Embed Size (px)
Citation preview

Communicable
Infectious
and
diseases
IntroductionIntroduction
Patient’s ProfilePatient’s Profile
Physical AssessmentPhysical Assessment
Anatomy and PhysiologyAnatomy and Physiology
PathophysiologyPathophysiology
Medical ManagementMedical Management
Laboratory and DiagnosticsLaboratory and Diagnostics
8
PULMONARY
TUBERCULOSIS
UPH – Dr. Jose G. Tamayo Medical University
COLLEGE OF NURSING STO. Niño, Biñan, Laguna
LEVEL IV
January 2008
Section

INTRODUCTION
TUBERCULOSIS
Is a disease caused by bacteria that attacks the lungs, or any part of the body such as the kidney, spine and brain. If not treated properly, TB can be fatal.
It is spread through the air from one person to another. the bacteria are put into the air when a person with active TB of the lungs or throat coughs or sneezes. People nearby may breathe in these bacteria and become infected.
Mycobacterium Tuberculosis - primarily infective agent
TUBERCULOSIS
Symptoms of Active TB may include:Bad cough that last longer than 2 weeksPain in the chestCoughing up of blood or sputumWeakness or fatigueWeight lossFeverUsually has a positive skin testSweating at nightMay spread TB to othersx-ray or positive sputum smear or culture
RISK FACTORS FOR TB:
Infected with HIV
Close contact with someone who has an active TB
Person without adequate health care
Living in the crowded or unsanitary living conditions
Have been with TB bacteria in the past two years
Infants and young children
People who injected illegal drugs
People with weak immune system
Elderly
Those that were not treated properly for TB in the past
Examination of the lungs by stethoscope can reveal crackles. Enlarge tender lymph nodes may be present in the neck or other areas. Fluids may be detectable around a lung. Clubbing of the fingers or toes may be present.
Test may include:
>chest x-ray >thoracentesis>sputum cultures >bronchoscopy>tuberculin skin test
The goal or treatment for pulmonary tuberculosis is to cure the infection with drugs that fight the tuberculosis bacteria. The initial treatment may involve a combination of many drugs, it is continued until lab tests show which medicine works best. Treatment usually last for six (6) months but longer treatment may be needed for person with AIDS or whose disease responds slowly.

PATIENT’S PROFILE
NAME : Mr.I.RADDRESS : Peter Street,
Dasmariñas CaviteSEX : MaleCIVIL STATUS : MarriedDATE OF BIRTH : September 6, 1972AGE : 36 yrs oldCITIZENSHIP : FilipinoRELIGION : Iglesia ni CristoDATE OF ADMISSION : January 4, 2008TIME OF ADMISSION : 10:55AM
PERSONAL DATA Patient is Mr. I.R, a 36 years old male from Peter St. Dasmariñas Cavite. He is married, an Iglesia ni Cristo. He is a former employee of a printing company for one and a half year, and worked as a financial encoder in a soda factory for five years and currently works as a tricycle driver. He was admitted at University of Perpetual Help Medical Hospital last January 4, 2008 at 10:55am.
CHIEF COMPLAINT Difficulty of Breathing
HISTORY OF PRESENT ILLNESS
Few days Prior to admission. Patient had episode of difficulty of breathing associated with non productive cough, temporarily relieved by Oxygen inhalation. Patient previously admitted in Trecemarteres Hospital, where in the patient was diagnose of PTB, Pneumonia.
2 Days PTA patient seek consultation for follow up to a private Medical Doctor where patient was prescribed home medications. 4 hrs. PTA patient has recurrent difficulty of breathing, patient mentioned to seek consultation at University of Perpetual Help Medical Hospital hence admitted.
PAST MEDICAL HISTORY
- September 1997 patient sought consultation and was diagnosed with PTB- Masinog Hospital - December 16,2007 –Patient was admitted
with the same diagnosis – at Trecemarteres Hospital - Patient has a history of allergy to shrimp paste - No known allergies to drugs
FAMILY HISTORY Mother = (+) HPN (+) PTB (+) DM ( -) CA
Father = (-) HPN (+) PTB (-) DM (-) CA
SOCIAL HISTORY
Patient is a cigarette smoker for 20 pack years, an alcoholic beverage drinker, consumes about 6-8 bottles per drinking spree. The patient’s usual hobbies are drawing, singing and playing billiards.
PHYSICAL ASSESSMENT
General appearance: Vital Signs:
• Thin body build BP=120/80mmHg• Dresses appropriately RR=32cpm• No body odor PR=116bpm• Weak in appearance T=38.1°C
Mental Status:
Conscious and coherentPleasantCooperativeOriented to time place and personUses simple words as means of communication
Skin:
• Color : fair complexion• Uniformity : generally uniform• Skin moisture : present in skin folds
and axilla• Skin turgor : dry skin with poor skin
turgor• Temperature : warm to touch
Nails
•Nail plate : convex curvature, 160° angle
•Nail condition : rough, thick, and brittle
•Nail bed color : brown•Texture : smooth texture•Capillary refill : within 2 seconds
Head and face•Skull : rounded and smooth contour
•Hair texture : black, fine and evenly distributed, silky and resilient, no infection and infestation
•Scalp : fair in complexion, no lesion and tenderness
•Facial movements : symmetric facial movement. Can elevate and lower
eyebrows, close the eyes, smile and puff cheek, show teeth and stick out tongue.
Eyes•Peri-orbital area : thick eyebrows, black in color
•Eyelashes : equally distributed, curled slightly outward
•Eye lids : skin intact, no discharge and discoloration closed symmetrically
•Conjunctiva : pale palpebral conjunctiva Bilateral blink response and symmetric firm eyeballs
•Pupils : equal in size and have both brisk reaction to light and
accommodation, 2-3mm on both right and left
•Iris : flat and round
Ears
Auricles: fair complexion, symmetrical elastic, and mobile when pinch, and
aligned with the outer cantus of the eyes.
NoseWith O2 inhalation at 3-5 lpm via nasal cannula
•External nose: fair complexion, symmetric and not tender
•Nasal septum: intact and in midline
•Nasal cavity: pink colored mucosa
Mouth and Pharynx
•Lips : dark lips, dry mucous membrane
•Teeth : yellowish in color
•Gums : dark in color and moist
•Tongue : in midline, slightly rough with whitish coating, moves freely and non-tender, smooth tongue base with prominent veins.
•Pharynx : pink and smooth
•Uvula : is in midlinePresence of gag reflex
Neck
•Neck muscles : equal in size
•Muscle strength : has resistance to pressureNormal head flexion (chin to chest)Head extension (chin points up)
•Lateral flexion: right and left
•Lateral rotation: right and left
•Trachea: midline
Chest
•Shape : symmetrical
•Spinal alignment : normal
•Breathing Pattern: Rate= Tachypneic Breath sounds= positive
crackles on right lung field
•Heart sounds : normal, no murmur
•Anterior and posterior lung expansion: decreased lung expansion
Abdomen
•Color: fair in complexion
•Contour: symmetrical
•Auscultation: normal bowel sounds, presence of muscles guarding
•Palpation: soft, flat, non-tender
Upper Extremities
No physical deformities noted.
•Muscles strength : normal and has resistance to force
•Pulses : radial and brachial pulses are normal and palpable
•Range of motion: shoulder can extend, abduct, adduct, and rotate
Elbows can flex and extend. Wrist can flex and extend. Phalanges abduct, adduct flex,
and extend. Pronation and supination of the forearms.
•Right arm: with IVF D5 NM x 12 hours
Lower extremities
No physical deformities on both leg noted.
•Pulses: popliteal, posterior tibial and dorsalis pedis are normal and palpable.
