Embed Size (px)
Citation preview

Case Series - Continuous Diffusion of Oxygen...S. Nicholas Desai, DPM, MBA, FACFAS, Medical Director, Foot Centers of Texas, Sugar Land, Texas
...as an Adjunctive Therapy to Moist Wound TherapyMark Q Niederauer, PhD; Shelly Monnens APRN-BC, FNP, MSN, RN, CWOCN, CWS, FACCWS, EO2 Concepts®
AbstractChronic wounds present a challenge in wound care. The current standard of care is moist wound therapy, which uses a moisture absorbent dressing below an occlusive dressing to keep the wound moist and manage wound drainage while controlling bioburden. These dressings are frequently used on patients who have impaired blood flow, and thus impaired oxygen supply, to the wound. By saturating, or even super-saturating, the wound with oxygen, it has been found that the wound repair process can be reinitiated and even accelerated. Other approaches to increase wound oxygen levels use short exposures to hyperbaric systemic oxygen or topical high oxygen flow rates applied to entire extremities. Our data suggest that neither high-pressure nor high flow-rates are required for oxygen to improve wound healing. Rather, improving local oxygen supply through Continuous Diffusion of Oxygen into a moist wound bed, and thus increasing the oxygen concentration directly over the site of injury, significantly improves tissue healing while simultaneously allowing for full patient mobility. The vast majority of these patients were unresponsive to other advanced wound care technologies such as hyperbaric oxygen therapy, advanced wound dressings or negative pressure wound therapy. Wounds that were, on average, 250 days old were brought to a successful outcome in 62 days on average using Continuous Diffusion of Oxygen as an adjunctive therapy to moist wound therapy.
IntroductionContinuous Diffusion of Oxygen (CDO) therapy was developed to enable the continuous treatment of wounds through the localized diffusion of oxygen directly into the wound site. To achieve continuous treatment, the device which delivers the therapy must be easily portable and capable of delivering oxygen continuously to the wound site. Although the concept of localized diffusion of oxygen directly into wounds is not a novel technique, the manner in which the TransCu O2® delivers the oxygen is unique to the market.
There are three primary methods of oxygen-based therapies which are used to treat chronic wounds: Hyperbaric Oxygen (HBO), Topical Oxygen (TO) and CDO. All three technologies are similar in that they use pure oxygen as an aid to wound healing. HBO therapy is used to treat a patient systemically with pure oxygen at elevated pressures. TO therapy is used to treat an area directly surrounding a patient’s wound using pure oxygen at pressures slightly above atmospheric. Both of these technologies only offer treatment for a relatively short period of time: typically 90 minutes per day, 3 to 5 days per week. Furthermore, neither of these technologies allows for patient mobility during treatment and can require significant time and expense associated with travel and preparation time for the patient.
CDO therapy offers several breakthroughs in oxygen therapy. It provides continuous oxygen therapy, which is over 20x the therapy time of competing intermittent oxygen therapies. Used with moist wound therapy dressings, it maintains a moist wound environment and allows for full patient mobility. Furthermore, the TransCu O2® device is silent, lightweight (nine ounces), handheld, and rechargeable. The TransCu O2® device also incorporates continuous monitoring of oxygen flow rates and pressures to ensure efficacious delivery of oxygen.
CDO therapy delivers oxygen using the same basic mechanism as breathing: direct diffusion of oxygen into the wound from the wet surface, whereas breathing involves direct diffusion of oxygen into the alveoli before it is picked up by hemoglobin. Using the TransCu O2® device, the oxygen is delivered directly to the wound via a cannula, which is placed underneath moist wound therapy (MWT) dressings. MWT is defined here as using a moisture absorbent dressing below a thin film dressing. The moisture absorbent dressing is used to control exudate. The thin film dressing is used to maintain a moist wound environment and protect the wound from external contamination. The flow of oxygen from the TransCu O2® device is such that it maintains a high concentration over the moist wound, yet does not dry the wound out. The patient has full mobility during treatment and their wound is continually treated (24 hours per day, 7 days per week). Dressings are changed in accordance with the physician’s directive and manufacturer’s guidelines to manage exudate.
