards already are close to thenew federal requirements and are therefore
unlikely to see large enrollment increases,will see only modest cost increases. In thecase of California, Medicaid costs would goup only about 4.5 percentage points higherthan they would have risen in the absenceof PPACAs requirements, or about $11.7billion between 2014 and 2023. But otherstates would see far bigger increases. Texas,for example, would receive the largest per-centage hit, being forced to absorb an in-crease 20 percentage points higher than itotherwise would have, a cost of $30.5 billion
from 2014 to 2023. New York would see thelargest cost increase in dollars, $65.5 billionover those 10 years, largely because of its al-ready high cost per enrollee.100 It is impor-tant to remember that these are costs overand above already rising Medicaid costs.
Arizona has already requested a waiverexempting the states Medicaid program
from the laws maintenance of effort re-quirement. That provision prohibits statesfrom changing their current eligibility lev-els, but Arizona is seeking to drop 280,000people from the program in order to help
close the states budget deficit. Several otherstates may follow suit.101
SCHIP would be continued until Sep-tember 30, 2019. Between 2014 and 2019,the federal government will increase its con-tribution to the program, raising the federalmatch rate by 23 percentage points (subjectto a 100 percent cap).102 States must main-tain their current income eligibility levelsfor the program.103
Individuals with incomes too high toqualify for Medicaid but below 400 percent
of the poverty level ($88,000 per year) will beeligible for subsidies to assist their purchaseof private health insurance. These subsidieswhich will be provided in the form of refund-able tax credits, are expected to total morethan $457 billion between 2014, when indi-viduals are first eligible for the payments, and2020.104
There are actually two separate credits de-signed to work more or less in conjunctionwith one another. The first is a premium taxcredit.105 The credit is calculated on a slid-
ing scale according to income in such a wayas to limit the total proportion of incomethat an individual would have to pay for in-surance.106 Thus, individuals with incomesbetween 133 and 200 percent of the povertylevel will receive a credit covering the costof premiums up to four percent of their in-come, while those earning 300400 percentof the poverty level will receive a credit forcosts in excess of 9.5 percent of their income
The second credit, a cost-sharing creditprovides a subsidy for a proportion of out-
of-pocket costs, such as deductibles and co-payments. Those subsidies are also provid-ed on a sliding income-based scale, so thatthose with incomes below 150 percent ofthe poverty level receive a credit that effec-tively reduces their maximum out-of-pocketcosts to 6 percent of a plans actuarial valuewhile those with incomes between 250 and
8/6/2019 Cato Simplified Analysis of ObamaCare
18/66
11
Plans offeredthrough theexchange mustmeet the federalrequirements fominimumbenefits.
400 percent of the poverty level would, afterreceiving the credit, have maximum out-of-pocket costs of no more than 30 percent ofa plans actuarial value.
As with many tax credits, the phase-out
of these benefits creates a high marginal taxpenalty as wages increase. In some cases,workers who increase their wages could ac-tually see their after-tax income decline asthe subsidies are reduced. This creates a per-verse set of incentives that can act as a pov-erty trap for low-wage workers.107
In addition to the individual subsidies,there will also be new government subsidiesfor some small businesses. Beginning thisyear, businesses with fewer than 25 employ-ees and average wages below $50,000 are eli-
gible for a tax credit to help offset the costof providing insurance to their workers.108To be eligible, employers must provide in-surance to all full-time workers and pay atleast 50 percent of the cost of that coverage.The actual amount of the credit dependson the size of the employer and the aver-age worker salary. Between 2011 and 2014,when the exchanges begin operation (seebelow), employers with 10 or fewer workersand an average wage below $25,000 per yearwould be eligible for a credit equal to 35
percent of the employers contribution. Fora typical family policy, the credit would bearound $2,000. The credit gradually phasesout as the size of the company and averagewages increase.
Once the exchanges are operational after2014, businesses with 10 or fewer employeesand average wages below $25,000 that pur-chase their insurance through the exchangewill be eligible for a credit of up to 50 per-cent of the employers contribution towarda workers insurance. Again, the credit is
phased out as the size of the company andaverage wages increase. The credit can onlybe claimed for two years.
In addition, the legislation establishes a$5 billion temporary reinsurance programfor employers who provide health insurancecoverage for retirees over age 55 who are notyet eligible for Medicare.109 The program
will reimburse insurers for 80 percent of re-tiree claims between $15,000 and $90,000.110Insurers are required to pass those savingson to employers through lower premiums,though how that will be enforced remains a
question.
111
The law also increases funding for com-munity health centers by $11 billion.112 Ap-proximately $1.5 billion would be used forthe construction of new health centers ininner-city or rural low-income communities,with the remainder designed to subsidizeoperations for existing centers. Communityhealth centers are expected to treat nearly 40million patients by 2015, nearly double to-days utilization.113
All together, this law represents a massive
increase in the welfare state, adding millionsof Americans to the roll of those dependent,at least to some extent, on government lar-gess. Yet for all the new spending, the Pa-tient Protection and Affordable Care Actfalls short of its goal of achieving universalcoverage (see below).
The Exchanges
Perhaps the most fundamental reorder-
ing of the current insurance market is thecreation of exchanges in each state. EzraKlein, one of the bills most prominent lib-eral supporters, maintains that that the ex-changes are the most important element inthe plan.114 The exchanges would functionas a clearinghouse, a sort of wholesaler ormiddleman, matching customers with pro-viders and products.