•Range of motion: normal on both leg

ANATOMY AND PHYSIOLOGY
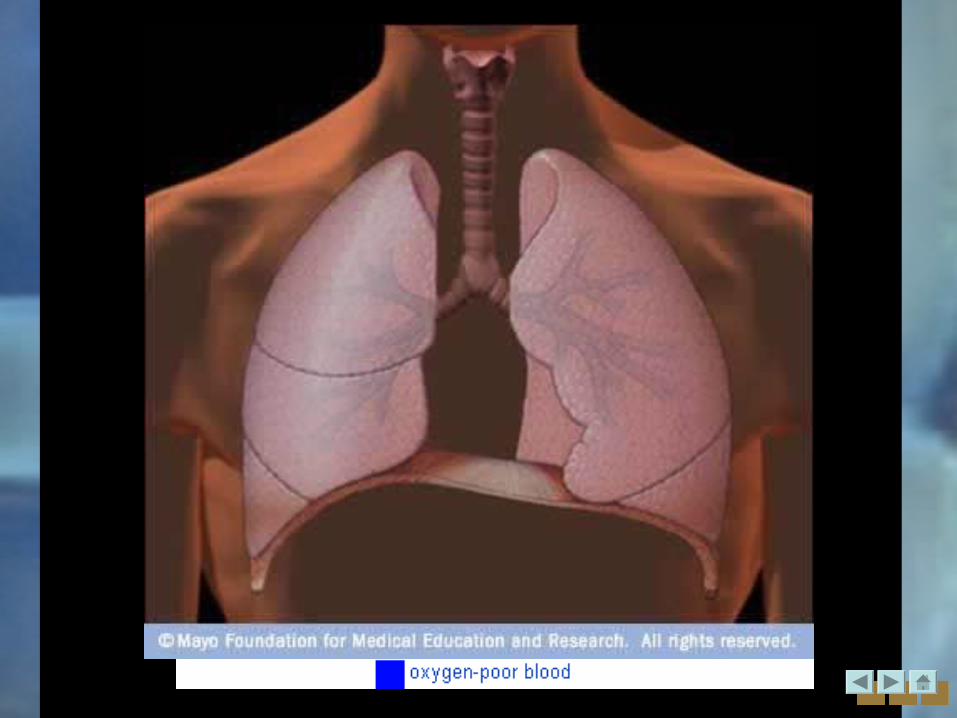
THE RESPIRATORY SYSTEM
Pathophysiology
Risk factors:Smoking – 2 packs/day
Nature of work- employee of printing company,
finance encoder, tricycle driver
AlcoholFamily History
Low nutritional status
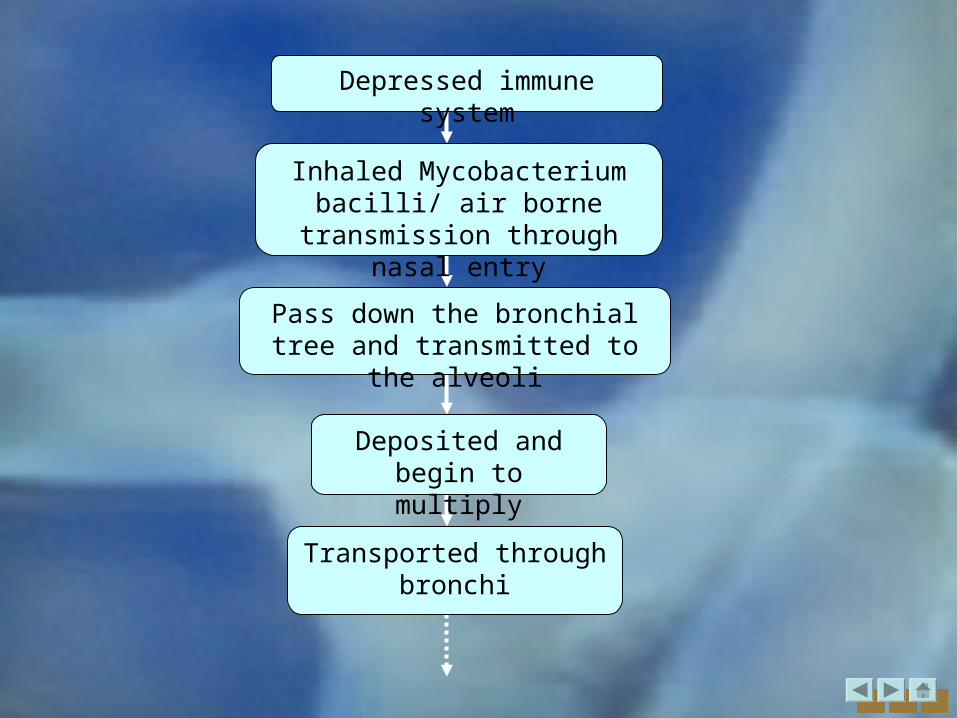
Inhaled Mycobacterium bacilli/ air borne transmission through
nasal entry
Pass down the bronchial tree and transmitted to the alveoli
Deposited and begin to multiply
Depressed immune system
Transported through bronchi
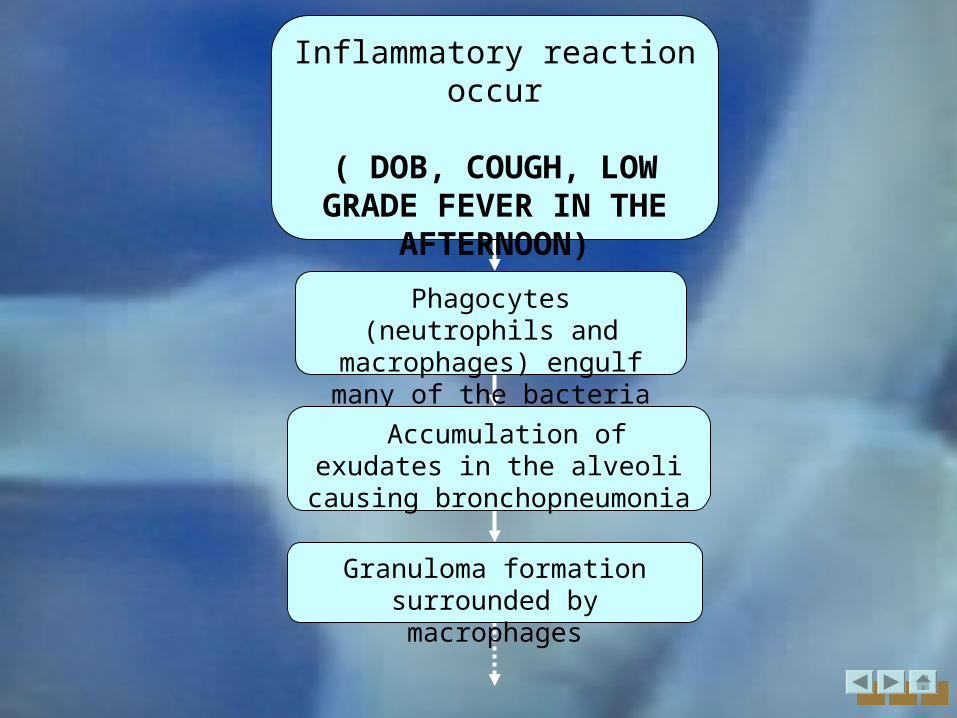
Phagocytes (neutrophils and macrophages) engulf many of
the bacteria
Accumulation of exudates in the alveoli causing
bronchopneumonia
Granuloma formation surrounded by macrophages
Inflammatory reaction occur
( DOB, COUGH, LOW GRADE FEVER IN THE
AFTERNOON)
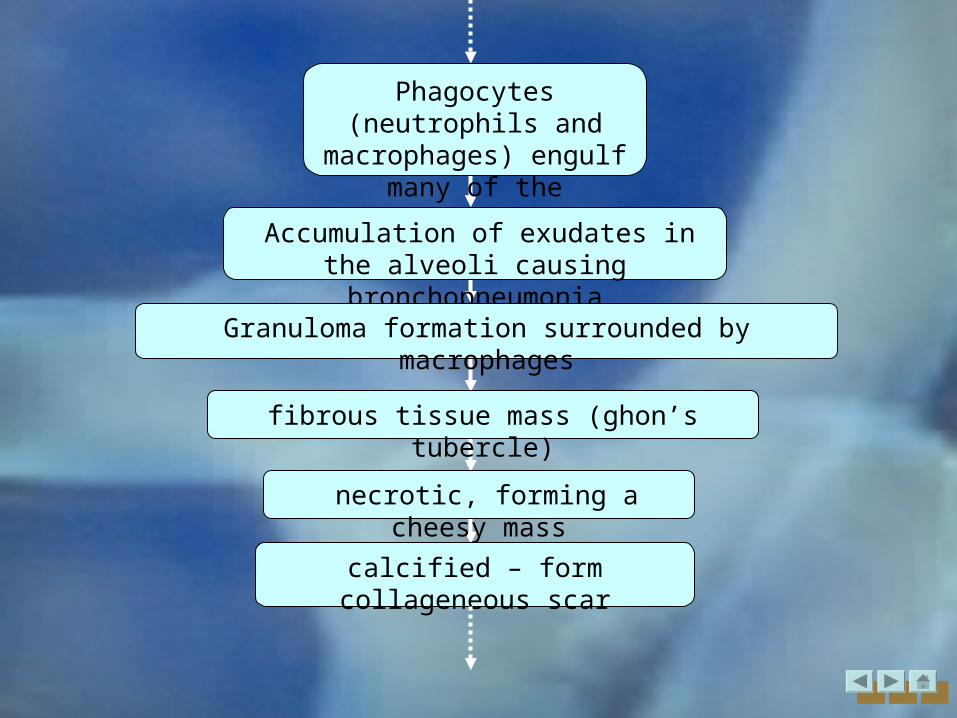
Phagocytes (neutrophils and macrophages) engulf
many of the bacteria
Accumulation of exudates in the alveoli causing bronchopneumonia
Granuloma formation surrounded by macrophages
fibrous tissue mass (ghon’s tubercle)
necrotic, forming a cheesy mass
calcified – form collageneous scar
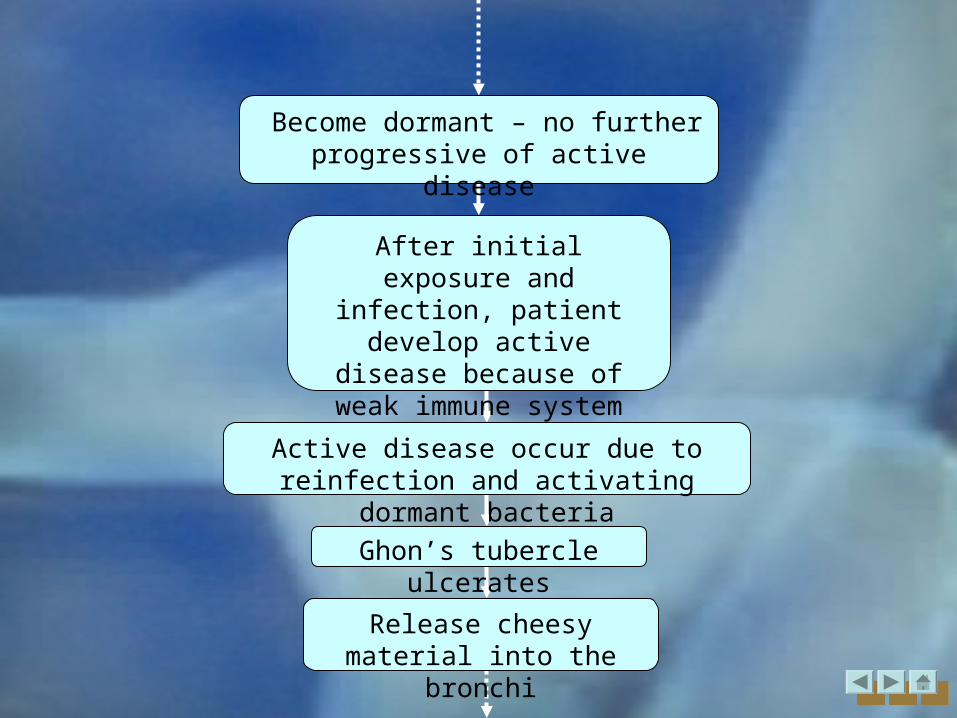
Become dormant – no further progressive of active disease
After initial exposure and infection, patient develop active disease because of
weak immune system response
