Embed Size (px)
Citation preview
CASE REPORT
Necrotizing Fasciitis of Abdominal Wallin AIDS
PRAVEEN K. ROY, MD, SANJAY C. PATEL, MD, and YASH P. KATARIA, MDKEY WORDS: necrotizing fasciitis; abdominal wall; AIDS; percutaneous endoscopic gastrostomy.
Necrotizing fasciitis (NF) is an uncommon soft tissueinfection, caused by toxin-producing virulent bacteria.It is characterized by widespread fascial necrosis withrelative sparing of the skin and underlying muscle.Recent outbreaks that have been publicized by the laypress variously as the “killer bug,” “flesh-eating bac-teria,” and “galloping gangrene,” have once againpiqued the interest of the public in this disorder (1).Although it can occur in any part of the body, theextremities, abdominal wall, and perineum are themost common sites of infection. It is often associatedwith systemic toxicity and is rapidly fatal unlesspromptly recognized and aggressively treated. Al-though immunodeficiency states have been identifiedas a risk factor, there is only one case of NF (involvingthe cervical region) reported in acquired immunode-ficiency syndrome (AIDS) (2). We describe a case ofnecrotizing fasciitis of the abdominal wall in a patientwith AIDS.
CASE REPORT
A 42-year-old female was admitted into our hospital witha one-day history of left upper quadrant abdominal painand fever. The pain was of rapid onset, sharp, and contin-uous. She denied any abdominal distension, diarrhea, orconstipation. Her past medical history included a history ofAIDS with a CD4 count of 10. Six months prior to presen-tation she had a percutaneous endoscopic gastrostomy(PEG) tube placed due to oral herpetic ulcerations. Twomonths prior to admission, the lesions resolved and thePEG tube was removed. Medications on admission in-cluded fluconazole, prednisone, zidovudine, clarithromycin,and trimethoprim-sulfamethoxazole. Vital signs on admis-sion were temperature of 102°F, blood pressure 150/80 mm
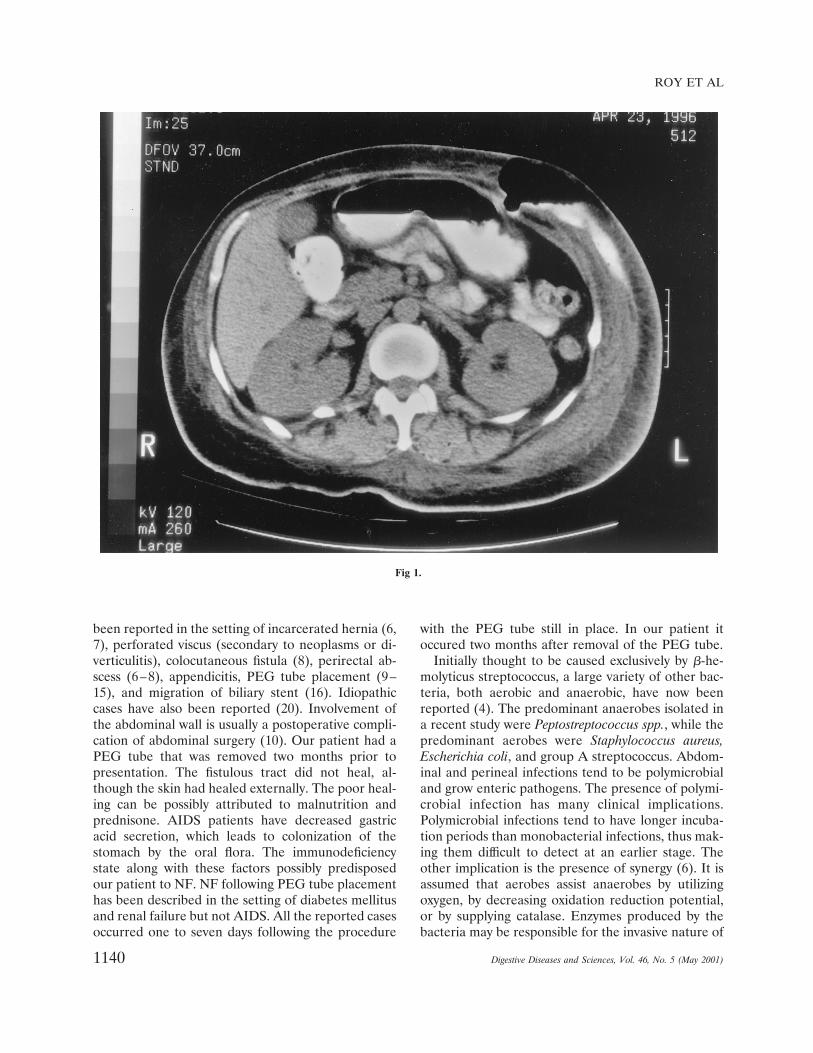
Hg, pulse 120 beats per min. On examination there wasmild erythema of the skin in the left upper quadrant. ThePEG tube site was well healed. Tenderness was present onpalpation. Initially there were no peritoneal signs. Labora-tory values on admission revealed white blood cell count of940 cells/mm3, hemoglobin 8.4 g/dl, platelets 266,000 cells/dl. Blood cultures were negative. Amylase and lipase werewithin normal limits. Liver function tests were also normal.Serum lactic acid level was elevated. Hypocalcemia waspresent. Over the next several hours she rapidly becamehypotensive, responding to intravenous fluids and vasopres-sors. The erythema on the abdominal wall expanded rapidlyto involve the left flank and most of the anterior abdominalwall. Peritoneal signs and crepitus were present at thisstage. Plain abdominal films of the abdomen did not revealany signs of perforation, obstruction, or gas in the subcuta-neous tissue. CT scan showed inflammation along the fas-cial planes, gas and fluid, and a persistent PEG tube tractfrom the skin (Figure 1). She was started on broad-spectrum intravenous antibiotics. Surgical treatment wasoffered to the patient, but she declined and died at homethree weeks later.