Exchanges would also allow individu-als and workers in small companies to takeadvantage of the economies of scale, both in
terms of administration and risk pooling,which are currently enjoyed by large employ-ers. The larger risk pools should theoreticallyreduce premiums, as would the exchangesability to use market share to bargain downthe prices of services.115
However, one should be skeptical of claimsthat the exchange will reduce premiums. In
8/6/2019 Cato Simplified Analysis of ObamaCare
19/66
12
President Obamahas always
been hostileto consumer-
directedhealth care.
Massachusetts, supporters of the Connec-tor claimed that it would reduce premiumsfor individual insurance policies by 25 to 40percent.116 Instead, premiums for policiessold through the Connector have been rising,
up 11 percent for the lowest cost plans sincethe program began.117
Beginning in 2014, one or more exchang-es would be set up by each state and largelyoperated according to rules developed bythat state. States would also have the optionof joining with other states and creating re-gional exchanges. If a state refuses to createan exchange, the federal government is em-powered to set one up within that state.118States are given considerable discretion overhow the exchanges would operate, but some
of the federal requirements are significant.Exchanges may be either a governmental
agency or a private nonprofit entity.119 Andstates would have the option of either main-taining separate insurance pools for the indi- vidual and small-group markets or of com-bining them into a single pool.120 The poolswould also include individual or small-grouppolicies sold outside the exchange.121 Existingplans could not be included in those pools,however.122
Initially, only businesses with fewer than 50
employees, uninsured individuals, or the self-employed may purchase insurance throughthe exchange. Members of Congress andsenior congressional staff are also requiredto purchase their insurance through the ex-change.123 However, beginning in 2017, stateshave the option of opening the exchange tolarge employers.124
Insurance plans offered for sale withinthe exchanges would be grouped into fourcategories based on actuarial value: bronze,the lowest cost plans, providing 60 percent
of the actuarial value of a standard plan asdefined by the secretary of HHS; silver, pro-viding 70 percent of the actuarial value; gold,providing 80 percent of the actuarial value;and platinum, providing 90 percent of theactuarial value.125 In addition, exchangesmay offer a special catastrophic plan to in-dividuals who are under age 30 or who have
incomes low enough to exempt them fromthe individual mandate.126
For all categories of plans, out-of-pocketexpenses would be limited according to theincome of the purchaser. For individuals
and families with incomes above 400 percentof the poverty level, out-of-pocket expenseswould be limited to $5,950 for individualsand $11,900 for families, approximately thecurrent limits for a health savings account(HSA). Those limits would also apply tothose who purchase the catastrophic planIndividuals with incomes between 300 and400 percent of the poverty level would haveout-of-pocket expenses limited to two-thirdsof the HSA limits ($3,987/individual and$7,973/family); 200 to 300 percent of poverty
would have out-of-pocket expenses limited toone-half of the HSA limits ($2,975/individualand $5,950/family); and those with incomesbelow 200 percent of poverty would have out-of-pocket expenses limited to one-third of theHSA limits ($1,983 per individual and $3,967per family).127 The reductions in out-of-pock-et expenses would occur within the plan insuch a way as to not change their overall ac-tuarial value.
CBO estimates that premiums for bronzeplans would probably average between $4,500
and $5,000 for an individual and between$12,000 and $12,500 for family policies.128
The more inclusive policies would have cor-respondingly higher premiums.
Plans offered through the exchange mustmeet the federal requirements for minimumbenefits. State mandated benefits are notpreempted, meaning that states may contin-ue to impose additional mandates (thoughstates must pay for the cost of the addition-al mandates in subsidized policies.)129
In addition to the state insurance plans,
the legislation authorizes the federal Officeof Personnel Management to contract withprivate insurers to ensure that each stateexchange offers at least two multi-state in-surance plans. These multi-state plans aresupposed to resemble the Federal EmployeeHealth Benefit Plan, but will operate separate-ly from the FEHBP and will have a separate
8/6/2019 Cato Simplified Analysis of ObamaCare
20/66
13
The fate of HSAis thereforedependent on aregulatory rulin
by the Secretaryof HHS.
risk pool.130 The multi-state plans must meetthe licensing and regulatory requirements ofeach state in which they are offered.131 At leastone plan must not include abortion cover-age, and one must be offered by a nonprofit
insurer. The legislation also provides start-upfunds for states to establish health insurancecooperatives, which may participate in thestates exchange.132
Exactly how significant the exchanges willprove to be remains to be seen. At the veryleast exchanges will change the way individu-als and small businesses purchase healthinsurance. However, if expanded to includelarge businesses or their employees, exchang-es represent a potential framework for a farmore extensive government intervention in
the insurance market.
Impact on Consumer-Directed Health Plans
The health care bill reverses much of
the progress in recent years toward moreconsumer-directed health care.
Consumer-directed health care is a broadterm used to describe a variety of insurancearrangements, including health savings ac-
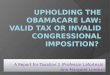
counts, flexible spending accounts (FSAs),and health reimbursement accounts (HRAs),based on the concept that patients (con-sumers) should have more control over theutilization of their health care dollars.133The goal is to simultaneously control costsand improve quality by creating incentivesfor consumers to make judgments based onprice and value; in short to purchase healthcare the way we buy other goods and servic-es.134 More than 46 million workers current-ly participate in consumer-directed health
plans (see Figure 3).President Obama has always been hos-
tile to consumer-directed health care. In hisbook, The Audacity of Hope, for example, hedismisses health savings accounts as beingbased on the idea that people have an ir-rational desire to purchase more than they
Figure 3
Workers with Consumer-Directed Health Plans
Source: Source for HRAs: Employer Benefit Research Institute, What Do We Know About Enrollment in
Consumer-Driven Health Plans? vol. 30, no. 12, December 2009.