Active disease occur due to reinfection and activating dormant bacteria
Ghon’s tubercle ulcerates
Release cheesy material into the bronchi
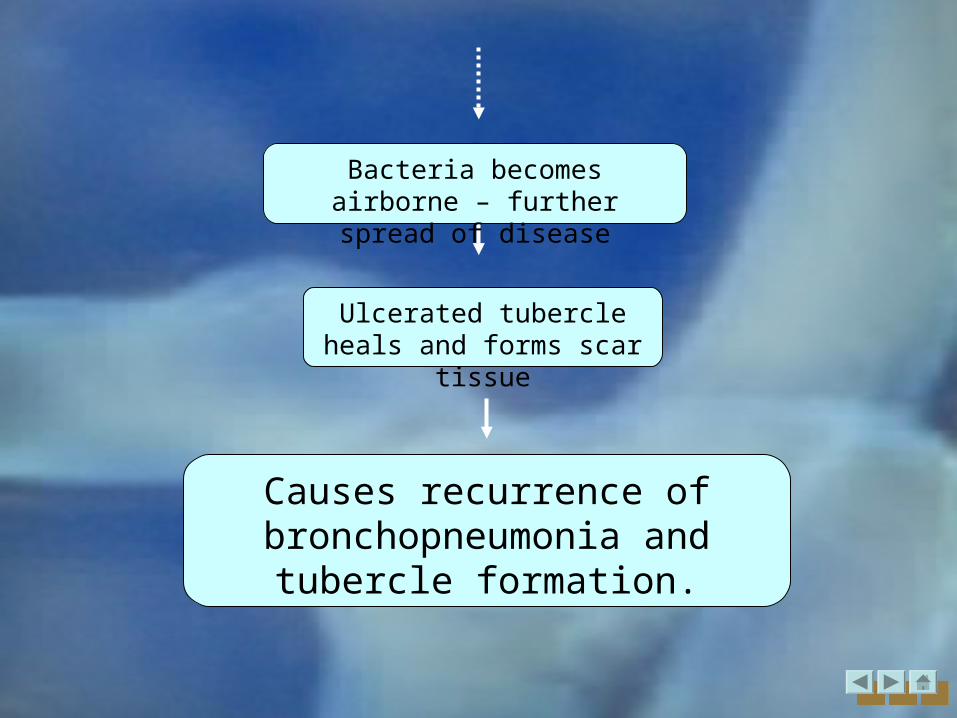
Ulcerated tubercle heals and forms scar tissue
Causes recurrence of bronchopneumonia and tubercle
formation.
Bacteria becomes airborne – further spread of disease

Medical management
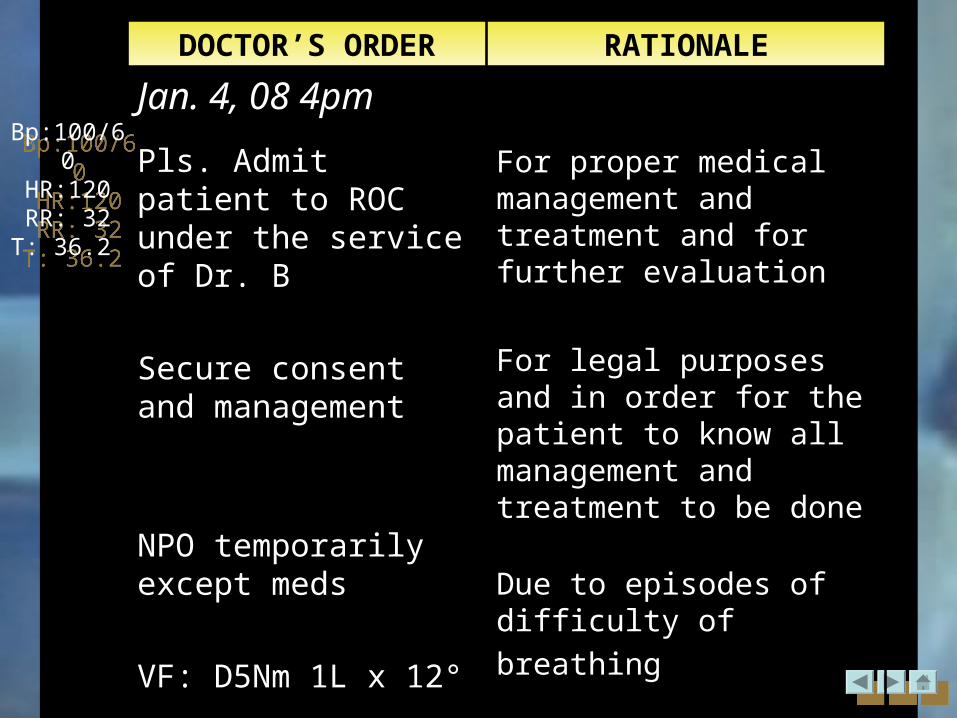
DOCTOR’S ORDER RATIONALE
Jan. 4, 08 4pm
Pls. Admit patient to ROC under the service of Dr. B
Secure consent and management
NPO temporarily except meds
VF: D5Nm 1L x 12°
For proper medical management and treatment and for further evaluation
For legal purposes and in order for the patient to know all management and treatment to be done
Due to episodes of difficulty
of breathing
For maintenance of fluid
and electrolytes
Bp:100/60HR:120RR: 32T: 36.2
Bp:100/60HR:120RR: 32T: 36.2
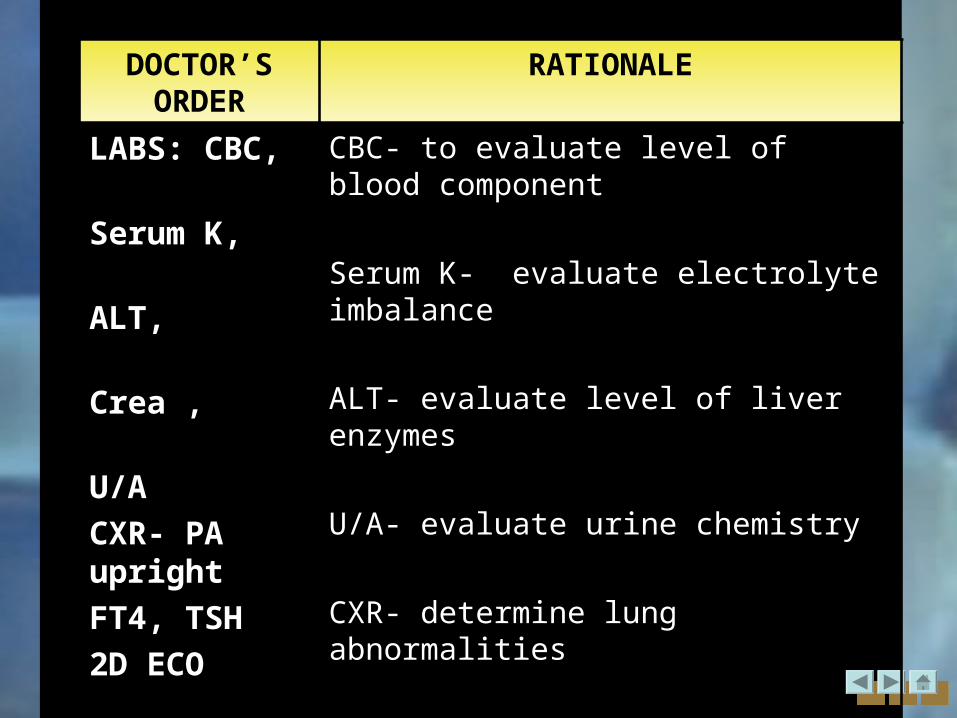
DOCTOR’S ORDER
RATIONALE
LABS: CBC,
Serum K,
ALT,
Crea ,
U/A
CXR- PA upright
FT4, TSH
2D ECO
CBC- to evaluate level of blood component
Serum K- evaluate electrolyte imbalance
ALT- evaluate level of liver enzymes
U/A- evaluate urine chemistry
CXR- determine lung abnormalities
2D ECO- to view the heart (cross sectional)
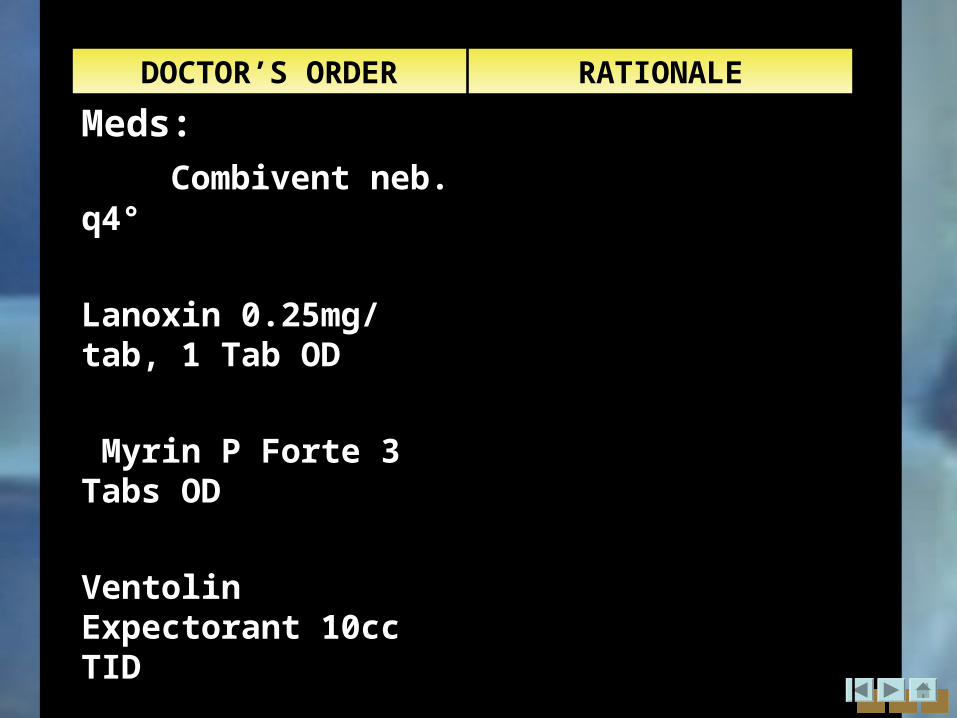
DOCTOR’S ORDER RATIONALE
Meds:
Combivent neb. q4°
Lanoxin 0.25mg/ tab, 1 Tab OD
Myrin P Forte 3 Tabs OD
Ventolin Expectorant 10cc TID
