Embed Size (px)
Citation preview

Case Studies in Fungal Infections and Antifungal Therapy
Wayne L. Gold MD, FRCPCAnnual Meeting of the Canadian Society of Internal MedicineNovember 4, 2017

Disclosures
No financial disclosures or industry relations.

Objectives
1. Review infections caused by two medically important classes of fungi that may be seen by specialists in Internal Medicine
2. Recognize risk factors for these infections3. Understand diagnostic approaches to patients with these
infections

Objectives
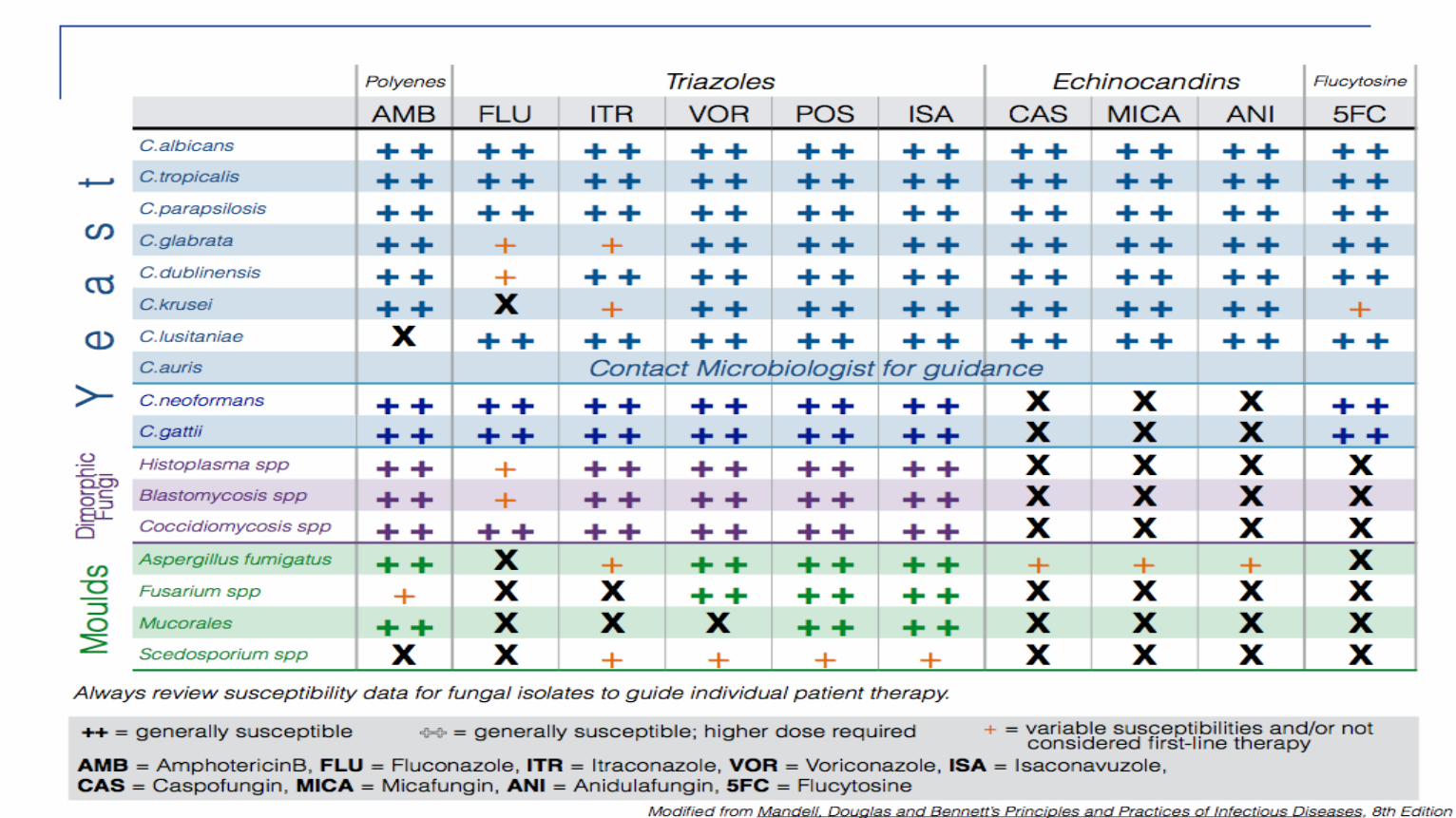
4. Review available antifungal therapies Classes of antifungal agents Polyenes - Amphotericin B Triazoles Echinocandins
Spectrums of activity Appropriate selection by clinical syndrome








Case 1

History
57-year-old woman PMH Type 2 diabetes mellitus Dyslipidemia Hypertension Alcohol use disorder

History of Present Illness
Three-day history Nausea, vomiting Epigastric abdominal pain Recent alcohol binge
Dx: acute pancreatitis (imaging, biochemistry)