8/6/2019 Cato Simplified Analysis of ObamaCare
21/66
14
The legislationdoes cut
Medicareand it should!
need.135 That hostility is reflected in thefinal legislative language. Notably, the leg-islation puts substantial new restrictionson such consumer-oriented innovations asHSAs and FSAs.
Roughly 10 million Americans currentlyhave health savings accounts.136 Nothing inthe legislation directly prohibits them. How-ever, the law does add several new restric-tions. For example, the tax penalty for HSAwithdrawals that are not used for qualifiedmedical expenses will be doubled from thecurrent 10 percent to 20 percent, startingthis year.137 In addition, the definition ofqualified medical expense has been mademore restrictive. Among other things, over-the-counter medications are no longer con-
sidered a qualified medical expense.138
Of greater concern is the potential im-pact of the law on high-deductible insuranceplans. Current law requires that an HSA beaccompanied by such a policy. However,many of the insurance regulations discussedabove raise questions about whether or nothigh-deductible plans will remain viable.
For example, the lowest permissible actu-arial value for an insurance plan (the bronzeplan) would be 60 percent.139 It is unclearwhether a plans actuarial value would in-
clude employer or individual contributionsmade to the individuals HSA. That decisionis left to the discretion of the Secretary ofHHS.140 Whether or not HSA contributionsare included can make as much as a 1020percent difference in a plans actuarial value.As a result, if the contributions are not in-cluded, many, if not most, high-deductibleplans will not qualify. The fate of HSAs istherefore dependent on a regulatory rulingby the secretary of HHS in an administra-tion avowedly hostile to HSAs.
The 80 percent minimum medical lossratio required of insurance plans could alsoprove problematic for HSAs. Again, howthis provision will work in practice will de-pend on rules to be developed by the secre-tary of HHS. But, the legislation makes nodistinction between traditional and high-deductible insurance plans. Few if any cur-
rent high-deductible policies meet this re-quirement.
In addition, there is reason to wonderwhether high-deductible insurance planswill likely be able to meet the laws require-
ment that insurance plans provide first-dollar coverage for all preventive servic-es.141 Currently, most high-deductible plansdo cover preventive services as defined by theIRS. However, as discussed above, under thePatient Protection and Affordable Care Actpreventive services will be defined by theU.S. Preventative Services Task Force andonce again, the secretary of HHS.142 If thenew definition of preventive services is moreexpansive than the IRS definition, as seemslikely, most current high-deductible plans
will once again be out of compliance.Finally, insurers must make certain that
their high-deductible plans are designed soas to comply with the laws limits on out-of-pocket expenses.
In theory, a high-deductible plan de-signed to work with health savings accountscould meet all the new requirements. Butindustry sources warn that a plan designedto those specifications would offer few if anyadvantages over traditional insurance andwould not be competitive in todays markets
As a result, insurers may stop offering high-deductible policies.143 And since the rules forHSAs require that they be accompanied by ahigh-deductible plan, the result would be toend HSAs.
The law also includes new limits on FSAswhich are currently used by as many as 30million Americans.144 Starting this year, themaximum tax-exempt contribution to anFSA was cut in half, from $5,000 annually tojust $2,500. 145 The new definition of quali-fied medical expense will also be applied
to FSAs, meaning that as with HSAs, FSAscan no longer be used to pay for over-the-counter medications.146
The impact of these provisions extendswell beyond their impact on workers whocurrently take advantage of such innovativeproducts as HSAs and FSAs. More signifi-cantly, the assault on these products repre-
8/6/2019 Cato Simplified Analysis of ObamaCare
22/66
15
sents a fundamental philosophical shift in
the health care debate. Through this legisla-tion, the president and democrats in Con-gress reject consumer-oriented health carereform in clear favor of government control.
Medicare Cuts
Despite denials from the Obama admin-istration and Democrats in Congress, thelegislation does cut Medicareand it should.Medicare is facing unfunded liabilities of
$50 to $100 trillion depending on the ac-counting measure used, making future ben-efit cuts both inevitable and desirable.147 Ofcourse it would have been better if the sav-ings from any cuts had been used to reducethe programs future obligations rather thanto fund a brand new entitlement program.And, clearly, not all Medicare cuts are created
equal.148 Still, that should not obscure the
necessity for dealing with Medicares loom-ing financial crisis (see Figure 4).
The legislation anticipates a net reduc-tion in Medicare spending of $416.5 billionover 10 years.149 Total cuts would actuallyamount to slightly more than $459 billion,but since the bill would also increase spend-ing under the Medicare Part D prescriptiondrug program by $42.6 billion, the actualsavings would be somewhat less.150
The key word here is anticipates, be-cause several of those cuts are speculative
at best. For example, the bill anticipates a23 percent reduction in Medicare fee-for-service reimbursement payments to provid-ers.151 But Medicare has been slated to makereductions to those payments since 2003,yet each year Congress has voted to defer thecuts. There is no reason to believe that Con-gress is now more likely to follow through
Figure 4
Medicare Cash Flow
Source: 2009 Annual Report of the Boards of Trustees of the Federal Hospital Insurance and Federal Supplementary Medical Insurance Trust Fun
Figure II.E2.
