Embed Size (px)
Citation preview
Releasing Time to Care™
Productive Ward Productive Mental Health Ward
CASIL Report
January 2012
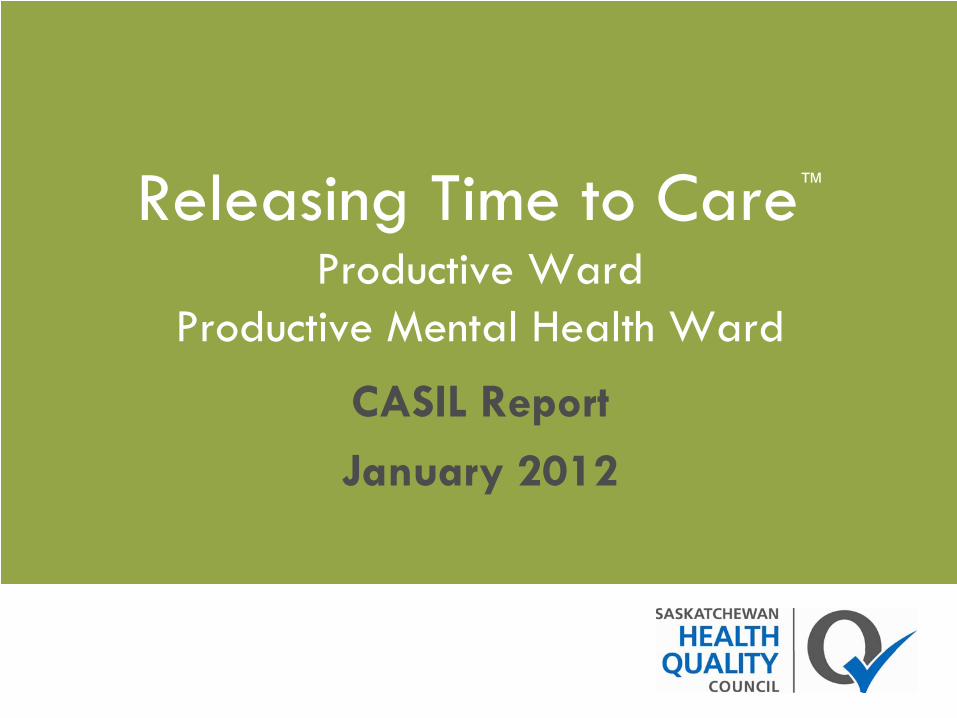
Releasing Time to Care™
(RTC)
Learn more about Releasing Time to Care™
in Saskatchewan
Learn more about Releasing Time to Care™
in England
What is a CASIL report?The “CASIL” framework was developed by the National Health Service Institute for Innovation and Improvement.
Health regions provide an update on RTC implementation activities through quarterly report submissions to HQC.
CASIL reporting focuses on five key areas:CompletionAdoption/Awareness ActivitiesImpactSpreadLessons Learned
See previous CASIL reports

CompletionQuarterly Report
Date
Number of sites that have completed all foundational modules + 1 process
module
Number of sites that have completed all modules
October 2009 2 -
January 2010 2 -
April 2010 14 -
July 2010 18 -
October 2010 18 -
January 2011 19 -
April 2011 23 1
July 2011 30 3
October 2011 41 4
January 2012 41 6
Adoption and awareness highlights
Cypress
Health Region
RTC activities continue to be reported to the board as part of the health region’s “Quality, Risk and Safety” monthly report.
Heartland Health Region
Boardwalks continue, with updates from the Admissions and Discharge team including “stakeholder survey” results shared with all, informing where the team will focus their improvement efforts.The PSAG/Shift Handover team continue to utilize the RTC Board and Boardwalk to share shift handover timing results of the process implemented early 2011 confirming the efficiency improvement is being sustained.
Adoption and awareness highlightsSaskatoon
Health Region
• Cathy Marshall, Manager of Nursing, 6300 Neuroscience, Royal University Hospital (RUH) and Nick Kadash, RN, have been touring Canada (Montreal, Toronto and Vancouver) to share their story of
RTC improvement. In October, Cathy and Nick travelled to Toronto and
presented at the Registered Nurses’
Association of Ontario. They are skilled ambassadors of change: Cathy shared her experiences in leading organizational change while Nick discussed change from a
front-line staff perspective.
• Pam Molnar, Manager of 5th Medicine at SPH, presented highlights
from her Master’s thesis to the managers of nursing and leadership in SHR. There were three major conclusions as a result of the research: 1. For RTC to be successful, organizational awareness and understanding is needed; 2. The leadership style of the nurse manager impacts RTC implementation, and; 3. Nurse manager and staff relationships are essential for employee engagement. Jackie Mann, VP of Acute Care
recognized that these findings could be generalized beyond the RTC to many other change initiatives. Maura Davies, CEO, SHR suggested that Pam’s recommendations be considered as the SHR develops an implementation plan for the newly adopted lean management system. Pam has succeeded in making a significant contribution to our understanding of leading change and influential role of the MON.
Adoption and awareness highlightsPrince Albert Parkland Health Region
• Inpatient Mental Health -
staff are being made aware of the advances we are trying to make in RTC. We have the minutes of the weekly
meetings posted for all to see and the RTC Board is being updated regularly. At this point we feel we are gaining momentum with staff involvement.
Sunrise Health Region
• RTC was highlighted via storyboards at the Regional Safety and Quality Fair.
• Article in Fall/Winter newsletter “Letter from Home”
to all residents, families, volunteers, general public, staff.
• Article in Sunrise Health Region “Connection”
(internal newsletter) December 2011.
Regina Qu’Appelle
Health Region
Leadership visits:Unit 6A, Regina General Hospital: Trent Truscott (Executive Director of Surgical and Specialty Care) and Dr. Joy Dobson (Senior Medical Officer)ICU and CSU, Pasqua Hospital: Dr. Joy Dobson, Dwight Nelson (President and CEO), Diane Larrivee (VP, Specialty Care), Val Davies (Executive Director, Cardiosciences & Critical Care), Lori Garchinski(Director, Cardiosciences), and Colleen Bryant (RQHR board member)
Adoption and awareness –
5A Surgery, SPH, Saskatoon Health Region
The RTC team on 5A Surgery, SPH, hosted a Christmas Potluck Dec 15th
. Representatives from almost all areas of the hospital attended, including Therapies, Social Work, Pharmacy, Facilities and Environmental Services, residents and physician partners. The new Manager of Nursing for 5A Surgery, Lorrie Laframbroise, noted that, “We made a quick decision to get in the Christmas spirit and host this event. While the 5A staff Christmas potluck has been a tradition, this was the best turnout we have ever had.”
This unit is just getting started with RTC and this event was a great medium to introduce RTC to members of the interdisciplinary team and support partners at SPH.
The RTC team on 5A Surgery, SPH, enjoying some Christmas cheer at their potluck.
Adoption and awareness –
Victoria Hospital, PAPHR
Levels 5 and 6 held re-
energizer meetings in December to refocus on RTC and try to get staff motivated once again in rolling out RTC.
Staff enjoyed a pizza lunch and reviewed the RTC basics. Since the re-
energizer, Level 6 has had three new staff members sign up for process module work.
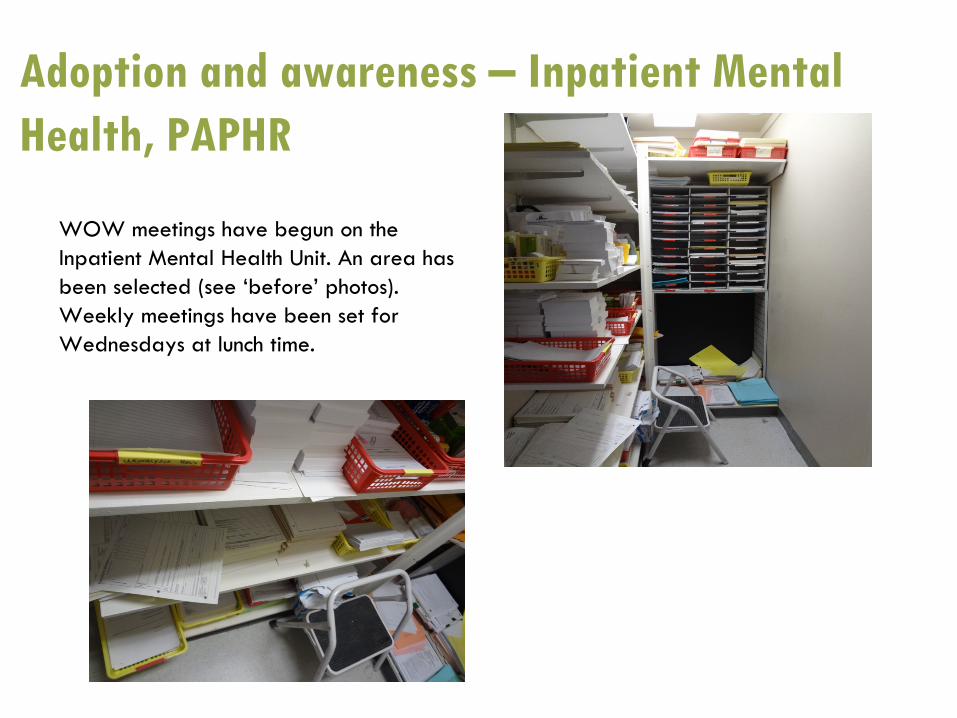
Adoption and awareness –
Inpatient Mental Health, PAPHR
WOW meetings have begun on the Inpatient Mental Health Unit. An area has been selected (see ‘before’
photos). Weekly meetings have been set for Wednesdays at lunch time.
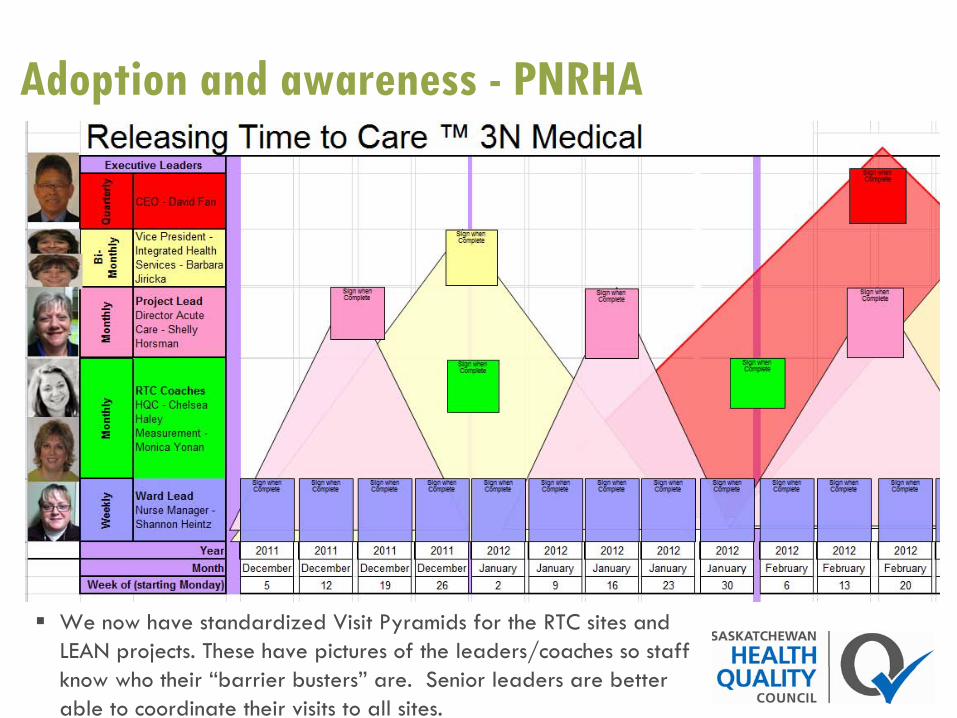
Adoption and awareness -
PNRHA
We now have standardized Visit Pyramids for the RTC sites and LEAN projects. These have pictures of the leaders/coaches so staff know who their “barrier busters” are. Senior leaders are better able to coordinate their visits to all sites.
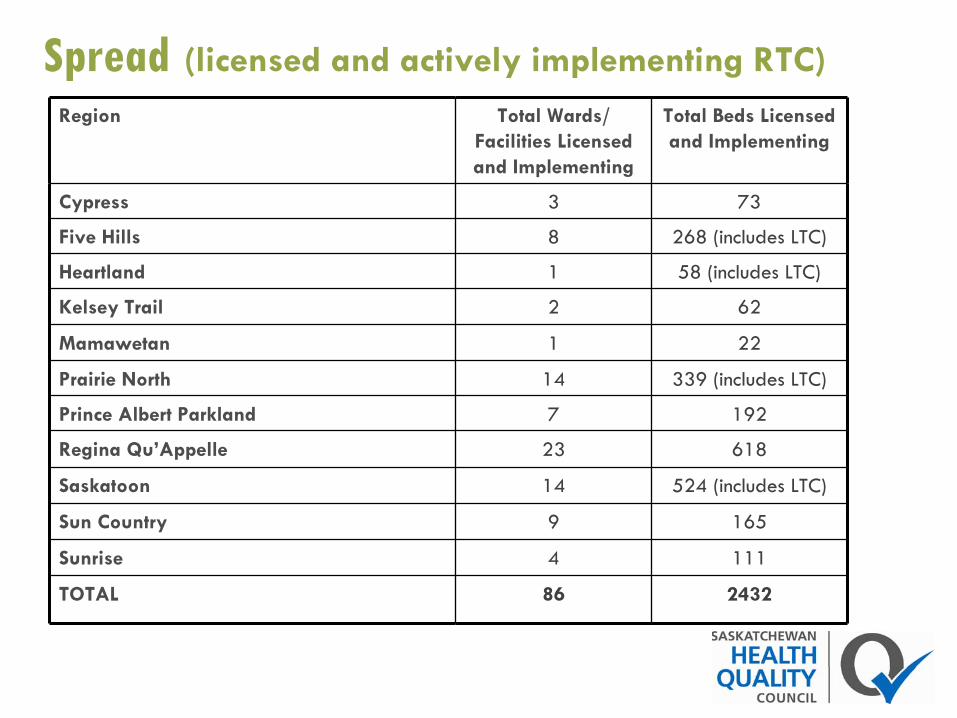
Spread
(licensed and actively implementing RTC)Region Total Wards/
Facilities Licensed and Implementing
Total Beds Licensed and Implementing
Cypress 3 73
Five Hills 8 268 (includes LTC)
Heartland 1 58 (includes LTC)
Kelsey Trail 2 62
Mamawetan 1 22
Prairie North 14 339 (includes LTC)
Prince Albert Parkland 7 192
Regina Qu’Appelle 23 618
Saskatoon 14 524 (includes LTC)
Sun Country 9 165
Sunrise 4 111
TOTAL 86 2432

Impact
Impact is evaluated in relationship to the four core objectives of RTC:
Improving patient safety and reliability of careImproving patient experienceImproving staff well-beingImproving efficiency of care
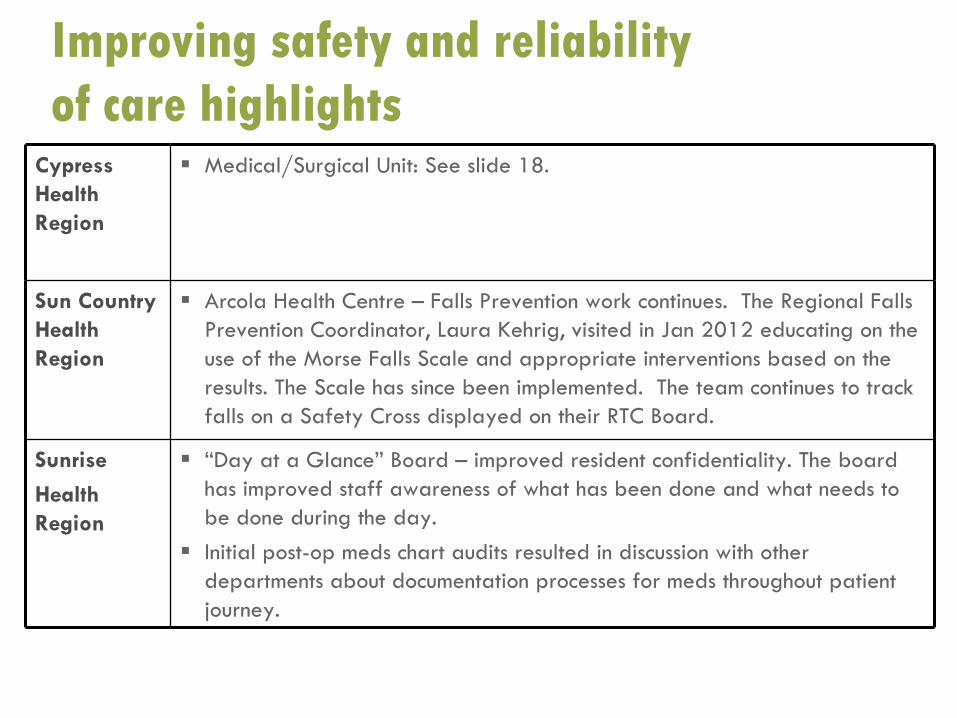
Improving safety and reliability of care highlights
Cypress Health Region
Medical/Surgical Unit: See slide 18.