DISCUSSION
This is the first case report of NF of the abdominalwall in AIDS. Most cases of NF in adults are associ-ated with a predisposing condition such as diabetesmellitus, immunodeficiency states, obesity, malig-nancy, renal failure, peripheral vascular disease, in-travenous drug abuse, and malnutrition (3). The ma-jority of the patents have two or more predisposingfactors (4). AIDS has not been reported to be a riskfactor. Necrotizing fasciitis can occur in any region ofthe body, most commonly involving the extremities,abdomen, and perineum. Retroperitoneal involve-ment has also been reported (5). The involvement ofthe abdominal wall is associated with a poor progno-sis. It can extend onto the flanks and the chest wall.No immediate inciting event could be found in ourpatient. Some inciting events reported include skinabrasion, cut, burn, laceration, bite, injection, andsurgical incision. In gastroenterology practice, NF has
Manuscript received August 2, 1999; revised manuscript receivedMarch 17, 2000; accepted July 31, 2000.
From the Department of Medicine, East Carolina UniversitySchool of Medicine, Greenville, North Carolina 27858.
Address for reprint requests: Dr. Praveen K. Roy, DigestiveDiseases Branch, National Institutes of Health, Bldg 10, Rm 9C-103, 10 Center Drive, Bethesda, Maryland 20892-1804.
Digestive Diseases and Sciences, Vol. 46, No. 5 (May 2001), pp. 1139–1142
1139Digestive Diseases and Sciences, Vol. 46, No. 5 (May 2001)0163-2116/01/0500-1139$19.50/0 © 2001 Plenum Publishing Corporation
been reported in the setting of incarcerated hernia (6,7), perforated viscus (secondary to neoplasms or di-verticulitis), colocutaneous fistula (8), perirectal ab-scess (6–8), appendicitis, PEG tube placement (9–15), and migration of biliary stent (16). Idiopathiccases have also been reported (20). Involvement ofthe abdominal wall is usually a postoperative compli-cation of abdominal surgery (10). Our patient had aPEG tube that was removed two months prior topresentation. The fistulous tract did not heal, al-though the skin had healed externally. The poor heal-ing can be possibly attributed to malnutrition andprednisone. AIDS patients have decreased gastricacid secretion, which leads to colonization of thestomach by the oral flora. The immunodeficiencystate along with these factors possibly predisposedour patient to NF. NF following PEG tube placementhas been described in the setting of diabetes mellitusand renal failure but not AIDS. All the reported casesoccurred one to seven days following the procedure
with the PEG tube still in place. In our patient itoccured two months after removal of the PEG tube.