DOCTOR’S ORDER RATIONALE
Refer to Dr. O for pulmo
O2 inhalation at 3 LPM via NC
Monitor V/S q 2° and record
Record I and O q shift
Refer accordingly
Provide better oxygenation
Serve as baseline and evaluate abnormality
To determine fluid balance
DOCTOR’S ORDER RATIONALE
Jan. 4, 08 7pm
Lanoxin 0.25mg/ tab, 1 Tab OD
Myrin P Forte 3 Tabs ODJan. 4, 08 11:58pm
Ventolin Expectorant 10cc TID
DOCTOR’S ORDER RATIONALE
Jan.5, 082:05am
Refer to Dr. O for pulmo
O2 inhalation at 3 LPM via NC
Jan.5, 08 10:50am
Monitor V/S q 2° and record
Record I and O q shift
Refer accordingly
Provide better oxygenation
Serve as baseline and evaluate abnormality
To determine fluid balance
DOCTOR’S ORDER RATIONALE
Jan.5, 08 10:50am
May have Soft diet w/ SAP
Vigocid 2.25mg IV q8°
ANST(-)
Give solu-cortef 150mg IV now then q8°
IVF to FF: D5Nm 1L x 12
For sputum AFB smear x3
Streptomycin SO41g IM OD ANST (-)
To prevent aspiration
For maintenance of fluid and electrolytes
Taken to isolate microorganism that is causing infection
DOCTOR’S ORDER RATIONALE
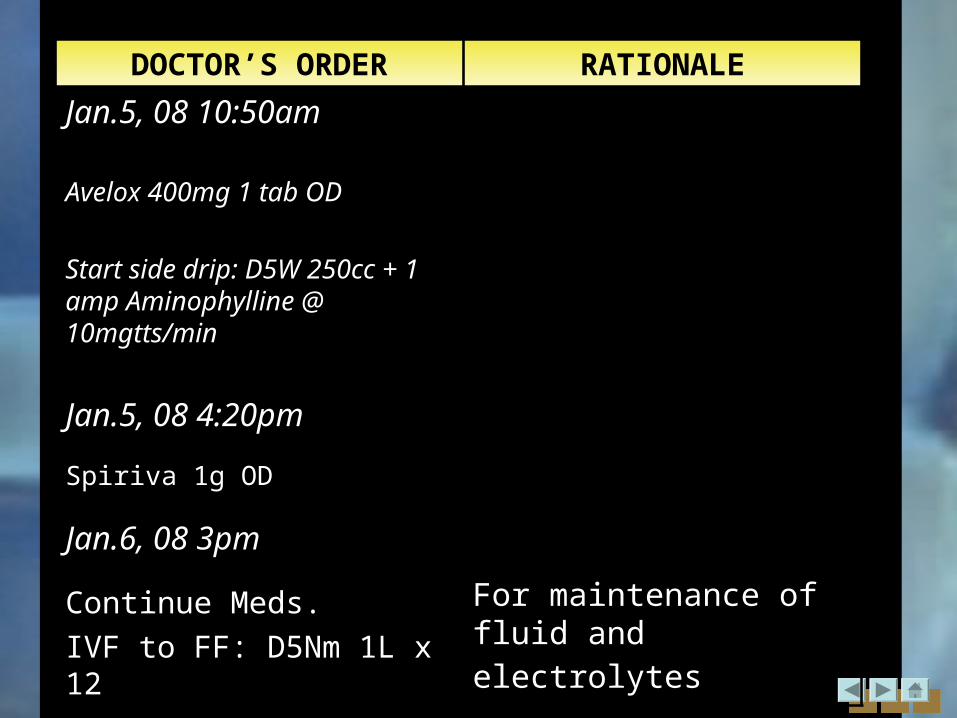
Jan.5, 08 10:50am
Avelox 400mg 1 tab OD
Start side drip: D5W 250cc + 1 amp Aminophylline @ 10mgtts/min
Jan.5, 08 4:20pm
Spiriva 1g OD
Jan.6, 08 3pm
Continue Meds.
IVF to FF: D5Nm 1L x 12
For maintenance of fluid and electrolytes
DOCTOR’S ORDER RATIONALE
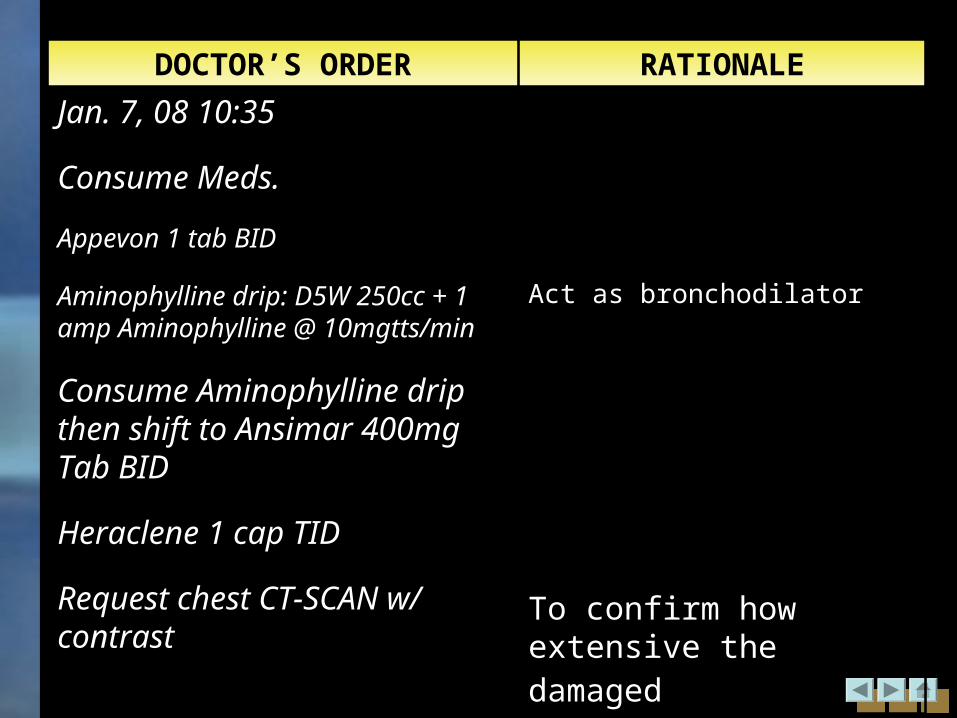
Jan. 7, 08 10:35
Consume Meds.
