Embed Size (px)
Citation preview

Case ReportTraumatic Isolated Trapezium Dislocation withoutFracture: A Case Report and Review of the Literature
Robert M. Kenyon, Enda G. Kelly, and Benny Padinjarathala
Trauma and Orthopaedics Department, University Hospital Waterford, Waterford, Ireland
Correspondence should be addressed to Robert M. Kenyon; [email protected]
Received 1 October 2015; Accepted 24 February 2016
Academic Editor: Pedro Carpintero
Copyright © 2016 Robert M. Kenyon et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Isolated dislocation of the trapezium is an uncommon injury. There are sixteen cases to date reported in the literature. Themanagement of these cases has varied from complete excision to open or closed reduction, with or without percutaneous wiring.This paper presents a case of an isolated dislocation of the trapezium without fracture, managed with closed reduction andpercutaneous wiring, resulting in a good functional outcome.
1. Introduction
Traumatic dislocation of the trapezium is a relatively rareinjury [1]. The most common mechanism associated withthis injury tends to be either a direct blow or a crushinjury [2]. Dislocation of the trapeziumwithout an associatedcarpal or metacarpal fracture is rarer still [3–6]. The strongdorsal ligamentous attachments to the trapezium ensurethat traumatic force will tend to result in first metacarpalfractures in preference to trapeziumdislocation [1]. Given thepropensity for a grinding or crushing force in these injuriesand the likelihood of extensive associated soft tissue damage,these cases often present as open injuries. We describe thecase of a closed trapezium dislocation with no associatedfracture.
2. Case Presentation
A 47-year-old right hand dominant male working as a stablehand presented to the emergency department of a tertiarytrauma and orthopedic referral center following a crushinjury to the left hand. The injury had occurred while thepatient had been assisting a friend to park a 4 × 4 vehicle.The vehicle had been reversing slowly towards a wall with thepatient’s hand behind the vehicle. The mechanism of injurysuggested axial loading of the thumb between the vehicle andthe wall. He presented directly to the emergency department
with severe pain, swelling, and an obvious deformity at thewrist. The patient had no background medical or surgicalhistory of note and reported no previous injuries to theaffected limb. He was an active smoker of 30 cigarettes perday.
On examination in the emergency department, he hadsignificant pain and swelling in the left wrist and forearm.There was a superficial abrasion over the dorsal aspect of theaffected hand; however, this was considered to be a closedinjury. There was significant tenderness over the carpals,particularly at the trapezium, with associated reduced rangeofmotion at thewrist and thumb.Therewas noneurovascularcompromise or associated tendon injury.
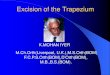
TheAP radiograph reveals disruption of the continuationof arc I between the proximal border of the triquetrum andthe proximal border of the trapezium, with the trapeziumdisplaced in a radial direction (Figure 1). This represents avolar dislocation of the trapezium. There was no associatedfracture of the trapezium or any other associated bonyinjuries.
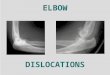
The patient subsequently underwent closedmanipulationunder general anesthesia. The surgeon achieved anatomicalreduction by gripping the patient’s thumb in one hand andapplying a distracting force, while simultaneously applyingpressure on the radial aspect of the trapeziumwith the thumbof the surgeon’s other hand.The trapeziumwas stabilizedwiththree 1.6mm Kirschner wires percutaneously inserted from
Hindawi Publishing CorporationCase Reports in OrthopedicsVolume 2016, Article ID 1798941, 3 pageshttp://dx.doi.org/10.1155/2016/1798941

2 Case Reports in Orthopedics
Figure 1: Preoperative radiographs.
Figure 2: Intraoperative radiographs.
the radial side. One wire passed from trapezium to scaphoid,one wire passed from trapezium to capitate, and one wirepassed from trapezium to trapezoid (Figure 2).The wrist wasimmobilized in a below-elbowmolded POP thumb spica cast.The patient was discharged later on the same day.
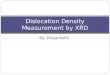
The patient remained in cast for a total of six weeksat which point the percutaneous wires were removed inthe outpatient department and the hand and wrist weremobilized (Figure 3). He was referred to the local handtherapy service. Follow-up examination at three monthsrevealed excellent range of motion (wrist flexion 60∘, wristextension 30∘, pronation 80∘, supination 80∘, and radialabduction at base of thumb 60∘). He had returned to fullmanual work activities at 8 weeks postoperatively and was nolonger requiring analgesia (Figure 4).
3. Discussion
A systematic method for evaluating the alignment of thecarpal bones is essential at the initial assessment of wristinjuries to ensure that uncommon fracture/dislocations arediagnosed and treated early. The assessment of carpal align-ment in trauma was first described in detail by Gilula in 1979[7].There are three arcs within the wrist seen on anteroposte-rior plain film radiograph, which if disrupted strongly suggestan abnormality of alignment at the site of disruption. Arc Iis the convex curve along the proximal surfaces of scaphoid,lunate, and triquetrum, arc II is the concave curve along thedistal surfaces of scaphoid, lunate, and triquetrum, and arcIII is the convex curve along the proximal surfaces of capitateand hamate. Carpal dislocations generally occur as a resultof high-energy trauma. Dislocations of the trapezium tend
Figure 3: Radiographs at 6 weeks.
Figure 4: Radiographs at 3 months.
to occur in either a volar or a radiodorsal direction [2]. Therelative strength of the ligaments attached to the trapeziumdorsally compared to those attaching to the volar surfaceresults in a greater propensity for volar dislocation [8].
There are only thirteen existing reports depicting a totalof sixteen cases of isolated trapezium dislocations publishedin the literature since the 1950s [1, 3–6, 8–15]. These includeboth open and closed dislocations and the majority of theseinvolve an associated fracture of either the trapezium or thesurrounding bones. Five cases report an isolated trapeziumdislocation without any associated fracture of the trapeziumor adjacent bones [3–6]. Of these, two report an open injury[4] and three report a closed injury [3, 5, 6]. In addition,there were also four reported cases that involved only minoravulsion type fractures of the trapezium [1, 8, 9, 12].
Excision of the trapezium has been described in thetreatment of isolated dislocation in which reduction wasnot possible [4, 8]. The potential risk of avascular necrosishas been suggested as the rationale for such an approach[4]. However, in general, this option is considered as asalvage technique only [2]. In the majority of reported cases,percutaneous fixation with Kirschner wires has been usedwith acceptable results [1, 5, 9–12, 14, 15]. An open reductiontechnique has been employed in all cases where the fracturewas open.Themanagement of closed dislocations has varied.Some studies advocate an open reduction, regardless ofwhether the injury is open or closed to begin with [9]. Three

