Slide 1
Dr. Sreejoy Patnaik
Shanti Omni Super Speciality Hospital Cuttack LAPAROSCOPY IN
UROLOGY
1
LAP- ENDO
History of Lap. UrologyThe first laparoscopic Nephrectomy was
performed in 1990 by Clayman
The procedure had an operative time of seven hours and required
a 1-unit transfusion and a six-day inpatient hospital stay.
Challenges of Uro lap. surgeryTechnically, more
demandingSpecialized teamSlightly more expensive, use of
consumablesAdvantages outweigh the challenges
4
Laparoscopic SurgeryKey hole surgery
Latest development of Urology
Obvious advantages over conventional open surgery
Smaller wound
Less pain
Quicker recovery, discharge, early return to work
5
Laparoscopic Urological SurgeryRevolutionary development in last
2 decades.
Experienced centres
Improves Patients peri-operative quality of life
Provides excellent view due to magnification less tissue trauma
& minimal blood loss.
Approaches The 3 three commonly used approaches are
Transperitoneal approachRetroperitoneal approachHand assisted
approachEndoscopic Procedures
Transperitoneal approachWider availabilityWorking spaceBetter
identification of important landmarksIntestinal Injury ?
Retroperitoneal approachRestricted rapid accessRenal pedicle
identification.Reduce the incidence of ileusInjury to the
intraperitoneal contents
Hand assisted approachImproved tactile feedbackBridge between
open surgeryLap Gelport TMLap Disc TM
ENDOSCOPIC APPROACHESCYSTOSCOPY-
TURP/BNI/TURBT/OIUURETEROSCOPY-RIGID URETETROSCOPY URSFLEXIBLE
URETEROSCOPY- RIRSPCNL- BY RIGID NEPHROSCPEMINI PERC - RENAL
STONES
Laparoscopic Urological ProceduresCommonest procedures performed
:-
Ablative Procedures: Urolithiases:Simple nephrectomy
PyelolithotomyPartial nephrectomy UreterolithomyRenal cyst
marsupilisation CystolithotomyRadical nephrectomy Urachal Cyst
excisionRadical cystectomyRadical prostatectomy
Reconstructive Procedures:PyeloplastyLower ureteric
reconstructionsBoari flap reconstructionUreteric
reimplanation/Psoas hitchIleal ureter implantationOrchipexyDonor
nephrectomy
Simple NephrectomyNon functioning KidneyPre renal transplant
nephrectomy
Transperitoneal approach Pneumoperitoneum - open technique or
closed technique. Ports are inserted in a strategic manner.
Preoperative CT Scan) if done helps in determining the location of
the kidney and deciding the location of port placement. Other
parameters which determine the site of port placement are extent of
truncal obesity and body mass index (BMI).
Positioning
Lateral decubitus positionNear the edge of the tableLower limb
is flexed
Technique
Left side colon is reflectedIliac bifurcationSuperiorly the
splenorenal Renocolic ligamentsIdentify the ureterGonadal
vesselsUreter is lifted Psoas landmark
12
(B) Retroperitoneal approach
Gaur etal15mm incision petit triangleLumbodorsal fasciaBalloon
dilator
(C) Hand assist approach
Insert a non dominantHand assist device is inserted Right lower
quadrant midway between umbilicus and anteriorsuperior iliac
Laparoscopic Radical NephrectomyT2 & T3a tumors.T1 tumors
contraindicated with IVC thrombus
Technique
TransperitonealLumbar & adrenal veins are doubly clipped
& cut.
Results
Advantage short hospitalLow analgesiaComparableOpen laparoscopic
approach is a standard of care in T1 & T2. Renal thrombus is
feasible
Laparoscopic partial nephrectomy
Small renal masses Lesions in a solitary kidneyBilateral renal
lesionsTechnique- Pneumoperitoneum
- Ports similar to simple nephrectomy
- Ureteric catheter placed per-urethrally - to instill methylene
blue- Identify the pelvicalyceal system prior to suturing- Colon
reflected and the ureter is lifted off the psoas muscle
- Dissection proceeds to the renal hilum- Renal hilum dissected
& satinsky applied - Renal tumor is cut with cautery or
harmonic
- Preferred scissors for excising the tumor should be with wide
jaws.
- Pelvicalyceal system is closed followed by the cortical
defect- An indwelling ureteric catheter or alternatively a double J
stent is placed for 48hours.
15
PyeloplastyPUJ ObstructionRGP prior to positioning the
patient5Fr pigtail catheter is inserted into the pelvicalyceal
system
Technique
30 degree Scope - pelvis is identified bulges outDismembered
Anderson hynes Pyeloplasty is preferred crossing vessel is
suspectedY-V plasty is preferred
The important steps of this procedure are
PyelotomySpatulation of the ureterPyelotomy is closed a 3-0/4-0
vicrylV stitch as anterior layer easier step to start , followed by
posterior layer.
