Embed Size (px)
Citation preview
Int J Clin Exp Med 2017;10(10):14834-14840www.ijcem.com /ISSN:1940-5901/IJCEM0058067
Case Report Treatment of organized chronic subdural hematoma using urokinase
Ruizhi Wang, Ligui Gao, Haiyan Fu, Wei Shi
Department of Neurosurgery, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, PR China
Received May 23, 2017; Accepted July 25, 2017; Epub October 15, 2017; Published October 30, 2017
Abstract: Craniotomy and membranectomy are widely accepted for the treatment of organized chronic subdural he-matoma (CSDH); however, to our knowledge, the efficacy of burr hole irrigation and drainage with urokinase (UK) for organized CSDH has not been previously investigated. This case report describes 4 cases of organized CSDH, which were cured by UK injection into the hematoma cavity after one burr hole surgery. All patients were male (aged 55, 55, 58, and 76 years). One patient underwent an initial single burr hole craniotomy with a partial membranectomy and a burr hole 13 and 21 days after the first procedure. UK was subsequently injected into the hematoma cavity. One patient underwent burr hole surgery twice in 10 days, and UK was injected into the hematoma cavity after the second burr hole operation. Two patients underwent one burr hole operation and UK injection into the hematoma cavity following surgery. Organized hematoma drainage was satisfactory following UK administration. All patients exhibited full recovery without recurrence of the CSDH. There was no morbidity or mortality associated with UK injec-tion. After a follow-up period of two months, a computed tomography (CT) scan indicated complete resolution of the hematoma in all 4 cases. These findings provide preliminary evidence that UK treatment after CSDH is a beneficial, safe, and effective treatment.
Keywords: Organized chronic subdural hematoma, urokinase, treatment
Introduction
Chronic subdural hematoma (CSDH) is one of the most common clinical entities of intracra-nial hemorrhage in neurosurgical departments [1]. Most CSDH cases are treated via one burr hole craniotomy with or without saline irriga- tion using closed-system drainage [2, 3]. Im- portantly, the failure of CSDH treatment via burr hole evacuation occurs because of orga-nized CSDH [4-7]. To date, a large craniotomy with membranectomy is recommended as the sole approach for organized CSDH [4, 6, 7]. The clinical application of burr hole drainage com-bined with urokinase (UK) for intracranial hem-orrhage has been widely reported and accept-ed; however, the efficacy of this approach for organized CSDH remains uncertain. Here, we report a novel technique that included UK in- jection into the hematoma cavity to drain or- ganized CSDHs. The primary aim of this study was to evaluate the outcome and safety of UK injection in the subdural space for the treat-ment of organized CSDH. The findings indicated
this approach led to optimal results in all four cases of organized CSDH.
Case report
Case 1