Initially thought to be caused exclusively by b-he-molyticus streptococcus, a large variety of other bac-teria, both aerobic and anaerobic, have now beenreported (4). The predominant anaerobes isolated ina recent study were Peptostreptococcus spp., while thepredominant aerobes were Staphylococcus aureus,Escherichia coli, and group A streptococcus. Abdom-inal and perineal infections tend to be polymicrobialand grow enteric pathogens. The presence of polymi-crobial infection has many clinical implications.Polymicrobial infections tend to have longer incuba-tion periods than monobacterial infections, thus mak-ing them difficult to detect at an earlier stage. Theother implication is the presence of synergy (6). It isassumed that aerobes assist anaerobes by utilizingoxygen, by decreasing oxidation reduction potential,or by supplying catalase. Enzymes produced by thebacteria may be responsible for the invasive nature of
Fig 1.
ROY ET AL
1140 Digestive Diseases and Sciences, Vol. 46, No. 5 (May 2001)

the infection. Heparinase, produced by Bacteroidesand Fusobacterium, results in intravascular coagula-tion, and collagenase produced by Clostridia causetissue destruction.
Owing to the paucity of skin findings in the disease,early diagnosis is often difficult and relies on a highindex of suspicion. The affected area is initially ery-thematous, edematous, without sharp margins, hot,shiny, and exquisitely tender. Skin breakdown withbullae formation and frank cutaneous gangrene fol-lows. Severe pain, which is localized and out of pro-portion to the presenting symptom, is an importantdiagnostic clue. Pain may be absent in patients withneurologic disorders. Other clinical features includefever (86%), tachycardia (80%), leukocytosis (78%),localized edema (77%), foul odor (70%), crepitations(39%), and local anesthesia (24%) (6). Systemic tox-icity is prominent. Hypotension can be a presentingsign in up to a third of patients. Laboratory evaluationcommonly reveals leukocytosis, thrombocytopenia,azotemia, and increased levels of creatinine phos-phokinase (CPK). Hypocalcemia and lactic acidosisoccur in the presence of extensive necrosis. Bloodcultures are frequently positive, although in our casethey were negative. Gram stain of the exudate usuallyreveals a mixture of organisms. The necrotic center isthe best place for obtaining a specimen. Culture ofthe soft tissue debris yields more organisms than swabculture. Frozen section of soft tissue biopsy has beenshown to aid in making an early diagnosis. Someinvestigators even advocate immediate surgical explo-ration with biopsy and frozen section examinationwhen the diagnosis is in doubt (3). Imaging studiescan also aid in diagnosing NF. Plain radiographs aremore sensitive than physical examination in detectingsoft tissue gas, and CT scans are even more accuratethan plain radiographs in detecting soft tissue gas.They are also helpful in delineating the extent ofspread of the infection and may also reveal the un-derlying pathology. Ultrasound is of limited value.MRI can also be used for diagnosis.
The cornerstone of management of NF is earlydiagnosis and aggressive treatment to reduce morbid-ity and mortality. Treatment modalities include sur-gical debridement, antibiotic therapy, intravenous flu-ids, and nutritional support. Significant morbidityexists if the surgery is delayed more than 12 hrs (18).Hyperbaric oxygen may be useful, although its efficacyhas not been proven in clinical studies. Mortality ratesas high as 76% have been reported. However, pro-spective studies have shown that mortality rate can bereduced to 10% by aggressive surgical management.
The proximate cause of death is usually overwhelm-ing sepsis and multiple organ failure (7).