Sun Country Health Region
Arcola Health Centre – Falls Prevention work continues. The Regional Falls Prevention Coordinator, Laura Kehrig, visited in Jan 2012 educating on the use of the Morse Falls Scale and appropriate interventions based on the results. The Scale has since been implemented. The team continues to track falls on a Safety Cross displayed on their RTC Board.
Sunrise
Health Region
“Day at a Glance” Board – improved resident confidentiality. The board has improved staff awareness of what has been done and what needs to be done during the day.Initial post-op meds chart audits resulted in discussion with other departments about documentation processes for meds throughout patient journey.
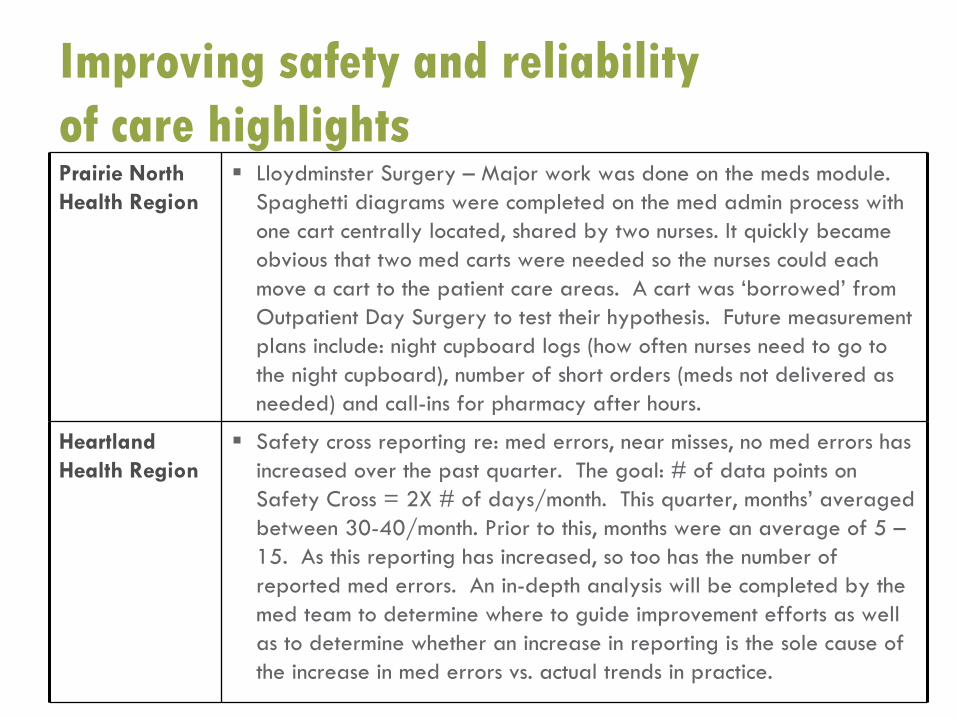
Improving safety and reliability of care highlightsPrairie North Health Region
Lloydminster Surgery – Major work was done on the meds module. Spaghetti diagrams were completed on the med admin process with one cart centrally located, shared by two nurses. It quickly became obvious that two med carts were needed so the nurses could each move a cart to the patient care areas. A cart was ‘borrowed’ from Outpatient Day Surgery to test their hypothesis. Future measurement plans include: night cupboard logs (how often nurses need to go to the night cupboard), number of short orders (meds not delivered as needed) and call-ins for pharmacy after hours.
Heartland Health Region
Safety cross reporting re: med errors, near misses, no med errors has increased over the past quarter. The goal: # of data points on Safety Cross = 2X # of days/month. This quarter, months’ averaged between 30-40/month. Prior to this, months were an average of 5 –15. As this reporting has increased, so too has the number of reported med errors. An in-depth analysis will be completed by the med team to determine where to guide improvement efforts as wellas to determine whether an increase in reporting is the sole cause of the increase in med errors vs. actual trends in practice.
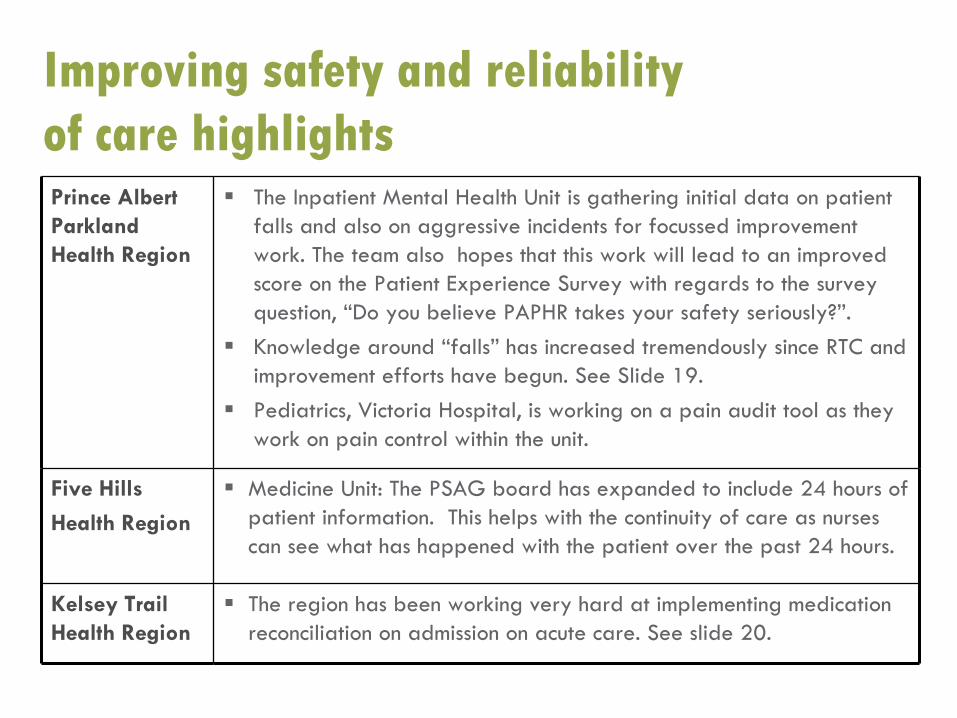
Prince Albert Parkland Health Region
The Inpatient Mental Health Unit is gathering initial data on patient falls and also on aggressive incidents for focussed improvement work. The team also hopes that this work will lead to an improved score on the Patient Experience Survey with regards to the survey question, “Do you believe PAPHR takes your safety seriously?”.Knowledge around “falls” has increased tremendously since RTC and improvement efforts have begun. See Slide 19.Pediatrics, Victoria Hospital, is working on a pain audit tool as they work on pain control within the unit.
Five Hills
Health Region
Medicine Unit: The PSAG board has expanded to include 24 hours of patient information. This helps with the continuity of care as nurses can see what has happened with the patient over the past 24 hours.
Kelsey Trail Health Region
The region has been working very hard at implementing medicationreconciliation on admission on acute care. See slide 20.
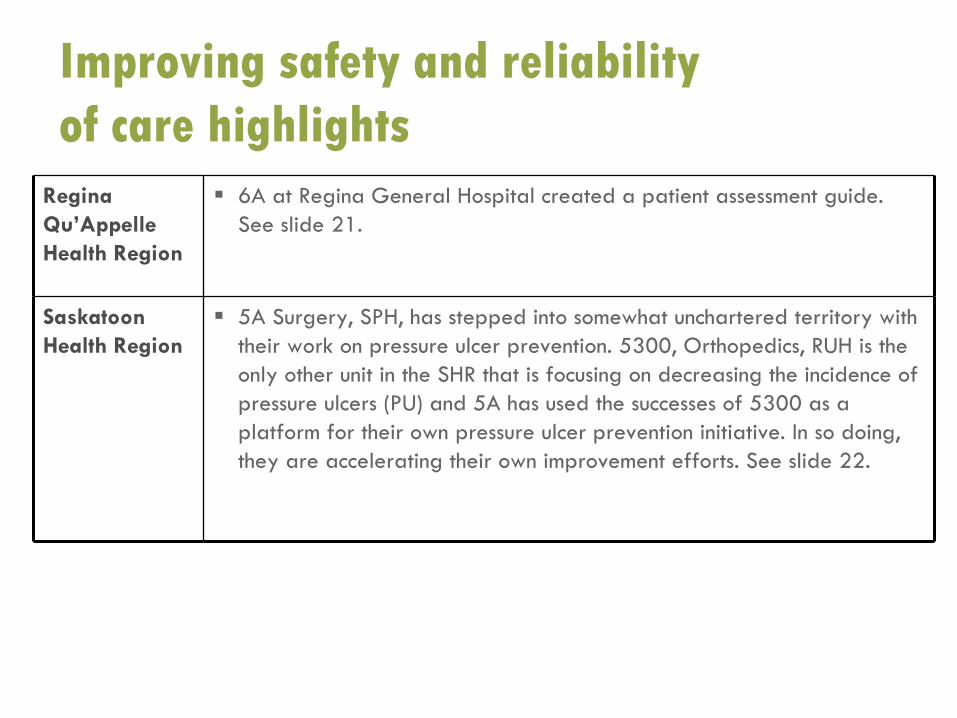
Improving safety and reliability of care highlights
Improving safety and reliability of care highlights
Regina Qu’Appelle Health Region
6A at Regina General Hospital created a patient assessment guide. See slide 21.
Saskatoon Health Region
5A Surgery, SPH, has stepped into somewhat unchartered territory with their work on pressure ulcer prevention. 5300, Orthopedics, RUH is the only other unit in the SHR that is focusing on decreasing the incidence of pressure ulcers (PU) and 5A has used the successes of 5300 as a platform for their own pressure ulcer prevention initiative. In so doing, they are accelerating their own improvement efforts. See slide 22.
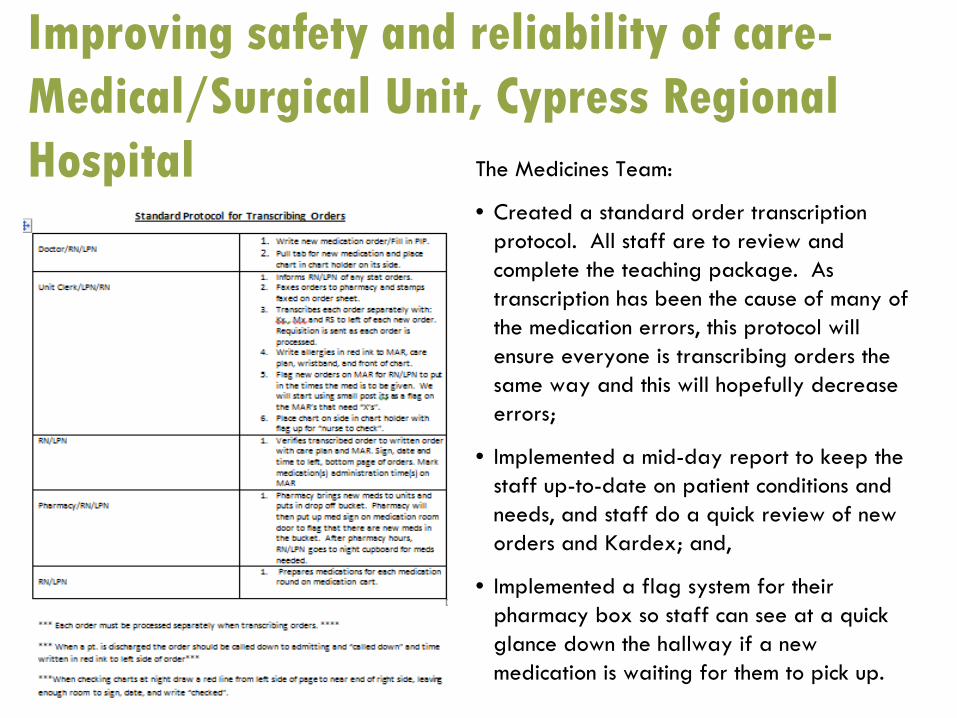
Improving safety and reliability of care- Medical/Surgical Unit, Cypress Regional
Hospital The Medicines Team:
• Created a standard order transcription protocol. All staff are to review and complete the teaching package. As transcription has been the cause of many of the medication errors, this protocol will ensure everyone is transcribing orders the same way and this will hopefully decrease errors;
• Implemented a mid-day report to keep the staff up-to-date on patient conditions and needs, and staff do a quick review of new orders and Kardex; and,
• Implemented a flag system for their pharmacy box so staff can see at a quick glance down the hallway if a new medication is waiting for them to pick up.