A 55-year-old man was admitted to our depart-ment following two months of headaches and one day of abnormal consciousness and vo- miting. He had experienced a head injury two months prior, and a post-traumatic computed tomography (CT) scan indicated that there were no abnormal findings. He was diagnosed with CSDH in the left hemisphere via a CT scan on the day of admission (Figure 1A). Gait distur-bance, urinary incontinence, and altered men-tal status were noted during the neurological examination after admission to our hospital. The routine laboratory results were unremark-able. An operation that included a one burr ho- le craniotomy and closed-system drainage was performed, and an organized hematoma was identified during the operation. The localized,
Treatment of organized CSDH using urokinase
14835 Int J Clin Exp Med 2017;10(10):14834-14840
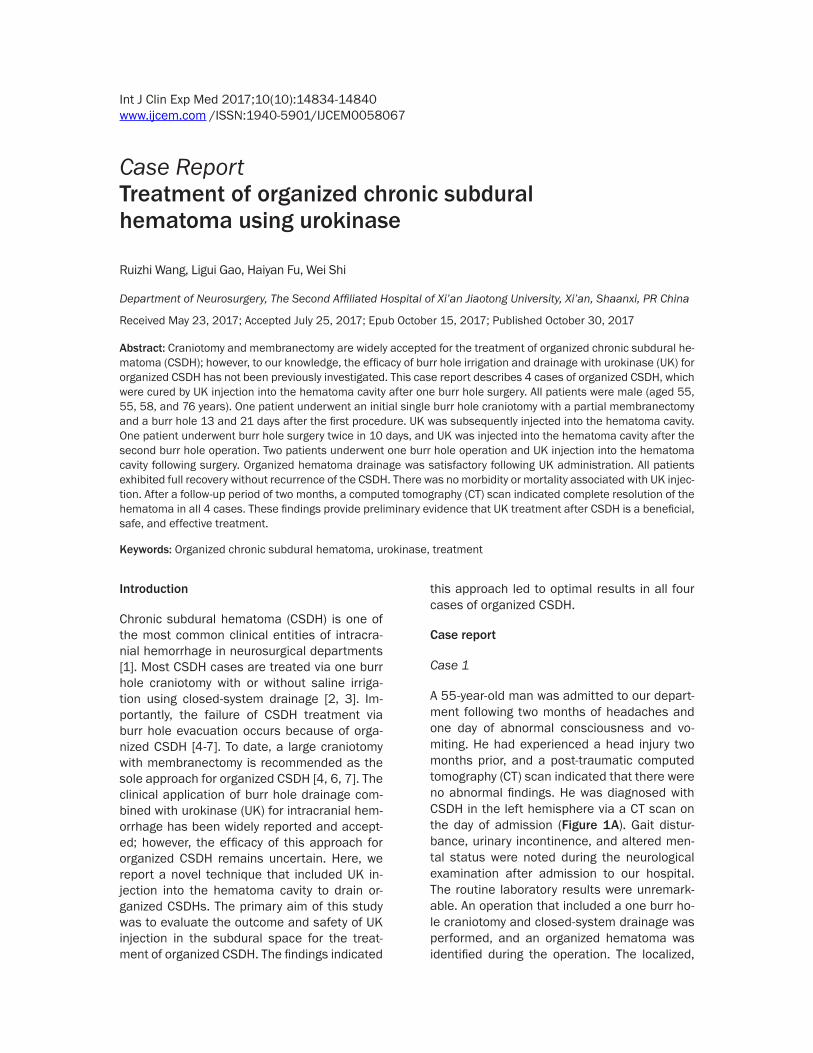
Figure 1. CT scan of Case 1. A. Preoperative CT scan indicates a CSDH in the right hemisphere with a mass effect. B. CT scan on day 1 after the initial burr hole indicates the partial CSDH was drained. C. CT scan on day 13 after the initial burr hole indicates CSDH recurrence. D. CT scan on day 8 after the craniotomy and partial membranectomy indicates recurrent CSDH. E. CT scan after 3 days of UK injections indicates a small amount of residual hematoma and a recovered midline shift. F. A two-month follow-up cranial CT scan indicates a complete resolution of the he-matoma.
organized hematoma under the burr hole was absorbed during the surgery, and the patient’s headaches, consciousness, and gait distur-bance remarkably improved one day after the operation with an alleviated mass effect (Figure 1B). Thirteen days after surgery, the patient exhibited dysphasia and seizures; a CT scan subsequently indicated an increased hemato-ma volume in the left hemisphere (Figure 1C). An operation that comprised a small cranioto-my and partial membranectomy under general anesthesia was performed to evacuate most of the organized clot, and his symptoms disap-peared the following day. Eight days after the second surgery, the patient complained of dys-phasia and headache. An increased subdural hematoma volume with a low density was iden-tified via CT scan (Figure 1D). Therefore, a sec-ond burr hole operation was performed, and the organized hematoma was identified during
the operation. After the operation, 20,000 in- ternational units (IUs) of UK (Tianjin Biochem Pharmaceutical Co., Ltd., Tianjin, China) was dissolved in three ml of saline and slowly inject-ed into the clot. The tube was subsequently flushed with two ml of normal saline, closed for two hours, and then opened to drain. A 120 ml volume of liquefied blood was drained after three days of UK injection. On day four after the second burr hole, a CT scan indicated a small amount of residual hematoma (Figure 1E). The patient was discharged 16 days after the oper-ation without neurological deficits. A two-month follow-up CT demonstrated a complete resolu-tion of the hematoma (Figure 1F).