8/6/2019 Cato Simplified Analysis of ObamaCare
23/66
16
Many otherproposed cuts
are actually stepsin the right
direction.
on such cuts. In fact, in a perfect exercise incynicism, the House has already passed sep-arate legislation to repeal them.
More likely, but still problematic, are $136billion in cuts to the Medicare Advantage pro-
gram. Currently, some 10.2 million seniors, 22percent of all Medicare recipients, are enrolledin the Medicare Advantage program, which al-lows Medicare recipients to receive their cov-erage through private insurance plans.152 Thebill would change the way payments are cal-culated for Medicare Advantage. CurrentlyMedicare Advantage programs receive pay-ments that average 14 percent more than tra-ditional fee-for-service Medicare,153somethingthat Democrats have derided as wasteful.154However, the program also offers benefits
not included in traditional Medicare, includ-ing preventive-care services, coordinated carefor chronic conditions, routine physical ex-aminations, additional hospitalization, skillednursing facility stays, routine eye and hearingexaminations, glasses and hearing aids, andmore extensive prescription drug coveragethan offered under Medicare Part D.155
The law imposes a new competitive bid-ding model on the Medicare Advantage pro-gram that will effectively end the 14 percentoverpayment.156 The change will be phased
in over three years beginning in 2012. In re-sponse, many insurers are expected to stopparticipating in the program, while otherswill increase the premiums they charge se-niors. Medicares chief actuary estimatesmore than 7 million seniors could be forcedout of their current insurance plan and backinto traditional Medicare.157 The Congres-sional Budget Office predicts these cutscould lead many plans to limit the benefitsthey offer, raise their premiums, or withdrawfrom the program. Already, Harvard Pilgrim
Health Care has dropped its Medicare Ad-vantage program, forcing 22,000 seniors inMassachusetts, New Hampshire, and Maineto seek other coverage.158
Particularly hard hit would be minori-ties and seniors living in underserved areas.For example, nearly 40 percent of African-American and 54 percent of Latino seniors
participate in Medicare Advantage, in partbecause lower-income seniors see it as alow-cost alternative to Medigap insurancefor benefits not included under traditionalMedicare.159 Interestingly, the law exempts
three counties in south Florida from theMedicare Advantage cuts.In addition, a new productivity adjust-
ment would be applied to reimbursementsto hospitals, ambulatory service centers,skilled nursing facilities, hospice centers,clinical laboratories, and other providers, re-sulting in an estimated savings of $196 bil-lion over 10 years.160 There would also be $3billion in cutbacks in reimbursement for ser- vices that the government believes are overused, such as diagnostic screening and im-
aging services. And, beginning next year, theutilization assumption used to determineMedicare reimbursement rates for high-costimaging equipment will be increased from 50to 75 percent, effectively reducing reimburse-ment for many services.161 This change is ex-pected to reduce total imaging expendituresby as much as $2.3 billion over 10 years.162
Other Medicare cuts include freezing reim-bursement rates for home health care and in-patient rehabilitative services and $1 billionin cuts to physician-owned hospitals.163
And, for the first time, the secretary oHHS would be permitted to use comparativeeffectiveness research in making reimburse-ment decisions. The use of comparative ef-fectiveness research has been extremely con-troversial throughout this debate. On the onehand, many health care experts believe thatmuch of U.S. health care spending is waste-ful or unnecessary.164 Medicare spending var-ies wildly from region to region, without anyevidence that the variation is reflected in thehealth of patients or procedural outcomes.165
A case could certainly be made that taxpayersshould not have to subsidize health care thathas not proven effective, nor can Medicareand Medicaid pay for every possible treatmentregardless of cost-effectiveness.
On the other hand, the use of such re-search in determining what procedures arereimbursed could fundamentally alter the
8/6/2019 Cato Simplified Analysis of ObamaCare
24/66
17
Savings from thcuts will not beused to dealwith Medicares
looming budgetshortfalls.
way medicine is practiced and could inter-pose government bureaucracies in determin-ing how patients should be treated. More-over, there are significant questions aboutwhether comparative effectiveness can pro-
vide a truly effective basis for determining re-imbursement policy.166 In fact, it could be ar-gued that Medicare is particularly unsuitedfor such a policy.167
Many others worry that the use of compar-ative effectiveness research for governmentprograms such as Medicare sets the stagefor its extension to private medical practice.There is no doubt that national health caresystems in other countries use comparativeeffectiveness research as the basis for ration-ing.168 Some of President Obamas health
care advisers, such as former senator TomDaschle have recommended that it be ex-tended to private insurance plans.169 And thepresident has named as the new director ofthe Center for Medicare and Medicaid Ser-vices Dr. Donald Berwick, who is an outspo-ken admirer of the British National HealthService, and particularly its National Insti-tute for Clinical Effectiveness, which makessuch cost-effectiveness decisions.170
Although some of the cuts describedabove are problematic, many other proposed
cuts in this bill are actually steps in the rightdirection. For example, the law reducesMedicare Part D subsidies by $10.7 billionfor high-income recipients. This means thatindividuals with incomes over $85,000 andcouples with incomes over $170,000 will nolonger have their prescription drug purchas-es subsidized by taxpayers.