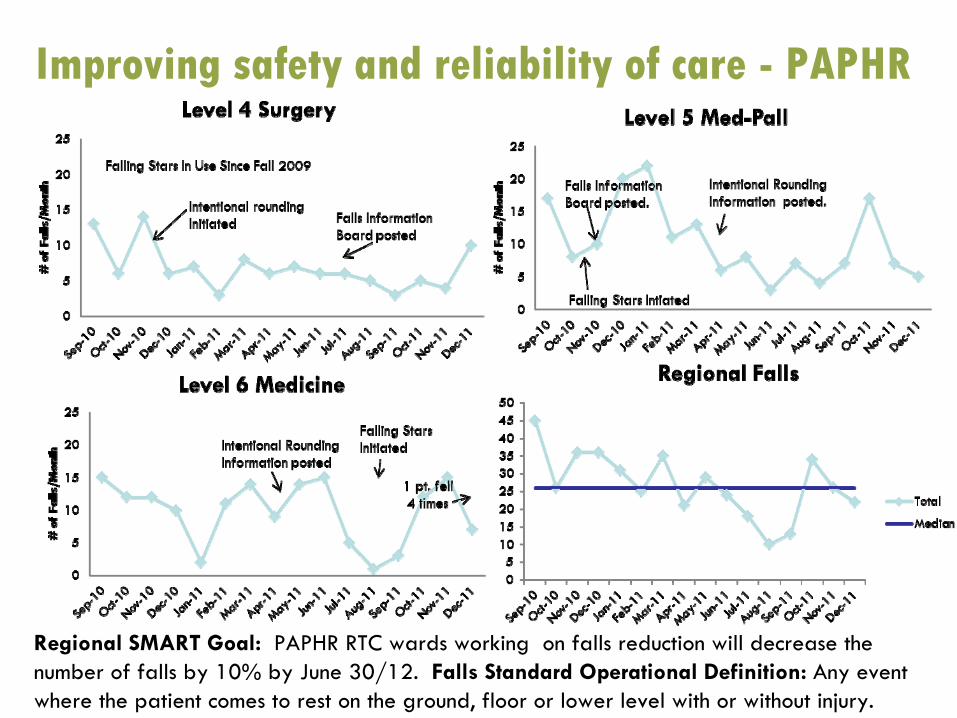
Improving safety and reliability of care -
PAPHR
Regional SMART Goal: PAPHR RTC wards working on falls reduction will decrease the number of falls by 10% by June 30/12. Falls Standard Operational Definition: Any event where the patient comes to rest on the ground, floor or lower level with or without injury.

Improving safety and reliability of care-, Nipawin Hospital, KTHR
Melfort and Nipawin have completed medication reconciliation education and audits are now monitoring progress.
Improving safety and reliability of care-6A, RGH, RQHR Unit 6A has created an assessment guide which allows the nurse to do a thorough head-to-
toe assessment on every patient, on every shift, in a focused and timely manner.
This assessment guide has improved communication among staff as all assessments are now documented in the same way. This communicates to staff exactly what the nurse assessed and if there have been any changes over recent shifts/days thereby improving patient safety and reliability of care!
In addition to safety…
Before this guide, it took a nurse an average of six minutes (per patient) to document an entire head-to-toe assessment. With the new guide, which allows the nurse to select an appropriate statement of assessment and/or make comments, the documentation time has been reduced to two minutes.
SAVINGS?
~120 hours per month or 1440 hours per year which is equivalent to 0.74 FTE to spend with patients yearly! This is a fabulous example of how a change can result in an
improvement that releases time to care!
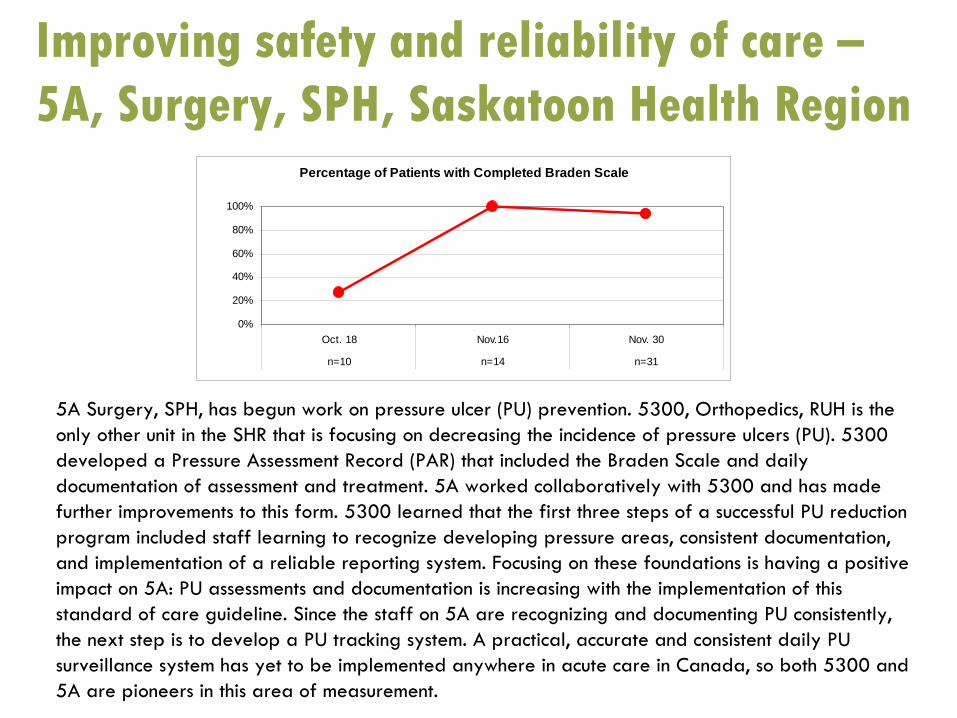
Improving safety and reliability of care – 5A, Surgery, SPH, Saskatoon Health Region
5A Surgery, SPH, has begun work on pressure ulcer (PU) prevention. 5300, Orthopedics, RUH is the only other unit in the SHR that is focusing on decreasing the incidence of pressure ulcers (PU).
5300 developed a Pressure Assessment Record (PAR) that included the Braden Scale and daily documentation of assessment and treatment. 5A worked collaboratively with 5300 and has made further improvements to this form. 5300 learned that the first three steps of a successful PU reduction program included staff learning to recognize developing pressure
areas, consistent documentation, and implementation of a reliable reporting system. Focusing on these foundations is having a positive impact on 5A: PU assessments and documentation is increasing with the implementation of this standard of care guideline. Since the staff on 5A are recognizing and documenting PU consistently, the next step is to develop a PU tracking system. A practical, accurate and consistent daily PU surveillance system has yet to be implemented anywhere in acute care in Canada, so both 5300 and 5A are pioneers in this area of measurement.
Percentage of Patients with Completed Braden Scale
0%
20%
40%
60%
80%
100%
Oct. 18 Nov.16 Nov. 30
n=10 n=14 n=31
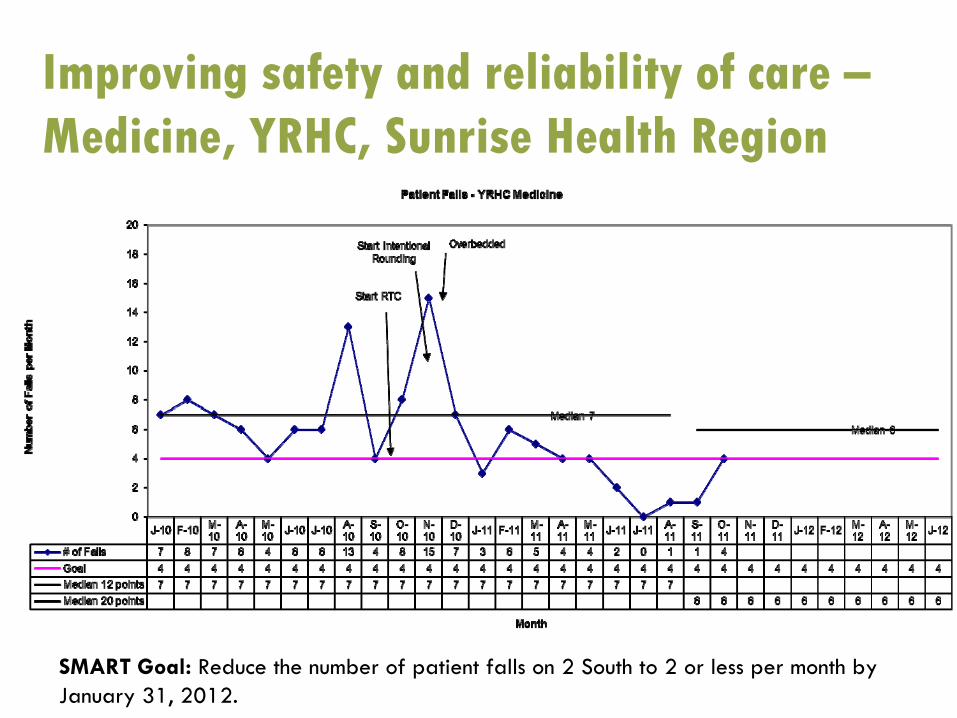
Improving safety and reliability of care – Medicine, YRHC, Sunrise Health Region
SMART Goal: Reduce the number of patient falls on 2 South to 2 or less per month by January 31, 2012.
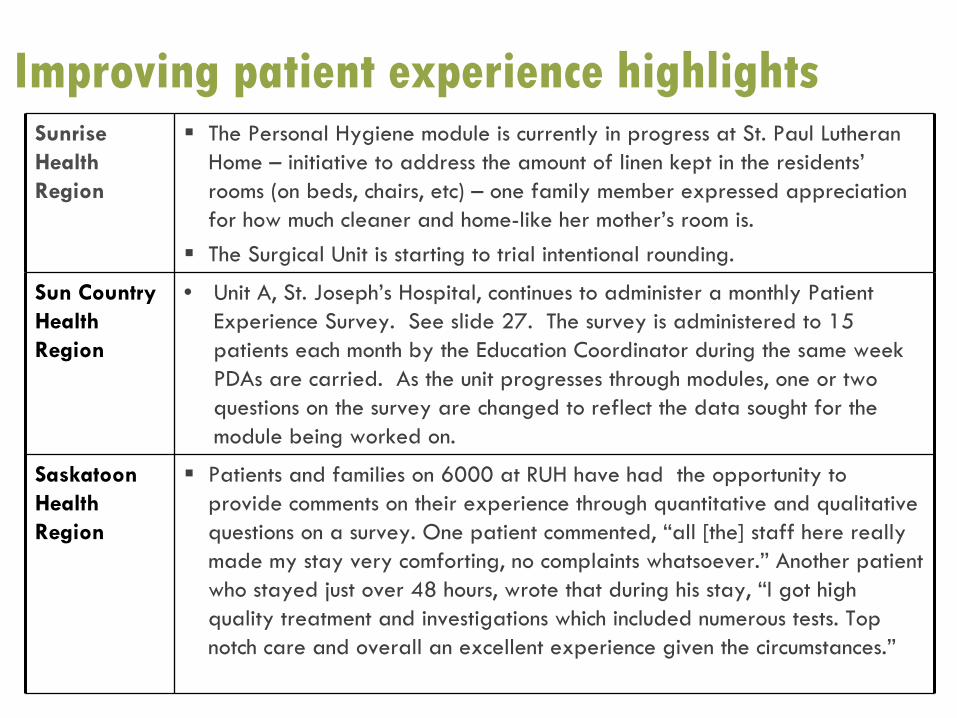
Improving patient experience highlightsSunrise Health Region
The Personal Hygiene module is currently in progress at St. Paul Lutheran Home – initiative to address the amount of linen kept in the residents’rooms (on beds, chairs, etc) – one family member expressed appreciation for how much cleaner and home-like her mother’s room is.The Surgical Unit is starting to trial intentional rounding.
Sun Country Health Region
• Unit A, St. Joseph’s Hospital, continues to administer a monthly Patient Experience Survey. See slide 27. The survey is administered to
15 patients each month by the Education Coordinator during the same
week PDAs
are carried. As the unit progresses through modules, one or two questions on the survey are changed to reflect the data sought for the module being worked on.
Saskatoon Health Region
Patients and families on 6000 at RUH have had the opportunity to provide comments on their experience through quantitative and qualitative questions on a survey. One patient commented, “all [the] staff here really made my stay very comforting, no complaints whatsoever.” Another patient who stayed just over 48 hours, wrote that during his stay, “I got high quality treatment and investigations which included numerous tests. Top notch care and overall an excellent experience given the circumstances.”
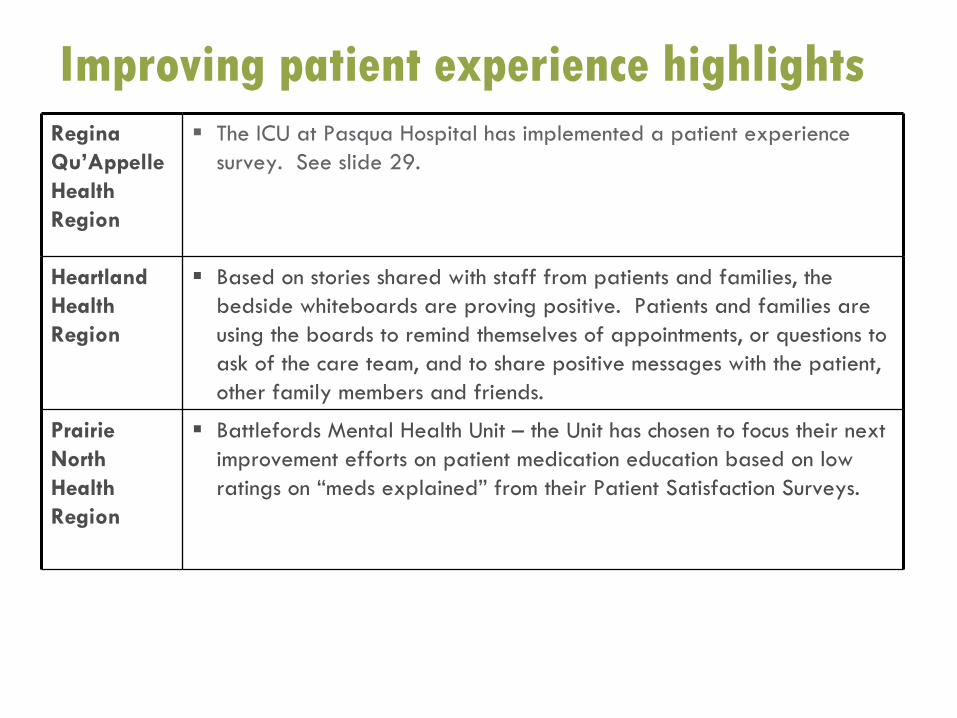
Improving patient experience highlightsRegina Qu’Appelle Health Region
The ICU at Pasqua Hospital has implemented a patient experience survey. See slide 29.
Heartland Health Region
Based on stories shared with staff from patients and families, the bedside whiteboards are proving positive. Patients and families are using the boards to remind themselves of appointments, or questions to ask of the care team, and to share positive messages with the patient, other family members and friends.