Case 2
A 76-year-old man presented with a 10-day his-tory of dizziness and decreased muscle power
Treatment of organized CSDH using urokinase
14836 Int J Clin Exp Med 2017;10(10):14834-14840
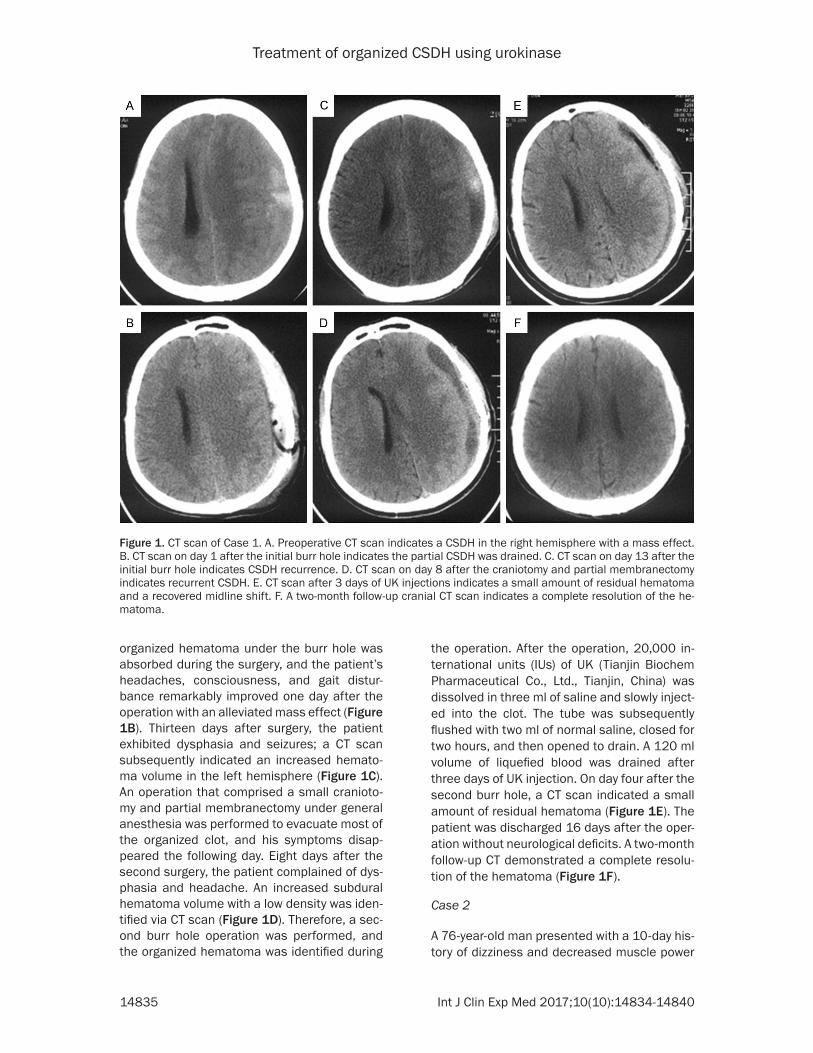
Figure 2. CT scan of Case 2. A. Preoperative CT scan indicates a right-sided CSDH with a mass effect. B. CT scan on day 10 af-ter the initial burr hole indicates recurrent CSDH. C. CT scan on day 1 after the second burr hole indicates a substantial amount of residual CSDH. D. CT scan after three days of UK injections indi-cates a small amount of residual hematoma. E. Two-month follow-up CT scan indicates excellent brain re-expansion.
in the right side of his body, particularly the limbs. His previous medical history was unre-markable with the exception of diabetes. A physical examination indicated 80% strength in the right upper and lower extremities. A CT scan indicated a CSDH in the left hemisphere (Figure 2A). The routine laboratory results were unremarkable with the exception of the plate- let number count, which was 63×109/L. An operation that comprised a one burr hole cra- niotomy was performed when the platelet num-ber count increased to 130×109/L. The orga-nized hematoma was identified during the op- eration. Approximately 10 ml of organized he- matoma under the burr hole was absorbed, and the patient’s strength in the right limbs returned to 100% one day after the burr hole procedure. On day 10 after the surgery, the patient complained of a headache and motor disturbances of the right limbs (80% strength). A CT image indicated the subdural hematoma volume had increased with a mixed density in the left hemisphere (Figure 2B). A second burr hole was performed 11 days after the initial procedure, and the organized hematoma was identified. A CT scan on day 1 after the second
burr hole indicates a substantial amount of residual CSDH (Figure 2C). A dose of 20,000 IU per day of UK was subsequently injected into the hematoma for three days. The total drain-age volume was 130 ml in three days, and a CT scan demonstrated a very small amount of residual hematoma (Figure 2D). The patient exhibited a good post-operative recovery and had no neurological deficits when discharged. A two-month follow-up CT scan indicated excel-lent brain re-expansion (Figure 2E).