In addition, the law will eliminate partof a Bush-era subsidy for businesses that in-cludes prescription drug coverage in retireehealth plans.171 Since 2006, as part of the
Medicare prescription drug program, com-panies have received a federal subsidy for 28percent (up to a cap of $1,330 per retiree)of the cost of providing prescription drugsto retired workers.172 Proponents justifiedthe subsidy on the grounds that companieswould otherwise dump workers into Medi-care, raising the cost of the Part D, prescrip-
tion drug plan. However, not only do busi-nesses receive the subsidy, they were alsoallowed to deduct the subsidy from theirtaxes, receiving what was in effect a secondsubsidy. In fact, UC Berkeley Economist
Brad DeLong estimates that by making theoriginal subsidy tax free, the federal govern-ment actually ends up subsidizing 63 per-cent of the cost of retiree drug benefits forsome companies.173 The health care legisla-tion retains the subsidy but eliminates thetax break beginning in 2013.174
This change received a great deal of pressattention when it forced several companies,such as Caterpillar, Lockheed Martin, andAT&T, to take charges against earnings ontheir Securities and Exchange Commission
(SEC) filings. Altogether those charges couldtotal more than $4.5 billion, reflecting fu-ture tax costs to those companies.175
Democrats reacted to the accountingchanges with outrage and threatened hearingson the issue. However, the charges appear tobe required under SEC rules, and Democratslater backed down.176 On the other side, Re-publicans attempted to score points by warn-ing that the change could reduce economicgrowth and reduce employment. They have apoint in that the money that the companies
will now have to pay in taxes is money thatcannot be used to expand operations or payworkers. However, not all tax breaks are cre-ated equal. This one, in particular, appears tobe a highly questionable form of corporatewelfare.
Finally, the new law establishes a new In-dependent Payment Advisory Board, whichwould have the powerto recommend chang-es to the procedures that Medicare will cover,and the criteria to determine when thoseservices would be covered, provided its rec-
ommendations improve the quality of careor improve the efficiency of the Medicareprograms operation.177 Starting in 2013, ifMedicare spending is projected to grow fasterthan the combined average rate of general in-flation and medical inflation (averaged overfive years), IPAB must submit recommenda-tions bringing spending back in line with
8/6/2019 Cato Simplified Analysis of ObamaCare
25/66
8/6/2019 Cato Simplified Analysis of ObamaCare
26/66
19
The combinatioof taxes andsubsidies in thislaw results in asubstantialredistributionof income.
care or through reductions in access to careor the quality of care.186
Congresss record in this regard is decid-edly mixed. As the bills proponents pointout, it is untrue to say that Congress has never
cut Medicare spending. At least 11 times since1980, Congress has passed Medicare cuts thatactually did take place.187 Most were mod-est reductions in payments to certain typesof providers, reductions in disproportion-ate share (DSH) payments to hospitals, orsmall increases in cost-sharing by seniors, orin Medicare premiums. At least in limited cir-cumstances, Congress has been able to trimMedicare.188
However, Medicare is still facing a $50100trillion funding gap, and Congress has proven
itself unable to take the steps necessary to dealwith this long-term gap. Some of the mostsignificant cuts that have been proposed havelater been reduced or repealed. For instance,in 1997, as part of the Balanced Budget Act,Congress established the sustainable growthrate (SGR), designed to hold annual increasesin Medicare reimbursements to a manageablegrowth rate. But in 2003, 2005, 2007, 2008,and this year (reaching back to 2009), Con-gress has overturned provider payment cutsthat would have been required by the SGR. A
bill before Congressthe infamous doc fix(see below)would permanently eliminate fu-ture SGR mandated cuts.189
In some ways the legislation is a victim ofMedicare itself. Because the legislation doesnothing to reform the programs unsustain-able structure, Congress is caught betweentwo unpalatable choices. If it makes the cutscalled for under the legislation, it risks, ac-cording to the CBO reductions in access tocare or the quality of care.190 But if it fails tomake those cuts, then the legislation will add
a huge new cost to an already exploding debt.That is a recipe for legislative paralysis.
Taxes
The Patient Protection and AffordableCare Act imposes more than $569 billion
in new or increased taxes over the first 10years.191 These include
Tax on Cadillac Insurance Plans.One of the most heavily debated new
taxes in the health care bill was thetax on high-cost insurance plans. Be-ginning in 2018, a 40 percent excisetax will be imposed on employer-provided insurance plans with an ac-tuarial value in excess of $10,200 foran individual or $27,500 for families.(The threshold is increased to $11,850for individuals and $30,950 for fami-lies whose head of household is overthe age of 55 or engaged in high-riskprofessions such as police, firefighters,
or miners.) The tax falls on the valueof the plan over the threshold and ispaid by the insurer, or the employerif self-insured.192 The benefit value ofemployer-sponsored coverage wouldinclude the value of contributions toemployees FSAs, HRAs, and HSAs. Itis estimated that 12 percent of work-ers will initially have policies that aresubject to the tax.193 However, the taxis indexed to inflation rather than thefaster-rising medical inflation, which
drives insurance premiums. As a re-sult, more and more workers will even-tually find their insurance plans fall-ing subject to the tax. In fact, a studyfor the benefits consulting firm Tow-ers Watson concludes, Assuming evenreasonable annual plan cost increasesto project 2018 costs, many of todaysaverage plans will easily exceed thecost ceilings directed at todays gold-plated plans.194
Payroll tax hike. The Medicare pay-
roll tax will be increased from 2.9 per-cent today to 3.8 percent for individu-als with incomes over $200,000 for asingle individual or $250,000 for acouple.195 The payroll tax hike wouldmean that in eight states, workerswould face marginal tax rates in excessof 50 percent (see Figure 5).196
8/6/2019 Cato Simplified Analysis of ObamaCare
27/66
20
Tax on Investment Income. Start-ing in 2013, the 3.8 percent Medicaretax will be applied to capital gains andinterest and dividend income if an in-dividuals total gross income exceeds
$200,000 or a couples income exceeds$250,000.197 The tax would only applyto the amount of income in excess ofthose limits, but would be based ontotal income. Thus, if a couple had$200,000 in wage income and $100,000in capital gains, $50,000 would betaxed. Moreover, the definition of capi-tal gains includes capital gains fromthe sale of real estate, meaning that anindividual who sold his or her homefor a profit of $200,000 or more would
be subject to the tax. Given the cur-rent weakness in the housing market,this would seem to create a particularlypernicious outcome. Numerous stud-ies have shown that high capital gainstaxes discourage investment, resultingin lower economic growth, fewer jobs,and reduced wages.