Prairie North Health Region
Battlefords Mental Health Unit – the Unit has chosen to focus their next improvement efforts on patient medication education based on lowratings on “meds explained” from their Patient Satisfaction Surveys.
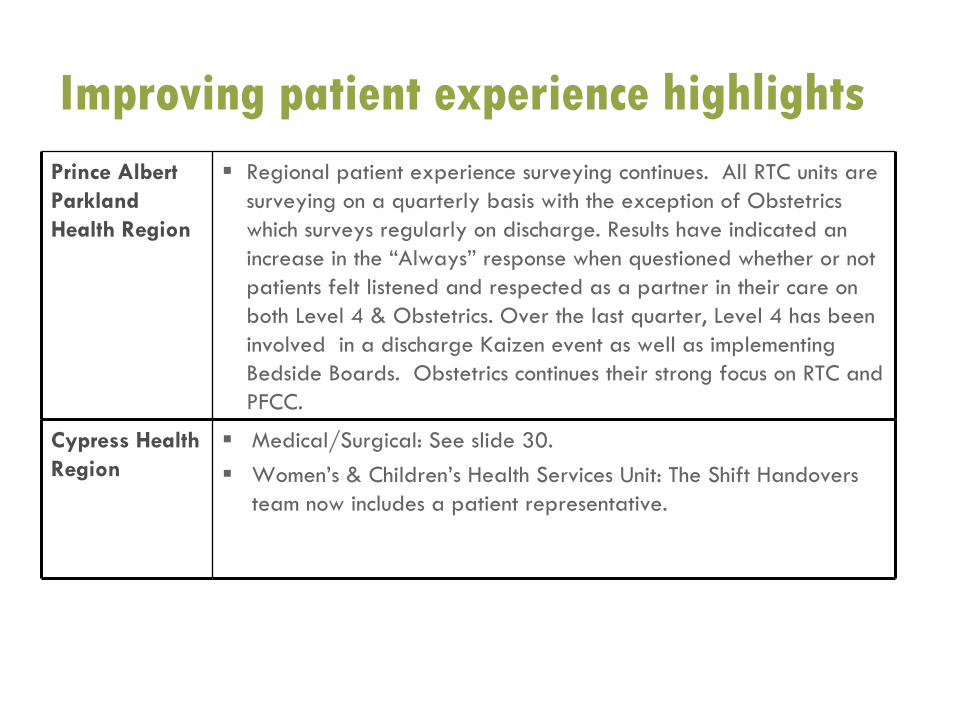
Improving patient experience highlightsPrince Albert Parkland Health Region
Regional patient experience surveying continues. All RTC units are surveying on a quarterly basis with the exception of Obstetrics which surveys regularly on discharge. Results have indicated an increase in the “Always” response when questioned whether or not patients felt listened and respected as a partner in their care on both Level 4 & Obstetrics. Over the last quarter, Level 4 has been involved in a discharge Kaizen event as well as implementing Bedside Boards. Obstetrics continues their strong focus on RTC and PFCC.
Cypress Health Region
Medical/Surgical: See slide 30.Women’s & Children’s Health Services Unit: The Shift Handovers team now includes a patient representative.
Improving patient experience –
Unit A, St. Joseph’s Hospital, Estevan, SCHR
Improving patient experience –
6000, RUH, SHR
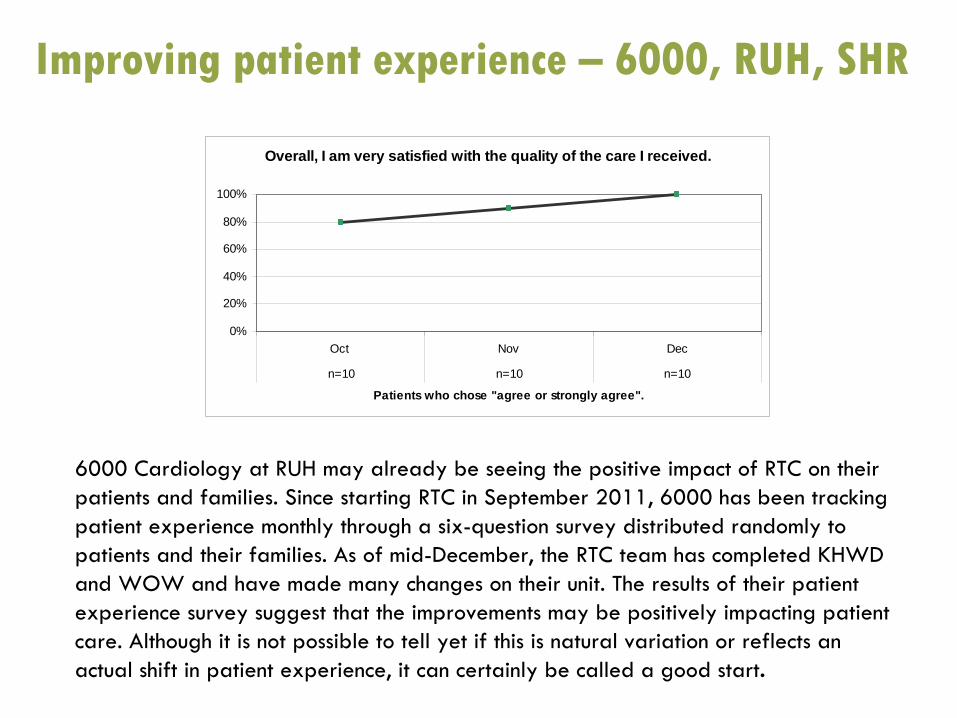
Overall, I am very satisfied with the quality of the care I received.
0%
20%
40%
60%
80%
100%
Oct Nov Dec
n=10 n=10 n=10
Patients who chose "agree or strongly agree".
6000 Cardiology at RUH may already be seeing the positive impact
of RTC on their patients and families. Since starting RTC in September 2011, 6000 has been tracking patient experience monthly through a six-question survey distributed randomly to patients and their families. As of mid-December, the RTC team has completed KHWD and WOW and have made many changes on their unit. The results of
their patient experience survey suggest that the improvements may be positively impacting patient care. Although it is not possible to tell yet if this is natural
variation or reflects an actual shift in patient experience, it can certainly be called a
good start.
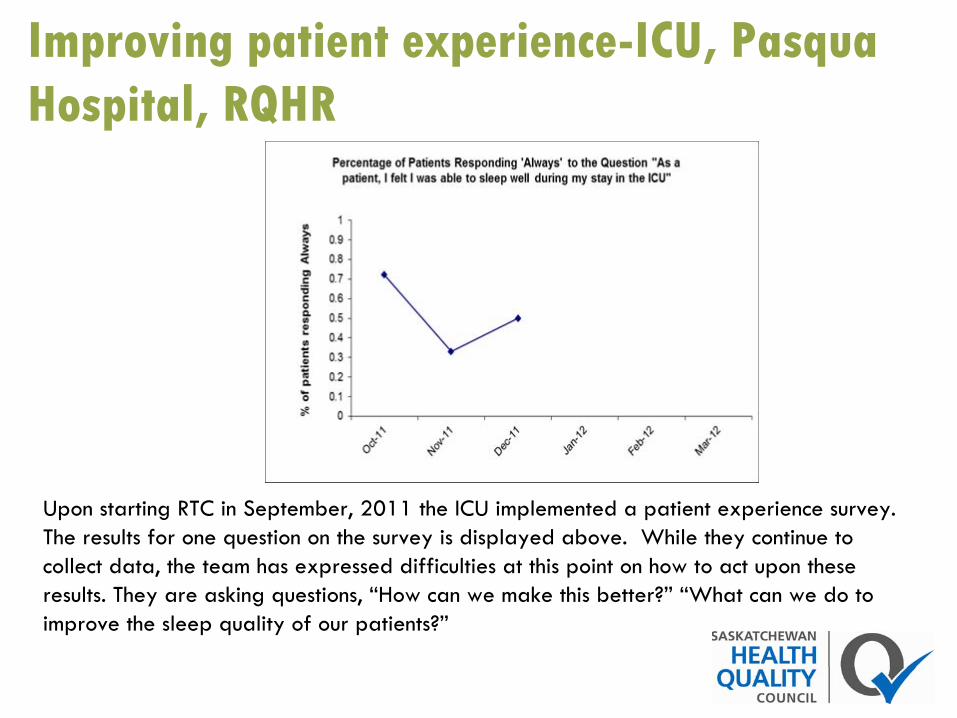
Improving patient experience-ICU, Pasqua Hospital, RQHR
Upon starting RTC in September, 2011 the ICU implemented a patient experience survey. The results for one question on the survey is displayed above. While they continue to collect data, the team has expressed difficulties at this point on how to act upon these results. They are asking questions, “How can we make this better?”
“What can we do to improve the sleep quality of our patients?”
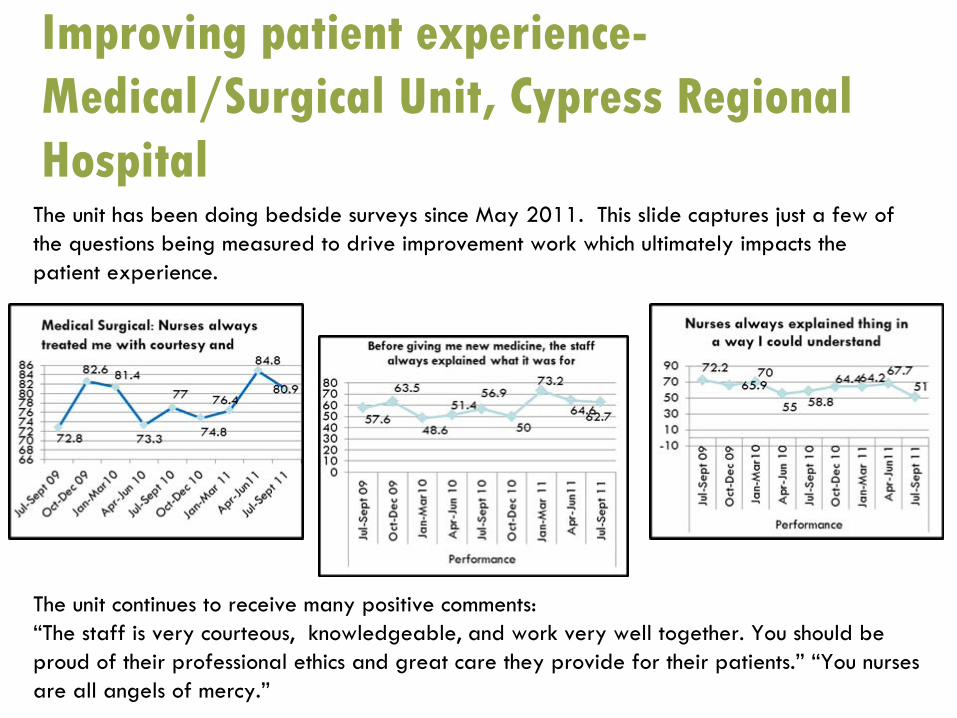
Improving patient experience- Medical/Surgical Unit, Cypress Regional
HospitalThe unit has been doing bedside surveys since May 2011. This slide captures just a few of the questions being measured to drive improvement work which ultimately impacts the patient experience.
The unit continues to receive many positive comments:“The staff is very courteous, knowledgeable, and work very well together. You should be proud of their professional ethics and great care they provide for their patients.”
“You nurses are all angels of mercy.”
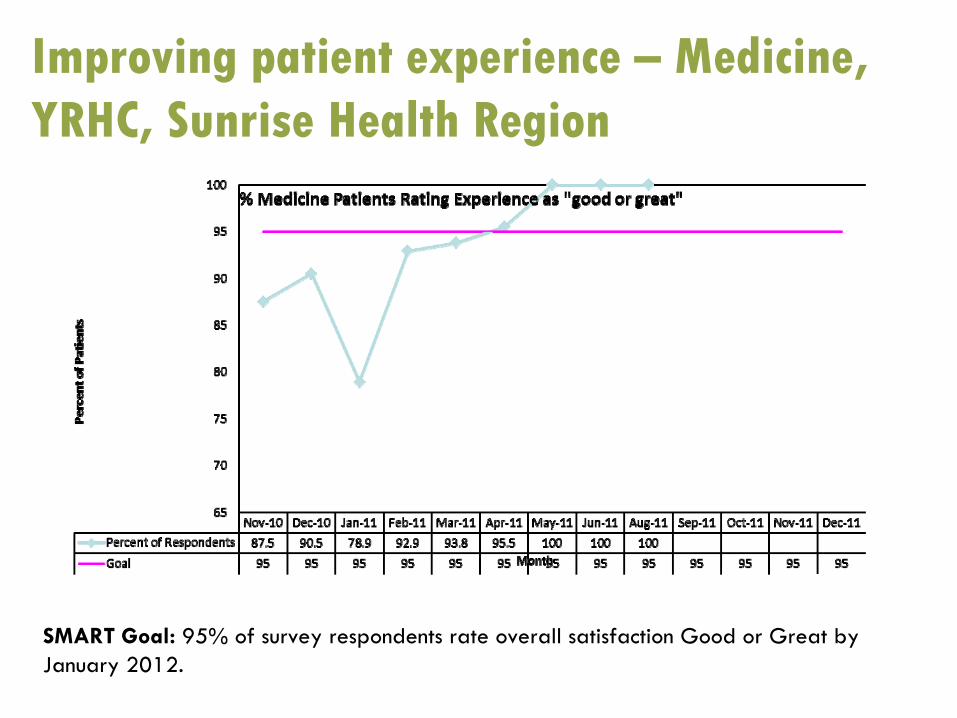
Improving patient experience –
Medicine, YRHC, Sunrise Health Region
SMART Goal: 95% of survey respondents rate overall satisfaction Good or Great by January 2012.
Improving staff well-being highlights
Cypress Health Region
Medical/Surgical: Continue with staff surveys. Staff provided feedback to the Medicines team: "It's great to finally see progress and improvements happening instead of just talking about it”.Women’s & Children’s Health Services: see slide 35.
Sun Country Health Region
St. Joseph’s Hospital – Maternity – staff satisfaction surveys were distributed to staff via pay stubs with a 50% completion rate. The results have been tallied and displayed graphically. The team plans to review the results, post to the RTC Board and discuss with staff to determine how to improve staff well-being. The team also plans to review the survey to determine if the right questions are being asked for future work.
Improving staff well-being highlightsPrince Albert Parkland Health Region
• SMART Goal: PAPHR RTC wards will decrease their sick time by 5% each fiscal quarter: Mar, Jun, Sept, Dec of 2012.
• Regionally, the Employee Health Department, has implemented an Attendance Management Program to assist in achieving this goal.
Heartland Health Region
Outlook Health Centre, Acute Care - The annual staff satisfaction survey will be distributed in January 2012. The KHWD team is hopeful that with implemented improvements including bedside charting and thereduction of interruptions during med times, staff satisfaction will have been positively impacted.Qualitatively, two new nursing staff expressed their immediate support and enthusiasm for bedside charting, when they learned, during their orientation, that the site has adopted this practice.