Efficacy of CDO therapy has previously been shown in a diabetic murine model which used MWT with a sham device as the control and compared it to MWT with CDO on full-excisional skin wounds.1 This study showed that CDO therapy increases the rate of wound closure, as measured by complete reepithelialization of the wound, by 128% compared to MWT alone. The paper also demonstrated accelerated wound closure as well as histological evidence indicating improved collagen organization in CDO-treated wounds.
The following review focuses on the clinical efficacy and safety for the use of CDO therapy on chronic wounds. Three cases which highlight the use of CDO therapy are presented, followed by a review of the overall results from the internal registry of wounds treated. Any costs cited are based on average costs for only the therapy being referenced and do not include the costs of nursing or other care.
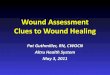
Case 1 - Diabetic Foot UlcerA 64 year old Hispanic male presented with a non-healing diabetic ankle ulceration. The age of the wound was greater than 2 months (>60 days). The wound was unresponsive to 20 sessions of HBO therapy, an intermittent, high-pressure oxygen therapy, at an estimated cost of $9,100. No noted improvement was seen in the wound during HBO therapy treatment even though vascular perfusion in the area was noted through TCOM. The wound was then treated with CDO therapy at a flow rate of 3 ml/hr. Within one week of CDO therapy, the dimensions of the wound were noted to decrease. The wound closed fully by 39 days for an estimated cost of $2,600. Note the quality of the new tissue repair.
Day 0 – Wound Size 3.0 x 2.6 cm" " " " " " " " " Day 39 – Full Closure of Wound Case 2 - Venous Stasis UlcerAn 89 year old female presents with a chronic non-healing venous stasis ulcer on the right leg. Patient has a history of type II diabeties, PVD, dementia, HTN, diverticulitis, vascular disease, left eye implant, anxiety, renal artery stenosis, alzheimer’s, stroke, femoral stenosis and osteoporosis. She has had a venous duplex ultrasound, arterial duplex. All impressions show severe occlusion in popliteal artery, femoral artery and post tibial artery which equates to advanced atherosclerotic arterial occlusion disease in right lower extremity. Patient treated continuously with CDO therapy at 10 ml/hr using a two-part moisture absorbent dressing and thin film layer. Previous therapy includes > 120 days (4 months) of negative pressure wound therapy (NPWT) at an estimated cost of $9,800. Full closure was achieved with CDO therapy at 10 ml/hr by 47 days (~ 1 ½ mos) for $3,100.
Day 2 – First Dressing Change" " " " " " " " " " " Day 47 – Full Closure of Wound
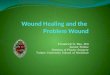
Case 3 - Skin GraftFemale with deep ulcer on right foot. Patient has already had partial amputation of left foot which was the result of a similar condition. Patient received a split thickness skin graft after undergoing wound bed preparation to increase vascularity through the application of CDO therapy. CDO was applied at 10 ml/hr for 9 days with a two-part absorbent foam layer and occlusive dressing to ensure take of graft. Graft continued to full closure.
Day 0 – Start of Treatment, Deep Pressure Ulcer " " " Day 14 – Split Thickness Graft Healing
Case Series Review - Internal RegistryHundreds patients have been, or were currently receiving, Continuous Diffusion of Oxygen (CDO) therapy with the TransCu O2®. The following statistics are based on data for 404 compliant patients for which we have verified final outcomes. The outcomes are classified as being either a Success (defined as therapy goals met or fully healed and closed) or a Failure (defined as removed for other reasons).
These outcomes are very significant when one takes into account that most wounds treated had already been treated with other advanced wound therapies, such as HBO therapy, negative pressure wound therapy, skin grafting, antibiotic treatment, etc. The majority of wounds were unresponsive to other advanced wound therapies prior to treatment with CDO therapy.
Overall success rate was 76% for compliant cases. The overall rate of compliance is 91%. The age of wounds prior to application of CDO therapy ranges from several weeks to over 15 years, with the average age of the wound prior to the start of CDO therapy being 466 days (~16 months). The time to achieve successful outcome is an average of 56 days (< 2 months). Outcomes for various wound types can be found in Table 1.