Appevon 1 tab BID
Aminophylline drip: D5W 250cc + 1 amp Aminophylline @ 10mgtts/min
Consume Aminophylline drip then shift to Ansimar 400mg Tab BID
Heraclene 1 cap TID
Request chest CT-SCAN w/ contrast
Act as bronchodilator
To confirm how extensive the damaged
DOCTOR’S ORDER RATIONALE
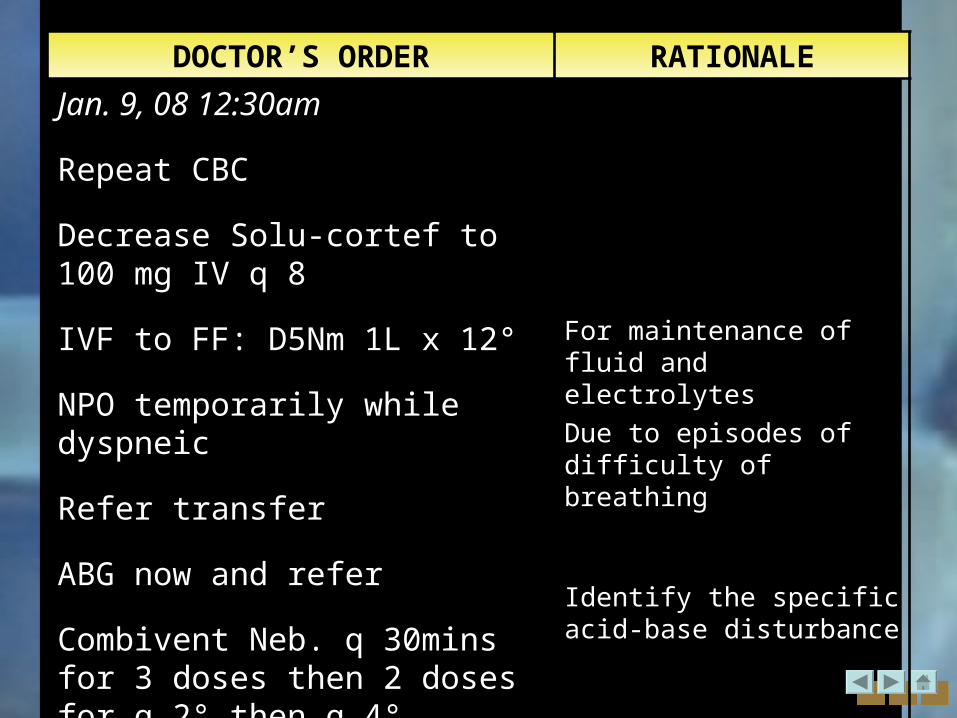
Jan. 9, 08 12:30am
Repeat CBC
Decrease Solu-cortef to 100 mg IV q 8
IVF to FF: D5Nm 1L x 12°
NPO temporarily while dyspneic
Refer transfer
ABG now and refer
Combivent Neb. q 30mins for 3 doses then 2 doses for q 2° then q 4° thereafter
For maintenance of fluid and electrolytes
Due to episodes of difficulty of breathing
Identify the specific acid-base disturbance
DOCTOR’S ORDER RATIONALE
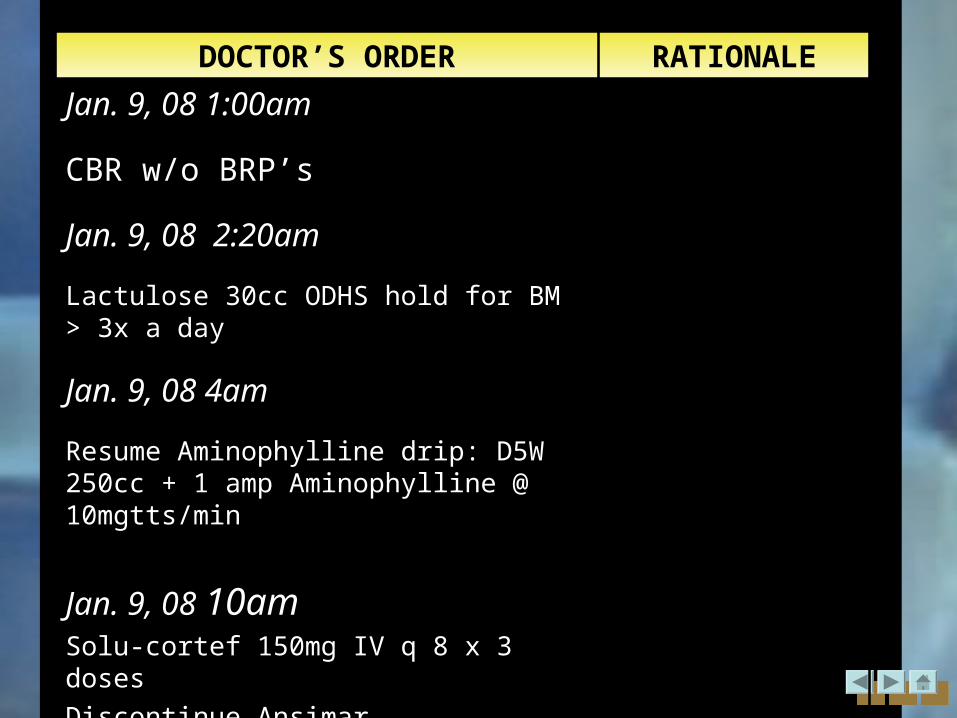
Jan. 9, 08 1:00am
CBR w/o BRP’s
Jan. 9, 08 2:20am
Lactulose 30cc ODHS hold for BM > 3x a day
Jan. 9, 08 4am
Resume Aminophylline drip: D5W 250cc + 1 amp Aminophylline @ 10mgtts/min
Jan. 9, 08 10amSolu-cortef 150mg IV q 8 x 3 doses
Discontinue Ansimar
DOCTOR’S ORDER RATIONALE
Jan. 9, 08 3:30pm
Continue other Meds.
V/S q 1 until stable
Inc. O2 inhalation to 5Lpm via NC
Jan. 10, 08 11:45am
Standby intubation set at bedside
Repeat ABG at 6am
Decrease myocardial O2 demand
For possible intubation
DOCTOR’S ORDER RATIONALE
Jan. 9, 08 2:40pm
Transfer patient to ICU now
Inc. O2 inhalation to 10Lpm
Jan. 9, 08 7:10pm
Continue Solu-cortef 150mg IV for 8°
Ranitidine 50mg IV q 8 while on NPO
Place high back rest
For f
Facilitate breathing, for better lung expansion
DOCTOR’S ORDER RATIONALE
Jan. 11, 08 7:10am
Dec. O2 to 5Lpm
Watch out for DOB and episodes of desaturation
Please limit visitor
Jan. 11, 08 11:10am
May have soft diet w/ sap
Transfer to room disposition c/o Dr. B and Dr. O
IVF to FF: D5Nm 1L x 12
Provide privacy
DOCTOR’S ORDER RATIONALEJan. 11, 08 11:10am
Pulmo:
Repeat CXR- PA
Repeat ABG
shift IV Ranitidine to oral 150mg
may have DAT
no BRP’s
refer if there will be episode of DOB
Dec. O2 at 2Lpm via NC
Consume Aminophylline drip then shift to Ansimar 400mg/tab, 1 tab BID
Pulmo:
Maintain nebulization q 4°
CXR- determine lung abnormalities
Identify the specific acid-base disturbance
Indicate improvement of condition
Indicate improvement of condition

Laboratory and diagnostics
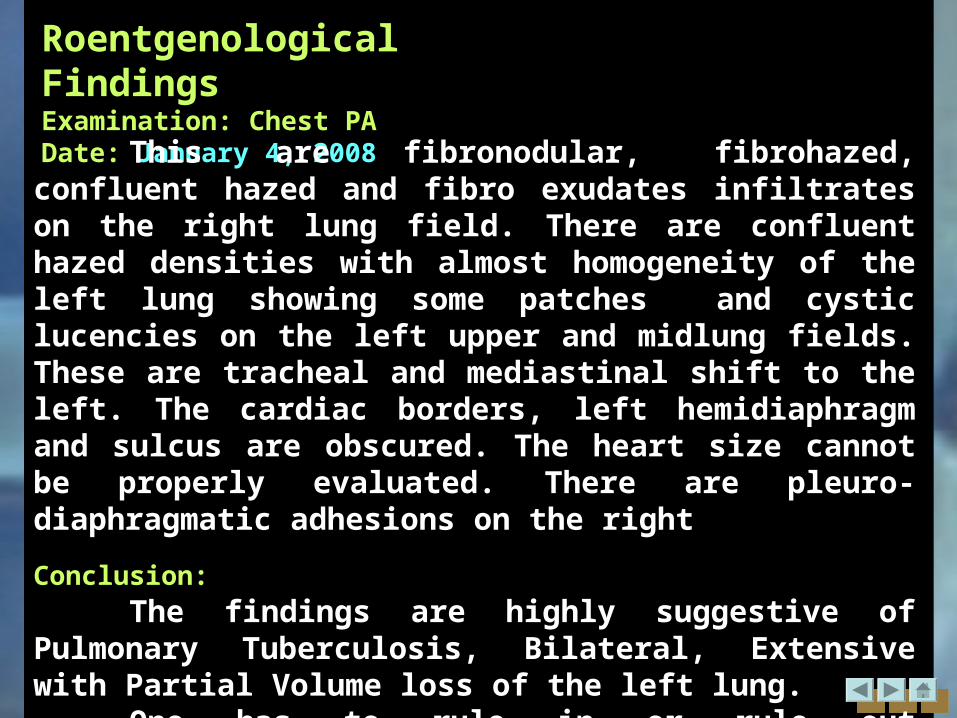
Roentgenological FindingsExamination: Chest PADate: January 4, 2008
This are fibronodular, fibrohazed, confluent hazed and fibro exudates infiltrates on the right lung field. There are confluent hazed densities with almost homogeneity of the left lung showing some patches and cystic lucencies on the left upper and midlung fields. These are tracheal and mediastinal shift to the left. The cardiac borders, left hemidiaphragm and sulcus are obscured. The heart size cannot be properly evaluated. There are pleuro-diaphragmatic adhesions on the right.
Conclusion:
The findings are highly suggestive of Pulmonary Tuberculosis, Bilateral, Extensive with Partial Volume loss of the left lung.
One has to rule in or rule out fibrothorax, left, pleuro-diaphragmatic adhesions, right.