History of Present Illness
Course complicated by ARDS and sepsis infected pancreatic necrosis requiring percutaneous
drainage ICU admission Intubation, ventilation Pressor support IV piperacillin/tazobactam Total parenteral nutrition - central venous catheter

History of Present Illness
Defervescence followed by recurrence of fever Cultures: Blood Endotracheal secretions Drainage fluid

Blood culture …

Candida species
Candida species
Normal human commensal organisms Skin Gastrointestinal tract (mouth to anus) Female genital tract Expectorated sputum (oropharynx)
Most common species: C. albicans, C. glabrata C. parapsilosis, C. tropicalis, C. krusei

Mucocutaneous Candidiasis
Oropharyngeal Esophageal AIDS Malignancies and their treatments Proton pump inhibitor therapy
Vaginal

Invasive Candidiasis
Normally non-pathogenic Invasive candidiasis is the price paid for advances in
modern medical therapies Primarily a nosocomial infection or associated with
ambulatory “medicalized” patients

Host Defenses Against Invasive Candidiasis
Intact skin Intact mucous membranes Normal sphincter function Normal neutrophil number and function

Risk Factors for Invasive Candidiasis
Exposure to broad-spectrum antimicrobial therapy Indwelling venous devices Total parenteral nutrition (CVC, alimentation solution) Gastrointestinal surgery Neutropenia Cytotoxic chemotherapy Intestinal mucositis Solid organ transplantation Intravenous drug use Low-birth-weight
.Adapted from Edwards JE Jr. Candida Species
In Principles and Practice of Infectious Diseases 8th Edition

Risk Factors for Invasive Candidiasis
Exposure to broad-spectrum antimicrobial therapy Indwelling venous devices Total parenteral nutrition (CVC, alimentation solution) Gastrointestinal surgery Neutropenia Cytotoxic chemotherapy Intestinal mucositis Solid organ transplantation Intravenous drug use Low-birth-weight
.Adapted from Edwards JE Jr. Candida Species
In Principles and Practice of Infectious Diseases 8th Edition

Invasive / Disseminated Candidiasis
Bloodstream Dissemination to: Eyes (2-20%) Bones/joints Skin Liver / spleen (immunocompromised hosts) Heart

Invasive Candidiasis - Diagnosis
Culture-based techniques Blood, tissue, fluids
Diagnostic imaging

What antifungal agent would you select from empiric treatment of this patient with candidemia?

How would you treat this patient?
A. An echinocandin Caspofungin, micafungin, anadulafungin
B. FluconazoleC. VoriconazoleD. Lipid-formulation amphotericin B

How would you treat this patient?
A. An echinocandin Caspofungin, micafungin, anadulafungin
B. FluconazoleC. VoriconazoleD. Lipid-formulation amphotericin B



Empiric Treatment of Candidemia –Non-Neutropenic Patients
Fluconazole 800 mg iv/po in patients who are not critically ill and without prior azole exposure
An echinocandin is recommended as empiric therapy when fluconazole is patients not meeting these criteria
Voriconazole offers little advantage over fluconazole for most Candida species (enhanced mould activity)
Amphotericin B has a greater potential for toxicity than other classes

Treatment of Candidemia –Non-Neutropenic Patients
Antifungal susceptibility testing is recommended for allbloodstream isolates
Candida glabrata is less susceptible to azole therapy Candida krusei is intrinsically resistant to fluconazole Candida parapsilosis is less susceptible to echinocandins Transition from an echinocandin (if used as initial therapy) to
fluconazole is recommended once patient has stabilized and if isolate is susceptible

What other processes of care are indicated for this patient?
Which of the following statements is false in patients with candidemia?A. A dilated ophthalmologic examination is indicated for all patientsB. Follow-up blood cultures should be performed daily until
candidemia is clearedC. An echocardiogram is indicated for all patientsD. All venous catheters should be removed / changedE. Recommended duration of therapy is 2 weeks after documented
clearance of candidemia in patients without metastatic complications

Which of the following statements is false?
A. A dilated ophthalmologic examination is indicated for all patientsB. Follow-up blood cultures should be performed daily until
candidemia is clearedC. An echocardiogram is indicated for all patientsD. All venous catheters should be removedE. Recommended duration of therapy is 2 weeks after documented
clearance in patients without metastatic complications

Treatment of Candidemia –Neutropenic Patients
An echinocandin or lipid formulation of amphotericin B is recommended as initial therapy
During persistent neutropenia, transition to fluconazole can be done once patient has stabilized and if isolate is susceptible

Blood culture …
Candida albicans

Management and Outcome Treatment initiated with caspofungin Hemodynamically unstable
Lines changed Dilated ophthalmologic examination - normal Day 2 – afebrile Day 3 – blood culture negative


Case 2

History
65-year-old man PMH Colorectal cancer - 2004 Resection, adjuvant chemotherapy
Metastatic progression (lung, pelvis) - 2006 Combination chemotherapy capecitabine, irinotecan, bevacizumab
Treatment complicated by pulmonary embolism

History of Present Illness
Four weeks prior to presentation Fever, dry cough treated with course of po antibiotics
Two-week history of purulent sputum, night sweats Prescribed moxifloxacin

Chest Radiograph

History of Present Illness
Fever resolved Increasing dyspnea, streaky hemoptysis, anorexia,
fatigue, night sweats No cigarette smoking, IVDU No recent travel No history of TB exposure

CT Thorax – Cavitary Lung Disease

How would you investigate this patient?