Donor NephrectomyDo no harm to the donor is the dictum
Technique
Port placement mirrors that of simple nephrectomyCT angiography
plays a pivotal role for strategic port placement.Ureter should be
lifted of the psoas in toto as an ureterogonadal packet.Dissection
of the artery should be a thermal and should be kept to the
minimum.Topical papvarine instillation on the vessel helps in
relieving spasmUpper pole should be separated from the spleen
securing the adrenal veinGraft should be adequately perfused by
intravenous infusion of mannitiol and furosemide prior to
retrievalRetrive the graft through a pfannesteil incision
Laparoscopic ureteral reimplanationSupine position a 11mm trocar
for camera insertion umbilicusUreter is lifted transected as
distally as possibleThe bladder is filled with 200ml salineLateral
and anterior peritoneum incised a boari flap is preferredSpatulated
ureter and the bladder flap are anastomosed in a tension free
manner with 4-0 polygalactin suturesA stent is kept indwelling for
6weeks after the surgery
Laparoscopic stone removalProcedure performed transperitoneal or
a retroperitoneal approachPlacement of a stent ureteric
catheterUreter lifted of the psoas The ureter is slingedUsing a
cold knife the ureter is incisedSpoon may be used for retrieving
the stoneStone may be entrapped in a bag for removalUreterotomy is
closed with a 3-0 absorbable suture and a drain is placed.
Advanced Laparoscopic Procedures
Laparoscopic ileal interposition
Laparoscopic retroperitoneal lymph node dissections
Laparoscopic radical cystectomy (LRC)Laproendoscopic single site
surgery (LESS)
Simple nephrectomyPyeloplastyReconstructive
proceduresUreteroneocystostomyLESS donor nephrectomyTechnically
feasible procedureSteep learning curve
Robot Assisted Laparoscopic UrologyProstatectomy ,Pyeloplasty,
Nephrectomy & Ureter reconstructionsDonor
nephrectomyAdrenalectomyAdvantages:Robotic platform Da Vinci SiHigh
definition visual magnificationBetter range of motion Additional
arm for retractionA unprecedented range of accuracy and
dexterityIts increased range of freedomProperty of motion
scalingProcedures requiring intracorporeal suturingSmall spaces
pelvisThe cost benefit ratio is likely to be a driving force in
further development and application of this technology
Laparoscopic NephrectomyBenign, non functioning kidneyRenal cell
carcinoma Almost all tumours can be removed laparoscopically
21
Laparoscopic Nephrectomy
LAP - URETEROLITOTOMY
LAP. PYELOLITHOTOMYVIDEO
LAP PARTIAL NEPHRECTOMYVIDEO
LAP RADICAL NEPHRO-URETECTOMYVIDEO
LAP URACHAL CYSTECTOMYVIDEO
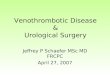
Laparoscopic Prostatectomy5 small incisions
Completely mimick all the principles of open surgery
Extraperitoneal approach, avoiding contact with intestine
28
Laparoscopic Prostatectomy4-5 hours surgery
Less blood loss, minimal blood transfusion requirement
Magnification allowing more accurate dissection and preservation
of continence and erection
Hospital stay of 2nights, early removal of urinary catheter.
29
Laparoscopic radical prostatectomy
Inverted fan shaped manner Endopelvic fascia incisedDorsal vein
securedVas deferens &Dissected secured hem-o-lokThe lateral
detrussor pillars are secured with clipsThe urethra is dissected be
to gain maximum length Posterior reconstruction stich RoccoThe van
velthowen technique (bidirectinal running suture) technique with
3-0 monocrylSatisfactory oncologic outcome
Radical Prostatectomy
31
ROBOTIC PROSTATECTOMY
Laparoscopic Prostatectomy v/s Robotic prostatectomyAssistance
from robot in suturing
3d view
High capital and recurring cost
33
What is new in laparoscopy in urology?Almost all urological
procedures can be done laparoscopically
Reproducible, similar if not better results than open
surgery
What is the standard of care?
Laparoscopic urological surgeriesProcedureStandard of
CareCurrent OpinionLaparoscopic Radical NephrectomyYesProven long
term results for tumour upto 7cmLaparoscopic radical
nephroureterectomyYesReplaces openLaparoscopic marsupilazation of
kidney cystYesReplaces openLaparoscopic adrenalectomyYesReplaces
openLaparoscopic pyeloplastyNot yetVery promising, awaiting long
term results
Laparoscopic urological surgeriesProcedureStandard of
careCurrent opinionLaparoscopic radical prostatectomyNoDivided
(laparoscopic, robotic assisted laparoscopic, open)Laparoscopic
varicocelectomyNoDivided (open microscope)Laparoscopic extra
peritoneal herniorraphyNoPromising, awaiting long term
resultsLaparoscopic ureterolithotomyNoAdvantage over open, but
other options availableLaparoscopic partial nephrectomyNoAt best,
similar to openLaparoscopic radical cystectomyNoAt best, similar to
open
Laparoscopic retroperitoneal lymp node dissection NoPromising,
Development stageLaparoscopic reimplatation of ureterNoEarly
development stageLaparoscopic augmentation cysto plastyNoEarly
development stage
SummarySurgery is moving towards minimally invasive surgery.
Urology - ESWL, Endoscopy, Percutaneous & Laparoscopy.
More than one or a combination of MIS modalities may be
used.
Endoscopic and Per cutaneous procedures almost treat all the
urolithiases, prostatic and bladder diseases.
Robotic Surgery is the future for dealing with Prostate and
Bladder.
37
THANK U FOR YOUR PATIENT HEARING