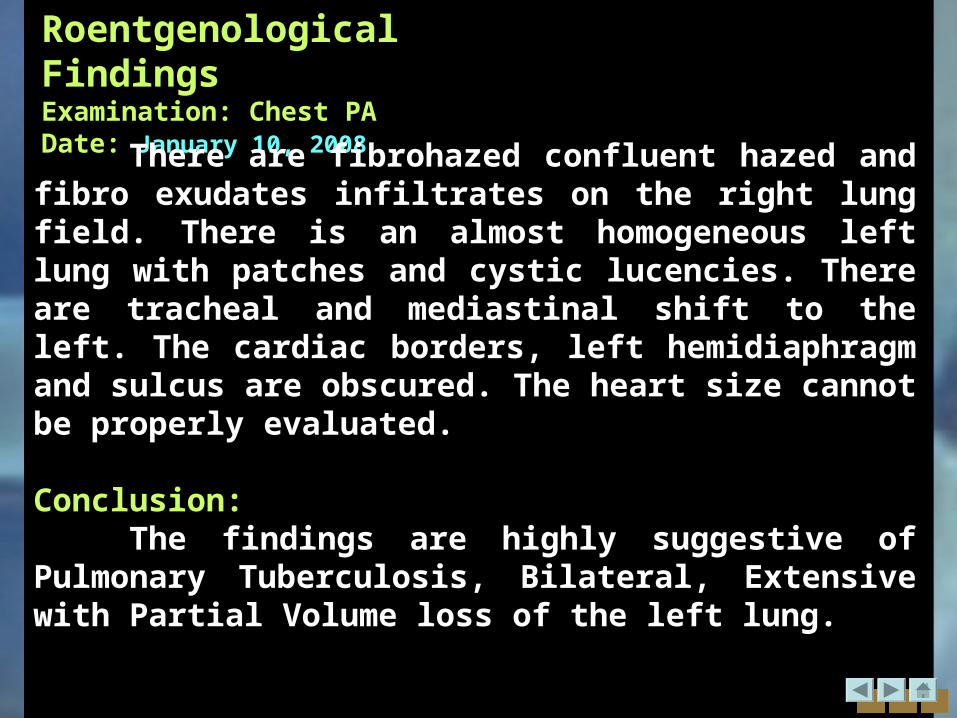
Roentgenological FindingsExamination: Chest PADate: January 10, 2008
There are fibrohazed confluent hazed and fibro exudates infiltrates on the right lung field. There is an almost homogeneous left lung with patches and cystic lucencies. There are tracheal and mediastinal shift to the left. The cardiac borders, left hemidiaphragm and sulcus are obscured. The heart size cannot be properly evaluated.
Conclusion:The findings are highly suggestive of Pulmonary
Tuberculosis, Bilateral, Extensive with Partial Volume loss of the left lung.
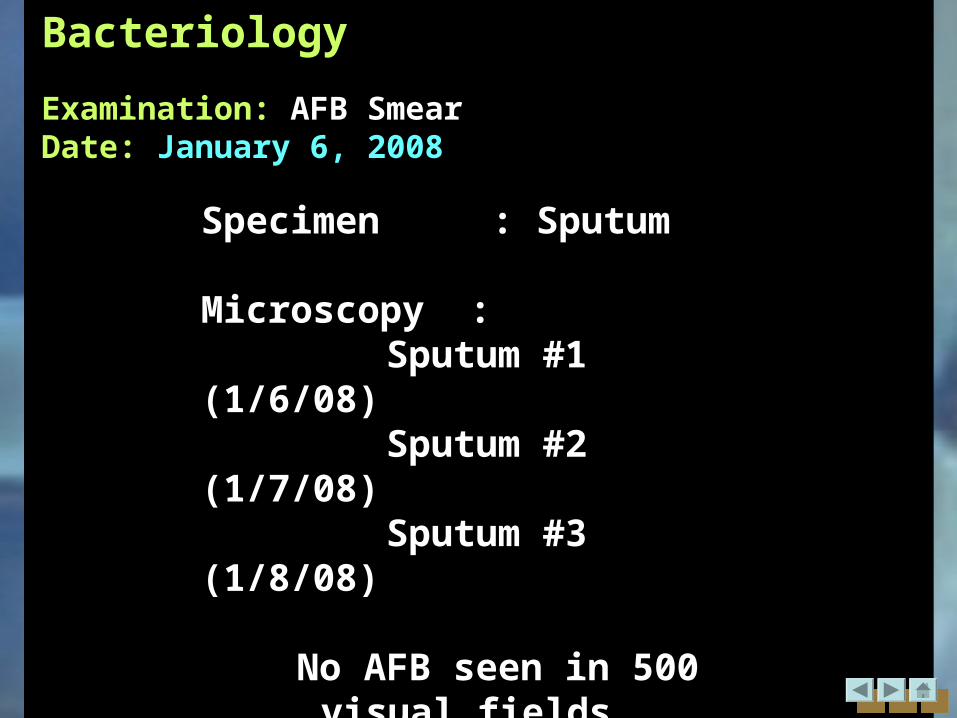
Bacteriology
Examination: AFB SmearDate: January 6, 2008
Specimen : Sputum
Microscopy : Sputum #1 (1/6/08) Sputum #2 (1/7/08) Sputum #3 (1/8/08)
No AFB seen in 500 visual fields .
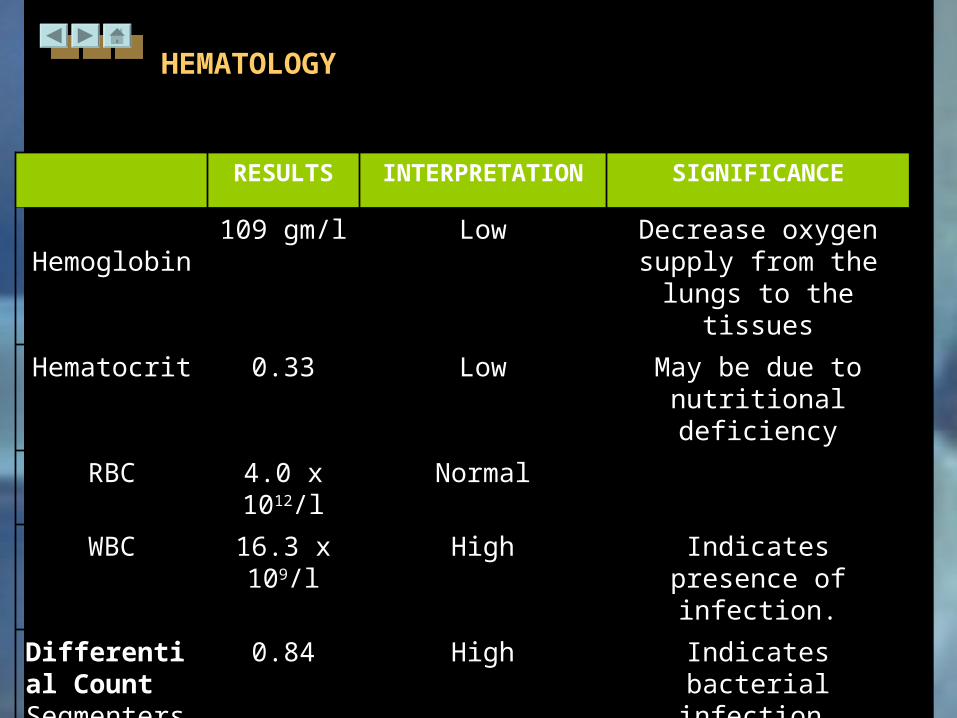
HEMATOLOGY
January 4, 2008
RESULTS INTERPRETATION SIGNIFICANCE
Hemoglobin 109 gm/l Low Decrease oxygen supply from the lungs to
the tissues
Hematocrit 0.33 Low May be due to nutritional deficiency
RBC 4.0 x 1012/l Normal
WBC 16.3 x 109/l High Indicates presence of infection.
Differential CountSegmenters
0.84 High Indicates bacterial infection.
Lymphocytes 0.16 Low Depressed immune system
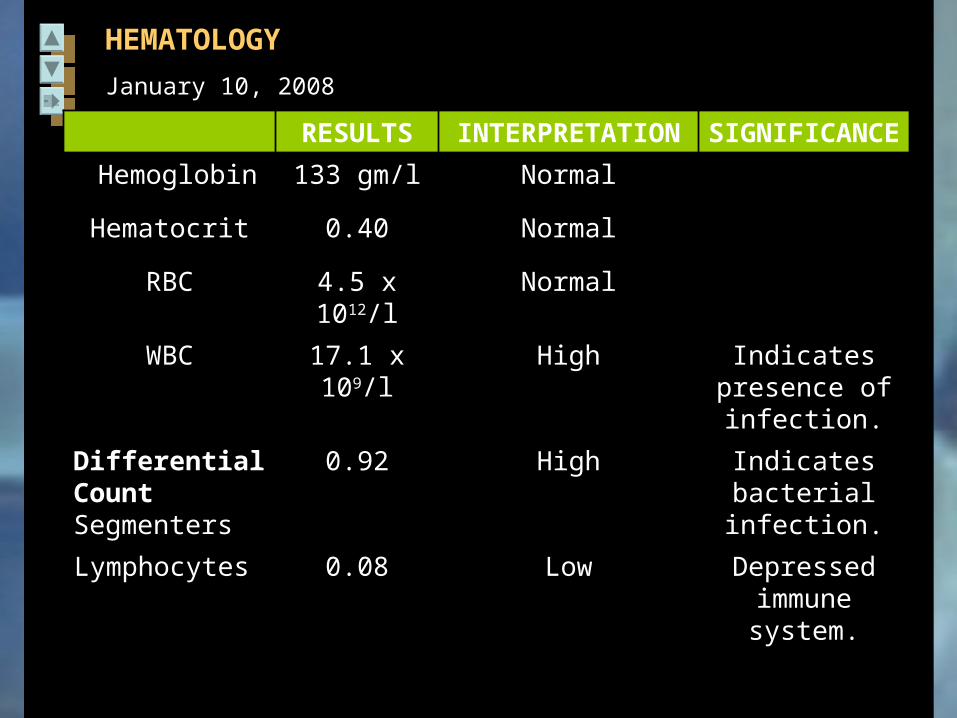
RESULTS INTERPRETATION SIGNIFICANCE
Hemoglobin 133 gm/l Normal
Hematocrit 0.40 Normal
RBC 4.5 x 1012/l Normal
WBC 17.1 x 109/l High Indicates presence of
infection.
Differential CountSegmenters
0.92 High Indicates bacterial infection.
Lymphocytes 0.08 Low Depressed immune system.