Limit on Itemized Deductions. Be-ginning in 2013, the threshold at whichtaxpayers can deduct medical expenseswill be raised from the current 7.5 per-cent of adjusted gross income to a new
floor of 10 percent.198 The increasedthreshold would be postponed until2016 for taxpayers age 65 or older.199
Tax on Prescription Drugs. Startingthis year, the legislation imposes a newtax on brand-name prescription drugsdesigned to raise a specific amount ofmoney annually. Rather than impos-ing a specific tax amount, the legisla-tion identifies a specific amount ofrevenue to be raised, ranging from $2.5billion in 2011 to $4.2 billion in 2018,
before leveling off at $2.8 billion there-after, and assigns a proportion of thatamount to pharmaceutical manufac-turers according to a formula based onthe companys aggregate revenue frombranded prescription drugs.200 Thestructure of this tax almost guaranteesthat it will be passed along to consum-
Figure 5
States with Marginal Tax Rates over 50 percent after PPACA
Source: Tax Foundation, Private Report.
8/6/2019 Cato Simplified Analysis of ObamaCare
28/66
21
The PatientProtection andAffordable CareAct is a tax and
regulatorynightmare.
ers through higher prices. Tax on Medical Devices. A 2.3 percent
federal sales tax is imposed on medi-cal devices, which includes everythingfrom CT scanners to surgical scis-
sors.
201
The secretary of HHS has theauthority to waive this tax for itemsthat are sold at retail for use by thegeneral public.202 However, almost ev-erything used by doctors, hospitals, orclinics would be taxed. The tax wouldalso fall on laboratory tests. The gov-ernments chief actuary has concludedthat this tax, as those on pharmaceuti-cal manufacturers and insurers wouldgenerally be passed through to healthconsumers.203 In fact, a study by the
Republican staff of the Joint EconomicCommittee estimates that the pass-through could cost the typical familyof four with job-based coverage an ad-ditional $1,000 a year in higher premi-ums.204
Additional Taxes on Insurers. Simi-lar to the tax on pharmaceutical com-panies, the legislation imposes a taxon health insurers based on their mar-ket share.205 The total assessment willbegin at $8 billion and rise to $14.3
billion by 2018. Thereafter the totalassessment will increase by the samepercentage as premium growth for theprevious year.206 The tax will be allo-cated according to a formula based onboth the total premiums collected byan insurer and the insurers adminis-trative costs.207 However, some insur-ers in Michigan and Nebraska receiveda special exemption.208 This tax is alsoexpected to be passed through to con-sumers through higher premiums.
(Interestingly, AARP is exempt fromthis tax on sales of its highly profit-able Medigap policies.)209
Tax on Tanning Beds. The legislationimposes a 5 percent tax on tanning sa-lons.210 While tanning may be seen asa luxury or frivolous expenditure, itis actually a recommended treatment
for psoriasis and certain other medicalconditions. The law makes no distinc-tion between tanning for medical orcosmetic reasons. This tax went intoeffect July 1, 2010.
The combination of taxes and subsidiesin this law results in a substantial redistri-bution of income. The new law will costfamilies earning more than $348,000 peryear, (top 1 percent of incomes) an addition-al $52,000 per year on average in new taxesand reduced benefits.211 In contrast, thoseearning $18,000$55,000 per year will see anet income increase of roughly $2,000 perfamily.212
The new law contains other tax-related
provisions that will add significantly tobusiness costs. For example, the legislationrequires that businesses provide a 1099 formto every vendor with whom they do morethan $600 worth of business over the courseof a year.213 This provision has proven so un-popular that there is strong bipartisan sup-port for repeal. In fact, on February 2, 2011,the Senate voted 81 to 17 to repeal this pro-vision. The House will likely follow suit.214
For both individual Americans and busi-nesses large and small, the Patient Protec-
tion and Affordable Care Act is a tax andregulatory nightmare.
The CLASS Act
The health care legislation establishes anew national long-term care program, calledthe Community Living Assistance and Sup-port Act (CLASS Act), designed to help se-niors and the disabled pay for such servicesas an in-home caretaker or adult day servic-
es.215The CLASS Act is theoretically designed
to be self-financed. Workers would be au-tomatically enrolled in the program, butwould have the right to opt out. Those whoparticipate will pay a monthly premiumthat has not yet been determined.216 How-ever, the CBO estimates that will be roughly
8/6/2019 Cato Simplified Analysis of ObamaCare
29/66
22
$123 per month for the average worker.217Other estimates suggest that the premiumscould be much higher, perhaps $180$240per month.218 Workers must contribute tothe program for at least five years before they
become eligible for benefits.