Prairie North Health Region
Sask. Hospital – focusing on staff wellness and Mental Health First Aid. Very aware of violence in workplace, violence prevention, workers’compensation issues and sick time.
Improving staff well-being highlightsSaskatoon Health Region
See slide 36.
Sunrise Health Region
Stores personnel have commented on a regular basis how much better it is to stock items in the rooms that have been WOW’d. Staff have indicated concern related to communication and have proposed some solutions that are beginning to be trialled.
Kelsey Trail Health Region
See slide 37.
Five Hills Health Region
Medicine: Staff well-being survey was updated in October and completed in November and December. The primary nursing assignment has impacted the unit and the team believes this is captured by the updated survey. See slide 38.
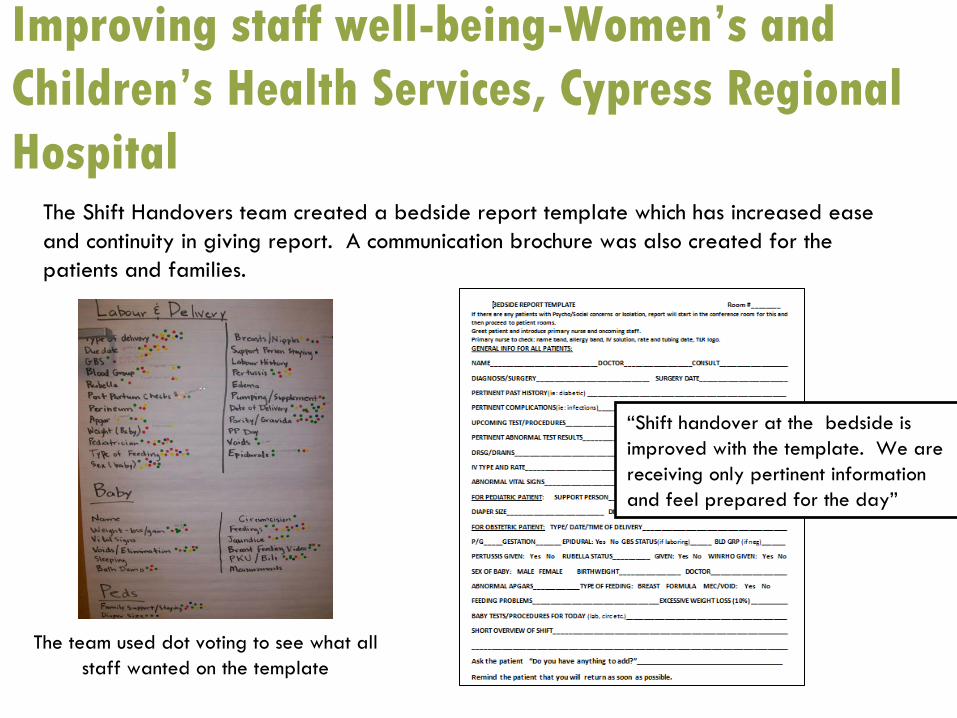
Improving staff well-being-Women’s and Children’s Health Services, Cypress Regional Hospital
The Shift Handovers team created a bedside report template which
has increased ease and continuity in giving report. A communication brochure was also created for the patients and families.
“Shift handover at the bedside is improved with the template. We are receiving only pertinent information and feel prepared for the day”
The team used dot voting to see what all staff wanted on the template
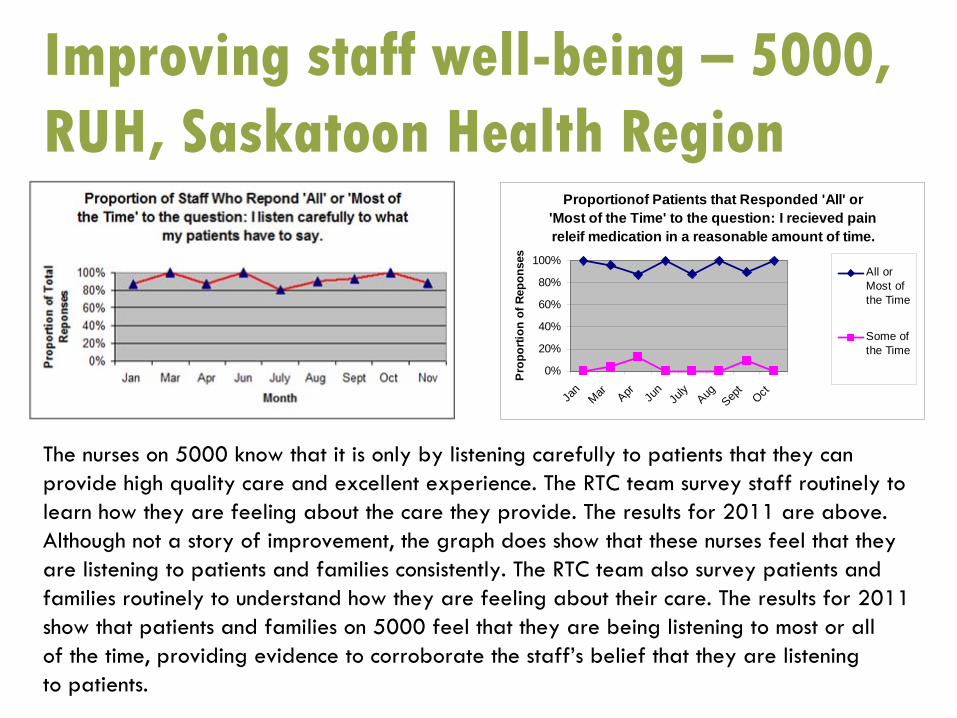
Improving staff well-being –
5000, RUH, Saskatoon Health Region
Proportionof Patients that Responded 'All' or 'Most of the Time' to the question: I recieved pain releif medication in a reasonable amount of time.
0%
20%
40%
60%
80%
100%
Jan
Mar Apr Jun
July
AugSep
tOct
Pro
porti
on o
f Rep
onse
s
All orMost ofthe Time
Some ofthe Time
The nurses on 5000 know that it is only by listening carefully to patients that they can provide high quality care and excellent experience. The RTC team
survey staff routinely to learn how they are feeling about the care they provide. The results for 2011 are above. Although not a story of improvement, the graph does show that these nurses feel that they are listening to patients and families consistently. The RTC team also survey patients and families routinely to understand how they are feeling about their care. The results for 2011 show that patients and families on 5000 feel that they are being
listening to most or all of the time, providing evidence to corroborate the staff’s belief that they are listening to patients.
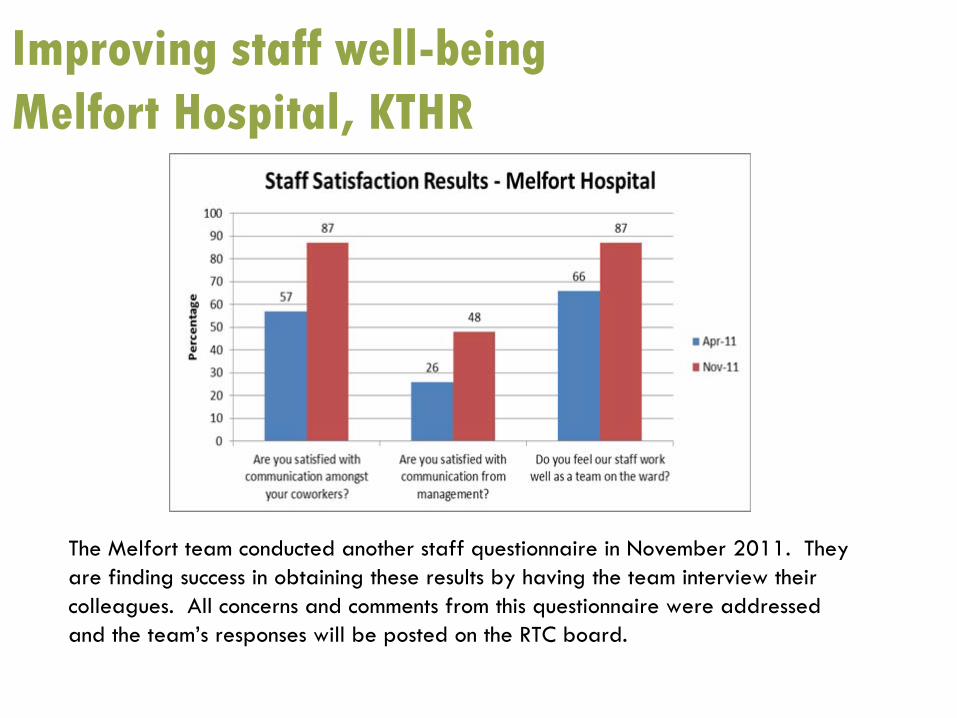
Improving staff well-being Melfort
Hospital, KTHR
The Melfort
team conducted another staff questionnaire in November 2011. They are finding success in obtaining these results by having the team interview their colleagues. All concerns and comments from this questionnaire were addressed and the team’s responses will be posted on the RTC board.
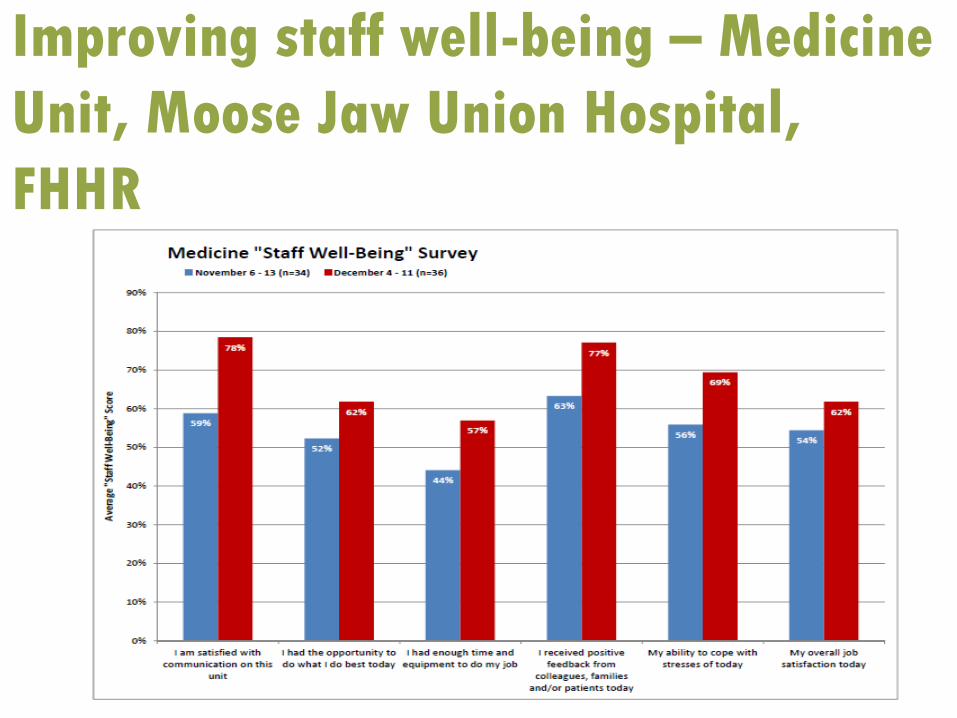
Improving staff well-being –
Medicine Unit, Moose Jaw Union Hospital, FHHR
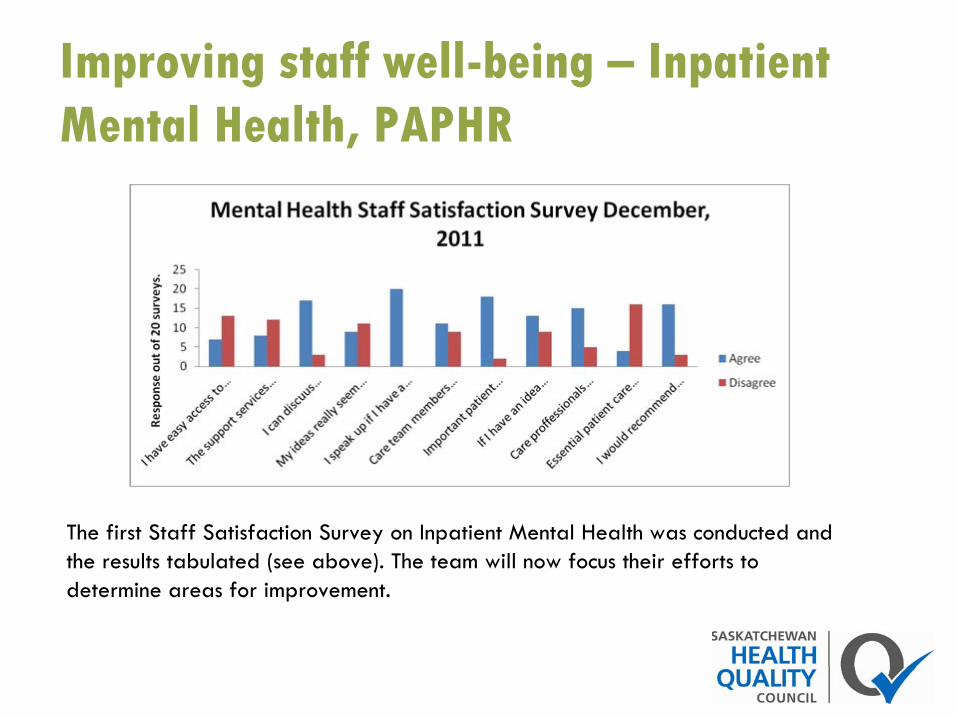
Improving staff well-being –
Inpatient Mental Health, PAPHR
The first Staff Satisfaction Survey on Inpatient Mental Health
was conducted and the results tabulated (see above). The team will now focus their
efforts to determine areas for improvement.
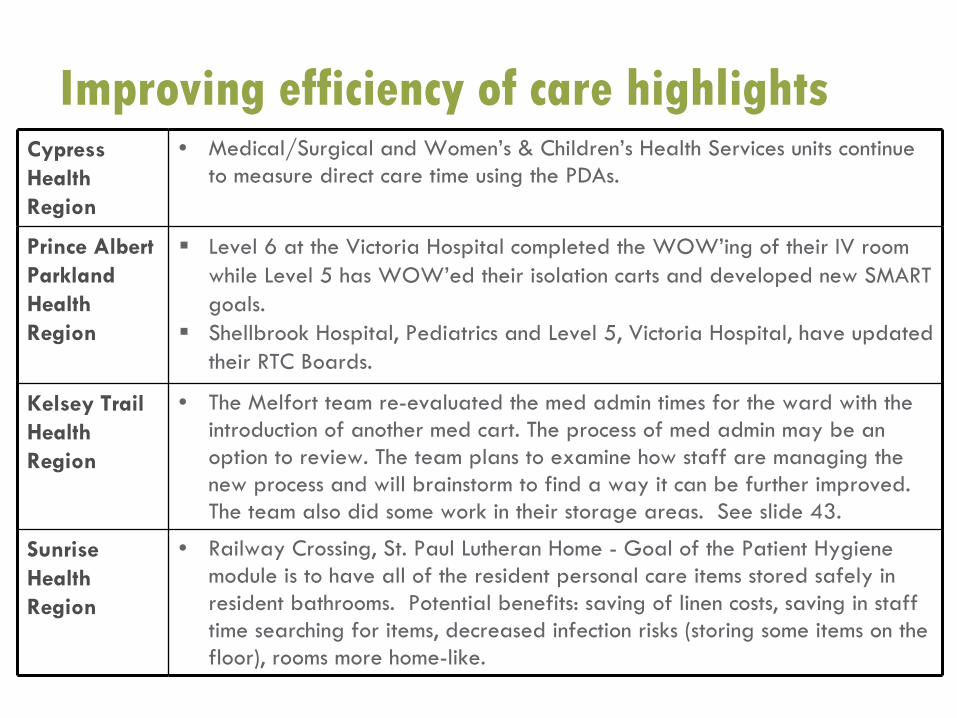
Cypress Health Region
• Medical/Surgical and Women’s & Children’s Health Services units continue to measure direct care time using the PDAs.