In consideration of a diagnosis of aspergillosis, which test is not recommended for diagnosis in this patient?
A. Expectorated sputum for microbiologic and cytologic examination
B. Fine needle aspiration of lesion with specimens sent for microbiologic and cytologic investigations
C. Bronchoscopy with specimens sent for microbiologic and cytologic investigations
D. Serum galactomannan

In consideration of a diagnosis of aspergillosis, which test is not recommended for diagnosis in this patient?
A. Expectorated sputum for microbiologic and cytologic examination
B. Fine needle aspiration of lesion with specimens sent for microbiologic and cytologic investigations
C. Bronchoscopy with specimens sent for microbiologic and cytologic investigations
D. Serum galactomannan

Invasive Aspergillosis - Diagnosis
Diagnostic imaging Culture-based techniques Tissue, fluids

Galactomannan in the Diagnosis of Aspergillosis
A cell wall constituent that is released extracellularly Recommended as a test for the diagnosis of invasive
aspergillosis in high-risk populations Hematologic malignancy, HSCT
Lacks sensitivity and specificity in other populations Can be applied to bronchoscopy specimens May be used for screening in high-risk populations – serial
measurements

Case – Sputum Examination
Sputum culture Negative for bacteria and fungi AFB smear –negative

Case – Fine Needle Aspiration
Microbiology Gram-stain - negative No fungal elements seen No bacterial or fungal pathogens isolated

Cytology - Fine Needle Aspiration

Cytology - Fine Needle Aspiration
Fungal elements seen – septate hyphae, 45o angles Foreign material seen
Morphology compatible with Aspergillus species

Aspergillus species
Filamentous moulds Environmental organisms – ubiquitous in soil, water

Risk Factors for Invasive Aspergillosis
Prolonged, profound neutropenia (>3 weeks) Most common in hematological malignancies, HSCT
Solid organ transplantation AIDS Systemic corticosteroids Primary immunodeficiency states (CGD) Chronic lung disease Anti TNFα agents Marijuana use

Risk Factors for Invasive Aspergillosis
Prolonged, profound neutropenia (>3 weeks) Most common in hematological malignancies, HSCT
Solid organ transplantation AIDS Systemic corticosteroids Primary immunodeficiency states (CGD) Chronic lung disease Anti TNFα agents Marijuana use

Aspergillosis – Clinical Syndromes
Colonization Pulmonary syndromes Other organ disease

Pulmonary Aspergillosis
Mycetoma – “fungus ball” Angioinvasive pulmonary aspergillosis Chronic necrotizing pulmonary aspergillosis Obstructing bronchial aspergillosis HIV/AIDS
Bronchial aspergillosis – lung transplantation Anastamotic dehiscence
Allergic bronchopulmonary aspergillosis




How would you treat this patient?

Which agent is not indicated in the treatment of aspergillosis?
A. PosacazoleB. CaspofunginC. Amphtotericin BD. FluconazoleE. Voriconazole

Which agent is not active against Aspergillus species?
A. PosacazoleB. CaspofunginC. Amphtotericin BD. FluconazoleE. Voriconazole


Treatment of Aspergillosis
Voriconazole is recommended as first-line therapy for invasive aspergillosis
Early therapy is recommended in patients highly suspected for this condition while awaiting diagnostic testing results
Liposomal amphotercin B is recommended as alternative therapy
Posaconazole and isavuconazole may be used Echinocandins are second-line therapie

Management
Voriconazole initiated Clinical and radiographic improvement observed


Antifungal Therapy

Antifungal Therapy
Amphotericin B Broad purpose for yeasts and moulds
Nephrotoxicity Electrolyte disturbance (K, Mg, Ca) Infusion-related side effects (“shake and bake”) Less adverse reactions with lipid formulations

Antifungal Therapy Triazoles
Yeast; Moulds with late generation agents (VOR, POS, ISUV) Enhanced mould activity with posaconazole, isavuconazole
Inhibitors and substrates for CYP enzymes drug-drug interactions
May prolong QTc (isavuconazole may shorten QTc) May cause hepatotoxicity Voriconazole – photopsia Therapeutic drug monitoring may be clinically helpful

Antifungal Therapy
EchinoCANDINS - CANDida; second-line agent for Apergillus species
Generally well tolerated Few drug interactions
Conclusions
Invasive fungal infections are the “collateral damage” of advances in medical therapy
Candida species and Aspergillus species are clinically important human pathogens – opportunistic pathogens
Increasing choices for antifungal therapy but … Increasingly resistant fungi are being recognized as
human pathogens