Case 3
A 58-year-old male was diagnosed with CSDH and underwent a burr hole craniotomy with closed-system drainage one month prior to ad- mission to our hospital. The patient complain- ed of a headache three days prior and was admitted to our hospital because of recurrent CSDH. His previous medical history indicated thrombocytopenia. CT and magnetic resonan- ce (MR) images indicated left CSDH with mul- tiple compartments and septations (Figure 3A-C). The routine laboratory results indicated that the platelet number count was 50×109/L,
Treatment of organized CSDH using urokinase
14837 Int J Clin Exp Med 2017;10(10):14834-14840
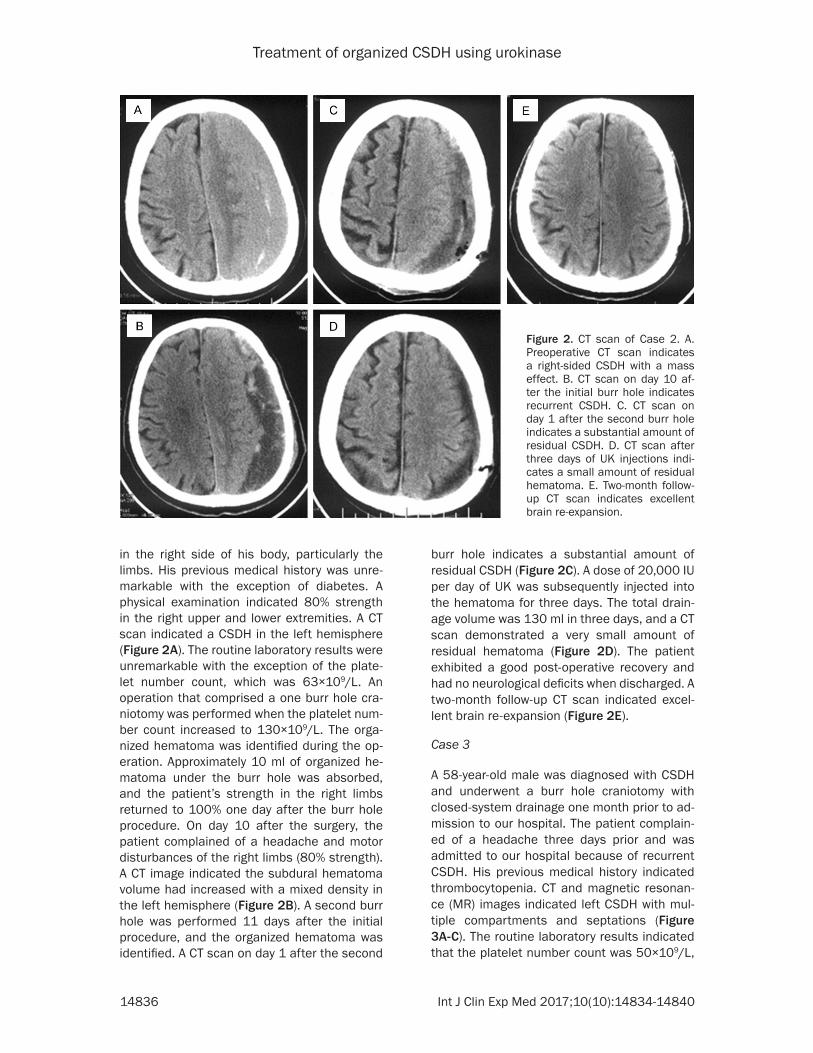
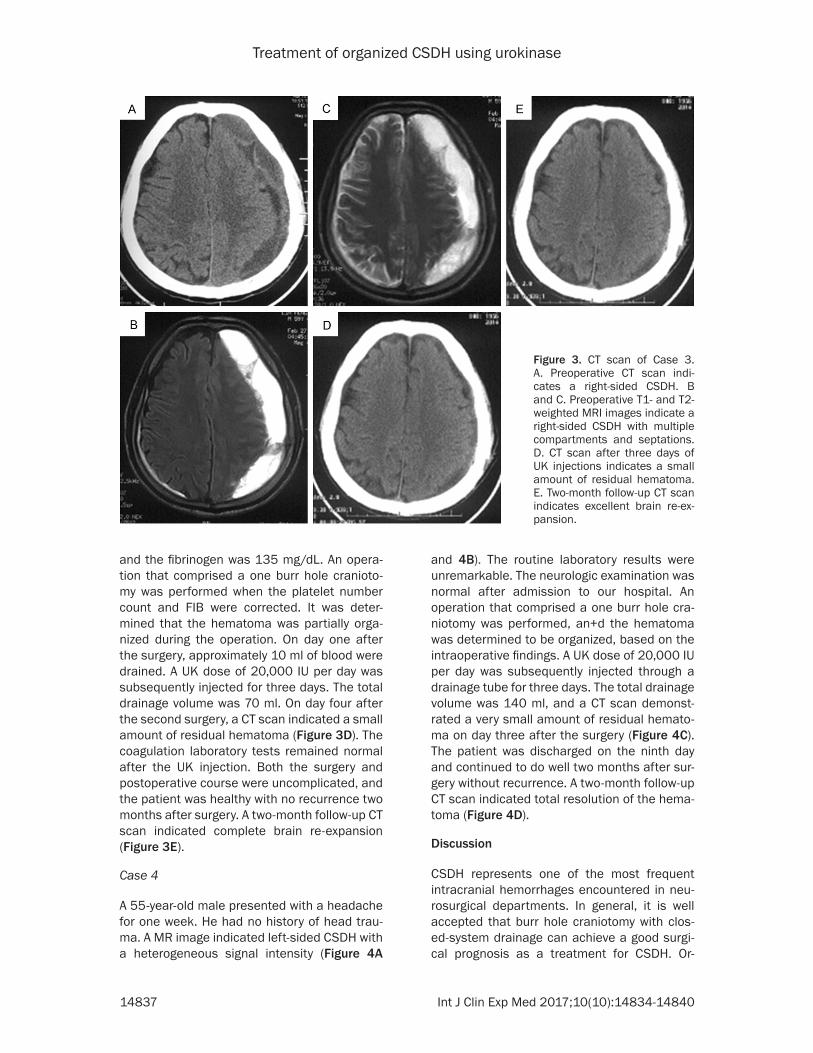
Figure 3. CT scan of Case 3. A. Preoperative CT scan indi-cates a right-sided CSDH. B and C. Preoperative T1- and T2-weighted MRI images indicate a right-sided CSDH with multiple compartments and septations. D. CT scan after three days of UK injections indicates a small amount of residual hematoma. E. Two-month follow-up CT scan indicates excellent brain re-ex-pansion.
and the fibrinogen was 135 mg/dL. An opera-tion that comprised a one burr hole cranioto- my was performed when the platelet number count and FIB were corrected. It was deter-mined that the hematoma was partially orga-nized during the operation. On day one after the surgery, approximately 10 ml of blood were drained. A UK dose of 20,000 IU per day was subsequently injected for three days. The total drainage volume was 70 ml. On day four after the second surgery, a CT scan indicated a small amount of residual hematoma (Figure 3D). The coagulation laboratory tests remained normal after the UK injection. Both the surgery and postoperative course were uncomplicated, and the patient was healthy with no recurrence two months after surgery. A two-month follow-up CT scan indicated complete brain re-expansion (Figure 3E).
Case 4
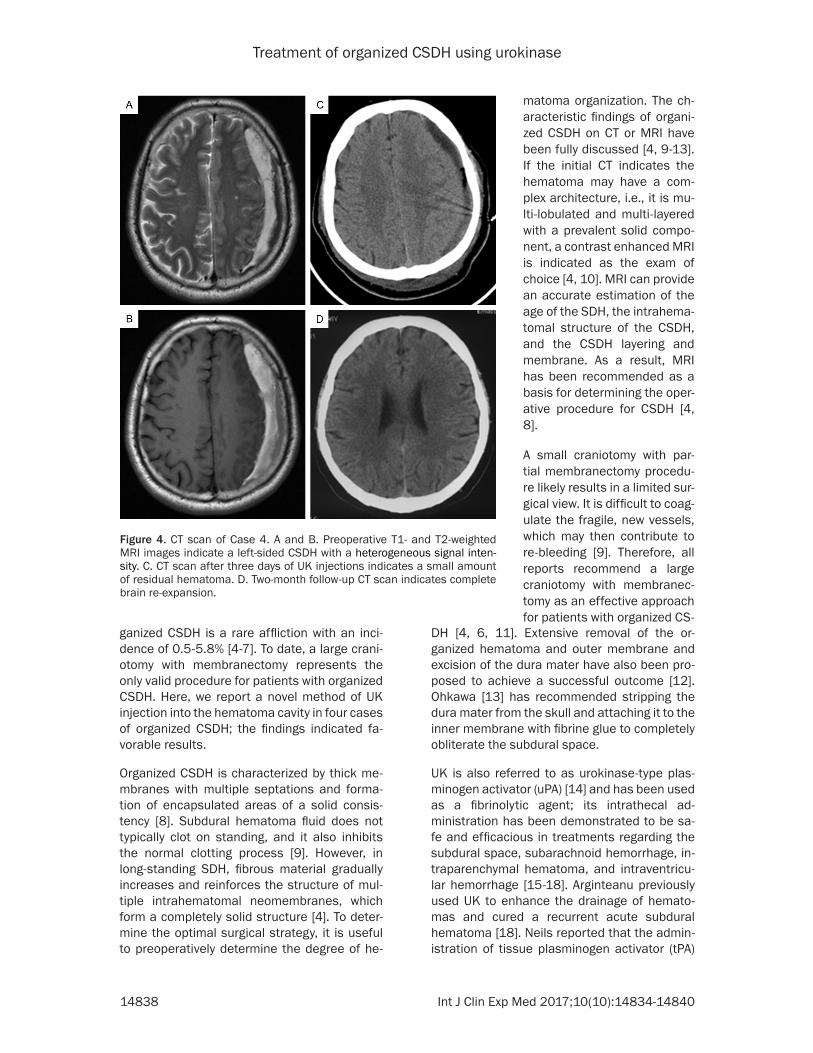