Prince Albert Parkland Health Region
Level 6 at the Victoria Hospital completed the WOW’ing of their IV room while Level 5 has WOW’ed their isolation carts and developed new SMART goals. Shellbrook Hospital, Pediatrics and Level 5, Victoria Hospital, have updated their RTC Boards.
Kelsey Trail Health Region
• The Melfort
team re-evaluated the med admin times for the ward with the introduction of another med cart. The process of med admin may be an option to review. The team plans to examine how staff are managing the new process and will brainstorm to find a way it can be further improved. The team also did some work in their storage areas. See slide 43.
Sunrise Health Region
• Railway Crossing, St. Paul Lutheran Home -
Goal of the Patient Hygiene module is to have all of the resident personal care items stored
safely in resident bathrooms. Potential benefits: saving of linen costs, saving in staff time searching for items, decreased infection risks (storing some items on the floor), rooms more home-like.
Improving efficiency of care highlights
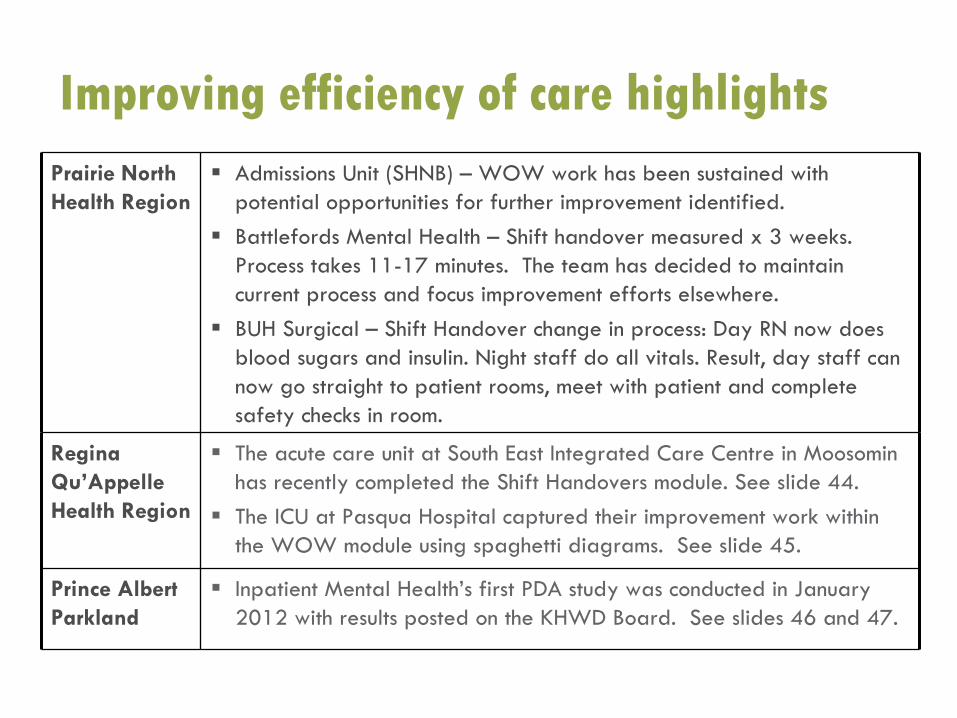
Prairie North Health Region
Admissions Unit (SHNB) – WOW work has been sustained with potential opportunities for further improvement identified.Battlefords Mental Health – Shift handover measured x 3 weeks. Process takes 11-17 minutes. The team has decided to maintain current process and focus improvement efforts elsewhere. BUH Surgical – Shift Handover change in process: Day RN now does blood sugars and insulin. Night staff do all vitals. Result, day staff can now go straight to patient rooms, meet with patient and completesafety checks in room.
Regina Qu’Appelle Health Region
The acute care unit at South East Integrated Care Centre in Moosominhas recently completed the Shift Handovers module. See slide 44.The ICU at Pasqua Hospital captured their improvement work within the WOW module using spaghetti diagrams. See slide 45.
Prince Albert Parkland
Inpatient Mental Health’s first PDA study was conducted in January 2012 with results posted on the KHWD Board. See slides 46 and 47.
Improving efficiency of care highlights
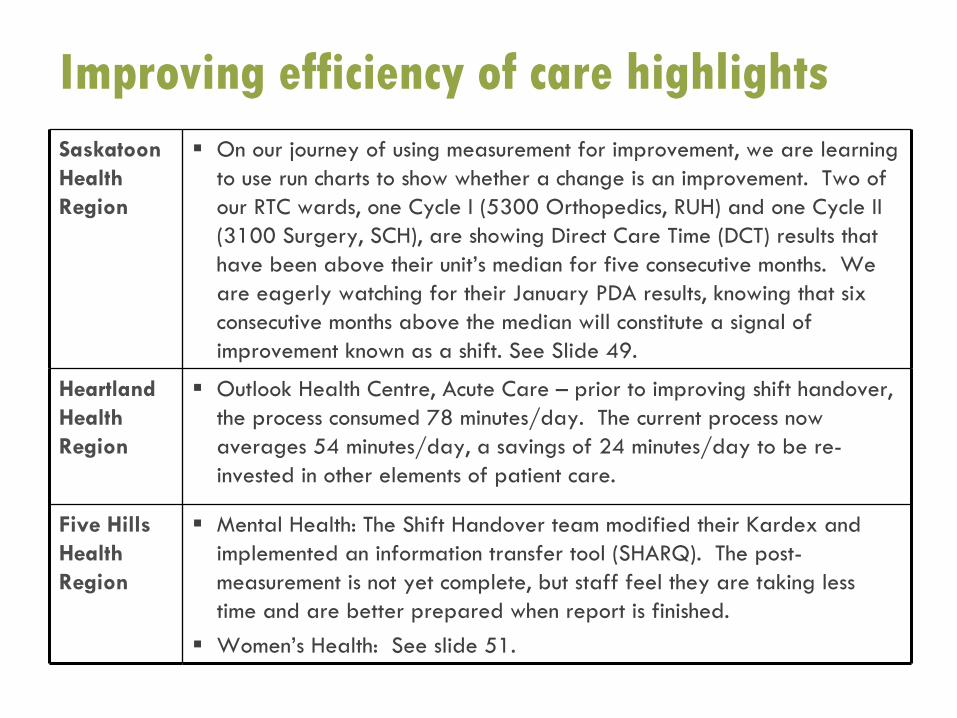
Saskatoon Health Region
On our journey of using measurement for improvement, we are learning to use run charts to show whether a change is an improvement. Two of our RTC wards, one Cycle I (5300 Orthopedics, RUH) and one Cycle II (3100 Surgery, SCH), are showing Direct Care Time (DCT) results that have been above their unit’s median for five consecutive months. We are eagerly watching for their January PDA results, knowing that six consecutive months above the median will constitute a signal of improvement known as a shift. See Slide 49.
Heartland Health Region
Outlook Health Centre, Acute Care – prior to improving shift handover, the process consumed 78 minutes/day. The current process now averages 54 minutes/day, a savings of 24 minutes/day to be re-invested in other elements of patient care.
Five Hills Health Region
Mental Health: The Shift Handover team modified their Kardex and implemented an information transfer tool (SHARQ). The post-measurement is not yet complete, but staff feel they are taking less time and are better prepared when report is finished.Women’s Health: See slide 51.
Improving efficiency of care highlights
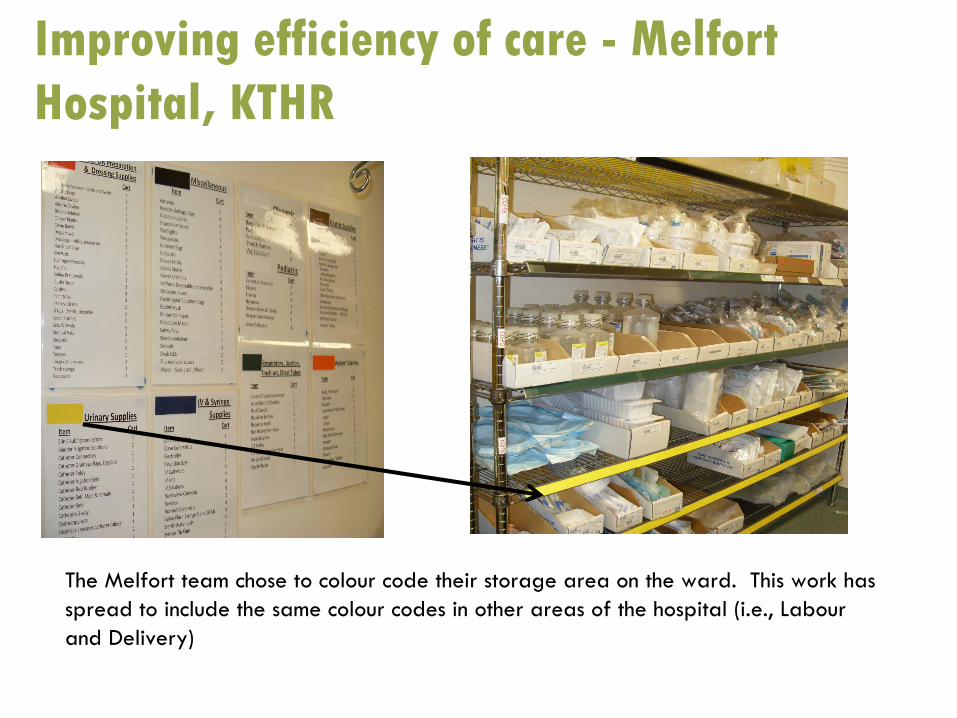
Improving efficiency of care -
Melfort Hospital, KTHR
The Melfort
team chose to colour code their storage area on the ward. This
work has spread to include the same colour codes in other areas of the hospital (i.e., Labour and Delivery)
Improving efficiency of care-Acute Care Unit, SICC, Moosomin, RQHR
The unit recently completed the Shift Handovers module. Prior to tackling this module, there were concerns regarding the communication around patient care that needed to be addressed as well as the time required to give report.
Initially, the average time for report was 37
minutes.
The unit trialed multiple report sheets and verbal vs. taped report. With each PDSA cycle, the unit continued to time report and decreased the time to 25
minutes.
After many small tests of change the unit decided on using a taped report in conjunction with a detailed report sheet. The amount of time spent on report was
reduced to an average of 16 minutes!
SAVINGS??
The unit reduced report time by 21 minutes. This translates to an additional 255 hours per year to spend with patients!
Each shift is relieved in a timelier manner and seems to have alleviated many concerns regarding communication of patient care. The unit plans on continuing PDSA cycles to ensure there is adequate and accurate information received in handover and that the report sheet is working the way it was intended.