Table 1: Clinical Efficacy of CDO Therapy from Internal Patient Registry for TransCu O2®
OverallDiabetic
Foot Ulcers
Venous Ulcers
Pressure Ulcers
Surgical Wounds
All Other Wounds
Number of Verified Patients 404 90 76 79 66 93
Success Rate (Compliant Only) 76% 80% 78% 76% 68% 77%
Avg. Patient Age, years 67 65 70 67 65 69
Avg. Wound Age Before CDO, days 466 593 511 551 284 346
Avg. CDO Therapy Time, days 56 55 76 59 43 49
Percent Compliance 91% 91% 93% 88% 93% 93%
DiscussionThe use of oxygen to treat wounds has recently undergone significant changes which enable the efficacious and safe delivery of oxygen directly to the wound bed. Recent published clinical studies which used intermittent diffusion of oxygen therapy have shown the following significantly positive effects of using diffusion of oxygen therapy:2-4
•" Faster wound closure•" Improved wound closure success rate•" Pain reduction•" Reduction in MRSA infection•" Increased VEGF expression and angiogenesis•" Reduced Venous Stasis recurrence
Our results using Continuous Diffusion of Oxygen therapy are similar to those for intermittent diffusion of oxygen therapy with regard to efficacy. However, CDO therapy has significant advantages over intermittent therapies such as HBO or TO, including ease of application (can be applied in any setting), continuous treatment of wound, full patient mobility during treatment, no known safety issues or risks, and lower cost. Wounds treated successfully thus far include venous stasis ulcers, pressure ulcers, diabetic foot ulcers, gangrenous ulcers, wound bed preparation for skin grafting, full and split thickness skin grafts, radiation burns, dehiscent surgical wounds and diabetic amputation wounds, among others. With regard to the safety of the device and technology, it is considered to be safe with no known risks to the patient. There have been no reported adverse effects or reactions associated with the use of CDO therapy in the literature.
ConclusionsAdvances continue to be made in many areas of wound care, including technique, dressings and advanced treatment modalities. There are currently three types of therapies being used clinically for delivering oxygen to treat wounds: Hyperbaric Oxygen (HBO), Topical Oxygen (TO) and Continuous Diffusion of Oxygen (CDO). Each of these technologies uses a unique method to deliver oxygen, which also affects the how the oxygen is used by the body to effect wound repair. HBO is currently the most widely used and commonly accepted form of oxygen therapy for wounds, yet TO has recently shown significant advances in technology supported by good clinical trial data.5-7 The newest oxygen therapy, CDO, can deliver continuous therapy, allows for full patient mobility, has good scientific evidence and is building a credible body of clinical evidence. The use of oxygen therapy for treatment of wounds is a viable option and should be considered as part of any formulary for advanced wound treatment.
CDO therapy has been shown to be safe and efficacious on a wide variety of wounds. Overall, our findings are in line with a significant body of experimental data suggesting that increasing oxygen supply to diabetic and chronic wounds improves wound healing.
References1. Asmis R, Qiao M, Zhao Q. Low-Flow Oxygenation of Full-Excisional Skin Wounds on Diabetic Mice Improves Wound
Healing by Accelerating Wound Closure and Reepithelialization. Int Wound J 2010; 7: 349-357.2. Gordillo GM, Roy S, Khanna S, Schlanger R, Khandelwal S, Phillips G, Sen CK. Topical Oxygen Therapy Induces
VEGF Expression and Improves Closure of Clinically Presented Chronic Wounds. Clin Exp Pharmacol Physiol. 2008; 35: 957-964.
3. Tawfick W, Sultan S. Does Topical Wound Oxygen (TWO2) Offer an Improved Outcome Over Conventional Compression Dressings (CCD) in the Management of Refractory Venous Ulcers (RVU)? A Parallel Observational Comparative Study. Eur J Vasc Endovasc Surg. 2009; 38(1): 125-32.
4. Blackman E, Moore C, Hyatt J, Railton R, Frye C. Topical Wound Oxygen Therapy in the Treatment of Severe Diabetic Foot Ulcers: A Prospective Controlled Study. Ostomy Wound Manage. 2010 Jun; 56(6): 24-31.
5. Sen CK. Wound Healing Essentials: Let There Be Oxygen. Wound Rep Reg 2009; 17: 1–18.6. Gordillo GM, Sen CK. Evidence-Based Recommendations for the Use of Topical Oxygen Therapy in the Treatment
of Lower Extremity Wounds. Intl J Lower Extremity Wounds 2009; 8: 105-111.7. Schreml S, Szeimies RM, Prantl L, Karrer S, Landthaler M, Babilas P. Oxygen in Acute and Chronic Wound Healing.
British J Dermatology 2010; 163: 257-268.