HEMATOLOGY
January 10, 2008
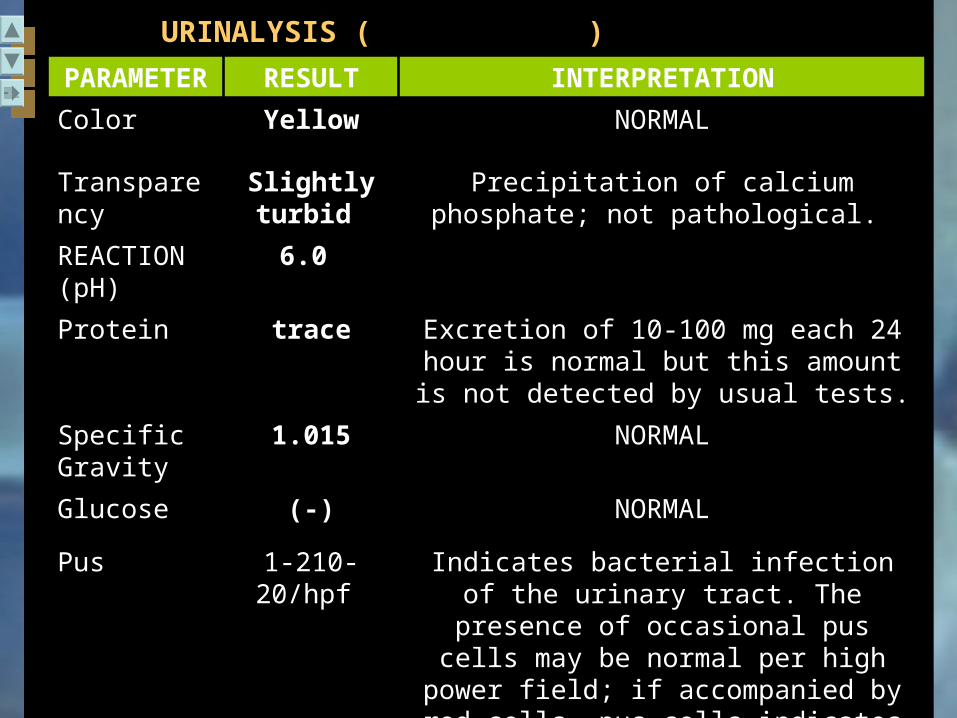
PARAMETER
RESULT INTERPRETATION
Color Yellow NORMAL
Transparency
Slightly turbid
Precipitation of calcium phosphate; not pathological.
REACTION (pH)
6.0
Protein trace Excretion of 10-100 mg each 24 hour is normal but this amount is not detected by
usual tests.
Specific Gravity
1.015 NORMAL
Glucose (-) NORMAL
Pus 1-210-20/hpf Indicates bacterial infection of the urinary tract. The presence of occasional pus cells
may be normal per high power field; if accompanied by red cells, pus cells
indicates inflammation.
URINALYSIS (January 5,2008 )
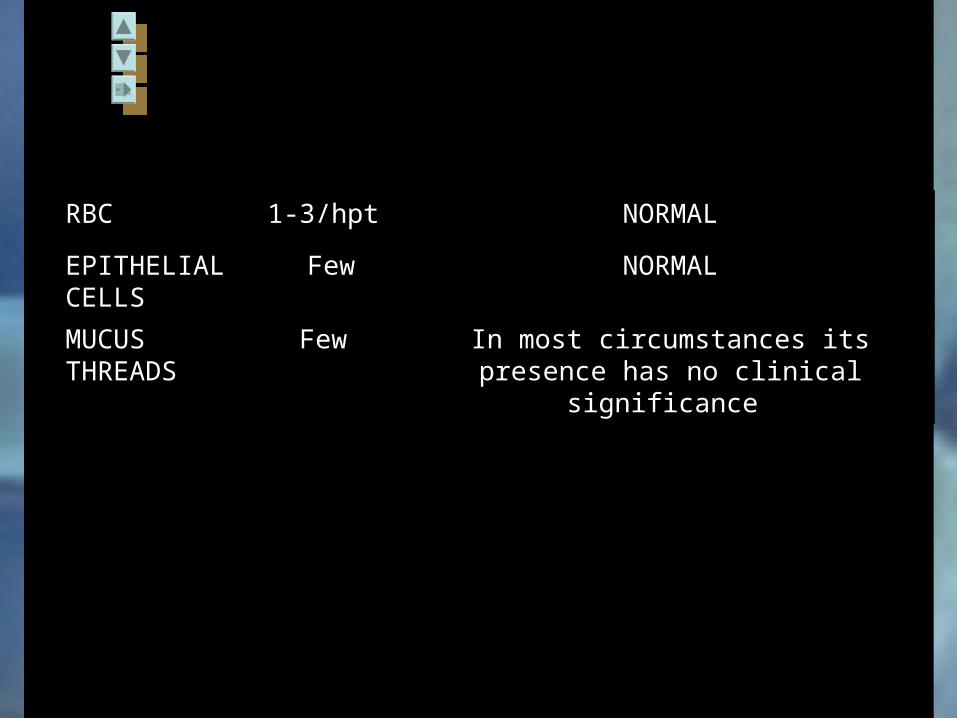
RBC 1-3/hpt NORMAL
EPITHELIAL CELLS
Few NORMAL
MUCUS THREADS
Few In most circumstances its presence has no clinical significance
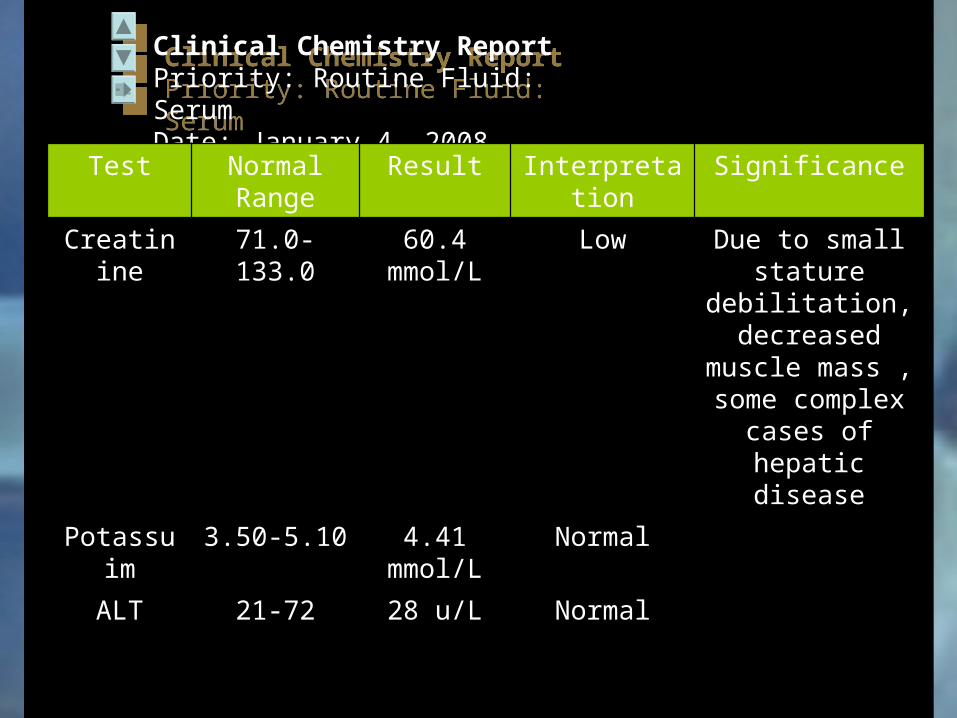
Clinical Chemistry ReportPriority: Routine Fluid: SerumDate: January 4, 2008
Clinical Chemistry ReportPriority: Routine Fluid: SerumDate: January 4, 2008
Test Normal Range
Result Interpretation Significance
Creatinine 71.0-133.0 60.4 mmol/L
Low Due to small stature
debilitation, decreased
muscle mass , some complex
cases of hepatic disease
Potassuim 3.50-5.10 4.41 mmol/L
Normal
ALT 21-72 28 u/L Normal
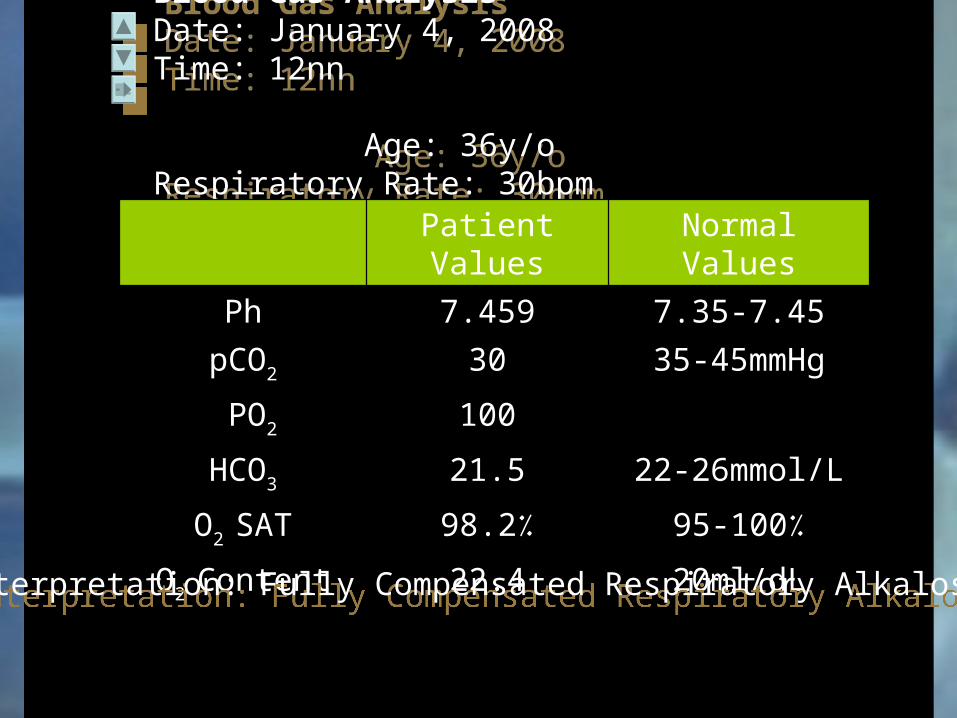
Blood Gas AnalysisDate: January 4, 2008 Time: 12nn Age: 36y/oRespiratory Rate: 30bpm Temperature: 37°C
Blood Gas AnalysisDate: January 4, 2008 Time: 12nn Age: 36y/oRespiratory Rate: 30bpm Temperature: 37°C
Patient Values Normal Values
Ph 7.459 7.35-7.45