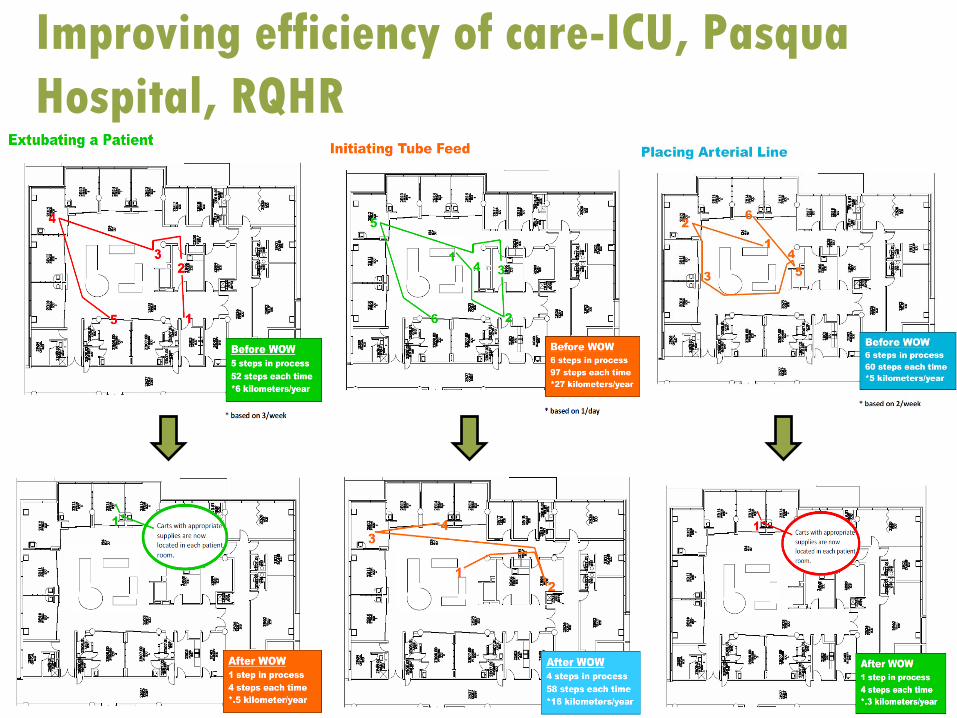
Improving efficiency of care-ICU, Pasqua Hospital, RQHR
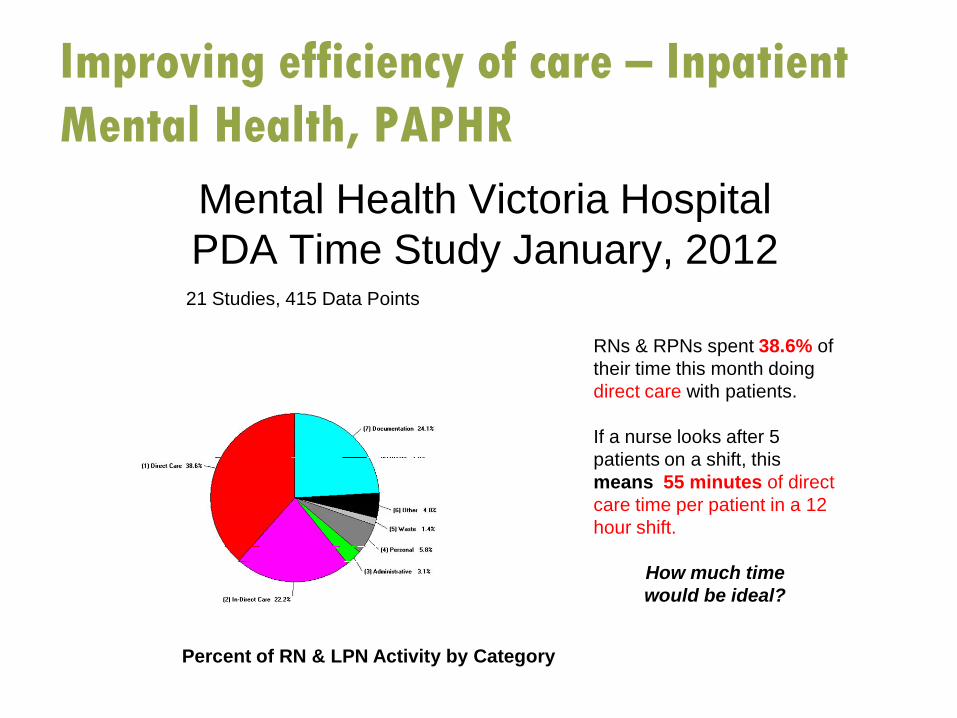
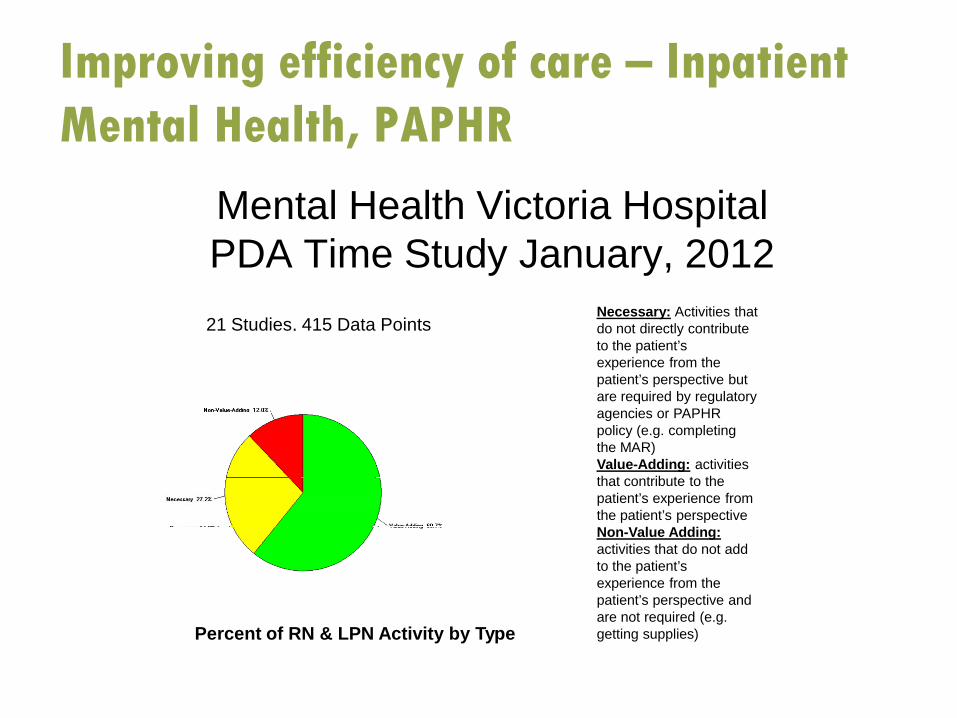
Mental Health Victoria HospitalPDA Time Study January, 2012
21 Studies, 415 Data Points
Percent of RN & LPN Activity by Category
RNs & RPNs spent 38.6% of their time this month doing direct care with patients.
If a nurse looks after 5 patients on a shift, thismeans 55 minutes of direct care time per patient in a 12 hour shift.
How much time would be ideal?
Improving efficiency of care –
Inpatient Mental Health, PAPHR
Improving efficiency of care –
Inpatient Mental Health, PAPHR
Mental Health Victoria HospitalPDA Time Study January, 201221 Studies, 415 Data Points
Necessary: Activities that do not directly contribute to the patient’s experience from the patient’s perspective but are required by regulatory agencies or PAPHR policy (e.g. completing the MAR)Value-Adding: activities that contribute to the patient’s experience from the patient’s perspectiveNon-Value Adding:activities that do not add to the patient’s experience from the patient’s perspective and are not required (e.g. getting supplies)Percent of RN & LPN Activity by Type
Improving efficiency of care, Victoria Hospital, PAPHR
Obstetrics, Victoria Hospital, PSAG Work
The development of PSAG concepts for discharge planning has been completed throughout Levels 4, 5 and 6 at the Victoria Hospital.
Obstetrics is trialing a new nursery PSAG sheet as well as starting to use some bedside boards.
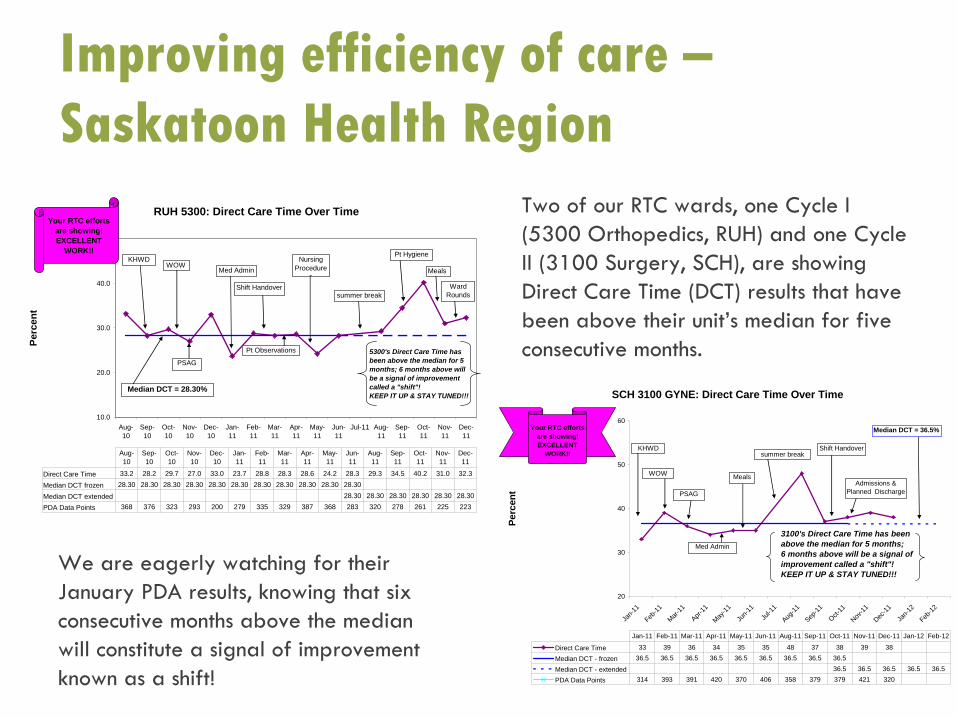
Improving efficiency of care – Saskatoon Health Region
RUH 5300: Direct Care Time Over Time
10.0
20.0
30.0
40.0
50.0
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Jul-11 Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
Perc
ent
Direct Care Time 33.2 28.2 29.7 27.0 33.0 23.7 28.8 28.3 28.6 24.2 28.3 29.3 34.5 40.2 31.0 32.3
Median DCT frozen 28.30 28.30 28.30 28.30 28.30 28.30 28.30 28.30 28.30 28.30 28.30
Median DCT extended 28.30 28.30 28.30 28.30 28.30 28.30
PDA Data Points 368 376 323 293 200 279 335 329 387 368 283 320 278 261 225 223
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-11
Feb-11
Mar-11
Apr-11
May-11
Jun-11
Aug-11
Sep-11
Oct-11
Nov-11
Dec-11
KHWDWOW
PSAG
Med Admin
Shift Handover
Pt Observations
Nursing Procedure
s
Pt Hygiene
Meals
Ward Roundssummer break
Median DCT = 28.30%
5300's Direct Care Time hasbeen above the median for 5months; 6 months above will be a signal of improvement called a "shift"! KEEP IT UP & STAY TUNED!!!
Your RTC efforts are showing!EXCELLENT
WORK!!
SCH 3100 GYNE: Direct Care Time Over Time
20
30
40
50
60
Jan-1
1Feb
-11Mar-
11
Apr-11
May-11
Jun-1
1
Jul-1
1Aug
-11Sep
-11Oct-
11Nov
-11Dec
-11Ja
n-12
Feb-12
Perc
ent
Direct Care Time 33 39 36 34 35 35 48 37 38 39 38
Median DCT - frozen 36.5 36.5 36.5 36.5 36.5 36.5 36.5 36.5 36.5
Median DCT - extended 36.5 36.5 36.5 36.5 36.5
PDA Data Points 314 393 391 420 370 406 358 379 379 421 320
Jan-11 Feb-11 Mar-11 Apr-11 May-11 Jun-11 Aug-11 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12
Median DCT = 36.5%
KHWD
WOW
PSAG
Med Admin
Meals
Shift Handover
Admissions & Planned Discharge
summer break
3100's Direct Care Time has been above the median for 5 months; 6 months above will be a signal of improvement called a "shift"!KEEP IT UP & STAY TUNED!!!
Your RTC efforts are showing!EXCELLENT
WORK!!
Two of our RTC wards, one Cycle I (5300 Orthopedics, RUH) and one Cycle II (3100 Surgery, SCH), are showing Direct Care Time (DCT) results that have been above their unit’s median for five consecutive months.
We are eagerly watching for their January PDA results, knowing that six consecutive months above the median will constitute a signal of improvement known as a shift!
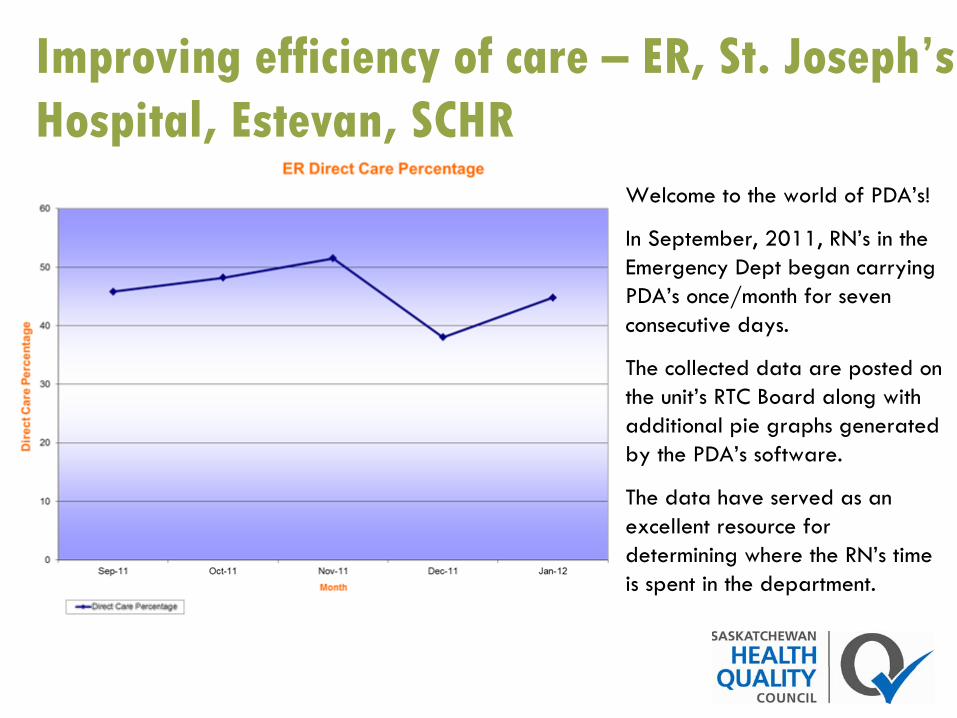
Improving efficiency of care –
ER, St. Joseph’s Hospital, Estevan, SCHR
Welcome to the world of PDA’s!
In September, 2011, RN’s in the Emergency Dept began carrying PDA’s once/month for seven consecutive days.
The collected data are posted on the unit’s RTC Board along with additional pie graphs generated by the PDA’s software.
The data have served as an excellent resource for determining where the RN’s time is spent in the department.
Improving efficiency of care -
Women’s Health Unit, Moose Jaw Union Hospital, FHHR
The unit recognized that a significant amount of time was being spent performing live (in-person) infant care teaching sessions. In an effort to reduce this time, the team created an ‘Infant Care’
video to teach parents how to care for their new infant.
Staff will provide additional teaching if the mother does not feel confident in the new information via video and/or if the mother has additional questions within regards to infant care.
In addition to potential time savings (data not yet available), the video also ensures that every mother on the unit will receive consistent information.
A survey has been created to get new parents’
feedback on the Infant Care video to ensure it is meeting the parents’
needs.
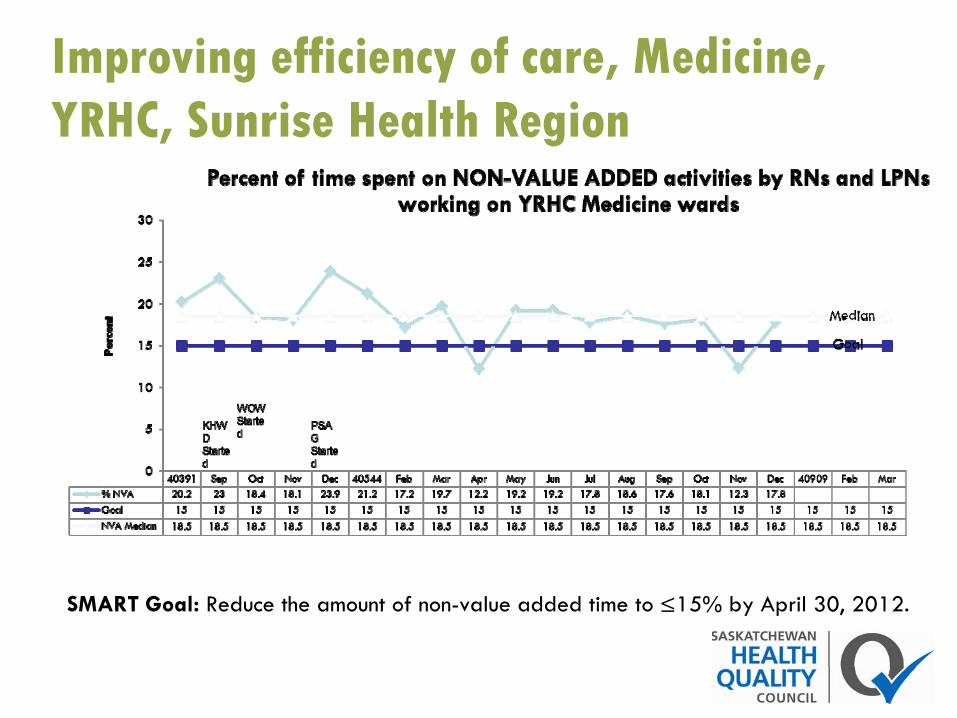
Improving efficiency of care, Medicine, YRHC, Sunrise Health Region
SMART Goal: Reduce the amount of non-value added time to ≤15% by April 30, 2012.