A 55-year-old male presented with a headache for one week. He had no history of head trau-ma. A MR image indicated left-sided CSDH with a heterogeneous signal intensity (Figure 4A
and 4B). The routine laboratory results were unremarkable. The neurologic examination was normal after admission to our hospital. An operation that comprised a one burr hole cra- niotomy was performed, an+d the hematoma was determined to be organized, based on the intraoperative findings. A UK dose of 20,000 IU per day was subsequently injected through a drainage tube for three days. The total drainage volume was 140 ml, and a CT scan demonst- rated a very small amount of residual hemato-ma on day three after the surgery (Figure 4C). The patient was discharged on the ninth day and continued to do well two months after sur-gery without recurrence. A two-month follow-up CT scan indicated total resolution of the hema-toma (Figure 4D).
Discussion
CSDH represents one of the most frequent intracranial hemorrhages encountered in neu-rosurgical departments. In general, it is well accepted that burr hole craniotomy with clos- ed-system drainage can achieve a good surgi-cal prognosis as a treatment for CSDH. Or-
Treatment of organized CSDH using urokinase
14838 Int J Clin Exp Med 2017;10(10):14834-14840
Figure 4. CT scan of Case 4. A and B. Preoperative T1- and T2-weighted MRI images indicate a left-sided CSDH with a heterogeneous signal inten-sity. C. CT scan after three days of UK injections indicates a small amount of residual hematoma. D. Two-month follow-up CT scan indicates complete brain re-expansion.
ganized CSDH is a rare affliction with an inci-dence of 0.5-5.8% [4-7]. To date, a large crani-otomy with membranectomy represents the only valid procedure for patients with organized CSDH. Here, we report a novel method of UK injection into the hematoma cavity in four cases of organized CSDH; the findings indicated fa- vorable results.