219
(Individualsage 55 or over at the time the program isfully implemented must not only contrib-ute for five years, but must be employed forat least three years following the programsimplementation date.)220 There is no healthunderwriting of participation or premiums.
The actual benefits to be provided underthe program are among the many detailsthat remain to be determined but will notbe less than an average of $50 daily ad-justed for inflation.221 Some estimates sug-
gest that benefits will average roughly $75per day, or slightly more than $27,000 peryear.222 Benefits will be paid directly to theindividual, not to the service provider, based
on the degree of an individuals impairment,and can be used to purchase home care andother community-based long-term care as-sistance, as well as certain nonmedical ser-vices.223 Benefits may be paid daily, weekly,
monthly, or deferred and rolled over frommonth to month at the beneficiarys discre-tion.224 There is no lifetime limit to benefits
Eligibility for benefits will be based onthe same criteria currently used to qualifyfor federal-tax-qualified long-term-care in-surance benefits. That is, a person must beunable to perform at least two activities ofdaily living from a list of six such activities,or need substantial supervision due to cog-nitive impairment.225 The secretary of HHSmay also develop different or additional eli-
gibility requirements.226
During the laws first five years it willcollect premiums, but not pay benefits. Asa result, over the first 10 years, the period
Source: Letter from Douglas Elmendorf, director, Congressional Budget Office, to House speaker Nancy Pelosi, March 20, 2010, and Letter from Douglas
Elmendorf, director, Congressional Budget Office, to Sen. Tom Harkin, November 25, 2009.
Figure 6
Effect of CLASS Act on Federal Budget
8/6/2019 Cato Simplified Analysis of ObamaCare
30/66
23
The CLASS Actmay representone of the healthcare legislationbiggest fiscaltime bombs.
conveniently included in the budget scoringwindow, the CLASS Act will run a surplus,collecting more in premiums than it paysout in benefits (see Figure 6).
Those premiums will accrue in a CLASS
Act Trust Fund, similar to the Social Securityand Medicare trust funds. Using trust fundaccounting measures, the premium pay-ments will reduce the federal deficit over thatperiod by roughly $70.2 billion.227 However,thereafter, the CLASS Act will begin to payout benefits faster than it brings in revenue.Although this time period falls outside theformal 10-year scoring window, CBO warns,In the decade following 2029, the CLASSprogram would begin to increase budget def-icits . . . by amounts on the order of tens of
billions of dollars for each 10-year period.228
CBO goes on to warn, We have grave con-cerns that the real effect of [the CLASS Act]would be to create a new federal entitlementprogram with large, long-term spending in-creases that far exceed revenues.
Trust fund accounting, of course, is littlemore than budgetary sleight of hand. Be-cause the government is structurally inca-pable of saving such surpluses, they becomesimply a source of current revenue for thegovernment to use for whatever purpose
seems most pressing at the time. It does notprovide resources with which to pay the fu-ture obligations that have been created.229Even Senate Budget Committee chairmanKent Conrad (D-ND), who eventually vot-ed for the bill, called it a Ponzi scheme ofthe first order, the kind of thing that Ber-nie Madoff would have been proud of.230 And the bipartisan Commission on FiscalResponsibility and Reform (the Bowles-Simpson Commission) recognized that theCLASS Act program will require large gen-
eral revenue transfers or collapse of its ownweight.231 The commission recommendedthat the CLASS Act be reformed in someunspecified way so as to make it crediblysustainable over the long term; otherwise itshould be repealed.
In addition, the structure of the programcreates a huge adverse selection risk that
could add to the programs financial insta-bility. As the actuarial firm Milliman Associ-ates points out, The voluntary aspect of theprogram allows low-risk individuals to nev-er sign up for the program while the guaran-
teed issue enables some of the highest-riskindividuals to join the program. This is aformula that is virtually certain to create fi-nancial instability in any insurance programunless there are other important provisionsto control risk.232
The law tries to ameliorate the adverseselection problem by requiring individualswho opt out of the program to pay a higherpremiumup to 250 percent higherif theylater decide to opt back in.233 But expertssuggest that these provisions will be insuf-
ficient to prevent gaming the system. Andother provisions actually make adverse selec-tion more likely. For example, the law limitsmarketing costs to no more than 3 percentof premiums. The resulting lack of market-ing will likely result in a low participationrate by the public at large, while those withhealth problems are most likely to seek outthe benefits. The American Academy of Ac-tuaries estimates that only about 6 percentof the U.S. population will participate in theprogram.234 And, Richard Foster suggests
that just 2 percent of workers will partici-pate after three years.235 Given such low par-ticipation levels, the covered population willalmost certainly be far sicker than generalinsurance pool. Foster warns that there is avery serious risk that the problem of adverseselection will make the CLASS program un-sustainable.236
Making matters worse, the legislationcaps premiums for low-income workersand undergraduate students and prohibitsfuture premium hikes for some groups of
retirees.237 Therefore, if the program is toremain self-sustaining, other workers willhave to bear a disproportionate share of fu-ture premium hikes. That in turn increasesthe risk that program premiums will exceedthose for products available in the privatemarket. Healthier individuals, in particular,would have an incentive to flee the program
8/6/2019 Cato Simplified Analysis of ObamaCare
31/66
24
Some estimatessuggest we willface a shortage
of more than150,000
physicians.
for less expensive private alternatives, leav-ing only the sickest and most expensive par-ticipants in the government plan. The ad-verse selection death spiral would be in fullforce, which could tempt the government to
solve the problem by making participationmandatory, forcing Americans into a pro-gram they may not want and to which thereare superior private alternatives.238 The onlyother alternative will be a taxpayer bailout.