Lessons learned
To capture lessons learned, HQC poses four
questions:
•
What went well this quarter?•
What didn’t go well this quarter?
•
If we had the last quarter to do over, we would have…
•
Any additional comments?
What went well this quarter? Comments from reports submitted by the regions:
Women’s and Children’s Health Services are making great strides in all their modules and look forward to starting the meals module.Template was created to assist staff in giving shift report at bedside.Including a patient representative on the Shift Handovers team.Medicine team has come up with 50 potential improvement ideas and are busy starting to implement. A few quick wins have given energy and excitement to the team and staff.WOW module completed with great interest from staff, even after some initial hesitation!Communication with maintenance for WOW module.Communication with team to keep staff engaged and working well as a team.Buy-in from staff for complete re-organization of storage room.Unit orientation has been expanded to include more RTC training which gives new staff a better introduction to what RTC is all about.
What went well this quarter? • “As time progresses, the proven sustainability of several initiatives, such as the shift
handover improvements, the WOW improvements and the success of the patient bedside communication boards is rewarding to see. t was exciting to see the initial results from these improvements, but to see these results prevail over the test of time brings a new sense of accomplishment to the RTC improvements completed to date. The sustainability of these improvements is deeply satisfying for the RTC Project Team”
(Outlook Health Centre, Acute Care). • The staff on Women’s Health “think differently”! Being part of project teams has
empowered the nursing staff to make necessary changes to their environment, making processes more efficient (Moose Jaw Union Hospital).
• Some of the project teams were relying on the Ward Lead to carry
out all the required tasks for the projects. This caused projects to be delayed and, as a result, RTC enthusiasm dropped. The teams met and clarified everyone’s responsibilities for all the project items. This allowed projects to be completed and enthusiasm has improved!
• Buy-in from most departments besides nursing seems to be great!; Positive feedback from families stopping and looking at the (RTC) board (Arcola Health Centre).

What went well this quarter? • Meals module started –
there is excitement about the patients first initiative; great buy-in in creation of teams –
people are wanting to participate; Stop Infections Now! –
data will be displayed on RTC boards; PDAs
now showing consistently between 35 and 36% direct care time; Medication administration focus group –
contributions towards the medication module (St. Joseph’s Hospital, Estevan, Unit A).
• People are excited for training in January and wanting to get going on PSAG; Team open to working on WOW –
they want to be part of the change so are signing up (St. Joseph’s Hospital, Estevan, Emergency).
• The team is excited and motivated; there has been a lot of participation in the creation and selection of the unit’s vision; a PDA start date has been selected; we are planning our RTC Kick Off Party; we have been gathering materials for our RTC Board (St. Joseph’s Hospital; Estevan, Long Term Care).
• Staff satisfaction survey was developed and distributed with a good return rate; the patient satisfaction survey has been developed and plans are being determined for administration; a policy has been developed for sleeping with baby; dot voting is complete for WOW areas (St. Joseph’s Hospital; Estevan, Maternity).
• Staff RTC Kick-off; Unveiling of the RTC Board; Staff buy-in (Kipling).• Maintaining improvement initiatives–
rooms that were WOW’d, Day at a Glance Board, silencing call bells; Three teams at Yorkton Regional Health Centre hold bi-
weekly meetings to ensure good communication about RTC in the facility. Second South had a change in their ward lead and now have two RN’s co-leading –
lots of enthusiasm and energy (Sunrise).
What went well this quarter? • Weekly RTC Meetings continuing; working on medication module –
working with pharmacist from Weyburn
General Hospital on medication reviews, have timed medication administration and interruptions, staff and Lean Specialist completed medications process mapping; Falls –
KHWD –
going to trial the Edmundson
risk assessment tool for psychiatric acute care; small changes to patient and staff satisfaction surveys; PSAG –
ordered more pictograms including a flight risk, aggression, sleep, smoking; audits are ongoing –
have removed some audits from roster (SCHR, Inpatient Mental Health).
• I think that the re-energizer meetings were done well and the areas have a renewed vision for 2012 (Victoria Hospital, PAPHR).
• Establishment of weekly meetings; set goals for patient experience, staff well-being, patient safety and reliability of care and for efficiency of care; started collecting data to align with our goals (Inpatient Mental Health, PAPHR).
• Great enthusiasm from new RTC teams, willingness to discuss problems and improvement ideas. Teamwork excellent. New managers willing to
let teams go to it!; PDA data coming together to make run charts that are more meaningful for teams who have been working more than a few months now; WOW: Effective, not perfect, but done well. Very motivational and visual for staff. Need to keep going with more! (PNRHA).
What went well this quarter? • Introduction of data early on in KHWD. Patient safety data were provided to each new
Cycle 3 team in an organized, meaningful way. As a result, teams
were better informed and able to select the most important safety indicator for their
patients. • Facilitators have made improvements in how the WOW concepts are introduced to new
teams. The introductory discussion is more clearly focuses on aspects of lean improvement. Discussion with teams includes the elements of 5Sing, the importance of standardized work, and the role of visual management. As a result, team members have a better understanding of these improvement methods.
• Including physician leaders in the Pyramid Visit process: Pyramid visits are a key component of the RTC within the Saskatoon Health Region. Since 2009, an SHR senior leader has visited every RTC unit every month. Our experience is
that this is a valuable experience for both leaders and staff. Beginning in February, 2012, physician leaders will also be making these Pyramid Visits on 6000 Cardiology, 6100 Oncology and 3100, Surgery, SCH. The goal is to inform and more directly involve physician partners in the quality improvement work on these units.
• Although time spent on shift handover was at a minimum, the nursing staff modified the Kardex
to further decrease the time spent in report.• Entire unit was involved in updating the Kardex. This resulted in having a tool that
meets everyone’s needs. Staff feel that there is more focus on key areas which impact patient care and their ability to provide that care.
What didn’t go well this quarter? Comments from reports submitted by the regions:
Continue to struggle with how to get team members to attend meetings.Auditing-staff are feeling overwhelmed by the number of audits that have to be required and feeling like it is added work. Need to get creative in ways to address these concerns.Difficulty in sustaining changes implemented.Communication with team and receiving ‘pushback’ regarding meetings around the board.Difficult to cover staff requirements and this is an ongoing challenge.The site continues to operate with a vacancy in one of the key leadership positions, the Assistant Head Nurse (AHN). While the Care Team Manager, Charge Nurses and front-line staff continue to do an exceptional job in stepping up to cover this vacancy, there is still a notable void in the overall team membership. The RTC Project Teams have provided a tremendous amount of leadership, guidance and support in moving ahead on various improvement initiatives. Nonetheless, an addition of an AHN to the team would add more capacity, in many ways, to help plan, design, implement, test, and refine so much of the improvement work completed to date and lighten the load across the RTC teams.
What didn’t go well this quarter? • Direct care time has not been measured for the past few quarters. This is being
looked at and will be measured in the next quarter.• Struggled with team members’
shift schedules which resulted in RTC meetings being delayed.
• Selected largest room for WOW.• Board meetings –
have no one to lead the meeting and invited guests showed up with no meeting.
• PDAs
–
still have problems with getting staff involved –
Lean training has helped.• Lost some PDA data –
almost 1 week.• Need a PDA expert –
facilitator can play a key role.• Because of small patient load and staff size, data collection has been challenging.• Small board meetings.• Meals module was difficult because it doesn’t fit how meals are delivered.• Medication administration was a huge change –
was difficult to communicate to everyone. Have taken pictures to illustrate the process –
keeping up with the audit.
What didn’t go well this quarter? Staff didn’t receive enough information to go ahead with projects – for example, how to purchase new cabinets and the amount acceptable to spend.Need to improve communication.RTC teams often voice that they feel like they aren’t keeping up or progressing fast enough. Graphs not kept up in places, need to look at what is being measured, is it still meaningful? Ask the questions again: What do we want to know about?PDAs can be utilized more. Teams need to see the results of their work over time.Frequent visits from measurement coordinators/improvement facilitators, leadership needs to occur in order to continue the communication throughout the system. Informal conversations can stimulate movement towards quality improvement along with formal SMART goals and measurement.Maintenance time to install the shelves has delayed the Patient Hygiene module implementation.Continue to experience challenges in staffing and management stability.
What didn’t go well this quarter? • Changes in managers and staff continue to present a challenge in
terms of maintaining the knowledge capacity of quality improvement at the
front line. RTC team members learn QI tools and processes. With changes in team membership, it is challenging to continually refresh this knowledge base.
• The shift to a lean management system at the provincial and regional level, presents a significant opportunity for change, but planning and deployment of this new initiative takes time. Although momentum on individual units remains strong, the shift in QI strategy does have an effect. Naturally, there is uncertainty about how RTC will be integrated into this new system that distracts our focus
and energy. • While teams were participating in the PDA data collection well in the spring of
2011, the willingness to carry the PDAs
has decreased on most units through the fall. Staff say that they are too busy, that the PDAs
are an interruption and that they just don’t want to carry them. There is a sense that resistance to carrying the devices is on the rise. This is a concern given the expectation of continuing to submit data monthly till 2013. Barb Wieler, Measurement Coordinator, has been working with teams to ensure that there is a high level of comfort, confidence and understanding of how to use the devices, but this has not translated into a higher level of engagement on most units. The SHR is committed to using the PDAs
on all of the acute care units and SUN is supportive of this initiative. The RTC team and senior leadership continue to actively seeking ideas from others about how to positively influence the adoption of PDAs.
If we had the last quarter to do over, we would have…
Comments from reports submitted by the regions:• Done the two modules (Patient Hygiene and Shift Handovers) at a slower, more
sustainable pace (in conjunction with other improvement initiatives being rolled out in the province).
• Spent more up-front time forecasting the implications and possible unintended consequences associated with the transfer of charting from the nursing station to the patient bedside. With a more in-depth problem analysis we would have developed a better sense of our current state in relation to charting practices and the impact of the move to the patient bedside, both positive and
negative. The insight garnered through a more thorough problem analysis would have also provided the basis for us to develop targeted, well-designed process, outcome and balancing measures. Our team is interested in assessing the
full impact of bedside charting on our practice and without laying this groundwork upfront we are doing a retrospective analysis. A retrospective look will be
quite helpful, but it would have been better to have benefitted from the insights and lessons stemming from this analysis earlier in the improvement cycle. .

If we had the last quarter to do over, we would have…
Comments from reports submitted by the regions:• Clarified project roles early on in the process so projects could move ahead at a
quicker pace.• Met right after pre-implementation training instead of waiting until after
Christmas to meet.• Started weekly meetings sooner.• Encouraged RTC teams by providing more focus on measurement and progress. • Set more SMART goals!• Replaced the maintenance staff to complete install and also replaced the Ward
Lead to dedicate more time to RTC (if we had sufficient staffing
to do so!).• Put additional administrative supports in place: There is a significant layer of
administrative work that is generated by teams and the speed of the PDSA cycles is in part dependent on a rapid and accurate turn around of data. It is more economical to have administrative staff do this work rather than
those providing direct patient care. We have been challenged to maintain the level and quality of administrative support that teams need to do their best work.
Additional comments from the regions• Kim Hunt, Clinical Nurse Educator (CNE) on 6A at the RGH, joined
the RTC movement within the last six months. The biggest lesson for her is learning the process for improvement. She looks forward to using this process in the future, working at a sustainable pace, and continuing to make improvements with her team!
• Denise Hextall, CNE on 3F Cardiosciences
at RGH and Ashley Hoffort, Clinical Resource Nurse (CRN) for ICU at the Pasqua
expressed the need to continue with the process at a slower and more sustainable pace. It has been expressed that in the attempt to complete modules within a certain timeframe, the ability to sustain and maintain the changes implemented has been difficult.
• RTC is not a “cookie cutter program and it needs to be individualized for each
unit”
–
Darren Entner, CRN for MPICU at RGH.• The Medicine Unit at MJUH has been working very hard this last quarter to re-
establish the RTC program and is seeing some very positive results with project progression and staff morale.
• Staffing is a big issue. We need to schedule RTC teams to do their RTC work, replaced by other staff, so they can concentrate on their RTC work. When RTC teams have dedicated time to meet, they are able to discuss ideas, plan their work, and accomplish amazing things very quickly and efficiently with few interruptions.
Additional comments from the regions• When first initiating change, it is difficult to get people on board. Committee
members have demonstrated success through RTC and this has drawn
other people to join the project who may have initially resisted change. Example, new staff members have joined the Patient Hygiene module team who may have
initially expressed resistance but are aware of the positive changes that may come about and wanted to be part of this module.
• With RQHR being in a seemingly continuous state of over-capacity in recent months, staff is beginning to feel the pressures of change. With a recent introduction of an Emergency Operations Centre (EOC) to deal with the over-capacity situation, staff has had to deal with sudden and unexpected changes such as an increase in hallway beds and non-gender specific rooms, along with attempting to sustain and introduce improvements to improve the patient experience. This has been very difficult for staff and the full effects remain to be seen.
A Final Story: Including patient feedback after discharge to improve care:
Since 2009, 3200 SCH has been working to transform the post-operative care experience by implementing a hip and knee care pathways. One of the unique elements of both the hip and knee pathways is the ability to follow up with patients after discharge. An RN or Advanced Practice Physiotherapist phone each patient 48 to 72 hours after they go home. The information captured from these calls is collated and the results are shared with surgical leadership, managers and staff. The results from November 2010 showed that patients had concerns in three areas: post-discharge pain control, wound care, and constipation. When the leadership team on 3200 heard these concerns, they decided to use the RTC modules and processes to improve patient care in these areas. The RTC team on 3200 used Patient Observations as the vehicle for improving pain care, and Nursing
Procedures to improve patient teaching related to wound care , improve inpatient bowel
care practices, and patient education within this same module. .The team is continuing to work collaboratively with physician providers to ensure that patients have the information and care they need prior to discharge. Very few acute care providers know what happens to patients after discharge. The RTC team and leaders on 3200 have demonstrated that this kind of feedback can be used to improve the in-hospital patient experience. This also shows that collaboration between different disciplines and teams can influence the quality of care for patients beyond their own boundaries. Lastly, the team on 3200 has also demonstrated that the processes and tools of RTC are being applied through multiple tests of change to address issues that are of provincial and regional interest and of real value to patients.
For more information
Kyla Avis, Program DirectorTel: (306)668-8810, ext. [email protected]
Michelle Murphy, QI ConsultantTel: (306)668-8810, ext [email protected]
Chelsea Haley, QI ConsultantTel: (306)668-8810, ext 150 [email protected]
Jennifer Wright, QI ConsultantTel: (306)668-8810, ext [email protected]