pCO2 30 35-45mmHg
PO2 100
HCO3 21.5 22-26mmol/L
O2 SAT 98.2٪ 95-100٪
O2 Content 22.4 20ml/dL
Interpretation: Fully Compensated Respiratory AlkalosisInterpretation: Fully Compensated Respiratory Alkalosis
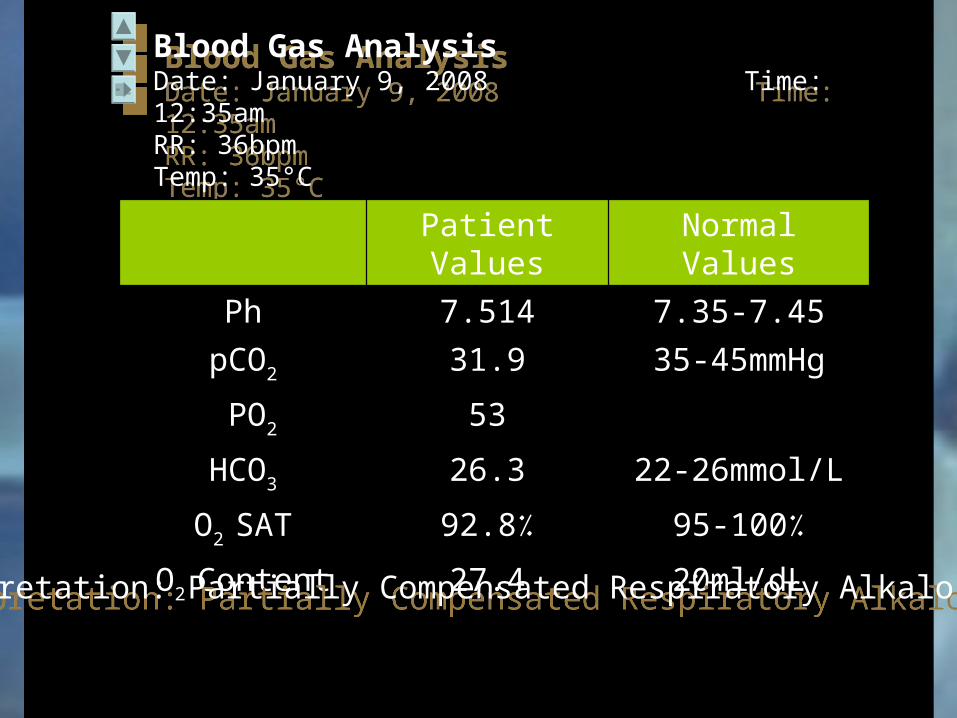
Blood Gas AnalysisDate: January 9, 2008 Time: 12:35amRR: 36bpm Temp: 35°C
Blood Gas AnalysisDate: January 9, 2008 Time: 12:35amRR: 36bpm Temp: 35°C
Patient Values Normal Values
Ph 7.514 7.35-7.45
pCO2 31.9 35-45mmHg
PO2 53
HCO3 26.3 22-26mmol/L
O2 SAT 92.8٪ 95-100٪
O2 Content 27.4 20ml/dL
Interpretation: Partially Compensated Respiratory Alkalosis Interpretation: Partially Compensated Respiratory Alkalosis
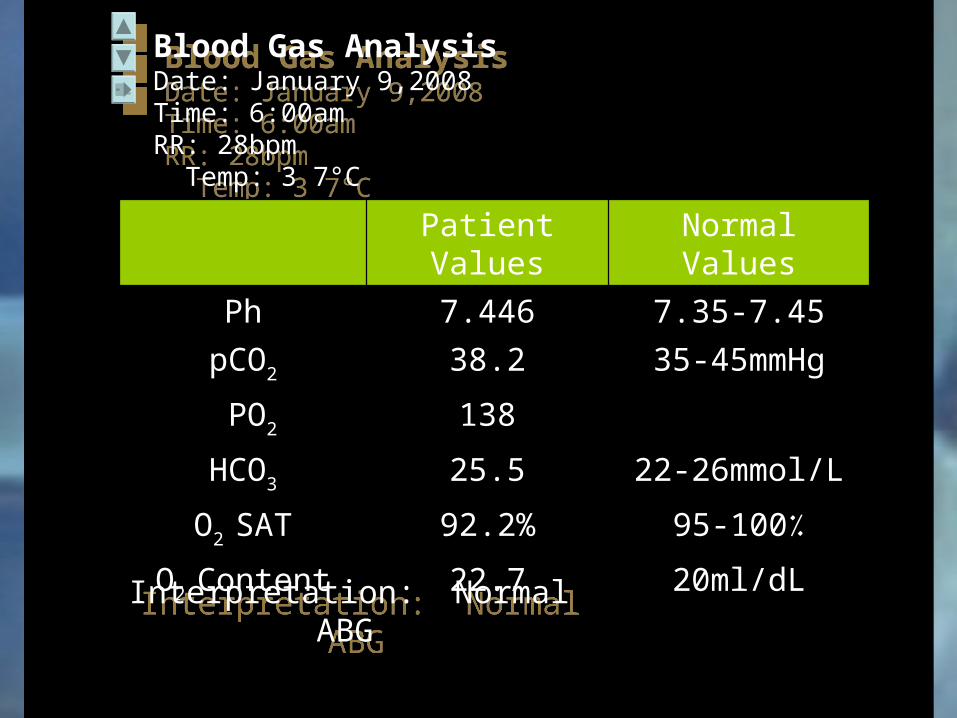
Blood Gas AnalysisDate: January 9,2008 Time: 6:00amRR: 28bpm Temp: 3 7°C
Blood Gas AnalysisDate: January 9,2008 Time: 6:00amRR: 28bpm Temp: 3 7°C
Patient Values Normal Values
Ph 7.446 7.35-7.45
pCO2 38.2 35-45mmHg
PO2 138
HCO3 25.5 22-26mmol/L
O2 SAT 92.2% 95-100٪
O2 Content 22.7 20ml/dL
Interpretation: Normal ABG
Interpretation: Normal ABG
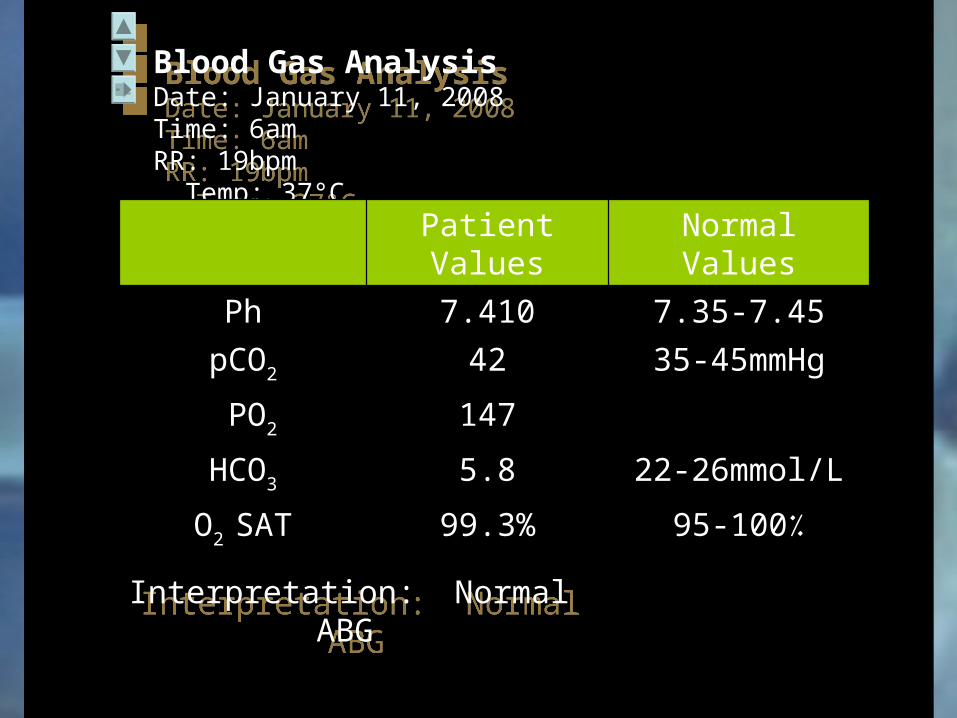
Blood Gas AnalysisDate: January 11, 2008 Time: 6amRR: 19bpm Temp: 37°C
Blood Gas AnalysisDate: January 11, 2008 Time: 6amRR: 19bpm Temp: 37°C
Patient Values Normal Values
Ph 7.410 7.35-7.45
pCO2 42 35-45mmHg
PO2 147
HCO3 5.8 22-26mmol/L
O2 SAT 99.3% 95-100٪
Interpretation: Normal ABG
Interpretation: Normal ABG
ECG FindingsDate: January 4,2008
Sinus Tachycardia
ECG FindingsDate: January 4,2008
Sinus Tachycardia





