The CLASS Act, therefore, while little de-bated, may represent one of the health carelegislations biggest fiscal time bombs.
Growing the Nanny State
A little-discussed provision of the healthcare legislation requires restaurant chainswith at least 20 locations or franchises topost calorie counts next to prices on menus,menu boards, and drive-through menus. Inaddition, restaurateurs would be required topost a brief statement regarding daily caloricintake and advise guests that additional nu-trition information is available. Other nu-trition data, which must be available on re-quest, would include calories from fat, totalfat, saturated fat, cholesterol, sodium, carbo-
hydrates, sugars, dietary fiber and protein.239More than 200,000 establishments will be af-fected by the change.240 The law also requiresnutrition information to be posted on foodand beverage vending machines.241
There is no doubt that the United Stateshas a serious obesity problem.242 However,posting calories is unlikely to have a signifi-cant impact. Studies show that only about56 percent of chain restaurant customerssaid they even notice posted calorie infor-mation, while even fewer, just 15 percent,
take the calorie information into accountwhen making their choices.243
But, while they are unlikely to signifi-cantly reduce obesity, the new regulationswill impose a cost on restaurants and con-sumers. Estimates suggest that the cost ofanalyzing calories runs as high as $1,000per meal.244 In addition there will be the
cost of changing all those menus and signsAnd, the cost of posting the information onvending machines has been estimated to beat least $56.4 million for the first year.245
While the financial cost of this provision
is not substantial, especially in the contextof other taxes and regulatory costs imposedby this law, it does represent yet anotherblow against individual responsibility.
Other Provisions
The legislation includes a number of pi-lot programs designed to increase quality ofhealth care or control costs. Most are wellintentioned but unlikely to have significant
impact, especially in the short term. Thesewould include programs such as bundledpayments, global payments, accountable-careorganizations and medical homes throughmultiple payers and settings.246 It would alsocreate a new Center for Innovation within theCenters for Medicare and Medicaid Services(CMS) to evaluate innovative models of care,and would require CMS to develop a Nation-al Quality Strategy to improve care delivery,health outcomes and population health.247
The federal government would also pro-
vide grants to states for incentives for Med-icaid beneficiaries to participate in healthy-lifestyle programs. A state option wouldenroll Medicaid beneficiaries with chronicillnesses into health homes that offer com-prehensive, team-based care, and a new op-tional Medicaid benefit would allow peoplewith disabilities to receive community-basedservices and supports.248 Other grants wouldprovide incentives for states to shift Med-icaid beneficiaries away from nursinghomes and toward care in the home or
community.249The law would also reward hospitals for
providing value-based care, and penalizehospitals that perform poorly on qualitymeasures such as preventable hospital read-missions.250
Of greater concern is a provision to es-tablish a private, nonprofit institute to con-
8/6/2019 Cato Simplified Analysis of ObamaCare
32/66
25
By 2019, CBOexpects there tobe more than23 million
uninsured.
duct comparative effectiveness research.251Many health care reform advocates believethat much of U.S. health care spending iswasteful or unnecessary. Certainly it is im-possible to draw any sort of direct correla-
tion between the amount of health carespending and outcomes.252 In fact, by someestimates as much as 30 percent of all U.S.health spending produces no discernablevalue.253 Medicare spending, for instance,varies wildly from region to region, withoutany evidence that the variation is reflectedin the health of patients or procedural out-comes.254 The Congressional Budget Officesuggests that we could save as much as $700billion annually if we could avoid treatmentsthat do not result in the best outcomes.255 It
makes sense, therefore, to test and developinformation on the effectiveness of varioustreatments and technology.
Critics fear, however, that comparativeeffectiveness research will not simply beused to provide information, but to imposea government-dictated method of practic-ing medicine. The legislation prohibits useof the research to create health care practiceguidelines or for insurance coverage deci-sions.256 The research would initially be in-formative only. Still, there is no doubt that
many reformers hope to ultimately use theinformation to restrict the provision of un-necessary care.257
The Patient Protection and AffordableCare Act also includes several provisionsaimed at increasing the health care workforce.This is particularly important given the lawsemphasis on increasing coverage and there-fore the demand for services. The UnitedStates already faces a potential shortage ofphysicians, especially primary-care physiciansand certain specialties such as geriatric care.
Some estimates suggest we will face a short-age of more than 150,000 physicians in thenext 15 years.258 The legislation itself couldexacerbate this trend if physicians find theirreimbursement rates reduced under Medicareand Medicaid, or find more bureaucratic in-terference with their medical decisionmaking.Indeed, one survey found that 45 percent of
physicians would at least consider the possi-bility of quitting as a result of this health carelegislation.259
The law attempts to combat this by in-creasing funding for physician and nurs-
ing educational loan programs, and wouldexpand loan forgiveness under the NationalHealth Service Corps.260 It would also fundnew educational centers in geriatric care,chronic-care management, and long-termcare.261 It also takes more controversial stepstoward increasing the supply