Case Reports in Orthopedics 3
cases demonstrated a successful closed reduction [3, 6, 11]and in the case of McKie et al. and Vente and de Ruiterthese dislocations were successfully treated without the useof percutaneous wiring [3, 6].
4. Conclusion
This case demonstrates that a closed, isolated dislocation ofthe trapezium with no associated fracture can be safely andeffectively treated with closed reduction and percutaneouswire fixation. The following learning points can be gleanedfrom the case and supporting literature:
(i) A systematicmethodof evaluating carpal alignment isessential to ensure early pick-up of uncommon carpalinjuries.
(ii) Axial loading of the wrist may result in an isolateddislocation of the trapezium without associated frac-tures.
(iii) Closed reduction should be attempted with percuta-neous wire fixation.
(iv) Open reduction should be employed if there is a fail-ure to achieve adequate reduction.
(v) Excision of the trapezium is rarely necessary.
Competing Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] B. I. Wintman, J. L. Fowler, and M. E. Baratz, “Traumatic dislo-cation of trapezium: case report and review of the literature,”American Journal of Orthopedics, vol. 29, no. 3, pp. 229–232,2000.
[2] S. E. Clarke and J. R. Raphael, “Combined dislocation of thetrapezium and the trapezoid: a case report with review of theliterature,” Hand, vol. 5, no. 1, pp. 111–115, 2010.
[3] L. D. McKie, L. G. Rocke, and T. C. Taylor, “Isolated dislocationof the trapezium,” Archives of Emergency Medicine, vol. 5, no. 1,pp. 38–40, 1988.
[4] C. L. Peterson, “Dislocation of the multangulum majus ortrapezium (and its treatment in 2 cases with extirpation),”ArchivumChirurgicumNeerlandicum, vol. 2, no. 4, pp. 369–376,1950.
[5] D. A. Sherlock, “Traumatic dorsoradial dislocation of the tra-pezium,”The Journal of Hand Surgery, vol. 12, no. 2, pp. 262–265,1987.
[6] J. P. Vente and K. de Ruiter, “Complete dislocation of thetrapezium multangulum majus,” The Netherlands Journal ofSurgery, vol. 35, no. 1, pp. 33–35, 1983.
[7] L. A. Gilula, “Carpal injuries: analytic approach and case exer-cises,” American Journal of Roentgenology, vol. 133, no. 3, pp.503–517, 1979.
[8] I. Goldberg, S. Amit, A. Bahar, andM. Seelenfreund, “Completedislocation of the trapezium (multangulummajus),”The Journalof Hand Surgery, vol. 6, no. 2, pp. 193–195, 1981.
[9] S. Boe, “Dislocation of the trapezium (multangulum majus): acase report,” Acta Orthopaedica, vol. 50, no. 1, pp. 85–86, 1979.
[10] A. F. M. Brewood, “Complete dislocation of the trapezium: acase report,” Injury, vol. 16, no. 5, pp. 303–304, 1985.
[11] A.W. Dunn, “Fractures and dislocations of the carpus,”The Sur-gical Clinics of North America, vol. 52, no. 6, pp. 1513–1538, 1972.
[12] T. Ichikawa and G. Inoue, “Complete dislocation of thetrapezium. Case report,” Scandinavian Journal of Plastic andReconstructive Surgery andHand Surgery, vol. 33, no. 3, pp. 335–337, 1999.
[13] M. U. Mumtaz and N. A. Drabu, “Open complete dislocation oftrapezium with a vertically split fracture: a case report,” CasesJournal, vol. 2, article 9092, 2009.
[14] L. P. Seimon, “Compound dislocation of a trapezium. A casereport,”The Journal of Bone & Joint Surgery—American Volume,vol. 54, no. 6, pp. 1297–1300, 1972.
[15] M. W. Siegel and H. Hertzberg, “Complete dislocation of thegreater multangular (trapezium). A case report,”The Journal ofBone & Joint Surgery—American Volume, vol. 51, no. 4, pp. 769–772, 1969.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com