In summary, we present the first case of NF of theabdominal wall in AIDS. Multiple factors includingthe immunodeficiency state in AIDS patients canpredispose these individuals to NF. Awareness of thisdisorder is important as early diagnosis and aggres-sive surgical debridement along with supportive mea-sures can be life-saving.
SUMMARY
Necrotizing fasciitis (NF) is an uncommon but po-tentially lethal soft-tissue infection. Mortality rate ishigh and has not changed since it was first describedby Meleny. Although immunodeficiency is a risk fac-tor for NF, there is only one reported case of NF inAIDS involving the cervical region. We report thefirst case of necrotizing fasciitis of the abdominal wallin an AIDS patient.
REFERENCES
1. Nowak R: Flesh eating bascteria: Not new but still worrisome.Science 264:1665, 1994
2. Chidzonga MM: Necrotizing fasciitis of the cervical region inan AIDS patient. J Oral Maxillofac Surg 54:638–640, 1996
3. Green RJ, Dafoe DC, Raffin TA: Necrotizing fasciitis. Chest110:219–229, 1996
4. Brook I, Frazier EH: Clinical and microbiological features ofnecrotizing fasciitis. J Clin Microbiol 33:2382–2387, 1995
5. Woodburn KR, Ramsay G, Gillespie G, et al: Retroperitonealnecrotizing fasciits. Br J Surg 79:342–344, 1992
6. Sudarsky LA, Laschinger JC, Coppa GF, et al: Improvedresults from a standardized approach in treating patients withnecrotizing fasciitis. Ann Surg 206:661–665, 1987
7. McHenry CR, Piotrowski JJ, Petrinic D, et al: Determinants ofmortality for necrotizing soft tissue infections. Ann Surg221:558–565, 1995
8. Francis KR, Lamaute HR, Davis JM, et al: Implications forrisk factors in necrotizing fasciits. Am Surg 59:304–308, 1993
9. Cave DR, Robinson WR, Brotschi EA: Necrotizing fasciitsfollowing percutaneous endoscopic gastrostomy. GastrointestEndosc 32:294–296, 1986
10. Person JL, Brower RA: Necrotizing fasciitis/myositis followingpercutaneous endoscopic gastrostomy. Gastrointest Endosc32:309, 1986
11. Grief JM, Ragland JJ, Ochsner MG, Riding R: Fatal necrotiz-ing fasciitis complicating percutaneous endoscopic gastros-tomy. Gastrointest Endosc 32:292–293, 1986
12. Korula J, Rice HE: Necrotizing fasciits and percutaneousendoscopic gastrostomy. Gastrointest Endosc 33:335–336, 1987
13. Haas DW, Dharamaraja P, Morrision JG, Potts JR: Necrotiz-ing fasciitis following percutaneous endoscopic gastrostomy.Gastrointest Endosc 34:487–488, 1988
14. Dietesheim JA, Richards W, Sharp K: Fatal and diastrouscomplications following percutaneous endoscopic gastrostomy.Am Surg 55:92–96, 1989
NECROTIZING FASCIITIS
1141Digestive Diseases and Sciences, Vol. 46, No. 5 (May 2001)

15. Martindale R, Witte M, Hodges G, et al: Necrotizing fasciits asa complication of percutaneous endoscopic gastrostomy. JPEN11:583–585, 1987
16. Marsman JW, Hoedmaker HP: Necrotizing fasciitis: Fatalcomplication of a migrated biliary stent. Aust Radiol1996:40:80–83,
17. McHenry CR, Brandt CP, Piotrowski JJ, et al: Idiopathicnecrotizing fasciits: Recognition incidence, and outcome oftherapy. Am Surg 60:490–494, 1994
18. Lille ST, Sato TT, Engrav LH, et al: Necrotizing soft tissueinfections: obstacles in diagnosis. J Am Coll Surg 182:7–11,1996
ROY ET AL
1142 Digestive Diseases and Sciences, Vol. 46, No. 5 (May 2001)





