Organized CSDH is characterized by thick me- mbranes with multiple septations and forma-tion of encapsulated areas of a solid consis- tency [8]. Subdural hematoma fluid does not typically clot on standing, and it also inhibits the normal clotting process [9]. However, in long-standing SDH, fibrous material gradually increases and reinforces the structure of mul- tiple intrahematomal neomembranes, which form a completely solid structure [4]. To deter-mine the optimal surgical strategy, it is useful to preoperatively determine the degree of he-
DH [4, 6, 11]. Extensive removal of the or- ganized hematoma and outer membrane and excision of the dura mater have also been pro-posed to achieve a successful outcome [12]. Ohkawa [13] has recommended stripping the dura mater from the skull and attaching it to the inner membrane with fibrine glue to completely obliterate the subdural space.
UK is also referred to as urokinase-type plas-minogen activator (uPA) [14] and has been used as a fibrinolytic agent; its intrathecal ad- ministration has been demonstrated to be sa- fe and efficacious in treatments regarding the subdural space, subarachnoid hemorrhage, in- traparenchymal hematoma, and intraventricu-lar hemorrhage [15-18]. Arginteanu previously used UK to enhance the drainage of hemato-mas and cured a recurrent acute subdural hematoma [18]. Neils reported that the admin-istration of tissue plasminogen activator (tPA)
matoma organization. The ch- aracteristic findings of organi- zed CSDH on CT or MRI have been fully discussed [4, 9-13]. If the initial CT indicates the hematoma may have a com-plex architecture, i.e., it is mu- lti-lobulated and multi-layered with a prevalent solid compo-nent, a contrast enhanced MRI is indicated as the exam of choice [4, 10]. MRI can provide an accurate estimation of the age of the SDH, the intrahema-tomal structure of the CSDH, and the CSDH layering and membrane. As a result, MRI has been recommended as a basis for determining the oper-ative procedure for CSDH [4, 8].
A small craniotomy with par- tial membranectomy procedu- re likely results in a limited sur-gical view. It is difficult to coag-ulate the fragile, new vessels, which may then contribute to re-bleeding [9]. Therefore, all reports recommend a large craniotomy with membranec-tomy as an effective approach for patients with organized CS-

Treatment of organized CSDH using urokinase
14839 Int J Clin Exp Med 2017;10(10):14834-14840
increased the drained hematoma volume and reduced the symptomatic recurrence rate of CSDH [19]. To date, the injection of UK into the hematoma cavity in organized CSDH treatment has not been reported. Our experience with these 4 patients provides robust, novel evi-dence that this approach is a safe procedure with no complications related to the adminis-tration of UK in such cases. In addition, UK administration via the subdural drain catheter led to the liquefaction of the organized hema-toma and promoted drainage of the clot, which made a large craniotomy unnecessary. The ad- dition of UK leads to a hyperfibrinolytic state, which subsequently results in no further hem-orrhage, but a more liquefied hematoma; this favors the drainage of the organized hemato- ma after burr hole procedures. Compared with the UK treatment method, the performance of a large craniotomy for CSDH patients requires more time and is more invasive. Moreover, the aggressive removal of membranes may evoke postoperative seizures, which result from brain damage via traction in an attempt to remove the membranes with tight adherence to the cortex [4].
Although membranectomy has been consid-ered a key technique that produces excellent results [4], in our four cases, we demonstrated that the brain completely re-expanded, where-as the hematoma membrane remained intact. These findings indicate full recovery of the or- ganized CSDH does not require membranecto-my. It is well known that the parietal mem-branes of hematoma vessels are fragile; thus, neomembranes undergo repetitive multifocal bleeding [4]. Therefore, these vessels are vul-nerable to mechanical manipulation and carry a high risk of re-bleeding [1]. Moreover, UK administration in dissolving coronary artery clots has been associated with intracerebral hemorrhage in 1.6% of patients [20]. In our cases, no patient had a history of aspirin me- dication, and we adopted a reasonable dose of 20,000 IU (diluted in three ml of the saline solution), which has been demonstrated to be safe and effective in intraventricular hemor-rhage [15, 17, 18]. After three UK injections, most organized hematomas were drained wi- thout re-bleeding, and the postoperative CT scans indicated brain re-expansion. The results of the 4 cases indicate this dose of UK is suf- ficient for the liquefaction of organized CSDH.
The toxicity of UK has not been previously dis-cussed in the management of non-traumatic intraventricular hemorrhage [21]. In contrast, uPA favorably influences injured brain cells by delaying neurodegeneration; thus, it may be beneficial as a neuroprotection for brain inju-ries [22].
Despite these promising findings, several li- mitations regarding this study must be consid-ered in the interpretation of these findings. First, it is a retrospective study and has limited cases from single institution. This limitation should be addressed in a larger, prospective study of organized CSDH treatment. Furthe- rmore, UK has no effect on calcified or fibrotic tissue which can be found in rare cases of organized CSDH.
Conclusion
This case report described four cases with or- ganized CSDH who obtained favorable results after UK injection into the hematoma cavity through a drainage tube. Based on the excel-lent recovery and reduced surgical invasion, this novel preliminary evidence supports the utility of this procedure for patients with orga-nized CSDHs.
Disclosure of conflict of interest
None.
Address correspondence to: Ruizhi Wang, Depart- ment of Neurosurgery, The Second Affiliated Hospi- tal of Xi’an Jiaotong University, 157 Xi Wu Road, Xi’an 710004, Shaanxi, PR China. Tel: 0086-159916- 35690; Fax: 0086-29-87678323; E-mail: wrz510@ 163.com
References
[1] Lee JY, Ebel H, Ernestus RI and Klug N. Various surgical treatments of chronic subdural hema-toma and outcome in 172 patients: is mem-branectomy necessary? Surg Neurol 2004; 61: 523-527.
[2] Gurelik M, Aslan A, Gurelik B, Ozum U, Karadag O and Kars HZ. A safe and effective method for treatment of chronic subdural haematoma. Can J Neurol Sci 2007; 34: 84-87.
[3] Okada Y, Akai T, Okamoto K, Iida T, Takata H and Iizuka H. A comparative study of the treat-ment of chronic subdural hematoma--burr hole drainage versus burr hole irrigation. Surg Neu-rol 2002; 57: 405-409.
Treatment of organized CSDH using urokinase
14840 Int J Clin Exp Med 2017;10(10):14834-14840
[4] Rocchi G, Caroli E, Salvati M and Delfini R. Membranectomy in organized chronic subdu-ral hematomas: indications and technical notes. Surg Neurol 2007; 67: 374-380; discus-sion 380.
[5] Sambasivan M. An overview of chronic subdu-ral hematoma: experience with 2300 cases. Surg Neurol 1997; 47: 418-422.
[6] Shrestha P, Pant B, Shrestha P and Rajbhan-dari P. Organized subdural hematoma with thick membrane in chronic subdural hemato-ma. JNMA J Nepal Med Assoc 2012; 52: 1-5.
[7] Imaizumi S, Onuma T, Kameyama M and Na-ganuma H. Organized chronic subdural hema-toma requiring craniotomy--five case reports. Neurol Med Chir (Tokyo) 2001; 41: 19-24.
[8] Callovini GM, Bolognini A, Callovini G and Gam-mone V. Primary enlarged craniotomy in orga-nized chronic subdural hematomas. Neurol Med Chir (Tokyo) 2014; 54: 349-356.
[9] Weir B and Gordon P. Factors affecting coagu-lation: fibrinolysis in chronic subdural fluid col-lections. J Neurosurg 1983; 58: 242-245.
[10] Kim JH, Kang DS, Kim JH, Kong MH and Song KY. Chronic subdural hematoma treated by small or large craniotomy with membranecto-my as the initial treatment. J Korean Neuro-surg Soc 2011; 50: 103-108.
[11] Mondorf Y, Abu-Owaimer M, Gaab MR and Oer-tel JM. Chronic subdural hematoma--cranioto-my versus burr hole trepanation. Br J Neuro-surg 2009; 23: 612-616.
[12] Fukazawa K, Sakakura M, Niwa S, Yamamoto J, Kuraishi K and Mouri G. [A case of organized chronic subdural hematoma showing an early recurrence after craniotomy]. No Shinkei Geka 2005; 33: 389-394.
[13] Ohkawa T, Ogura M, Tanaka S, Terada T and Itakura T. [Craniotomy for organized subdural hematoma]. No Shinkei Geka 2005; 33: 357-362.
[14] Blasi F, Vassalli JD and Dano K. Urokinase-type plasminogen activator: proenzyme, receptor, and inhibitors. J Cell Biol 1987; 104: 801-804.
[15] Coplin WM, Vinas FC, Agris JM, Buciuc R, Mi-chael DB, Diaz FG and Muizelaar JP. A cohort study of the safety and feasibility of intraven-tricular urokinase for nonaneurysmal sponta-neous intraventricular hemorrhage. Stroke 1998; 29: 1573-1579.
[16] Nyquist P and Hanley DF. The use of intraven-tricular thrombolytics in intraventricular hem-orrhage. J Neurol Sci 2007; 261: 84-88.
[17] Ziai WC, Triantaphyllopoulou A, Razumovsky AY and Hanley DF. Treatment of sympathomimetic induced intraventricular hemorrhage with in-traventricular urokinase. J Stroke Cerebrovasc Dis 2003; 12: 276-279.
[18] Arginteanu MS, Byun H and King W. Treatment of a recurrent subdural hematoma using uroki-nase. J Neurotrauma 1999; 16: 1235-1239.
[19] Neils DM, Singanallur PS, Wang H, Tracy P, Klopfenstein J, Dinh D, Elwood PW, Fassett D, McCall T, Lin J and Tsung A. Recurrence-free chronic subdural hematomas: a retrospective analysis of the instillation of tissue plasmino-gen activator in addition to twist drill or burr hole drainage in the treatment of chronic sub-dural hematomas. World Neurosurg 2012; 78: 145-149.
[20] Aldrich MS, Sherman SA and Greenberg HS. Cerebrovascular complications of streptoki-nase infusion. JAMA 1985; 253: 1777-1779.
[21] Gaberel T, Magheru C and Emery E. Manage-ment of non-traumatic intraventricular hemor-rhage. Neurosurg Rev 2012; 35: 485-494; dis-cussion 494-485.
[22] Cho E, Lee KJ, Seo JW, Byun CJ, Chung SJ, Suh DC, Carmeliet P, Koh JY, Kim JS and Lee JY. Neuroprotection by urokinase plasminogen ac-tivator in the hippocampus. Neurobiol Dis 2012; 46: 215-224.